jc.2013-文献
Evidence Acquisition:The major source of data acquisition included PubMed research strategies. Original articles,systematic reviews and meta-analyses,and included relevant citations were screened.
Evidence Synthesis:In untreated GHD,cardiovascular risk is increased due to abnormal lipid profile (increased total and low-density lipoprotein cholesterol,increased triglycerides,and reduced high-density lipoprotein cholesterol)and impaired glucose metabolism.Emerging cardiovascular risk factors/markers such as proinflammatory cytokines,C-reactive protein,and adipokines are also increased in GHD patients.Increased cardiovascular morbidity and mortality have also been re-ported in GHD.GH treatment has been shown to improve both traditional and emerging cardio-vascular risk factors and markers.However,evidence on the effects of GH replacement on cardio-vascular events and mortality is limited.
Conclusion:The GHD population may be considered at high cardiovascular risk,and GH substitu-tion may be expected to bring an added value to patients with hypopituitarism in terms of car-diovascular protection.However,there is too limited evidence(rarely coming from randomized and controlled studies)to recommend GH treatment based on the cardiovascular status of the patients.(J Clin Endocrinol Metab99:18–29,2014)
G H deficiency(GHD)of the adult is now recognized as a
well-defined clinical condition,characterized by sev-eral signs and symptoms such as reduced quality of life(1–3) and physical fitness(4),osteopenia,osteoporosis(5–8),and increased cardiovascular risk(9),which are at least partially reversible by GH substitution(1–10).It is still an open issue whether GH replacement may be able not only to improve cardiovascular risk factors but also to decrease cardiovascu-lar morbidity and mortality.The aim of this review was to updatethecurrentknowledgeonthecardiovascularriskpro-file in adults with GHD with or without GH replacement.Traditional and emerging cardiovascular risk factors(Figure 1),as well as their impact on clinical endpoints,will be evaluated.
Traditional Cardiovascular Risk Factors in GHD Adults
Lipids
Adults with GHD often have significant changes in their lipid profile(11).Indeed,increased low-density li-
ISSN Print0021-972X ISSN Online1945-7197 Printed in U.S.A.
Copyright?2014by The Endocrine Society Received May30,2013.Accepted October7,2013. First Published Online November11,2013Abbreviations:ADMA,asymmetrical dimethylarginine;BMI,body mass index;CRP,C-re-active protein;GHD,GH deficiency;HDL,high-density lipoprotein;LDL,low-density lipo-protein;LV,left ventricular;MetS,metabolic syndrome;PAPP-A,pregnancy-associated plasma protein A;sdLDL,small dense LDL.
https://www.360docs.net/doc/067488158.html, J Clin Endocrinol Metab,January2014,99(1):18–29doi:10.1210/jc.2013-2394
poprotein(LDL)and triglycerides have been documented in both sexes,whereas decreased high-density lipoprotein (HDL)has been observed only in women;the elevated total cholesterol/HDL ratio regarded both men and women(11).No differences in additional risk factors, such as lipoprotein(a)(12,13)and apolipoprotein B(14), were found between GHD and controls(11).
GH replacement was able to positively affect lipid pro-file in GHD patients:total cholesterol and LDL signifi-cantly decreased,whereas HDL increased(15–18)(Table
1).GH replacement may also de-
crease triglycerides(17).However,
Florakis et al(19)showed that GH
treatment was able to decrease total
cholesterol and LDL and to slightly
increase HDL,but no change was
observed for triglycerides.A meta-
analysis including37trials con-
firmed the positive effects of GH
treatment on total and LDL choles-
terol but did not find any effect on
triglycerides(20).Also,in a recent
long-term prospective study,15
years of GH replacement reduced
total cholesterol and LDL and in-
creased HDL,but no significant vari-
ations were observed for triglycer-
ides(21).Therefore,even if some
studies did not find an improvement
in lipid profile with long-term GH
replacement(22,23),it can be sum-
marized that GHD adults have a high
cardiovascular risk lipid profile at
baseline and that in most of the stud-
ies,GH treatment tends to reverse to
normal the total and LDL/HDL cho-
lesterol levels.
Two other emerging issues de-
serve to be addressed.In fact,there is
recent evidence that small dense LDL
(sdLDL)may be independent cardio-
vascular risk factors(24).A small
study by Rizzo et al(25)found that
sdLDLs were common among pa-
tients with GHD and that GH re-
placement did not affect LDL size.
Conversely,Salman et al(26)did not
find any difference in sdLDLs be-
tween subjects with GHD and con-
trols.The second issue is whether
GH may have additive effects on
3-hydroxy-3-methylglutaryl coen-
zyme A reductase inhibitor(statin) treatment.Interestingly,a synergistic,rather than addi-tive,and proportional to baseline cholesterol value effect of this combination was reported(27).Therefore,in hy-percholesterolemic GHD,clinicians should carefully bal-ance relative risk/benefit profiles and eventually combine the two treatments.
Glucose metabolism and insulin resistance Adult patients with GHD have increased visceral fat mass and often have an impaired glucose metabolism to-
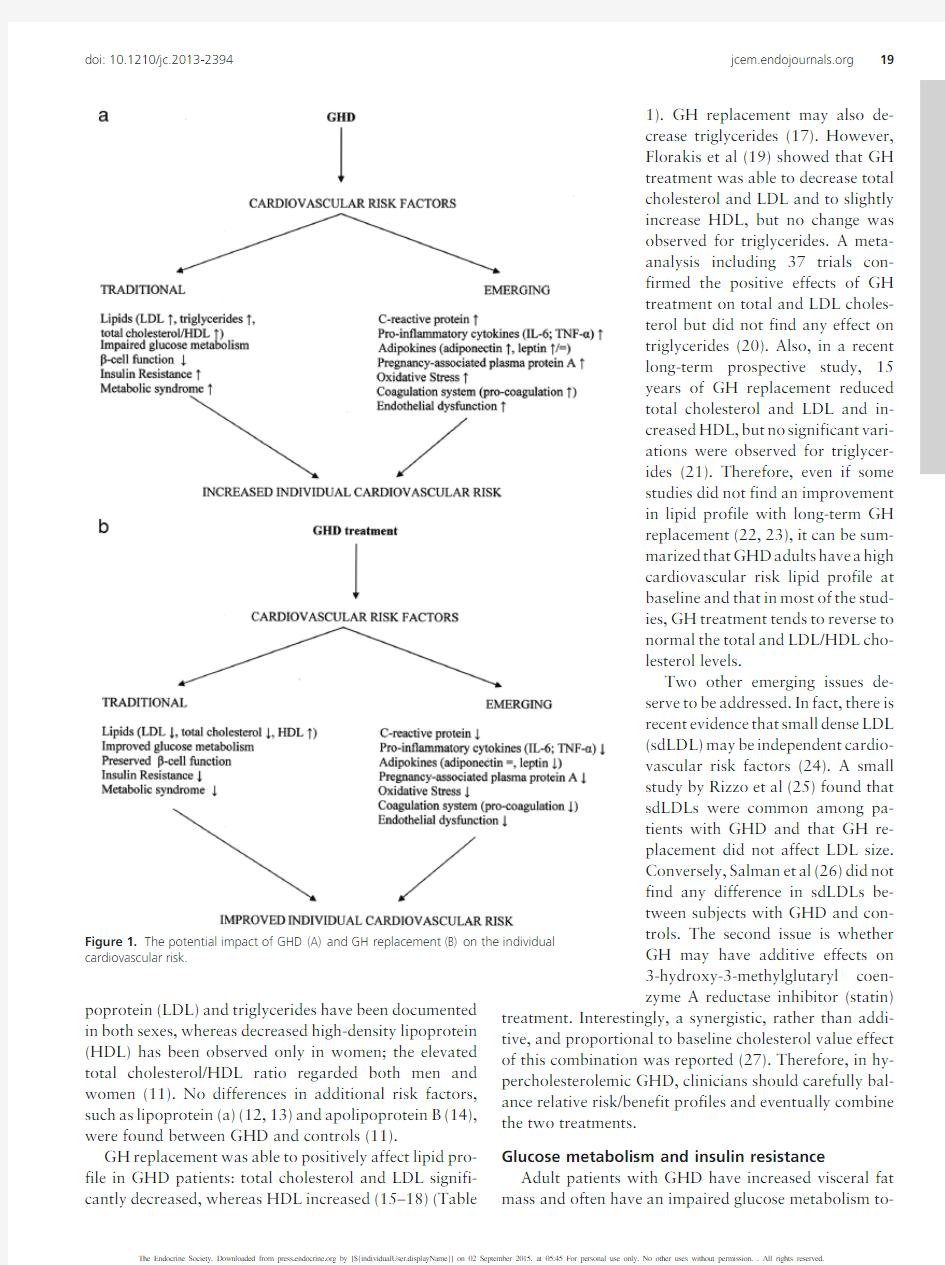
Figure1.The potential impact of GHD(A)and GH replacement(B)on the individual
cardiovascular risk.
doi:10.1210/https://www.360docs.net/doc/067488158.html,19
gether with insulin resistance(9,10).The glycometabolic effects of GH therapy in GHD are conflicting.Indeed, some studies have documented an improvement in glucose metabolism and insulin sensitivity(15,28,29),but other investigations have observed no effect(30,31)or at best a marginal effect(32–35).These conflicting data seem to be due to the duration of treatment.A short-term(up to 1y)GH substitution seems to deteriorate glucose metab-olism(32,36,37),whereas long-term treatment did not lead to significant variations in glucose and insulin me-tabolism(38);on the contrary,slightly lower fasting glu-cose levels were observed(39).In most of the long-term studies,an initial increase in glucose and insulin levels with an impairment of insulin sensitivity could be ob-served.This glycometabolic deterioration at the begin-ning of GH substitution may be caused by a decline of peripheral glucose utilization(40).After initial deteri-oration,glucose tolerance can improve,with glucose and insulin levels returning to baseline levels(15,41). Insulin resistance could be exacerbated acutely by GH in GHD(42),whereas it has been shown that GH re-placement decreasing visceral fat mass did not worsen insulin resistance(43).Moreover,low-dose24-to48-week GH treatment improved insulin sensitivity,pre-served?-cell function,and improved glucose metabo-lism without affecting body composition or inducing lipolysis in a small group of six adults with severe GHD, likely via an increased IGF-1bioavailability(44).
In synthesis,glycometabolic effects of GH substitution seem to be biphasic(mimicking what is observed for bone effects),leading initially to deterioration of an already al-tered glucose metabolism,but in the long-term,particu-larly with low-dose GH,an improvement of glucose han-dling is reported.
Metabolic syndrome(MetS)
The metabolic syndrome(MetS)is a cluster of risk fac-tors(visceral obesity,impaired glucose metabolism,low HDL,high triglycerides,and hypertension)mainly asso-ciated with insulin resistance,inflammation,and endo-thelial dysfunction(45).MetS predicts the development of diabetes(41)and is strongly associated with cardiovascu-lar diseases in the general population(45,46)and in di-abetic patients(47).The prevalence of MetS is increased in GHD patients(48).van der Klaauw et al(48)documented that GHD patients had a prevalence of MetS more than 2-fold higher when compared with the general popula-tion,mainly due to an increased prevalence of hyperten-sion,abdominal obesity,and triglyceride levels.Also,At-tanasio et al(49)found that MetS prevalence was increased in GHD patients.Interestingly,lean individuals with GHD had larger waist circumference and more ab-dominal adiposity with a proportional increase in sc and visceral tissue with respect to control subjects.Also,adi-pose tissue of obese GHD patients expressed many pro-inflammatory markers(50).
Table1.Summary of Studies of the Effects of GH Treatment on Lipid Profile
First Author (Ref.)No.of
patients Mean GH Dose
Duration of
Treatment,y Outcome
Chrisoulidou(22)120.7mg/d7TC,LDL,HDL,and TG unchanged Florakis(19)240.3mg/d 1.5TC2,LDL2,HDL1,TG
unchanged
G?therstr?m(17)118Initially0.98mg/d,gradually
titrated to0.48mg/d
5TC2,LDL2,HDL1,TG2
Svensson(15)11Initially1.1mg/d,gradually
titrated to0.61mg/d 7LDL2,HDL1,TC and TG
unchanged
Arwert(34)23Initially0.97mg/d,gradually
titrated to0.4mg/d 10TC2(5th year),LDL2,HDL1,TG
unchanged
van der Klaauw (16)63Initially0.2mg/d,gradually
titrated to0.5mg/d
7TC2,LDL2,HDL1,TG
unchanged
Colson(18)124Initially0.3mg/d,gradually
titrated to0.5mg/d 5TC2,LDL2,HDL and TG
unchanged
Monson(27)610.32mg/d1TC2,LDL2,HDL and TG
unchanged
G?therstr?m(53)87Initially0.98mg/d,gradually
titrated to0.47mg/d 10TC2,LDL2,HDL1,TG
unchanged
Colao(54)226?g/kg?d5TC2,HDL1,TG2 Spielhagen(23)81Initially0.29mg/d,gradually
titrated to0.43mg/d
10TC and LDL unchanged
Elbornsson(21)109Initially0.55mg/d,gradually
titrated to0.4mg/d 15TC2,LDL2,HDL1,TG
unchanged
TC,total cholesterol;LDL,low-density lipoprotein;HDL,high-density lipoprotein;TG,triglycerides;2significant decrease;1significant increase. 20Gazzaruso et al Growth Hormone and the Heart J Clin Endocrinol Metab,January2014,99(1):18–29
In a large study,waist circumference decreased after1 and2years of GH treatment,respectively,but remained unchanged after5years of GH substitution when com-pared with baseline(51,52).G?therstr?m et al(53)ob-served that the reduction in body fat,after correction for age and sex,was sustained during10-year GH treatment. In addition,there was a sustained improvement in serum lipid profile and glycated hemoglobin(53).The response to treatment of HDL and body composition were more marked in men,whereas women had more marked reduc-tion in glycated hemoglobin(53).Other studies suggested that GH replacement did not affect the risk of type2di-abetes in GHD with normal body mass index(BMI)(52). However,in severe GHD with increased prevalence of cardiovascular risk factors and surrogate markers of early atherosclerosis(intima-media thickness),5-year GH re-placement improved all metabolic parameters,reducing insulin resistance(54).
MetS is clinically an appropriate label for patients with GHD who do not often have a prominently altered car-diometabolic feature but show a cluster of mild altera-tions.There has been a long debate on MetS being an independent clinical entity(55,56);in our opinion,GHD patients are often good examples of MetS clinical expres-sivity,and what could appear relatively modest changes in cardiometabolic parameters determined by GH substitu-tion should be read in the context of a global improvement of MetS and of the added cardiovascular risk that MetS is bearing.
Traditional Cardiovascular Risk Factors During the Transition Period From Adolescence to Adulthood
Discontinuation of GH during the transition phase in GHD increased fat mass and diastolic blood pressure,with significant worsening in total and LDL cholesterol(57, 58).Beneficial effects on fat mass and LDL/HDL ratio of continuing GH replacement during the transition phase in childhood onset-GHD patients was also reported(59). Other authors,but not all(60,61),showed a significant increase in fat mass also in partial GHD after GH discon-tinuation.Therefore,suspending GH during the transition period may cause unfavorable changes in cardiometabolic risk factors that may improve when GH treatment is re-sumed.No data are available for emerging cardiovascular risk factors in the GHD transition phase.
Emerging Cardiovascular Risk Factors
C-Reactive protein(CRP)
CRP is a marker of inflammation and is now considered an independent cardiovascular risk factor(62).Elevated CRP levels are associated with negative cardiovascular prognosis(62,63)and can predict the development of type 2diabetes(64,65),hypertension(66),and MetS(67).
Both lean and obese subjects with GHD have an ap-proximately4-to5-fold increase in CRP(50),suggesting a proinflammatory state linked directly to GHD(68,69). Earlier studies had provided conflicting results on the ef-fect of GH therapy on CRP.Bollerslev et al(70)showed that GH replacement was associated with reduced CRP, independently of weight or immune-modulating actions, even greater than that observed in a previous controlled study that enrolled only women(71).A significant nega-tive correlation between CRP and IGF-1at baseline and between the changes in CRP and IGF-1after GH therapy was documented(71),whereas a decrease in body fat did not predict changes in CRP during GH treatment.Finally, Deepak et al(72)recently reported a significant GH-me-diated reduction in CRP levels in GHD that was not af-fected by changes in body composition.Therefore,GHD is likely a proinflammatory state(see also below),and GH treatment may interrupt the vicious circle linking endo-crine abnormality,inflammation,and atherosclerosis. Proinflammatory cytokines
Several proinflammatory factors may be involved in pathophysiological mechanisms of GHD cardiovascular complications.Among them,IL-6and TNF-?may have a major role in causing endothelial dysfunction(73,74).
Increased IL-6levels have been documented in patients with GHD independently of BMI or obesity;in addition, GH replacement was able to effectively reduce IL-6pro-duction from monocytes(75).Bollerslev et al(70)showed that IL-6was increased in GHD and that GH reduced IL-6 similarly to CRP in men.
Also,TNF-?was significantly higher in children with GHD than in controls;in addition,long-term GH therapy was able to effectively reduce its levels.These data sug-gested that GH could play an inhibitory role on TNF-?release in humans(76).
Adipokines
Adipose tissue produces a large variety of peptides with endocrine,paracrine,or autocrine actions called adipo-kines(72–74,77,78).The most abundant adipokine is adiponectin(72–74),which is decreased in obese patients, positively associated with insulin sensitivity,and inversely associated with the risk of type2diabetes(79,80),exert-ing anti-inflammatory,antiatherogenic,and insulin-sen-sitizing effects(78,79).Leptin is another important adi-pokine involved in the central control of energy homeostasis(77,78);its activity is modulated by the sol-uble isoform of its receptor(78).Leptin is usually elevated
doi:10.1210/https://www.360docs.net/doc/067488158.html,21
in obese subjects and can play an atherogenic,prothrom-botic,and angiogenic role by stimulating vascular inflam-mation,oxidative stress,and smooth muscle hypertrophy (78).
Recently,it was observed that GHD was associated with an altered adipokine protein expression pattern and an increased adipocyte diameter:this may predispose the adipose tissue to hypoxia and chronic inflammation(50, 81).Conflicting data are available in the literature on lep-tin levels in GHD patients.Some studies found that levels were higher in GHD patients than in controls(81–84),but others did not(85).One study in humans also failed to detect any effect of GH on circulating leptin concentra-tions(86).In children with GHD,adiponectin and soluble leptin receptor levels were higher than in controls,whereas no differences in other adipokines were observed(87).A 12-month trial of GH replacement caused a decrease in leptin levels concomitantly with a restoration of normal IGF-1concentrations(87).After1year GH also an in-crease in adiponectin levels was observed(83). Pregnancy-associated plasma protein A(PAPP-A) PAPP-A is a high-molecular-weight metalloproteinase produced by human artery vascular smooth muscle cells, which degrades IGF binding protein-4,increasing the lev-els of local unbound IGF-1(88).PAPP-A is expressed in eroded and ruptured atherosclerotic plaques and has been proposed as a marker of increased risk of atherothrom-botic events(88).Elevated PAPP-A levels were observed in acute coronary syndrome(89)and ischemic stroke(90).
PAPP-A levels were higher in GHD patients than in controls,and GH replacement lowered PAPP-A levels (91),which correlated positively with BMI and waist-hip ratio before and after treatment(91).Li et al(92)recently confirmed that in GHD patients,PAPP-A and CRP sig-nificantly increased with respect to matched controls with-out correlation between their levels.The study by Li et al suggested,but did not prove,that the rise of serum PAPP-A was a direct response to decreased systemic IGF-1and hypothesized that PAPP-A could play a role in the devel-opment of atherosclerosis in GHD(10,92).
These recent studies interestingly updated our knowl-edge on the interaction between GH and cytokines.In fact, they somewhat upgraded the role of the latter from simple markers of altered body composition and increased fat cell activity to a possible causative link between the lack of GH/IGF-1and cardiovascular disease.
Oxidative stress
Oxidative stress seems to play a major role in the gen-esis and development of atherosclerosis(73,74).The ac-tion of oxidative stress on atherosclerosis is mediated by lipid peroxidation,in particular of LDL(74).
Conflicting data are available on oxidative stress in pa-tients with GHD.Smith et al(93)found that oxidative stress did not play a significant role in the proatherogenic state of patients with GHD,but González-Duarte et al(94) recently observed an important increase in oxidated LDL in these subjects.Some studies showed that short-term GH administration reduced lipid peroxidation in GHD(95, 96).
Coagulation system
Thrombosis plays a major role in the development of cardiovascular events due to an excess of procoagulative factors or impaired fibrinolysis(97).Therefore,coagula-tion abnormalities can be risk factors for cardiovascular morbidity and mortality(98).In patients with GHD,a reduced protein S activity that was normalized after GH replacement was recently documented(99).Data regard-ing the association between GHD and impaired fibrino-lysis are conflicting.Some,but not all,studies found an impaired fibrinolytic activity(due to an excess of plasmin-ogen activator inhibitor1and fibrinogen)that did im-prove after GH replacement(100–103).
Endothelial dysfunction
Endothelial dysfunction is crucial in the development of atherothrombosis and progression to cardiovascular dis-eases(104).Asymmetrical dimethylarginine(ADMA)is an endogenous inhibitor of endothelial nitric oxide syn-thase,an enzyme involved in correct endothelial function (105),considered a marker of endothelial dysfunction and potential risk factor for atherothrombosis(105).In GHD, an increase in ADMA was documented(106),and GH replacement reduced ADMA and improved endothelial function(107).
Cardiac function and morphology
Impaired cardiac functional reserve(108,109)associ-ated with chronotropic incompetence and impaired pres-sure-generating capacity was reported in severe GHD (110).Earlier investigations also documented reduced left ventricular(LV)mass,abnormalities in contractility and stroke volume index,reduced ejection fraction,and dia-stolic dysfunction(9,111).A meta-analysis showed that GH replacement was associated with positive effects on LV mass,intraventricular septum,diastolic function,and stroke volume index,whereas no effects were observed on systolic parameters(9,112).In a5-year follow-up study, Cenci et al(113)documented a post-GH improvement in exercise capacity and maximum oxygen uptake.In addi-tion,in that study LV mass increased progressively during
22Gazzaruso et al Growth Hormone and the Heart J Clin Endocrinol Metab,January2014,99(1):18–29
GH replacement,with no significant changes in other pa-rameters(113).However,a magnetic resonance imaging study showed that untreated GHD was not associated with impaired systolic function or reduced LV mass,and that1year only of GH replacement at physiological doses did not affect cardiac mass or function(114).Similar re-sults were obtained in another investigation,even if a sig-nificant decrease in amino-terminal pro-brain natriuretic peptide,a marker of heart failure,was observed after GH replacement(115).Two recent studies did not observe significant improvement in cardiac function or morphol-ogy with different dose regimens of GH(low,moderate,or high dose)during a quite short period of treatment(1y) (116,117).
Mortality and Cardiovascular Events in Adult GHD
Retrospective studies suggested that hypopituitarism may be associated with significant increased mortality,espe-cially in women(118–123).These studies showed a high prevalence of untreated GHD,whereas other hormone deficiencies were conventionally replaced.This increased mortality seemed to be particularly associated with car-diovascular and cerebrovascular disease(118–123). These findings suggested that a GHD state may expose to and worsen the risk for cardiovascular disease,even if other factors,including GHD etiology(especially cranio-pharyngioma)and untreated estrogen deficiency could have been additional independent risk factors.
Stochholm et al(124)found significantly increased morbidity in GHD patients.This increased morbidity was due to several risk factors,including unfavorable meta-bolic profile,leading to cardiovascular diseases in both genders(124).However,at present there are no data on the real incidence of cardiovascular events in large cohorts of GHD patients.Assessment of coronary calcium depos-its by computed tomography has been recently validated as a reliable tool to estimate the risk for the development of coronary artery disease(125).Recently,coronary cal-cium deposits were associated with low IGF-1levels in patients with untreated GHD,and this was observed also in subjects with low Framingham score and independently of hypertension or insulin resistance(126).
By using the Framingham and European Society of Car-diology scoring systems,Schneider et al(127)observed that GH replacement could reduce the cardiovascular risk by one-half within2years with high cholesterol,elevated systolic blood pressure,male sex,and low IGF-1levels being potential predictors of positive response(127).In-terestingly,the cardiovascular risk remained significantly higher in controls than in treated patients after4years of follow-up;this suggested a sustained effect of GH therapy. Another study showed that GH replacement could pro-vide protection from fatal myocardial infarctions with rapid time course(121).Data from the KIMS database indicated that mortality rates for GH-replaced patients were similar to those of the background population(128). Furthermore,a meta-analysis of blinded,randomized, placebo-controlled trials showed that GH replacement may have beneficial effects on cardiovascular risk,show-ing improvement in lean and fat mass,total and LDL cho-lesterol,and diastolic pressure(20).However,long-term controlled trials on global mortality and the impact of GH treatment on cardiovascular morbidity and mortality are lacking.
Recently,van Bunderen et al(129)demonstrated an increased mortality rate for all-cause mortality in adult GHD treated with GH;in particular,an elevated mortality due to cardiovascular events was observed in women.On the contrary,mortality due to malignancies was not in-creased in adults receiving GH treatment(129).Gaillard et al(130)analyzed the cause-specific mortality in GHD adults on GH replacement and found that malignancies and cardiovascular and cerebrovascular disease were the most common causes of death.Nevertheless,mortality from cardiovascular diseases was lower in this study than in previous studies(130).It is not clear whether the ob-served difference in cardiovascular mortality between these studies may be the result of GH replacement only or of improved medical care and adequate control of hyper-tension and hyperlipidemia.Cerebrovascular mortality remained elevated in GH-treated patients.
Summary of Recent Findings,Open Issues, and Conclusions
Recent findings
The recent meta-analysis by Elbornsson et al(21)con-firmed the positive effect of GH treatment on total cho-lesterol,LDL,and HDL,whereas no positive effects were observed on triglycerides.In addition,it was observed that in patients treated with GH,statin therapy could have a synergistic rather than additive effect on cholesterol levels (27).Long-term treatment with GH was shown to im-prove the constellation of metabolic parameters of MetS and to have positive effects on body composition(38–40, 43,44,48,49).It has also recently emerged that GH re-placement can improve inflammation,as documented by a reduction in CRP(70,72),TNF-?(76),and IL-6(70). Positive effects of GH replacement were also observed for several adipokines,such as adiponectin,leptin,and
doi:10.1210/https://www.360docs.net/doc/067488158.html,23
PAPP-A(81),which may represent not only a marker but also the possible link between GHD,inflammation,and atherosclerosis(10,92).Conversely,the most recent in-terventional studies failed to consistently show GH-me-diated improvement in cardiac and prognostic outcomes (114–117,125–127).
Open issues
GHD is associated with an unfavorable pattern of tra-ditional cardiovascular risk factors.Moreover,nontradi-tional and emerging markers of cardiovascular risk are also altered in adult GHD patients.As a consequence, GHD is characterized by increased cardiovascular mor-tality and morbidity.GH replacement is expected to im-prove cardiovascular outcomes of GHD patients.In fact, it was reported by many authors to positively affect both traditional and emerging cardiovascular risk factors.Al-though initial evidence suggested that these results were linked to a reduced global cardiovascular mortality and morbidity in GHD patients,specific,long-term,and large trials are lacking.However,with our current knowledge about positive effects of GH,albeit on surrogate cardio-vascular markers,it might be difficult to get acceptance/ approval for(placebo)controlled long-term studies that may be considered unethical.Moreover,interpretation of available studies on hard cardiovascular endpoints is af-fected by several factors.First,the doses used for GH re-placement and the cutoff for interpreting normalization of IGF-1have been significantly lowered over time(131–134).In fact,from early weight-based dosing derived from pediatric care up to0.07–0.1IU/kg daily(135–137), mainly due to side effects(related to fluid retention),adult practice shifted to individualized starting low doses,gen-erally less than1IU(200–300?g)per day(131),gradually titrated until obtaining target IGF-1in the normal range for age(131,134).The use of very low doses of GH min-imized side effects while producing similar or even better (44)metabolic effects than high doses previously used.In fact,for all metabolic targets,possibly a U-shaped curve may be envisaged with excessively high GH doses leading to an acromegaly-like effect(138–142).Therefore,for pa-tients with longer follow-up,beneficial effects of current low-dose GH regimens may be counterbalanced by po-tentially harmful effects of initially used high-dose GH. Second,cardiovascular events remain quite a rare occur-rence in GHD,which in turn is a rare condition(9),and therefore it is difficult to design studies with these end-points.On the other hand,this is not a big issue for sur-rogate markers,the changes of which may well occur,as reported in our review,very early or after relatively short-term trials of GH treatment.In this regard,studies with very long follow-up published in the last few years are reassuring,showing a consistency of the effects of GH on cardiovascular markers/risk factors between positive short-time and long-time responses,and even(as happens for bone effects)(138,143)a change from negative effects in the short term to positive effects in the long term(glu-cose metabolism).Third,age of onset of GHD(144)as well as age per se of the patients may be relevant to the definition of a population at high cardiovascular risk,as well as to the expected vs observed events,particularly in terms of length of necessary follow-up(clearly more pro-longed for young patients)and in terms of concomitant/ coexistent risk factors with high prevalence in the general population(hypertension,diabetes,and obesity)not nec-essarily linked to GHD.Unfortunately,due to the relative rarity of the disease,mixed populations are involved in the studies in terms of age of onset,sex(females require higher GH doses than males to achieve the same biological ef-fects)(9),etiology(post-Cushing,acromegaly,or cranio-pharyngioma are subgroups of patients at pre-existing high cardiovascular risk),and additional pituitary defects (eg,cortisol deficiency may often be over-replaced,and this may represent an additional cardiovascular risk fac-tor)(145).Therefore,due to this inhomogeneous compo-sition of the group of GHD adults and awaiting subgroup-specific guidelines,every patient should be evaluated at the individual level.Fourth,the types of studies available on the effects of GH on cardiovascular risk factors/markers but especially on cardiovascular events are also of mixed quality and generally characterized by open,uncontrolled, and observational features.Therefore,selection bias as well as causality of the reported observations can rarely be ruled out.Finally,do we have enough evidence to consider reduction of cardiovascular risk an indication for pre-scribing GH to GHD patients(146)?This issue is still very sensitive because of the cost of treatment and its potential side effects.Unfortunately,8years after our previous re-view on the topic(9)and despite many further studies having been published,there is still no definitive answer to this question,and therefore cardiovascular effects of GH therapy in GHD should still be considered an expected benefit of treatment but not an indication to it. Conclusions
Therefore,in conclusion,the GHD population may be considered at high cardiovascular risk,and GH substitu-tion may be expected to bring an added value to patients with hypopituitarism in terms of cardiovascular protec-tion.However,due to limitations of the available data there is too limited evidence(rarely coming from random-ized/controlled studies)to recommend GH treatment based on the cardiovascular status of the patients.
24Gazzaruso et al Growth Hormone and the Heart J Clin Endocrinol Metab,January2014,99(1):18–29
Acknowledgments
Address all correspondence and requests for reprints to:Prof Andrea Giustina,Chair of Endocrinology,University of Brescia, A.O.Spedali Civili di Brescia,Scala7,Piano2,Piazzale Spedali Civili1,25123Brescia,Italy.E-mail:a.giustina@libero.it.
The study was partially supported by MIUR(Italian Ministry for Education University and Research)and the University of Brescia.
Disclosure Summary:The authors have nothing to disclose.
References
1.Rosilio M,Blum WF,Edwards DJ,et al.Long-term improvement of
quality of life during growth hormone(GH)replacement therapy in adults with GH deficiency,as measured by questions on life satis-faction-hypopituitarism(QLS-H).J Clin Endocrinol Metab.2004;
89(4):1684–1693.
2.Koltowska-H?ggstr?m M,Mattsson AF,Shalet SM.Assessment of
quality of life in adult patients with GH deficiency:KIMS contri-bution to clinical practice and pharmacoeconomic evaluations.Eur J Endocrinol.2009;161(suppl1):S51–S64.
3.J?rgensen AP,Fougner KJ,Ueland T,et al.Favorable long-term
effects of growth hormone replacement therapy on quality of life, bone metabolism,body composition and lipid levels in patients with adult-onset growth hormone deficiency.Growth Horm IGF Res.
2011;21(2):69–75.
4.Widdowson WM,Gibney J.The effect of growth hormone replace-
ment on exercise capacity in patients with GH deficiency:a meta-analysis.J Clin Endocrinol Metab.2008;93(11):4413–4417.
5.Doga M,Bonadonna S,Gola M,Mazziotti G,Nuzzo M,Giustina
A.GH deficiency in the adult and bone.J Endocrinol Invest.2005;
28(8):18–23.
6.Holmes SJ,Economou G,Whitehouse RW,Adams JE,Shalet SM.
Reduced bone mineral density in patients with adult onset growth hormone deficiency.J Clin Endocrinol Metab.1994;78:669–674.
7.Canalis E,Giustina A,Bilezikian JP.Mechanisms of anabolic ther-
apies for osteoporosis.N Engl J Med.2007;357(9):905–916.
8.Rosén T,Hansson T,Granhed H,Szucs J,Bengtsson BA.Reduced
bone mineral content in adult patients with growth hormone defi-ciency.Acta Endocrinol(Copenh).1993;129:201–206.
9.Gola M,Bonadonna S,Doga M,Giustina A.Clinical review:growth
hormone and cardiovascular risk factors.J Clin Endocrinol Metab.
2005;90(3):1864–1870.
10.Gola M,Giustina A.Growth hormone deficiency and cardiovascu-
lar risk:do we need additional markers?Endocrine.2012;42(2): 240–242.
11.Abdu TA,Neary R,Elhadd TA,Akber M,Clayton RN.Coronary
risk in growth hormone deficient hypopituitary adults:increased predicted risk is due largely to lipid profile abnormalities.Clin En-docrinol(Oxf).2001;55(2):209–216.
12.Gazzaruso C,Coppola A,Montalcini T,et al.Lipoprotein(a)and
homocysteine as genetic risk factors for vascular and neuropathic diabetic foot in type2diabetes mellitus.Endocrine.2012;41(1):89–
95.
13.Gazzaruso C,Garzaniti A,Falcone C,Geroldi D,Finardi G,Fratino
P.Association of lipoprotein(a)levels and apolipoprotein(a)phe-notypes with coronary artery disease in type2diabetic patients and in non-diabetic subjects.Diabet Med.2001;18(7):589–594.
14.Robinson JG,Wang S,Jacobson TA.Meta-analysis of comparison
of effectiveness of lowering apolipoprotein B versus low-density li-poprotein cholesterol and nonhigh-density lipoprotein cholesterol for cardiovascular risk reduction in randomized trials.Am J Cardiol.
2012;110(10):1468–1476.15.Svensson J,Fowelin J,Landin K,Bengtsson BA,Johansson JO.Ef-
fects of seven years of GH-replacement therapy on insulin sensitivity in GH-deficient adults.J Clin Endocrinol Metab.2002;87(5):2121–2127.
16.van der Klaauw AA,Romijn JA,Biermasz NR,et al.Sustained
effects of recombinant GH replacement after7years of treatment in adults with GH deficiency.Eur J Endocrinol.2006;155(5):701–708.
17.G?therstr?m G,Svensson J,Koranyi J,et al.A prospective study of
5years of GH replacement therapy in GH-deficient adults:sustained effects on body composition,bone mass,and metabolic indices.
J Clin Endocrinol Metab.2001;86(10):4657–4665.
18.Colson A,Brooke AM,Walker D,et al.Growth hormone deficiency
and replacement in patients with treated Cushing’s disease,prolacti-nomas and non-functioning pituitary adenomas:effects on body composition,glucose metabolism,lipid status and bone mineral density.Horm Res.2006;66(6):257–267.
19.Florakis D,Hung V,Kaltsas G,et al.Sustained reduction in circu-
lating cholesterol in adult hypopituitary patients given low dose titrated growth hormone replacement therapy:a two year study.
Clin Endocrinol(Oxf).2000;53(4):453–459.
20.Maison P,Griffin S,Nicoue-Beglah M,Haddad N,Balkau B,Chan-
son P.Impact of growth hormone(GH)treatment on cardiovascular risk factors in GH-deficient adults:a Metaanalysis of Blinded,Ran-domized,Placebo-Controlled Trials.J Clin Endocrinol Metab.
2004;89(5):2192–2199.
21.Elbornsson M,G?therstr?m G,Bos?us I,Bengtsson B?,Johanns-
son G,Svensson J.Fifteen years of GH replacement improves body composition and cardiovascular risk factors.Eur J Endocrinol.
2013;168(5):745–753.
22.Chrisoulidou A,Beshyah SA,Rutherford O,et al.Effects of7years
of growth hormone replacement therapy in hypopituitary adults.
J Clin Endocrinol Metab.2000;85(10):3762–3769.
23.Spielhagen C,Schwahn C,M?ller K,et al.The benefit of long-term
growth hormone(GH)replacement therapy in hypopituitary adults with GH deficiency:results of the German KIMS database.Growth Horm IGF Res.2011;21(1):1–10.
24.Stalenhoef AF,de Graaf J.Association of fasting and nonfasting
serum triglycerides with cardiovascular disease and the role of rem-nant-like lipoproteins and small dense LDL.Curr Opin Lipidol.
2008;19(4):355–361.
25.Rizzo M,Trepp R,Berneis K,Christ ER.Atherogenic lipoprotein
phenotype and low-density lipoprotein size and subclasses in pa-tients with growth hormone deficiency before and after short-term replacement therapy.Eur J Endocrinol.2007;156(3):361–367. 26.Salman S,Uzum AK,Telci A,Alagol F,Ozbey NC.Serum adipo-
kines and low density lipoprotein subfraction profile in hypopitu-itary patients with growth hormone deficiency.Pituitary.2012;
15(3):386–392.
27.Monson JP,J?nsson P,Koltowska-H?ggstr?m M,Kourides I.
Growth hormone(GH)replacement decreases serum total and LDL-cholesterol in hypopituitary patients on maintenance HMG CoA reductase inhibitor(statin)therapy.Clin Endocrinol(Oxf).2007;
67(4):623–628.
28.Hwu CM,Kwok CF,Lai TY,et al.Growth hormone(GH)replace-
ment reduces total body fat and normalizes insulin sensitivity in GH-deficient adults:a report of one-year clinical experience.J Clin Endocrinol Metab.1997;82(10):3285–3292.
29.Yuen KC,Dunger DB.Impact of treatment with recombinant hu-
man GH and IGF-I on visceral adipose tissue and glucose homeo-stasis in adults.Growth Horm IGF Res.2006;16(suppl A):S55–S61.
30.Bülow B,Link K,Ahrén B,Nilsson AS,Erfurth EM.Survivors of
childhood acute lymphoblastic leukaemia,with radiation-induced GH deficiency,exhibit hyperleptinaemia and impaired insulin sen-sitivity,unaffected by12months of GH treatment.Clin Endocrinol (Oxf).2004;61(6):683–691.
31.Hana V,Silha JV,Justova V,Lacinova Z,Stepan JJ,Murphy LJ.The
effects of GH replacement in adult GH-deficient patients:changes in
doi:10.1210/https://www.360docs.net/doc/067488158.html,25
body composition without concomitant changes in the adipokines and insulin resistance.Clin Endocrinol(Oxf).2004;60(4):442–450.
32.Bramnert M,Segerlantz M,Laurila E,Daugaard JR,Manhem P,
Groop L.Growth hormone replacement therapy induces insulin resistance by activating the glucose-fatty acid cycle.J Clin Endocri-nol Metab.2003;88(4):1455–1463.
33.Gillberg P,Bramnert M,Thorén M,Werner S,Johannsson https://www.360docs.net/doc/067488158.html,-
mencing growth hormone replacement in adults with a fixed low dose.Effects on serum lipoproteins,glucose metabolism,body com-position,and cardiovascular function.Growth Horm IGF Res.
2001;11(5):273–281.
34.Arwert LI,Roos JC,Lips P,Twisk JW,Manoliu RA,Drent ML.
Effects of10years of growth hormone(GH)replacement therapy in adult GH-deficient men.Clin Endocrinol(Oxf).2005;63(3):310–316.
35.Spina LD,Soares DV,Brasil RR,Lobo PM,Lúcia Concei??o F,
Vaisman M.Glucose metabolism and visceral fat in GH deficient adults:two years of GH-replacement.Pituitary.2004;7(3):123–129.
36.Boguszewski CL,Meister LH,Zaninelli DC,Radominski RB.One
year of GH replacement therapy with a fixed low-dose regimen improves body composition,bone mineral density and lipid profile of GH-deficient adults.Eur J Endocrinol.2005;152(1):67–75. 37.Spina LD,Soares DV,Brasil RR,et al.Glucose metabolism and
visceral fat in GH deficient adults:1year of GH replacement.
Growth Horm IGF Res.2004;14(1):45–51.
38.Cenci MC,Concei??o FL,Soares DV,et al.Impact of5years of
growth hormone replacement therapy on cardiovascular risk factors in growth hormone-deficient adults.Metabolism.2008;57(1):121–129.
39.Roemmler J,Kuenkler M,Schneider HJ,Dieterle C,Schopohl J.
Comparison of glucose and lipid metabolism and bone mineraliza-tion in patients with growth hormone deficiency with and without long-term growth hormone replacement.Metabolism.2010;59(3): 350–358.
40.Oliveira CR,Salvatori R,Barreto-Filho JA,et al.Insulin sensitivity
and?-cell function in adults with lifetime,untreated isolated growth hormone deficiency.J Clin Endocrinol Metab.2012;97(3):1013–1019.
41.Giavoli C,Porretti S,Ronchi CL,et al.Long-term monitoring of
insulin sensitivity in growth hormone-deficient adults on substitu-tive recombinant human growth hormone therapy.Metabolism.
2004;53(6):740–743.
42.Sesmilo G,Biller BM,Llevadot J,et al.Effects of growth hormone
administration on inflammatory and other cardiovascular risk markers in men with growth hormone deficiency.A randomized, controlled clinical trial.Ann Intern Med.2000;133(2):111–122.
43.Beauregard C,Utz AL,Schaub AE,et al.Growth hormone decreases
visceral fat and improves cardiovascular risk markers in women with hypopituitarism:a randomized,placebo-controlled study.
J Clin Endocrinol Metab.2008;93(6):2063–2071.
44.Arafat AM,M?hlig M,Weickert MO,Sch?fl C,Spranger J,Pfeiffer
AF.Improved insulin sensitivity,preserved beta cell function and improved whole-body glucose metabolism after low-dose growth hormone replacement therapy in adults with severe growth hor-mone deficiency:a pilot study.Diabetologia.2010;53(7):1304–1313.
45.Nikolopoulou A,Kadoglou NP.Obesity and metabolic syndrome as
related to cardiovascular disease.Expert Rev Cardiovasc Ther.
2012;10(7):933–939.
46.Ma X,Zhu S.Metabolic syndrome in the prevention of cardiovas-
cular diseases and diabetes–still a matter of debate?Eur J Clin Nutr.
2013;67(5):518–521.
47.Gazzaruso C,Solerte SB,De Amici E,et al.Association of the met-
abolic syndrome and insulin resistance with silent myocardial isch-emia in patients with type2diabetes mellitus.Am J Cardiol.2006;
97(2):236–239.48.van der Klaauw AA,Biermasz NR,Feskens EJ,et al.The prevalence
of the metabolic syndrome is increased in patients with GH defi-ciency,irrespective of long-term substitution with recombinant hu-man GH.Eur J Endocrinol.2007;156(4):455–462.
49.Attanasio AF,Mo D,Erfurth EM,et al.Prevalence of metabolic
syndrome in adult hypopituitary growth hormone(GH)-deficient patients before and after GH replacement.J Clin Endocrinol Metab.
2010;95(1):74–81.
https://www.360docs.net/doc/067488158.html,ropec J,PenesováA,SkopkováM,et al.Adipokine protein ex-
pression pattern in growth hormone deficiency predisposes to the increased fat cell size and the whole body metabolic derangements.
J Clin Endocrinol Metab.2008;93(6):2255–2262.
51.Filipsson H,Monson JP,Koltowska-H?ggstr?m M,Mattsson A,
Johannsson G.The impact of glucocorticoid replacement regimens on metabolic outcome and comorbidity in hypopituitary patients.
J Clin Endocrinol Metab.2006;91(10):3954–3961.
52.Abs R,Feldt-Rasmussen U,Mattsson AF,et al.Determinants of
cardiovascular risk in2589hypopituitary GH-deficient adults-a KIMS database analysis.Eur J Endocrinol.2006;155(1):79–90.
53.G?therstr?m G,Bengtsson BA,Bosaeus I,Johannsson G,Svensson
J.A10-year,prospective study of the metabolic effects of growth hormone replacement in adults.J Clin Endocrinol Metab.2007;
92(4):1442–1445.
54.Colao A,Di Somma C,Spiezia S,et al.Growth hormone treatment
on atherosclerosis:results of a5-year open,prospective,controlled study in male patients with severe growth hormone deficiency.J Clin Endocrinol Metab.2008;93(9):3416–3424.
55.Kahn R,Buse J,Ferrannini E,Stern M.The metabolic syndrome:
time for a critical appraisal.Joint statement from the American Di-abetes Association and the European Association for the Study of Diabetes.Diabetologia.2005;48(9):1684–1699.
56.Simmons RK,Alberti KG,Gale EA,et al.The metabolic syndrome:
useful concept or clinical tool?Report of a WHO Expert Consul-tation.Diabetologia.2010;53(4):600–605.
57.Vahl N,Juul A,J?rgensen JO,Orskov H,Skakkebaek NE,Chris-
tiansen JS.Continuation of growth hormone(GH)replacement in GH-deficient patients during transition from childhood to adult-hood:a two-year placebo-controlled study.J Clin Endocrinol Metab.2000;85(5):1874–1881.
58.Johannsson G,Albertsson-Wikland K,Bengtsson BA.Discontinu-
ation of growth hormone(GH)treatment:metabolic effects in GH-deficient and GH-sufficient adolescent patients compared with con-trol subjects.Swedish Study Group for Growth Hormone Treatment in Children.J Clin Endocrinol Metab.1999;84(12):4516–4524.
59.Attanasio AF,Shavrikova E,Blum WF,et al.Continued growth
hormone(GH)treatment after final height is necessary to complete somatic development in childhood-onset GH-deficient patients.
J Clin Endocrinol Metab.2004;89(10):4857–4862.
60.Tauber M,Jouret B,Cartault A,et al.Adolescents with partial
growth hormone(GH)deficiency develop alterations of body com-position after GH discontinuation and require follow-up.J Clin Endocrinol Metab.2003;88(11):5101–5106.
61.Mauras N,Pescovitz OH,Allada V,Messig M,Wajnrajch MP,
Lippe B.Limited efficacy of growth hormone(GH)during transition of GH-deficient patients from adolescence to adulthood:a phase III multicenter,double-blind,randomized two-year trial.J Clin Endo-crinol Metab.2005;90(7):3946–3955.
62.Rietzschel E,De Buyzere M.High-sensitive C-reactive protein:uni-
versal prognostic and causative biomarker in heart disease?Bio-mark Med.2012;6(1):19–34.
63.Bisoendial RJ,Boekholdt SM,Vergeer M,Stroes ES,Kastelein JJ.
C-reactive protein is a mediator of cardiovascular disease.Eur Heart J.2010;31(17):2087–2091.
64.Pradhan AD,Manson JE,Rifai N,Buring JE,Ridker PM.C-reactive
protein,interleukin6,and risk of developing type2diabetes mel-litus.JAMA.2001;286(3):327–334.
65.Hu G,Jousilahti P,Tuomilehto J,Antikainen R,Sundvall J,Salomaa
V.Association of serum C-reactive protein level with sex-specific
26Gazzaruso et al Growth Hormone and the Heart J Clin Endocrinol Metab,January2014,99(1):18–29
type2diabetes risk:a prospective Finnish study.J Clin Endocrinol Metab.2009;94(6):2099–2105.
66.Sesso HD,Buring JE,Rifai N,Blake GJ,Gaziano JM,Ridker PM.
C-reactive protein and the risk of developing hypertension.JAMA.
2003;290(22):2945–2951.
67.Yang T,Chu CH,Hsieh PC,et al.C-reactive protein concentration
as a significant correlate for metabolic syndrome:a Chinese popu-lation-based study.Endocrine.2013;43(2):351–359.
68.Lee SD,Huang CY,Shu WT,et al.Pro-inflammatory states and
IGF-I level in ischemic heart disease with low or high serum iron.
Clin Chim Acta.2006;370(1–2):50–56.
69.McCallum RW,Sainsbury CA,Spiers A,et al.Growth hormone
replacement reduces C-reactive protein and large-artery stiffness but does not alter endothelial function in patients with adult growth hormone deficiency.Clin Endocrinol(Oxf).2005;62(4):473–479.
70.Bollerslev J,Ueland T,J?rgensen AP,et al.Positive effects of a
physiological dose of GH on markers of atherogenesis:a placebo-controlled study in patients with adult-onset GH deficiency.Eur J Endocrinol.2006;154(4):537–543.
71.Sesmilo G,Miller KK,Hayden D,Klibanski A.Inflammatory car-
diovascular risk markers in women with hypopituitarism.J Clin Endocrinol Metab.2001;86(12):5774–5781.
72.Deepak D,Daousi C,Javadpour M,et al.The influence of growth
hormone replacement on peripheral inflammatory and cardiovas-cular risk markers in adults with severe growth hormone deficiency.
Growth Horm IGF Res.2010;20(3):220–225.
73.Libby P.Inflammation in atherosclerosis.Arterioscler Thromb Vasc
Biol.2012;32(9):2045–2051.
74.Wong BW,Meredith A,Lin D,McManus BM.The biological role
of inflammation in atherosclerosis.Can J Cardiol.2012;28(6):631–641.
75.Serri O,St-Jacques P,Sartippour M,Renier G.Alterations of mono-
cyte function in patients with growth hormone(GH)deficiency: effect of substitutive GH therapy.J Clin Endocrinol Metab.1999;
84(1):58–63.
76.Andiran N,Yordam N.TNF-alpha levels in children with growth
hormone deficiency and the effect of long-term growth hormone replacement therapy.Growth Horm IGF Res.2007;17(2):149–153.
77.Pardo M,Roca-Rivada A,Seoane LM,Casanueva FF.Obesidomics:
contribution of adipose tissue secretome analysis to obesity re-search.Endocrine.2012;41(3):374–383.
78.Sahin-Efe A,Katsikeris F,Mantzoros CS.Advances in adipokines.
Metabolism.2012;61(12):1659–1665.
79.Brochu-Gaudreau K,Rehfeldt C,Blouin R,Bordignon V,Murphy
BD,Palin MF.Adiponectin action from head to toe.Endocrine.
2010;37(1):11–32.
80.Kim HS,Jo J,Lim JE,et al.Adiponectin as predictor for diabetes
among pre-diabetic groups.[published online ahead of print Feb-ruary06,2013]Endocrine.doi:10.1007/s12020–013–9890–5.
81.Chaves VE,Júnior FM,Bertolini GL.The metabolic effects of
growth hormone in adipose tissue.Endocrine.2013;44(2):293–302.
82.Miyakawa M,Tsushima T,Murakami H,Isozaki O,Demura H,
Tanaka T.Effect of growth hormone(GH)on serum concentrations of leptin:study in patients with acromegaly and GH deficiency.
J Clin Endocrinol Metab.1998;83(10):3476–3479.
83.Giavoli C,Cappiello V,Corbetta S,et al.Different effects of short-
and long-term recombinant hGH administration on ghrelin and adi-ponectin levels in GH-deficient adults.Clin Endocrinol(Oxf).2004;
61(1):81–87.
84.Fisker S,Vahl N,Hansen TB,et al.Serum leptin is increased in
growth hormone-deficient adults:relationship to body composition and effects of placebo-controlled growth hormone therapy for1 year.Metabolism.1997;46(7):812–817.
85.Florkowski CM,Collier GR,Zimmet PZ,Livesey JH,Espiner EA,
Donald RA.Low-dose growth hormone replacement lowers plasma leptin and fat stores without affecting body mass index in adults with
growth hormone deficiency.Clin Endocrinol(Oxf).1996;45(6): 769–773.
86.Berneis K,Vosmeer S,Keller U.Effects of glucocorticoids and of
growth hormone on serum leptin concentrations in man.Eur J En-docrinol.1996;135(6):663–665.
87.López-Siguero JP,López-Canti LF,Espino R,et al.Effect of recom-
binant growth hormone on leptin,adiponectin,resistin,interleu-kin-6,tumor necrosis factor-?and ghrelin levels in growth hor-mone-deficient children.J Endocrinol Invest.2011;34(4):300–306.
88.Conti E,Carrozza C,Capoluongo E,et al.Insulin-like growth fac-
tor-1as a vascular protective factor.Circulation.2004;110(15): 2260–2265.
89.Heeschen C,Dimmeler S,Hamm CW,Fichtlscherer S,Simoons ML,
Zeiher AM.Pregnancy-associated plasma protein-A levels in pa-tients with acute coronary syndromes:comparison with markers of systemic inflammation,platelet activation,and myocardial necrosis.
J Am Coll Cardiol.2005;45(2):229–237.
90.FialováL,PileckováN,Bauer J,et al.Pregnancy-associated plasma
protein-A in patients with cerebrovascular diseases–a pilot study.
Prague Med Rep.2006;107(1):37–45.
91.Joaquin C,Aguilera E,et al.Effects of GH treatment in GH-deficient
adults on adiponectin,leptin and pregnancy-associated plasma pro-tein-A.Eur J Endocrinol.2008;158(4):483–490.
92.Li L,Ren W,Li J,et al.Increase in serum pregnancy-associated
plasma protein-A is correlated with increase in cardiovascular risk factors in adult patients with growth hormone deficiency.Endo-crine.2012;42(2):375–381.
93.Smith JC,Lang D,McEneny J,et al.Effects of GH on lipid peroxi-
dation and neutrophil superoxide anion-generating capacity in hy-popituitary adults with GH deficiency.Clin Endocrinol(Oxf).
2002;56(4):449–455.
94.González-Duarte D,Madrazo-Atutxa A,Soto-Moreno A,Leal-
Cerro A.Measurement of oxidative stress and endothelial dysfunc-tion in patients with hypopituitarism and severe deficiency adult growth hormone deficiency.Pituitary.2012;15(4):589–597. 95.Ozbey N,Telci A,Cakatay U,Yurci A,Molvalilar S.Determination
of oxidative protein and lipid damage in adult hypopituitary patients with GH deficiency.J Endocrinol Invest.2003;26(10):1001–1007.
96.Scacchi M,Valassi E,Pincelli AI,et al.Increased lipid peroxidation
in adult GH-deficient patients:effects of short-term GH adminis-tration.J Endocrinol Invest.2006;29(10):899–904.
97.Sanz J,Moreno PR,Fuster V.The year in atherothrombosis.J Am
Coll Cardiol.2012;60(10):932–942.
98.Jax TW,Peters AJ,Plehn G,Schoebel FC.Hemostatic risk factors in
patients with coronary artery disease and type2diabetes-a two year follow-up of243patients.Cardiovasc Diabetol.2009;8:48.
99.Cakir I,Tanriverdi F,Karaca Z,et al.Evaluation of coagulation and
fibrinolytic parameters in adult onset GH deficiency and the effects of GH replacement therapy:a placebo controlled study.Growth Horm IGF Res.2012;22(1):17–21.
100.Beshyah SA,Markussis V,Harbourne T,Nicolaides AN,Johnston DG.Haemostatic mechanisms are normal despite increased vas-cular mortality in hypopituitary adults.Horm Metab Res.1993;
25(8):449–450.
101.Gómez JM,Sahún M,Vila R,et al.Peripheral fibrinolytic markers, soluble adhesion molecules,inflammatory cytokines and endothe-lial function in hypopituitary adults with growth hormone defi-ciency.Clin Endocrinol(Oxf.)2006;64(6):632–639.
102.Kvasnicka J,Marek J,Kvasnicka T,et al.Increase of adhesion molecules,fibrinogen,type-1plasminogen activator inhibitor and orosomucoid in growth hormone(GH)deficient adults and their modulation by recombinant human GH replacement.Clin Endo-crinol(Oxf).2000;52(5):543–548.
103.Johansson JO,Landin K,Johannsson G,Tengborn L,Bengtsson BA.Long-term treatment with growth hormone decreases plas-minogen activator inhibitor-1and tissue plasminogen activator in growth hormone-deficient adults.Thromb Haemost.1996;76(3): 422–428.
doi:10.1210/https://www.360docs.net/doc/067488158.html,27
104.Gazzaruso C,Coppola A,Giustina A.Erectile dysfunction and coronary artery disease in patients with diabetes.Curr Diabetes Rev.2011;7(2):143–147.
105.Siervo M,Corander M,Stranges S,Bluck L.Post-challenge hyper-glycaemia,nitric oxide production and endothelial dysfunction: the putative role of asymmetric dimethylarginine(ADMA).Nutr Metab Cardiovasc Dis.2011;21(1):1–10.
106.Krzyzanowska K,Mittermayer F,Schnack C,Hofer M,Wolzt M, Schernthaner G.Circulating ADMA concentrations are elevated in hypopituitary adults with and without growth hormone defi-ciency.Eur J Clin Invest.2005;35(3):208–213.
107.Setola E,Monti LD,Lanzi R,et al.Effects of growth hormone treatment on arginine to asymmetric dimethylarginine ratio and endothelial function in patients with growth hormone deficiency.
Metabolism.2008;57(12):1685–1690.
108.Juárez-Orozco LE,Glauche J,Alexanderson E,et al.Myocardial perfusion reserve in spared myocardium:correlation with infarct size and left ventricular ejection fraction.Eur J Nucl Med Mol Imaging.2013;40(8):1148–1154.
109.Giubbini R,Bertagna F.Myocardial perfusion reserve in spared myocardium:one more tessera of the complex mosaic of LV re-modelling after myocardial infarction.Eur J Nucl Med Mol Im-aging.2013;40(8):1146–1147.
110.Moisey R,Orme S,Barker D,et al.Cardiac functional reserve is diminished in growth hormone-deficient adults.Cardiovasc Ther.
2009;27(1):34–41.
111.Groban L,Lin M,Kassik KA,Ingram RL,Sonntag WE.Early-onset growth hormone deficiency results in diastolic dysfunction in adult-life and is prevented by growth hormone supplementation.
Growth Horm IGF Res.2011;21:81–88.
112.Maison P,Chanson P.Cardiac effects of growth hormone in adults with growth hormone deficiency:a meta-analysis.Circulation.
2003;108:2648–2652.
113.Cenci MC,Soares DV,Spina LD,et al.Effects of5years of growth hormone(GH)replacement therapy on cardiac parameters and physical performance in adults with GH deficiency.Pituitary.
2009;12:322–329.
114.Andreassen M,Faber J,Kjaer A,Petersen CL,Kristensen L?.Car-diac function in growth hormone deficient patients before and after 1year with replacement therapy:a magnetic resonance imaging study.Pituitary.2011;14:1–10.
115.Gruson D,Alexopoulou O,Pasquet A,Cumps J,Ketelslegers JM,Maiter D.Impact of growth hormone(GH)treatment on circulating Nt-proBNP concentrations and on cardiac function in adult GH-deficient patients.Scand J Clin Lab Invest.2012;
72:387–394.
116.Cenci MC,Soares DV,Spina LD,et https://www.360docs.net/doc/067488158.html,parison of two dose regimens of growth hormone(GH)with different target IGF-1 levels on glucose metabolism,lipid profile,cardiovascular function and anthropometric parameters in GH-deficient adults.Growth Horm IGF Res.2012;22:116–121.
117.Newman CB,Frisch KA,Rosenzweig B,et al.Moderate doses of hGH(0.64mg/d)improve lipids but not cardiovascular function in GH-deficient adults with normal baseline cardiac function.J Clin Endocrinol Metab.2011;96:122–132.
118.Rosén T,Bengtsson BA.Premature mortality due to cardiovas-cular disease in https://www.360docs.net/doc/067488158.html,ncet.1990;336(8710):285–288.
119.Bates AS,Van’t Hoff W,Jones PJ,Clayton RN.The effect of hy-popituitarism on life expectancy.J Clin Endocrinol Metab.1996;
81(3):1169–1172.
120.Bülow B,Hagmar L,Mikoczy Z,Nordstr?m CH,Erfurth EM.
Increased cerebrovascular mortality in patients with hypopituitar-ism.Clin Endocrinol(Oxf).1997;46(1):75–81.
121.Svensson J,Bengtsson BA,Rosén T,Odén A,Johannsson G.Ma-lignant disease and cardiovascular morbidity in hypopituitary adults with or without growth hormone replacement therapy.
J Clin Endocrinol Metab.2004;89(7):3306–3312.122.Tomlinson JW,Holden N,Hills RK,et al.Association between premature mortality and hypopituitarism.West Midlands Pro-spective Hypopituitary Study https://www.360docs.net/doc/067488158.html,ncet.2001;357(9254): 425–431.
123.Burman P,Mattsson AF,Johannsson G,et al.Deaths among adult patients with hypopituitarism:hypocortisolism during acute stress,and de novo malignant brain tumors contribute to an in-creased mortality.J Clin Endocrinol Metab.2013;98(4):1466–1475.
124.Stochholm K,Laursen T,Green A,et al.Morbidity and GH defi-ciency:a nationwide study.Eur J Endocrinol.2008;158(4):447–457.
125.Vliegenthart R,Morris https://www.360docs.net/doc/067488158.html,puted tomography coronary ar-tery calcium scoring:review of evidence base and cost-effectiveness in cardiovascular risk prediction.J Thorac Imaging.2012;27(5): 296–303.
126.CannavòS,Marini F,CurtòL,et al.High prevalence of coronary calcifications and increased risk for coronary heart disease in adults with growth hormone deficiency.J Endocrinol Invest.2011;34(1): 32–37.
127.Schneider HJ,Klotsche J,Wittchen HU,et al.Effects of growth hormone replacement within the KIMS survey on estimated car-diovascular risk and predictors of risk reduction in patients with growth hormone deficiency.Clin Endocrinol(Oxf).2011;75(6): 825–830.
128.Monson JP.Long-term experience with GH replacement ther-apy:efficacy and safety.Eur J Endocrinol.2003;148(suppl2): S9–S14.
129.van Bunderen CC,van Nieuwpoort IC,Arwert LI,et al.Does growth hormone replacement therapy reduce mortality in adults with growth hormone deficiency?Data from the Dutch National Registry of Growth Hormone Treatment in adults.J Clin Endo-crinol Metab.2011;96(10):3151–3159.
130.Gaillard RC,Mattsson AF,Akerblad AC,et al.Overall and cause-specific mortality in GH-deficient adults on GH replacement.Eur J Endocrinol.2012;166(6):1069–1077.
131.Molitch ME,Clemmons DR,Malozowski S,Merriam GR,Vance ML.Evaluation and treatment of adult growth hormone deficien-cy:an Endocrine Society clinical practice guideline.J Clin Endo-crinol Metab.2011;96(6):1587–1609.
132.Doga M,Bonadonna S,Gola M,Mazziotti G,Giustina A.Growth hormone deficiency in the adult.Pituitary.2006;9(4):305–311. 133.Doga M,Bonadonna S,Gola M,et al.Current guidelines for adult GH replacement.Rev Endocr Metab Disord.2005;6(1):63–70. 134.Giustina A,Barkan A,Chanson P,et al.Guidelines for the treat-ment of growth hormone excess and growth hormone deficiency in adults.J Endocrinol Invest.2008;31(9):820–38.
135.Cuneo RC,Salomon F,Wilmshurst P,et al.Cardiovascular effects of growth hormone treatment in growth-hormone-deficient adults:stimulation of the renin-aldosterone system.Clin Sci (Lond).1991;81(5):587–592.
136.Johannsson G,Bengtsson BA,Andersson B,Isgaard J,Caidahl K.
Long-term cardiovascular effects of growth hormone treatment in GH-deficient adults.Preliminary data in a small group of patients.
Clin Endocrinol(Oxf).1996;45(3):305–314.
137.Johannsson G,Rosén T,Bengtsson BA.Individualized dose titra-tion of growth hormone(GH)during GH replacement in hypop-ituitary adults.Clin Endocrinol(Oxf).1997;47(5):571–581. 138.Giustina A,Mazziotti G,Canalis E.Growth hormone,insulin-like growth factors,and the skeleton.Endocr Rev.2008;29(5):535–559.
139.Mazziotti G,Gola M,Bianchi A,et al.Influence of diabetes mel-litus on vertebral fractures in men with acromegaly.Endocrine.
2011;40(1):102–108.
140.Melmed S,Casanueva FF,Klibanski A,et al.A consensus on the diagnosis and treatment of acromegaly complications.Pituitary.
2013;16(3):294–302.
28Gazzaruso et al Growth Hormone and the Heart J Clin Endocrinol Metab,January2014,99(1):18–29
141.Maison P,Tropeano AI,Macquin-Mavier I,Giustina A,Chan-son P.Impact of somatostatin analogs on the heart in acromeg-aly:a metaanalysis.J Clin Endocrinol Metab.2007;92(5):1743–1747.
142.Giustina A,Casanueva FF,Cavagnini F,et al.Diagnosis and treat-ment of acromegaly complications.J Endocrinol Invest.2003;
26(12):1242–1247.
143.Mazziotti G,Bianchi A,Bonadonna S,et al.Increased prevalence of radiological spinal deformities in adult patients with GH defi-ciency:influence of GH replacement therapy.J Bone Miner Res.
2006;21(4):520–528.144.Attanasio AF,Lamberts SW,Matranga AM,et al.Adult growth hormone(GH)-deficient patients demonstrate heterogeneity be-tween childhood onset and adult onset before and during human GH treatment.Adult Growth Hormone Deficiency Study Group.
J Clin Endocrinol Metab.1997;82(1):82–88.
145.Mazziotti G,Porcelli T,Bianchi A,et al.Glucocorticoid replace-ment therapy and vertebral fractures in hypopituitary adult males with GH deficiency.Eur J Endocrinol.2010;163(1):15–20. 146.Giustina A.Does growth hormone replacement therapy improve cardiac function?Nat Clin Pract Endocrinol Metab.2007;3(9):6 14–615.
Mark Your Calendar for Clinical Endocrinology Update September 4-6, 2014, San Francisco, California
https://www.360docs.net/doc/067488158.html,/CEU
doi:10.1210/https://www.360docs.net/doc/067488158.html,29
鲁迅研究考试复习资料(完整版)
鲁迅研究复习资料(完整版) 【名词解释】(鲁迅自考笔记) 1“匕首”、“投枪”——这是鲁迅对杂文的社会作用的认识,他认为杂文应该针砭时弊批判现实社会的黑暗,具有独特的战斗性。 2.“过客”——这是鲁迅在散文诗《野草》中所塑造的艺术形象。他是鲁迅反抗黑暗,反抗绝望的精神象征。 3.“吃人”——这是鲁迅在小说《狂人日记》中对中国历史所作的形象化的总结,其内涵是指封建专制统治对人的精神控制和毒害。 4.真的猛士——这是鲁迅在《纪念刘和珍君》一文中所提到的。一种“敢于正视现实、正视人生”的人生态度,也是鲁迅的理想人格的精神象征。 5.《摩罗诗力说》—。这是鲁迅早期撰写的一部介绍外国文化、文学的论文,从中反映了鲁迅对外国文化、文学的基本态度,是研究鲁迅的美学思想、比较文学思想的重要文章。 6.“社会相”是对鲁迅杂文的形象概括。体现出鲁迅杂文是一部活的近代和现代的中国社会史,更是对社会各种现象洞幽烛微的精辟见解的诠释。 7.精神胜利法“是鲁迅的小说《阿Q正传》中主人公阿Q最突出的思想性格特点。充分体现了作者对国民劣根性的揭露和批判。 8.“超人”哲学是指鲁迅早期曾接受过的德国哲学家尼采的哲学主张。其理论鼓吹所谓超人是人的生物进化的顶点,一切历史文化都是由他们创造的,而普通群众则是低劣的庸众。 9.“中间物”是鲁迅自己的说法。他在《坟》的后记中说,在进化的链条中,一切都是中间物。这是鲁迅对自己身在传统与现代之中的体验,也是他自我否定意识的体现。 10.“油滑”即“古今杂揉”的手法,鲁迅称之为“油滑”的手法,是直接从中国传统戏剧里借用来的既为作品真实地展现的古代人物、环境、生活所吸引,又因现代语言情节、细节不断插入,提醒而冷静思索作品的现实意义,以批判的眼光审视作品所描写的一切。从而使小说获得更为深广的社会意义。 11.“媚态的猫”,是鲁迅杂文中社会相的一种。“媚态的猫”实际上是以物喻人,不仅指现代评论派的资产阶级文人,也勾勒了一切反动黑暗势力的共同特征。 12.“民族魂”是对鲁迅的崇高评价。他是我国革命由旧民主主义转折到新民主主义的历史关头,用文学来思考时代的要求,记录时代的步音,参与和鼎助时代发展的旷世巨人。鲁迅是现代中国“民族魂”的代表,也是现代“民族魂”的塑造者之一。 13.“为人生”鲁迅创作的文学主张,而且要改良这人生“的主张,取材”多采自病态社会的不幸的人们“,用意在”揭出病苦,引起疗救的注意。 14.“叛逆的猛士”是鲁迅对自己的期望。鲁迅先生作为一个觉醒者,他毅然肩负起了唤醒民众的责任,希望能打破黑暗世界建立光明之中国。 15.《坟》是鲁迅最早的一部杂文集是作者对五四后中国历史国民性的解剖。题目含有埋葬过去开拓未来之意。16.“叭儿狗”是鲁迅杂文中议论形象化的典型,社会相的一种。指中国社会中奴才的嘴脸。17.宴之敖者“是鲁迅的《故事新编》中《铸剑》中的人物。是向残暴的统治者反抗和复仇的形象。寄托着作者的理想。18.“进化论”是鲁迅在南京求学时开始接受的进步思想。他采取批判的继承态度最终在四。一二政变后彻底放弃了此思想。【填空题】 1.鲁迅是中国新文学的伟大(开拓者和先驱者)。 2.阿Q是鲁迅小说(阿Q)中所塑造的一个落后的、不觉悟的农民形象。 3.前苏联著名的作家(法捷耶夫)(论鲁迅)一文中,高度赞扬鲁迅是“属于作为人类明灯的作家之列的。……是中国文学的骄傲”。
土木工程英文文献
2.1 Reinforced Concrete Plain concrete is formed from a hardened mixture of cement ,water ,fine aggregate, coarse aggregate (crushed stone or gravel),air, and often other admixtures. The plastic mix is placed and consolidated in the formwork, then cured to facilitate the acceleration of the chemical hydration reaction lf the cement/water mix, resulting in hardened concrete. The finished product has high compressive strength, and low resistance to tension, such that its tensile strength is approximately one tenth lf its compressive strength. Consequently, tensile and shear reinforcement in the tensile regions of sections has to be provided to compensate for the weak tension regions in the reinforced concrete element. It is this deviation in the composition of a reinforces concrete section from the homogeneity of standard wood or steel sections that requires a modified approach to the basic principles of structural design. The two components of the heterogeneous reinforced concrete section are to be so arranged and proportioned that optimal use is made of the materials involved. This is possible because concrete can easily be given any desired shape by placing and compacting the wet mixture of the constituent ingredients are properly proportioned, the finished product becomes strong, durable, and, in combination with the reinforcing bars, adaptable for use as main members of any structural system. The techniques necessary for placing concrete depend on the type of member to be cast: that is, whether it is a column, a bean, a wall, a slab, a foundation. a mass columns, or an extension of previously placed and hardened concrete. For beams, columns, and walls, the forms should be well oiled after cleaning them, and the reinforcement should be cleared of rust and other harmful materials. In foundations, the earth should be compacted and thoroughly moistened to about 6 in. in depth to avoid absorption of the moisture present in the wet concrete. Concrete should always be placed in horizontal layers which are compacted by means of high frequency power-driven vibrators of either the immersion or external type, as the case requires, unless it is placed by pumping. It must be kept in mind, however, that over vibration can be harmful since it could cause segregation of the aggregate and bleeding of the concrete. Hydration of the cement takes place in the presence of moisture at temperatures above 50°F. It is necessary to maintain such a condition in order that the chemical hydration reaction can take place. If drying is too rapid, surface
文献信息分类
文献信息分类 第一节文献分类及文献分类法 一、文献分类 以文献分类法为工具,根据文献所反映的学科知识内容与其他显著属性,分门别类地、系统地组织与揭示文献的一种方法。 二、文献分类法 指按照一定的思想观点,以科学分类和知识分类为基础,并结合文献的特点,对概括文献情报内容特征及某些外表特征的概念或术语,进行逻辑划分和系统排列而形成的类目一览表。 第二节《中国图书馆分类法》概述 《中国图书馆图书分类法》就我国建国以后编制出版的具有代表性的大型综合性文献分类法,简称《中图法》。第四版正式改名为《中国图书馆分类法》,其简称仍称《中图法》。《中图法》(第五版)已于2010年9月由国家图书馆出版社正式出版。 一、《中图法》(第五版)的修订重点及特色 《中图法》的修订是一项持续性、系统性的工作,每版修订都有其重点和特色。此次修订幅度较大,新增1631个类目,停用或直接删除约2500个类目,修改类约5200多个。其修订特点有: 1. 确定了特别处理的大类、重点修订大类和局部调整大类。 根据用户使用意见、《分类法研究与修订调研报告》以及“修订报告”对《中图法》(第四版)存在问题的分析,此次修订确定“A马克思主义、列宁主义、毛泽东思想、邓小平理论”为特别处理的大类,“F经济”、“TP自动化技术、计算机技术”、“U交通运输”为重点修订大类,“D政治、法律”、“G文化、科学、教育、体育”、“TS轻工业、手工业、生活服务业”等与政治、经济、文化、生活、计算机技术相关类为局部调整大类。最后的修订结果也基本体现了这些修订重点。 2. 增加复分标记、“一般性问题”的禁用标记。 对一组类目或多组类目需要复分时,以前各版次的《中图法》只有一个说明性注释来规定,而具体需要复分的类目不再一一注释说明。第五版为增强类目复分助记性、降低复分难度,对这些类下无直接复分注释而又需复分的类目的类名后增加了相应标记,并区别8个通用附表、专类复分或仿分的标记,标记符分别对应为①②③④⑤⑥⑦⑧⑨(①~⑧分别代表用《中图法》后附的8张不同的通用复分表复分,⑨表示专类复分或仿分。)与《中国分类主题词表》主题词对应类号的复分标记一致。 对专类下一组具有总论性和通用复分性问题,《中图法》通常设置“一般性问题”类加以概括,因此,规定“一般性问题”类只起仿分概括说明作用,不用于类分文献,其主题归入“一般性问题”类的直接上位类。第五版对“一般性问题”类进行了规范,对不具有此特点的类作了类名修改,对具有此特点的“一般性问题”类,在其类名后增加了禁用类分文献的标记,标记符为,以便提示分类人员,避免误标引并造成与其上位类分类不一致问题。 3. 完善类目的参见注释,补充类目反向参照。 《中图法》前几版相关类目参照是人工按类分别注释,因此,很多相关联的类目只有单向参照。(第四版)修订时,借助“《中国分类主题词表》的维护管理系统”对类目的参见注释进行了完善。首先规范参见注释,区分“参见”与“见注”;其次补充需要建立反向参照
鲁迅作品教学 文献综述
“鲁迅作品与语文教材”的文献综述 聊城大学文学院2013级教育硕士王伟 新课程改革之后,在一个《课程标准》的前提下,语文教材开始多元化,各地编写的语文教材在选文上的自主性加大,鲁迅的“进”与“出”就成了一个我们必须面对的现实。一些人很偏激地认为应该把鲁迅“请出”语文教材,这是因为他们自身肤浅地误读了鲁迅。一些人很坚决地主张鲁迅作品在语文教材中的“霸主”地位,这是因为他们对鲁迅精神的深刻理解与膜拜。我觉得应该理性地去看待这个问题。在超星发现和中国知网上学习了2001年至2013年的有关“鲁迅作品与语文教材”方面的论文,按照“篇名”“核心期刊”“精确”的标准检索,分别检索到实际相关的论文970篇和23篇,下载了87篇,选取了我个人认为有代表性的论文12篇,作者包括专家学者教授、教育部门领导、一线教师,目的是既能学习语文课程标准的理论研究的前沿,又学习语文课程标准在具体实践过程中遇到的各种问题,包括可取之处、需要整改之处、有待商讨之处,以做到把有关语文课程标准理论与实践放在一起来进行学习,达到最佳学习效果。 通过学习,我从三个方面为2001年至2013年有关“鲁迅作品与语文教材”做一下文献综述。敬请老师的批评指正!老师,您的一个字也许就是开启我封闭落后心灵的一把钥匙,也许就是照亮我前行的一盏灯烛。所以,我更愿意接受您的批评…… 一、鲁迅作品在中学语文教材的变迁 代表性文章有王平.邓越的《鲁迅作品在中语文课本中的变迁》,尹奇岭的《鲁迅作品在中学语文“存续”与“删减”之争》,温儒敏的《语文课并没有“鲁迅大撤退”》。 (一)《鲁迅作品在中学语文课本中的变迁》 开篇对鲁迅作品在中学语文教材中的地位、作用和影响做了高度的评价和概括。全文共分为两大部分对问题进行阐释。 1.选文变迁是教育思想和价值观。这一部分剖析了鲁迅语文教材作品在每一个时期的变化,详尽有序。即民国:推广白话文的先锋——建国初:民族新文化的风向标——“文革”:被神圣化的政治工具——改革开放:“人间鲁迅”形象的还原——新世纪:多元化语境的回归。一语中的,恰切到位,把鲁迅作品在语文教科书中的作用、地位完整地展现于此。这一过程也就是“神化的鲁迅”到“本色的鲁迅”的过渡,从过度关注人的社会性到关注个体生命本身的存在。这个过程注定是曲折的,尽管是曲折的,毕竟我们认识到了。 2.文章重点解读的是第五个时期,即新世纪:多元化语境的回归。文章引用了人教版新课程高中语文教材执行主编温儒敏教授发表文章中的话作了说明:“总课量少了,课文总篇数也相应要减少。就是说,鲁迅篇目在必修课中的减少,是由于课程结构变化与整个课时减少决定的。”从编者的角度再次阐述鲁迅作品经受了历史的考验,依然屹立于语文教材之中,先生所塑造的人物形象已深深扎根于一代又一代的国人心中,成为经典。在这里,文章严肃地指出了鲁迅作品不能被语文教材删除的根本原因:“鲁迅所思考过、焦虑过的问题,也正如一个个幽灵,依然徘徊在新世纪的天空。虽然‘匡正时弊,重铸民魂’的传统不同程度被一些人漠视淡忘,但鲁迅精神不会过时也不会撤退,它早已融进了我们这个饱经沧桑的民族血脉,它所具有的意义生长点,使其历久弥新,随着时代的发展,真正成为中国人的脊梁。” (二)尹奇岭的《鲁迅作品在中学语文“存续”与“删减”之争》
浙江省历年本科鲁迅研究试题及部分答案
浙江省2014年10月高等教育自学考试 一、单项选择题(本大题共10小题,每小题1分,共10分) 1.鲁迅哪部小说被认为中国现代文学史上的第一篇白话小说? A.《孔乙己》 B.《药》 C.《祝福》√ D.《狂人日记》 2.下列哪部作品收录于鲁迅《呐喊》小说集? A.《肥皂》√ B.《兔和猫》 C.《孤独者》 D.《为了忘却的纪念》 3.九斤老太是哪部作品中的人物? A.《头发的故事》 B.《故乡》√ C.《风波》 D.《高老夫子》 4.鲁迅的两篇小说被称为代表20世纪中国短篇小说艺术最高水平的,其一《示众》,其二是 A.《祝福》 B.《示众》√ C.《孔乙己》 D.《阿 Q 正传》 5.《在酒楼上》把自己的生活道路概括为“像一只苍蝇饶了一点小圈子,又回来停在原地点”的是 A.方玄绰 B.陈士成 C.涓生√ D.吕纬甫 6.“我是我自己的,他们谁也没有干涉我的权利!”这是小说( )中子君喊出的宣言,也是人的觉醒的声音。 A.《幸福的家庭》√ B.《伤逝》 C.《肥皂》 D.《离婚》 7.下列哪部作品不属于《故事新编》? A.《补天》 B.《理水》√ C.《复仇》 D.《铸剑》 8. 中老女人的遭遇所象征、展示的是精神界战士与他所生活的世界———现实人间的真 实关系:带着极大的屈辱,竭诚奉献了一切,却被为之牺牲的年轻一代(甚至是天真的孩子), 以致整个社会无情地抛弃和放逐。 √A.《颓败线的颤动》 B.《死地》 C.《吃白相饭》 D.《算账》 9.鲁迅的《文化偏至论》写于哪年? √A.1907 B.1908 C.1917 D.1919 10.“自己背着因袭的重担,肩住了黑暗的闸门,放他们到宽阔光明的地方去;此后幸福的度日, 合理的做人。”选自哪个作品? A.《我之节烈观》√ B.《我们现在怎样做父亲》 C.《夜颂》 D.《导师》 二、双项选择题 ( 本大题共 5 小题 ,每小题 2 分 , 共 10 分 ) 11.下列哪些作品不属于《彷徨》? ?? A.《示众》 B.《祝福》√ C.《孔乙己》 D.《在酒楼上》 E.《离婚》 12.鲁迅小说创作具有哪两个特点? √A.“表现的深切” B.“思想激进” C.再现性强 D.理想主义√ E.“格式的特别” 13.鲁迅在《孤独者》这篇小说里,始终突出的是两个感受。而且都是趋于极端的,一个是极端 的感,一个是极端的感。 √(类)A.异端 B.兴奋 C.希望√D.绝望 E.反抗 14.鲁迅的杂文创作坚持开展哪两个原则? √A.文明批评 B.常态批评√C.社会批评 D.常情批评 E.文学批评 15.以下哪些著作曾对《铸剑》中的故事作过类似的记载? √A.《搜神记》√ B.《春秋》 C.《汉书》 D.《列异传》 E.《史记》
土木工程毕业设计外文文献翻译修订版
土木工程毕业设计外文文献翻译修订版 IBMT standardization office【IBMT5AB-IBMT08-IBMT2C-ZZT18】
外文文献翻译 Reinforced Concrete (来自《土木工程英语》) Concrete and reinforced concrete are used as building materials in every country. In many, including the United States and Canada, reinforced concrete is a dominant structural material in engineered construction. The universal nature of reinforced concrete construction stems from the wide availability of reinforcing bars and the constituents of concrete, gravel, sand, and cement, the relatively simple skills required in concrete construction, and the economy of reinforced concrete compared to other forms of construction. Concrete and reinforced concrete are used in bridges, buildings of all sorts underground structures, water tanks, television towers, offshore oil exploration and production structures, dams, and even in ships. Reinforced concrete structures may be cast-in-place concrete, constructed in their final location, or they may be precast concrete produced in a factory and erected at the construction site. Concrete structures may be severe and functional in design, or the shape and layout and be whimsical and artistic. Few other building materials off the architect and engineer such versatility and scope. Concrete is strong in compression but weak in tension. As a result, cracks develop whenever loads, or restrained shrinkage of temperature changes, give rise to tensile stresses in excess of the tensile strength of the concrete. In
民族地区图书馆文献信息资源建设与共享初探
2012年11月 内蒙古科技与经济 N ov ember 2012 第21期总第271期 Inner M o ngo lia Science T echnolo gy &Economy N o .21T o tal N o .271 民族地区图书馆文献信息资源建设与共享初探 张志伟 (呼伦贝尔市科技情报研究所,内蒙古呼伦贝尔 021008) 摘 要:简要分析了民族地区图书馆现状及文献信息资源建设与共享的必要性,阐述了知识经济环境下民族地区图书馆实现文献信息资源建设与共享的有效途径。 关键词:民族地区;图书馆;信息资源;建设;共享 中图分类号:G258.2 文献标识码:A 文章编号:1007—6921(2012)21—0072—03 文献信息资源交流共享是社会经济、科学技术发展到一定阶段,是图书馆事业发展到一定规模与水平的必然产物,是图书馆资源共享的核心。近年来,民族地区各级图书馆在文献信息资源建设方面取得了不俗的成绩,但大多因所处地理环境边远,经济水平相对滞后,文化发展工作薄弱,使地方文献信息资源的交流与共享受限。因此,民族地区图书馆抓住西部大开发战略实施的有利时机,在构建自身特色的基础上,加强文献信息资源交流共建共享,已成为当前的一项重要任务。 1 民族地区图书馆现状及文献信息资源建设与共享的必要性 图书馆可以称得上是信息资源的集散地,它承载着为地区社会经济文化发展搜集、整理和提供政治、经济、学术研究、文化信息的任务。可是随着网络技术日益广泛地应用,民族地区图书馆却因经费不足、服务手段落后、管理体制滞后、对信息资源重要性尚认识不足、馆藏文献信息资源保障率低、数据库建设水平低等各种原因,无法顺利实现社会价值,生存空间愈见狭小。 由于我国民族地区幅员辽阔、人口众多,因此民族方面的文献信息资源非常殷实,其范围之广、内容之多是其他地区望尘莫及的。据统计数据显示,全国民族地区有超过3000万册的藏书量,民族文学类图书及音像制品累计达到5万余种,许多民族都拥有自己的特色文献精品,例如:蒙古族的《甘珠尔》、藏族的《大藏经》、维吾尔族的《福乐智慧》等民族宗教文献成果。诸如此类的文献对我国历史和文化发展、民族融合、区域经济发展等的研究极具参考价值,是我国文献信息资源中不容小视的组成部分。可与此同时此类地区的图书馆又因为“呈缴”制度不健全、经费不足,造成文献收集率锐减、文献老化现象日益凸显、馆藏信息匮乏与读者需求增大的矛盾愈来愈突出。 数字化时代的到来,文献信息资源向社会化、全 球化共享迈进,资源共享对充分合理开发利用文献信息资源有着重要的现实意义,同时也是现代化图 书馆馆际协作网络化的最终目的。传统图书馆在文献收藏上各自为政、相互间缺少协作和沟通、重复购置,造成了图书的积压和经济上的浪费。想要改变现状,让有限的经费发挥最大的效用,就必须努力实现文献信息资源的交流共享。 2 如何更好地实现文献信息资源的建设与共享2.1 突出自身特色,强化实有馆藏及文献数字化建设 愈是民族的,就愈是世界的。对民族地区图书馆来说,要更多地体现民族地方的文献特色,特色是生命之基,力量之源,它不仅体现优势,更显出办馆效益,从某种程度上来讲只有构建自身特色,寻找适合自身发展的道路,才能在“信息爆炸”的数字化时代站稳脚跟,才有与他馆资源共享的资格。2.1.1 特色文献馆藏建设。现实馆藏是指本馆自己拥有的能为读者直接开展服务的实有馆藏。现阶段,纸质文献距完全实现数字化还有一段距离,数字化网络信息也尚不能完全替代纸质文献,两者传播方式和载体的不同,产生利用上的差异,决定了现实馆藏存在的价值。民族地区图书馆现实馆藏今后的建设应突出2大内容:首先是民族文献收藏。民族文献即以政治、经济、教育、地理、历史、文化生活等为视角研究和记载我国各少数民族文化,具体囊括了: 使用汉文记载的关于民族问题的文献; 使用少数民族文字记载的文献; 用象形文字和抽象符号记载和语言相传的具有史料价值的口碑文献。它们是中华民族文献的重要组成。尤其要强化民族文字文献的收藏。其次是地方文献收藏。地方文献即关于地方的一切书刊资料,其内容十分广泛,从纵向看,包括古代到当代;从横项看,蕴含了所有自然和人文内涵,如政治、经济、历史、地理、自然、人物、军事等等;从文献信息形式的视角来说,涵盖书刊、报纸等所有文字的和图籍的资料。地方文献不但能显现 ? 72? 收稿日期:2012-08-31 作者简介:张志伟(1974-),女,馆员,毕业于吉林大学经济管理专业。
民族地方文献与民族地区公共文化服务分析
民族地方文献与民族地区公共文化服务分析 民族地区所具有的特点致使公共文化服务表现出特殊性,而民族地区的文献却承载了该地方的民族文化,所以,民族地区图书馆一定要积极的收藏当地文献,并结合地区特色,对自己的服务品牌进行打造,进而对民族地区有效实施便利性、基本性以及均等性与公益性的公共文化服务。 标签:民族地区文献公共文化服务 公共文化服务就是公共部门想要保护公民拥有的文化权利,并使公民在文化这方面提出的要求得到满足。而对公共文化产品进行管理的过程来说,图书馆提供给人们的服务活动是主要公共文化服务,民族文献属于民族地区图书馆当中的主要馆藏,可以促使民族地区所具有的公共文化服务作用得到充分发挥。 一、民族地区提供的公共文化服务所具有的特殊性 1.民族特点使文化需求变得极其特殊 所有的少数民族都具有数据自己民族一种语言,有部分少数民族还具有较为浓厚的宗教信仰,这些民族在长时间的发展过程中,形成了一个独具特色的文化传统和风俗习惯以及种种民族特点,致使他们变得极其特殊,且文化需求也极具个性[1]。 2.民族居住特点使民族地区拥有了特殊的公共文化服务 少数民族虽然人口非常少,但分布面积却很广,我国64.5%的面积都是民族自治区。而在创建公共文化服务这个体系时,一定要对便利性、基本性以及均等性与公益性等加以分析和考虑。此外,民族地区的实际居住情况以及自然条件使公共文化服务成本非常高,半径极大,想要使公共文化服务实现便利性以及均等性非常困难。 3.民族地区图书馆所提供的文化服务具有特殊性 现在民族地区图书馆在为人们提供服务时,不但要使用汉语这种国家通用的语言,还应该提供给他们本民族的语言文字服务,收集一些同该民族文化相符合的文献信息资源,把他们当作该民族人民的读物,这样少数民族人民就可以感觉到图书馆对自己的认可以及认同,进而获得到更多的文献信息,并使自己的阅读权利得到保障[2]。 二、民族地方文献当中承载了民族地方的文化 民族文化属于某一个民族在经过不断地发展而形成的精神和物质两项结果的总和。而少数民族呈现出来的文化属于中华民族文化当中不可分割以及最主要
鲁迅选修课2000字论文
浅谈鲁迅和胡适 张昆昱计算机与通信工程学院13级中加6班20136156 这两位文坛巨匠,与我相比,实在高出不止千千万,我且以一介书生的小视角来浅谈一下两位先生,希望已故两位先生不会介意后生的失礼。 鲁迅先生在中国的文坛地位远远高于胡适先生,但凡了解中国的同学对两位都不陌生,但是很多人对于后者只是处于知道有这么一个人的阶段,对于其生平却不知一二。学习了本门课程,老师不拘一格的讲课风格吸引了我去对二人做个小小的比较。 首先,我们可以对比一下两位。 对文化事业的贡献上看,胡适的功绩是不可抹杀的,鲁胡二人也是各有千秋。一般说来,胡适开风气的作用更大,而鲁迅则更深刻。 对于胡适在学术文艺上的成绩,学者们的评价很不一致。近今大陆上的某些学者,对胡适的学术成就大加推崇,认为他在鲁迅之上,而台湾的新儒家,则直斥其浅薄,别的国学家也一直在对他进行暗批。但从对文化事业的贡献上看,胡适的功绩是不可抹杀的,鲁胡二人也是各有千秋。一般说来,胡适开风气的作用更大,而鲁迅则更深刻。 在为人处世上,鲁迅与胡适确有不同。一般说来,胡适比较随和、宽容,而鲁迅则较为顶真、急切。这两种性格各有优缺点。 很多人会说,你这不是等同于没说吗?其实,客观的评价两个人物,我们不能简简单单得出孰高孰低的结论。常言“金无赤足,人无完人”不是没有根据的。言归正传,我在这里不是要否定鲁迅先生的成就,也不是要替胡适伸冤,只是想公平的评价一下两人而已。 胡适适是在现代文化史上有重大贡献的人物,同时也是开创性的人物。他是白话文运动的先锋,他的“易卜生主义”影响很大。在“五四”时期,鲁迅与胡适是同一营垒中的人。大革命失败后,鲁迅对国民党的专制与屠杀给予激烈的批判,而胡适也对国民党钳制舆论、扼杀思想自由提出公开声讨,在这方面他们都是五四的传人。晚年的鲁迅倾向左翼,卷入左联的活动,胡适与国民党的关系更是千丝万缕,但他们都没有加入政党。从思想气质上说,两人十分不同。在学术上,胡适引入规范,告诉大家现代学术要按照什么方式和方法做,影响深远。鲁迅的学术研究充满洞见,但他更强调的是不断打破规范,总是怀疑这些极易体制化的知识具有压迫性。胡适是典型的现代化派,相信历史的进步,文章平易流畅,气质上是乐观的。鲁迅与胡适一样对传统展开批评,但没有胡适的那种乐观气息和十分的自信。原因大致有两点,一个是他在反对传统的时候,总是觉得自己的灵魂里也中了传统的毒,想要摆脱而不能,所以他的文化批评和文明批评的矛头所向也对着自己,只是别人不大察觉而已。鲁迅对传统的批评中有一种胡适所没有的切肤之痛。另一个是他虽然以进化论的观念批判传统,但并不认为现代的国家比过去的国家更开明。大约是在1907年,鲁迅以西方为例说,君主专制打破了宗教专制,法国大革命打破了君主专制,倡导民主自由,实行多数统治,一人专制尚有反抗的余地,多数专制很可能比独夫专制还要恐怖。他赞成革命,赞成立宪制,但是他对这些所谓的“现代”从来不迷信。1929年,他对冯雪峰说,我也不要去你们未来的黄金世界,因为那里还会有将叛徒处刑的吧。他是在
辽宁自考07565鲁迅研究学习资料
辽宁自考07565鲁迅研究学习资料 1童少年时期对封建思想、封建思想文化封建教育的批判 对宣扬封建道德观念的的《二十四孝》极为不满(老莱娱亲、郭巨埋儿)对封建家长制度、封建教育制度,对迷信、封建落后的陋习的不满。后来于五四文化运动时期对于封建传统的猛烈扫荡,奠定了坚实的基础。 2南京求学时期受达尔文进化论思想的影响 达尔文进化论认为,自然界中的一切生物都依照生存竞争,自然淘汰的规律发展着、严复结合当时的中国民族危亡的客观情势,由此发出“学习西方,与天争胜,自强保种”的救国思想。鲁迅接受了这一观点:新的必胜旧的,将来必胜过去,青年必胜老年。这就构成了鲁迅进化论信仰即社会发展观的基本特点,而特别强调只有通过斗争才能取得社会的发展和民族的解放。 3日本留学时期思想经历 在哲学上提出了“掊物质而张灵明,任个人而排众数”强调主观精神在人类社会中的地位与作用,发扬人物内在精神,强调少数天才和英雄人物在创造历史中的作用。宣扬主观唯心主义与唯意志论的看法(暂时迷误)个性解放毕竟属于资产阶级思想范畴带有历史唯心主义色彩,却建立在革命民主主义场上,与尼采不同。4辛亥革命前后的主要思想状况 对辛亥革命热烈欢呼到严重失望,并没有单纯地沉湎于忧愤之中,他对辛亥革命的经验教训,进行了认真的反思 ①资产阶级在政治上的软弱、妥协。 ②中国革命任务的艰巨性、长久性 ③严重脱离广大人民群众。在苦闷和寂寞中继续奋进、战斗(辛亥之后,动乱不
止)缅怀古代先贤。从历史遗产中汲取精神力量,重视反抗精神。(对中国传统文化糟粕的批判,积累了充足的资料。从学术意义上看。也给研究中国字体史和文学史做了必要的准备) 5五四时期的政治思想 ○1在政治思想上,基于强烈的民主主义要求,彻底的反对封建主义,第一篇白话小说《狂人日记》中,就把斗争的矛头直指向封建主义。揭露“吃人”的本质,并根本否定。 ②1919年10月《我们现在怎样做父亲》抨击了封建的的“孝”道观念,对三纲愤怒声讨。 ③鲁迅对保古派的批判,主要着重在对“二重思想”(新旧并存中体西用)的挞伐上,充分体现了鲁迅反对封建主义的彻底性。 6五卅前后能用阶级观点分析社会问题 首先表现在他对青年的看法上。其次鲁迅阶级论的思想因素的增长,还表现在他对某些日常生活现象的分析上(对中国菜的分析)。还十分明确地认识到了武装斗争的重要意义,尤其重视“国民性”的改造问题。对人民群众在历史上的作用有了新的认识。本时期文艺思想的主导倾向是现实主义,艺术应当是社会现实的真实反映。 7厦门时期认识到了无产阶级专政的历史必然性 肯定了无产阶级专政是历史的必然,在厦门期间,用阶级观点来观察和分析问题,表现得更加明显、更加全面了。马克思主义认为,阶级斗争必然导致无产阶级专政。(不同的解释,因为阶级属性和社会地位不同的缘故) 8广州时期“已经基本跨入了无产阶级世界观的门槛”的几个重要标志,
土木工程外文文献及翻译
本科毕业设计 外文文献及译文 文献、资料题目:Designing Against Fire Of Building 文献、资料来源:国道数据库 文献、资料发表(出版)日期:2008.3.25 院(部):土木工程学院 专业:土木工程 班级:土木辅修091 姓名:武建伟 学号:2008121008 指导教师:周学军、李相云 翻译日期: 20012.6.1
外文文献: Designing Against Fire Of Buliding John Lynch ABSTRACT: This paper considers the design of buildings for fire safety. It is found that fire and the associ- ated effects on buildings is significantly different to other forms of loading such as gravity live loads, wind and earthquakes and their respective effects on the building structure. Fire events are derived from the human activities within buildings or from the malfunction of mechanical and electrical equipment provided within buildings to achieve a serviceable environment. It is therefore possible to directly influence the rate of fire starts within buildings by changing human behaviour, improved maintenance and improved design of mechanical and electrical systems. Furthermore, should a fire develops, it is possible to directly influence the resulting fire severity by the incorporation of fire safety systems such as sprinklers and to provide measures within the building to enable safer egress from the building. The ability to influence the rate of fire starts and the resulting fire severity is unique to the consideration of fire within buildings since other loads such as wind and earthquakes are directly a function of nature. The possible approaches for designing a building for fire safety are presented using an example of a multi-storey building constructed over a railway line. The design of both the transfer structure supporting the building over the railway and the levels above the transfer structure are considered in the context of current regulatory requirements. The principles and assumptions associ- ated with various approaches are discussed. 1 INTRODUCTION Other papers presented in this series consider the design of buildings for gravity loads, wind and earthquakes.The design of buildings against such load effects is to a large extent covered by engineering based standards referenced by the building regulations. This is not the case, to nearly the same extent, in the
民族文献阅读推广研究
民族文献阅读推广研究 民族文献阅读推广活动作为少数民族地区图书馆的组成部分,对传承和弘扬民族文化具有举足轻重的作用。近年来,阿拉善盟图书馆虽在阅读推广方面有了一定的成绩,但是蒙古文民族文献的阅读推广工作仍然需要加强和完善。本文以阿拉善盟图书馆为例,就如何加强蒙古文民族文献的閱读推广工作,结合馆情实际做以探索研究。 标签:蒙古文民族文献阅读推广研究 随着社会发展,蒙古族历史文化逐渐面临消失,作为少数民族地区的图书馆,自然有责任和义务为推广民族文献阅读贡献自己的力量。所以少数民族地区图书馆以其丰富的蒙古文馆藏文献和信息资源优势,担负着倡导和实践全民阅读、营造和推广全民阅读氛围的责任。 一、蒙古文民族文献阅读推广工作的重要意义 “全民阅读”倡导了三年,终于“大力推动”了,今年全国两会期间,“全民阅读”第四次被写入《政府工作报告》,今年首次使用了“大力推动全民阅读”,并列为2017年重点工作任务,重要性可见一斑。蒙古文民族文献是记载蒙古族文明历史发展的珍贵资源,而图书馆是书香社会的家园,是推动全民阅读的倡导者、组织者和实践者,如何推广蒙古文民族文献,实现蒙古文文献资源的传播,意义重大。 蒙古文民族文献阅读推广,能让馆藏蒙古文文献信息资源最大限度地得到利用。蒙古文民族文献作为记载蒙古族文明历史发展的珍贵资源,其文献应当成为阅读推广的特色和重点。阿拉善地区位于祖国北部边疆,是一个主要以蒙古族为主,以汉族占大多数的多民族地区,在历史的进程中,形成了其本民族本地区特有的文化特点,阿拉善民族地方文献特色馆藏也是盟图书馆一大亮点领域,以收集卫拉特历史文化为主的民族地方文献为重点,包括以研究北方少数民族历史文化的独具地域特色的文献馆。近年来,对特色文献进行研究、挖掘和保护方面有着一定的成绩。我们将依托丰富的馆藏资源,在扩大民族文化影响力中发挥本馆得天独厚的优势,让更多的蒙古族群众走进图书馆、认识图书、利用图书馆,从而改善少数民族文化生活状况,提升少数民族生活质量。 二、蒙文读者的文化需求及阅读推广中存在的问题 1.蒙文文献阅读现状堪忧 首先,我们对到馆读者的阅读状况如何,进行了一些调查,调查分析显示,蒙古族读者占比总体不容乐观。导致蒙古族读者占比不高的主要原因:一是,阿拉善地区蒙古族人口占比就少。阿拉善地区地广人稀,三旗两区常住人口近24.7万,其中蒙古族只占28.3%;二是,对外宣传不够,导致很多蒙古族读者对图书
鲁迅研究论文
论“吃人”命题与中国文化的关系 ——浅谈祥林嫂之悲剧“吃人”,作为中国现代文学语言中一个常用的比喻词汇,它总是与鲁迅先生紧密地联系在一起,这不仅是因为他在《狂人日记》中第一次明确地提出了“吃人”问题,更因为它常常被认为是鲁迅对中国历史和传统文化的本质内涵所做出的独特发现和惊人概括;所以,在众多的鲁迅研究者那里,“吃人”便被赋予了非同一般词汇可比的特殊意义:它是“鲁迅文化观中具有一贯性的思想”,也是鲁迅“理想人性思考的一个反题”,更是“鲁迅思想研究中具有基石意义的内容”。 在鲁迅的许多小说中,很多都包含有“吃人”的寓意,例如《祝福》,相较于《狂人日记》、《孔乙己》,还是一个封建礼教吃人的问题,还是一个吃人主题的延续。祥林嫂作为一个典型的中国封建时代的贫苦农民,同样是被那样一个社会吃掉的。祥林嫂是悲剧的,祥林嫂之死是很凄惨的。那么,祥林嫂究竟是怎样被“吃掉”的? 祥林嫂是一个受尽封建礼教压榨的穷苦农家妇女。丈夫死后,狠心的婆婆要将她出卖。她被逼出逃,到鲁镇鲁四老爷家做佣工,受尽鄙视、虐待。很快她又被婆婆家抢走,卖到贺家成亲。贺老六是个纯朴忠厚的农民,很快又有了儿子阿毛,祥林嫂终于过上了安稳日子。然而命运多舛,贺老六受地主的身心摧残饮恨死去,不久,阿毛又被狼吃掉。经受双重打击的祥林嫂,丧魂落魄,犹如白痴,可是人们还说她改嫁“有罪”,要她捐门槛“赎罪”,不然到了“阴间”还要受苦。她千辛万苦积钱捐了门槛后,依然摆脱不了人们的歧视。最后,她沿街乞讨,在除夕的鞭炮声中,惨死在街头。 文本中有这么一句话“大家仍然叫她祥林嫂”。这是祥林嫂的第二个丈夫贺老六死后,祥林嫂再次来到鲁镇,大家对她的称呼。然而祥林嫂已经再嫁,大家都不叫她“贺六嫂”,为什么仍然叫她“祥林嫂”呢? 小说写于辛亥革命爆发之后,帝制政权虽被推翻,但代之而起的却是地主阶级的军阀官僚的统治,封建社会的基础并没有彻底摧毁,中国的广大人民,尤其是农民,日益贫困化,他们过着饥寒交迫的生活,宗法观念、封建礼教仍然是压在人民头上的精神枷锁。在这样的背景之下,祥林嫂改嫁是“有罪”的,在“大家”眼里,祥林嫂是克夫克子的命,克死了第一任丈夫,第二任丈夫也死了,连她的儿子都被狼吃掉了。所以大家都认为祥林嫂是“不吉利”的,雇主鲁四老爷把她看成是伤风败俗的不祥之物,一切祭祀用品都用不着她沾手。镇上的人们也以挖苦祥林嫂为乐趣,都嘲笑她,奚落她,厌弃她。而笃信鬼神的女佣人柳妈又用死后的锯刑来吓唬