Will management of appendicitis have the
Journal of Visceral Surgery(2014)151,331—333
EDITORIAL
Will management of appendicitis have the
same fate as management of duodenal
ulcer?
KEYWORDS
Appendicitis;
Appendectomy;
Antibiotherapy;
Epidemiology
A report published in February2014by the Directorate of Research,Studies,Evaluation and
Statistics(DREES)of the ministry of Social Affairs and Health highlights the long decline in
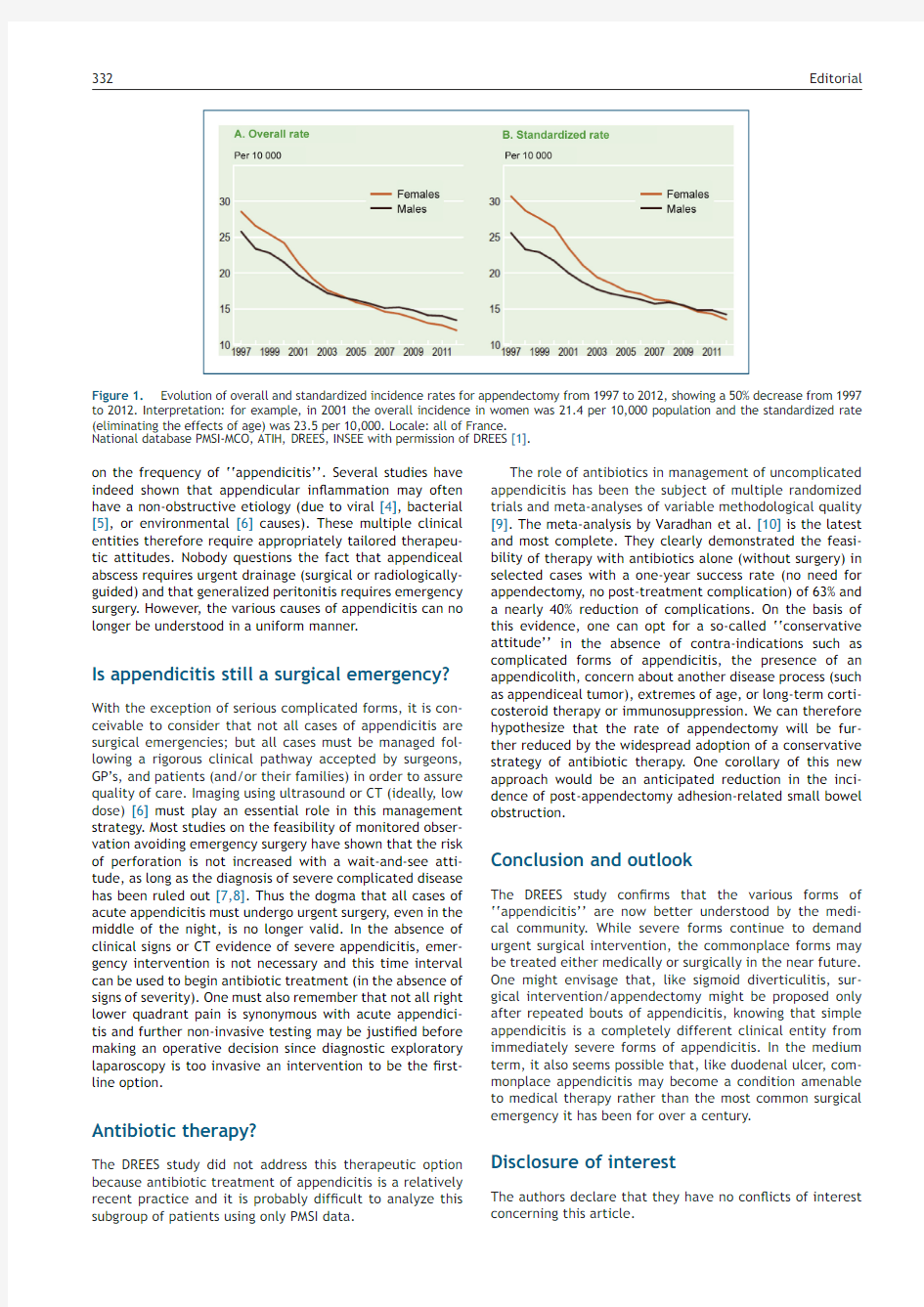
the frequency of appendectomy in France[1].The frequency of appendectomy has fallen
from more than300,000cases annually in the1980s to83,400in2012,a nearly four-fold
decrease(Fig.1).This analysis based on Program of medicalization of information systems
(PMSI)data also provides two more speci?c bits of information:the rate of serious or com-
plicated forms of appendicitis(appendiceal abscess or peritonitis)has remained relatively
stable,while the seasonable variability of non-complicated appendicitis has decreased
from1997through2012.The authors feel that this is related to‘‘a more timely recourse
to appropriate surgical care’’through the use of additional diagnostic testing(laboratory
and clinical scores,ultrasound,CT scan).In the authors’opinion,this decreased rate of
appendectomy bears witness to‘‘a change of attitude with regard to appendicitis by fam-
ily practitioners,pediatricians and surgeons as well as by families.’’But since this study
evaluated appendectomy rather than appendicitis,one can not exclude the possibility that
the decrease in the rate of appendectomy might also be due to a decline in the incidence
of appendicitis due to improved hygiene and dietary habits[2]of the French population.
This study con?rms the perception shared by all practitioners:we operate less and less
frequently on appendicitis.Older surgeons have lived through a period when our professors
forbade leaving a patient with appendicitis unoperated overnight while awaiting a change
of on-call surgeons.In recent years,surgeons have begun to recognize that‘‘appendicitis’’
is not a single entity but rather a variety of types of appendicitis that require different
management strategies.
Appendicitis:one or several clinical entities?
The DREES study con?rms the literature data by differentiating commonplace uncom-
plicated appendicitis from complicated appendicitis(abscess or peritonitis).These are
probably separate entities[3],since the natural evolution of simple appendicitis rarely
progresses to severe forms,as evidenced by the absence of a decline in the rate of severe
appendicitis,despite an increased rate of appendectomies in the United States in the1990s
[3].
On the other hand,the seasonal variation in the rate of appendectomy found in
the DREES study suggests several possible etiologies for appendicitis.The changing fre-
quency of‘‘appendectomy’’in France is thus consistent with the data in the literature
https://www.360docs.net/doc/0115352842.html,/10.1016/j.jviscsurg.2014.05.002
1878-7886/?2014Elsevier Masson SAS.All rights reserved.
332
Editorial
Figure1.Evolution of overall and standardized incidence rates for appendectomy from1997to2012,showing a50%decrease from1997 to2012.Interpretation:for example,in2001the overall incidence in women was21.4per10,000population and the standardized rate (eliminating the effects of age)was23.5per10,000.Locale:all of France.
National database PMSI-MCO,ATIH,DREES,INSEE with permission of DREES[1].
on the frequency of‘‘appendicitis’’.Several studies have indeed shown that appendicular in?ammation may often have a non-obstructive etiology(due to viral[4],bacterial [5],or environmental[6]causes).These multiple clinical entities therefore require appropriately tailored therapeu-tic attitudes.Nobody questions the fact that appendiceal abscess requires urgent drainage(surgical or radiologically-guided)and that generalized peritonitis requires emergency surgery.However,the various causes of appendicitis can no longer be understood in a uniform manner.
Is appendicitis still a surgical emergency? With the exception of serious complicated forms,it is con-ceivable to consider that not all cases of appendicitis are surgical emergencies;but all cases must be managed fol-lowing a rigorous clinical pathway accepted by surgeons, GP’s,and patients(and/or their families)in order to assure quality of care.Imaging using ultrasound or CT(ideally,low dose)[6]must play an essential role in this management strategy.Most studies on the feasibility of monitored obser-vation avoiding emergency surgery have shown that the risk of perforation is not increased with a wait-and-see atti-tude,as long as the diagnosis of severe complicated disease has been ruled out[7,8].Thus the dogma that all cases of acute appendicitis must undergo urgent surgery,even in the middle of the night,is no longer valid.In the absence of clinical signs or CT evidence of severe appendicitis,emer-gency intervention is not necessary and this time interval can be used to begin antibiotic treatment(in the absence of signs of severity).One must also remember that not all right lower quadrant pain is synonymous with acute appendici-tis and further non-invasive testing may be justi?ed before making an operative decision since diagnostic exploratory laparoscopy is too invasive an intervention to be the?rst-line option.
Antibiotic therapy?
The DREES study did not address this therapeutic option because antibiotic treatment of appendicitis is a relatively recent practice and it is probably dif?cult to analyze this subgroup of patients using only PMSI data.
The role of antibiotics in management of uncomplicated appendicitis has been the subject of multiple randomized trials and meta-analyses of variable methodological quality [9].The meta-analysis by Varadhan et al.[10]is the latest and most complete.They clearly demonstrated the feasi-bility of therapy with antibiotics alone(without surgery)in selected cases with a one-year success rate(no need for appendectomy,no post-treatment complication)of63%and a nearly40%reduction of complications.On the basis of this evidence,one can opt for a so-called‘‘conservative attitude’’in the absence of contra-indications such as complicated forms of appendicitis,the presence of an appendicolith,concern about another disease process(such as appendiceal tumor),extremes of age,or long-term corti-costeroid therapy or immunosuppression.We can therefore hypothesize that the rate of appendectomy will be fur-ther reduced by the widespread adoption of a conservative strategy of antibiotic therapy.One corollary of this new approach would be an anticipated reduction in the inci-dence of post-appendectomy adhesion-related small bowel obstruction.
Conclusion and outlook
The DREES study con?rms that the various forms of ‘‘appendicitis’’are now better understood by the medi-cal community.While severe forms continue to demand urgent surgical intervention,the commonplace forms may be treated either medically or surgically in the near future. One might envisage that,like sigmoid diverticulitis,sur-gical intervention/appendectomy might be proposed only after repeated bouts of appendicitis,knowing that simple appendicitis is a completely different clinical entity from immediately severe forms of appendicitis.In the medium term,it also seems possible that,like duodenal ulcer,com-monplace appendicitis may become a condition amenable to medical therapy rather than the most common surgical emergency it has been for over a century.
Disclosure of interest
The authors declare that they have no con?icts of interest concerning this article.
Editorial333
References
[1]Oberlin P,Mouquet MC.?La longue diminution des appendicec-
tomies en France?,études et résultats,n o868,DREES,Febru-ary;2014http://www.drees.sante.gouv.fr/IMG/pdf/er868.pdf (February24,2014).
[2]Walker AR,Segal I.What causes appendicitis?J Clin Gastroen-
terol1990;12:127—9.
[3]Livingston EH,Woodward WA,Sarosi GA,Haley RW.Disconnect
between incidence of non-perforated and perforated appen-dicitis:implications for pathophysiology and management.Ann Surg2007;245:886—92.
[4]Alder AC,Fomby TB,Woodward WA,Haley RW,Sarosi G,Liv-
ingston EH.Association of viral infection and appendicitis.Arch Surg2010;145:63—71.
[5]Livingston EH,Fomby TB,Woodward WA,Haley RW.Epidemi-
ological similarities between appendicitis and diverticulitis suggesting a common underlying pathogenesis.Arch Surg 2011;146:308—14.
[6]Kim K,Kim YH,Kim SY,et al.Low-dose abdominal CT for evalu-
ating suspected appendicitis.N Engl J Med2012;366:1596—605.
[7]Ingraham AM,Cohen ME,Bilimoria KY,et al.Effect of delay to
operation on outcomes in adults with acute appendicitis.Arch Surg2010;145:886—92.
[8]The United Kingdom National Surgical Research Collabo-
rative.Safety of short,in-hospital delays before surgery for acute appendicitis:multicentre cohort study,sys-tematic review,and meta-analysis.Ann Surg2014, https://www.360docs.net/doc/0115352842.html,/10.1097/SLA.0000000000000492[E-pub ahead of print].
[9]Kao LS,Boone D,Mason RJ.Antibiotics vs.appendec-
tomy for uncomplicated acute appendicitis.J Am Coll Surg 2013;216:502—5.
[10]Varadhan KK,Neal KR,Lobo DN.Safety and ef?cacy of
antibiotics compared with appendicectomy for treatment of uncomplicated acute appendicitis:meta-analysis of ran-domised controlled trials.BMJ2012;344:e2156.
K.Slim a,?,P.Oberlin b
a Service de chirurgie digestive,CHU Estaing,1,
place Lucie-Aubrac,63003Clermont-Ferrand,
France
b DREES,bureau?état de santéde la population?,
ministère des Affaires Sociales et de la Santé,14,
avenue Duquesne,75350Paris07SP,France
?Corresponding author.
E-mail address:kslim@chu-clermontferrand.fr
(K.Slim)
Available online2June2014