复合微孔止血粉
World J Urol (2013) 31:523–527
DOI 10.1007/s00345-011-0815-8
ORIGINAL ARTICLE
Athermal nerve sparing robot-assisted radical prostatectomy: initial experience with microporous polysaccharide hemospheres as a topical hemostatic agent
Rafael Nunez-Nateras · Kimberly J. Hurd · Erin N. Ferrigni ·
Erik P. Castle · Paul E. Andrews · Mitchell R. Humphreys
Received: 26 April 2011 / Accepted: 13 December 2011 / Published online: 25 December 2011
? Springer-Verlag 2011
Abstract
Purpose Microporous polysaccharide hemospheres (MPH) are hemostatic beads engineered from plant starch to acceler-ate the natural clotting cascade. The purpose of this report is to detail our initial experience with MPH as a topical hemo-static agent during robot-assisted radical prostatectomy (RARP).
Methods We examined a single surgeon series of 30 con-secutive RARP’s dividing patients into MPH or non-MPH groups. The last ten procedures utilized the MPH, which were matched 1:2 to non-MPH procedures for comparison. Nerve-sparing procedures were performed when clinically indicated and all done athermally. All demographic data, length of operation, margin status, blood loss, change in hemoglobin, and need for blood transfusion were prospec-tively collected and analyzed.
Results The baseline characteristics were the same. The post-operative decrease in hemoglobin was less in the MPH group (1.8g/dL MPH group vs. 3.2g/dL non-MPH). One patient in each group required a blood transfusion. Conclusions These preliminary W ndings support the role for MPH as a potential hemostatic agent during athermal nerve-sparing RARP.
Keywords Topical hemostatic agent ·
Robot-assisted radical prostatectomy ·
Microporous polysaccharide hemospheres Introduction
The advancement of minimally invasive surgical tech-niques has produced various challenges compared to tradi-tional open surgical approaches. These limitations include visualization, available instrumentation, spatial constraints, and accessibility that can all impede the ability of the sur-geon to e Y ciently control bleeding [1]. Acute blood loss has been the most frequently reported intraoperative com-plication during radical prostatectomy [2]. Because of the rich blood supply of the prostate pedicle and neurovascular bundles, there is potential for a signi W cant amount of bleed-ing during and after radical prostatectomy. Intraoperative bleeding cannot only a V ect perioperative morbidity and transfusion requirement, but it can also obscure the sur-geon’s W eld of vision of the prostatic apex and neurovascu-lar bundles impairing accurate surgical dissection [3].
Preservation of the neurovascular bundles (NVB) and concomitant structures are of the utmost importance in appropriately selected patients during radical prostatectomy in order to preserve sexual function and continence [4]. Excess blood loss near or from the NVB can create pressure at the vesicourethral anastomosis after surgery that can dis-place or cause separation of the anastomosis thereby increasing the risk of a urine leak or alternatively can put undo strain on the NVB themselves. Excessive pressure on the NVB can impede continence, urinary function, and thus overall patient satisfaction [4]. Attempts to control blood loss can result in additional injury if thermal energy or neu-rotoxic hemostatic agents are used.
Most surgeons attempt to limit neurovascular injury through a variety of techniques and methods. Limiting the amount of thermal injury near the NVB and minimizing the manipulation of these structures should be the endeavor of every surgeon. This often results in an accepted increase in
R. Nunez-Nateras (&) · K. J. Hurd · E. N. Ferrigni · E. P. Castle · P. E. Andrews · M. R. Humphreys
Mayo Clinic Arizona, 5777 E Mayo Blvd,
Phoenix, AZ 85054, USA
e-mail: nunez.rafael@https://www.360docs.net/doc/0d16213335.html,
venous oozing from the NVB. Thus, many surgeons turn to topical hemostatic agents to prevent signi W cant blood loss, hematoma formation, and post-operative bleeding during nerve-sparing surgery. The ideal hemostatic agent should be non-immunogenic, economical, readily available, easy to deploy, and biodegradable.
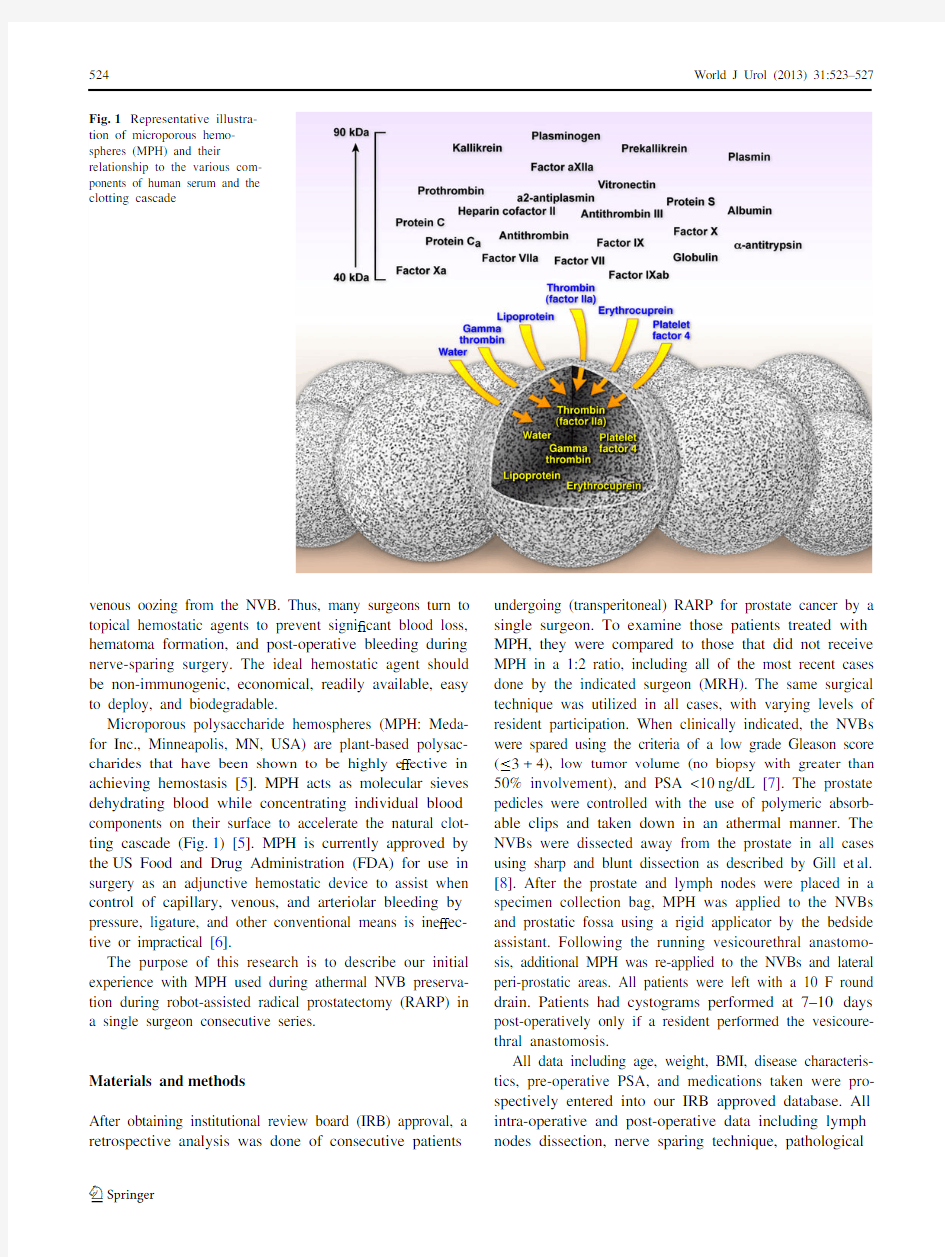
Microporous polysaccharide hemospheres (MPH: Meda-for Inc., Minneapolis, MN, USA) are plant-based polysac-charides that have been shown to be highly e V ective in achieving hemostasis [5]. MPH acts as molecular sieves dehydrating blood while concentrating individual blood components on their surface to accelerate the natural clot-ting cascade (Fig.1) [5]. MPH is currently approved by the US Food and Drug Administration (FDA) for use in surgery as an adjunctive hemostatic device to assist when control of capillary, venous, and arteriolar bleeding by pressure, ligature, and other conventional means is ine V ec-tive or impractical [6].
The purpose of this research is to describe our initial experience with MPH used during athermal NVB preserva-tion during robot-assisted radical prostatectomy (RARP) in a single surgeon consecutive series.
Materials and methods
After obtaining institutional review board (IRB) approval, a retrospective analysis was done of consecutive patients undergoing (transperitoneal) RARP for prostate cancer by a single surgeon. To examine those patients treated with MPH, they were compared to those that did not receive MPH in a 1:2 ratio, including all of the most recent cases done by the indicated surgeon (MRH). The same surgical technique was utilized in all cases, with varying levels of resident participation. When clinically indicated, the NVBs were spared using the criteria of a low grade Gleason score (·3+4), low tumor volume (no biopsy with greater than 50% involvement), and PSA <10ng/dL [7]. The prostate pedicles were controlled with the use of polymeric absorb-able clips and taken down in an athermal manner. The NVBs were dissected away from the prostate in all cases using sharp and blunt dissection as described by Gill et al.
[8]. After the prostate and lymph nodes were placed in a specimen collection bag, MPH was applied to the NVBs and prostatic fossa using a rigid applicator by the bedside assistant. Following the running vesicourethral anastomo-sis, additional MPH was re-applied to the NVBs and lateral peri-prostatic areas. All patients were left with a 10 F round drain. Patients had cystograms performed at 7–10days post-operatively only if a resident performed the vesicoure-thral anastomosis.
All data including age, weight, BMI, disease characteris-tics, pre-operative PSA, and medications taken were pro-spectively entered into our IRB approved database. All intra-operative and post-operative data including lymph nodes dissection, nerve sparing technique, pathological
Fig.
1Representative illustra-
tion of microporous hemo-spheres (MPH) and their relationship to the various com-ponents of human serum and the clotting cascade
analysis, surgical time, estimated blood loss, change in hemoglobin, length of surgery, length of catheterization,and prostate size were collected as well. The data were ana-lyzed with commercially available software, SPSS ? version 10.0 statistical package (SPSS Inc., Chicago, IL, USA). All data were statistically analyzed with chi-square and Mann–Whitney U test for categorical and continuous variables,respectively. A two-sided P value <0.05 was considered as statistically signi W cant.
Results
Patient demographic data are in Table 1. Both groups were similar in make up and disease characteristics. Figure 2a–c represents the NVBs in a representative patient before and after MPH application as well as after the vesicourethral anastomosis, respectively. The surgical and pathological outcomes are presented in Table 2. The change in hemoglo-bin after 24h was much less in the MPH group, but this did not translate into a statistically signi W cant lower transfusion rate. While one patient in each group required a transfusion,the MPH patient actually bled from his left obturator fossa where MPH was not applied. The subsequent cross-sectional imaging from that patient’s scan revealed no hematoma or bleeding from the NVBs or prostatic fossa,Fig.3. Urinary extravasation was identi W ed in two patients in the non-MPH group requiring prolonged catheterization.There were no other complications identi W ed in the 30day peri-operative period.
Discussion
To our knowledge, this is the W rst study to detail the use of MPH during robot-assisted prostate surgery. The various techniques of nerve preservation during RARPs described in the literature signi W cantly improve functional outcomes for patients and are an important consideration for sexually active patients. However, due to the vascular investments
of the prostate and NVB, there is a potential for bleeding during prostatectomy that can a V ect patient outcomes [8].This report describes our experience with a topical hemo-static agent (MPH) during athermal NVB preservation dur-ing RARP.
The surgeries were all done by a single surgeon (MRH)who has been performing RARP since 2003, thereby decreasing the confounding e V ects of experience and learn-ing curve on the speci W c surgical technique. The age, BMI,ASA, pre-operative Gleason, and PSA scores were not
Table 1Median patient demographic data
MPH group
Non-MPH group P Number of patients 1020Age (years)63 (51–77)64 (49–74)0.372BMI (kg/m 2)29 (22–36)29 (22–41)0.614ASA score
2 (2–3) 2 (2–3)0.802Pre-operative PSA (ng/mL) 6.1 (3.7–9.4) 6.2 (1.3–16)
0.721Pre-operative Gleason sum 7 (6–7)7 (6–8)0.911On aspirin at surgery (%)
5 (50%)
7 (35%)
0.461
Fig.2
a Representative image of bilateral neurovascular preservation after robot-assisted radical prostatectomy.
b Representative image of the same patient after application of the MPH to the neurovascular bun-dles.
c Representative image of the same patient after the vesicoure-thral anastomosis with MPH application to the anterior urethral vesical junction
signi W cantly di V erent in either group. Interestingly 50%,compared to 35%, of the MPH patients were on aspirin at the time of surgery thereby presumably increasing their potential risk for bleeding. However, the estimated blood loss and change in hemoglobin values favored the patients in the MPH group, regardless of concomitant use of anti-platelet therapy.
One patient from each group required a blood transfu-sion. However, for the patient in the MPH group, this was
due to a bleed originating in the obturator fossa, as a result of the lymphadenectomy where no MPH was applied. It is di Y cult to place the MPH in the right obturator fossa due to the location of the assistant ports during RARP. In the future, this could be over come by de-docking the robot and placing the applicator through a contralateral port.
Other topical hemostatic agents have been used dur-ing surgeries to decrease bleeding. The topical applica-tion of BioGlue (CryoLife, Inc., Kennesaw, GA)generally requires a dry W eld prior to application [9].Therefore, acute, vigorous bleeding cannot be controlled by this agent. MPH can be applied to an actively bleed-ing source because of its unique mechanism [1, 5]. Evi-cel (Ethicon Inc., Somerville, NJ) is a human product that uses tranexamic acid. It has been reported to be neu-rotoxic and has caused convulsions, hyperexcitability,and death in rats [10]. Another concern of this product is that it has a prolonged preparation time of up to 40min to reconstitute [10]. QuickClot (Z-Medica Corp., Wal-lingford, CT) is composed of zeolite, a microporous crystalline aluminosilicate, which absorbs X uid causing an exothermic reaction [11]. This has been associated with necrosis and third degree thermal injury in the sur-rounding tissue and should never be used intracorparally [12]. MPH is not associated with any exothermic or known neurotoxicity.
The active mechanism of hemoconcentrating endoge-nous clotting factors, which initiates particle swelling by osmotic forces, provides natural sca V olding on which a W brin matrix can form. The clot formed by the expanded MPH beads, platelets, and clotting proteins has been shown to be more resilient than a purely natural clot [13]. The MPH is then enzymatically broken down into small water-soluble fragments that leave no trace or radiographic evidence within 12h of application [14,15]. Because MPH is derived from a plant source, the risk of disease transmission or allergic reaction is mini-mal [15]. The production costs are theoretically low because it is manufactured from a readily available source.
Despite the encouraging preliminary results, there are limitations to this study that should be considered. There were only 30 patients examined in this initial study, which hampers the power of this study. A larger randomized pro-spective trial is needed to validate these W ndings and better de W ne the role for MPH in prostate surgery. Long-term fol-low up is also needed as yet unrecognized e V ects due to MPH may have a negative impact on long-term NVB recovery. This data represent a single surgeon series at a training facility, and resident participation and experience could impact variations in surgical technique. However,direct supervision was present during all phases of every surgical procedure.
Table 2Median surgical characteristics and outcomes
a
Four patients had positive margins: pT2c 3+3, pT3a 4+3, pT3a 5+4, and pT3b 4+3
MPH group
Non-MPH group P Lymphadenectomy (%)10 (100%)20 (100%)–Nerve sparing –
Bilateral 9/1016/20Unilateral 1/102/20None
0/102/20Pathologic prostate size (g)62 (45–98)
68 (33–118)0.328Post-op Gleason sum 7 (6–8)7 (6–9)0.476OR time (min)195 (126–335)239 (165–294)
0.038Negative margins 100%80%a
0.272EBL (mL)
170 (50–400)220 (50–750)0.371Change in Hgb (g/dL) 1.8 (0.1–5) 3.2 (1.6–6.4)0.020Transfusion (%) 1 (10%) 1 (5%)0.999Length of stay (days) 1 (1-3) 1 (1-4)0.024Catheterization (days)
9 (6–14)
10 (7–30)
0.514Fig.
3Computed tomography image of the one patient in the MPH treated group that required a blood transfusion. Note the location of the bleed was from the left obturator fossa in the area of the node dissec-tion where no MPH was applied
Conclusions
This preliminary study indicates that MPH may be a useful adjunctive hemostatic agent during RARP. The changes in post-operative hemoglobin were minimized with no dis-cernible complications in the 30day peri-operative period. MPH appears to be a useful hemostatic tool that the urolo-gist should considering adding to their armamentarium. Acknowledgments The authors especially thank Desert Mountain C.A.R.E. for their support of prostate cancer research and this project.
Con X ict of interest The authors have no con X icts of interest or W nancial relationships with any of the materials sited in this work. No additional outside funding was utilized to complete this work. The authors have maintained control of the primary data throughout all phases of this work.
References
1.Humphreys MR, Lingerman JE, Terry C et al (2008) Renal injury
and the application of polysaccharide hemospheres: a laparoscopic experimental model. J Endourol 22:1375–1381
2.Kordan Y, Barocas D, Altamar H et al (2010) Comparison of
transfusion requirements between open and robotic-assisted lapa-roscopic radical prostatectomy. BJU 106:1036–1040
3.Farnham S, Webster T, Herrell D et al (2006) Intraoperative blood
loss and transfusion requirements for robotic-assisted radical pro-statectomy versus radical retropubic prostatectomy. Urology 67:360–367
4.Montorsi F, Salonia A, Nazareno S et al (2005) Improving the
preservation of the urethral sphincter and neurovascular bundles
during open radical retropubic prostatectomy. Eur Urol 48:938–945
5.Humphreys MR, Castle EP, Andrews PE et al (2008) Microporous
polysaccharide hemospheres for management of laparoscopic tro-car injury to the spleen. J Am Surg 195:99–103
6.Food and Drug Administration Approval Letter (2006) Arista AH
absorbable Hemostat-P050038
7.Fanning DM, Kay E, Fan Y et al (2009) Prostate cancer grading:
the e V ect of strati W cation of needle biopsy Gleason score 4+3 as high or intermediate grade. BJU 105:631–635
8.Gill IS, Ukimura O, Rubinstein M et al (2005) Lateral pedicle con-
trol during laparoscopic radical prostatectomy: re W ned technique.
J Urol 65:23–27
9.Nadler RB, Loeb S, Rubenstein RA et al (2006) Use of BioGlue in
laparoscopic partial nephrectomy. Urology 68:416–418
10.Schwartz M, Madariaga J, Hirose R et al (2004) Comparison of a
new W brin sealant with standard topical hemostatic agents. Arch Surg 139:1148–1154
11.Sefck J, McCormick AV (1999) Prediction of crystallization dia-
grams for synthesis of zeolites. Chem Eng Sci 54:3513
12.Wright JK, Kalns J, Wolf EA et al (2004) Thermal injury resulting
from application of a granular mineral hemostatic agent. J Trauma 57:224–230
13.Dong Y, Schrader L, Drake JF et al (2001) Hemostatic does re-
sponse of degradable starch microspheres (DSM45) as measured by thromboelastography. Presented at: Network for advancement of transfusion alternatives 2nd annual symposium, Berlin, Germany
14.Hamdi G, Ponchel G (1999) Enzymatic degradation of epichloro-
hydrin crosslinked starch microspheres by alpha-amylase. Pharm Res 16:867–875
15.Murat FL, Ereth MH, Dong Y et al (2004) Evaluation of micropo-
rous polysaccharide hemospheres as a novel agent in open partial nephrectomy: favorable experimental results in the porcine model.
J Urol 172:1119–1122
壳聚糖的功用详解
壳聚糖的功用详解,每位卫康家人必备的资料 壳聚糖的应用 1、食道癌——壳聚糖兑水,虫草兑水喷。每小时交替使用。 2、降压——壳聚糖每天6粒。 3、拉肚子——孩子1粒壳聚糖抖在饭里。 4、孩子长的过快——肌肉裂断,加壳聚糖。 5、癌症——每天50粒,可以活命。 6、身上所有包块——均需壳聚糖。 7、肾衰竭——壳聚糖加虫草。 8、减肥——壳聚糖加银兰。 9、肠胃不好,便秘——壳聚糖。 10、白癜风——壳聚糖,虫草,金苓,五个月。 11、糖尿病——壳聚糖加虫草。 12、脑血栓——壳聚糖,银兰,虫草。 壳聚糖溶液的作用 2粒壳聚糖+纯净水35毫升+白醋2毫升——壳聚糖啫喱水 一、浓度:加200毫升纯净水 1、去角质,每天2-3次 2、足,手上的白癣 3、伤口愈合,淡化瘢痕 4、喂鱼5-10毫升 二、浓度:1000毫升
1、皮肤过敏 2、黑斑,汗斑,湿疹,皮炎 3、香港脚,富贵手 4、代替洗发精 三、浓度:2000毫升 1、面疮,颜面白癣 2、荨麻疹 3、基础化妆 4、男士剃须后使用 壳聚糖的妙用 1、外伤:有外伤、烧伤烫伤、溃疡时可以将产品直接敷于伤口处,有止血止疼、止痒、杀菌、消炎之功效,且愈后不留疤痕。 2、治带状疱疹:用白醋把产品调成稠糊状,涂抹于患处,3-7天可痊愈。 3、治褥疮:将伤处清理消毒后,把产品直接敷于患处,1-3天可结痂愈合。 4、治口腔、食道溃疡:将产品直接倒入口中含放2-3次/日,1-2天可痊愈。 5、治红斑狼疮:内服:每日3次,每次4-6粒;外涂:把产品用白醋调匀,涂抹于患处,一个疗程可痊愈。 6、治面瘫:每天3次,每次3-4粒,2-7天(麻痹的面部神经修复)痊愈。 7、治便秘:早晚服2-4粒/次,饭前服用,多喝水。多吃水果蔬菜效果明显。对肠胃炎和痔疮有奇效!8、治脚气:将产品直接敷于患处,2-3天痊愈不复发。用白醋调和以后,涂抹于手脚表面可预防、治疗脚气、手脚发痒、脱皮。 9、治疗湿疹:用白醋把产品调匀,涂于患处2-4天可痊愈。此法对治疗男女阴部瘙痒、阴湿、湿疹有奇效!2-3次可痊愈。 10、减肥:早晚服用,每次6-10粒,饭前服用,配合晚餐少吃主食效果显著。
医用生物可吸收止血材料的研究现状与临床应用
中国组织工程研究第16卷第21期 2012–05–20出版 Chinese Journal of Tissue Engineering Research May 20, 2012 Vol.16, No.21 ISSN 1673-8225 CN 21-1581/R CODEN: ZLKHAH 3941 1College of Orthopedics and Traumatology, Fujian University of Traditional Chinese Medicine, Fuzhou 350108, Fujian Province, China; 2Orthopedic Trauma Center, the 175 Hospital of Chinese PLA, Affiliated Southeast Hospital of Xiamen University, Zhangzhou 363000, Fujian Province, China Zhang Shao-feng★, Studying for master’s degree, College of Orthopedics and Traumatology, Fujian University of Traditional Chinese Medicine, Fuzhou 350108, Fujian Province, China zhangshaofeng017@ https://www.360docs.net/doc/0d16213335.html, Corresponding author: Hong Jia-yuan, Master’s supervisor, Associate chief physician, Orthopedic Trauma Center, the 175 Hospital of Chinese PLA, Affiliated Southeast Hospital of Xiamen University, Zhangzhou 363000, Fujian Province, China hongjy175@ https://www.360docs.net/doc/0d16213335.html, Received: 2011-11-12 Accepted: 2012-01-09 医用生物可吸收止血材料的研究现状与临床应用★ 张少锋1,洪加源2 Research status and clinical application of biomedical absorable hemostic materials Zhang Shao-feng1, Hong Jia-yuan2 Abstract BACKGROUND: Now, various hemostasis materials are developed with different components and mechanisms. Due to their different characteristics, the applications are different. OBJECTIVE: To review the commonly used clinical absorbable hemostatic materials at home and abroad, and to summarize the composition, hemostatic mechanism and clinical application for guiding clinicians to use them effectively. METHODS: A computer-based search of CNKI and PubMed databases (2002-02/2011-05) were performed for articles related to hemostatic materials using the key words of “biological material, hemostatic material, bioresorbable material, hemostatic effect, hemostatic mechanism” in Chinese and English, respectively. Literatures on application of biomedical absorbable hemostatic materials were adopted, and others about duplicated study and contents inconsistent with the research purpose were excluded. RESULTS AND CONCLUSION: Currently, fibrin glue, cellulose, xycellulose, α-cyanoacrylate tissue glue, chitosan and so on are adsorbable hemostasis materials in clinic. The hemostatic reason of chitosan is that the chitosan has some quantitative electric charge, which can directly occur cross linking reaction with the red blood cells on the wound surface to form blood clot, and the hemostasis process is independent of blood coagulation factor and platelet in vivo. Delightfully, α-cyanoacrylate tissue glues not only are used to cardiovascular surgery for small vascular anastomisis, to neurosurgery for repairing cerebral dura mater, to orthopedics for cohereing the fracture and repairing the soft tissues and so on, but also are the prefer material for intervention embolotherapy. While the fibrin glue can not only be local hemostasis, prevent conglutination and seepage, but also mainly be slow-release trager, bone material frame. However, different hemostasis materials have different hemostasis mechanisms and effects, so only to sufficiently comprehend the characteristic of different hemostasis materials can use them more reasonable and available. Zhang SF, Hong JY. Research status and clinical application of biomedical absorable hemostic materials. Zhongguo Zuzhi Gongcheng Yanjiu. 2012;16(21): 3941-3944. [https://www.360docs.net/doc/0d16213335.html, https://www.360docs.net/doc/0d16213335.html,] 摘要 背景:目前市场已开发出多种不同组成和不同机制的止血材料,因其不同特性而应用各异。 目的:概述国内外临床常用医用可吸收止血材料,对其组成、止血机制及临床应用进行总结,指导临床医生更加合理有效 地应用止血材料。 方法:应用计算机检索CNKI和PubMed数据库中2002-02/2011-05关于止血材料的文章,以“生物材料,止血材料,生 物可吸收材料,止血效果,止血机制”或“biomaterial,hemostatic material,bioresorbable material,hemostatic effect,hemostatic mechanism”为中、英文关键词。纳入与生物可吸收止血材料及其应用相关的文章;排除重复研究的内容和与 研究目的不相符的文献。 结果与结论:目前国内外主要应用的可吸收止血材料为纤维蛋白胶、氧化纤维素和氧化再生纤维素、α-氰基丙烯酸酯类组 织胶、壳聚糖等。壳聚糖的止血性在于壳聚糖带有一定量的电荷,它的分子直接与创面上的红细胞发生交联反应形成血凝 块,它的止血过程不依赖于机体凝血因子和血小板。α-氰基丙烯酸酯类黏合剂已应用于血管外科的中小管径血管吻合、神 经外科的中硬脑膜修补、各类软组织修补、骨科中骨折的黏合等,并且成为介入栓塞治疗中的首选材料。在骨科领域纤维 蛋白胶除了局部止血、防止粘连和渗漏外主要是作为缓释载体,骨材料支架而发挥作用。氧化纤维素和氧化再生纤维素已 成功应用于神经外科、耳鼻喉科、肝胆外科等。不同的止血材料其止血机制和止血效果均不同,只有充分了解各种止血材 料性能,才能合理、有效应用。 关键词:止血材料;生物材料;生物可吸收;止血效果;止血机制 doi:10.3969/j.issn.1673-8225.2012.21.033 张少锋,洪加源.医用生物可吸收止血材料的研究现状与临床应用[J].中国组织工程研究,2012,16(21):3941-3944. [https://www.360docs.net/doc/0d16213335.html, https://www.360docs.net/doc/0d16213335.html,] 0 引言 出血是创伤后主要并发症,出血过多必将引起休克,危及生命。因此及时有效止血对挽救患者生命具有重要意义。有效的止血不但是外科手术中需要解决的重要问题,也是战、创伤中提高伤员生存率的关键问题。出血后如何止血一直困扰着人类。在古代,古人用中草药或药膏等止血,而古埃及人使用蜂蜡、油脂等的混合物来止血[1]。随着科学技术的不断发展,骨蜡等非可吸收性止血材料已大量应用于临床,但这些非可吸收性止血材料引起的术区感染和其他并发症在所难免。近年来医用可吸收止血材料引起了各国医学界和产业界的高度重视,许多大型医药公司都致力于研发新型止血材料[2]。目前市场已开发出多种不同组成和不同机制的止血材料,因其不同特性而应用各异。 万方数据
美司特止血粉作为新型壳聚糖止血粉止血作用的实验研究
美司特止血粉作为新型壳聚糖止血粉止血作用的实验研究 美司特速效止血粉通用名称壳聚糖粉状医用功能敷料主要成分壳聚糖是 由β-(1,4)糖苷键连接的氨基葡萄糖大分子天然聚合物,是自然界中唯一带 有正电荷作用的多糖。壳聚糖具有多种生物学功能,作为创伤修复材料,国内 外大量科学研究结果证明:具有良好的止血作用、抗菌抑菌作用、镇痛作用、 加快创面伤口愈合和减少疤痕增生等作用。 实验目的: 探讨通过剂型改造和结构改变制备的一种新型壳聚糖止血粉的止血作用。 实验方法; 取成年SD大鼠24只,雌雄不限,体重210g~240g,制备肝中叶切除出血模型,根据切口使用止血材料不同随机分为 3 组(n=8),A1组300 mg 云南白药,B1 组300 mg pH6.5 的新型壳聚糖止血粉,C1 组300 mg pH7.5 的新型壳聚糖止血粉,记录出血时间及出血量。采用Lee 等方法进行体外促凝血实验。分别取0.2 mL 终浓度为0.2 mg/mL 的云南白药(A2 组)、pH6.5 的新型壳聚糖止血粉(B2 组)及pH7.5 的新型壳聚糖止血粉(C2 组)溶液,与2mL 新西兰兔耳中央动脉血混匀,记录凝血时间。并取B2 组及C2 组壳聚糖血凝块进行扫描电镜观察。 实验结果 A1、B1 及C1 组出血时间分别为(292±31)、(261±23)、(224±28)s,出血量分别为(1.63±0.21)、(1.47±0.18)、(1.18±0.17)g;B1 组及C1 组出血时间及出血量与A1 组比较,差异均有统计学意义(P<0.05);且C1 组优于B1组(P<0.05)。A2、B2及C2组凝血时间分别为(653±41)、(255±20)、(202±11)s,B2、C2 组与A2 组比较,差异均有统计学意义(P<0.05);且C2 组优于B2 组(P<0.05)。扫描电镜下可见B2 组及C2 组血细胞均聚集于壳聚糖周围。 实验结论 美司特速效止血粉采用壳聚糖粉末制成。产品淡黄色无定型粉末,含水量不得大于10%,壳聚糖含量不低于80%。具有良好的止血作用。
壳聚糖_海藻酸钠_云南白药复合膜止血效果实验研究
第31卷第2期 2011年4月健康研究Health Research Vol.31No.2Apr.2011收稿日期:2010-05-20 基金项目:杭州师范大学2009-2010学年学生科研批准立项项目(0983XXM128) 作者简介:卢斌(1989-),男,浙江金华人,本科。 通讯作者:章志量(1961-),男,浙江杭州人,教授,硕士研究生导师,研究方向:外科学。 DOI :10.3969/j.issn.1674-6449.2011.02.004基础医学 壳聚糖/海藻酸钠—云南白药复合膜 止血效果实验研究 卢斌,胡思思,诸娴,张良田,章志量 (杭州师范大学临床医学院,浙江杭州310036) 摘要:目的观察壳聚糖/海藻酸钠—云南白药复合膜的止血性能。方法制备壳聚糖/海藻酸钠—云南白药复合膜 组(I 组)同时设立模型对照组与明胶海绵对照组:壳聚糖/海藻酸钠复合止血膜组(II 组),壳聚糖止血膜组(III 组),明胶海绵组(IV 组)进行比较。半定量评价改良壳聚糖止血膜的止血效果。结果: 结果显示I 组与模型对照组及明胶海绵对照组的止血时间显著差异(P <0.01)。结论 壳聚糖/海藻酸钠—云南白药复合膜表现出显著的协同作用,止血作用显著强于其他各组,复合后膜的止血效果得到了较大提高,可望在创伤止血、外科手术上得到 广泛应用。 关键词:壳聚糖;海藻酸钠;云南白药;止血 中图分类号:R319文献标识码:A 文章编号:1674-6449(2011)02-0094-03Experimental Study of Hemostasis Effect of Chitosan /sodium-Alginate-Yunnanbaiyao Composite Film LU Bin ,HU Si-si ,ZHU Xian ,ZHANG Liang-tian ,ZHANG Zhi-liang (Clinical College of Hangzhou Normal University ,Hangzhou ,Zhejiang 310036,China ) Abstract :Objective To investigate the role of chitosan /sodium-alginate-yunnanbaiyao composite films on hemostasis function.Methods Four groups were compared :chitosan /sodium-alginate-yunnanbaiyao composite film group (Ⅰ), Chitosan /sodium-alginate composite film group (Ⅱ),chitosan hemostatic film group (Ⅲ)and gelfoam group (Ⅳ)The hemostatic effect of different groups were analyzed by semi-quantitative evaluation.Results The hemostatic time of Group Ⅰwas significantly shorter than other three groups (P <0.01).Conclusion Chitosan /sodium alginate-yunnanbaiyao composite film has better hemostatic effect ,compared with other three groups.There is a significant synergistic action among chitosan /sodium ,alginate and yunnanbaiyao.This method can be widely used for the treatment of traumatic and surgical hemorrhage. Key words :Chitosan ;Sodium Alginate ;Yunnanbaiyao ;Hemostasis
创伤急救止血包扎技术操作流程
创伤急救止血包扎技术操作流程 某伤员在意外事故中受伤,左前臂中段有一伤口6×8cm,呈喷射性大出血。请你抢救。 1、戴手套。 2、操作者准备好后立正,大声向评委报告: 报告评委,x号做创伤急救技术操作准备完毕,请指示! 评委说:开始!(计时) 3、评估周围环境安全: (1)、操作者用眼光从左到右扫视,上下扫视后。 (2)、大声说:“现场环境安全”! (3)快速走向伤员,用右手四指握住伤员压在左上臂上部中点偏内,用力将肱动脉压向肱骨,小声说:我是救援人员,我来帮你,请你不要着急。请你配合我们! 4、认真检查伤员伤情及出血情况。大声说:“左前臂中段掌面有一伤口6×8cm,有动脉出血。” 5、引导病人快速止血:指导伤员用健肢右手拇指在左上臂肱动脉止血协助指压止血,同时操作者立即将伤员左前臂抬起(超过心脏高度),大声说:抬高2分钟。 6、准备物品(转身开始到物品准备完全,端物品盘放下20秒) 止血带1个、三角巾2张、10公分无菌敷料1张、弹力绷带1个、标牌1个、笔1支、胶布1个、剪刀1把。 7、接着在左上臂1∕3先加布垫保护皮肤,再上止血带,检查止血效果(扪左前臂桡动脉搏动),扣上标牌并报告止血时间。 8、快速包扎: (1)、认真检查在左前臂的伤口,大声说:没有异物和骨折! (2)、操作者用右手拿无菌纱布一面,(敷料手接触面不能接触创面,敷料应大于损伤创面),盖在左前臂伤口创面上。 (3)、再用弹力绷带先在敷料远端环形扎两圈使其牢固,然后螺旋形向上包扎,每一圈适当加压压住上一圈的三分之二,使绷带卷边缘保持整齐,最后平绕一圈,在伤肢外侧用绷带扣固定,包扎完毕敷料不能有外露,要整齐、美观、大方。(4)、用三角巾悬吊伤肢80-85度,三角巾打平节在左侧的锁骨上,留出手指末端,便于检查止血效果。 9、伤员取半卧位。(操作计时结束) 10、操作者大声说:报告评委,x号做创伤急救技术操作完毕,请指示! 11、评委说:归队! 12、操作者向右转!跑步离开!
壳聚糖相关的所有产品资料
壳聚糖相关的所有产品资料 1.壳聚糖栓 产品组成:壳聚糖、聚乙二醇单硬脂酸酯制成栓粒,加指套或推注器组成。主要性能:1. 装量允差为±10%。融变时限≤60min.3. PH应在4.5~6.5。4. 壳聚糖栓对金黄色葡萄球菌、大肠杆菌、白色念珠菌的抑菌率大于90%。5. 经Co60辐照灭菌,产品无菌。 适用于:细菌性阴道病和霉菌性阴道炎引起的阴部瘙痒灼痛、阴道分泌物增多、外阴充血肿胀的症状。 2.壳聚糖敷料 产品组成:本产品分为非粘型和自粘型。非粘型单独由敷芯制成,材料是非织造壳聚糖纤维无纺布;自粘型由背衬、敷芯、隔离纸(膜)组成,背衬由无纺布基材涂医用压敏胶制成,敷芯由非织造壳聚糖纤维无纺布或非织造壳聚糖纤维无纺布与非织造吸水纤维布复合组成,隔离纸(膜)由格拉辛纸(PET膜)制成。适用于:适用于体表创口保护、促进伤口愈合、预防伤口感染。 3.壳聚糖凝胶 产品组成:该产品由壳聚糖、卡波姆、羧甲基纤维素钠、甘油、纯化水等组成。Ⅰ型产品采用聚乙烯材料注塑成型的推助器包装;II型产品采用塑料软管包装。主要性能:a)壳聚糖含量不低于2.5%;b)ph值为5.0-7.8;c)微生物限度:细菌菌落总数不大于100cfu/g,大肠埃希菌,金黄色葡萄球菌、白色念珠菌不得检出。 适用于:该品适用于细菌性、霉菌性阴道炎和宫颈炎患者。 4.壳聚糖漱口液 产品组成:产品为壳聚糖、ε-聚赖氨酸、纳他霉素、阿斯巴甜、柠檬香精、纯化水组成的溶液。 适用于:用于抑制口腔内细菌总数,改善口臭、口腔溃疡疾病。 5.壳聚糖抗菌膜 产品组成:产品由膜和夹持器两部分组成;膜是由壳聚糖、壳碘〔CMCTS-g-(PAANa-CO-PVP)-I2和明胶制成;夹持器采用的医用高分子材料(医用聚丙烯)制成,夹持器的弹簧应操作灵活;膜的凝冻浓度倒置10秒钟应不流下;对大肠杆菌和金黄色葡萄球菌的抑菌率应≥50%;膜的细菌内毒素应不大于0.5EU/ml;膜应不大于极轻微刺激和不大于轻微细胞毒性;产品应无迟发型超敏反应和急性全身毒性反应;产品经钴-60γ灭菌,应无菌。 适用于:产品用于轻度宫颈糜烂的治疗,慢性宫颈炎手术创面的保护、促进愈合。 6.壳聚糖护脐带 产品组成:由脐贴(壳聚糖无纺布、碳纤维、吸水棉)、弹性基带和魔术贴组成。 适用于:供新生儿脐带结扎后为残端保护时一次性使用。 7.壳聚糖妇科凝胶 产品组成:壳聚糖妇科凝胶由壳聚糖凝胶和给药器组成。壳聚糖凝胶以壳聚糖为主要成分,泊洛沙姆为辅料制成。给药器由保护帽、外套、推杆组成。 适用于:适用于念珠菌阴道炎的辅助治疗。
创伤止血技术
创伤止血技术 在各种突发创伤中,常有外伤大出血的紧张场面。出血是创伤的突出表现,因此,止血是创伤现场救护的基本任务。有效止血能减少出血,保存有效血容量,防止休克的发生。因此,现场及时有效地止血,是挽救生命、降低死亡率的,为病人赢得进一步治疗时间的重要技术。 血液是维持生命的重要物质。成人的血液约占人体的8%。失血的速度和数量是影响病人健康和生命的重要因素。突然失血占全身容量20%(约800毫升)以上时,可造成轻度休克、脉搏增快(可达100次/分钟);失血20%~40%(约800~1600毫升)时,可造成中度休克,脉搏每分钟100~120次甚至120次以上;失血40%(约1600毫升)以上时,可造成重度休克,脉搏细弱,摸不清。 一、出血的种类(按出血部位分类): 1、皮下出血:多因跌、撞、挤、挫伤,造成皮下软组织内出血,形成血肿、瘀斑,可短期自愈。 2、内出血:体表见不到出血,血液由破裂的血管,流入组织、脏器或体腔内(如胸腔内、腹腔内和颅腔内),只能根据伤病人的全身或局部症状来判断如面色苍白、吐血、腹部疼痛、便血、脉搏快而弱等,情况较严重,现场无法处理,需急送医院处理。 3、外出血:体表可见到,血液经皮损出流出体外。据血管损伤的种类将出血分为动脉出血、静脉出血和毛细血管出血。 动脉出血:血色鲜红,出血呈喷射状,与脉搏节律相同,速度快、量多。危险性大。 静脉出血:血色暗红,血流较缓慢,呈涌出状或持续流出,速度少缓慢,量中等。危险性较动脉性出血小。 毛细血管出血:血色鲜红,血液像水珠流从创面渗出,量少,常可自动凝固而止血。危险性小。 二、止血方法 (一)包扎止血: 普通包扎止血:是最常用的止血方法,适用于静脉及毛细血管或创口较小的小动脉出血。有条件时,先用生理盐水冲洗伤口,伤口周围用75%酒精消毒,再用消毒纱布覆盖创口,用绷带或三角巾包扎。无条件时也可用干净毛巾或其他软质布料覆盖包扎。 加压包扎止血:适用于全身各部位的小动脉、静脉、毛细血管出血。用敷料或其他洁净
壳聚糖止血材料的制备及性能评价
壳聚糖止血材料的制备及性能评价 韦其全潘峰刘坤材料学院2005级 指导教师:李保强 一、课题研究目的 在日常生活中突发性事故的急救治疗,在医院对病人的手术过程中的创伤止血,特别是战争中受伤战士的救护,病患者的局部快速且有效的止血非常重要。因为未受控制的出血是导致突发事故,术中大出血或战场伤亡的主要原因。在伊拉克战争中,战场上有50%阵亡人员是由于出血过多导致的。尽早的控制出血成为降低患者伤亡的最佳策略。创伤止血材料是应用于创伤出血救治,是平战时救护常用的物品,创伤止血材料的研究对于战创伤救治具有重要意义,临床常用的止血材料如止血纱布、止血绷带存在着局限性:如止血时间较长、易与伤口粘连而不易换药、对伤口的感染和化脓无能为力。快速止血和功能性止血将是未来止血药物发展的方向。目前,以壳聚糖为原料的止血材料正成为国内外研究的热点之一。我们希望通过对近年来国内外研制的新型快速止血材料的成分和止血机制的研究,制备一种高效的快速止血材料。 二、课题背景 美国HemCon公司推出的以冻干壳聚糖为基质的止血绷带(HemCon Bandage)能迅速止住大量出血,这种已消毒的绷带的柔韧性好, 可供军队战斗时使用, 甚至在极其恶劣的天气和地形亦可使用, 它可使伤 口形成结实的有粘附性的血块, 然后转运伤员。美国俄勒冈州的萨姆医疗产品公司以其从虾壳中提取出来的一种颗粒状混合物CLEOX命名的CLEOX止血粉,能迅速止住动脉出血,再出血率为零。 壳聚糖基止血材料在制备与性能检验方面存在以下问题:首先单一组分壳聚糖止血材料存在效果不显著;其次壳聚糖或壳聚糖/胶原、壳聚糖/明胶复合膜的柔韧性差,且存在成膜率低的问题;最后很少文献报道了止血材料的力学性能,而这恰恰直接关系到使用止血材料时的可操作性(如拉伸或延展性能)。李保强等研究表明,壳聚糖/羧甲基壳聚糖混合能成功制得止血薄膜,但存在机械性能不理想,止血评价不完善等问题。 基于壳聚糖止血材料的现状和问题,我们提出了通过溶液浇注制备甘油改性的CS/CMCS复合载药膜的方法,其中通过加入甘油以改善复合膜的柔韧性,加入酚磺乙胺为促进止血剂,研究止血剂对复合止血膜的力学性能的影响,最后采用兔子耳朵出血模型评价复合止血材料效果。 三、课题研究主要内容 1.原料 壳聚糖、羧甲基壳聚糖(青岛海汇生物工程有限公司)、乙酸(天津)、甘油、酚磺乙胺(新乡)、新西兰大白兔(购于哈尔滨兽研所) 2.复合膜制备过程 1)用电子天平称取4g壳聚糖(CS),将其溶于200ml的2%醋酸溶液,进行机械连续搅拌2h左右使 其充分溶解,然后静置数小时脱泡; 2)用电子天平称取4g羧甲基壳聚糖(CMCS),将其溶于200ml蒸馏水,进行机械连续搅拌2h左右 使其充分溶解,然后静置脱泡; 3)配置质量分数分别为10%,15%,20%,25%,30%的甘油50ml; 4)将上述三种溶液按16:4:5混合,并滴加4%的盐酸调节pH为3左右,搅拌至澄清。
壳聚糖无纺布敷料对切割伤伤口止血和促进愈合作用的研究
壳聚糖无纺布敷料对切割伤伤口止血和促进愈合作用的研究① 100850 北京 军事医学科学院放射医学研究所 谷庆阳 高亚兵 陈肖华 李永兰②刘春杰 杨 红 崔玉芳 王德文 摘 要 制备家兔切割伤模型,分别以壳聚糖敷料和纱布包扎创面,血止后以氰化高铁血红蛋白试剂及光度比色法检测敷料中血红蛋白的含量。借此估计出血量。重新包扎创面,并于分阶段取材后应用常规病理学手段结合图像分析法观察病变。结果表明:壳聚糖包扎组出血量明显少于纱布对照组。伤后9天,壳聚糖治疗组创面肉芽组织层较厚于油纱布对照组,其中胶原纤维含量亦较多,伤口愈合较快。提示:壳聚糖无纺布对切割伤有止血作用并有微弱的促进愈合使用。 关键词 壳聚糖;创伤和损伤;伤口愈合 中国图书资料分类号 R64 A STUDY ON THE HE MOSTAT I C AND HEAL ING EFFECTS OF CH IT OSAN ON INC ISED WOUND Gu Q ingyang,Gao Yab ing,Chen X iaohua et a l.In stitu te of R adiati on M edicine,A cadem y of M ilitary M edical Sciences,B eijing100850 Abstract Incised w ounds w ere m ade in rabb its,and som e of the w ounds w ere dressed w ith ch ito san,and o thers w ith gauze.A fter b leeding stopped,hemoglob in in dressings w as m easu red to determ ine the hemo staic ef2 fect.W ounds w ere redressed,and healing p rocess w as studied h isto logically.T he resu lts show ed that less H b w as detected in ch ito sandressing than in gauze.O n day9after w ounding,the con ten t of granu lati on tissue and co llagen fo rm ati on in the ch ito san dressed w ounds w as mo re than that in V aseline gauze dressed group.It sug2 gests that ch ito san dressing is effective in hemo stasis fo r incised w ounds and m ay be helpfu l in w ound healing p rocess. Key words ch itin;w ounds and in ju ries;w ound healing 壳聚糖是甲壳质的脱乙酰基产物,是一种多糖物质,其化学名为Β(124)222氨基222脱氧2D2葡聚糖。据文献报道,壳聚糖对神经损伤修复〔1~3〕及骨关节损伤修复〔4~6〕有一定促进作用,并可能有止血作用〔2〕。本研究旨在家兔切割伤模型的基础上,对壳聚糖无纺布敷料对切割伤创面的作用及其机制作一探讨,并与临床常用敷料作对照,为临床使用新型、经济、实用、效佳的敷料提供实验依据。 1 材料与方法 家兔5只,雌性,体重(212±011)kg,麻醉方法:按35m g kg体重于兔耳静脉缓慢注入2%戊巴比妥钠。将动物背部剪毛并以75%乙醇溶液消毒后,沿脊柱两侧对称性各剪4个圆形伤口,直径115c m,深度先至皮肤全层,然后仔细避开皮下组织层中较大的血管,剪(分离)至筋膜层。这样的伤口以渗血为主。两侧伤口对称性分别敷以壳聚糖无纺布和灭菌纱布,轻压1m in。45m in后伤口停止出血,揭下敷料,放入预先配制好的氰化高铁血红蛋白试剂5m l中仔细清洗。以紫外分光光计560nm波长光度比色,以其中H b的含量代表出血量。动物伤口经壳聚糖无纺布及油纱布分别重新包扎后,将动物置于单笼饲养。于伤后3、6、9、14和21天各活杀1只动物取材,并记录伤口大小,以QU AN T I M ET970型图像分析仪测算其伤口平均面积。标本经H E染色,备查。 2 结 果 211 壳聚糖敷料的创面止血效果 壳聚糖包扎组及纱布对照组H b光度吸收值如表1。纱布对照组A 值平均为119447±0162384,壳聚糖治疗组A值平均为019695±0171777(P<0.01)。A值高说明出血量多,止血效果差。以成组设计的t检验分析,两组之间比较差异有显著性意义(P<0.01),说明壳聚糖敷料对伤口渗血确有一定的止血作用。 谷庆阳,医学硕士,助理研究员。主要从事放射病理学研究,已在国内外杂志正式发表论著二十余篇。 ①“九?五”军队医药卫生科研基金重点课题(96Z008)②武警北京二总队十六支队医院
壳聚糖相关所有品资料
壳聚糖相关所有品资料
————————————————————————————————作者:————————————————————————————————日期:
壳聚糖相关的所有产品资料 1.壳聚糖栓 产品组成:壳聚糖、聚乙二醇单硬脂酸酯制成栓粒,加指套或推注器组成。主要性能:1. 装量允差为±10%。融变时限≤60min.3. PH应在4.5~6.5。4. 壳聚糖栓对金黄色葡萄球菌、大肠杆菌、白色念珠菌的抑菌率大于90%。5. 经Co60辐照灭菌,产品无菌。 适用于:细菌性阴道病和霉菌性阴道炎引起的阴部瘙痒灼痛、阴道分泌物增多、外阴充血肿胀的症状。 2.壳聚糖敷料 产品组成:本产品分为非粘型和自粘型。非粘型单独由敷芯制成,材料是非织造壳聚糖纤维无纺布;自粘型由背衬、敷芯、隔离纸(膜)组成,背衬由无纺布基材涂医用压敏胶制成,敷芯由非织造壳聚糖纤维无纺布或非织造壳聚糖纤维无纺布与非织造吸水纤维布复合组成,隔离纸(膜)由格拉辛纸(PET膜)制成。适用于:适用于体表创口保护、促进伤口愈合、预防伤口感染。 3.壳聚糖凝胶 产品组成:该产品由壳聚糖、卡波姆、羧甲基纤维素钠、甘油、纯化水等组成。Ⅰ型产品采用聚乙烯材料注塑成型的推助器包装;II型产品采用塑料软管包装。主要性能:a)壳聚糖含量不低于2.5%;b)ph值为5.0-7.8;c)微生物限度:细菌菌落总数不大于100cfu/g,大肠埃希菌,金黄色葡萄球菌、白色念珠菌不得检出。 适用于:该品适用于细菌性、霉菌性阴道炎和宫颈炎患者。 4.壳聚糖漱口液 产品组成:产品为壳聚糖、ε-聚赖氨酸、纳他霉素、阿斯巴甜、柠檬香精、纯化水组成的溶液。 适用于:用于抑制口腔内细菌总数,改善口臭、口腔溃疡疾病。 5.壳聚糖抗菌膜 产品组成:产品由膜和夹持器两部分组成;膜是由壳聚糖、壳碘〔CMCTS-g-(PAANa-CO-PVP)-I2和明胶制成;夹持器采用的医用高分子材料(医用聚丙烯)制成,夹持器的弹簧应操作灵活;膜的凝冻浓度倒置10秒钟应不流下;对大肠杆菌和金黄色葡萄球菌的抑菌率应≥50%;膜的细菌内毒素应不大于0.5EU/ml;膜应不大于极轻微刺激和不大于轻微细胞毒性;产品应无迟发型超敏反应和急性全身毒性反应;产品经钴-60γ灭菌,应无菌。 适用于:产品用于轻度宫颈糜烂的治疗,慢性宫颈炎手术创面的保护、促进愈合。 6.壳聚糖护脐带 产品组成:由脐贴(壳聚糖无纺布、碳纤维、吸水棉)、弹性基带和魔术贴组成。 适用于:供新生儿脐带结扎后为残端保护时一次性使用。 7.壳聚糖妇科凝胶 产品组成:壳聚糖妇科凝胶由壳聚糖凝胶和给药器组成。壳聚糖凝胶以壳聚糖为主要成分,泊洛沙姆为辅料制成。给药器由保护帽、外套、推杆组成。 适用于:适用于念珠菌阴道炎的辅助治疗。
创伤急救-止血技术操作规程
创伤急救—止血技术操作规范 【评估】 1、评估环境是否安全,危重伤员应观察复苏是否有效等情况。 2、正确评估需要止血伤口的局部情况,确定止血方法,正确选择用物。 3、了解伤员心理状况。 【准备】 护士:具有争分夺秒的急救意识,具备组织急救和指导伤员自救、互救能力。环境:安全。 物品:1、制式材料:三角巾、无菌敷料、止血带(橡皮止血带、卡式止血带、充气式止血带等)、绷带、标示卡,绞棒等。 2、就便材料:围巾,布条,领带,筷子、树枝等。 体位:根据伤员受伤部位不同给予相应体位。 【方法】 一、指压法止血技术操作 适用于中等或较大动脉的出血,以及较大范围的静脉和毛细血管出血,创伤急救中常用于临时止血。 头面部指压止血技术操作流程: 评估伤员伤情是否适宜操作→伤员取坐位(病情允许)→正确判断头面部出血部位→选择指压血管,做指压点定位和压迫→ 头顶部出血→颞浅动脉→压迫同侧耳屏前方颧弓根部搏动点→将动脉压向颧骨 颜面部出血→面动脉→压迫同侧下颌骨前缘约3cm凹陷处搏动点→将动脉压向下颌骨。 头颈部出血→颈总动脉→拇指或其他四指压迫同侧气管外侧与胸锁乳突肌前缘中点之间强搏动点→用力压向第五颈椎横突处。 头后部出血→枕动脉→压迫同侧耳后乳突下稍后方搏动点→将动脉压向乳突→快速临时阻断血流→观察并记录止血效果。 二、加压包扎止血法技术操作 适用于小动脉,中,、小静脉或毛细血管出血。 1、直接压迫止血法技术操作流程: 评估伤员伤情是否适宜操作→取卧位或坐位→抬高伤肢→检查伤口出血情况及有无异物或骨折→无异物或骨折→取大于伤口3cm的敷料覆盖→手指并拢,压迫出血部位5—15分钟→出血停止后在原位加盖另一块敷料(切记不要除去第一块纱布,否则可能会引起再次出血)→绷带或三角巾包扎→力度适中→观察肢端末梢循环情况并记录。 2、间接压迫止血法技术操作流程: 评估伤员伤情是否适宜操作→取卧位或坐位→抬高伤肢→检查伤口出血情况及有无异物或骨折→有异物→妥善固定异物→用绷带卷或棉垫置于异物两侧保护异物→绷带加压包扎(包扎时注意固定伤口内异物)→观察肢端末梢循环情
创伤急救基本技术
第一节创伤急救基本技术 止血 常用的止血方法有以下几种: 1.加压包扎法:用敷料盖住伤口,再用绷带加压包扎。这种方法急救中最常用。 2.填塞止血法:用消毒的纱布,棉垫等敷料填塞在伤口内,再用绷带,三角巾成四头带加压包 ,松紧度以达到止血为宜,常用于颈部、臂部等较深伤口。 3.指压止血法:用手指压迫出血的血管上端,即近心端,使血管闭合阻断血流达到止血目的。 适用于头面颈部及四肢的动脉出血急救。 4.屈曲加垫止血法:当前臂或小腿出血时,可在肘窝、窝内放置绵纱垫、毛巾或衣服等物品, 屈曲关节,用三角巾或布带作“8”字固定。注意有骨折或关节脱位时不能使用,因此法伤员痛苦较大 ,不宜首选。 止血带止血: 适用于四肢大血管破裂出血多或经其它急救止血无效者。常用气囊止血带或三尺左右长的橡皮管 ;急救时可用布带、绳索、三角巾或毛巾替代,称绞紧止血法。使用时应注意以下几点: 1.止血带必须上在伤口的近心端,肘关节以下的伤口,应将止血带扎在上臂,膝关节以下伤口 应将止血带扎在大腿。 2.在上止血带前先包一层布或单衣。 3.上止血带之前应抬高患肢2~3分钟,以增加静脉回心血流量。
4.应标记、注明上止血带的时间,并每隔45~60分钟放松止血带一次,每次放松时间为3~5 分钟;松开止血带之前用手压迫动脉于近端。 5.扎止血带松紧要适宜,以出血停止、远端摸不到动脉搏动为好。 6.不可用电线、铁丝等作止血带用。 具体操作方法:橡皮带止血法:先在止血带部位垫一层布或单衣,再左手拇食中指持止血带头端 ,另一手拉紧止血绕肢体缠2~3圈,并将橡皮带未端压在紧缠的橡皮管下固定。 绞紧止血法:先垫衬垫,再将带系在垫上绕肢体一圈打结,在结下穿一棒,旋转此棒使带绞紧, 至不流血为止,最后将棒固定在肢体上。 包扎 包扎在急救中应用广泛,其主要目的是压迫止血,保护伤口,固定敷料减少污染,固定骨折与关 节,减少疼痛。常用的材料有三角巾、多头带、绷带,亦可用毛巾、手绢、布单、衣物等替代。 1.一般伤口包扎时要注意以下几点: (1)迅速暴露伤口并检查,采用急救措施。 (2)有条件者应对伤口妥善处理,如清除伤口周围油污,碘酒、酒精消毒皮肤等。 (3)包扎材料,尤其是直接覆盖伤口的纱布应严格无菌,没有时亦应尽量用相对干净的材料覆盖 ,如清洁毛巾、衣服、布类等。 (4)包扎不能过紧过松。
创伤与急救技能经典.doc
一、死因分析 创伤是能量转移到人体的结果,随着社会的发展呈逐年上升趋势。现代创伤的特点是致伤能量高、死亡和致残率高,社会危害极大。所以掌握创伤与急救的基本技能,有效降低死亡率和致残率是摆在急诊工作者面前的前沿课题。就其死亡原因分析如下: 1.40岁以上年龄组危害人们健康的杀手依次为心、脑血管 病和恶性肿瘤:生活提高,高脂饮食、过度饮酒、吸烟等不良嗜好和环境恶化是主要原因。 2.在40岁以下年龄组第一杀手是创伤并仍在增加:交通事故、工伤、矿难、空难、地震、海啸、战争等。该群体是社会和家庭的中流砥柱,其危害和影响远大于上述疾病。 3.创伤导致死亡常见原因:[1]早期数分钟内死亡:脑干损伤、窒息、心脏和大血管贯通伤及高位脊髓损伤。[2]数小时内 死亡:多因休克和不能控制的大出血。[3]晚期死亡:常因合并SIRS(全身炎症反应综合症)、 SEPSIS(脓毒症)、ARDS(急 性呼吸窘迫综合症)、 SEPTIC SHOCK(脓毒性休克)和MODS (多器官功能不全综合症)等。 二、创伤常见原因及特点 1.交通伤:高能创伤,常见多发伤和复合伤。
2.坠落伤:常见传导伤和对冲伤,以脊柱和脊髓损伤、骨盆骨折为主。 3.机械伤:常导致肢体开放性损伤或断肢、断指,组织挫伤,血管、神经、肌腱损伤和骨折。 4.锐器伤:伤口深,胸腹部可致内脏或大血管损伤,一般伤情较重。 5.跌伤:老年人常见,前臂、大腿骨折,脊柱压缩性骨折。 6.火器伤:既有穿透效应又有震荡效应,其损伤程度比弹道面积大数十倍。 三、创伤现场救护 1.主要类型: ⑴闭合性损伤:无开放性伤口。 ⑵开放性损伤:有开放性伤口。 ⑶多发伤:同一致伤因素,多处受伤,至少有一处致命伤。 ⑷复合伤:多个致伤因素所致,至少有一处致命伤,如创伤+烧伤等。 2.现场救护目的 维持生命:先救命,即首先支持生命体征。 减少出血:利用现场条件,控制大出血,防止休克发生。 保护伤口:防止暴露伤口的污染。 固定骨折:防止转运途中继发损伤。 防止并发症及伤势恶化:操作要轻柔,规范,目的明确。