WMRT-GB-TRFS-GB-QUALITY TESTING-V51

Instructions:说明
1)All sections of this Test Request Form must be completed in full and submitted with each sample. Forms that are not legible, not signed, or if
any pertinent information is missing, test completion will be delayed or testing will be rejected.本申请表中的全部项目必须填写完整,随每种样品一起提交。如果表格不清晰、没有签名或缺少相关的信息,则会延误试验的完成,或者是拒绝试验。
2)Submit the correct numbers of samples. If you are unsure of the number of samples, it is submitter’s responsibility to conta ct the lab with
questions.提交正确的样品编号,如不不确认,提交者有责任就存在的问题和实验室沟通。
3)Include documentation for claim substantiation. 要提交产品属实的证明性文件。
4)In lieu of testing, provide approved documentation (refer to test protocols and/or the Walmart Document Review and Validity outline).
需要给实验室提交许可文件(参考测试协议和/或Walmart审查有效性概述)
5)Date and sign page 2 of this form. Include Page 3 of this TRF when submitting to the lab.
在本表格的第2页上面签上名字及日期,提交时连同本表格的第3也一起提交给实验室。
6)If you have any questions, contact the local lab or submit inquiry to walmarttesting@https://www.360docs.net/doc/174877908.html,
如有问题,请联系当地实验室或发邮件至walmarttesting@https://www.360docs.net/doc/174877908.html,
Quotation Required Before Testing -Testing pending receipt, by BV, of signed quotation with complete information and samples
试验前报价要求—测试要等签字的报价单连同完整的样品信息确认后方可进行。
Please refer to the most recent Bureau Veritas L ocation Sheet for a list of lab locations #-M andatory 强制性
Please Check One:
Wal-Mart Wal-Mart Canada https://www.360docs.net/doc/174877908.html, USA, LLC Sam’s Club Sam’s .com Mas
Phase Pre-Production Production In-Store Re-Buy/Replenishment
# Program Domestic Direct Import-WGS Direct Import-DSG Gift with Purchase
Private Label Brand: Yes If Yes, Please list brand name No
Please Type or Print 请打印
Supplier Name 供应商名称
Supplier Address:供应商地址
Supplier Contact Name:供应商联系人
Telephone:电话Fax: Email:
Invoicing Information if Different from Above:如果和上述信息不一致,则提供下列发票信息。
Company Name:公司名称
Company Address:公司地址
Contact Name:联系人
Telephone:电话Fax: Email:
If order was received from Direct Sourcing Group (DS G): The following section MUST be completed如果从直接采购商那收到订单:必须填写下列内容。
Agent Name:
Agent QA Name:
Agent Merchandiser Name 名称: Agent Merchandiser Telephone电话:
Email电邮:
Service Required 服务类型
Regular Service (Product Testing– 6 days/ (Transit Testing– 10days)一般服务(产品测试—6天/(运输—10天)
*Rush Service Please contact the local laboratory for Test Turn Around Time level) 加急服务,请联系当地实验室
*Priority Service (Next Business Day) 优先服务(第二个工作日)
*Same Business Day Sample receipt required by 10:30 a.m. 当日服务:要求上午10:30之前收到样品
*Express Service (Fastest Turn Around Time for some selected tests require longer testing time ) 快递服务
* Please confirm availability of non-regular service with your local BV lab and the associated surcharges. 对于非一般的服务类型所需的附加费用,请联系当地的BV实验室。
CPSIA General Conformity Certificate / Children’s Product Certificate (GCC / CPC)
DOMESTIC ONLY
Do you want a GCC /
Yes No If yes the following Importer/Domestic manufacturer information MU ST be completed CPC?
Name of Importer/Domestic Manufacturer:
Mailing Address/ Tel No.:
Date of Manufacture (MM/DD/YY):
Place of Manufacture : City : Province: Country:
Please provide name, full mailing address, e-mail address and telephone number of the person maintaining test records in support of the certification:
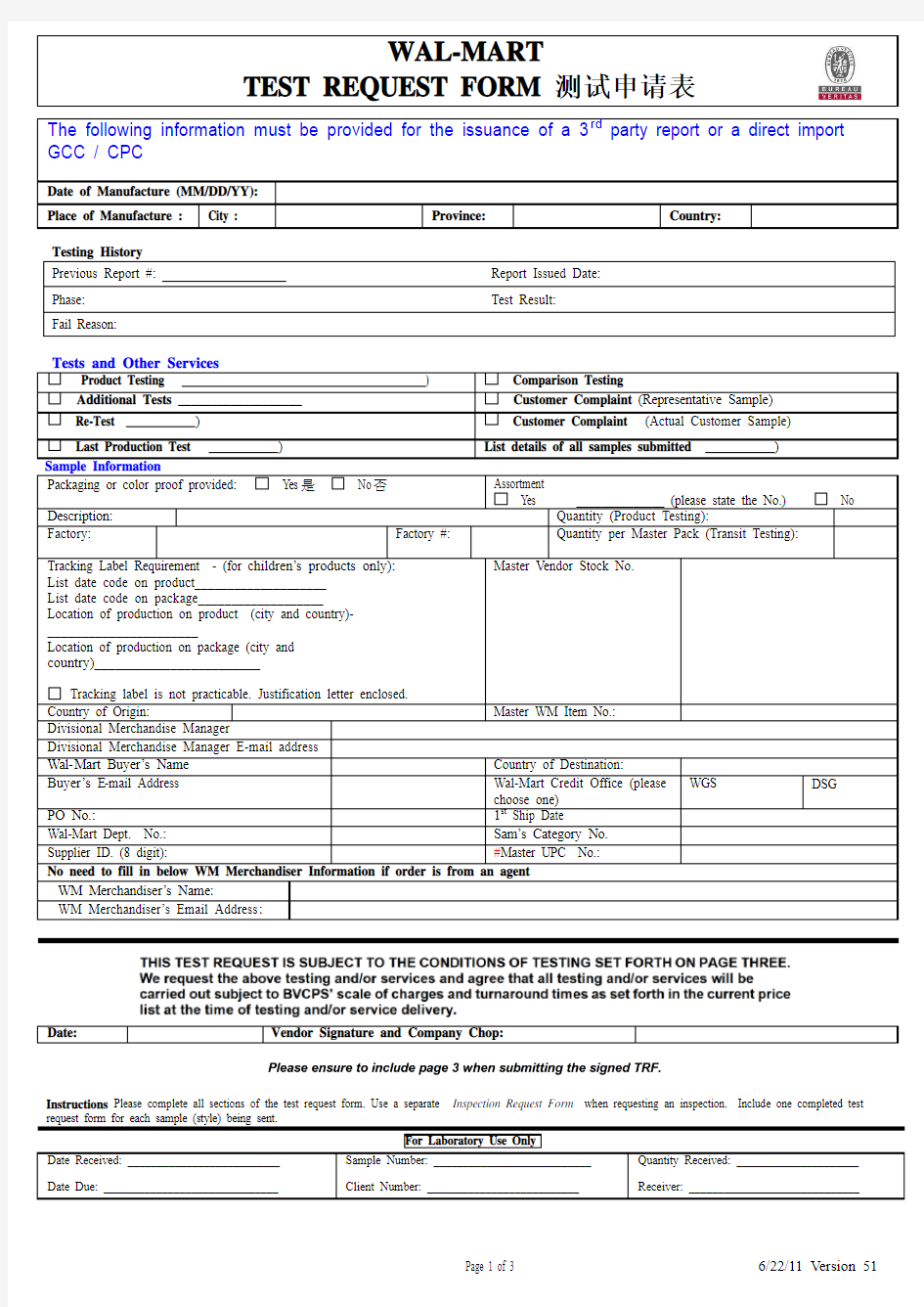
The following information must be provided for the issuance of a 3rd party report or a direct import GCC / CPC
Date of Manufacture (MM/DD/YY): Place of Manufacture : City :
Province:
Country:
Testing History Previous Report #: Report Issued Date: Phase: Test Result:
Fail Reason:
Tests and Other Services
Product Testing ) Comparison Testing
Additional Tests ___________________ Customer Complaint (Representative Sample) Re-Test )
Customer Complaint (Actual Customer Sample) Last Production Test ) List details of all samples submitted )
Sample Information
Packaging or color proof provided: Yes 是 No 否
Assortment
Yes ______________ (please state the No.)
No
Description:
Quantity (Product Testing):
Factory:
Factory #:
Quantity per Master Pack (Transit Testing):
Tracking Label Requirement - (for c hildren’s products only): List date code on product____________________ List date code on package___________________ Location of production on product (city and country)-______________________
Location of production on package (city and country)________________________
Tracking label is not practicable. Justification letter enclosed. Master Vendor Stock No.
Country of Origin: Master WM Item No.:
Divisional Merchandise Manager Divisional Merchandise Manager E-mail address Wal-Mart Buyer’s Name Country of Destination:
Buyer’s E -mail Address
Wal-Mart Credit Office (please choose one)
WGS DSG
PO No.: 1st Ship Date Wal-Mart Dept. No.: Sam’s Category No. Supplier ID. (8 digit): #Master UPC No.:
No need to fill in below WM Merchandiser Information if order is from an agent
WM Merchandiser’s Name :
WM Merchandiser’s Email Address :
Date:
Vendor Signature and Company Chop:
Instructions Please complete all sections of the test request form. Use a separate Inspection Request Form when requesting an inspection. Include one completed test request form for each sample (style) being sent.
For Laboratory Use Only
Date Received: __________________________
Date Due: ______________________________ Sample Number: ___________________________
Client Number: __________________________ Quantity Received: _____________________
Receiver: _____________________________