Combination tramadol plus acetaminophen for postsurgical pain

Scienti?c paper
Combination tramadol plus acetaminophen for postsurgical pain
Adam B.Smith,D.O.a,*,Thanjavur S.Ravikumar,M.D.b,Marc Kamin,M.D.c,
Donna Jordan,B.S.N.c,Jim Xiang,Ph.D.c,
Norman Rosenthal,M.D.c,on behalf of the CAPSS-115Study Group?
a Department of Surgery,University of North Texas Health Science Center,855Montgomery St.,Fort Worth,TX76107,USA
b Department of Surgery,Monte?ore Medical Center,Bronx,NY,USA
c Ortho-McNeil Pharmaceutical,Raritan,NJ,USA
Manuscript received April17,2003;revised manuscript October17,2003
Abstract
Background:This multicenter,randomized,double-blind,active-and placebo-controlled trial evaluated tramadol plus acetaminophen (APAP)for orthopedic(n?153)and abdominal(n?152)postsurgical pain.
Methods:Patients with moderate pain or greater were randomized to an initial two tablets of37.5mg tramadol plus325mg APAP(n?98),codeine30mg plus APAP300mg(n?109),or placebo(n?98);thereafter,they received1to2tablets every4to6hours as needed for pain for6days.Outcome measures were pain relief and pain intensity,total pain relief,sum of pain intensity differences,and sum of pain relief and pain intensity differences during4hours and the daily averages.
Results:Tramadol plus APAP was superior to placebo for total pain relief,sum of pain intensity differences,and sum of pain relief and pain intensity differences(P?0.015);tramadol plus APAP and codeine plus APAP did not separate(P?0.281).For average daily pain relief,average daily pain intensity,and overall medication assessment,tramadol plus APAP was superior to placebo(P?0.038);codeine plus APAP did not separate from placebo(P?0.125).Discontinuation because of adverse events occurred in8.2%of tramadol plus APAP, 10.1%of codeine plus APAP,and3.0%of placebo patients.Except for constipation(4.1%tramadol plus APAP vs10.1%codeine plus APAP)and vomiting(9.2%vs14.7%,respectively),adverse events were similar for active treatments.
Conclusions:Tramadol plus APAP(mean dose4.4tablets)was effective and well tolerated for postsurgical pain and showed better tolerability than did codeine plus APAP.?2004Excerpta Medica,Inc.All rights reserved.
Keywords:Abdominal surgery;Acetaminophen;Codeine;Combination therapy;Orthopedic surgery;Postsurgical pain;Tramadol
The quality of postoperative patient care depends critically on effective pain management,which includes accurately assessing pain and monitoring the patient’s response to treatment[1].Inadequate postoperative pain treatment can contribute to unnecessary discomfort,increased morbidity, delayed discharge,and unanticipated readmission to hospi-tal[2–4].In cases of outpatient hernia surgery,supplemen-tary medication may be needed during outpatient care after postoperative treatment with nonsteroidal anti-in?ammatory drugs(NSAIDs)or opioids[2].Furthermore,orthopedic postoperative patients,who have a high incidence of severe pain in postanesthesia care[4,5],are responsive to acet-aminophen(APAP)combined with opioids as an alternative to NSAIDs for management of their outpatient postopera-tive pain[6].Clearly,additional effective analgesic options are needed,and they need to be optimally utilized.
The combination tablet,tramadol37.5mg plus APAP 325mg,has been found to be an effective,versatile treat-ment for acute nociceptive pain associated with orthopedic surgery[7],osteoarthritis?are[8],and oral surgery[9,10]. Tramadol,an unscheduled medication,exhibits both mild ?-opioid receptor binding and norepinephrine and serotonin reuptake inhibition.This dual mechanism may explain the lower rates of abuse and decreased incidence of respiratory depression compared with scheduled opioids[11,12].APAP may have multiple mechanisms of action,which are be-lieved to include inhibition of prostaglandin-E2release in the spinal cord[13]and inhibition of nitric oxide synthesis
This research was supported by Ortho-McNeil Pharmaceutical,Raritan,
NJ.
*Corresponding author.Tel.:?1-817-735-5450;fax:?817-735-5454.
E-mail address:adsmith@https://www.360docs.net/doc/908047358.html,
?Members of the CAPSS-115Study Group are listed in the Appendix.
The American Journal of Surgery187(2004)521–527
0002-9610/04/$–see front matter?2004Excerpta Medica,Inc.All rights reserved.
doi:10.1016/j.amjsurg.2003.12.038
mediated by N -methyl-D-aspartate or substance P [14].The solitary uses of tramadol,APAP,or propacetamol,which is rapidly hydrolyzed to APAP,in pain management after ortho-pedic surgery have been previously reported [6,15–17].
The purpose of this study was to evaluate the ef ?cacy and safety of the combination analgesic tramadol plus APAP in the treatment of postsurgical pain in patients undergoing an orthopedic or an abdominal procedure.
Methods Study design
Treatment of postsurgical pain with tramadol 37.5mg plus APAP 325mg (Ultracet;Ortho-McNeil,Raritan,NJ)was compared with codeine 30mg plus APAP 300mg and with placebo in a multicenter,randomized,double-blind,active-and placebo-controlled,parallel-group study.The study population consisted of approximately 300patients in generally good health who had undergone a therapeutic arthroscopic procedure of the knee or shoulder or who had undergone abdominal surgery for inguinal or ventral hernia repair.Patients were selected if they met inclusion criteria,which included having at least moderate postsurgical pain,being appropriate for pain management with an oral anal-gesic,and giving informed consent.Pain assessment was based on scores ?40mm on a pain visual analog scale (from 0to 100where 0?no pain and 100?extreme pain)and at least 2on a pain intensity scale (from 0to 3where 0?none,1?mild,2?moderate,and 3?severe).Female participants were required either to be using an appropriate
contraceptive method and to have a negative pregnancy test within 5days of study initiation or to be postmenopausal and/or incapable of becoming pregnant due to hysterectomy or other surgical procedure.
Included among the key exclusion criteria were use of analgesics within 3hours of study medication or concomi-tant use of sedatives (other than during surgery);oral anti-emetics or steroid injections on the day of surgery;admin-istration of long-acting nerve blocks or epidural anesthesia;use of tramadol within 30days of study entry;inability to tolerate tramadol hydrochloride or previously failed treat-ment with tramadol hydrochloride;contraindication to opi-oids or APAP;morbid obesity;history of abnormal hepatic and/or renal function,chronic alcohol abuse or substance abuse,or unstable medical disease;indication of major psychiatric disorder or treatment with antipsychotic medi-cation;or use of an investigational drug or device within 30days of study entry.
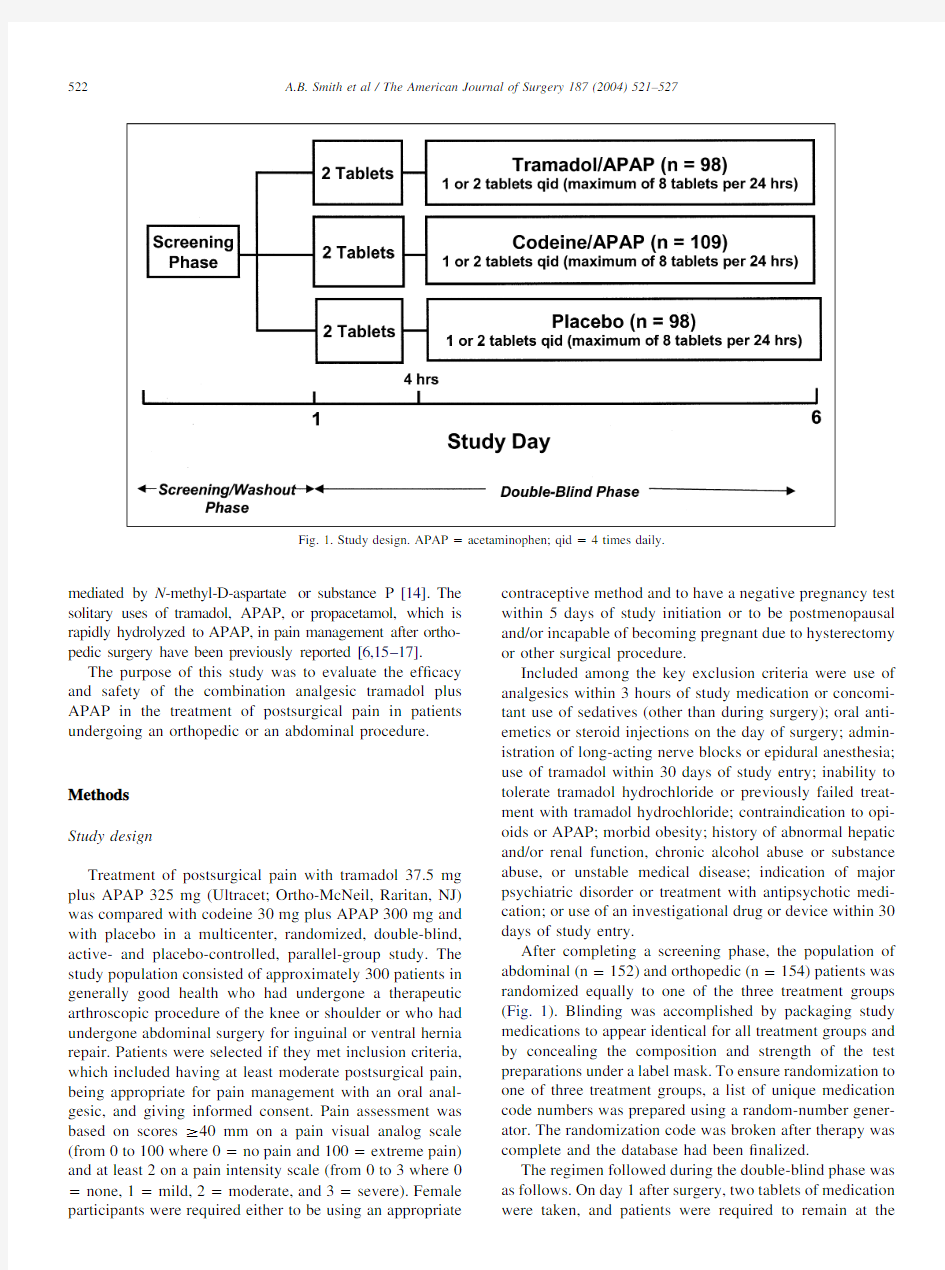
After completing a screening phase,the population of abdominal (n ?152)and orthopedic (n ?154)patients was randomized equally to one of the three treatment groups (Fig.1).Blinding was accomplished by packaging study medications to appear identical for all treatment groups and by concealing the composition and strength of the test preparations under a label mask.To ensure randomization to one of three treatment groups,a list of unique medication code numbers was prepared using a random-number gener-ator.The randomization code was broken after therapy was complete and the database had been ?nalized.
The regimen followed during the double-blind phase was as follows.On day 1after surgery,two tablets of medication were taken,and patients were required to remain at
the
Fig.1.Study design.APAP ?acetaminophen;qid ?4times daily.
522 A.B.Smith et al /The American Journal of Surgery 187(2004)521–527
study facility throughout the4-hour evaluation period.Sub-
sequent doses of1to2tablets were taken at least4hours
after the?rst dose and were allowed every4to6hours as
needed for pain through day6.During outpatient treatment,
pain intensity and pain relief were rated on days1to6in the
outpatient diary.The medication was not to exceed300mg
tramadol plus2600mg APAP or240mg codeine plus2400
mg APAP per24-hour period.Patients who received sup-
plemental pain medication or who required the use of anti-
emetics were discontinued from the study.
Patients were predominantly recruited from within inves-
tigators’medical practices.The protocol was reviewed at
each site and approved by an Institutional Review Board.
Patients gave signed written consent at screening before any
of the study-related procedures were performed.Twenty-
seven investigators participated in the study.The trial was
conducted in compliance with the Declaration of Helsinki as
last amended in1989and with the International Committee
on Harmonisation Topic6Guideline for Good Clinical
Practices.Known instances of nonconformance were docu-
mented and were not considered to have had any impact on
the overall conclusions of the study.
Outcome measures
The primary ef?cacy variables were total pain relief
(TOTPAR),sum of pain intensity differences(SPID),and
sum of pain relief and pain intensity differences(SPRID)
during the?rst4hours after the?rst dose of study medica-
tion on day1.These ef?cacy variables were calculated from
pain relief and pain intensity difference measurements made
at30minutes and again at1,2,3,and4hours after the drug
was given.Pain intensity was ranked on a4-point Likert
scale(0?none,1?mild,2?moderate,3?severe),and
pain relief was measured using a6-point Likert scale(4?
complete relief,3?a lot,2?moderate,1?slight,0?no,
and?1?worse pain).
Secondary ef?cacy variables included average daily pain
intensity scores and average daily pain relief scores reported
on days1to6.At the end of each day,patients recorded the
average postsurgical pain intensity(using the4-point Likert
scale previously mentioned)as well as the amount of pain
relief(based on the6-point Likert scale)they experienced
since the last assessment compared with the pain they ex-
perienced before initiation of the study medication.In ad-
dition,at study completion both patients and investigators
rated the study medication overall using a?ve-point scale(2?very good,1?good,0?no change,?1?poor,and?2?very poor).Safety evaluations performed during study visits included physical examinations and recording of vital
signs and adverse events.
Statistical analysis
Statistical analyses were performed on the intention-to-
treat population,which was composed of all randomized patients who took at least one dose of study medication and who recorded at least one postrandomization ef?cacy mea-surement.The primary ef?cacy variables(TOTPAR,SPID, and SPRID)were analyzed by an analysis of covariance model using baseline pain intensity score as a quantitative covariate and treatment,surgery type,and treatment by surgery type interaction as qualitative factors.Treatment by surgery type interaction was to be tested and dropped from the model if not signi?cant.Analysis incorporated the pain measurements made during the?rst4hours after the?rst dose of study medication.The primary comparison was between tramadol plus APAP and placebo;additional com-parisons were also performed between codeine plus APAP and placebo as well as between tramadol plus APAP and codeine plus APAP.Similarly,an analysis was performed of secondary outcomes:average daily pain intensity,aver-age daily pain relief for days1to6,?nal visit pain intensity,?nal visit pain relief,ef?cacy failures,and overall medica-tion assessment.Analysis used the analysis of covariance model with baseline pain intensity score as a quantitative covariate and surgery type and treatment as qualitative fac-tors.For analyses of pain relief scores and overall medica-tion assessments,the baseline pain intensity score was the covariate.
For the inpatient portion(?rst4hours)and outpatient portion(days1to6)of the study,Kaplan-Meier estimates of the cumulative distribution of time to discontinuation be-cause of lack of ef?cacy were determined.The event for the time-to-event analysis was discontinuation because of lack of ef?cacy.Kaplan-Meier estimates were assessed for sta-tistical signi?cance of differences in distributions by a log-rank test.The statistical signi?cance of any difference be-tween tramadol plus APAP and placebo in the proportion of patients who discontinued medication because of lack of ef?cacy was assessed using the logistic regression analysis with treatment and surgery type as qualitative factors.
Statistical tests of main effects were performed at the 2-sided,??0.05signi?cance level.The sample size(50 patients/treatment group/surgery type)was selected using general guidelines for the design of single-dose,oral post-surgery studies and was not powered for intersurgical type analysis.The evaluable-for-safety population consisted of those randomized patients who received at least one dose of study medication and who had at least one postbaseline safety evaluation.
Results
Demographics
After randomization(n?306)was accomplished,the intention-to-treat population(n?305)consisted of152 patients undergoing abdominal surgery(49.8%)and153 patients undergoing orthopedic(50.2%)procedures and in-cluded215(70.5%)men and90(29.5%)women.The pa-
523
A.B.Smith et al/The American Journal of Surgery187(2004)521–527
tients had a mean age of47.3years(range18to79years), a mean baseline pain visual analog scale score of62.9mm, and a baseline pain intensity score of2.2(Table1).The treatment groups were comparable with respect to these variables and other characteristics at baseline.Treatment by surgery type interaction was not signi?cant;therefore,re-sults from the abdominal and orthopedic surgery types were pooled.
Treatment response:drug,active control,and placebo groups
Tramadol plus APAP was signi?cantly better than pla-cebo on all of the primary outcome measures—TOTPAR, SPID,and SPRID—during the?rst4hours(Table2).No statistically signi?cant differences were found for primary ef?cacy measures between tramadol plus APAP and co-deine plus APAP(Table2).
Tramadol plus APAP was also signi?cantly better than placebo in measurement of all secondary ef?cacy variables: average daily pain relief(P?0.013;Fig.2),average daily pain intensity(P?0.038),?nal visit pain intensity(P?0.046),and?nal visit pain relief(P?0.025).Tramadol plus APAP was also numerically better than codeine plus APAP in decreasing average daily pain intensity,but this did not reach statistical signi?cance(P?0.072).Codeine plus APAP did not separate from placebo for these secondary variables(P?0.125).
During the?rst4hours,the tramadol plus APAP group had a lower incidence of discontinuation because of ef?cacy failures(23.5%)compared with the placebo group(39.8%, P?0.021)and the codeine plus APAP group(25.7%,P?not signi?cant).The Kaplan-Meier cumulative distribution of time to discontinuation because of lack of ef?cacy for this group was lower than that for placebo during the?rst4 hours(P?0.019;Fig.3)and during the course of the study (P?0.003;Fig.4).
Tramadol plus APAP was evaluated as signi?cantly bet-ter than placebo(P?0.001)in patients’overall medication assessments(Fig.5)with more patients noting a very good or good analgesic response(P?0.005).Physicians,too, gave signi?cantly higher overall assessments for tramadol plus APAP(P?0.005)and for codeine plus APAP(P?0.035)than for placebo.
Table1
Demographic characteristics for postsurgical pain patients
Characteristic Tramadol/APAP
(n?98)Placebo
(n?98)
Codeine/APAP
(n?109)
Mean age in years(?SD)46.2(?15.0)(range18–77)48.9(?15.2)(range18–79)46.9(?15.5)(range20–77) Sex,n(%)
Male70(71.4)68(69.4)77(70.6)
Female28(28.6)30(30.6)32(29.4)
Race,n(%)
White89(90.8)90(91.8)100(91.7)
Black7(7.1)8(8.2)8(7.3)
Asian1(1.0)0(0.0)0(0.0)
Other1(1.0)0(0.0)1(0.9)
Surgical procedure,n(%)
Abdominal49(50.0)49(50.0)54(49.5)
Orthopedic49(50.0)49(50.0)55(50.5)
Baseline PVA*in mm(mean?SD)61.6(?12.4)63.5(?15.4)63.5(?14.2)
Baseline pain intensity score?(mean?SD) 2.2(?0.4) 2.3(?0.4) 2.2(?0.4)
*PVA?Pain visual analog scale from0to100where0mm?no pain and100mm?extreme pain.
?Scale0to3where0?none,1?mild,2?moderate,3?severe.
APAP?acetaminophen.
Table2
Summary and analysis of primary ef?cacy measures*
Primary ef?cacy measures Tr/APAP
(n?98)
Placebo
(n?98)
Cod/APAP
(n?109)
P values
Tr/APAP vs
placebo
Tr/APAP vs
Cod/APAP
Cod/APAP
vs placebo
TOTPAR,mean(?SD) 6.5(?4.5) 4.5(?4.4) 5.8(?4.2)0.0040.2810.052 SPID,mean(?SD) 2.7(?2.3) 2.0(?2.3) 2.7(?2.4)0.0150.8640.019 SPRID,mean(?SD)9.2(?6.5) 6.6(?6.5)8.5(?6.3)0.0050.4320.033
*Assessments conducted for the?rst4hours after the?rst dose of medication.P value is for the speci?ed treatment contrast using an analysis of covariance model with baseline pain intensity score as covariate.
Cod/APAP?codeine plus acetaminophen;Tr/APAP?tramadol plus acetaminophen.
524 A.B.Smith et al/The American Journal of Surgery187(2004)521–527
The mean daily dose of tramadol plus APAP was 163mg tramadol and 1,415mg APAP (4.4tablets at a cost of $3.61/day),and the mean daily dose of codeine plus APAP was 130mg codeine and 1,296mg APAP (4.3tablets at a cost of $1.76/day).Adverse events
Treatment-emergent adverse events reported by the 2groups receiving active medication were similar.The great-est differences in adverse event incidences in the active treatment groups were noted for constipation (4.1%tram-adol plus APAP vs 10.1%codeine plus APAP)and vomit-ing (9.2%tramadol plus APAP vs 14.7%codeine plus APAP;Table 3).One serious adverse event (constipation)was considered by an investigator to be related to a study medication (codeine plus APAP).Discontinuation because of adverse events occurred in 8.2%of tramadol plus APAP patients,in 10.1%of codeine plus APAP patients,and in 3.0%of placebo patients.
Comments
The results of this study show that postsurgical pain associated with arthroscopic procedures of the knee or shoulder or with abdominal hernia surgery was successfully decreased by treatment with 37.5mg tramadol plus 325mg APAP tablets.The combination of tramadol plus APAP was superior to placebo as an analgesic as measured by all primary (TOTPAR,SPID,and SPRID)and secondary ef ?-cacy outcomes (average daily pain relief,average daily pain intensity,?nal visit pain intensity,?nal visit pain relief,and overall medication assessment scores).Clinical effective-ness was also shown by the estimated rates of discontinua-tion because of lack of ef ?cacy during the 4hours after surgery as well as during the 6-day course of outpatient treatment.This ?nding is consistent with results from a recent meta-analysis of postsurgical patients treated with tramadol plus APAP [18].Moreover,in their overall med-ication assessments,patients evaluated tramadol plus APAP as superior to placebo,and a greater number of patients also gave higher combined ratings of “very good ”or “good ”for the combination tablet compared with codeine plus APAP.These assessments were consistent from orthopedic patients undergoing shoulder or hip procedures and from
abdominal
Fig.2.Average daily pain relief for 3treatment groups during 6days.Pain relief scale:complete ?4,a lot ?3,moderate ?2,slight ?1,none ?0,worse ??1.P value based on analysis of covariance model with surgery type and treatment as qualitative factors and baseline values as covariate.APAP ?
acetaminophen.
Fig.3.Kaplan-Meier cumulative distribution of time to discontinuation because of lack of ef ?cacy during the ?rst 4hours of treatment.APAP ?
acetaminophen.
Fig.4.Kaplan-Meier cumulative distribution of time to discontinuation because of lack of ef ?cacy during a 6-day course of treatment.APAP ?
acetaminophen.
Fig. 5.Patients ’overall medication assessment.APAP ?acetamino-phen.
525
A.B.Smith et al /The American Journal of Surgery 187(2004)521–527
surgery patients with inguinal or ventral hernia repair.The favorable outcome of tramadol plus APAP combination tablets in this surgical pain model further extends their utility as a versatile therapy in managing acute pain.
By combining drugs with different mechanisms of action and pharmacokinetic pro?les,one can enhance ef?cacy even though lower doses of the individual drugs are used [12].In3single-dose trials of oral surgery patients experi-encing moderate or severe pain after surgery,treatment with the combination of tramadol plus APAP showed superior performance to tramadol alone for overall pain relief,time to onset,and duration of action and superior performance to APAP for overall pain relief and duration of action[10]. When compared with other commonly used combination opioid analgesics,as done in this study,two tablets of tramadol plus APAP provided pain relief comparable to that provided by60mg codeine plus600mg APAP during the immediate postoperative period,and there was a numerical trend favoring tramadol plus APAP tablets during the out-patient phase.Furthermore,in a single-dose,double-blind study of oral surgery patients,two tablets of tramadol plus APAP showed ef?cacy comparable to that of10mg hydro-codone plus650mg APAP[9].
In addition to the potential for increased ef?cacy with combined medications,decreased rates of adverse events would be expected and consistent with the decreased dose of each medication.This study showed that a greater per-centage of patients treated with codeine plus APAP(51%) experienced treatment-emergent adverse events than did patients treated with tramadol plus APAP or placebo(40% and39%,respectively).In another study,examination of tolerability of hydrocodone plus APAP in adults treated for pain after orthopedic surgery found that89%of patients experienced adverse events[19].
We found that vomiting was more frequent in patients receiving codeine plus APAP(14.7%)than in those receiv-ing tramadol plus APAP(9.2%),a frequency comparable to that found with placebo patients(9.1%).The higher-than-expected rates of nausea for all3groups most likely repre-sented the postanesthetic effect.For the course of the study, constipation rates in patients taking a mean of4.4tablets of tramadol plus APAP daily were comparable with the rates in placebo patients but50%lower than the rates in patients receiving a mean of4.3tablets of codeine plus APAP per day.
The favorable tolerability pro?le seen in this study is consistent with previous studies of tramadol plus APAP tablets and is consistent with the rationale of combination therapy.In a single-dose,double-blind study of oral surgery patients,common treatment-emergent adverse events were signi?cantly decreased by treatment with tramadol plus APAP compared with hydrocodone plus APAP treatment and included a signi?cant decreased in nausea(14.0%vs 36.0%)and vomiting(12.0%vs30.0%)[9].In a compara-tive trial of treatment for chronic pain,the combination medication37.5mg tramadol plus325mg APAP was better tolerated than30mg codeine plus300mg APAP[20].In that study,constipation—a common adverse event with opioids—was signi?cantly lower in the tramadol plus APAP group(11%vs21%).This favorable tolerability pro?le was also observed in patients?65years old being treated for acute painful osteoarthritis?are[21].
Including tramadol in a combination analgesic offers the advantage of an unscheduled opioid with demonstrated ef-?cacy after orthopedic surgery as well as low abuse poten-tial and decreased incidence of respiratory depression [11,15,22,23].Moreover,use of the combination with APAP,rather than a nonselective or selective NSAID,may avoid other issues relevant to surgical patients who are at risk for gastrointestinal,hematologic,and renal complica-tions[12,24,25].Although cyclooxygenase(COX)-2inhib-itors,developed to address the gastrointestinal side effects of typical NSAIDs,have demonstrated ef?cacy for postsur-gical pain in orthopedic patients[19],recent reports of impaired fracture healing have identi?ed another potential limitation.In the rat model,treatment with COX-2inhibi-tors was associated with delayed bone healing,suggesting that COX-2activity is necessary for normal bone repair [26].High doses of other NSAIDs in humans have also been linked to delays in healing fractures and repair of spinal surgery[27].
In summary,these results indicate that tramadol plus APAP tablets,a combination analgesic,were effective and well tolerated for treatment of postsurgical pain in patients undergoing abdominal or orthopedic procedures. Appendix
Members of the CAPSS-115Study Group included:Od-est Frank Cannon Jr.,M.D.,and Sidney Ernest Clevinger, M.D.,Ocala,FL;Thomas M.Corbyons,M.D.,and Mark W.Hollmann,M.D.,DeLand,FL;Richard K.Gaines, M.D.,and J.Richard Rhodes,M.D.,South Daytona,FL; Michael M.Leighton,M.D.,and Barry M.Miskin,M.D., West Palm Beach,FL;Paul Lunseth,M.D.,Tampa,FL; Joseph Portoghese,M.D.,Orlando,FL;Michael Drass, M.D.,Altoona,PA;Richard C.Earnhardt,M.D.,Fred-ericksburg,VA;Kenneth J.Edwards,M.D.,St.Joseph,MI; Eric H.Franks,M.D.,and Stephen Konlian,M.D.,Salis-
Table3
Treatment-emergent adverse events with?4.5%incidence among
postsurgical pain patients*
Adverse event Tramadol/APAP Placebo Codeine/APAP
Nausea21(21.4)16(16.2)26(23.9)
Dizziness10(10.2)3(3.0)9(8.3)
Vomiting9(9.2)9(9.1)16(14.7)
Headache8(8.2)8(8.1)8(7.3)
Somnolence5(5.1)1(1.0)4(3.7)
Constipation4(4.1)5(5.1)11(10.1)
*Values expressed as number of events(%).
APAP?acetaminophen.
526 A.B.Smith et al/The American Journal of Surgery187(2004)521–527
bury,MD;David Garry,M.D.,and Scott T.Jackson,M.D., Provo,UT;David S.Jevsevar,M.D.,St.George,UT;Ran-dall Kay Jones,M.D.,West Jordan,UT;Michael H.Bourne, M.D.,Salt Lake City,UT;Richard Jones,M.D.,Dallas,TX; Adam B.Smith,D.O.,Ft.Worth,TX;Thanjavur S.Ravi-kumar,M.D.,Bronx,NY;Benjamin Rigor,M.D.,Louis-ville,KY;Samuel Berry Thompson Jr.,M.D.,and William Everett Tucker Jr.,M.D.,Little Rock,AR;Roger J.Volk-mann,M.D.,Wenatchee,WA.
References
[1]McQuay H,Moore A,Justins D.Treating acute pain in hospital.Br
Med J1997;314:1531–5.
[2]McEvoy A,Livingstone JI,Cahill https://www.360docs.net/doc/908047358.html,parison of diclofenac
sodium and morphine sulphate for postoperative analgesia after day case inguinal hernia surgery.Ann R Coll Surg Engl1996;78:363–6.
[3]Chung F.Recovery pattern and home-readiness after ambulatory
surgery.Anesth Analg1995;80:896–902.
[4]Fortier J,Chung F,Su J.Predictive factors of unanticipated admission
in ambulatory surgery:a prospective study(abstr).Anesthesiology 1996;85:A27.
[5]Chung F,Ritchie E,Su J.Postoperative pain in ambulatory surgery.
Anesth Analg1997;85:808–16.
[6]Peduto VA,Ballabio M,Stefanini S.Ef?cacy of propacetamol in the
treatment of postoperative pain:morphine-sparing effect in orthope-dic surgery.Acta Anaesthesiol Scand1998;42:293–8.
[7]Bourne MH,Rosenthal NR,Xiang J,et https://www.360docs.net/doc/908047358.html,bination tramadol and
acetaminophen tablets(Ultracet?)for the treatment of orthopedic postsurgical pain:a multicenter,randomized,double-blind,placebo-controlled study.J Pain2003;4(2suppl1):88.
[8]Silver?eld JC,Kamin M,Wu S-C,et al.Tramadol/acetaminophen
combination tablets for the treatment of osteoarthritis?are pain:a multicenter,outpatient,randomized,double-blind,placebo-con-trolled,parallel-group,add-on study.Clin Ther2002;24:282–97. [9]Fricke JR Jr,Karim R,Jordan D,et al.A double-blind,single-dose
comparison of the analgesic ef?cacy of tramadol/acetaminophen combination tablets,hydrocodone/acetaminophen combination tab-lets,and placebo after oral surgery.Clin Ther2002;24:953–68. [10]Medve RA,Wang J,Karim R.Tramadol and acetaminophen tablets
for dental pain.Anesth Prog2001;48:79–81.
[11]Cicero TJ,Adams EH,Geller A,et al.A postmarketing surveillance
program to monitor Ultram(tramadol hydrochloride)abuse in the United States.Drug Alcohol Depend1999;57:7–22.[12]Raffa RB.Pharmacology of oral combination analgesics:rational
therapy for pain.J Clin Pharm Ther2001;26:257–64.
[13]Muth-Selbach US,Tegeder I,Brune K,et al.Acetaminophen inhibits
spinal prostaglandin E
2
release after peripheral noxious stimulation.
Anesthesiology1999;91:231–9.
[14]Bjorkman R,Hallman KM,Hedner J,et al.Acetaminophen blocks
spinal hyperalgesia induced by NMDA and substance P.Pain1994;
57:259–64.
[15]Tarradell R,Pol O,Farre M,et al.Respiratory and analgesic effects
of meperidine and tramadol in patients undergoing orthopedic sur-gery.Methods Find Exp Clin Pharmacol1996;18:211–8.
[16]Delbos A,Boccard E.The morphine-sparing effect of propacetamol
in orthopedic postoperative pain.J Pain Symptom Manage1995;10: 279–86.
[17]McQuay HJ,Carroll D,Frankland T,et al.Bromfenac,acetamino-
phen,and placebo in orthopedic postoperative pain.Clin Pharmacol Ther1990;47:760–6.
[18]Edwards JE,McQuay HJ,Moore https://www.360docs.net/doc/908047358.html,bination analgesic ef?-
cacy:individual patient data meta-analysis of single-dose oral tram-adol plus acetaminophen in acute postoperative pain.J Pain Symptom Manage2002;23:121–30.
[19]Gimbel JS,Brugger A,Zhao W,et al.Ef?cacy and tolerability of
celecoxib versus hydrocodone/acetaminophen in the treatment of pain after ambulatory orthopedic surgery in adults.Clin Ther2001;23: 228–41.
[20]Mullican WS,Lacy JR.Tramadol/acetaminophen combination tablets
and codeine/acetaminophen combination capsules for the treatment of pain:a comparative trial.Clin Ther2001;23:1429–45.
[21]Rosenthal N,Wu S,Jordan https://www.360docs.net/doc/908047358.html,bination tramadol and acetamin-
ophen tablets(Ultracet?)for the treatment of pain associated with osteoarthritis?are in an elderly population.J Am Geriatr Soc2002;
50(suppl):S145.
[22]Tarkkila P,Tuominen M,Lindgren https://www.360docs.net/doc/908047358.html,parison of respiratory
effects of tramadol and oxycodone.J Clin Anesth1997;9:582–5. [23]Tarkkila P,Tuominen M,Lindgren https://www.360docs.net/doc/908047358.html,parison of respiratory
effects of tramadol and pethidine.Eur J Anaesthesiol1998;15:64–8.
[24]Gardner GC,Simkin PA.Adverse effects of NSAIDs.Pharmacol
Ther1991;16:750–5.
[25]Power I,Barratt S.Analgesic agents for the postoperative period.
Nonopioids.Surg Clin North Am1999;79:275–95.
[26]Simon AM,Manigrasso MB,O’Connor JP.Cyclo-oxygenase2func-
tion is essential for bone fracture healing.J Bone Miner Res2002;
17:963–76.
[27]Giannoudis PV,MacDonald DA,Matthews SJ,et al.Nonunion of the
femoral diaphysis:the in?uence of reaming and non-steroidal anti-in?ammatory drugs.J Bone Joint Surg Br2000;82:655–8.
527
A.B.Smith et al/The American Journal of Surgery187(2004)521–527
ERP 仓库管理系统
身体仓库管理系统 1、模块说明:每个模块一般可分为六组:基本资料、日常作业、凭证打印、清单与报表、 批次处理、查询作业 1.1 基本资料:产品类别设定、编码原则设定、产品编码、仓别设定、单据性质设定 1.1.1 产品类别设定:此为后续报表数据收集索引和分类之依据 1.1.2 编码原则设定:据此不同公司可采取不同的分段和方式进行自动编码,包 括产品编码、供应商编码、客户资料编码、人员编码等, 都要依此进行自定义。 Eg: A 一般产品编码通用原则为:大分类(3码)+中分类(3码)+小分类(3码)+ 流水码(4码),共计13码左右即可。 Eg: B 编码不必赋予太多特殊意义,亦造成编码上的混乱,以简单明了,易 识别为原则。 1.1.3 产品编码:包括基本项目、采购、生管、仓库、业务、品管、生产、财务 会计、其它,其可根据不同部门使用状况来分类定义,同 时便于基础资料的收集与输入,及日后使用之管理和维护。 1.1.4 仓别设定:此为各仓别属性设定之基础 1.1.5 单据性质设定:此为各“日常作业”之单据性质设定基础。 Eg:A库存异动单对库存的影响可分为:增加、减少 调拨单对库存的影响为:平调 成本开帐/调整单对成本的影响可分为:增加、减少 Eg:B可依不的部门或个人进行单据别的区别使用和管理。 Eg:C单据的编码方式:单别+单据号,或可采用自由编码的方式进行等 Eg:D单据表尾的备注与签核流程等。 Eg:E单据电脑审核流程。 1.2 日常作业:库存异动建立作业、调拨建立作业、成本开帐/调整建立作业、盘点资 料建立作业、批号管理建立作业、借入/出建立作业、借入/出还回作 业 1.2.1 库存异动建立作业:此单据适用于非生产性物料的异动(或增或减),及库存 盘盈亏之调整用,如没有上线制令管理系统亦可通过 此作业进行库存异动作业。 1.2.2 调拨单建立作业:此单据适用于各仓之间的物料调拨之用,不对库存变化 产生影响。 1.2.3 成本开帐/调整建立作业:此单据适用于系统开帐之各仓库存成本资料的输 入,亦是日常“成本重计作业”所产生之单据。 1.2.4 盘点资料建立作业:此单据适用于盘点时库存数量之输入 1.2.5 批号管理建立作业:此单据适用于物料在产品生产过程中的使用和追溯的 管理,及先进先出原理 1.2.6 借入/出建立作业:此单据适用于所有借入/出作业记录之凭证 1.2.7 借入/出还回建立作业:此单据适用所有借入/出还回作业记录之凭证,如无 法归还之作业,则通过进货或销货来做关联性作 业。 1.3 凭证打印:库存异动单凭证、调拨单凭证、成本开帐/调整单凭证、盘点清单凭证、 批号管理凭证、借入/出凭证、借入/出还回凭证
仓库管理系统使用手册
仓库管理系统 ——使用手册
目录 第1章系统概述 (1) 1.1引言 (1) 1.2系统特点....................................................... 错误!未定义书签。第2章系统安装 ............................................ 错误!未定义书签。 2.1系统环境要求............................................... 错误!未定义书签。 2.2单机版的安装............................................... 错误!未定义书签。 2.3网络版的安装............................................... 错误!未定义书签。 2.3.1 程序包文件介绍....................................................... 错误!未定义书签。 2.3.2 数据库的安装与配置............................................... 错误!未定义书签。 2.3.3 客户端的安装与配置............................................... 错误!未定义书签。 2.4系统注册....................................................... 错误!未定义书签。第3章基本操作 (2) 3.1系统启动 (2) 3.2重新登录 (2) 3.3修改密码 (2) 3.4记录排序 (3) 3.5快速查找功能 (3) 3.7窗口分隔 (3) 3.8数据列表属性设置 (3) 3.9数据筛选 (4) 3.10数据导入 (4) 3.11报表设计 (5)
华硕笔记本键盘使用说明
华硕篇 华硕的组合键虽然不是很强大,都是常用的组合键.但比起以前增加了许多功能,而且只有880克的S200来讲,这么小的机有这么多的组合键已经算是难得了. FN+F1:降低屏幕亮度 FN+F2:升高屏幕亮度 FN+F3:等待状态 FN+F4:休眠状态 FN+F5:降低音量 FN+F6:增加音量 FN+F7:静音 FN+F10:切换显示器 FN+F11:等于按下NUM LOCK键 FN+F12:等于按下Scroll lock键 FN+Insert:等于按下打印键(PRINT SCREEN) FN+del:等于按下SysRQ键 FN+向上方向键:等于按下Page Up 键 FN+向下方向键:等于按下Page Down 键 FN+向左方向键:等于按下Page Home键 FN+向右方向键:等于按下Page End键 FN+T:拉伸屏幕 下面为以前的机型S8200快捷键比较简单,大家可以对比一下 FN+F5:增加亮度 FN+F6:减低亮度 FN+F7:关闭/打开屏幕 FN+F8:前换显示器 FN+F9:静音 FN+F10:增加音量 FN+F11:减少音量 FN+F12:等于按下PAUSE间 FN+insert:等于按下num lock键 FN+del:等于按下Scr Lock键 华硕X80系列及华硕F8系列组合键 Fn + F1 进入待机或休眠模式 Fn + F2 开启内置无线网络功能(视选购机型而不同) Fn + F3 E-mail快捷键,开启互联网邮件程序 Fn + F4 因特网快捷键,立即开启互联网浏览器
Fn + F5 调暗液晶显示屏亮度 Fn + F6 调亮液晶显示屏亮度 Fn + F7 液晶屏背光光源开关 Fn + F8 切换液晶显示屏显示,外接显示器或电视 Fn + F9 触摸板锁定快捷键,可以锁定触摸板功能 Fn + F10 静音开关(仅适用于WINDOWS系统下) Fn + F11 降低音量(仅适用于WINDOWS系统下) Fn + F12 提高音量(仅适用于WINDOWS系统下) Fn + Ins 开启或关闭数字键盘功能 Fn + <空格键> 等同于性能设置快捷键,按下后可设置系统性能与省电之间的关系 Fn + C 此组合键可切换屏幕至不同的颜色设置选项,在屏幕画面左上方将出现一些画面 Fn + V 此组合键可以开启摄像头程序 Fn + T 此组合键可开启Power for phone程序
仓库管理系统需求分析说明书
智能仓库管理系统 需求规格说明书 拟制:仇璐佳日期:2010年3月17日星期三审核:日期: 批准:日期: 文档编号:DATA-RATE-SRS-01 创建日期:2010-03-17 最后修改日期:2020-04-24 版本号:1.0.0 电子版文件名:智能仓库管理系统-需求规格说明书-
文档修改记录
基于web智能仓库管理系统详细需求说明书(Requirements Specification) 1.引言 1.1 编写目的 本系统由三大模块构成,分别是:系统设置,单据填开,库存查询。 其中: 系统设置包括:管理员的增加,修改,删除,以及权限管理;仓库内货物的基本资料的增加,修改,删除;工人,客户等的基本资料的增加,修改,删除。 单据填开模块包括:出库单,入库单,派工单,等单据的填开及作废操作。 库存查询系统包括:库存情况的查询,各项明细的查询,工人工资的查询,正在加工产品查询等。 报表导出模块包括:按月,按季度,按年的报表导出功能。 1.2 背景说明 (1)项目名称:基于web智能仓库管理系统 (2)项目任务开发者:东南大学成贤学院06级计算机(一)班仇璐佳,软件基本运行环境为Windows环境,使用MyEclipse7.1作为开发工具,使用struts2作为系统基本框架,Spring作为依赖注入工具,hibernate对MySql所搭建的数据库的封装,前台页面采用ext的js框架,动态能力强,界面友好。 (3)本系统可以满足一般企业在生产中对仓库管理的基本需求,高效,准确的完成仓库的进出库,统计,生产,制造等流程。 1.3 术语定义 静态数据--系统固化在内的描述系统实现功能的一部分数据。
仓库管理系统(软件需求说明书)
1引言 (2) 1.1编写目的 (2) 1.2背景 (2) 1.3定义 (3) 1.4参考资料 (3) 2任务概述 (3) 2.1目标 (3) 2.2用户的特点 (9) 2.3假定和约束 (9) 3需求规定 (9) 3.1对功能的规定 (9) 3.2对性能的规定 (9) 3.2.1精度 (9) 3.2.2时间特性要求 (9) 3.2.3灵活性 (9) 3.3输人输出要求 (9) 3.4数据管理能力要求 (10) 3.5故障处理要求 (10) 3.6其他专门要求 (10) 4运行环境规定 (11) 4.1设备 (11) 4.2支持软件 (11) 4.3接口 (11) 4.4控制 (11)
软件需求说明书 1引言 1.1编写目的 企业的物资供应管理往往是很复杂的,烦琐的。由于所掌握的物资种类众多,订货,管理,发放的渠道各有差异,各个企业之间的管理体制不尽相同,各类统计计划报表繁多,因此物资管理必须实现计算机化,而且必须根据企业的具体情况制定相应的方案。 根据当前的企业管理体制,一般物资供应管理系统,总是根据所掌握的物资类别,相应分成几个科室来进行物资的计划,订货,核销托收,验收入库,根据企业各个部门的需要来发放物资设备,并随时按期进行库存盘点,作台帐,根据企业领导和自身管理的需要按月,季度,年来进行统计分析,产生相应报表。为了加强关键物资,设备的管理,要定期掌握其储备,消耗情况,根据计划定额和实际消耗定额的比较,进行定额的管理,使得资金使用合理,物资设备的储备最佳。 所以一个完整的企业物资供应管理系统应该包括计划管理,合同托收管理,仓库管理,定额管理,统计管理,财务管理等模块。其中仓库管理是整个物资供应管理系统的核心。 开发本系统的目的在于代替手工管理、统计报表等工作,具体要求包括: 数据录入:录入商品信息、供货商信息、名片、入库信息、出库信息、退货信息等信息; 数据修改:修改商品信息、供货商信息、名片、帐号等信息; 统计数据:统计仓库里面的商品的数量,种类,并计算库存总价值; 数据查询:输入查询条件,就会得到查询结果; 数据备份:定期对数据库做备份,以免在数据库遇到意外破坏的时候能够恢复数据库,从而减少破坏造成的损失。
仓库管理系统说明书
二、仓库信息管理系统分析与设计 (一)《仓库信息管理系统》的需求建模 1、需求分析 仓库信息管理系统要能完成以下功能: 仓库存放的货物品种繁多,堆存方式以及处理方式也非常复杂,随着业务量的增加,仓库管理者需要处理的信息量会大幅上升,因此往往很难及时准确的掌握整个仓库的运作状态。针对这一情况,为了减轻仓库管理员和操作员的工作负担,此系统在满足仓库的基本管理功能基础上发挥信息系统的智能化。 根据要求可将系统分为四个模块 (1)用户登录模块 普通操作员和管理人员登录此系统,执行仓库管理的一些操作,但是普通操作员和管理人员所能执行的功能不一样。 (2)仓库管理模块 管理员工作需要登陆系统,才能够进行操作,系统中的各项数据都不允许外人随便查看和更改,所以设置登陆模块是必须的。可以执行仓库进货,退货,领料,退料;商品调拨,仓库盘点等功能。(3)业务查询模块 在用户登录系统后,可以执行库存查询,销售查询,仓库历史记录查询。 (4)系统设置模块 显示当前仓库系统中的信息,在系统中可以执行供应商设置,仓库设置。 2、功能模块分析 (1)登录模块 ①普通操作员:显示当天仓库中的所有库存的信息。 ②管理员:修改仓库中的库存信息。 ③用户注销:在用户执行完仓库功能时,注销。 ④用户退出。 (2)管理模块 ①仓库库存的进货与退货; ②仓库中的库存需要领料和退料功能; ③仓库也可以完成不同地区的商品在此仓库的商品调拨任务; ④用户人员也可以在当天之后对仓库中的库存进行盘点。 (3)查询模块 ①显示当前仓库商品信息,并执行库存查询; ②显示仓库信息,对商品的销售量进行查询; ③此系统还可以对仓库历史记录进行查询。 (4)设置模块 ①供应商设置 ②仓库设置 3、工作内容及要求 ①进一步细化需求分析的内容,识别出系统的参与者,并完成用例图; ②将用例图中的每个用例都写成相应的事件流文档; ③进一步使用活动图来描述每个用例,为后续的系统设计做好准备;
仓库管理系统(详细设计说明书)
1引言 (3) 1.1编写目的 (3) 1.2背景 (3) 1.3定义 (3) 1.4参考资料 (3) 2程序系统的结构 (4) 3用户登录界面程序设计说明 (5) 3.1程序描述 (5) 3.2功能 (5) 3.3性能 (5) 3.4输人项 (6) 3.5输出项 (6) 3.6算法 (6) 3.7流程逻辑 (6) 3.8接口 (7) 3.9存储分配 (7) 4仓库管理模块(02)设计说明 (7) 4.1程序描述 (7) 4.2功能 (8) 4.3性能 (8) 4.4输人项 (8) 4.5输出项 (8) 4.6算法 (8) 4.7流程逻辑 (9) 4.8接口 (10) 5仓库查询模块(03)设计说明 (11) 5.1程序描述 (11) 5.2功能 (11) 5.3性能 (11) 5.4输人项 (11) 5.5输出项 (11) 5.6算法 (12) 5.7流程逻辑 (12) 6系统设置模块(04)设计说明 (13) 6.1程序描述 (13) 6.2功能 (13) 6.3性能 (13) 6.4输人项 (13) 6.5输出项 (13) 6.6算法 (14)
6.7流程逻辑 (14) 6.8接口 (14) 6.9测试计划 (14)
详细设计说明书 1引言 1.1编写目的 本文档为仓库管理系统详细设计文档(Design Document),对作品进行系统性介绍,对使用的技术机制进行分析,对各个模块进行功能描述,并给出主要数据流程和系统结构 本文档的预期读者是本系统的需求用户、团队开发人员、相关领域科研人员 1.2背景 项目名称:仓库管理系统--详细设计说明书 项目任务开发者:大连交通大学软件学院R数学072班张同骥06,软件基本运行环境为Windows环境 1.3定义 Mysql:数据库管理软件 DBMS:数据库管理系统 Windows 2003/XP:运行环境 JSP :软件开发语言 Myeclipse :开发工具 1.4参考资料 《软件工程应用实践教程》清华大学出版社 《系统分析与设计》清华大学出版社 《数据库系统概论》高等教育出版社 《Windows网络编程》清华大学出版社 《VC技术》清华大学出版社
(仓库管理)仓库管理系统软件设计说明书改后
(仓库管理)仓库管理系统软件设计说明书改后
仓库管理系统 软件设计说明书
目录 1. 介绍 (1) 1.1 目的 (1) 1.2 范围 (1) 1.3 定义、缩写词 (1) 1.4 内容概览 (1) 2. 体系结构表示方法 (1) 3. 系统要达到的目标和限制 (2) 4. 用例视图 (2) 4.1 系统用例图 (2) 4.2 产品类别 (3) 4.3 检索产品 (4) 4.4 产品详细 (5) 4.5 管理员注册 (6) 4.6 查看订单 (7) 4.7 下订单 (8) 4.8 管理员登录系统 (9) 4.9 管理员退出系统 (10) 4.10 日常管理 (11) 4.11 商品信息管理 (12) 4.12 供应信息管理 (12) 4.13 名片信息管理 (13) 4.14 配送状态处理 (14) 5. 逻辑视图 (16) 5.1 总览 (16) 5.2 主要Package的介绍 (17) 6. 过程视图 (19) 6.1 管理员盘点 (19) 6.2 产品管理 (20) 6.3 订单处理数据 (22) 6.4 仓库物流管理 (23)
6.5 管理员查询 (24) 7. 部署视图 (24) 8. 流程逻辑 (25) 9. 规模和性能 (26) 10. 质量 (26)
软件设计说明书 1. 介绍 1.1 目的 本文档为仓库管理系统详细设计文档(Design Document),对作品进行系统性介绍,对使用的技术机制进行分析,对各个模块进行功能描述,并给出主要数据流程和系统结构 本文档的预期读者是本系统的需求用户、团队开发人员、相关领域科研人员 1.2 范围 对作品进行系统性介绍,对使用的技术机制进行分析,对各个模块进行功能描述,并给出主要数据流程和系统结构 1.3 定义、缩写词 Mysql:数据库管理软件 DBMS:数据库管理系统 Windows 2003/XP:运行环境 JSP :软件开发语言 Myeclipse :开发工具 1.4 内容概览 ?仓库管理系统 管理员将各项产品进行编排设备号,位置号,从而有效划分区域管理 ?设置系统 设置各项分类的标签,便于其他人进行查询及复查 ?仓库查询系统 进入系统后客户或者管理员有效快捷查询产品各项目录 ?用户登录系统 用户如果要进行查询操作,需要输入正确的用户名和密码,如果输入错误,则停留在登录页; 2. 体系结构表示方法 这篇文档使用一系列视图反映系统架构的某个方面; 用例视图:概括了架构上最为重要的用例和它们的非功能性需求; 逻辑视图:展示了描述系统关键方面的重要用例实现场景(使用交互图); 部署视图:展示构建在处理节点上的物理部署以及节点之间的网络配置(使用部署图);
仓库管理系统需求说明书
《管理信息系统》报告书 2013-2014 学年第 1 学期 仓库管理系统 专业: 信息管理与信息系统 班级: 2班 姓名: XXXXX 学号: 20113444 电话: XXXXXXXXXX 指导教师:王老师 信息科学与工程学院 2013.12.13
1引言 1.1背景 随着社会经济的发展和工业生产的加速,仓库的进出更为频繁,仓库信息更为重要。传统仓库管理完全由人来完成,以手工记录为主,当企业的物流业务成长到一定规模之后,随着订单数量的增加,客户需求不断个性化,执行效率就成为物流发展的瓶颈,单纯依靠人力资源的增加已不能提升出入库执行的速度,反而带来成本的大幅度上升与差错频频。计算机信息管理技术的迅速发展恰恰解决了这个问题,它使计算机技术与现代的管理技术相互配合,来更加准确、高速地完成工业企业日常的仓库管理工作。使企业能够以最少的人员来完成更多的工作。 随着我国市场经济的进一步开展,强大的信息保障,有力的电子化管理,使各大企业在国内经济市场的大潮中把现代高科技的信息技术发挥的淋漓尽致。越来越多有远见的企业家,不惜重金从国外购买高新技术,高的投资、合理的管理往往换来巨大的利润。经营的物质技术手段由简单落后转变成 高科技与人工手段并存,进而更多地将高科技应用到零售商业。国内实施WMS的条件日益成熟。主 要是物流业在过去的两年里随着国家经济的发展,而日新月异,现代一体化物流的管理思想日益为企业所接受,对仓库有了新定位和认识,从而对管理系统也提出了新的要求。所以从仓库管理的周期来考虑,一个能够高效管理的仓库系统就是一个优秀的仓库系统。 1.2开发目的及意义 对于中小型企业,仓库管理工作主要是进货商品的入库管理和销售商品的出库管理及库存商品的保管管理。现有的管理工作主要依靠手工完成,工作量大,且效率不高。为了能更好地利用现代信息技术的成果,提高管理工作的效率和水平,以适应企业发展的需要,决定开发库存管理系统。 商品流通的仓储及配送中心的出入库,库存、配送等管理,能够使管理工作节省人力。减少差错、提高工作效率,并保障。商品流转的顺利进行应用计算机系统与手持终端的结合可以方便、准确地完成商品流转的相关管理。
仓库管理系统详细设计说明书
仓库管理系统 详细设计说明书 班级:xx 姓名:xx 学号:xx 日期:xx年xx月xx日
目录 第一章需求分析 (3) 一、问题背景及描述 (3) 二、功能分析 (3) 三、建立系统流程图 (3) 四、建立数据流图 (5) 五、建立数据字典 (7) 六、算法描述 (9) 七、建立E-R图 (10) 八、建立状态图 (12) 第二章概要设计............................................................................................. 错误!未定义书签。 一、软件体系结构模型........................................................................... 错误!未定义书签。 二、用面向数据流的方法设计系统软件结构....................................... 错误!未定义书签。 三、数据库逻辑结构设计....................................................................... 错误!未定义书签。第三章详细设计 (14) 一、数据库物理结构设计....................................................................... 错误!未定义书签。 二、模块过程设计与界面设计 (14) 第四章数据库设计 (20) 一、数据字典的设计 (20) 二、数据表的设计 (21) 第五章编码和单元测试................................................................................. 错误!未定义书签。第六章程序运行 (22) 一、登陆界面 (22) 二、主控制界面 (23) 三、客户管理子模块界面 (24) 四、用户管理子模块界面 (25) 五、产品入库子模块界面 (26) 六、产品出库子模块界面 (27) 七、产品查询子模块界面 (30) 八、修改产品信息子模块界面 (30) 九、帮助信息子模块界面....................................................................... 错误!未定义书签。第七章心得体会 (32) 参考文献........................................................................................................... 错误!未定义书签。
仓库管理系统使用说明书
仓库管理系统使用手册 项目名称:仓库管理系统 小组成员:杜彦军、付东娜、王丽、邢白雪、郭雨辰 编写日期:2013年12 月13日
目录 1、引言 (3) 1.1 编写目的 (3) 1.2 编写背景 (3) 2、软件概述 (3) 3、开发环境搭建 (3) 3.1安卓软件开发包下载 (3) 3.2 软件的安装 (3) 4、详细使用说明 (7) 4.1 用户管理模块 (7) 4.1.1 用户注册 (7) 4.1.2 用户登录 (12) 4.1.3 用户密码修改 (15) 4.2 基本信息模块 (19) 4.1.2 商品信息管理 (19) 4.1.3 客户信息管理 (26) 4.1.4 供应商信息管理 (32) 4.3 库存管理模块 (39) 4.3.1 商品入库信息管理 (39) 4.3.2 商品出库信息管理 (45) 4.3.3 库存信息查询 (51) 4.4 关于模块 (52)
1、引言 1.1 编写目的 为了使用户更好的了解和使用本产品,使用户更进一步的了解本产品方便正确操作使用,特别编写了用户使用说明手册。 1.2 编写背景 仓储在企业的整个供应链中起着只至关重要的作用,如果不能保障正确的进货和库存的控制及发货,将会导致管理费用的增加,服务的质量难以保证,从而影响企业的竞争力。传统简单、静态的仓库管理已无法保证企业各种资源的有效使用。如今的仓库作业和库存控制作业已十分复杂化多样化,仅靠工人记忆和手工录入不但费时费力,而且容易出错,给企业带来巨大的损失。 为了更好的保障企业的利益,我们出开发了android版仓库管理系统。 2、软件概述 3、开发环境搭建 3.1安卓软件开发包下载 (1)java JDK下载:https://www.360docs.net/doc/908047358.html,/javase/downloads/index.jsp (2)Eslipse下载:https://www.360docs.net/doc/908047358.html,/downloads (3)Android SDK1.5:https://www.360docs.net/doc/908047358.html, (4)ADT插件 3.2 软件的安装 (1)安装JDK完成即可,无需配臵环境变量。
华硕键盘按键使用说明较全版
华硕键盘按键使用说明话外音:Ctrl+alt+a QQ剪切快捷键 退出键 换行键 大小写切换键 上档键(按住后打字母为大写字母) 控制键(一般和其它按键共同使用,详见word快捷键使用方法) 改写数据键(一般和其它按键共同使用,详见word快捷键使用方法) 可以复制当前屏幕内容 可以删除光标后面的字符 可以删除光标前面字符
回车键,换行键 翻页键,可以用于部分软件尤其图片查看软件翻页 FN+F1:降低屏幕亮度 FN+F2:升高屏幕亮度 FN+F3:等待状态 FN+F4:休眠状态 FN+F5:降低音量 FN+F6:增加音量 FN+F7:静音 FN+F10:切换显示器 FN+F11:等于按下NUM LOCK键 FN+F12:等于按下Scroll lock键 FN+Insert:等于按下打印键(PRINT SCREEN) FN+del:等于按下SysRQ键 FN+向上方向键:等于按下Page Up 键 FN+向下方向键:等于按下Page Down 键 FN+向左方向键:等于按下Page Home键 FN+向右方向键:等于按下Page End键
FN+T:拉伸屏幕 下面为以前的机型S8200快捷键比较简单,大家可以对比一下 FN+F5:增加亮度 FN+F6:减低亮度 FN+F7:关闭/打开屏幕 FN+F8:前换显示器 FN+F9:静音 FN+F10:增加音量 FN+F11:减少音量 FN+F12:等于按下PAUSE间 FN+insert:等于按下num lock键 FN+del:等于按下Scr Lock键 华硕X80系列及华硕F8系列组合键 Fn + F1 进入待机或休眠模式 Fn + F2 开启内置无线网络功能(视选购机型而不同) Fn + F3 E-mail快捷键,开启互联网邮件程序 Fn + F4 因特网快捷键,立即开启互联网浏览器 Fn + F5 调暗液晶显示屏亮度 Fn + F6 调亮液晶显示屏亮度 Fn + F7 液晶屏背光光源开关 Fn + F8 切换液晶显示屏显示,外接显示器或电视
仓库管理软件使用说明书样本
百度文库 韦氏盈创仓库管理系统用户手册 厦门韦氏盈创科技有限公司-版权所有
目录 1引言 (3) 编写目的 (3) 参考资料 (3) 术语和缩略词 (3) 2软件概述 (4) 软件功能 (4) 软件运行 (5) 本系统运行在PC 及其兼容机上,使用WINDOWS 操作系统,在软件安装后,直接点 击相应图标,就可以显示出软件的主菜单,进行需要的软件操作。 (5) 系统要求 (5) 3系统使用 (5) 系统登录 (5) 人员信息维护 (6) 3.2.1个人密码修改 (7) 3.2.2权限设置 (7) 3.2.3添加新成员 (8) 3.2.4人员信息浏览 (9) 货品信息维护 (10) 3.3.1货品信息查询 (10) 3.3.2货品信息增加 (11) 3.3.3货品信息删改 (11) 仓库信息维护 (12) 3.4.1仓库信息浏览 (12) 3.4.2仓库信息添加 (13) 存放规则维护 (13) 3.5.1存放规则浏览 (14) 3.5.2添加存放规则 (14) 货物进出记录 (15) 3.6.1货物进出浏览 (15) 3.6.2货物进出添加 (16) 库存信息 (16) 系统功能 (17)
1引言 编写目的 韦氏盈创仓库管理系统是一个公司工作中不可缺少的一部分,他对于公司的人员以及财务的管理者和被管理者都非常重要。所以仓库管理系统应该为管理者和被管理者提供充足的信息和快捷的数据处理手段,但长期以来,人们使用传统的人工方式或性能较低的仓库管理系统来管理公司日常事务,操作流程比较繁琐,错误率比较高。一个成功的管理系统应提供快速的信息检索功能,增加和修改功能。参考资料 《软件需求规格说明书》 《概要设计说明书》 《详细设计说明书》 术语和缩略词 . 人工智能 API (Application Programming Interface) 应用(程序)编程接口Software Quality Assurance软件质量保证 UI Testing界面测试
仓库管理系统详细设计说明书
仓库管理系统详细设计说明书
仓库管理系统 详细设计说明书 班级:xx 姓名:xx 学号:xx 日期:xx年xx月xx日
目录 第一章需求分析 ........................................................... 错误!未定义书签。 一、问题背景及描述.............................................. 错误!未定义书签。 二、功能分析 ......................................................... 错误!未定义书签。 三、建立系统流程图.............................................. 错误!未定义书签。 四、建立数据流图.................................................. 错误!未定义书签。 五、建立数据字典.................................................. 错误!未定义书签。 六、算法描述 ......................................................... 错误!未定义书签。 七、建立E-R图 ...................................................... 错误!未定义书签。 八、建立状态图...................................................... 错误!未定义书签。第二章概要设计 ........................................................... 错误!未定义书签。 一、软件体系结构模型.......................................... 错误!未定义书签。 二、用面向数据流的方法设计系统软件结构....... 错误!未定义书签。 三、数据库逻辑结构设计 ...................................... 错误!未定义书签。第三章详细设计 ........................................................... 错误!未定义书签。 一、数据库物理结构设计 ...................................... 错误!未定义书签。 二、模块过程设计与界面设计 .............................. 错误!未定义书签。第四章数据库设计 ....................................................... 错误!未定义书签。 一、数据字典的设计.............................................. 错误!未定义书签。 二、数据表的设计.................................................. 错误!未定义书签。第五章编码和单元测试 ............................................... 错误!未定义书签。第六章程序运行 ........................................................... 错误!未定义书签。
仓库管理软件使用说明书样本
韦氏盈创仓库管理系统 V1.0 用户手册 厦门韦氏盈创科技有限公司-版权所有
目录 1引言 (3) 1.1编写目的 (3) 1.2参考资料 (3) 1.3术语和缩略词 (4) 2软件概述 (4) 2.1软件功能 (4) 2.2软件运行 (5) 2.3系统要求 (5) 3系统使用 (5) 3.1系统登录 (5) 3.2人员信息维护 (6) 3.2.1个人密码修改 (7) 3.2.2权限设置 (7) 3.2.3添加新成员 (8) 3.2.4人员信息浏览 (9) 3.3货品信息维护 (10) 3.3.1货品信息查询 (10) 3.3.2货品信息增加 (11) 3.3.3货品信息删改 (12) 3.4仓库信息维护 (12) 3.4.1仓库信息浏览 (13) 3.4.2仓库信息添加 (13) 3.5存放规则维护 (14) 3.5.1存放规则浏览 (14)
3.5.2添加存放规则 (15) 3.6货物进出记录 (16) 3.6.1货物进出浏览 (16) 3.6.2货物进出添加 (16) 3.7库存信息 (17) 3.8系统功能 (18) 1引言 1.1编写目的 韦氏盈创仓库管理系统是一个公司工作中不可缺少的一部分,他对于公司的人员以及财务的管理者和被管理者都非常重要。所以仓库管理系统应该为管理者和被管理者提供充足的信息和快捷的数据处理手段,但长期以来,人们使用传统的人工方式或性能较低的仓库管理系统来管理公司日常事务,操作流程比较繁琐,错误率比较高。一个成功的管理系统应提供快速的信息检索功能,增加和修改功能。 1.2参考资料 《软件需求规格说明书》 《概要设计说明书》 《详细设计说明书》
华硕bios手册
ASUS Win Flash User’s Guide
Contents Chapter 1ASUS Win Flash (1) 1.1Introduction (1) 1.2How to upgrade BIOS (1)
Chapter 1ASUS Win Flash 1.1 Introduction ASUS Win Flash is a tool to update BIOS in Windows. Please verify the exact model and download the latest BIOS file for your Notebook from ASUS Download Site. Please ensure that you have installed ASUS Win Flash Utility before using update procedure. You may install the program via Driver & Utility CD if you cannot find the program from Start -> All Programs->ASUS Utility. 1.2 How to upgrade BIOS 1.Click Start \ All Programs \ ASUS Utility \ WINFLASH \ WINFLASH
2. Select and open the updated BIOS image file 3.Please confirm the loaded BIOS information as displayed in the following image
(仓库管理)仓库管理系统使用说明书
(仓库管理)仓库管理系统 使用说明书
目录1、引言2 1.1编写目的2 1.2编写背景2 2、软件概述3 3、开发环境搭建3 3.1安卓软件开发包下载3 3.2软件的安装3 4、详细使用说明7 4.1用户管理模块7 4.1.1用户注册7 4.1.2用户登录12 4.1.3用户密码修改15 4.2基本信息模块19 4.1.2商品信息管理19 4.1.3客户信息管理26 4.1.4供应商信息管理32 4.3库存管理模块39 4.3.1商品入库信息管理39 4.3.2商品出库信息管理45 4.3.3库存信息查询51 4.4关于模块52
1、引言 1.1编写目的 为了使用户更好的了解和使用本产品,使用户更进一步的了解本产品方便正确操作使用,特别编写了用户使用说明手册。 1.2编写背景 仓储在企业的整个供应链中起着只至关重要的作用,如果不能保障正确的进货和库存的控制及发货,将会导致管理费用的增加,服务的质量难以保证,从而影响企业的竞争力。传统简单、静态的仓库管理已无法保证企业各种资源的有效使用。如今的仓库作业和库存控制作业已十分复杂化多样化,仅靠工人记忆和手工录入不但费时费力,而且容易出错,给企业带来巨大的损失。 为了更好的保障企业的利益,我们出开发了android版仓库管理系统。 2、软件概述 3、开发环境搭建 3.1安卓软件开发包下载 (1)javaJDK下载:.downloads/ (2)Eslipse下载: (3)ADT插件 3.2软件的安装 (1)安装JDK完成即可,无需配置环境变量。
(2)解压exlipse,无需安装,解压后,直接打开就行。 (3)安装SDK: 在AndroidDevelopers下载android-sdk_r05-,下载完成后解压到任意路径。 ·运行SDK,点击AvailablePackages。如果没有出现可安装的包,请点击Settings,选中Misc中的"Force..."这项,再点击AvailablePackages。 ·选择希望安装的SDK及其文档或者其它包,点击InstallationSelected、AcceptAll、InstallAccepted,开始下载安装所选包 ·在用户变量中新建PATH值为:AndroidSDK中的tools绝对路径(本机为D:\AndroidDevelop\android-sdk-windows\tools)。“确定”后,重新启动计算机。重启计算机以后,进入cmd命令窗口,检查SDK是不是安装成功。 运行android–h如果有类似以下的输出,表明安装成功: (4)安装ADT (1)打开浏览器,进入Android开发者官方主页,地址 (2)“./”。 (3)单击“SDK”选项卡,单击页面右侧的“ADT16.0.1”链接。(3)滚动页面到“DownloadingtheADTPlugin”,复制
华硕笔记本使用说明书
Notebook
PC
U s e r ’s
Manual
C1128 1.00 2002 10
2
50
70
3
(0 ) 122 )
30 (50
4
pre-load
Fn+F7
5
................................................................................................................................................. 2 ......................................................................................................................................... 3 ......................................................................................................................................................... 6
1-1
..................................................................................................................... 12 ............................................................................................................................................12 ............................................................................................................................................13 ............................................................................................................................................14 ............................................................................................................................................15 ............................................................................................................................................16 ............................................................................................................................................17
1-2
................................................................................................................................. 18 1-2-1 DVD-ROM 1-2-2 CD-RW 1-2-3 1-2-4 1-2-5 1-2-6 / ............................................................................................................18 .........................................................................................................................18 ............................................................................................................... 19 PortBar II .......................................................................................................20
..................................................................................................................21 PortDockII .................................................................................................22
........................................................................................................................................ 22 ............................................................................................................................ 22 ........................................................................................................................................ 22
6