Chimeric Antigen Receptor–Modified T Cells for Acute Lymphoid Leukemia_nihms-474709
Patients with relapsed and chemotherapy-refractory pre–B-cell ALL have a poor prognosis
despite the use of aggressive therapies such as allogeneic hematopoietic stem-cell
transplantation 1,2 and bispecific CD19 antibody fragments.3 Chimeric antigen receptor–
modified T cells that target the lineage-specific antigens CD19 and CD20 have been
reported to be effective in adults with CLL and B-cell lymphomas.4-9 However, the effects
of chimeric antigen receptor T cells on ALL blasts, a more immature leukemia that
progresses more rapidly, have not been fully investigated. In particular, there has been
uncertainty about whether chimeric antigen receptor T cells would expand in vivo in patients
with ALL and whether they would have antileukemic efficacy in patients with relapsed
disease, high tumor burdens, or both.
We previously reported the in vivo expansion and robust antileukemic effects of CTL019
(formerly CART19) cells in three patients with CLL.7,8 CTL019 is a chimeric antigen
receptor that includes a CD137 (4-1BB) signaling domain and is expressed with the use of
lentiviral-vector technology.10 Here we report the use of CTL019 in two children with
refractory and relapsed ALL. Both children had remission of leukemia, accompanied by the
robust expansion of CTL019 in vivo, with CTL019 detected in bone marrow and the CSF.
The antileukemic effects were potent, given that one child had chemotherapy-refractory
disease that precluded allogeneic donor stem-cell transplantation, and the other child had
had a relapse after allogeneic cord-blood transplantation and had resistance to
blinatumomab, a chimeric bispecific anti-CD3 and anti-CD19 monoclonal antibody.Case Reports Patient 1 was a 7-year-old girl with a second recurrence of ALL. She had received a
diagnosis 2 years earlier. A remission with a negative test for minimal residual disease had
been achieved, then she had a relapse 17 months after the original diagnosis. She had a
second remission after reinduction chemo-therapy, but the cancer recurred 4 months later,
and she did not have a response to further intensive chemotherapy, including clofarabine,
etoposide, and cyclophosphamide. Her karyotype at baseline was 48,XX,del(9)(p21.3),
+11,del(14)(q2?q24),+16/46, XX[4]. Peripheral-blood mononuclear cells (PBMCs) were
collected by means of apheresis before administration of the intensive chemotherapy, with
the anticipation that there might be an insufficient number of circulating T cells available for
cell manufacturing after such intensive treatment. The patient received an infusion of
CTL019 cells that had been expanded with anti-CD3 and anti-CD28 antibodies and
lentivirally transduced to express the anti-CD19 chimeric antigen receptor; the total dose
was 108 CD3+ cells per kilogram (1.2×107 CTL019 cells per kilogram), given over a period
of 3 consecutive days, as previously described.7,8 She did not receive lymphocyte-depleting
chemotherapy before treatment with the CTL019 infusions, with the most recent cytotoxic
therapy having been given 6 weeks before CTL019 infusion. No immediate infusion-related
toxic effects were noted, but she was hospitalized for low-grade fevers that progressed to
high fevers by day 4, and on day 5 (Fig. 1A), she was transferred to the pediatric intensive
care unit. This was followed by rapid progression to respiratory and cardiovascular
compromise requiring mechanical ventilation and blood-pressure support.
NIH-PA Author Manuscript NIH-PA Author Manuscript
NIH-PA Author Manuscript
Patient 2 was a 10-year-old girl with ALL who had had a second relapse after undergoing
transplantation of umbilical-cord blood from an unrelated donor (HLA-4/6) 28 months after
diagnosis and 10 months before CTL019 infusion. She had had graft-versus-host disease
(GVHD) after the transplantation, which resolved with treatment; she was not receiving
immunosuppressive therapy at the time of her relapse. She did not have another remission,
in spite of multiple cytotoxic and biologic therapies. Her baseline karyotype was
46,XX,del(1)(p13),t(2;9)(q?21;q?21), t(3;17)(p24;q23),del(6)(q16q21),del(9)(q13q22),
der(16)t(1;?;16)(p13;?p13.3)[9]//46,XY[1]. Before PBMC collection, she received two
cycles of blinatumo mab,3 a CD19-targeted bispecific antibody treatment for ALL, with no
response. Sixty-eight percent of her peripheral-blood cells were of donor origin at the time
of PBMC collection. CTL019 T cells were manufactured and infused at a total dose of 107
CD3+ cells per kilogram (1.4×106 CTL019 cells per kilogram) in a single dose; etoposide–
cyclophosphamide chemotherapy had been administered for lymphocyte depletion the week
before. Her bone marrow on the day before CTL019 infusion was replaced by a population
of CD19+CD34+ ALL cells, with variable expression of CD19 on flow cytometry (Fig. S1
in the Supplementary Appendix, available with the full text of this article at https://www.360docs.net/doc/ce16484044.html,). The
patient had no immediate infusion-related toxic effects, but a fever developed on day 6 and
she was admitted to the hospital. She had no cardio-pulmonary toxic effects and did not
receive glucocorticoids or anticytokine therapy. Her fever was of unknown origin but was
suspected to be due to the cytokine-release syndrome (Fig. 1B); she also had myalgias and 2
days of confusion (grade 3), all of which spontaneously resolved. She had no evidence of
GVHD after the infusion of the CTL019 cells. Although these cells had been collected from
the patient, the infused cells were all of donor (cord blood) origin.Methods
The patients were the first two enrolled in an institutional review board–approved phase 1clinical trial (https://www.360docs.net/doc/ce16484044.html, number, NCT01626495) that was designed to assess the safety and feasibility of infusing autologous CTL019 T cells in children with relapsed or refractory B-cell cancers. All authors discussed and interpreted the results and vouch for the data and analyses. No commercial sponsor was involved in the study.The materials and methods used in CTL019 production have been reported previously,7,8with the exception of the lentiviral vector for this protocol, which was produced at Children's Hospital of Philadelphia. CTL019 was detected and quantified in clinical specimens as previously reported.7,8 Additional experimental details are included in the Supplementary Appendix.
Results Induction of Remission in Both Patients
Both children had an increase in circulating lymphocytes and neutrophils in the 2 weeks
after CTL019 infusion, as shown by plots depicting the total white-cell count, absolute
lymphocyte count, and absolute neutrophil count relative to the timing of CTL019 infusion
(Fig. 1C). Most of the lymphocytes were T cells that expressed the chimeric antigen receptor
(Fig. 2, and Fig. S2 in the Supplementary Appendix). In both children, high-grade, most
NIH-PA Author Manuscript NIH-PA Author Manuscript
NIH-PA Author Manuscript
likely noninfectious fevers were documented, followed by elevations in lactate
dehydrogenase (LDH) levels (Fig. 1A). The elevations in LDH levels and the high-grade
fevers were similar to those previously described in patients with CLL after CTL019
infusion.7,8 Approximately 1 month after infusion, morphologic remission of leukemia
(minimal residual disease, <0.01%) was achieved in both children. Results of flow-
cytometric assays of minimal residual disease were confirmed by molecular detection of
clonal IgH transcripts by means of deep sequencing (Table 1).
The clinical remission in Patient 1 was associated with a molecular remission that had
persisted for 9 months as of January 2013. High-throughput DNA sequencing of the IGH
locus revealed a pronounced decrease in total rearranged IGH sequence reads on day 23 in
blood and marrow specimens. The malignant clone was not detected in the blood or marrow
in more than 1 million cell equivalents that were sequenced on day 180 (Table 1). In
contrast, rearranged T-cell– receptor sequences were readily detected in blood and marrow,
findings that indicate the integrity of the DNA tested at all time points.
Toxicity of CTL019
Grade 3 and 4 adverse events are summarized in Table 2. Both patients had acute toxic
effects, which consisted of fever and a cytokine-release syndrome that evolved into the
macrophage activation syndrome. Both patients were monitored and given prophylaxis for
the tumor lysis syndrome. Both had substantial elevations in LDH levels, the causes of
which were probably multi-factorial but could have included the tumor lysis syndrome. Each
uric acid value in Patient 1 was either below or within the normal range, and she received
allopurinol on days 5 and 6 only. Patient 2 received prophylactic allopurinol on days 0
through 14 and had abnormal uric acid values of 4.8 to 5.7 mg per deciliter (286 to 339 μmol
per liter) on days 8 through 10, which were consistent with mild tumor lysis syndrome.
Severe cytokine-release syndrome developed in Patient 1. Glucocorticoids were
administered to this patient on day 5, with a brief response in the fever curve but without
remission of hypotension. A single course of anticytokine therapy, consisting of etanercept
and tocilizumab, was given on day 7, with rapid clinical effects: within hours, defervescence
occurred, and the patient was weaned from vasoactive medications and ventila-tory support
as the clinical and radiologic manifestations of the acute respiratory distress syndrome
resolved. She did not have laboratory evidence of the tumor lysis syndrome; however,
biochemical evidence of the macrophage activation syndrome was noted, with elevation of
the ferritin level to 45,529 ng per deciliter on day 11, coagulopathy with an elevated d-dimer
level and hypofibrinogenemia, hepatosplenomegaly, and elevated levels of
aminotransferases, LDH (Fig. 1A), and triglycerides, as well as a cytokine profile that was
consistent with the macrophage activation syndrome. Her ferritin level decreased to 2368 ng
per deciliter by day 26, and the clinical and laboratory abnormalities of the macrophage
activation syndrome resolved.
In Patient 2, although there was no direct evidence of the tumor lysis syndrome other than
fever and changes in the LDH level (Fig. 1A), features of the macrophage activation
syndrome also developed, with elevations in the ferritin level to 33,360 ng per deciliter on
day 7, peaking at 74,899 ng per deciliter on day 11; aminotransferase levels that reached
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
grade 4 for 1 day; and an elevated serum d-dimer level. These biochemical changes were
reversible: on day 21, the amino-transferase elevations were grade 1, and the ferritin level
3894 ng per deciliter. The patient was discharged from the hospital on day 16.
Both children had prominent elevations in a number of cytokines and cytokine receptors in
the serum (Fig. 1B). In both, elevations in interferon-γ and interleukin-6 were most
prominent. These observations are similar to the pattern observed previously in patients with
CLL who also had a remission of leukemia after CTL019 infusion.8 The peak cytokine
elevations were temporally correlated with systemic inflammation as determined by changes
in core body temperature (Fig. 1A and 1B).
In Vivo Expansion of CTL019
The fraction of CTL019 T cells in circulation progressively increased in vivo to 72% of T
cells in Patient 1 and 34% of T cells in Patient 2 (Fig. 2A). The initial transduction
efficiency was 11.6% and 14.4% for the T cells infused in Patient 1 and Patient 2,
respectively. In both children, the absolute lymphocyte count increased substantially (Fig.
1C) and the number of CTL019 cells progressively increased from baseline in vivo (Fig. 2A,
and Fig. S2 in the Supplementary Appendix), reflecting a robust and selective expansion of
CTL019 cells. The selective increase in T cells expressing CTL019 in both children is
consistent with an antileukemic mechanism involving CD19-driven expansion and with the
subsequent elimination of cells expressing CD19 (Fig. 3, and Fig. S3A and S3B in the
Supplementary Appendix).
Molecular deep-sequence analysis of T-cell receptors (TCRs) in the peripheral-blood and
marrow samples obtained from Patient 1 on day 23, when more than 65% of CD3+ cells in
peripheral blood and marrow were shown to be CTL019+ on flow cytometry, revealed the
absence of a dominant T-cell TCR clonotype in both compartments, with the 10 most
abundant T cells present at frequencies of 0.2 to 0.7% in bone marrow and 0.2 to 0.8% in
peripheral blood. Six of the 10 dominant clones were shared between the two compartments.
In addition, both CD4 and CD8 chimeric antigen receptor T cells were present. Thus, the
chimeric antigen receptor T cells appeared to proliferate after CD19-stimulated expansion
and not by means of TCR signals or clone-specific events such as activation by integration
of the lentivirus.
Expansion and Morphologic Features of CTL019 Chimeric Antigen Receptor T Cells
In both children, CTL019 cells expanded in the peripheral blood and bone marrow to levels
that were more than 1000 times as high as the original engraftment levels (Fig. 2A and 2B).
The frequency of CTL019 cells increased to more than 10% of circulating T cells by day 20
in both children (Fig. S2 in the Supplementary Appendix), with the absolute magnitude of
CTL019 expansion similar to that observed in patients with CLL.8 Unexpectedly, cells in
the CSF also showed a high degree of CTL019 gene marking and persisted at a high
frequency at 6 months (Fig. 2B). The presence of CTL019 cells in the CSF was surprising,
given that neither child had detectable central nervous system (CNS) leukemia according to
analysis of cytospin preparations at the time of infusion or at the evaluation 1 month after
treatment. Furthermore, prior studies of chimeric antigen receptor therapy for B-cell cancers NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
have not shown the presence of chimeric antigen receptor T cells in the CNS.4,6,9,11-13 The
morphologic features of the lymphocytes in the blood and CSF are shown for both children
in Figure 2D. Because more than 70% of lymphocytes in circulation on day 10 were
CTL019 cells (Fig. 2A and 2B), most of the large granular lymphocytes in the peripheral
blood, as shown in Figure 2D, are probably CTL019 cells. Similarly, because many
lymphocytes in the CSF obtained from Patient 2 on day 23 were CTL019 cells (Fig. 2B and
2C), the CSF lymphocytes shown in Figure 2D most likely represent the morphologic
features of CTL019 cells in vivo that have migrated to the CSF.
Induction of B-Cell Aplasia
In both children, CD19+ cells in bone marrow and blood were eliminated within 1 month
after CTL019 infusion (Fig. 3, and Fig. S3A and S3B in the Supplementary Appendix). In
Patient 1, a large proportion of cells remaining in the marrow at day 6 after infusion were
CD19+CD20+ leukemic blast cells. This population of cells was not detectable by day 23,
an effect that has been maintained (Fig. S3A in the Supplementary Appendix). Marrow in
this patient remained in remission for 9 months, and peripheral-blood counts remained
normal for more than 11 months. Patient 1 did not receive chemotherapy in the 6 weeks
before CTL019 infusion, which indicates that the CTL019 cells were sufficient to ablate
normal and leukemic B cells in this patient.
Emergence of CD19 Escape Variant in Patient 2
Patient 2 had a clinical relapse that was apparent in the peripheral blood 2 months after
CTL019 infusion, as evidenced by the reappearance of blast cells in the circulation. These
cells were CD45+dim, CD34+ and did not express CD19 (Fig. 3). The absence of the
original dominant CD34dim+CD34+CD19dim+ cells is consistent with a potent
antileukemic selective pressure of the CTL019 chimeric antigen receptor T cells directed to
CD19 (Fig. S3B in the Supplementary Appendix). Deep sequencing of IGH revealed the
presence of the malignant clone in peripheral blood and marrow as early as day 23 (Table 1),
despite a clinical assessment of no residual disease by means of flow cytometry at this time
point (Fig. S1 in the Supplementary Appendix). In addition, deep sequencing of DNA
isolated from bone marrow cells obtained at the time of clinical relapse revealed that the
CD45+dimCD34+CD19– cells are clonally related to the initial dominant CD45dim
+CD34+CD19dim+ cells, since they share the same IGH sequence.Discussion
We report the induction of remission of relapsed and refractory leukemia in the first two
patients treated on this protocol. Remission has been sustained in one patient and was
accompanied by relapse due to the emergence of CD19– blasts in the other patient. High
levels of genetically modified CTL019 cells were detected in the CNS in both patients.
Systemic elevations of proinflammatory cytokines, which were reversible, were concomitant
with peak T-cell expansion and tumor-cell elimination and therefore consistent with on-
target activity of CTL019 cells against CD19+ target cells. The induction of complete
remission in refractory CD19+ ALL after infusion of chimeric antigen receptor T cells is
encouraging, particularly given the low frequency of remissions after the infusion of
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
allogeneic donor lymphocytes that do not express chimeric antigen receptors.14-16 Deep
sequencing indicated that the CTL019 chimeric antigen receptor infusion was associated
with a sustained 5-log 10 reduction in the frequency of malignant B cells in Patient 1,
providing further evidence of potent antitumor effects in chemotherapy-refractory leukemia.
The unfortunate emergence of CD19– blast cells in one patient is consistent with previous
reports that document the presence of CD19– precursor cells in some patients with
ALL.17,18 It is possible that the coinfusion of chimeric antigen receptor T cells redirected to
specificities, such as CD22, in addition to CD19 might decrease the likelihood of this event.
Thus far, we have not observed a relapse with CD19– escape cells in adults with CLL after
treatment with CTL019 cells,8 a finding that suggests this issue may be specific to a subset
of acute leukemias. Finally, the induction of remission in Patient 1 did not require
concomitant chemotherapy and is consistent with our previous observation that remissions
in CLL could be delayed for several weeks after chemotherapy.7 Thus, concomitant
administration of cytotoxic chemotherapy may not be necessary for chimeric antigen
receptor– mediated antitumor effects.
Both children with ALL had substantial toxic effects after CTL019 infusion. The induction
of B-cell aplasia was expected and indicates that the chimeric antigen receptor T cells can
function in patients with relapsed acute leukemia. Both children also had clinical and
laboratory evidence of the cytokine-release syndrome and the macrophage activation
syndrome within a week after infusion. The cytokine profile observed in these children is
similar to the cytokine patterns previously observed in children with hemophagocytosis and
the macrophage activation syndrome or hemophagocytic lymphohistiocytosis.19,20 The
macrophage activation syndrome is characterized by hyperinflammation with prolonged
fever, hepatosplenomegaly, and cytopenias. Laboratory findings that are characteristic of
this syndrome are elevated levels of ferritin, triglycerides, aminotransferases, bilirubin
(primarily conjugated), and soluble interleukin-2 receptor α chain and decreased levels of
fibrinogen.21 Recent studies indicate that tocilizumab (anti–interleukin-6 receptor
monoclonal antibody) holds promise for glucocorticoid-resistant GVHD,22-24 and our results
are consistent with these data.
The vigorous in vivo expansion of CTL019, persistent B-cell aplasia, and prominent
antileukemic activity suggest that CTL019 cells have substantial and sustained effector
functions in children with advanced ALL. The highly efficient migration of chimeric antigen
receptor T cells to the CSF is encouraging as a mechanism for surveillance to prevent
relapse in the CNS 25 and supports the testing of chimeric antigen receptor T-cell–directed
therapies for CNS lymphomas and primary CNS cancers. With the exception of B-cell
aplasia, the duration of which is currently undefined, immune-based therapies such as
CTL019 may have a favorable profile of long-term adverse effects, as compared with the
high-dose regimens of chemotherapy and radiation therapy that are the current standard of
care for most cases of relapsed pediatric leukemia.26Supplementary Material
Refer to Web version on PubMed Central for supplementary material.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Acknowledgments
Supported in part by grants from the National Institutes of Health (1R01CA165206, to Dr. June; and R01CA102646
and R01CA116660, to Dr. Grupp) and the Leukemia and Lymphoma Society.
We thank Timothy Macatee for sample processing and flow-cytometric analysis; Irina Kulikovskaya and Minnal
Gupta for the quantitative polymerase-chain-reaction assay; Erica Suppa for the Luminex assay; Saar Gill,
Marybeth Helfrich, and Jessica Hulitt for assistance with images and flow-cytometric data analysis; Zhaohui Zheng,
Andrea Brennan, Julio Cotte, and members of the Clinical Cell and Vaccine Production Facility for development of
methods for clinical-scale ex vivo lentiviral transduction and for cell manufacturing; the Human Immunology Core
for provision of reagents; Christine Strait, Margaret Tartaglione, Elizabeth Veloso, Lester Lledo, and Joan Gilmore
for assistance in clinical research support; Edward Behrens and Donald Siegel for advice; Children's Hospital of
Philadelphia Vector Core (Katherine High) for clinical-grade vector production; Kenneth Cornetta and the National
Gene Vector Bioreposi-tory at the Indiana University School of Medicine for postinfusion testing of the product for
replication-competent lentivirus; Cindy Desmarais, Harlan Robins, and Nishanth Marthandan at Adaptive
Biotechnologies for assistance with molecular analysis of minimal residual disease; and Bipulendu Jena and
Laurence Cooper for provision of the chimeric antigen receptor anti-idio-type detection reagent.References 1. Barrett AJ, Horowitz MM, Pollock BH, et al. Bone marrow transplants from HLA-identical siblings as compared with chemotherapy for children with acute lymphoblastic leukemia in a second remission. N Engl J Med. 1994; 331:1253–8. [PubMed: 7935682]2. G?kbuget N, Stanze D, Beck J, et al. Outcome of relapsed adult lymphoblastic leukemia depends on response to salvage chemotherapy, prognostic factors, and performance of stem cell transplantation.Blood. 2012; 120:2032–41. [PubMed: 22493293]3. Bargou R, Leo E, Zugmaier G, et al. Tumor regression in cancer patients by very low doses of a T cell-engaging antibody. Science. 2008; 321:974–7. [PubMed: 18703743]4. Till BG, Jensen MC, Wang J, et al. Adoptive immunotherapy for indolent non-Hodgkin lymphoma and mantle cell lymphoma using genetically modified autologous CD20-specific T cells. Blood.2008; 112:2261–71. [PubMed: 18509084]
5. Kochenderfer JN, Wilson WH, Janik JE, et al. Eradication of B-lineage cells and regression of
lymphoma in a patient treated with autologous T cells genetically engineered to recognize CD19.
Blood. 2010; 116:4099–102. [PubMed: 20668228]
6. Brentjens RJ, Rivière I, Park JH, et al. Safety and persistence of adoptively transferred autologous
CD19-targeted T cells in patients with relapsed or chemotherapy refractory B-cell leukemias.
Blood. 2011; 118:4817–28. [PubMed: 21849486]
7. Porter DL, Levine BL, Kalos M, Bagg A, June CH. Chimeric antigen receptor-modified T cells in
chronic lymphoid leukemia. N Engl J Med. 2011; 365:725–33. [PubMed: 21830940]
8. Kalos M, Levine BL, Porter DL, et al. T cells expressing chimeric receptors establish memory and
potent antitumor effects in patients with advanced leukemia. Sci Transl Med. 2011; 3:95ra73.
9. Savoldo B, Ramos CA, Liu E, et al. CD28 costimulation improves expansion and persistence of
chimeric antigen re ceptor–modified T cells in lymphoma patients. J Clin Invest. 2011; 121:1822–6.
[PubMed: 21540550]
10. Milone MC, Fish JD, Carpenito C, et al. Chimeric receptors containing CD137 signal transduction
domains mediate enhanced survival of T cells and increased antileukemic efficacy in vivo. Mol
Ther. 2009; 17:1453–64. [PubMed: 19384291]
11. Jensen MC, Popplewell L, Cooper LJ, et al. Anti-transgene rejection responses contribute to
attenuated persistence of adoptively transferred CD20/CD19-specific chimeric antigen receptor
redirected T cells in humans. Biol Blood Marrow Transplant. 2010; 16:1245–56. [PubMed:
20304086]
12. Kochenderfer JN, Dudley ME, Feldman SA, et al. B-cell depletion and remissions of malignancy
along with cytokine-associated toxicity in a clinical trial of anti-CD19 chimeric-antigen-receptor-
transduced T cells. Blood. 2012; 119:2709–20. [PubMed: 22160384]
NIH-PA Author Manuscript
NIH-PA Author Manuscript
NIH-PA Author Manuscript
13. Till BG, Jensen MC, Wang J, et al. CD20-specific adoptive immunotherapy for lymphoma using a chimeric antigen receptor with both CD28 and 4-1BB domains: pilot clinical trial results. Blood.2012; 119:3940–50. [PubMed: 22308288]14. Kolb HJ, Schattenberg A, Goldman JM, et al. Graft-versus-leukemia effect of donor lymphocyte transfusions in marrow grafted patients. Blood. 1995; 86:2041–50. [PubMed: 7655033]15. Collins RH Jr, Shpilberg O, Drobyski WR, et al. Donor leukocyte infusions in 140 patients with relapsed malignancy after allogeneic bone marrow transplantation. J Clin Oncol. 1997; 15:433–44.[PubMed: 9053463]16. Collins RH Jr, Goldstein S, Giralt S, et al. Donor leukocyte infusions in acute lymphocytic leukemia. Bone Marrow Transplant. 2000; 26:511–6. [PubMed: 11019840]17. Hotfilder M, R?ttgers S, Rosemann A, et al. Leukemic stem cells in childhood high-risk ALL/t(9;22) and t(4;11) are present in primitive lymphoid-restricted CD34+CD19? cells. Cancer Res.2005; 65:1442–9. [PubMed: 15735032]18. le Viseur C, Hotfilder M, Bomken S, et al. In childhood acute lymphoblastic leukemia, blasts at different stages of immunophenotypic maturation have stem cell properties. Cancer Cell. 2008;14:47–58. [PubMed: 18598943]19. Tang Y, Xu X, Song H, et al. Early diagnostic and prognostic significance of a specific Th1/Th2cytokine pattern in children with haemophagocytic syndrome. Br J Haematol. 2008; 143:84–91.[PubMed: 18673367]20. Behrens EM, Canna SW, Slade K, et al. Repeated TLR9 stimulation results in macrophage activation syndrome–like disease in mice. J Clin Invest. 2011; 121:2264–77. [PubMed: 21576823]21. Janka GE. Familial and acquired hemophagocytic lymphohistiocytosis. Annu Rev Med. 2012;63:233–46. [PubMed: 22248322]22. Drobyski WR, Pasquini M, Kovatovic K, et al. Tocilizumab for the treatment of steroid refractory graft-versus-host disease. Biol Blood Marrow Transplant. 2011; 17:1862–8. [PubMed: 21745454]23. Tawara I, Koyama M, Liu C, et al. Interleukin-6 modulates graft-versus-host responses after experimental allogeneic bone marrow transplantation. Clin Cancer Res. 2011; 17:77–88.[PubMed: 21047980]24. Le Huu D, Matsushita T, Jin G, et al. IL-6 blockade attenuates the development of murine
sclerodermatous chronic graft-versus-host disease. J Invest Dermatol. 2012; 132:2752–61.
[PubMed: 22810302]
25. Pullen J, Boyett J, Shuster J, et al. Extended triple intrathecal chemotherapy trial for prevention of
CNS relapse in good-risk and poor-risk patients with B-progenitor acute lymphoblastic leukemia:
a Pediatric Oncology Group study. J Clin Oncol. 1993; 11:839–49. [PubMed: 8487048]
26. Garcia-Manero G, Thomas DA. Salvage therapy for refractory or relapsed acute lymphocytic
leukemia. Hematol Oncol Clin North Am. 2001; 15:163–205. [PubMed: 11253606]
NIH-PA Author Manuscript
NIH-PA Author Manuscript
NIH-PA Author Manuscript
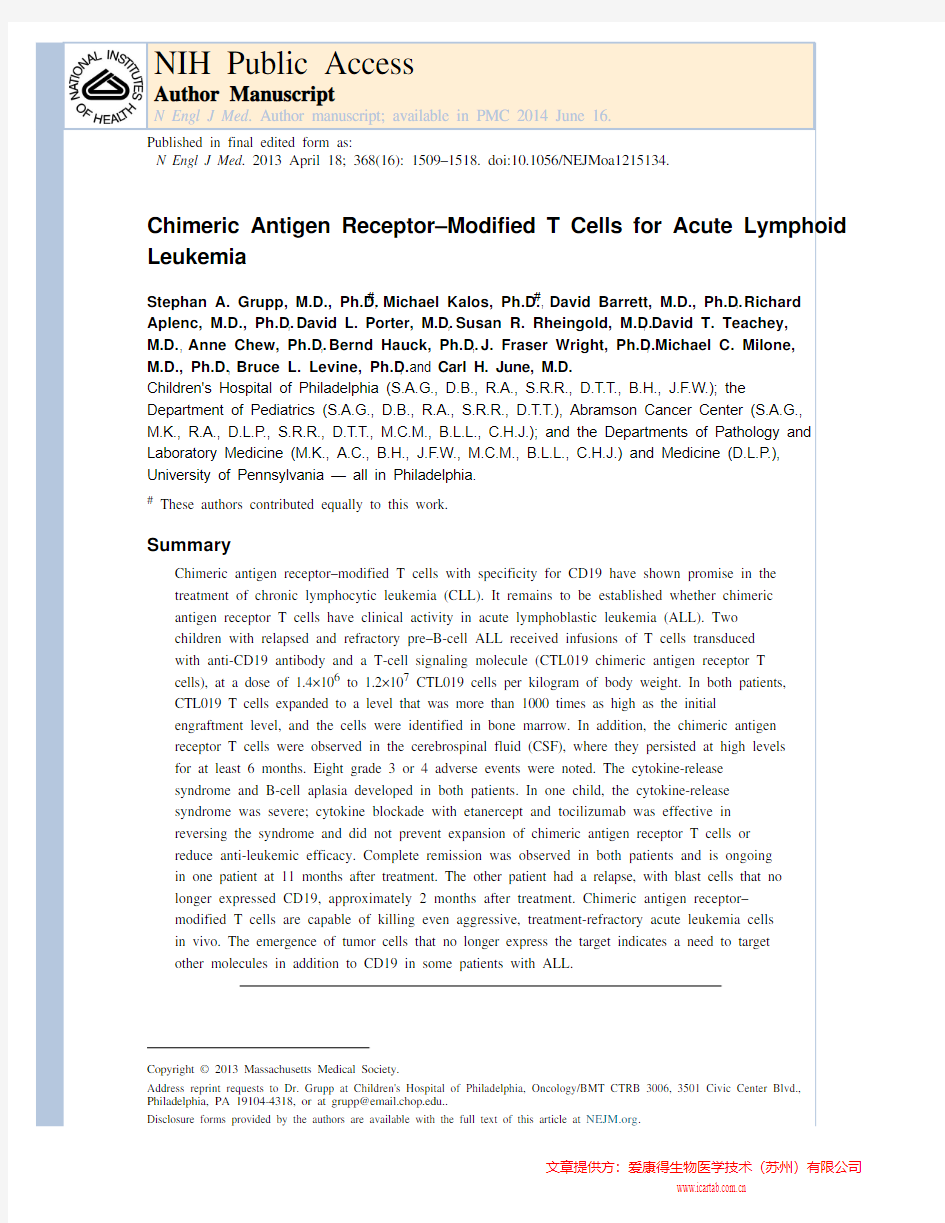
Figure 1. Clinical Responses to CTL019 Infusion in Two Children with Relapsed,
Chemotherapy-Refractory Acute Lymphoblastic Leukemia (ALL)
The two children, both of whom had CD19+ B-cell– precursor ALL, received infusions of
CTL019 cells on day 0. Panel A shows changes in serum lactate dehydrogenase (LDH)
levels and body temperature after CTL019 infusion, with the maximum temperature per 24-
hour period indicated by the circles. Patient 1 was given methylprednisolone starting on day
5 at a dose of 2 mg per kilogram of body weight per day, tapered to 0 by day 12. On the
morning of day 7, etanercept was given at a dose of 0.8 mg per kilogram. At 6 p.m. on day
7, tocilizumab was given at a dose of 8 mg per kilogram. A transient improvement in
NIH-PA Author Manuscript
NIH-PA Author Manuscript
NIH-PA Author Manuscript
pyrexia occurred after the administration of glucocorticoids on day 5, with complete
resolution of fevers occurring after the administration of cytokine-directed therapy. Panel B
shows serum levels of cytokines and inflammatory markers measured at the indicated time NIH-PA Author Manuscript
points after CTL019 infusion. Cytokine values are shown with the use of a semilogarithmic
plot indicating change from baseline. Baseline values (on day 0 before infusion) in Patient 1
and Patient 2, respectively, were as follows: interleukin-1β, 0.9 and 0.2 pg per milliliter;
interleukin-6, 4.3 and 1.9 pg per milliliter; interferon-γ, 0.08 and 0.23 pg per milliliter;
tumor necrosis factor α (TNF-α), 1.5 and 0.4 pg per milliliter; interleukin-2 receptor α,
418.8 and 205.7 pg per milliliter; interleukin-2, 0.7 and 0.4 pg per milliliter; interleukin-10,
9.9 and 2.3 pg per milliliter; and interleukin-1 receptor α, 43.9 and 27.9 pg per milliliter.
Pronounced elevations in a number of cytokines and cytokine receptors developed in both
patients, including soluble interleukin-1 receptor α; interleukin-2 receptor; interleukin-2, 6,
and 10; TNF-α; and inter fer on-γ. Panel C shows changes in the circulating absolute
neutrophil count (ANC), absolute lymphocyte count (ALC), and white-cell count. The
increase in the ALC was primarily from activated CTL019 T lymphocytes. NIH-PA Author Manuscript
NIH-PA Author Manuscript
Figure 2. Expansion and Visualization of CTL019 Cells in Peripheral Blood, Bone Marrow, and
Cerebrospinal Fluid (CSF)
Panel A shows the results of flow-cytometric analysis of peripheral blood stained with
antibodies to detect CD3 and the anti-CD19 chimeric antigen receptor. Both the x and y axes
are log 10 scales. Depicted is the percentage of CD3 cells expressing the chimeric antigen
receptor in Patients 1 and 2. Panel B shows the presence of CTL019 T cells in peripheral
blood, bone marrow, and CSF as assessed by means of a quantitative real-time polymerase-
chain-reaction (PCR) assay. Genomic DNA was isolated from samples of whole blood, bone
marrow aspirate, and CSF collected at serial time points before and after CTL019 infusion.
NIH-PA Author Manuscript
NIH-PA Author Manuscript
NIH-PA Author Manuscript
The 1% marking line represents the number of detected transgene copies that would be
expected if 1% of the total cells in the sample contained a single integration of the chimeric
antigen receptor transgene. Panel C shows flow-cyto-metric detection of CTL019 cells in NIH-PA Author Manuscript
CSF from Patients 1 and 2. FMO denotes fluorescence minus one. Both the x and y axes are
log10 scales. Panel D shows activated large granular lymphocytes in Wright-stained smears
of the peripheral blood and cytospin preparations of CSF from Patient 2. NIH-PA Author Manuscript
NIH-PA Author Manuscript
Figure 3. CD19 Expression at Baseline and at the Time of Relapse in Patient 2Bone marrow samples were obtained from Patient 2 before CTL019 infusion and at the time of relapse, 2 months later. Mononuclear cells isolated from marrow samples were stained for CD45, CD34, and CD19 and analyzed on an Accuri C6 flow cytometer. After a gating on live cells, the blast gate (CD45+ side scatter [SSC] low) was subgated on CD34+ cells, and histograms were generated for CD19 expression. The vertical line in each graph represents the threshold for the same gating on isotype controls. Pretherapy blasts (Panel A) have a range of distribution of CD19, with a small population of very dim-staining cells seen as the tail at the left of the histogram at 102 on the x axis. The numbers on the x axis are arbitrary fluorescence intensity units. The sample obtained at the time of relapse (Panel B) does not have any CD19+ blasts. Analysis of CD19 expression on the pretreatment blast population revealed a small population of CD19+dim or CD19– cells. The mean fluorescence intensity
of this small population of cells was 187 units, which is similar to that of the anti-CD19–
stained blast cells at relapse, 201 units. The pretherapy marrow sample was hypocellular,
with 10% blasts, and the marrow sample at relapse was normocellular, with 68% blasts,
accounting for differences in the number of events (cells) available for acquisition.
NIH-PA Author Manuscript
NIH-PA Author Manuscript
NIH-PA Author Manuscript
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Table 1
Induction of Molecular Remission in the Blood and Bone Marrow of the Patients.*
Patient and Tissue No. of Cell
Equivalents
Analyzed
Total Reads of
T-Cell
Receptor β
Total Reads
of IGH
Total
Unique
Reads of
IGH
Dominant Clone Reads Tumor Clone
Frequency %
Patient 1
Blood
Day –1111,340525,717189618597.88
Day 23218,2101,651,1290000
Day 87288,1521,416,3780000
Day 180420,5711,276,0986200 Marrow
Day –1317,460348,68759,79131859,77499.97
Day 23362,8191,712,5073723389.19
Day 87645,333425,12810110100.00
Day 180952,381800,67045700 Patient 2
Blood
Day –1152,5841,873,11638,1705230,42579.71
Day 23417,3711,462,9119251819.60 Marrow
Day –1158,7302,417,99268,3686550,88774.43
Day 23305,0671,978,6001,4141194666.90
Day 60916,571NA530,833206363,73668.90
*
Molecular analysis of minimal residual disease was performed as described in the Supplementary Appendix on DNA isolated from whole blood or bone marrow. Day –1 indicates the day before infusion of CTL019 cells. NA denotes not available.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Table 2
Grade 3 or 4 Adverse Events.*
Event Grade Description Duration Patient 1
Febrile neutropenia3Peak temperature of 40.7°C; event resolved on day 7 (within hours after
administration of tocilizumab)
7 days
Hypotension4Shock requiring pressor support; by day 7, only pressor support was tapered
dose of dobutamine; by day 12, no pressors required
4 days at grade 4 Acute vascular leak syndrome4Life-threatening; pressor support or ventilatory support required 4 days at grade 4
Acute respiratory distress
syndrome
4Intubation required; chest radiograph clear on day 812 days Patient 2
Febrile neutropenia3Peak temperature of 40.3°C; event resolved on day 6 6 days Encephalopathy3Parents reported confusion; MRI scan was normal 3 days Elevated AST4Peak AST value: 1060 U/liter (grade 4) 1 day at grade 4 Elevated ALT4Peak ALT value: 748 U/liter (grade 4) 1 day at grade 4
*
Adverse events were graded according to the Common Terminology Criteria for Adverse Events, version 3.0. ALT denotes alanine aminotransferase, AST aspartate aminotransferase, and MRI magnetic resonance imaging.
单克隆抗体的制备及应用
单克隆抗体的制备及应用 单克隆抗体是由淋巴细胞杂交瘤产生的、只针对复合抗原分子上某一单个抗原决定簇。单克隆抗体技术(monoclonal antibody technique):一种免疫学技术,将产生抗体的单个B淋巴细胞同骨髓肿瘤细胞杂交,获得既能产生抗体,又能无限增殖的杂种细胞,并以此生产抗体。是仅由一种类型的细胞制造出来的抗体,对应于多克隆抗体、多株抗体——由多种类型的细胞制造出来的一种抗体。 1 单克隆抗体的优点与局限性: 单克隆抗体的优点:(1)杂交瘤可以在体外“永久”地存活并传代,只要不发生细胞株的基因突变,就可以不断地生产高特异性、高均一性的抗体。(2)可以用相对不纯的抗原,获得大量高度特异的、均一的抗体。(3)由于可能得到“无限量”的均一性抗体,所以适用于以标记抗体为特点的免疫学分析方法,如IRMA和ELISA等。(4)由于单克隆抗体的高特异性和单一生物学功能,可用于体内的放射免疫显像和免疫导向治疗。 总体来说,即:高特异性、高纯度、重复性好、敏感性强、成本低和可大量生产等。 单克隆抗体的局限性:(1)单克隆抗体固有的亲和性和局限的生物活性限制了它的应用范围。由于单克隆抗体不能进行沉淀和凝集反应,所以很多检测方法不能用单克隆抗体完成。 (2)单克隆抗体的反应强度不如多克隆抗体。(3)制备技术复杂,而且费时费工,所以单克隆抗体的价格也较高。 2 单克隆抗体的制备: 单克隆抗体的制备原理:应用细胞杂交技术使骨髓瘤细胞与免疫的淋巴细胞二者合二为一,得到杂种的骨髓瘤细胞。这种杂种细胞继承两种亲代细胞的特性,它既具有B淋巴细胞合成专一抗体的特性,也有骨髓瘤细胞能在体外培养增殖永存的特性,用这种来源于单个融合细胞培养增殖的细胞群,可制备抗一种抗原决定簇的特异单克隆抗体。 单克隆抗体的制备过程:抗原准备、动物的选择与免疫、细胞融合、选择杂交瘤细胞及抗体检测、杂交瘤的克隆化、杂交瘤细胞的冻存与复苏、单克隆抗体的纯化等步骤。 抗原准备 抗原,是指能够刺激机体产生(特异性)免疫应答,并能与免疫应答产物抗体和致敏淋巴细胞在体外结合,发生免疫效应(特异性反应)的物质。抗原的基本特性有两种,一是诱导免疫应答的能力,也就是免疫原性,二是与免疫应答的产物发生反应,也就是抗原性。很多物质都可以成为抗原,抗原的具体分类可以参见抗原,在进行单克隆抗体制备过程中,很多物质都可以成为抗原,在常规的科研实验中,科研者经常选用每只小鼠/大鼠每次注射10~50ug 重组蛋白、偶联多肽、偶联小分子等作为抗原产生特异性的单克隆抗体。 动物的选择与免疫
单克隆抗体制备的基本原理
单克隆抗体制备的基本原理 一、单克隆抗体的概念 抗体(antibody)是机体在抗原刺激下产生的能与该抗原特异性结合的免疫球蛋白。常规的抗体制备是通过动物免疫并采集抗血清的方法产生的,因而抗血清通常含有针对其他无关抗原的抗体和血清中其他蛋白质成分。一般的抗原分子大多含有多个不同的抗原决定簇,所以常规抗体也是针对多个不同抗原决定簇抗体的混合物。即使是针对同一抗原决定簇的常规血清抗体,仍是由不同B细胞克隆产生的异质的抗体组成。因而,常规血清抗体又称多克隆抗体(polyclonal antibody),简称多抗。由于常规抗体的多克隆性质,加之不同批次的抗体制剂质量差异很大,使它在免疫化学试验等使用中带来许多麻烦。因此,制备针对预定抗原的特异性均质的且能保证无限量供应的抗体是免疫化学家长期梦寐以求的目标。随着杂交瘤技术的诞生,这一目标得以实现。 1975年,Kohler和Milstein建立了淋巴细胞杂交瘤技术,他们把用预定抗原免疫的小鼠脾细胞与能在体外培养中无限制生长的骨髓瘤 细胞融合,形成B细胞杂交瘤。这种杂交瘤细胞具有双亲细胞的特征,既像骨髓瘤细胞一样在体外培养中能无限地快速增殖且永生不死,又能像脾淋巴细胞那样合成和分泌特异性抗体。通过克隆化可得到来自单个杂交瘤细胞的单克隆系,即杂交瘤细胞系,它所产生的抗体是针
对同一抗原决定簇的高度同质的抗体,即所谓单克隆抗体(monoclonal antibody,McAb),简称单抗。 与多抗相比,单抗纯度高,专一性强、重复性好、且能持续地无限量供应。单抗技术的问世,不仅带来了免疫学领域里的一次**,而且它在生物医学科学的各个领域获得极广泛的应用,促进了众多学科的发展。 德国科学家柯勒(Georges Ko1er)和英国科学家米尔斯坦(Cesar Milstein)两人由此杰出贡献而荣获1984年度诺贝尔生理学和医学奖。 二、杂交瘤技术 (一)杂交瘤技术的诞生 淋巴细胞杂交瘤技术的诞生是几十年来免疫学在理论和技术两方面 发展的必然结果,抗体生成的克隆选择学说、抗体基因的研究、抗体结构与生物合成以及其多样性产生机制的揭示等,为杂交瘤技术提供了必要理论基础,同时,骨髓瘤细胞的体外培养、细胞融合与杂交细胞的筛选等提供了技术贮备。1975年8月7日,Kohler和Milstein 在英国《自然》杂志上发表了题为“分泌具有预定特异性抗体的融合细胞的持续培养”(Continuous cultures of fused cells secreting antibody of
KLF转录因子抑制轴突再生的分子机制
KLF转录因子抑制轴突再生的分子机制 转录因子(KLFs)的Kruppel-样家族的分子机制在增殖细胞中的研究比在有丝分裂后细胞中的研究更集中,如神经元。来自美国加州大学圣地亚哥分校Jeffrey L. Goldberg 教授所在团队最近发现,KLFs具有调节中枢神经系统神经元,包括视网膜神经节细胞,海马和皮层神经元内在细胞轴突生长的能力。至少有15/17 的KLF家族成员可在神经元中表达,其中至少有5种结构独特的亚科,这对决定了这一复杂的家族因子如何在神经元中调节轴突生长和再生的复杂遗传程序是很重要的。通过细节化神经系统中KLF家族的分子机制,包括结合配体和靶基因,并比较它们在神经系统之外定义的机制,我们可以更好地理解KLFs如何调控神经轴突生长和轴突再生。相关研究内容发表在2014年8月第15期《中国神经再生研究(英文版)》杂志上。 Article: “Molecular mechanisms of the suppression of axon regeneration by KLF transcription factors" by Akintomide Apara1, Jeffrey L. Goldberg2 (1 University of Miami Miller School of Medicine, Miami, FL, USA; 2 Shiley Eye Center, University of California San Diego, La Jolla, CA, USA) Apara A, Goldberg JL. Molecular mechanisms of the suppression of axon regeneration by KLF transcription factors. Neural Regen Res. 2014;9(15):1418-1421. 欲获更多资讯:Neural Regen Res
单克隆抗体制备中筛选杂交瘤细胞的原理
单克隆抗体制备过程中筛选杂交瘤细胞的原理和方法单克隆抗体制备过程中,有两次筛选过程,第一次是选出杂交瘤细胞(用选择培养基),第二次是进一步选出能产生我们需要的抗体的杂交瘤细胞。 第一次筛选的原理和方法: 细胞融合后,杂交瘤细胞的选择性培养是第一次筛选的关键。普遍采用的HAT选择性培养液是在普通的动物细胞培养液中家次黄嘌呤、氨基蝶呤和胸腺嘧啶核苷酸。其一居室细胞中的DNA合成油两条途径: 一条途径是生物合成途径(“D途径”),即由氨基酸及其其他小分子化合物合成氨基酸,为DNA分子的合成提供原料。再此合成过程中,叶酸作为重要的辅酶参与这一过程,而HAT培养液中氨基蝶呤是一种叶酸的拮抗物,可以阻断DNA合成的D途径。 另一条途径是应急途径(“S途径”),她是利用次黄嘌呤——鸟嘌呤磷酸核苷转移酶和胸腺嘧啶核苷激酶催化次黄嘌呤和胸腺嘧啶生成相应的核苷酸,两种酶缺一不可。 因此,在HAT培养液中,未融合的效应B 细胞核两个效应B细胞融合的D途径被氨基蝶呤阻断,随S途径正常,但因缺乏在体外培养液中增殖的能力,一般10天左右会死亡。对于骨髓瘤细胞以及自身融合细胞而言,由于通常采用的骨髓瘤细胞是次黄嘌呤-鸟嘌呤磷酸核苷转移酶缺陷型细胞,因此自身没有S途径,且D途径又被氨基蝶呤阻断,所有在HAT培养液中也不能增殖而很快死亡。只有骨髓瘤细胞与效应B细胞相互融合形成的杂交瘤细胞,既具有效应B细胞的S途径,又具有骨髓瘤细胞在体外培养液中长期增殖的特性,因此能在HAT培养液中选择性存活下来,并不断增殖。 第二次筛选的原理和方法: 在单克隆抗体的生产过程中,由于效应B细胞的特异性是不同的,经HAT培养液第一次筛选出的杂交瘤细胞产生的抗体存在差异,必须对杂交瘤细胞进行第二次筛选,
单克隆抗体在肿瘤治疗中的应用
单克隆抗体在肿瘤治疗中的应用 抗体分子是生物学及医学领域中用途最为广泛的蛋白质分子。利用传统的免疫方法或通过细胞工程和基因工程技术制备的抗肿瘤特异性抗原、肿瘤相关抗原、独特型决定簇、某些细胞因子受体、激素及一些癌基因产物的多克隆抗体、单克隆抗体或基因工程抗体等使肿瘤的被动免疫治疗发生了改观。人们可以用单抗单独应用于肿瘤治疗,也可以以单抗为特异性载体而将与其偶联的放射性核素、抗癌药物、毒素、酶和其他类型生物制剂“携运”至肿瘤部位,发挥相应的抗瘤效应,这种免疫偶联物亦称为“生物导弹”。 人们最初期望用类似于抗感染的被动免疫方法来治疗肿瘤,即用特异性的同种或异种抗血清或患同类肿瘤“痊愈”病人的血清注射给肿瘤病人。由于人类肿瘤细胞抗源性、肿瘤细胞异质性等诸多理论上的问题未能解决,因而要获取特异性强且效价高的抗肿瘤抗血清很不现实。直到20世纪70年代中期B 淋巴细胞杂交瘤技术的建立,人类在这领域的研究才向前迈进一大步。B淋巴细胞与鼠的骨髓瘤细胞融合,在选择性培养基的条件下,筛选出杂交瘤细胞,筛选出的杂交瘤细胞继承了其亲代细胞的性质,既可分泌抗体,又能无限传代。由特异抗原致敏的某个B细胞克隆所产生的抗体即为单克隆抗体。这种由杂交瘤技术制备的单抗是杂交瘤细胞所分泌的抗体,其质地均一,纯度高,效价高,且能重复大量生产。由于单克隆抗体特异性高,能在多种抗原中识别特异性抗原决定簇,已帮助人类鉴定出多种肿瘤相关抗原,但某种肿瘤是否存在特异性抗原至今未获普遍认同。 目前认为单抗的作用机制有阻断作用、信号传导作用以及靶向作用等三种作用机制:11阻断作用 现用于临床的大部分未偶联单抗主要用于自身免疫和免疫抑制,是通过阻断和调节作用完成的。几乎在所有的单抗应用中,通常都是通过阻断免疫系统的一种重要的胞浆或受体-配体相互作用而实现的。另一种相类似的阻断活性可能存在于单抗的抗病毒感染中,通过阻断和抵消病原体的进入和扩散表现出对机体的防御功能,短期给予单抗后可取得长期疗效。21信号传导作用许多抗癌单抗是通过恢复效应因子,直接启动信号机制而获得细胞毒效应的。在抗-Id的临床试验中,B细胞受体(BCR)与抗体的交联导致正常细胞和肿瘤细胞的生长受抑制和凋亡。对trastuaumab而言,单抗结合可诱导一系列在肿瘤生长控制中起作用的信号传递,该抗原是生长因子受体家族的一个成员,能提供重要的有丝分裂信号,其单抗似乎能阻断与促进肿瘤生长有关的重要的配体-受体相互作用。31靶向作用单抗靶向肿瘤细胞的首要目的是产生肿瘤特异性反应物,然后由免疫系统中的活化因子将其消灭,如早期抗-Id单抗在淋巴瘤中的应用。研究表明:利用单抗与化学药物、放射性核素以及毒素形成的偶联物具有对肿瘤细胞的选择性杀伤作用,同时具有更高的疗效,并且对耐药性肿瘤细胞也有杀伤作用。这些研究结果为应用于肿瘤治疗的可行性提供了重要依据。单克隆抗体用于抗肿瘤治疗有2种基本的方式,一是单抗的单独应用,二是
1单克隆抗体药物----科普知识
1 单克隆抗体药物----科普知识 单克隆抗体药物 2009-10-19 15:47 1986年,美国FDA批准了第一个单克隆抗体药物上市,距今已经整整20年了。截止到现在,全世界共有21个治疗用抗体药物被批准上市,实现300亿美元的销售额,在国际,也在国内形成了抗体药物开发热潮。巨大的市场前景和现存的技术问题及壁垒并存的现实不可避免地引发抗体药物新一轮技术革命。而其结果又将毫无疑问地改变抗体药物的市场格局。抗体药物的研究开发能否真能成为中国生物技术药物开启国际市场大门的新钥匙?什么是我们首选的切入点,又如何形成我们自己的特色和竞争优势?回顾国际抗体药物20年风雨飘摇的发展经历,总结其中的经验教训无疑会给我们一些有益的启示。 1986年,美国FDA批准上市了第一个抗体药物Orthoclone,用于治疗移植物抗宿主病(GVHD),翻开了生物医药历史崭新的一页。时隔8年,美国才批准了第二个抗体药物上市。进入21世纪,抗体药物研发上市的速度明显加快。20年后的今天,全球共批准上市21个抗体药物。进入临床验证的数量也直线上升,从上个世纪80年代的70个,到90年代新增140个,以及2000年至2005年6月又增加的130个,预计2010年将再增 240个【1】,显示抗体药物研究异常活跃。目前共有150余个抗体药物正在临床评估中,其中16个已进入III期临床【2】。 抗体药物研发进展迅速及竞争激烈的主要原因是1)抗体药物具有高度特异性,是靶向治疗的基础,在这一方面远优于小分子药物;2)虽然在世界范围内20年仅仅批准上市了21个抗体药物,事实上其淘汰率仍明显低于小分子药物,临床转化率以及批准成功率都较高,以治疗癌症的抗体药物为例,其批准成功率为29%;3)抗体药物即使在专利保护到期后,由于其生产条件的复杂性,也很难受到通用名药价格的威胁;4)更为重要的是已上市的抗体药物具有很高的市场回报率,大大刺激了投资热情。目前,上市抗体药物中已盈利的有8个,其中4个已经成为年销售额10亿美元以上的“重磅弹”,5个销售总额超过30亿美元【3】。预计2005-2010年抗体药物销售的平均增长率为20%,年销售额将超过300亿美元,市场潜力巨大。 但具有讽刺意味的是,从药物经济学的角度看,抗体药物并非很好的药物候选者。首先,单克隆抗体是大分子糖蛋白,结构复杂、不利储存、不能口服、进入体内5-7天才能到达靶位置。其次,抗体药物研发费用较高,达10-18亿美元,高于小分子药物平均研发费的9亿美元。第三,目前抗体药物的单剂用量大,药物的质量标准高,生产成本高昂,导致价格昂贵,以致被喻为“经济负作用”。以治疗肿瘤的抗体药物Avastin为例,单个病人年度费用高达5万美元【4】。然而,正在形成的巨大市场是抗体药物研发的不竭驱动力。 我国在单克隆抗体技术起步非常早,80年代曾出现过研究热潮,但产业化成就还微不足道。目前,受国际抗体研发进展的影响,又出现了新一轮的“抗体热”,北京、上海、广州等纷纷成立了由研究机构、企业和投资商的联合抗体研发中心和公司。面对国际抗体药物竞争的新态势,我国抗体药物产业是否遇到了真正的机遇?我们选择的切入点是什么,又如何形成自己的特色和竞争优势?抗体药物的研究开发能否成为中国生物技术药物开启国际市场大门的新钥匙?回顾国际抗体药物20年风雨飘摇的发展经历,总结其中的经验教训无疑会给我们一些有益的启示,这是本文的主要目的。 一、上市抗体药物的发展现状 从第一个抗体药物上市至今20年内,全球共批准了21个抗体药物,其中美国18个(包括9个被欧盟
单克隆抗体制备中筛选杂交瘤细胞的原理
单克隆抗体制备中筛选杂交瘤细胞的原理 标准化管理部编码-[99968T-6889628-J68568-1689N]
单克隆抗体制备过程中筛选杂交瘤细胞的原理和方法 单克隆抗体制备过程中,有两次筛选过程,第一次是选出杂交瘤细胞(用选择培养基),第二次是进一步选出能产生我们需要的抗体的杂交瘤细胞。 第一次筛选的原理和方法: 细胞融合后,杂交瘤细胞的选择性培养是第一次筛选的关键。普遍采用的HAT选择性培养液是在普通的动物细胞培养液中家次黄嘌呤、氨基蝶呤和胸腺嘧啶核苷酸。其一居室细胞中的DNA合成油两条途径: 一条途径是生物合成途径(“D途径”),即由氨基酸及其其他小分子化合物合成氨基酸,为DNA分子的合成提供原料。再此合成过程中,叶酸作为重要的辅酶参与这一过程,而HAT培养液中氨基蝶呤是一种叶酸的拮抗物,可以阻断DNA合成的D途径。 另一条途径是应急途径(“S途径”),她是利用次黄嘌呤——鸟嘌呤磷酸核苷转移酶和胸腺嘧啶核苷激酶催化次黄嘌呤和胸腺嘧啶生成相应的核苷酸,两种酶缺一不可。 因此,在HAT培养液中,未融合的效应B细胞核两个效应B细胞融合的D途径被氨基蝶呤阻断,随S途径正常,但因缺乏在体外培养液中增殖的能力,一般10天左右会死亡。对于骨髓瘤细胞以及自身融合细胞而言,由于通常采用的骨髓瘤细胞是次黄嘌呤-鸟嘌呤磷酸核苷转移酶缺陷型细胞,因此自身没有S途径,且D途径又被氨基蝶呤阻断,所有在HAT培养液中也不能增殖而很快死亡。只有骨髓瘤细胞与效应B细胞相互融合形成的杂交瘤细胞,既具有效应B细胞的S途径,又具有骨髓瘤细胞在体外培养液中长期增殖的特性,因此能在HAT培养液中选择性存活下来,并不断增殖。 第二次筛选的原理和方法: 在单克隆抗体的生产过程中,由于效应B细胞的特异性是不同的,经HAT培养液第一次筛选出的杂交瘤细胞产生的抗体存在差异,必须对杂交瘤细胞进行第二次筛选,选出能产生特定抗体的杂交瘤细胞。二次筛选通常采用有限稀释克隆细胞的方法,将杂交瘤细胞多倍稀释,接种在多孔的细胞培养板上,是每孔细胞不超过一个,通过培养让其增殖,然后检测各孔上清液中的细胞分泌的抗体,上清液可与特定抗原结合的培养孔为阳性孔。阳性孔中的细胞还不能保证是来自单个细胞,继续进行有限
单克隆抗体的制备技术和纯化及鉴定
单克隆抗体的制备技术和纯化及鉴定 一、实验目的: 单克隆抗体制备是细胞免疫学的一个重要里程碑,它涵盖了细胞培养、细胞融合、免疫动物和抗体效价检测等各个方面内容。了解单克隆抗体制备的原理、主要步骤和方法。 二、实验原理: 骨髓瘤细胞在体外培养能大量无限增殖,但不能分泌特异性抗体;而抗原免疫的B淋巴细胞能产生特异性抗体,但在体外不能无限增殖。将免疫脾细胞与骨髓瘤细胞融合后形成的杂交瘤细胞,继承了两个亲代细胞的特性,既具有骨髓瘤细胞能无限制增殖的特性,又具有免疫B细胞合成和分泌特异性抗体的能力。经在HAT培养基[含有次黄嘌呤(H)、氨基喋呤(A)和胸腺嘧啶核苷(T)]中进行选择性培养,未融合的脾细胞因不能在体外长期存活而死亡;未融合的骨髓瘤细胞合成DNA的主要途径被培养基中的氨基蝶呤阻断,又因缺乏次黄嘌呤-鸟嘌呤-磷酸核糖转移酶(HGPRT),不能利用培养基中的次黄嘌呤完成DNA 的合成过程而死亡。只有融合的杂交瘤细胞由于从脾细胞获得了次黄嘌呤-鸟嘌呤-磷酸核糖转移酶,因此能在HAT培养基中存活和增殖。经过克隆选择,可筛选出能产生特异性单克隆抗体的杂交瘤细胞,在体内或体外培养,即可无限制地大量制备单克隆抗体。 三、试剂与器材: 细胞培养板、解剖器械、平皿、酶标仪、加样器、细胞计数板、CO2培养箱、倒置显微镜等。 四、操作方法: 1、抗原制备; 一般而言,抗原的纯度不很重要,特别是免疫原性较强的抗原。 A.可溶性抗原(蛋白质)以1mg/ml~5mg/ml的溶液加等量的弗氏完全佐剂乳化,分多点小鼠皮下注射,总量为~,间隔3~5周再同样注射一次,
10天后,断尾取血一滴,测抗体效价,选滴度高的小鼠做融合试验。一个月后可以经静脉(尾静脉)给予无佐剂抗原~,3~4天后,杀死小鼠取脾做融合用。 B. 颗粒性抗原如抗原来源方便,可以不加佐剂而增加免疫次数,缩短间隔时间。例如用羊红血球免疫小白鼠,以1%浓度每只皮下注射0.2ml,每周2次,共免疫5~8次,取脾前3天,再免疫一次即可。有人认为最后一次免疫剂量要大,大到近于免疫耐受的程度更好。 2、免疫动物; 目前应用最广的是小白鼠和大白鼠,尤以小白鼠为好。就品系而言以Balb/ c小白鼠应用最广,因为所有的小白鼠骨髓瘤系均从Balb/c小白鼠系诱导出来。Balb/c系小白鼠必须用纯系的,雌雄均可,以8~12周龄为宜。 大白鼠也可,能产生较多量的单克隆抗体。现在已经在小鼠杂交瘤的基础上,发展了小鼠-大鼠,小鼠-人以及人-人杂交瘤技术。 免疫程序、剂量和方法是关系到是否能得到所需要的单克隆抗体的关键之一。 正常小鼠脾脏含有能产生各种不同抗体的B淋巴细胞,一只纯种小白鼠估计能产生×107~×107种不同的抗体。因此一只正常的小白鼠的脾细胞与小鼠骨髓瘤融合,只能有千万分之一的机会获得某一种特定抗体。所以为了提高得到某种杂交瘤的机会,必须加强免疫,使产生特异性抗体的B淋巴细胞大量增加。 B淋巴细胞的不同发育阶段对获得阳性杂交瘤也有很大影响。有人认为处在转化时期的B淋巴细胞可能更易于融合,而免疫以后7~8天,虽然是抗体产生的高峰时期,但形成有活力的杂交瘤细胞的可能反而减少。故一般认为加强免疫后的第三天应杀鼠取脾做细胞融合。 3、免疫脾细胞和骨髓瘤细胞的制备; 脾细胞制备 (1) 免疫过的血清抗体滴度高的Balb/c鼠,拉颈或用CO2处死小白鼠。 (2) 将小鼠放于70%酒精中浸泡消毒,取出固定于板上,在无菌条件下取脾。
单克隆抗体制备与应用
单克隆抗体制备与应用 姓名:王志豪学号:10073485 班级:工优070 关键词:单克隆抗体,人抗体,杂交瘤细胞 摘要:1975年德国学者Kohler和英国学者Milstein成功地将骨髓瘤细胞和产生抗体的B淋巴细胞融合为杂交瘤细胞,其分泌的抗体是由识别一种抗原决定簇 的细胞克隆所产生的均一性抗体,称之为单克隆抗体。从鼠源单抗之后,单抗历经了鼠源性抗体、嵌合抗体、人源化抗体、人源性抗体4个发展阶段。随着分子生物学和细胞生物学的发展,单抗理论几乎应用到生物学研究的每一个区域。 1975 年, Kohler 和Milstein 创立了杂交瘤技术制备单克隆 抗体,此后单克隆抗体迅速广泛地应用于生物学和医学的各个领域。单克隆抗体可用于分析抗原的细微结构及检验抗原抗体未知的结构 关系;生产出针对复杂生物混合物中的特定分子的抗体,可用于分离、分析及纯化该特定分子抗原;其试剂可用于临床诊断和治疗,或用于 以单抗为弹头的“生物导弹”药物等。但单克隆抗体技术自问世以来,在临床治疗方面进展缓慢,主要原因是目前单克隆抗体大多是鼠源性的,而鼠源单抗应用于人体治疗时存在诸多问题:鼠源单抗在人体中 常不能有效激活补体和Fc 受体相关的效应系统;被人体免疫系统所 识别,产生人抗鼠抗体(HAMA) 反应;且在人体循环系统中很快被清除。因此,在保持对特异抗原表位的高亲和力的基础上人源化和全人化的改造,减少异源抗体的免疫原性成为单抗研究的重点。此外,传统杂交瘤技术还存在制备周期较长,成本较高,杂交瘤细胞不稳定抗性会丢
失等缺陷。近年来,随着分子生物学技术的发展,出现了嵌合单克隆抗体和由转基因小鼠、噬菌体展示技术、核糖体展示技术及共价展示技术所制备的单克隆抗体。这些技术可有效解决传统杂交瘤技术所存在的问题,为单克隆抗体的应用提供更广阔的空间。 1994 年, 美国Cell Genesys 公司和Genpharm公司宣布转基因小鼠作为生产全人抗体的载体问世。这项技术是将人抗体基因微位点转入小鼠体内,产生能分泌人抗体的转基因小鼠。其前提是人的抗体基因片段在小鼠体内进行重排并表达,并且这些片段能与小鼠细胞的信号机制相互作用,即在抗原刺激后,这些片段可被选择、表达并活化B 细胞分泌人抗体。这些转基因小鼠的不足之处在于转移基因片段较小,仅30kb 左右,因此这种抗体库在面对抗原多样性时,其抗体应答显得单薄而不足。此后,Green 等人利用基因打靶技术将编码人抗体轻重链的基因片段大约18Mb 的DNA 全部转到自身抗体基因位点已被灭活的小鼠基因组中,再经过繁育筛选,建立了稳定的转基因小鼠品系。这样得到的转基因小鼠对特异的抗原能产生高亲和力的人抗体。用传统的杂交瘤技术,将表达特异抗体的转基因小鼠B 细胞和骨髓瘤细胞融合,获得杂交瘤细胞系,产生人源抗体。利用转基因小鼠技术已获得了一系列抗IL8 、TNFα以及EGFR 的人单克隆抗体,这些细胞因子在肿瘤或其他疾病中起着重要的作用,因此其单克隆抗体作为导向剂具有重要的临床治疗意义。目前生产的单抗大多是鼠源性的,但其在临床应用方面还存在着很大的弊端,主要是鼠源单抗与NK 等免疫细胞表面Fc 段受体亲和力弱,产生的抗体依赖性细胞介导的细胞毒
单克隆抗体制备过程中经过两次筛选
单克隆抗体制备过程中经过两次筛选 单克隆抗体制备过程中,总共有两次筛选,第一次筛选出杂交瘤细胞,第二次筛选出能产生特异性抗体的杂交瘤细胞,两次筛选的原理和方法是不相同的。 第一次筛选的原理与方法:细胞融合后,杂交瘤细胞的选择性培养是第一次筛选的关键。普遍采用的HAT选择性培养液是在普通的动物细胞培养液中加入次黄嘌呤(H)、氨基喋呤(A)和胸腺嘧啶核苷酸(T)。其依据是细胞中的DNA合成有两条途径:一条途径是生物合成途径(“D途径”),即由氨基酸及其他小分子化合物合成核苷酸,为DNA分子的合成提供原料。在此合成过程中,叶酸作为重要的辅酶参与这一过程,而HAT培养液中氨基喋呤是一种叶酸的拮抗物,可以阻断DNA合成的“D途径”。另一条途径是应急途径或补救途径(“S途径”),它是利用次黄嘌呤—鸟嘌呤磷酸核苷转移酶(HGPRT)和胸腺嘧啶核苷激酶(TK)催化次黄嘌呤和胸腺嘧啶核苷生成相应的核苷酸,两种酶缺一不可。因此,在HAT培养液中,未融合的效应B细胞和两个效应B细胞融合的“D途径”被氨基喋呤阻断,虽“S途径”正常,但因缺乏在体外培养液中增殖的能力,一般10d左右会死亡。对于骨髓瘤细胞以及自身融合细胞而言,由于通常采用的骨髓瘤细胞是次黄嘌呤—鸟嘌呤磷酸核苷转移酶缺陷型(HGPRT)细胞,因此自身没有“S途径”,且“D途径”又被氨基喋呤阻断,所以在HA T培养液中也不能增殖而很快死亡。惟有骨髓瘤细胞与效应B细胞相互融合形成的杂交瘤细胞,既具有效应B细胞的“S途径”,又具有骨髓瘤细胞在体外培养液中长期增殖的特性,因此能在HA T培养液中选择性存活下来,并不断增殖。 第二次筛选的原理和方法:在实际免疫过程中,由于采用连续注射抗原的方法,且一种抗原决定簇刺激机体形成相对应的一种效应B淋巴细胞,因此,从小鼠脾脏中取出的效应B淋巴细胞的特异性是不同的,经HA T培养液筛选的杂交瘤细胞特异性也存在差异,所以必须从杂交瘤细胞群中筛选出能产生针对某一预定抗原快定簇的特异性杂交瘤细胞。通常采用有限稀释克隆细胞的方法,将杂交瘤细胞多倍稀释,接种在多孔的细胞培养板上,使每一孔含一个或几个杂交瘤细胞(理论上30%的孔中细胞数为0时,才能保证有些孔中是单个细胞),再由这些单细胞克隆生长,最终选出分泌预定特异抗体的杂交细胞株进行扩大培养。因此,单克隆抗体制备过程中,两次筛选的原理和方法是不相同的。 单克隆抗体制备的基本原理与过程 原理: B淋巴细胞在抗原的刺激下,能够分化、增殖形成具有针对这种抗原分泌特异性抗体的能力。B细胞的这种能力和量是有限的,不可能持续分化增殖下去,因此产生免疫球蛋白的能力也是极其微小的。将这种B细胞与非分泌型的骨髓瘤细胞融合形成杂交瘤细胞,再进一步克隆化,这种克隆化的杂交瘤细胞是既具有瘤的无限生长的能力,又具有产生特异性抗体的B淋巴细胞的能力,将这种克隆化的杂交瘤细胞进行培养或注入小鼠体内即可获得大量的高效价、单一的特异性抗体。这种技术即称为单克隆抗体技术。 过程: 1)免疫脾细胞的制备制备单克隆抗体的动物多采用纯系Balb/c小鼠。免疫的方法取决于所用抗原的性质。免疫方法同一般血清的制备,也可采用脾内直接免疫法。 2)骨髓瘤细胞的培养与筛选在融合前,骨髓瘤细胞应经过含8-AG的培养基筛选,防止细胞发生突变恢复HGPRT 的活性(恢复HGPRT的活性的细胞不能在含8-AG的培养基中存活)。骨髓瘤细胞用10%小牛血清的培养液在细胞培养瓶中培养,融合前24h换液一次,使骨髓瘤细胞处于对数生长期。 3)细胞融合的关键: 1技术上的误差常常导致融合的失败。例如,供者淋巴细胞没有查到免疫应答。这必然要失败的。 2融合试验最大的失败原因是污染,融合成功的关键是提供一个干净的环境,以及适宜的无菌操作技术。 4)阳性克隆的筛选应尽早进行。通常在融合后10天作第一次检测,过早容易出现假阳性。检测方法应灵敏、准确、而且简便快速。具体应用的方法应根据抗原的性质,以及所需单克隆抗体的功能进行选择。常用的方法有RIA法、ELISA法和免疫荧光法等。其中ELISA法最简便,RIA法最准确。阳性克隆的筛选应进行多次,均阳性时才确定为阳性克隆进行扩增。 5)克隆化克隆化的目的是为了获得单一细胞系的群体。克隆化应尽早进行并反复筛选。这是因为初期的杂交瘤细胞是不稳定的,有丢失染色体的倾向。反复克隆化后可获得稳定的杂交瘤细胞株。克隆化的方法很多,而最常用的是有限稀释法。 (1)显微操作法:在显微镜下取单细胞,然后进行单细胞培养。这种方法操作复杂,效率低,故不常用。 (2)有限稀释法:将对数生长期的杂交瘤细胞用培养液作一定的稀释后,按每孔1个细胞接种在培养皿中,细胞增值后成为单克隆细胞系。第一次克隆化时加一定量的饲养细胞。由于第一次克隆化生长的细胞不能保证单克隆化,所以为获得稳定的单克隆细胞株需经2~3次的再克隆才成。应该注意的是,每次克隆化过程中所有有意义的细胞都
单克隆抗体的制备流程
单克隆抗体的制备流程 (一)动物的选择与免疫 1.动物的选择纯种BALB/C小鼠,较温顺,离窝的活动范围小,体弱,食量及排污较小,一般环境洁净的实验室均能饲养成活。目前开展杂交瘤技术的实验室多选用纯种BALA/C小鼠。 2.免疫方案选择合适的免疫方案对于细胞融合杂交的成功,获得高质量的McAb 至关重要。一般在融合前两个月左右根据确立免疫方案开始初次免疫,免疫方案应根据抗原的特性不同而定。 (1)可溶性抗原免疫原性较弱,一般要加佐剂,半抗原应先制备免疫原,再加佐 剂。常用佐剂:福氏完全佐剂、福氏不完全佐剂。 初次免疫抗原1~50μg加福氏完全佐剂皮下多点注射或脾内注射(一般0.8~1ml,0.2ml/点) ↓3周后 第二次免疫剂量同上,加福氏不完全佐剂皮下或ip(腹腔内注射)(ip剂量不宜超过0.5ml) ↓3周后 第三次免疫剂量同一,不加佐剂,ip(5~7天后采血测其效价) ↓2~3周 加强免疫,剂量50~500μg为宜,ip或iv(静脉内注射) ↓3天后 取脾融合 目前,用于可溶性抗原(特别是一些弱抗原)的免疫方案也不断有所更新,如:① 将可溶性抗原颗粒化或固相化,一方面增强了抗原的免疫原性,另一方面可降低抗 原的使用量。②改变抗原注入的途径,基础免疫可直接采用脾内注射。③使用细胞 因子作为佐剂,提高机体的免疫应答水平,增强免疫细胞对抗原的反应性。 (2)颗粒抗原免疫性强,不加佐剂就可获得很好的免疫效果。以细胞性抗原为例,免疫时要求抗原量为1~2×107个细胞。 初次免疫1×107/0.5ml ip ↓2~3周后 第二次免疫1×107/0.5ml ip ↓3周后 加强免疫(融合前三天)1×107/0.5ml ip或iv ↓ 取脾融合 (二)细胞融合
单克隆抗体在肿瘤治疗中的应用
单克隆抗体在肿瘤治疗中的应用 【摘要】单克隆抗体在一段相当短的时间内成为治疗癌症的主流方法。它们的第一个用途是作为致癌受体酪氨酸激酶受体拮抗剂,但今天单克隆抗体已成为长期寻求的有效化疗药物靶向递送的载体并作为操纵抗癌免疫反应的功能的强大的工具。在临床上有更加可喜的成果,未来将有可能看到持续增长治疗性抗体和它们的衍生物的发展。 由于单克隆抗体药物专一性强、疗效显著,为抗肿瘤治疗开辟了一条新的途径,因此成为近年来研究的热点药物之一。单克隆抗体抗体是由B 淋巴细胞转化而来的浆细胞分泌的,每个B淋巴细胞株只能产生一种它专有的、针对一种特异性抗原决定簇的抗体。这种从一株单一细胞系产生的抗体就叫单克隆抗体,简称单抗。这些抗体具有相同的结构和特性。抗体与特异性表达的肿瘤细胞表面蛋白质结合,从而阻碍蛋白质的表达,起到抗肿瘤作用。抗体还可使B 淋巴细胞产生免疫反应,诱导癌细胞凋亡。早期单抗为鼠源性单抗,易被人体免疫系统识别,应用受到限制。后来采用基因工程的方法生产人源或人鼠嵌合型单抗,广泛应用于临床。 单抗药物治疗主要是利用其靶向性来干预肿瘤发生发展过程中的各个通路,或是激活宿主对肿瘤的免疫等。随着生物医学的不断发展,一定会出现具有更高靶向性的单抗药物。但是,单抗药物还存在一些尚未解决的问题,最突出的问题是如何降低单抗的免疫原性,单抗的异源性所引起的抗体反应,不但降低了单抗的效价,而且会给患者带来严重的后果。因此,对异源性单抗进行改造以及人源性单抗的研制成为单抗研究的重要方向 1.EGEG疗法 表皮生长因子受体EGFR是一种细胞表面蛋白,与多种癌症密切相关,也是癌症治疗的主要靶标。基因编码信息被翻译为特定蛋白,不过,许多蛋白必须经由翻译后程序激活,比如自身磷酸化。蛋白激活影响着许多重要的细胞过程,包括细胞增殖、分化和迁移。若EGFR 出现故障使这些过程脱离控制,就会导致癌症。然而,尽管EGFR与癌症有着密切关联,人们对EGFR的激活机制还并不完全了解。 受体酪氨酸激酶是一个细胞表面受体大家族,EGFR也是其中一员。EGFR有一个细胞外的配体结合域,和一个细胞内的激酶区域。EGFR激活是其配体EGF结合到配体结合域,诱导受体二聚化,随后二聚体的两个激酶区域相互磷酸化。因为在相对较低的浓度下,即使没有EGF诱导的二聚化,单独的激酶域在溶液中也能自激活。二聚化是指两个同样的分子聚合形成单个化合物。研究发现,除了配体EGF结合以外,EGFR激活还需要EGFR跨膜螺旋和
单克隆抗体的制备
单克隆抗体的制备 摘要:单克隆抗体技术是现代生命科学研究的重要工具,在基因和蛋白质的结构和功能研究方面有着不可或缺的作用。近年来,随着分子生物学技术的发展,出现了嵌合单克隆抗体和由转基因小鼠、噬菌体展示技术、核糖体展示技术及共价展示技术所产生的单克隆抗体。这些技术将有效解决单克隆抗体的鼠源性等问题。下面主要讲述制备单抗的实验过程。 关键词:抗体,单克隆,肿瘤,细胞融合,淋巴细胞 现代生物技术制药工业始于1971年,现已创造出35个重要治疗药物,全球大约有2500多家公司,主要产品有重组蛋白质药品、重组疫苗和诊断、治疗用的单克隆机体三大类。我国自80年代在采用现代生物技术改造传统生物技术制药产业方面已取得初步成果。但我国生物技术诊断试剂、酶工程、动植物细胞工程医药产品、现代生物技术支撑技术、后处理技术和制剂技术等方面与国外还存在差距。 1.国外现代生物技术产业发展的现状 自1971年Cetus公司成立至今,现代生物技术制药工业已走完了二十五年的路程,创造出35个重要的治疗药物,目前已在治疗癌症、多发性硬化症、贫血、发育不良,糖尿病、肝炎、心力衰竭、血友病、囊性纤维变性和一些罕见的遗传性疾病中取得良好效果。在医药工业中,传统生物技术(包括近代生物技术)已为人类提供了许多重要药品,在保障人类生命健康和推动社会进步中发挥了巨大作用;现代生物技术以其特有的高新技术又为人类提供了传统生物技术难以获得的极微量的珍贵药品。由于这一系列现代生物技术新型药物的出现,使过去无法治疗的疑难疾病得到了治疗。同时,应用现代生物技术DNA重组,细胞融合以及细胞大规模培养等现代生物技术发展和提高传统生物技术的生产水平,为抗生素、氨基酸、维生素以及基体激素等药品的生产,构建了高产新菌株,创造新工艺,提高生产能力,降低生产成本,促进生产发展。
髓鞘相关抑制因子在中枢神经系统轴突再生中的作用
髓鞘相关抑制因子在中枢神经系统轴突再生中的作用 王养华△(综述),许卫红※(审校) (福建医科大学附属第一医院脊柱外科,福州350004) 中图分类号:R651 文献标识码:A 文章编号:1006-2084(2012)09-1312-03 摘要:成熟哺乳动物中枢神经系统损伤后轴突的再生是极其有限的。中枢神经再生困难之一是其内在的髓鞘相关抑制因子(MAIs)的存在,Nogo-A蛋白、髓鞘相关糖蛋白、少突胶质细胞髓鞘糖蛋白是三个经典的MAIs。这三个分子由少突胶质细胞产生,并通过Nogo受体和配对免疫球蛋白样受体B共同的神经受体激活小GTP酶Ras同源基因家族成员(Rho),进而活化的RhoA激活Rho相关激酶抑制中枢神经系统轴突的再生。现就MAIs在中枢神经系统轴突再生中的作用予以综述,并探讨其可能的治疗措施以促进中枢神经轴突再生和功能恢复。 关键词:轴突再生;抑制因子;受体 Role of Myelin-as s oc iate d Inhibit ors in t he Cent ral Nervous System Axonal Re generation WANG Yang-hua,XU Wei-hong.(Department of Spinal Surger y,the Fir st Affiliated Hos pital of Fujian Medical Uni-ver sity,Fuzhou350004,China) Abst rac t:The r egeneration of the rear ax le axon of the central ner vous system of mature mammals is ex-tremely limited after damage.C entr al ner ve regener ation is difficult because of its inherent myelin-a ssocia ted inhibitors(MAIs).Nogo-A pr otein,my elin-associated gly copr otein,oligodendrocy tes myelin glycoprotein pro-tein are three classical MAIs.The three molecules a re all produced by oligodendrocy tes,and through the Nogo r eceptors and pair immunoglobulin-like r eceptor B a ctivate sm all GTP enzyme Ras homology g ene family m ember s(Rho),and the a ctivated RhoA a ctivates Rho r elated kina se,thus inhibites the neur ite regenera tion of the central nervous system.H ere is to make a review on the r ole of MAIs in the central ner vous system ax-onal r egeneration,explor ing possible treatments to promote the regener ation and function recov ery. Key words:Axona l r egeneration;Inhibitory factor;Receptor 人们发现抑制性因子在中枢神经系统再生过程 中发挥了重要作用。研究表明,髓鞘来源的抑制因 子可能是中枢神经抑制因素中最重要的,已经确定 的髓鞘相关抑制因子(m yelin-associated inhibitors, M AIs)包括N ogo-A蛋白、髓鞘相关糖蛋白(m yelin- a ssociated glycopr otein,M AG)和少突胶质细胞髓鞘糖 蛋白(oligodendrocytes myelin glycoprotein protein, O Mgp)[1]。现重点讨论M AIS对中枢神经的抑制作 用,特别强调Nogo-N ogo受体轴在中枢神经系统轴突 生长中的作用。 1 MAIs M AIs是中枢神经系统的髓鞘成分少突胶质细胞 表达的蛋白质。MAIs抑制体外和体内轴突的生长, M AIs包括Nogo-A蛋白、M AG、OM gp。这三者与神经 元Nogo受体1(N gR1)互相作用,也表现出了对第二轴 突生长抑制受体即配对免疫球蛋白样受体B(pair im- munoglobulin-like r eceptor B,PirB)的亲和力,它们与受 体结合后激活下游信号转导通路,抑制轴突的再生[2]。 2 Nogo-A 在中枢神经系统髓鞘的抑制成分中,Nogo-A蛋 白是其中一个最具M AIs特点的抑制因子,主要在 少突胶质细胞表达。Nogo分为3个亚型:Nogo-A、 N ogo-B和Nogo-C。Nogo-A蛋白的两个抑制部分已被 确定[3]:①Nogo-66是与神经元细胞膜上的NgR1互 相作用的66个氨基酸片段,相邻的24个氨基酸序 列,虽然本身不起抑制作用,但是可促进Nogo-66结合NgR1的亲和力。N ogo-66也可以直接与PirB结合。 ②N ogo-A蛋白的氨基-N ogo 序列通过另一个独立的机制扰乱神经功能。Nogo蛋白的另外两个Nogo亚型(N ogo-B 和N ogo-C)含有N ogo-A中抑制性的N ogo-66环,缺乏氨基-N ogo序列。N ogo-A在中枢神经系统表达,不在外周神经系统表达,这意味着N ogo-A 在中枢神经系统再生的抑制中可能占有重要地位。研究发现,脊髓损伤后Nogo-A在 神经元的表达逐渐升高,导致神经再生困难[4];而沉默Nogo基因可以介导轴突再生以促进脱髓鞘疾病的功能恢复[5]。即使是Nogo基因最小的突变在锥体束切断术后也促进了轴突的生长[6]。此外,抗Nogo-A抗体促进中枢神经系统损伤后轴突生长及功能恢复。目前最新研究抗Nogo-A抗体已经发展到脊髓损伤的临床试验阶段[7]。研究已表明,Nogo-A 先使生长锥塌陷从而在体外抑制突起生长,并在使用基因缺失的、中和抗体、体内的药物拮抗剂的哺乳类动物脊髓损伤模型中抑制轴突再生[8]。大量实验数据表明Nogo-A在体内的作用,在小鼠、大鼠、灵长类动物急性脊髓损伤模型中观察到恢复表型[9]。 3 MAG MAG属于免疫球蛋白超家族的成员,是一种细胞表面蛋白。虽然M AG同时表达于中枢神经系统和周围神经系统的神经胶质细胞,但是在周围神经系统髓鞘快速清除,而在有中枢神经系统清除较慢,伤后可能只在中枢神经系统留下M AG以抑制轴突在体内再生[10]。MAG在中枢神经系统有两个功能:维持髓鞘的完整性和抑制中枢神经系统轴突再生。MAG在体外可以明显地抑制突起的生长,引起生长锥的塌陷,抑制包括神经节细胞在内的多种神经元突起的生长,通过免疫耗竭MAG后,可明显减少髓鞘对轴突生长的抑制作用。但是,在MAG基因缺失小鼠模型中并没有观察到促进中枢神经系统髓鞘的轴突生长以及脊髓损伤小鼠模型沉默,M AG的表达
单克隆抗体的制备、纯化及鉴定
单克隆抗体的制备、纯化及鉴定 一、实验目的: 单克隆抗体制备是细胞免疫学的一个重要里程碑,它涵盖了细胞培养、细胞融合、免疫动物和抗体效价检测等各个方面内容。了解单克隆抗体制备的原理、主要步骤和方法。 二、实验原理: 骨髓瘤细胞在体外培养能大量无限增殖,但不能分泌特异性抗体;而抗原免疫的B淋巴细胞能产生特异性抗体,但在体外不能无限增殖。将免疫脾细胞与骨髓瘤细胞融合后形成的杂交瘤细胞,继承了两个亲代细胞的特性,既具有骨髓瘤细胞能无限制增殖的特性,又具有免疫B细胞合成和分泌特异性抗体的能力。经在HAT培养基[含有次黄嘌呤(H)、氨基喋呤(A)和胸腺嘧啶核苷(T)]中进行选择性培养,未融合的脾细胞因不能在体外长期存活而死亡;未融合的骨髓瘤细胞合成DNA的主要途径被培养基中的氨基蝶呤阻断,又因缺乏次黄嘌呤-鸟嘌呤-磷酸核糖转移酶(HGPRT),不能利用培养基中的次黄嘌呤完成DNA的合成过程而死亡。只有融合的杂交瘤细胞由于从脾细胞获得了次黄嘌呤-鸟嘌呤-磷酸核糖转移酶,因此能在HAT培养基中存活和增殖。经过克隆选择,可筛选出能产生特异性单克隆抗体的杂交瘤细胞,在体内或体外培养,即可无限制地大量制备单克隆抗体。 三、试剂与器材: 细胞培养板、解剖器械、平皿、酶标仪、加样器、细胞计数板、CO2培养箱、倒置显微镜等。 四、操作方法: 1、抗原制备; 一般而言,抗原的纯度不很重要,特别是免疫原性较强的抗原。 A.可溶性抗原(蛋白质)以1mg/ml~5mg/ml的溶液加等量的弗氏完全佐剂乳化,分多点小鼠皮下注射,总量为0.3ml~0.6ml,间隔3~5周再同样注射一次,10天后,断尾取血一滴,测抗体效价,选滴度高的小鼠做融合试验。