californium-252 brachytherapy combined with external-beam radiotherapy for cervical cancer long-term
顺铂英文

顺铂英文篇一:常用肿瘤化疗药物英文名及缩写常用肿瘤化疗药物英文名及缩写2013-02-07 14:29:43篇二:常见抗肿瘤药物中英文对照# AAclacinomycin ACLA 阿克拉霉素 Alemtuznmab 阿来组单抗, 抗CD52嵌合抗体All-tra retinoic acid, ATRA, RA 全反式维甲酸, 维A酸Aminoglutethimide AG 氨基导眠能, 氨鲁米特, 氨苯哌酮Anastrozole, Arimidex 瑞宁得, 阿纳托唑, 阿那曲唑Arsenic trioxide AS2O3 三氧化二砷 A araginase L-A 门冬酰胺酶 BBevacizumab, Avastin BEV 抗血管内皮生长因子单克隆嵌合抗体Bicalutamide, Casodex 比卡鲁胺 Bleomycin BLM 博来霉素Busulfan, Myleran BUS, F 白消安, 马利兰 CCalichcamicin 人源化抗CD33单克隆抗体 Camptothecin CPT 喜树碱 Carboplatin, Paraplatin C 卡铂 Carmofur HCFU 卡莫氟, 嘧福禄Carmustine BCNU 卡莫司汀,卡氮芥Chlorambucil, Leukeran CLB 苯丁酸氮芥, 痛可宁Ci latin PDD, CDDP 顺铂Cladribine, 2-chlorooxyadenosine CDA,2-Cd A 2-氯脱氧腺苷, 克拉屈滨 Colchicine COL 秋水仙碱Colchicine amide COLM 秋水仙酰胺 Compound Diphenoxylate Tablets 苯乙哌啶Cyclocytidine CCY 环胞苷, 安西他滨 Cyclopho hamide CTX 环磷酰胺Cytarabine, Cytosine arabinoside Ara-C 阿糖胞苷Dacarbazine DTIC 达卡巴嗪, 氮烯咪胺 DDactinomycin, Actinomycin D ACD 放线菌素D, 更生霉素Daunorubicin DNR 柔红霉素, 正定霉素 Dexamethasone DXM 地塞米松 Dexrazoxane 右雷佐生 Diphenhy dramine 苯海拉明Doxorubicin, Adriamycin ADM 阿霉素, 多柔比星 EElemene Emulsion 榄香烯乳Epirubicin, Epidoxorubicin EPI 表阿霉素, 表柔比星Estramustine EM 癌腺治, 雌二醇氮芥, 雌莫司汀Etoposide VP-16 足叶乙苷, 鬼臼乙叉甙, 依托泊苷, 足叶已甙Exemestane EXE 依西美坦, 艾罗美新 FFemara, Letrozole LTZ 来曲唑Floxuridine FUDR 5-氟脱氧尿苷, 氟尿苷Fludarabine FA 氟达拉宾Fluorouracil, Fluoracil 5-Fu 氟尿嘧啶Flutamide, Eulexin 氟硝丁酰胺, 缓退瘤Folic acid 叶酸Ftorafur, Tegafur FT207 替加氟, 喃氟啶,呋氟尿嘧啶 FudR 氟苷 GGemcitabine, Gemzar GEM 健择, 双氟胞苷, 吉西他滨 Gemtuzumab Ozogamicin, Mylotarg TM CMA-676 卡奇霉素, 吉妥组单抗, 人源化抗CD33嵌合抗体卡奇霉素免疫复合物 Glivec, Imatinib STI 571 格列卫, 甲磺酸伊马替尼 HHomoharringtonine 高三尖杉酯碱Human granulocyte colony stimulating factor G-CSF 重组粒细胞集落刺激因子Human granulocyte-macrophage colony stimulating factor GM-CSF 重组巨噬细胞粒细胞集落刺激因子Hydrocortisone 氢化可的松Hydroxycamptothecin HCPT 羟基喜树碱, 羟喜树碱Hydroxyurea, Hydroxycarbamide HU 羟基脲 IIdarubicin IDA 去甲氧柔红霉素Ifosfamide Ifo hamide IFO 异环磷酰胺Interferon IFN 干扰素Interferon alfa IFNαα-干扰素Interferon-β IFNββ-干扰素 Interlukin 2 rIL-2 白细胞介素2 Ire a, Gefitinib ZD1839 易瑞沙 Irinotecan CPT-11 依利替康 LLeucovorin, Calcium folinate CF, LV 亚叶酸钙Leuprolide 瘤破利得, 醋酸亮丙瑞林 Leuprolide depot 瘤破利得库 Liposomal Doxorubicin 阿霉素脂质体 Lomustine CCNU 洛莫司汀, 环已亚硝脲 Loperamide, Imodium 洛哌丁胺, 易蒙停, 氯苯呱酰胺MMechlorethamine, Mustine, Chlormethine HN2 盐酸氮芥, 氮芥 Megace MA 甲地孕酮 Melphalan 美法仑Melphalan, Alkeran MEL 苯丙氨酸氮芥Me a 美司钠Methotrexate MTX 甲氨蝶呤 Methylprednisone MPED 甲基强的松 Mitomycin MMC 丝裂霉素Mitoxantrone, Novantrone MIT, NVT 米托蒽醌Mitramycin MTH 光辉霉素 NNilutamide 尼鲁特米Nimustine ACNU 尼莫司汀, 嘧啶亚硝脲 Nocardia rubra cell wall skeleton N-CWS 胞必佳, 红色诺卡氏菌细胞壁骨架 O Oxaliplatin L-OHP 草酸铂, 奥沙利铂PPemetrexed, Alimta 阿灵达Pingyangmycin PYM 平阳霉素Prednisone PED, PDN 强的松, 泼尼松Procarbazine PCB, PCZ 甲基苄肼 Provera MPA 甲孕酮, 乙酸甲羟孕酮 RRaltitrexed, Tomudex 雷替曲塞 Retinoic acid RA 维甲酸Rituximab, Rituxan, Mabthera 美罗华, 利妥昔单抗 TTamoxifen TAM 三苯氧胺Taxol, Paclitaxel TAX, PTX 紫杉醇, 泰素Taxotere, Docetaxel DOC 多西紫杉醇, 泰索帝Temozolomide, Temodal TEM, TMZ 替莫待尔Teniposide VM-26 替尼泊苷,威猛 Thalidomide 沙利度胺, 反应停 Topotecan TPT 拓扑替康 Trastuzumab, Herceptin 赫赛汀Tumor Necrosis Factor TNF 肿瘤坏死因子UUracil, UFT 优福定 VVi lastine VLB 长春花碱, 长春碱Vincristine, Oncovin VCR 长春新碱Vindesin VDS 长春地辛Vinorelbine NVB 长春瑞滨XXeloda, Capecitabine Cap, BOF-A2 希罗达, 卡培他滨, 氟嘧啶氨甲酸酯 ZZoladex, Goserelin depot 诺雷德库, 戈舍瑞林篇三:顺铂顺铂顺铂本品是中心以二价铂同两个氯原子和两个氨分子结合的重金属络合物,类似于双功能烷化剂,可与DNA复制。
银杏达莫联合依达拉奉右莰醇治疗急性脑梗死的疗效分析

DOI:10.19368/ki.2096-1782.2023.11.181银杏达莫联合依达拉奉右莰醇治疗急性脑梗死的疗效分析张楠,冯彦梅邳州市中医院脑病科,江苏邳州221300[摘要]目的探究急性脑梗死应用银杏达莫联合依达拉奉右莰醇治疗的临床疗效。
方法选取2020年6月—2022年12月邳州市中医院收治的78例急性脑梗死患者为研究对象,以随机数表法分为两组,对照组39例应用依达拉奉右莰醇治疗,研究组39例应用银杏达莫联合依达拉奉右莰醇治疗,对比两组疗效、不良反应、血液流变指标、神经功能缺损评分、日常生活能力评分及炎性因子水平。
结果研究组总有效率高于对照组(94.87% vs 79.49%),差异有统计学意义(χ2=4.129,P<0.05)。
治疗前,两组血液流变指标、神经功能缺损评分、功能恢复评分及炎性因子水平比较,差异无统计学意义(P>0.05)。
治疗后,研究组红细胞沉降率、血浆黏度水平均较对照组更低,差异有统计学意义(P<0.05)。
研究组神经功能缺损评分为(5.65±0.68)分,较对照组的(6.29±1.07)分更低,功能恢复评分为(3.68±0.63)分,较对照组的(3.22±0.58)分更高,差异有统计学意义(t= 3.153、3.355,P<0.05)。
研究组白介素-6、肿瘤坏死因子水平比对照组更低,差异有统计学意义(P<0.05)。
两组不良反应发生率比较,差异无统计学意义(P>0.05)。
结论银杏达莫联合依达拉奉右莰醇用于急性脑梗死治疗,患者血液流变学及神经功能均得到极大缓解,炎性因子水平降低,日常生活能力提升,安全可靠。
[关键词]银杏达莫;依达拉奉右莰醇;急性脑梗死;神经功能;生活能力;不良反应[中图分类号]R743 [文献标识码]A [文章编号]2096-1782(2023)06(a)-0181-04Analysis of the Efficiency of Ginkgundamo Combined with Edaravone and Dexborneol in the Treatment of Acute Cerebral InfarctionZHANG Nan, FENG YanmeiDepartment of Cerebral Disease, Pizhou Hospital of Traditional Chinese Medicine, Pizhou, Jiangsu Province, 221300 China[Abstract] Objective To investigate the clinical efficacy of acute cerebral infarction treated with Ginkgundamo com⁃bined with edaravone and dexborneol. Methods 78 patients with acute cerebral infarction admitted to Pizhou Hospital of Traditional Chinese Medicine from June 2020 to December 2022 were selected as the research objects. They were divided into two groups by random number table. 39 patients in the control group were treated with edaravone and dex⁃tranol, and 39 patients in the study group were treated with ginkgundamo combined with edaravone and dextranol. The efficacy, adverse reactions, hemorheological indicators, neurological deficit scores, fuctional recoveny scores, and lev⁃els of inflammatory factors of the two groups were compared. Results The total effective rate of the research group was higher than that of the control group (94.87% vs 79.49%), and the difference was statistically significant (χ2=4.129, P< 0.05). Before treatment, there was no statistically significant difference between the two groups in terms of blood rheol⁃ogy indicators, neurological deficit score, daily living ability score, and inflammatory factor levels (P>0.05). After treat⁃ment, the erythrocyte sedimentation rate and plasma viscosity level in the study group were lower than those in the control group, and the difference was statistically significant (P<0.05). The neurological deficit score of the study group was (5.65±0.68) points, which was lower than the control group´s (6.29±1.07) points, and the fuctional recoveny score was (3.68±0.63) points, which was higher than the control group´s (3.22±0.58) points, and the difference was sta⁃[作者简介] 张楠(1988-),女,本科,主治医师,主要从事脑病科临床工作。
(完整word版)内科学专业英语词汇

Respiratory systemabdominal breathing 腹式呼吸abscess 脓肿acetylcysteine 乙酰半胱氨酸,痰易净(用作各种支气管与肺部疾病的辅药)acid-base balance 酸碱平衡acidosis 酸中毒acute tracheobronchitis 急性气管-—支气管炎acute cor pulmonale 急性肺源性心脏病acute lung injury, ALI 急性肺损伤acute upper respiratory tract infection 急性上呼吸道感染adenosine deaminase, ADA 腺苷脱氨酶adenocarcinoma 腺癌adenopharyngitis 咽扁桃体炎adult respiratory distress syndrome , ARDS 成人呼吸窘迫综合症aerobe 需氧菌aerodermectasia 皮下气肿aeroporotomy 呼吸道通气术(如用插管法或气管切开术)afebrile 无热(度)的,无发热病的β2-receptor agonist β2受体激动剂airway hyperresponsiveness, AHR 气道高反应性airway obstruction 气道阻塞airway remodeling 气道重塑alkalemia 碱血症alkalosis 碱中毒allergic airway inflammation, AAI 变态反应性气道炎症allergic bronchial-pulmonary aspergillosis, ABPA 变态反应性支气管肺曲菌病allergic granulomatosis 过敏性肉芽肿病allergy 变态反应性;变态反应,过敏反应alveolus ([pl.]alveoli )肺泡amantadine 金刚烷胺(抗病毒药)ambroxol 盐酸氨溴索(化痰药)aminophylline 氨茶碱(用于舒张支气管平滑肌,平喘及利尿)amphoric breath sound 空瓮性呼吸音ampicillin 氨卡青霉素amygdala 扁桃体amygdalitis 扁桃体炎·1·anaerobe 厌氧菌anaerosis 呼吸间断(尤指新生儿)anaphylaxis 过敏性,过敏反应,过敏症anaphylactic shock 过敏性休克anectasis 先天性扩张不全,原发性肺不张angina 咽峡炎,咽痛;绞痛anion gap, AG 阴离子间隙anoxia 缺氧(症)antasthmatic 止喘的,镇喘的、止喘药,镇喘药anthracosis 炭末沉着病,炭肺antibechic 镇咳的,镇咳药antibiotic 抗菌的,抗生的、抗菌素,抗生素anticancer 抗癌的anticarcinogen 抗癌药anticholinergic 抗胆碱能的、抗胆碱能药(副交感神经阻滞药)antiemetic 消水肿的,消水肿药antifebrile 解热的、解热药antifungal 抗真菌的、杀真菌药antigen—antibody reaction 抗原抗体反应antihemorrhagic 抗出血的,抗出血药物anti-infectious 抗感染的anti—infective 抗感染的,抗感染药anti—inflammatory 抗炎的,消炎的,消炎药antimycobacterial 抗分支杆菌的antineoplastic 抗肿瘤的、抗肿瘤药antiphthisic 抗痨的,抗结核的antipneumococcic 抗肺炎球菌的antispasmodic 镇痉的、镇痉药,解痉药antistaphylococcic 抗葡萄球菌的α1—antitrypsin,α1-AT α1—抗胰蛋白酶antituberculin 抗结核菌素antituberculotic 抗结核的、抗结核药antitussive 镇咳的、镇咳药apnea 呼吸暂停、窒息apneumatosis 肺无气,先天性肺不张apneumia 无肺(畸形)artificial respiration 人工呼吸asbestosis 石棉肺,石棉沉着病asphyxia 窒息aspiration pneumonia 吸入性肺炎·2·aspirin induced asthma, ASA 阿司匹林引起的哮喘asthma 气喘,哮喘asthmatiform 气喘样的,哮喘样的asthmogenic 气喘原的,致气喘的、致喘剂atopy 遗传性过敏症auscultate 听诊auscultator 听诊者;听诊器axillary node 腋窝淋巴结bacille Calmette Guerin , BCG 卡介菌(BCG vaccine 卡介苗) backache 背痛bacteria ( bacterium的复数)细菌bactericide 杀菌剂bacteriemia 菌血症Bamberger-Marie disease (Eugen Bamberger ; Pierre Marie)肥大性肺性骨关节病bambuterol 班布特罗(β2受体激动剂)barrel chest 桶状胸bathypnea 深呼吸bechic 咳嗽的、镇咳药beclomethasone dipropionate , BDP 二丙酸倍氯米松(糖皮质激素)benzopyrene 苯并芘benzylpenicillin 苄青霉素,青霉素Gbody mass index, BMI 体重指数Bouchut’s repspiration (jean A. E。
盐酸苯海拉明注射液说明书

盐酸苯海拉明注射液说明书【药品名称】通用名称:盐酸苯海拉明注射液英文名称:Diphenhydramine Hydrochloride Injection【成分】本品主要成分为:盐酸苯海拉明。
其化学名称:N, N-二甲基-2-(二苯基甲氧基)乙胺盐酸盐。
【性状】本品为无色的澄明液体【适应症】主要用于:急性重症过敏反应,可减轻输血或血浆所致的过敏反应;手术后药物引起的恶心呕吐;帕金森病和锥体外系症状;牙科局麻,当病人对常用的局麻药高度过敏时, 1%苯海拉明液可作为牙科用局麻药;其他过敏反应病, 不宜口服用药者。
【规格】1ml :20mg【用法用量】深部肌内注射,一次20mg (1支),一日1~2次。
【不良反应】( 1)常见的有:中枢神经抑制作用、共济失调、恶心、呕吐、食欲不振等。
( 2)少见的有:气急、胸闷、咳嗽、肌张力障碍等。
有报道给药后可发生牙关紧闭并伴喉痉挛。
( 3)偶可引起皮疹、粒细胞减少,贫血及心率紊乱。
【禁忌】重症肌无力、闭角型青光眼、前列腺肥大者禁用。
对本品及赋形剂过敏者禁用。
新生儿、早产儿禁用。
【注意事项】(1)幽门十二指肠梗阻、消化性溃疡所致幽门狭窄、膀胱颈狭窄、甲状腺功能亢进、心血管病、高血压以及下呼吸道感染(包括哮喘)者不宜用本品。
(2)对其他乙醇胺类高度过敏者,对本品也可能过敏。
(3)应用本药后避免驾驶车辆、高空作业或操作机器。
(4)肾功能衰竭时,给药的间隔时间应延长。
(5)本品的镇吐作用可给某些疾病的诊断造成困难。
【孕妇及哺乳期妇女用药】(1)妊娠期使用本品,有使婴儿腭裂、腹股沟疝和泌尿生殖器官畸形发生率增多的可能,孕妇应慎用。
(2)本品有少量可从乳汁排出,哺乳期妇女不宜使用。
【儿童用药】尚不明确。
【老年用药】可发生反应迟钝、头晕等。
【药物相互作用】(1)本品可短暂影响巴比妥类药和磺胺醋酰钠等的吸收。
(2)和对氨基水杨酸钠同用可降低后者血药浓度。
(3)可增强中枢神经抑制药的作用【药物过量】婴儿与儿童用药过量可致激动、幻觉、抽搐,甚至死亡;成人用药过量可致发热、震颤、呼吸困难、低血压。
常用化疗药物缩写大全
常用化疗药物缩写大全2015年08月28日A英文名简写名中文名Aclacinomycin ACLA阿克拉霉素Alemtuznmab阿来组单抗,抗CD52嵌合抗体All-trans retinoic acid ATRA,RA全反式维甲酸,维A酸Aminoglutethimide AG氨基导眠能,氨鲁米特,氨苯哌酮Anastrozole,Arimidex瑞宁得,阿纳托唑,阿那曲唑Arsenic trioxide AS2O3三氧化二砷Asparaginase L-ASP门冬酰胺酶B英文名简写名中文名Bevacizumab,Avastin BEV抗血管内皮生长因子单克隆嵌合抗体Bicalutamide,Casodex比卡鲁胺Bleomycin BLM博来霉素Busulfan,Myleran BUS,BSF白消安,马利兰C英文名简写名中文名Calichcamicin人源化抗CD33单克隆抗体Camptothecin CPT喜树碱Carboplatin,Paraplatin CBP卡铂Carmofur HCFU卡莫氟,嘧福禄Carmustine BCNU卡莫司汀,卡氮芥Chlorambucil,Leukeran CLB苯丁酸氮芥,痛可宁Cisplatin DDP、顺铂CDDP2-氯脱氧腺苷,克拉屈滨Cladribine,2-chlorooxyadenosine CDA,2-CdAColchicine COL秋水仙碱Colchicine amide COLM秋水仙酰胺Compound Diphenoxylate Tablets苯乙哌啶Cyclocytidine CCY环胞苷,安西他滨Cyclophosphamide CTX环磷酰胺Cytarabine,Cytosine arabinoside Ara-C阿糖胞苷D英文名简写名中文名Dacarbazine DTIC达卡巴嗪,氮烯咪胺Dactinomycin,Actinomycin D ACD放线菌素D,更生霉素Daunorubicin DNR柔红霉素,正定霉素Dexamethasone DXM地塞米松Dexrazoxane右雷佐生Diphenhy dramine苯海拉明Doxorubicin,Adriamycin ADM阿霉素,多柔比星E英文名简写名中文名Elemene Emulsion榄香烯乳Epirubicin,Epidoxorubicin EPI表阿霉素,表柔比星Estramustine EM癌腺治,雌二醇氮芥,雌莫司汀Etoposide VP-16足叶乙苷,鬼臼乙叉甙,依托泊苷,足叶已甙Exemestane EXE依西美坦,艾罗美新F英文名简写名中文名Femara,Letrozole LTZ来曲唑Floxuridine FUDR5-氟脱氧尿苷,氟尿苷Fludarabine FA氟达拉宾Fluorouracil,Fluoracil5-Fu氟尿嘧啶Flutamide,Eulexin氟硝丁酰胺,缓退瘤Folic acid叶酸Ftorafur,Tegafur FT207替加氟,喃氟啶,呋氟尿嘧啶FudR氟苷G英文名简写名中文名Gemcitabine,Gemzar GEM健择,双氟胞苷,吉西他滨Gemtuzumab Ozogamicin, Mylotarg TM CMA-676卡奇霉素,吉妥组单抗,人源化抗CD33嵌合抗体卡奇霉素免疫复合物Glivec,Imatinib STI571格列卫,甲磺酸伊马替尼H英文名简写名中文名Homoharringtonine高三尖杉酯碱Human granulocyte colony stimulatingfactorG-CSF重组粒细胞集落刺激因子Human granulocyte-macrophage colony stimulating factor GM-CSF 重组巨噬细胞粒细胞集落刺激因子Hydrocortisone氢化可的松Hydroxycamptothecin HCPT羟基喜树碱,羟喜树碱Hydroxyurea,Hydroxycarbamide HU羟基脲I英文名简写名中文名Idarubicin IDA去甲氧柔红霉素Ifosfamide Ifosphamide IFO异环磷酰胺Interferon IFN干扰素Interferon alfa IFNαα-干扰素Interferon-βIFN-ββ-干扰素Interlukin2rIL-2白细胞介素2 Iressa,Gefitinib ZD1839易瑞沙Irinotecan CPT-11依利替康L英文名简写名中文名Leucovorin,Calcium folinate CF,LV亚叶酸钙Leuprolide瘤破利得,醋酸亮丙瑞林Leuprolide depot瘤破利得库Liposomal Doxorubicin阿霉素脂质体Lomustine CCNU洛莫司汀,环已亚硝脲Loperamide,Imodium洛哌丁胺,易蒙停,氯苯呱酰胺M英文名简写名中文名HN2盐酸氮芥,氮芥Mechlorethamine,Mustine,ChlormethineMegace MA甲地孕酮Melphalan美法仑Melphalan,Alkeran MEL苯丙氨酸氮芥Mesna美司钠Methotrexate MTX甲氨蝶呤Methylprednisone MPED甲基强的松Mitomycin MMC丝裂霉素Mitoxantrone,Novantrone MIT,NVT米托蒽醌Mitramycin MTH光辉霉素N英文名简写名中文名Nilutamide尼鲁特米Nimustine ACNU尼莫司汀,嘧啶亚硝脲Nocardia rubra cell wall skeleton N-CWS胞必佳,红色诺卡氏菌细胞壁骨架O英文名简写名中文名Oxaliplatin L-OHP、OXA草酸铂,奥沙利铂P英文名简写名中文名Pemetrexed,Alimta阿灵达Pingyangmycin PYM平阳霉素Prednisone PED,PDN强的松,泼尼松Procarbazine PCB,PCZ甲基苄肼Provera MPA甲孕酮,乙酸甲羟孕酮R英文名简写名中文名Raltitrexed,Tomudex雷替曲塞Retinoic acid RA维甲酸Rituximab,Rituxan,Mabthera美罗华,利妥昔单抗T英文名简写名中文名Tamoxifen TAM三苯氧胺Taxol,Paclitaxel TAX,PTX紫杉醇,泰素Taxotere,Docetaxel DOC多西紫杉醇,泰索帝Temozolomide,Temodal TEM,TMZ替莫待尔Teniposide VM-26替尼泊苷,威猛Thalidomide沙利度胺,反应停Topotecan TPT拓扑替康Trastuzumab,Herceptin赫赛汀Tumor Necrosis Factor TNF肿瘤坏死因子U英文名简写名中文名Uracil UFT优福定V英文名简写名中文名Vinblastine VLB长春花碱,长春碱Vincristine,Oncovin VCR长春新碱Vindesin VDS长春地辛Vinorelbine NVB长春瑞滨X英文名简写名中文名Xeloda,Capecitabine Cap BOF-A2希罗达,卡培他滨,氟嘧啶氨甲酸酯Z英文名简写名中文名Zoladex,Goserelin depot诺雷德库,戈舍瑞林。
Xofigo 放射性治疗药剂指南说明书
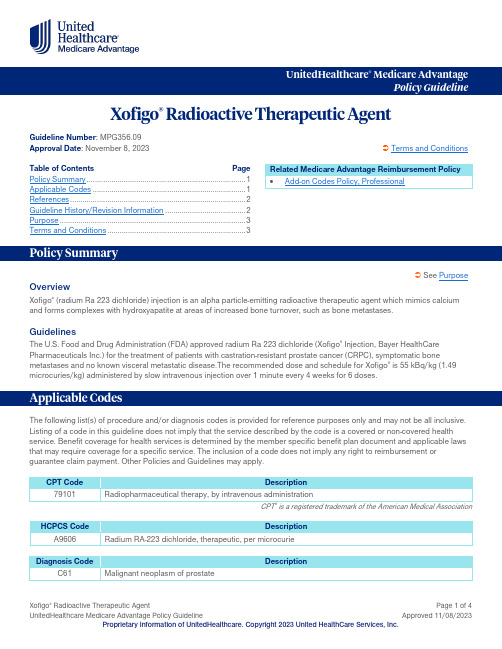
UnitedHealthcare ® Medicare AdvantagePolicy GuidelineXofigo ® Radioactive Therapeutic AgentGuideline Number : MPG356.09Approval Date : November 8, 2023 Terms and ConditionsTable of Contents Page Policy Summary ............................................................................. 1 Applicable Codes .......................................................................... 1 References ..................................................................................... 2 Guideline History/Revision Information ....................................... 2 Purpose .......................................................................................... 3 Terms and Conditions . (3)See PurposeOverviewXofigo ® (radium Ra 223 dichloride) injection is an alpha particle-emitting radioactive therapeutic agent which mimics calcium and forms complexes with hydroxyapatite at areas of increased bone turnover, such as bone metastases.GuidelinesThe U.S. Food and Drug Administration (FDA) approved radium Ra 223 dichloride (Xofigo ® Injection, Bayer HealthCare Pharmaceuticals Inc.) for the treatment of patients with castration-resistant prostate cancer (CRPC), symptomatic bonemetastases and no known visceral metastatic disease.The recommended dose and schedule for Xofigo ® is 55 kBq/kg (1.49 microcuries/kg) administered by slow intravenous injection over 1 minute every 4 weeks for 6 doses.The following list(s) of procedure and/or diagnosis codes is provided for reference purposes only and may not be all inclusive. Listing of a code in this guideline does not imply that the service described by the code is a covered or non-covered health service. Benefit coverage for health services is determined by the member specific benefit plan document and applicable laws that may require coverage for a specific service. The inclusion of a code does not imply any right to reimbursement or guarantee claim payment. Other Policies and Guidelines may apply.CPT Code Description 79101 Radiopharmaceutical therapy, by intravenous administrationCPT ® is a registered trademark of the American Medical AssociationHCPCS Code DescriptionA9606 Radium RA-223 dichloride, therapeutic, per microcurieDiagnosis Code DescriptionC61Malignant neoplasm of prostateRelated Medicare Advantage Reimbursement Policy • Add-on Codes Policy, ProfessionalDiagnosis CodeDescriptionAnd at least one of the following:C79.51 Secondary malignant neoplasm of boneC79.52 Secondary malignant neoplasm of bone marrowCMS Local Coverage Determinations (LCDs) and ArticlesLCDArticleContractor Medicare Part A Medicare Part BN/A A54559 Billing and Coding: Xofigo Billing Instructions PalmettoAL, GA, NC, SC,TN, VA, WV N/AA55052 Billing and Coding: Radiopharmaceutical Agents Retired 12/29/2022WPSAK, AL, AR, AZ, CA, CO, CT, DE, FL, GA, HI, IA, ID, IL, IN, KS, KY, LA, MA, MD, ME, MI, MO, MS, MT, NC, ND, NE, NH, NJ, NM, NV, OH, OK, OR, PA, RI, SC, SD, TN, TX, UT, VA, VT, WA, WI, WV, WYIA, IN, KS, MI, MO, NECMS Benefit Policy ManualChapter 15; § 50 Drugs and BiologicalsCMS Claims Processing ManualChapter 12; § 30.5 Payment for Codes for Chemotherapy Administration and Nonchemotherapy Injections and Infusions Chapter 14; § 10 General Ambulatory Surgical CenterChapter 17; § 90.2 Drugs, Biologicals, and RadiopharmaceuticalsOther(s)CGS Website (Submitting Claims for Xofigo/Radium 223)CMS HCPCS Codes for which ASP Reporting is in Units of Measure Other Than an NDC, Updated July 2023, CMS Website Xofigo Package Insert, Bayer Healthcare Pharmaceuticals WebsiteRevisions to this summary document do not in any way modify the requirement that services be provided and documented in accordance with the Medicare guidelines in effect on the date of service in question.Date Summary of Changes11/08/2023Policy Summary OverviewRemoved and relocated language pertaining to the U.S. Food and Drug Administration (FDA)approval of radium Ra 223 dichloride (Xofigo ® Injection, Bayer HealthCare Pharmaceuticals Inc.) usage (refer to the Guidelines section) GuidelinesRevised language to indicate:Date Summary of Changeso The U.S. Food and Drug Administration (FDA) approved radium Ra 223 dichloride (Xofigo®Injection, Bayer HealthCare Pharmaceuticals Inc.) for the treatment of patients with castration-resistant prostate cancer (CRPC), symptomatic bone metastases and no known visceralmetastatic diseaseo The recommended dose and schedule for Xofigo® is 55 kBq/kg (1.49 microcuries/kg)administered by slow intravenous injection over 1 minute every 4 weeks for 6 dosesSupporting InformationUpdated References section to reflect the most current informationArchived previous policy version MPG356.08The Medicare Advantage Policy Guideline documents are generally used to support UnitedHealthcare Medicare Advantage claims processing activities and facilitate providers’ submission of accurate claims for the specified services. The document can be used as a guide to help determine applicable:Medicare coding or billing requirements, and/orMedical necessity coverage guidelines; including documentation requirements.UnitedHealthcare follows Medicare guidelines such as NCDs, LCDs, LCAs, and other Medicare manuals for the purposes of determining coverage. It is expected providers retain or have access to appropriate documentation when requested to support coverage. Please utilize the links in the References section above to view the Medicare source materials used to develop this resource document. This document is not a replacement for the Medicare source materials that outline Medicare coverage requirements. Where there is a conflict between this document and Medicare source materials, the Medicare source materials will apply.The Medicare Advantage Policy Guidelines are applicable to UnitedHealthcare Medicare Advantage Plans offered by UnitedHealthcare and its affiliates.These Policy Guidelines are provided for informational purposes, and do not constitute medical advice. Treating physicians and healthcare providers are solely responsible for determining what care to provide to their patients. Members should always consult their physician before making any decisions about medical care.Benefit coverage for health services is determined by the member specific benefit plan document* and applicable laws that may require coverage for a specific service. The member specific benefit plan document identifies which services are covered, which are excluded, and which are subject to limitations. In the event of a conflict, the member specific benefit plan document supersedes the Medicare Advantage Policy Guidelines.Medicare Advantage Policy Guidelines are developed as needed, are regularly reviewed and updated, and are subject to change. They represent a portion of the resources used to support UnitedHealthcare coverage decision making. UnitedHealthcare may modify these Policy Guidelines at any time by publishing a new version of the policy on this website. Medicare source materials used to develop these guidelines include, but are not limited to, CMS National Coverage Determinations (NCDs), Local Coverage Determinations (LCDs), Medicare Benefit Policy Manual, Medicare Claims Processing Manual, Medicare Program Integrity Manual, Medicare Managed Care Manual, etc. The information presented in the Medicare Advantage Policy Guidelines is believed to be accurate and current as of the date of publication and is provided on an "AS IS" basis. Where there is a conflict between this document and Medicare source materials, the Medicare source materials will apply.You are responsible for submission of accurate claims. Medicare Advantage Policy Guidelines are intended to ensure that coverage decisions are made accurately based on the code or codes that correctly describe the health care services provided. UnitedHealthcare Medicare Advantage Policy Guidelines use Current Procedural Terminology (CPT®), Centers for Medicare andMedicaid Services (CMS), or other coding guidelines. References to CPT® or other sources are for definitional purposes only and do not imply any right to reimbursement or guarantee claims payment.Medicare Advantage Policy Guidelines are the property of UnitedHealthcare. Unauthorized copying, use, and distribution of this information are strictly prohibited.*For more information on a specific member's benefit coverage, please call the customer service number on the back of the member ID card or refer to the Administrative Guide.。
抗生素药敏纸片中英文对照表

头孢噻吩
KF
强力霉素
DO
头孢噻肟
CTX
青霉素
P
妥布霉素
TOB
庆大霉素
CN
万古霉素
VA
四环素
TE
西索霉素
SIS
羧苄西林
CAR
新霉素
N
头替坦
CTT
新生霉素
NV
头孢西丁
FOX
亚胺配能
IPM
头孢唑啉
KZ
氧氟沙星
OFX
头孢唑肟
ZOX
制霉菌素
NS
土霉素
OT
竹桃霉素
OL
壮观霉素
SH
[此文档可自行编辑修改,如有侵权请告知删除,感谢您的支持,我们会努力把内容做得更好]
CPD
美西林
MEL
头孢呋新钠盐
CXM
米诺环素
MH
头孢克罗
CEC
莫匹罗星
MUP
头孢克肟
CFM
奈啶酸
NA
头孢拉定
CE
奈替米星
NET
头孢孟多
MA
诺氟沙星
NOR
头孢哌酮
CFP
哌拉西林
PRL
头孢羟氨苄
CFR
哌拉西林/他唑巴坦
TZP 7.5:1
头孢曲松
CRO
哌拉西林/他唑巴坦
TZP 10:1
头孢噻定
CR
陪氟沙星
抗生素药敏纸片中英文对照表
抗生素名称
代码
抗生素名称
代码
阿米卡星
AK
阿齐红霉素
AZM
阿莫西林
AML
氨苄西林
AMP
Apramycin
中药学切片

中药学切片PB001PB002 绵马贯众叶柄基部横切PB003 掌叶大黄根茎横切PB004 何首乌块根横切PB005 威灵仙横切PB006 川乌横切PB007 怀牛膝横切PB008 川牛膝横切PB009 银柴胡横切PB010 黄连根横切(味连)PB011 北豆根横切PB012 山豆根横切PB013 甘草根横切PB014 地黄根横切PB015 赤芍根横切PB016 桔梗根横切PB017 玄参根横切PB018 丹参根横切PB019 防风根横切PB020 黄精根横切PB021 知母根横切PB022 射干根横切PB023 苦参根横切PB024 白芷根横切PB025 地榆根横切PB026 黄芪根横切PB027 人参根横切PB028 龙胆根横切PB029 黄芩根横切PB030 柳叶白前根茎横切PB031 南沙参根横切PB032 巴戟天根横切PB033 苍术根横切PB034 直立百部横切PB035 石菖蒲根茎横切PB036 天麻块茎横切PB037 黄丝郁金横切PB038 莪术横切PB039 麦冬根横切PB040 半夏根横切PB041 当归根横切PB042 党参根横切PB043 大黄根横切PB044 川贝母根茎横切PB045 白术根茎横切PB046 三七根横切PB047 天门冬根横切PB048 北细辛根横切PB049 北柴胡根横切PB050 野葛根横切PB051 板蓝根横切PB052 关木通茎横切PB053 鸡血藤横切PB054 沉香三切面PB055 络石藤茎横切PB056 青风藤横切PB057 黄连茎横切PB058 连翘茎横切PB059 酸枣茎横切PB060 绞股蓝茎横切PB061 荆芥茎横切PB062 穿心莲茎横切PB063 肉桂(树皮)横切PB064 杜仲皮横切PB065 川黄柏横切PB066 地骨皮横切PB067 香加皮横切PB068 厚朴(树皮)横切PB069 秦皮横切PB070 番泻叶横切PB071 大青叶横切PB072 地黄叶横切PB073 枇杷叶横切PB074 木通叶横切PB075 绞股蓝叶横切PB076 金银花叶横切PB077 栀子叶横切PB078 慈姑气生叶横切PB079 杜仲叶横切PB080 金银花花冠表面装片PB081 金银花雄蕊整体装片PB082 枸杞花纵切PB083 荆芥花横切PB084 枸杞花横切PB085 车前草花纵切PB086 月季花瓣横切PB087 小茴香分果横切PB088 牵牛子横切PB089 阳春砂种子横切PB090 五味子横切PB091 山楂果实横切PB092 苦杏仁种子横切PB093 枸杞果横切PB094 慈姑胚纵切PB095 罂粟果实横切PB096 合欢种子横切PB097 无花果果实纵切PB098 桃仁横切PB099 蛇床子分果横切PB100 瓜蒌皮横切PB101 薄荷叶横切PB102 薄荷茎横切PB103 薄荷茎纵切PB104 麻黄茎横切PB105 藿香茎纵切PB106 藿香茎横切PB107 益母草茎横切PB108 穿心莲叶横切PB109 淡竹叶横切PB110 石斛茎横切PB111 五倍子切片PB112 车前草根纵切PB113 灵芝菌盖纵切PB114 灵芝菌盖横切PB115 鹿茸纵切PB116 徐长卿根横切PB117 玉竹根茎横切PB118 商陆根横切PB119 天花粉根横切PB120 狼毒根横切PB121 虎杖根横切PB122 草乌根横切PB123 白头翁根横切PB124 秦艽根横切PB125 紫苏梗茎横切PB126 茜草根横切PB127 紫草根横切PB128 紫苑根横切PB130 白花蛇草茎横切PB131 补骨脂果实横切PB132 牡丹根皮横切PB133 祖师麻叶横切PB134 延胡萦叶横切PB135 两三金根横切PB136 两三银根横切PB137 川芎根横切PB138 南星根横切PB139 泽漆根横切PB140 红藤茎横切PB141 细叶十大功劳叶横切PB142 仙鹤草根横切PB143 桔梗茎离析装片PB144 天竺葵离析装片PB145 一品红茎纵切PB146 扶芳腾茎横切PB147 鱼腥草茎横切PB148 火炭母茎横切PB149 金毛狗脊根横切PB150 金毛狗脊叶柄基部横切PB151 马齿苋茎横切PB152 石微根横切PB153 茵陈蒿茎横切PB154 独活根横切PB155 紫萁叶柄基部横切PB156 浙贝母鳞茎横切PB157 沉香横切PB158 沉香纵切PB159 沉香径向切PB160 三叶木通横切PB161 白木香横切PB162 白木香纵切PB163 白木香径向切PB164 白木香三切面PB165 柿蒂横切PB166 广霍香茎纵切PB167 广霍香茎横切PB168 车前草根横切PB169 艾叶横切PB170 白微根横切PB171 白芍根横切PB172 赤芍根横切PB174 远志根横切PB175 甘遂根横切PB176 藁本根横切PB177 重楼根横切PB178 山药根横切PB179 姜黄根横切PB180 高良姜根横切PB181 广防己根横切PB182 白及根横切PB183 川续断根横切PB184 仙鹤草茎横切PB185 紫金牛茎横切PB186 金钱草茎横切PB187 川木通茎横切PB188 大血藤茎横切PB189 钩藤茎横切PB190 白花蛇舌草茎横切PB191 侧柏嫩枝横切PB192 合欢皮切片PB193 海桐皮切片PB194 苦楝皮切片PB195 陈皮切片PB196 功劳叶横切PB197 桉叶横切PB198 臭梧桐叶横切PB199 辛夷花蕾纵切PB200 槐米花苞纵切PB201 洋金花粉末装片PB202 蒲黄花粉装片PB203 肉豆蔻果实切片PB204 连翘果实切片PB205 槟榔种子切片PB206 白豆蔻种子切片PB207 石韦叶柄中部横切PB208 石韦叶横切PB209 淫羊霍叶横切PB210 紫花地丁叶横切PB211 马鞭草叶横切PB212 荆芥叶下表皮PB213 佩兰叶上表皮装片PB214 佩兰叶下表皮装片PB215 青蒿叶表皮装片PB216 冬虫夏草虫体横切PB217 冬虫夏草子座横切PB218 马钱子非腺毛切片Chinese pharmacyBacillus subtilisRhizobium meliloti,nitrogen fixing in root of legumeSpirillum volutams,large spirllumStaohylococcusOscillatoriaNostocEuglenaChlamydomonasProtococcusUlothrixCladophoraOedogoniumSpirogyra,one chloroplast in each cellSpirogyra,several chloroplasts in each cellSpirogyra,conjugation,several stagesDiatomsLaminaria japonica,sec.of soriRhizopus,bread mold,development of sporangiaPenicillium,sec,showing conidia on broom–like conidiophores w.m Aspergillus,conidia on spherical conidiophores w.mSaccharomyces,yeast w.m.showing nucleus & buddingPeziza,cup–fungus,sec.of apothecium with asciUstilago tritici,loose smut of wheatUstilago zeae,com smut,sec of pustule showing development of chlamydospores Coprinus,sec.showing basidia & sporesLichen,sec.of vegetative portion of thallusLichen,sec.of apotheciumMarchantia polymorpha,sec.of thallusMarchantia,sec.of cupule with gemmaeMarchantia,gemmae w.m.(vegetative reproduction)Marchantia,sec.of archegonial branch showing archegoniaMarchantia,sec.of antheridial branch showing archegoniaMarchantia,sec.of mature sporophyteMoss,L.S of antheridial cluster with antheridiaMoss,L.S of archegonial head with archegoniaMoss,protonema w.m.Moss,sporophyte attached to the gametophyte w.mFem,sec.of leaf with sporangiaFem,X.S.of rhizomeSalvinia,floating ferm,L.S.of sporocarpsFern prothallium w.m. of young specimen showing antheridia onlyFern prothallium w.m. of young specimen showing archegonia onlyFern prothallium typical specimen showing both antheridia &archegonia w.mFem prothallium,w.m.young sporophyteGinkgo.X.S of leaf &petiolePinus,X.S of leafPinus,first year stem X.SPinus,mature wood X.SPinus,mature wood rad secPintus,mature wood tang.secPintus.macerated wood tracheids &other cells isolatedPinus,cec. Of? young male strobilus showing meiosisPinus,median L.S. of male strobilus with axis, microsporophylls &microsporangiums Pinus,X.S of male strobilus with microsproesPinus,w.m. of mature pollen grainsPinus,L.S. of young female cone showing bracts &ovuliferous scales bearing ovules Daucus,carofa,X.S. of fleshy tap rootHelianthus,sunflower X.S. of mature rootCuscuta,sosser,onhost X.S.showing haustoriumRanunculus,X.S. of young root showing protoxylem &protophloem Ranunculus,X.S. of mature root showing metaxylem &radial bundle typeVicia,L.S. of root-tip for mitosisVicia faba,kidney bean,L.S. of young root tip showing root capVicia faba,X.S.of young root showing root hairVicia,X.S. of older rootVicia faba,X.S.of root showing development of lateral rootsIpomoea,sweat potato.X.S. of fleshy root showing food storageAllium,onion,L.S. of root-tips showing every stage in cell division &mitosis Allium,root-tip X.S. at several different levelsOrchid.X.S. of aerial rootZea mays,com.L.S. of root tip showing root cap etcZea mays,com.L.S. of root.polyarch arrangementRice.X.S. of root showing aerenchymaTriticum,wheat,X.S. of rootCuscuta,pumpkin.X.S. of stem,best type for study of phloem,showing sieve plates etc Cuscuta,L.S. of stem,showing sieve tubes etcHelianthus. Sunflower stem X.S. showing typical dicot stemHelianthus,sunflower stem.L.S.Pelargonium,geranium,X.S. of young stemPelargonium.X.S. of old stem showing secondary vascular tissue &corkCotton,stem X.SRicinus,caster bean,X.S. of stem showing typical vascular structureBuxus L.S. of stem tip showing meristematic tissueMymphaea,water lily,X.S.of aquatic stem showing air chamberNymphaea,water lily,X.S. of aguatic stem showing reduced vascular tissue &sipcular cells Solanum,lrish potato,X.S. of mature tuber stainted for starch grainsTilia,basswood,X.S. of lst year stemTilia,X.S. of 2 year stemTilia,X.S. of 3-year stemTilia,X.S. of older stem(4 or 5 years)showing mature structure with annual ringsTilia.L.S. of older stem(4 or 5 years)Tilia,macerated wood,showing individual wood fibersSalix,willow.X.S. of stemNerium stem X.SSambucus,elder,sec.of bark with lenticelZea mays,com,X.S.of stem showing typical monocot stemZea,stem L.SZea X.S.of young stem enclosed in sheath,leavesRice X.S. of stemTricicum,wheat,X.S. of stem showing few scattered bundlesLeaf bud L.S.showing liaf developmentPittosporum,X.S.ofa typical dicot leafCotton,leaf X.SVicia,dicot leaf, w.m.of epidermis showing stomataNerium leaf X.S.showing sunken stomata pits cuticle etcNicotiana,tobacce X.S.of leaf with glandular hairsPelargonium,geranium,X.S.of leaf showing cystolith in a xerophyteFicus,rubber plant,X.S.of leaf showing cystolith in a xerophyteNymphaea,water lily,X.S.of floating leaf showing spongy tissue, air chambers &spicular cells Allium,onion,w.m.of epidermis showing cells &nucleiLris,w.m.of epidermis shoing stomata)Lilium,X.S.of a typical monocot leafZea mays,com,X.S.of liaf showing separate bundlesTriticum,wheat.X.S.of leaf(grass type)Rice,X.S.of leafCapsella,sec.of developing flower spike showing various staegs in the development of the floral partsLilium,X.S.of typical monocot flowerPollen types w.m. of a great variety of pollens,mixedPollen tubes w.m.of germinated pollenZea mays,corn.L.S.of kernel through embryoTricicum,wheat,L.S.of endosperm showing stored foodRicinus,castro bean,X.S.of endosperm showing stored foodDiospyros,endosperm section showing plasmodesmaCapsella,L.S.of ovule with embryo at early stage showing origin of plerome.periblem &dermatogenCapsella,L.S.of embryo with cotyledons just differentiatingCapsella,L.S.of embryo with young cotyledonsCapsella.L.S.of mature embryo with cotyledonsLilium,X.S.of anther showing pollen grainsLilium,L.S.of anther showing pollen chambersgrainsLilium,X..S.of very young anther showing early sporogenous tissueLilium,X.S.of young anther showing microspore mother cellsLilium,X.S.of anther with microspore mother cells in prophaseLilium,anther sec.showing lst division (heterotypic)in microspore mother cellsLilium anther sec.showing second division(homeotypic)Lilium sec.of anther showing teradsLilium sec.of anther showing pollen grains at time of shedding(2-cell stage)Lilium,w.m. of mature pollenLilium,L.S.of style &stigma,showing pollen grainsLilium,X.S.of of ovary showing general structure & arrangement of of ovulesLilium,X.S.of.young ovary showing ovules with megaspore mother cells(uninuclear embryo sac Lilium,X.S.of ovary,ovules showing first division of megaspore mother? cell.heterotypic division Lilium,X.S.of ovary,ovules showing binucleate embryo sac.Capsella,L.S.of embryo with cotyledons just differentiatingEuglenaPlasmodium vivax,parasite of benign tertian malaria blood smearparamecium stained for general structure two different stainingtechniquesParamecium,various stages of fissionParamecium,various stages of conjugationParamecium,stained to show ciliaProtozoa mixed speciesHydra,extended specimen showing general structure w.m.Hydra,with bud w.mHydra,XS.showing detailed structure of ectoderm &endodermHydra X.S.through testisHydra X.S.through ovaryHydra L.S.through hypostome & basal diskHydra L.S.through adult &budHydra w.m. of tentaclesPlanaria with intestines injected&stainedSchistosoma japonicum,blood fluke,male w.mSchistosoma japonicum,blood fluke,female w.mSchistosoma japonicum,male&female in copulaSchistosoma japonicum,ova w.m.Schistosoms japonicum,miracidia w.mSchistosoma japonicum,cercaria w.mTaenia solium human tapeworm,scolex,w.mTaenia solium,ova w.mTaenia hydatigena,mature proglottidAscaris X.S.of male in regionof sex organsAscaris X.S.of female in region of sex organsAscaris,ova w.mAscaris,an excellent slide to demonstrate animal mitosisNereis,parapodium w.mEarthworm(pheretima)X.S.back of clitellumEarthworm,X.S.selected to show setaeEarthworm,X.S.through clitellumEarthworm,median L.S.of anterior endClam gill X.S.showing general structureAphis gossypii,w.m.Daphnia w.m.of fall female,with ephippiumCyclops w.m.with egg sacsCulex,common house mosquito,female w.mCulex,common house mosquito,male w.mCulwx,common house mosquito,larva w.mCulwx,common house mosquito,pupa w.mButterfly,w.m.of sucking tube (Siphoning type)Mosquito heads,male & female on same slide long slender piercing sucking type w.mHoney bee mouth parts (lapping type)House fly proboscis (sponging type)Cricket wings,showing file &scraper w.mHouse fly wing &halteris(rudimentary under wing )w.m.Honey bee wings,hooks&ridge forlocking wings together in flight w.mButterfly,wing scales,portion selected to show detailsHoney bee,three legs showing eye brush,antenna cleaner,pollen basket,pollen comb etc w.m. Butterfly,wing scales,portion selected to show detailsGrasshopper jumping leg,w.m.Mantis w.m.of front leg,usedfor graspingInsect legs,four typical legs on each slide(jumping,grasping,digging &swimming )showing adaptationsAmtenna types five kinds(plumose,pectinate,aristate,lnmellate,moniliform)Gizzard,cricket,flat mount of lining showing pattern of chitinous teethPrawn eye L.S.through ommatidiaCornea,flat mount to show facetsInsect trachea,w.m.showing cellular structure tracheal rings &fine branchingMalpighian tubules,grasshopper,w.m.Striated muscle,grasshopper,X.S.&L.S.on each slideGrasshopper,sec.of testis showing mitosisAmphioxus(Branchiostoma )w.m.of mature small specimenAmphioxus X.S.through mouthAmphioxus X.S.through pharynx,anterior to the gonads,showing gills Amphioxus X.S.through posterior portion of pharynx.to show gonads Amphioxus X.S.of intestinal region,anterior to the atriopore Amphioxus X.S.of intestinal region between atriopore&anus Amphioxus X.S.of tailAmphioxus X.S.through male &female specimens in region of gonads Amphioxus X.S.of pharynx,intestinal region & tail on one slideFrog small intestine,cross sectionFrog skin,section showing serous gland & pigment cells etcFrog skin flat mount to show pigment cellsSquamous epithelium scrapings from human mouthSquamous epithelium amphibian epidermisStratified squamous epitheliumCuboidal epitheliumSimple columnar epitheliumPseudostratified ciliated columnar epithelium from trachea Columnar epithelium macerated,intestinal mucosaCiliated epithelium macerated,mouth epithelium of frogCiliated epithelium ,sec.of clam gillTransitional epithelium,wall of bladderMitochondria sec.of liverMitochondria,kidneyGolgi apparatus in epithelial cells of intestineWhite fibrous tissue L.S.of rat tail showing rows of tendon cells Areolar connective tissue,white & elastic fibers &interstitial cells Mucoid tissue,from umbilical cordReticular tissue,trom lymph gland,bielschowski stainAdipose tissueHyaline cartilage,rabbitElastic cartilageFiber -cartilageBone,human,ground thin X.SBone,human,ground thin L.S.Bone,developing,cartilage,type,joint of finger or head of femur of fetus Bone,developing,developing ,membrane type,skull,of foetal head Blood,fishBlood,frogBlood,chickenBlood,pigeonBlood,sparrowBlood,human,Wright s stainBlood,human,H.&EBlood,rabbitStriated muscle,teased preparation showing whole fibres,nuclei,fibrillae,striations Striated muscle.X.S.& L.S.showing nuclei,fibrillae & striationsSmooth (involunatry )muscle,teased preparationSmooth muscle ,X.S.& L.S.Hiatr,uscle,teased preparation showing branching character striations &intercalated disks Heart muscle L.S.showing intercalated disksMuscle & tendon L.SNerve cells,section spinal cord,motor nerve cells,silver impregnatedPyramidal cells,cerebrum Golgi stainPurkinje cells,cerebellum,Golgi stainNerve X.S.& L.S.,H. & ESpinal ganglion,L.S.,H.& E.showing nerve fibers & nerve cellsSpinal ganglion,human L.S.Bielschowski silver stainedMotor nerve endings in intercostal muscles,gold impregnatedTongue,rabbie sec.showing taste budsTongue,cat L.S.showing thick horny layerParotid gland,a purely serous glandSublingual gland,a mixed glandPalatine tonsilEsophagus X.S.dog upper region showing esophageal.GlandEsophagus & trachea L.S.of both organsLarynx oesophagus L.S.of both organsEsophagus & stomach L.S.showing junctionBody of stomach,sec,of wall showing typical fundic glandsStomachus pyloricus,sec.from lower portion of the stomachStomach & duodenum L.S.of the junctionDtomach X.S.showing Brunner s gland & intestinal glandsJejunum,X.S.typical slide for intestine with villiLleum,X.S.showing aggregated lymphoid nodules in mucosaLarge intestine ,X.S.Appendix,human,X.S.Liver ,humanLiver,pig,fibrous trabeculae between lobulesLiver ,rabbit,stained to show glycogenGall bladder,X.SBile duct,X.SPancreas,secreting acini & islands of langerhansTrachea,X.S.ciliated epithelium,cartiage & fibrous tissreTrachea,L.SLung,human,general structureLung,rabbit injectedLung rabbit,thick sec,of pattern of alveoli,in relation of bronchiolesHeart,rat X.S.through atrium cordisHeart,rat,L.S.Aorta,human X.S.H.E.& elastic tissue stainArtery,& vein,elastic tissue stain as aboveVena cava,X.S.elastic tissue stainSpread of rat mesentery,stained to show blood vesselsKidney,human,sec.cortex & medullar with glomerulus tubuleskidney,guinea-pig L.S.of whole organ through pelvisKidney,rabbit,section,blood vessels injectedUreter,X.S.Urinary bladderOvary,rabbit,ses.for general structure,numerous developing eggsUeerine tube (oviduct),human,sec,through ampullaUterus,X.S.of entire uterus of rabbit ,showing all coatsPlacenta,human,sec.showing chorionic villi,etc.Umbilical cord,human X.STestis,human,showing general structureSpermatozoa,human sperm smearBull,sperm smearSheep,sperm smearRabbit testis,fixed &stained for mitosis,best slide for spermatogenesis Rabbit,sperm smearGuinea pig testis,fixed & stained for mitosis,Best slide for spermatogenesis Guinea pig ,sperm smearEpididymis,tubules filled with SpermatozoaVae deferens,human,X.SProstateCerebrum,rabbit,impregnated with silverCerebellum,rabbit,impregnated with silverWhole brain,rabbit L.S.Spinal cord,silver impregnated X..S.showing motor cell nerve fiberEar,internal cochlea (organ of corti)guinea pigEar,internal near median sec.of guinea pig cochleaEye,cornea,human fibrous tissue,stratified epitheliumEye ,iris,radial secRetina sec,humanLacrimal gland, human,a typical serous gland。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
CLINICAL INVESTIGATIONCALIFORNIUM-252BRACHYTHERAPY COMBINED WITH EXTERNAL-BEAM RADIOTHERAPY FOR CERVICAL CANCER:LONG-TERM TREATMENT RESULTS X IN L EI,M.D.,P H.D.,C HENG-Y UAN Q IAN,M.S C.,Y I Q ING,M.D.,K E-W EI Z HAO,M.D., Z HENG-Z HOU Y ANG,M.D.,P H.D.,N AN D AI,M.D.,Z HAO-Y ANG Z HONG,M.D.,C HENG T ANG,M.S C., Z HENG L I,M.S C.,X IAN-Q ING G U,M.S C.,Q IAN Z HOU,M.S C.,Y AN F ENG,M.S C.,Y AN-L I X IONG,M.S C.,J IN-L U S HAN,M.D.,AND D ONG W ANG,M.D.,P H.D.Cancer Center,Research Institute of Surgery and Daping Hospital,Third Military Medical University,Chongqing,ChinaPurpose:To observe,by retrospective analysis,the curative effects and complications due to californium-252(252Cf)neutron intracavitary brachytherapy(ICBT)combined with external-beam radiotherapy(EBRT)in the treatmentof cervical cancer.Methods and Materials:From February1999to December2007,696patients with cervical cancer(Stages IB toIIIB)were treated with252Cf-ICBT in combination of EBRT.Of all,31patients were at Stage IB,104at IIA,363atIIB,64at IIIA,and134at IIIB.Californium-252ICBTwas delivered at7–12Gy per insertion per week,with a totaldose of29–45Gy to reference point A in three tofive insertions.The whole pelvic cavity was treated with8-MVX-ray external irradiation at2Gy per fraction,four times per week.After16–38Gy of external irradiation,the center of the whole pelvicfield was blocked with a4-cm-wide lead shield,with a total external irradiationdose of44–56Gy.The total treatment course was5to6weeks.Results:Overall survival rate at3and5years for all patients was76.0%and64.9%,respectively.Disease-free3-and5-year survival rates of patients were71.2%and58.4%,te complications included vaginalcontracture and adhesion,radiation proctitis,radiation cystitis,and inflammatory bowel,which accounted for5.8%,7.1%,6.2%,and4.9%,respectively.Univariate analysis results showed significant correlation of stage,age,histopathologic grade,and lymph node status with overall survival.Cox multiple regression analysis showedthat the independent variables were stage,histopathologic grade,tumor size,and lymphatic metastasis in allpatients.Conclusion:Results of this series suggest that the combined use of252Cf-ICBTwith EBRT is an effective method fortreatment of cervical cancer.Ó2011Elsevier Inc.Cervical cancer,Brachytherapy,Californium-252,Treatment results.INTRODUCTIONCervical cancer ranks as the third leading cause of cancer death among women.It was estimated that in2008,75,400 women were diagnosed with cervical cancer and33,900 died of this disease in China(1,2).Radiotherapy,in the form of a combination of intracavitary brachytherapy (ICBT)with external-beam radiotherapy(EBRT),is consid-ered one treatment option for advanced cervical cancer. Gamma-radiation-emitting isotopes,such as60Co,137Cs, and192Ir,are often used in ICBT.Despite progress in after-loading techniques and computer technology,the survival rate of cervical cancer patients shows little improvement.Sev-eral groups have reported that g-brachytherapy-based concur-rent chemoradiation improves the survival of patients with locally advanced cervical carcer(3–7).In addition to theabove-mentioned g sources,neutron sources,especiallycalifornium-252,may play an important role in brachytherapy.Californium-252(252Cf),discovered in1950(8),emitsa mixedflux of2.1–2.3-MeV neutrons and0.5–1.0MeV g-rays with a half-life of2.65years.Neutrons are high linear energy transfer(LET)radiation resulting in radiobiologicaleffects.These effects include a high relative biological effec-tiveness(RBE)value,low oxygen enhancement ratio,inhi-bition of cell damage repair,and minimal dependence ofradiation sensitivity on the cell cycle.In the late1960s 252Cf was applied as a new radiation source in ICBT for treating gynecologic malignant tumors in the United States,the former Soviet Union,and Japan(9).Reprint requests to:Dong Wang,M.D.,Ph.D.Cancer Center, Research Institute of Surgery and Daping Hospital,Third Military Medical University,No.10Changjiang Zhilu,Yuzhong District,Chongqing400042,China’’Tel:+86-23-68894062, Fax:+86-23-68894062;E-mail:dongwang64@ Supported by the National Natural Science Foundation of China (30970761).C.-y.Q.and X.L.contributed equally to this work.Conflict of interest:none.Received April23,2010,and in revised form July29,2010. Accepted for publication Aug4,2010.1Int.J.Radiation Oncology Biol.Phys.,V ol.-,No.-,pp.1–7,2011CopyrightÓ2011Elsevier Inc.Printed in the USA.All rights reserved0360-3016/$-see front matterdoi:10.1016/j.ijrobp.2010.08.039Although252Cf is not widely used worldwide,and no stan-dard treatment regimen exists,there have been a number of pilot studies demonstrating that252Cf-ICBT is an effective method in the treatment of cervical cancer(10–12). Maruyama et al.(12,13)applied252Cf-ICBT combined with EBRT to treat cervical cancer patients in Stages IB, II,III,and IV A,and the5-year overall survival(OS)rates were87%,62%,33%,and20%,respectively.Marjina(14) studied345patients with cervical cancer in Stages II–III treated with252Cf-ICBT and EBRT.The5-year survival rate for Stages II and III was72.3%.Zhao et al.(15)reported that for Stage II,the3-year and5-year survival rates were 90.9%and76.2%,respectively.For Stage III,the3-year and5-year survival rates were81.5%and61%,respectively. The3-year and5-year OS rates were87.5%and70%,re-spectively.By comparison,it was reported that the5-year survival rates for cervical cancer patients in Stages IIB and IIIB who received g-brachytherapy were65–75%and35–50%for Stages IIB and IIIB,respectively(16–19).In a French Cooperative Group study of1875patients who received g-brachytherapy,Barillot et al.(20)reported5-year survival rates of83.5%,81%,71%,69%,and47.5% for Stages IB,IIA,IIB,IIIA,and IIIB,respectively.Tacev et al.(11)compared252Cf and conventional g-radiation in the brachytherapy of advanced cervical cancer.They found that the overall5-year survival rate of patients treated with252Cf neutron brachytherapy for Stage IIB was better by 18.9%than that of those receiving g-radiation(75.2%vs.56.3%,p<0.001).For IIIB,the improvement was22.8% (66.1%vs.43.3%,p<0.003).Recently we analyzed the current status of brachytherapy on cervical cancer in China by reviewing published articles from1990to2009.The results showed3-year OS rates of 95.3%and75.0%for Stage II and Stage III,respectively, and5-year OS rates of89.2%and75.0%in553patients with252Cf brachytherapy.The3-year OS rates of Stages II and III were83.3%and65.7%,respectively,and5-year OS rates were66.4%and58.4%in1613patients with g-bra-chytherapy(21).Until now,a large portion of cervical cancer patients were still treated with radiation therapy alone in China.Among other factors,the‘‘cost increase’’has argued against com-bined chemoradiation treatment.However,in1999,we im-plemented thefirst252Cf neutron remote afterloading system in China to treat cervical cancers.The afterloading unit is remotely controlled.The dose equivalent rate from the neutrons,for occupational exposures,does not exceed 10m Sv/h on the afterloader shielding surface,which is the limit recommended by the International Commission on Ra-diological Protection(22).Presently18252Cf afterloading systems have been installed in China,with more than3000 cervical cancer patients treated by252Cf-ICBT.In this article, the follow-up data of696cervical cancer patients treated with252Cf neutron brachytherapy and EBRT at our depart-ment are retrospectively analyzed,and the survival rate and cure rates of252Cf neutron brachytherapy for cervical cancer are presented.METHODS AND MATERIALSPatient populationFrom February1999to December2007,696previously un-treated patients with biopsy-proven cervical cancer were treated with252Cf-ICBT and concurrent EBRT at the Cancer Center,Re-search Institute of Surgery and Daping Hospital,Third Military Medical University.All patients had complete medical records and received physical examinations including staging at pelvic ex-amination by a gynecologic oncologist,radiation oncologist,or both.All carcinomas were definitively diagnosed by pathologic as-sessment,which showed normal hemogram and liver and kidney functions.Patients were examined by chest radiograpy,abdominal B-type ultrasonography,computed tomography(CT),positron emission tomography,or magnetic resonance imaging scan of the pelvic cavity to evaluate abdominal,visceral,osseous,nodal,and genitourinary puted tomography facilitated measure-ment of tumor diameter for cervical,especially endocervical tu-mors.The staging of the illness was determined according to the International Federation of Gynecology and Obstetrics(1997)rec-ommendations.Blood transfusions were given to anemic patients and those with severe bleeding to a minimum hemoglobin level of10g/dL.Patient characteristics are listed in Table1.252Cf-ICBTCalifornium-252-ICBT was applied by an LZH-1000afterload-ing system(Lin Den Science and Technology,Shenzhen,China; Fig.1),which contained a526-m g252Cf source.The following for-mula is used to convert252Cf dose to Gy equivalent(Gy-eq):D Gy-eq¼DnÂRBEnþD gÂRBE g;where Dn=252Cf neutron component dose,D g=252Cf g-compo-nent dose,RBEn=relative biological effectiveness of neutrons, Table1.Characteristics of696patients with cervical cancer Characteristics Patients% Total patients696Age(y),median,range46.3(16–81)Follow-up(mo),median(range)44(24–129)Stage(FIGO)IB31 4.5 IIA10414.9 IIB36352.1 IIIA649.2 IIIB13419.3 HistopathologySquamous cell carcinoma67897.4 Adenocarcinoma15 2.2 Others30.4 Histopathologic grade(G)G1(well differentiated)29842.8 G2(moderately differentiated)31244.8 G3(poorly or undifferentiated)8612.4 Tumor size(cm)<424435.0 4–625837.1 >619427.9 Lymph node statusPostive15221.8 Negative33047.4 Unknown21430.8 Abbreviation:FIGO=international federation of gynecology and obstetrics.2I.J.Radiation Oncology d Biology d Physics V olume-,Number-,2011and RBE g =relative biological effectiveness of g -radiation.The RBE value of the 252Cf neutron component is 2–3(23,24).During each applicator insertion,the uterus was first dilated with a dilater.A tricavity applicator (Fig.2)without 252Cf was inserted into the uterine cavity.Rectal barium enema was given to each pa-tient to visualize the rectum.The barium was pulled out as much as possible after radiography.A urine catheter was inserted into the bladder,and 7mL contrast media was injected into a Foley cath-eter.Anterior and posterior vaginal packing was performed after the insertion to fix the applicators and to maximize the distance between the source and the anterior rectal wall and posterior bladder wall.Then,orthogonal radiographs of the pelvic cavity were taken to show the extent and size of the tumor.These radiographs were the basis on which an individualized treatment plan was developed by the treatment planning software of the afterloading system.The dose was prescribed to point A,defined by the Manchester system as 2cm superior (along the tandem)to the flange abutting external cervical os and 2cm lateral from the axis of the tandem.The Inter-national Commision on Radiation Units and Measurements rectal reference point was defined along a lead wire on the rectum wall.The reference dose point of Foley in the bladder was the lowest point of contrast medium in the supine position film.The dose to point A for each patient was 7–12Gy per fraction,administered once per week.Californium-252-ICBT was delieverd in 2to 3h per insertion and performed three to five times in total.The ICBT treatment sched-ules for different tumor stages are listed in Table 2.The total 252Cf-ICBT dose to point A was 29–45Gy-eq in 3to 5fractions.The dose to bladder and rectum was less than 60%of point A,and the dose ra-tio of cervix and vagina was 1:1(Fig.3).Median calculated doses at International Commision on Radiation Units and Measurements ref-erence points from single ICBT were 7.1Gy (range,3.8–9.3Gy)for the rectum and 6.5Gy (range,5.1–8.3Gy)for the bladder.External-beam radiotherapyExternal-beam radiotherapy was given by 8-MV X-ray beams from an Elekta Precise linear accelerator (Elekta,Stockholm,Swe-den)with the position of the tumor target determined by CT scan.The linear accelerator is equipped with multileaf collimators to form conformal radiation fields.The EBRT dose was delivered to the pelvis through anterior and posterior parallel-opposed portals.The fields extended superiorly to the L4–5interspace and inferiorly to the middle part of the lower margin of the obturator t-erally,the fields extended at least 1.5cm beyond the bony margin of the pelvis at the widest point.The total dose of EBRT to the whole pelvis was 44–56Gy (2Gy per fraction per day).The composite dose of ERBT plus 252Cf-ICBT is shown in Table 2.Center shield-ing,with the placement of a 4-cm rectangular midline lead block of 5half value layer in both fields,was applied after 16–38Gy pelvic radiotherapy.The goal of the midline block technique was to spare the bladder and rectum (thereby reducing toxicity)while permitting increased doses to the cervix from the ICBT (thereby improving lo-cal tumor control).The total time of 8-MV X-ray EBRT combined with 252Cf brachytherapy was 5to 6weeks (Table 2).Follow-upFollow-up was performed for each patient every 3months in the first 2years after treatment and every 6monthsthereafter.Fig.1.Californium-252afterloading system.(a)Afterloading application module;(b)treatment control system;(c)treat-ment planningsystem.Fig.2.Tricavity applicator.Table 2.Treatment schedules Stage EBRT (Gy)252Cf-ICBT (Gy fr.)Treatment time (d)WP WP with MB IB 162829/3–40/432–36IIA 20–2422–2840/4–45/532–39IIB 24–2820–2838/4–42/434–41IIIA 30–3418–3238/4–42/434–42IIIB34–3816–2038/4–45/535–42Abbreviations:EBRT =external-beam radiotherapy;ICBT =in-tracavitary brachytherapy;WP =whole-pelvic irradiation;MB =midline block;fr.=fraction.252Cf brachytherapy for cervical cancer–>252Cf brachytherapy for cervical cancer d X.L EI et al .3Checkups included a physical examination,routine blood cell counts,chest radiograpy,intravenous urography,and cystoscopy.If clinical suspicion of recurrence was present,additional investiga-tions including biopsy and CT,positron emission tomography,or magnetic resonance imaging scan of the abdomen and pelvis were to be done.Treatment failures were classified as pelvic recur-rences or distant metastases.Patients who died of causes other than cervical cancer but showed no evidence of other diseases at the last checkup were included in the OS rate.The follow-up examinations ended in December 2009.Late complications were graded according to the Radiation Ther-apy Oncology Group/European Organization for Research and Treatment of Cancer (RTOG/EORTC)late radiation morbidity scoring scheme.Statistical analysisA Statistical Package for Social Sciences software package (SPSS 13.0for Windows;SPSS,Chicago,IL)was used for analy-sis.The Kaplan-Meier actuarial method was used to analyze OS and disease-free survival (DFS).Durations of survival were calcu-lated from the start of treatment.Endpoint was any death for OS and local recurrence or metastasis for DFS (including deaths observed during treatment).The patients lost to follow-up were considered censored observations.Patients alive without recurrence were cen-sored on the date of the last follow-up.The log–rank test was used to determine any significant differences.Cox multiple regression analysis was used to detect the impact of factors on DFS and OS.Tumor stage,patient age,histopathologic grade,tumor size,and lymph node status were the variable factors for analyzing actuarial OS and DFS at 5years.A statistical result was regarded as signif-icant with p values <0.05or with a 95%confidence level.RESULTSGeneral outcomeMedian follow-up time for all patients was 44months (range,24–130months),65patients (9.3%)were lost to follow-up.Of all alive patients at the time of this analysis,477patients (68.5%)had no evidence of disease,and 28(4.0%)were with cancer,including 7(1.0%)with local re-lapse and 21(3.0%)with distant metastasis.Among expired patients,173(24.9%)died from cancer,15(2.2%)from clin-ical causes,and 3(0.4%)from late complications.The pat-terns of failure included local relapse in only 50patients (7.2%),distant metastasis in 109(16.0%),and local relapse with distant metastasis in 14(2.0%).Distribution of sites of distant metastases for all patients was as follows:bone =32,lung =28,para-aortic lymph nodes =27,left supraclavic-ular lymph nodes =18,and inguinal nodes =12.During follow-up a second malignant primary tumor was detected in 11patients (1.6%),including 3patients with cancer in the lung,3in the breast,3in the ovary,1in the liver,and 1in the bone.Survival ratesSurvival of each patient was calculated from the first ther-apy to the last follow-up examination.Overall survival at 3and 5years for all patients was 76.0%and 64.9%,respec-tively.Actuarial OS rates at 3and 5years for Stages IB,IIA,IIB,IIIA,and IIIB patients were 95.0%and 84.4%,85.3%and 77.7%,76.2%and 66.1%,68.3%and 54.2%,Fig.3.Isodose distribution for a typical 252Cf treatmentplan.Fig.4.Kaplan-Meier overall survival curves for all patients treated by 252Cf intracavitary brachytherapy with external-beam radiother-apy.4I.J.Radiation Oncology d Biology d Physics V olume -,Number -,2011and 68.5%and 55.9%,respectively (p =0.0003)(Fig.4).Disease-free 3-year and 5-year survival rates were 71.2%and 58.4%,respectively.Actuarial DFS rates at 3and 5years for Stages IB,IIA,IIB,IIIA,and IIIB patients were 86.8%and 77.2%,80.0%and 74.1%,71.9%and 60.5%,59.1%and 46.9%,and 65.5%and 42.5%,respectively (p =0.001)(Fig.5).There was no significant difference in survival rates between IB and IIA (p =0.681)or between IIIA and IIIB (p =0.608),whereas there were statistically significant dif-ferences among IB/IIA,IIB,and IIIA/IIIB using the log–rank test (p <0.05).Analysis of factors related to prognosis of cervical cancer The results of univariate analysis of factors related to prognosis in cervical cancer showed that stage,age,histopa-thology,histopathologic grade,and lymphatic metastasis were factors that influenced patient prognosis (Table 3).However,Cox multiple regression analysis showed that stage,histopathologic grade,tumor size,and lymphatic me-tastasis,but not age,were independently sigificant prognos-tic factors (Table 4).In addition,there was no significant difference between squamous cell carcinoma and adenocar-cinoma in our analysis.Late complicationsLate complications in our series were observed in the va-gina,rectum,urinary tract,and bowel and graded accord-ing to RTOG/EORTC scoring criteria.Of all,161patients (23.1%)developed late complications due to te radiation complications are shown in Table 5.The majority of late complications were at Grades 1and 2,and the most common late radiation complications were vaginal contracture and adhesion.The most common Grade 3complications were proctitis (1.1%)and hematuria (1.0%).The most common Grade 4complications were rectovaginal fistula (1.1%)and vesicovaginal fistula (0.6%).Two patients died of uncontrolled rectal bleeding,and 1patient died of rectovaginal fistula.Radiation procti-tis often occurred at 9months,and vaginal contracture and adhesion usually occurred 1year after completion of radio-therapy.Fig.5.Kaplan-Meier disease-free survival curves for all patients treated by 252Cf intracavitary brachytherapy with external-beam radiotherapy.Table 3.Factors relating to 3-year and 5-year overallsurvival Parametern 3-y (%)5-y (%)p Stage 0.0003IB 3195.084.4IIA 10485.377.7IIB 36376.266.1IIIA 6468.354.2IIIB 13468.555.9Age (y)0.011#5045878.268.6>5023871.957.5Histopathology0.452Squamous cell carcinoma 67876.165.8Adenocarcinoma1577.053.9Histopathologic grade (G)0.000G129848.934.4G231274.761.8G38685.077.0Tumor size (cm)0.003<424482.073.64–625876.764.8>619468.155.5Lymph node status 0.000Postive 15262.954.2Negative 33083.371.8Unknown21474.363.1Table 4.Multivariate analysis results for overall survival byCox multiple regression method Variables B Sig.Exp(B)95%CI for Exp(B)Stage 0.1930.006 1.213 1.056–1.393Age0.2870.051 1.3330.999–1.778Histopathologic grade À0.6710.0000.5110.419–0.624Tumor Size0.2640.004 1.302 1.090–1.557Lymph node status0.1880.0181.2071.032–1.411Abbrevaitions:Sig.=significance;CI =confidence interval.Table te radiation complications according to RTOG/EORTC scoring Late complication Grade 1Grade 2Grade 3Grade 4Grade 5Vaginal contracture and adhesion 22(3.2)10(1.4)6(0.9)2(0.3)Proctitis 19(2.7)11(1.6)8(1.1)9(1.3)3(0.4)Cystitis18(2.6)12(1.7)7(1.0)6(0.9)Inflammatory bowel 15(2.1)10(1.4)14(2.0)3(0.4)Total74(10.6)43(6.1)35(5.0)20(2.9)3(0.4)Abbreviation:RTOG/EORTC =radiation therapy oncology group/european organization for research and treatment of cancer.Values are number (percentage).252Cf brachytherapy for cervical cancer d X.L EI et al .5DISCUSSIONIonizing radiation can be divided into high-LET and low-LET.High-LET radiation involves particles,such as neu-trons,that are more effective in killing cells.The resistance of a tumor cell population to low-LET radiation might be one of the factors that cause failure of conventional radiotherapy in treatment of cervical cancer.The studies focusing on the cellular level of biological effects of252Cf demonstrated that the neutron component in the overall biological effect sur-passed that of g-radiation(25–27).The RBE value of neutrons is several times higher than that of photons.To achieve an equivalent biological effect to that of photons, clinicians may prescribe a lower total dose of neutrons in fewer fractions.Additionally,the results of clinical research on252Cf brachytherapy demonstrated that it is able to eliminate tumor cells resistant to conventional g-radiation(11,12).The procedure of252Cf-ICBT combined with EBRT ap-plied in our study was based on Maruyama’s empiricalfind-ings in an early application of the252Cf source in the initial phase of radiotherapy(26).In our series,252Cf-ICBT was started in the initial phase of radiotherapy(within1week of the initial EBRT).It then continued once per week,with the EBRT given on the other4days of the week.Thus the overall treatment time in our study was usually within6weeks be-cause of early application of the252Cf source in the initial phase of radiotherapy.Several studies have demonstrated that overall treatment time was a significant prognostic factor for patients with cervical cancer treated with radiotherapy (28–31).The American Brachytherapy Society also recommends keeping the total treatment duration to less than8weeks(32).In conventional photon brachytherapy (such as with192Ir or60Co),the ICBTwas started immediately or2weeks after the completion of EBRT,and the overall treatment time is usually7–9weeks(32–36).In addition,Maruyama et al.’s study(37)showed that higher fraction dose and lower fequency of252Cf-ICBT can attain better curative effects but have fewer complica-tions.Californium-252neutron therapy is suited to higher fractions and a shorter course of treatment,because a suffi-cient dose administered over a short time can kill hypoxic and radioresistant tumor cells and reduce tumor repopulation and radioresistant pared with higher-fraction dos-ing,lower-fraction dosing has a higher RBE value and may cause more complications.In our practice,patients were treated with252Cf brachytherapy,7–12Gy per insertion once per week.In contrast,the optimal dose for192Ir brachy-thepy was usually<7.5Gy per insertion(32).An important issue in the treatment of cervical cancer is reducing the incidence rate of late te com-plications in our series were observed in the vagina,rectum, bladder,and small bowel,as described and graded in Table5 according to RTOG/EORTC scoring criteria.Severe late rec-tal and bladder complications were relatively low,with crude incidence rates of2.8%and1.9%,respectively.Ferrigno et al.(38)reported that the5-year incidence rates of late complications in the rectum,bladder,and small bowel were16%,11%,and14%,respectively,whereas incidence rates of late complications were17.4%for Grade1/2, 10.9%for Grade3/4,and1.4%for Grade5(fatal)in patients treated with high-dose-rate192Ir ICBT.Considering these data,the incidence of late complications in our study was much lower(i.e.,7.1%for radiation proctitis,6.2%for radi-ation cystitis and4.9%for inflammatory bowel).The use of252Cf-ICBT for cervical cancer has distinct ad-vantages.However,252Cf has only been used for a short time,and further studies are needed to examine the best frac-tion dose and the suitable time of therapy as well as252Cf neutron brachytherapy-based concurrent chemoradiation. In addition,the application of neutron radiation in external irradiation of tumors is still problematic.CONCLUSIONThe results of our study show that the combined use of 252Cf-ICBT with ERBT is a highly effective approach for cervical cancer.Furthermore,complications in patients treated by252Cf-ICBT are not more frequent or severe than for those treated by conventional g-ICBT.REFERENCES1.Parkin DM,Bray F,Ferlay J,et al.Global cancer statistics,2002.CA Cancer J Clin2005;55:74–108.2.WHO/ICO Information Centre on HPV and Cervical Cancer(HPV Information Centre).Human papillomavirus and related cancers in China.Summary report2010.Available at:www.who.int/hpvcentre/en/.Accessed July16,2010.3.Keys HM,Bundy BN,Stehman FB,et al.Cisplatin,radiation,and adjuvant hysterectomy compared with radiation and adjuvant hysterectomy for bulky stage IB cervical carcinoma.N Engl J Med1999;340:1154–1161.4.Morris M,Eifel PJ,Lu J,et al.Pelvic radiation with concurrentchemotherapy compared with pelvic and para-aortic radiation for high risk cervical cancer.N Engl J Med1999;340:1137–1143.5.Rose PG,Bundy BN,Watkins EB,et al.Concurrent cisplatin-based radiotherapy and chemotherapy for locally advanced cervical cancer.N Engl J Med1999;340:1144–1153.6.Whitney CW,Sause W,Bundy BN,et al.Randomized compar-ison offluorouracil plus cisplatin versus hydroxyurea as an ad-junct to radiation therapy in stages IIB-IV A carcinoma of the cervix with negative para-aortic lymph nodes:A Gynecologic Oncology Group and Southwest Oncology Group study.J Clin Oncol1999;17(5):1339–1348.7.Peters WA3rd,Liu PY,Barrett RJ2nd,et al.Concurrent che-motherapy and pelvic radiation therapy compared with pelvic radiation therapy alone as adjuvant therapy after radical surgery in high-risk early-stage cancer of the cervix.J Clin Oncol2000;18:1606–1613.8.Thomson SG,Street K2nd,Chiroso A,et al.The new ele-ment californium(atomic number98).Phys Rev1950;80: 790–796.9.Schlea CS,Stoddard DH.Californium isotopes proposed forintracavitary and interstitial radiation therapy with neutrons.Nature1965;206:1058–1059.6I.J.Radiation Oncology d Biology d Physics V olume-,Number-,201110.Maruyama Y,van Nagell JR,Yoneda J,et al.A review ofcalifornium-252neutron brachytherapy for cervical cancer.Cancer1991;68:1189–1197.11.Tacev T,Ptackova B,Strnad V.Californium-252(252Cf)versusconventional gamma radiation in the brachytherapy of ad-vanced cervical carcinoma:Long-term treatment results ofa randomized study.Strahlenther Onkol2003;179:377–384.12.Maruyama Y,Kryscio R,van Nagell JR,et al.Neutron brachy-therapy is better than conventional radiotherapy in advanced cervical ncet1985;1:1120–1121.13.Maruyama Y,van Nagell JR,Yoneda J,et al.Feasibility studyof Californium-252for the therapy of stage IV cervical cancer.Cancer1988;61:2448–2452.14.Marjina LA.High dose rate252Cf neutron intraluminal brachy-therapy for treatment of cervical carcinoma and corpus carci-noma.Chin J Radiat Oncol1997;6:145–146.15.Zhao H,Wang K,Sun J,et al.Clinical report on external irra-diation combined with californium-252neutron intraluminal brachytherapy for cervical carcinoma treatment.Tumori 2007;93:636–640.16.Logsdon MD,Eifel PJ.FIGO IIIB squamous cell carcinomaof the cervix:An analysis of prognostic factors emphasizing the balance between external beam and intracavitary radia-tion therapy.Int J Radiat Oncol Biol Phys1999;43:763–775.17.Lowrey GC,Mendenhall WM,Million RR.Stage IB or IIA-Bcarcinoma of the intact uterine cervix treated with irradiation:A multivariate analysis.Int J Radiat Oncol Biol Phys1992;24:205–210.nciano RM,Martz K,Coia LR,et al.Tumor and treatmentfactors improving outcome in stage III-B cervix cancer.Int J Radiat Oncol Biol Phys1991;20:95–100.19.Benedet J,Odicino F,Maisonneuve P,et al.Carcinoma of thecervix uteri.J Epidemiol Biostat2001;6:7–43.20.Barillot I,Horiot JC,Pigneux J,et al.Carcinoma of the intactuterine cervix treated with radiotherapy alone:A French coop-erative study:Update and multivariate analysis of prognostic factors.Int J Radiat Oncol Biol Phys1997;38:969–978. 21.Shan J,Wang D,Lei X,et al.Review and analysis ofcalifornium-252neutron brachytherapy on cervical cancer in China.Chin Clin Oncol2009;14:803–807.22.International Commission on Radiological Protection.Rec-ommendations of the International Commission on Radiolog-ical Protection.ICRP publication26.Oxford:Pergamon;1997.23.Rjabukin JS.Relative biological effectiveness of252Cf[in Rus-sian].Med Radiol1985;30:53–59.24.Feola JM,Nava A,Maruyama Y.Biological effects of Cf-252neutrons at low dose rate.Int J Radiat Biol Relat Stud Phys Chem Med1982;41:33–46.25.Hall EJ.A comparison of radium and californium252usingcultured mammalian cells.A suggested extrapolation to radio-therapy.Radiology1972;102:173–179.26.Maruyama Y,Feola JM,Beach JL.HeLa cell tumor response to60Co,Cs-137,Cf-252radiations and cisplatin chemotherapy in nude mice.Cancer1984;54:247–252.27.Ban S,Iida S,Awa AA,et al.Lethal and mutagenic effects of252Cf radiation in cultured human cells.Int J Radiat Biol Relat Stud Phys Chem Med1987;52:245–251.28.Fyles A,Keane TJ,Barton M,et al.The effect of treatment du-ration in the local control of cervix cancer.Radiother Oncol 1992;25:273–279.nciano RM,Pajak TF,Martz K,et al.The influence of treat-ment time on outcome for squamous cell cancer of the uterine cervix treated with radiation:A patterns-of-care study.Int J Ra-diat Oncol Biol Phys1993;25:391–397.30.Perez CA,Grigsby PW,Castro-Vita H,et al.Carcinoma of theuterine cervix.1.Impact of prolongation of overall treatment time and timing of brachytherapy on outcome of radiation ther-apy.Int J Radiat Oncol Biol Phys1995;32:1275–1288.31.Girinsky T,Rey A,Roche B,et al.Overall treatment time in ad-vanced cervical carcinomas:A critical parameter in treatment outcome.Int J Radiat Oncol Biol Phys1993;27:1051–1056.32.Nag S,Erickson B,Thomadsen B,et al.The American Brachy-therapy Society recommendations for high-dose-rate brachy-therapy for carcinoma of the cervix.Int J Radiat Oncol Biol Phys2000;48:201–211.33.Eifel PJ,Morris M,Wharton T,et al.The influence of tumorsize and morphology on the outcome of patients with FIGO stage IB squamous cell carcinoma of the uterine cervix.Int J Radiat Oncol Biol Phys1994;29:9–16.34.Komaki R,Brickner TJ,Hanlon AL,et al.Long-term results oftreatment of cervical carcinoma in the United States in1973, 1978,and1983:Patterns of care study(PCS).Int J Radiat Oncol Biol Phys1995;31:973–982.35.Perez CA,Grigsby PW,Chao KS,et al.Tumor size,irradiationdose,and long-term outcome of carcinoma of uterine cervix.Int J Radiat Oncol Biol Phys1998;41:307–317.36.Kapp KS,Stuecklschweiger GF,Kapp DS,et al.Prognosticfactors in patients with carcinoma of the uterine cervix treated with external beam irradiation and IR-192high-dose-rate bra-chytherapy.Int J Radiat Oncol Biol Phys1998;42:531–540.37.Maruyama Y,Mesina J,Yudelev M,et al.New understandingfrom Cf brachytherapy trials and considerations for neutron therapy of bulky gyn carcinoma for future.Strahlenther Oncol 1994;170:253–263.38.Ferrigno R,dos Santos Novaes PE,Pellizzon AC,et al.High-dose-rate brachytherapy in the treatment of uterine cervix can-cer.Analysis of dose effectiveness and late complications.Int J Radiat Oncol Biol Phys2001;50:1123–1135.252Cf brachytherapy for cervical cancer d X.L EI et al.7。