博路定说明书
BD系列 闭式回路轴向柱塞传动单元 产品样本说明书

MAKING MODERN LIVING POSSIBLE产品样本BD系列闭式回路轴向柱塞传动单元产品样本BD系列 闭式回路轴向柱塞传动单元11012499 • AC • Jul 20109-2版本说明版本历史B D 系列 闭式回路轴向柱塞传动单元产品样本BD系列 闭式回路轴向柱塞传动单元11012499 • AC • Jul 20109-3BD 系列静液传动单元 .............................................................................................................................9-5BDU-10 S ,原理图 ....................................................................................................................................9-6BDU-21 L ,原理图.....................................................................................................................................9-7系统示意图, BDU-06/10S ........................................................................................................................9-8系统示意图, BDU-06/10S ........................................................................................................................9-8系统示意图, BDU-10L/21L/21H ............................................................................................................9-9系统示意图, BDU-10L/21L/21H, BDP-10L..........................................................................................9-9特征及可选项............................................................................................................................................9-10工作参数 .....................................................................................................................................................9-11传动油规格 ................................................................................................................................................9-11效率曲线 , BDU-06S, 10S ........................................................................................................................9-12效率曲线 , BDU-10L/21L, 21H, BDP-10L ...........................................................................................9-13概况 ...............................................................................................................................................................9-14输入速度 .....................................................................................................................................................9-14系统压力 .....................................................................................................................................................9-14补油压力 .....................................................................................................................................................9-15补油入口压力............................................................................................................................................9-15壳体压力 .....................................................................................................................................................9-15液压油 ..........................................................................................................................................................9-15温度及粘度 ................................................................................................................................................9-16液压油及过滤器.......................................................................................................................................9-17油箱 ...............................................................................................................................................................9-17控制轴作用力............................................................................................................................................9-17独立刹车系统............................................................................................................................................9-17主轴负载 .....................................................................................................................................................9-18轴选项 ..........................................................................................................................................................9-19旁通阀 ..........................................................................................................................................................9-21高压溢流阀(HPRV)及补油单向阀 (过压保护) ..............................................................................9-21带阻尼孔补油单向阀 .............................................................................................................................9-22可选集成油箱............................................................................................................................................9-24过滤器 ..........................................................................................................................................................9-24风扇 ...............................................................................................................................................................9-24概述工作参数系统设计参数特征及可选项技术规格目录产品样本BD系列 闭式回路轴向柱塞传动单元11012499 • AC • Jul 20109-4元件选型型号代码推荐安装及保养维护安装图纸最高系统压力............................................................................................................................................9-25 输入功率 .....................................................................................................................................................9-26 元件寿命 .....................................................................................................................................................9-27BDU 型号代码 ...........................................................................................................................................9-29 BDP 型号代码............................................................................................................................................9-31 壳体安装 .....................................................................................................................................................9-32 轴安装 ..........................................................................................................................................................9-32样机调试程序............................................................................................................................................9-32操作 ...............................................................................................................................................................9-32保养维护 .....................................................................................................................................................9-32BDU-06S .......................................................................................................................................................9-33 BDU-10S .......................................................................................................................................................9-35BDU-10L .......................................................................................................................................................9-35BDU-21L .......................................................................................................................................................9-39BDU-21H ......................................................................................................................................................9-39BDP-10L .......................................................................................................................................................9-43可选风扇 .....................................................................................................................................................9-43目录B D 系列 闭式回路轴向柱塞传动单元产品样本BD系列 闭式回路轴向柱塞传动单元11012499 • AC • Jul 20109-5BD 系列静液传动单元适应用于能量的传递及控制。
关于博路定
关于博路定®(恩替卡韦)片剂的指示和重要的安全信息:指示:博路定(恩替卡韦)是一种处方药,用于治疗慢性乙型肝炎病毒(HBV)有活跃的病毒和肝功能损害的成年人。
∙目前还没有治愈乙肝的方法。
BARACLUDE不会治愈乙肝∙BARACLUDE的可能:∙降低乙肝病毒在体内的量∙降低乙肝病毒的繁殖和感染新的肝细胞的能力∙改善肝脏的条件∙它不知道,是否BARACLUDE的会降低罹患肝癌或肝功能损害(肝硬化),这可能是造成的机会慢性乙肝病毒感染∙它不知道BARACLUDE的,如果是用于儿童的安全和有效的重要的安全信息:什么是最重要的信息,我应该知道的有关BARACLUDE的?∙您的乙肝病毒感染可能变得更糟,如果你停止服用BARACLUDE,这通常发生在6个月内后停止BARACLUDE的。
以BARACLUDE按照规定准确,不跑你的药或停止服用BARACLUDE您的医疗保健提供者交谈。
您的医疗保健提供者应监测您的健康,并定期进行血液检查检查您的肝脏,如果你停止服用BARACLUDE。
∙如果你有或艾滋病毒感染,不被用药物进行治疗,而服用BARACLUDE,艾滋病毒可能某些艾滋病毒药物产生耐药性,成为更难治疗。
你应该得到爱滋病病毒抗体测试,然后再开始服用BARACLUDE和随时随地后,当有机会接触到艾滋病毒。
BARACLUDE可能会导致严重的副作用,包括:∙乳酸性酸中毒(积聚在血液中的酸)。
有些人已经采取像BARACLUDE的BARACLUDE或药物的人已经开发出一种称为乳酸性酸中毒情况严重。
乳酸性酸中毒是一种严重的可造成死亡的紧急医疗必须在医院接受治疗。
BARACLUDE的普遍参与的患者病重由于他们的肝脏疾病或其他医疗条件的乳酸性酸中毒的报告。
∙马上打电话给你的医疗服务提供者,如果你:感觉非常虚弱或疲倦;有不寻常的(不正常)的肌肉疼痛;有麻烦呼吸,有恶心,呕吐,胃痛,觉得冷(尤其是在你的胳膊和腿);感到头晕目眩,或轻为首;有快速或不规则的心跳。
博路定说明书
博路定说明书【通用名】:恩替卡韦片【商品名】:博路定片【适应症】本品适用于病毒复制活跃,血清转氨酶ALT 持续升高或肝脏组织学显示有活动性病变的慢性成人乙型肝炎的治疗。
【汉语拼音】EntikaweiPian【英文名】:Entecavir Tablets【化学名】:其化学名称为2-氨基-9-[(1S,3R,4S)-4- 羟基-3-羟甲基-2-亚甲基环戊基卜1 ,9-二氢-6H-嘌呤-6-酮-水合物。
【成份】本品主要成分为:恩替卡韦。
【性状】本品为薄膜衣片,除去包衣后显白色。
【药理毒理】药理作用微生物学作用机制本品为鸟嘌呤核苷类似物,对乙肝病毒(HBV多聚酶具有抑制作用。
它能够通过磷酸化成为具有活性的三磷酸盐,三磷酸盐在细胞内的半衰期为15小时。
通过与HBV多聚酶的天然底物三磷酸脱氧鸟嘌呤核苷竞争,恩替卡韦三磷酸盐能抑制病毒多聚酶(逆转录酶)的所有三种活性:(1)HBV多聚酶的启动;(2)前基因组mRN逆转录负链的形成;(3)HBVDN正链的合成。
恩替卡韦三磷酸盐对HBVDN多聚酶的抑制常数(Ki)为0.0012卩M。
恩替卡韦三磷酸盐对细胞的a、B、$ DNA多聚酶和线粒体丫DNA多聚酶抑制作用较弱,Ki 值为18至于160卩M抗病毒活性在转染了野生型乙肝病毒的人类HepG2细胞中,恩替卡韦抑50%^毒DNA合成所需浓度(EC50为0.004卩M恩替韦对拉米夫定耐药病毒株(rtL180M,rtM204V )的EC50 的中位值是0.26卩M范围0.01至0.059卩M),而恩替卡韦对在细胞培养液中生长的1型人类免疫缺陷(HIV)无临床相关活性(EC50>1Qx M)o每天或每周一次使用本品能降低北美土拨鼠的长期研究表明,每周口服0.5mg/kg恩替卡韦(相当于人体1.0mg的剂量)能将其中的3只土拨鼠的病毒DNA保持在不可测水平(病毒DNA水平<200拷贝/ml , PCRt)长达3年之久。
DIDS_阴离子运输抑制剂_67483-13-0_Apexbio

Limited solubility
Store at +4°C
For obtaining a higher solubility , please warm the tube at 37°C and shake it in the ultrasonic bath for a while.Stock solution can be stored below -20°C for several months.
实验操作
细胞实验: 细胞系 溶解方法
反应时间 应用
来源于 6-8 周龄 Sprague-Dawley 大鼠的 DRG(背根神经节)神经 元细胞
在 DMSO 中的溶解度>10mM。为了获得更高的浓度,可以将离心 管在 37℃加热 10 分钟和/或在超声波浴中震荡一段时间。原液可 以在-20℃以下储存几个月
0.1, 1, 3, 10, 100μm 作用 2min,加入第一滴药物开始同时观察
在 DGR 神经元中,尽管 DIDS 并没有诱导 TRPV1(瞬时受体电位 香草酸亚型 1 型)自身的活化,但是显著提高了辣椒素或低 pH 诱导的 TRPV1 电流。DIDS 可以以激动剂依赖的方式改变 TRPV1 通道功能。
请测试所有化合物在室内的溶解度,实际溶解度和理论值可能略 有不同。这是由实验系统的误差引起的,属于正常现象。
参考文献: [1] Wulff, Heike. "New light on the “Old” chloride channel blocker DIDS." ACS chemical biology 3.7 (2008): 399-401. [2] Hogg, R. C., Q. Wang, and W. A. Large. "Effects of Cl channel blockers on Ca‐activated chloride and potassium currents in smooth muscle cells from rabbit portal vein." British journal of pharmacology 111.4 (1994): 1333-1341. [3] Nelson, Mark T., et al. "Chloride channel blockers inhibit myogenic tone in rat cerebral arteries." The Journal of Physiology 502.2 (1997): 259-264. [4] Lyons, John C., Brian D. Ross, and Chang W. Song. "Enhancement of hyperthermia effect in vivo by amiloride and DIDS." International Journal of Radiation Oncology* Biology* Physics 25.1 (1993): 95-103
Philips HeartStart Intrepid监护 除颤器TBI建议说明书
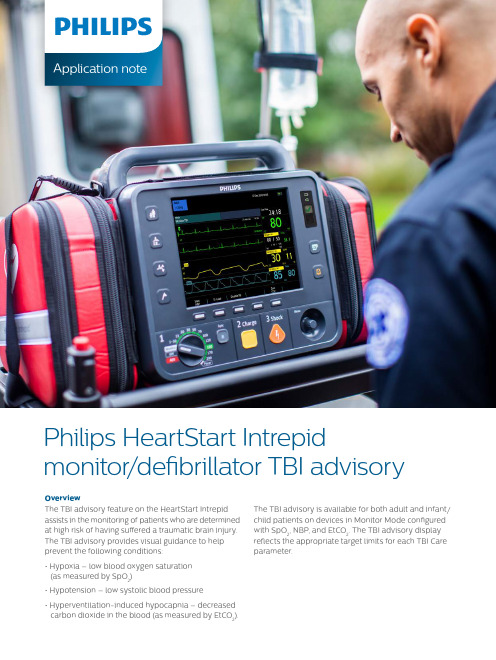
Application notePhilips HeartStart Intrepidmonitor/defibrillator TBI advisory OverviewThe TBI advisory feature on the HeartStart Intrepidassists in the monitoring of patients who are determinedat high risk of having suffered a traumatic brain injury.The TBI advisory provides visual guidance to helpprevent the following conditions:• Hypoxia – low blood oxygen saturation(as measured by SpO 2)• Hypotension – low systolic blood pressure• Hyperventilation-induced hypocapnia – decreasedcarbon dioxide in the blood (as measured by EtCO 2).The TBI advisory is available for both adult and infant/child patients on devices in Monitor Mode configured with SpO 2, NBP, and EtCO 2. The TBI advisory display reflects the appropriate target limits for each TBI Care parameter.IntroductionEvery year, 2.2 million people in the UnitedStates suffer a traumatic brain injury (TBI), with approximately 52,000 deaths and 280,000 hospitalizations.1 The economic burden of TBI is more than USD 60 billion per year.1 TBI occurs when an external mechanical force inflicts sudden trauma to the head disrupting the normal function of the brain.2However, subsequent preventable (secondary) injury to the brain can add dramatically to the primary injury, and the extent of damage during this time is significantly influenced by the early care the patient receives.3 The emphasis on early recognition and early treatment of TBI should be similar to that of other pathologies where survivability and recovery are time-dependent, i.e., sudden cardiac arrest.4TBI PathophysiologyThe brain accounts for the consumption of 20% of bodily oxygen and 25% of the blood glucose. Because of this, cerebral blood flow (CBF) is critical for ensuring adequate brain metabolism and preventing cerebral ischemia. CBF is a function of cerebral perfusion pressure (CPP) and cerebral vascular resistance (CVR), CPP is calculated by subtracting intracranial pressure (ICP) from mean arterial blood pressure (MAP) (CPP= MAP-ICP). Normal ICP ranges from 10-15 mmHg, and normal MAP ranges from 70-95 mmHg; therefore, the average CPP is approximately 60-80 mmHg. CBF is regulated through several mechanisms in the healthy patient; however, disruption of those mechanisms can have catastrophic consequences on the brain and its control of body systems.ICP and TBIThe cerebrum, cerebellum, and brainstem use approximately 80% of the intracranial space (1,200 cc), with blood vessels and cerebral spinal fluid utilizing the remaining volume at 12% (150 cc) and 8% (90 cc), respectively. Cerebral swelling and hemorrhage secondary to TBI increase the cerebral volume and require the body to compensate for the increased volume by reducing the volume of other brain structures and cerebrospinal fluid within the cranium. If the amount of room available to compensate forthe increasing volume is less than the expanding volume, then an increase in ICP will occur. Initially,the brain compensates for an increase in cerebral mass by compressing the cerebral venous blood vessels and, as cerebral volume continues to increase, cerebrospinal fluid is pushed from the skull into the spinal space. The initial compensatory mechanisms can maintain ICP close to normal; however, once those mechanisms are exhausted, ICP quickly rises. The continued increase in ICP impedes arterial flow into the cranial space and constricts cerebral blood vessels. These mechanisms decrease CBF and, subsequently, the cardiocerebrovascular system attempts to compensate for the decreased CBF by increasing SBP. This further increases ICP.The decreased CBF also causes cerebral ischemiaand neuronal hypoxia. If spontaneous ventilationis compromised, pCO2increases, and this results in cerebral vasodilation and additional increases in ICP. Cerebral edema secondary to neuronal injury and cerebral ischemia leads to a further exacerbation of ICP. Ultimately, the continued increase of ICP will lead to profoundly compromised CBF, resulting in death. Figure 1.552Three critical factors of TBI (the 3 H-Bombs)The National EMS TBI Guidelines published by theBrain Trauma Foundation emphasize the importanceof maintaining adequate cerebral oxygenation andperfusion by avoiding three critical factors.7• Hypoxia• Hypotension• Hyperventilation (that leads to hypocapnea andcerebral vasoconstriction)A single incidence of any one of these factorsdramatically increases patient mortality.3 However,maintaining End-Tidal Carbon Dioxide (EtCO2), arterialblood oxygenation (SpO2), and a systolic bloodpressure (SBP) within guidelines established by theTraumatic Brain Injury Foundation have demonstratedimproved outcomes in patients with severe TBI.3HypocapniaPreventing hyperventilation induced hypocapnia(EtCO2<32 mmHg) is critical because of its directcorrelation to CBF.3,7 For example, a patient who hasa pCO2 of 40 mmHg has a CBF of 50 ml per 100g ofbrain tissue per minute.8 However, if pCO2drops to30 mmHg, then CBF will drop to 40ml per 100g ofbrain tissue per minute, a 20% decrease in CBF.8 Therelationship between CBF and pCO2is so delicate thata 1 mmHg change in pCO2can alter CBF up to 5% anddecreasing pCO2by relatively little (i.e., <32 mmHg) isassociated with significant mortality.3,8-10Unfortunately, unrecognized inadvertenthyperventilation in TBI patients is still a majorproblem, at least in the prehospital environment. Inthe San Diego RSI Trial, 59% of patients intubatedbefore arriving at the hospital experienced at leastone incident of hyperventilation resulting in anEtCO2value of less than 25 mmHg.9 The importanceof monitoring EtCO2cannot be overstated. Onestudy observed that prehospital intubation in asetting where capnography was not used reporteda mortality rate of 33%; conversely, the ability tomonitor patients’ EtCO2level and use a ventilator wasassociated with a statistically significant, 18% lowerrelative rate of death.11Figure 1: Relationship between increased intracranial pressure and decreased cerebral perfusion.34Hypotension and hypoxiaMultiple studies have demonstrated a strong correlationbetween a single episode of hypotension (SBP <90mmHg) or hypoxia (SpO 2<90%) and decreased patientsurvival.7,12-14 Independently, hypotension or hypoxiahave a dramatic deleterious effect on patient mortality.However, when a patient experiences both hypotensionand hypoxia, the adjusted probability of death doublesagain (beyond that of either alone).15The Excellence in Prehospital Injury Care (EPIC)TBI study examined the outcome of 13,151 patientswho had suffered major (moderate/severe/critical)TBI over a seven-year period. The researcherscompared the mortality rate of patients whoexperienced neither hypoxia nor hypotension(n=11,545), hypotension only (n=604), hypoxia only(n=790), or hypotension and hypoxia (n=212) in theprehospital environment.15 The study concludedthat having at least one episode of hypotension orhypoxia (alone) resulted in a 20.7% (n=125) and 28.1%(n=222) mortality rate, respectively. The combinationof both hypoxia and hypotension was associated witha 43.9% (n=93) mortality rate.15 Comparatively, patients who did not experience hypoxia or hypotension had a 5.6% (n=644) rate of death.15 The adjusted analysis found that a patient that experiences both hypotension and hypoxia in the prehospital environment has a 600% (aOR = 6.1) higher likelihood of dying than someone who experiences neither.15Another important finding of the EPIC TBI study was the absence of any identifiable SBP threshold in relation to patient mortality. The study identified that over the range of 40 mmHg to 120 mmHg SBP there was a consistent decrease in survival for every 10 mmHg drop and a progressive association between decreasing SBP and both unadjusted and adjusted risk of death.1 In other words, a patient with a SPB of 60 mmHg is 4 times as likely to die than a patient with a SBP of 135 mmHg.1 The implications are obvious: the injured brain is highly sensitive to a lack of perfusion, and the levels of systemic blood pressure associated with increased mortality may be far above the “classic” threshold for “hypotension” (SBP<90 mmHg).1Importance of treating and preventing hypotension, hypoxia, and hypocapnia Researchers from the EPIC TBI study worked with ArizonaEMS agencies to implement prehospital TBI guidelinesfocusing on three areas of prevention and treatment (thethree “H-Bombs”):• Preventing and treating hypoxia by use of high-flowO 2 and emphasis on basic airway maneuvers• Preventing and treating hypotension by rapidlyinfusing isotonic fluids• Preventing hyperventilation by using appropriateventilation rates, adjuncts, and EtCO 2In the EPIC Study, adjusted survival to hospital dischargedoubled (aOR 2.03) for patients with severe TBI (headregion severity score = 3-4) and tripled (aOR 3.28) forpatients with severe TBI that also received positivepressure ventilation (PPV) via bag-valve mask orendotracheal intubation (ETI). The increased survival ofpatients with severe TBI receiving PPV was attributedto the emphasis on maintaining EtCO 2 between 35 and 45 mmHg, rate-timers that gave visual cues for proper manual ventilation and using flow-controlled ventilation bags to help prevent hyperventilation and overventilation.One of the most important findings of the EPIC Study was that the initial improvement of patient survival faded over time, and this was most likely because of the diminished emphasis on following the prehospital TBI guidelines. The researchers could not require retraining of the study participants. Therefore, a method of ensuring that hypoxia, hypotension, and hypocapnea are recognized early should be available to all prehospital providers. The authors concluded that their findings make it likely that the use of monitoring technology that can give cues and real-time feedback to providers during the resuscitation of brain injured patients will improve outcomes by helping to prevent secondary brain injury from hypoxia, hypotension, and hyperventilation.10HeartStart Intrepid Traumatic Brain Injury advisory OverviewThe TBI advisory feature on the HeartStart Intrepidassists in the monitoring of patients who are determinedat high risk of having suffered a traumatic brain injury.The TBI advisory provides visual guidance to helpprevent the following conditions:• Hypoxia – low blood oxygen saturation (asmeasured by SpO2)• Hypotension – low systolic blood pressure• Hyperventilation-induced hypocapnea – decreasedcarbon dioxide in the blood (as measured by EtCO2).The TBI Advisory is available for both adult and infant/child patients on devices in Monitor Mode configuredwith SpO2, NBP, and EtCO2. The TBI Advisory displayreflects the appropriate target limits for each TBI Care parameter.Notes:• These limits must be pre-established andpre-configured prior to using this feature (see “Configuration – TBI Advisory” in the HeartStart Intrepid Instructions for Use).• If a physiological alarm condition occurs, it will have a higher priority than the TBI advisory and will obscure the TBI Indicators.56Enabling the TBI advisory1. TBI: Ensure an SpO 2 sensor, NBP cuff, and EtCO 2 tubing are connected to the patient2. Press the [Enable TBI] soft key.If no patient age has been entered, the Patient Age number selector appears.3. If prompted, enter the patient age.The patient age is displayed in the status area next to patient name/ID.When age is entered, mode text changes from Monitor to Monitor TBI.Notes:• The TBI Advisory is only available in Monitor Mode and is not available during the acquisition of a 12-lead ECG.• Devices must be configured with SpO 2, NBP, andEtCO 2 measurement parameters, and all threeparameters must be in use.• TBI Advisory can only be enabled when TBI limits are pre-configured on the device.• The neonatal patient category is not supported.Displaying the TBI advisoryThe TBI advisory display appears in the numeric parameter area. A TBI limit bar is displayed at the top of the corresponding measure box for NBP , EtCO 2, and SpO 2.TBI for systolic blood pressure (SBP)Systolic blood pressure that falls outside theestablished TBI limits is indicated by a yellow bar, and TBI SBP > High Limit or TBI SBP < Low Limit is displayed, as shown in Figure 2.Systolic blood pressure within limits the setting for the TBI configuration is indicated by TBI SBP on a green bar, as shown in Figure 3.TBI for EtCO 2 If the EtCO 2 value falls outside the established TBI limits, TBI EtCO 2 > High Limit or TBI EtCO 2 < Low Limit is displayed in a yellow TBI bar as shown in Figure 4.If the EtCO 2 value is within the limits setting for the TBI configuration, TBI EtCO 2 is displayed in a green bar as shown in as shown in Figure 5.WARNING: To ensure correct functioning of the CO 2 measurement, use only approved CO 2 accessories as listed in the HeartStart Intrepid Instructions for Use, Chapter 18:Supplies and Accessories.Figure 5: TBI within limits.Figure 2: TBI outside limits.Figure 3: TBI within limits.Figure 4: TBI outside limits.7TBI for SpO 2For SpO 2, there is no upper limit, only a lower limitthreshold for SpO 2 is set. If the SpO 2 value falls belowthe established TBI limit, TBI SpO 2 < Low Limit isdisplayed on a yellow TBI bar as shown in Figure 6.If the SpO 2 value is above the limit set for the TBIconfiguration, the TBI bar is green, and the text TBI SpO 2is displayed on a green bar as shown in Figure 7.Figure 6: SPO 2below TBI limit.Figure 7: SPO 2 above TBI limit.References1. Spaite, D. W., Hu, C., Bobrow, B. J., Chikani, V., Sherrill,D., Barnhart, B., . . . Adelson, P. D. (2017). Mortality andprehospital blood pressure in patients with majortraumatic brain injury: Implications for the hypotension threshold. JAMA Surgery, 152(4), 360-368.2. Rosenfeld, J. V., Maas, A. I., Bragge, P., Morganti-Kossmann, M. C., Manley, G. T., & Gruen, R. L. (2012).Early management of severe traumatic brain injury.The Lancet, 380(9847), 1088-1098.3. Spaite, D. W., Bobrow, B. J., Stolz, U., Sherrill, D., Chikani,V., Barnhart, B., . . . Denninghoff, K. R. (2014). Evaluation of the impact of implementing the emergency medical services traumatic brain injury guidelines in arizona:The excellence in prehospital injury care (epic) study methodology. Academic Emergency Medicine, 21(7), 818-830. doi:doi:10.1111/acem.12411.4. Gaither, J. B., Spaite, D. W., Bobrow, B. J., Denninghoff,K. R., Stolz, U., Beskind, D. L., & Meislin, H. W. (2012).Balancing the potential risks and benefits of out-of-hospital intubation in traumatic brain injury:The intubation/hyperventilation effect. Annals ofEmergency Medicine, 60(6), 732-736.5. Bledsoe, B. E., Porter, R. S., & Cherry, R. A. (2001). Head,facial, and neck trauma. In Paramedic care: Principles & practices trauma emergencies (1 ed., Vol. 4, pp. 285-286). Upper Saddle River, NJ: Prentice Hall.6. Sanders, M. J. (2012). General principles ofpathophysiology. In K. McKenna, L. M. Lewis, & G.Quick (Eds.), Mosby’s paramedic textbook (4th ed., pp.211-256). Burlington, MA: Jones & Bartlett Learning.7. Carney, N., Totten, A. M., O’Reilly, C., Ullman, J. S.,Hawryluk, G. W., Bell, M. J., . . . Ghajar, J. (2017).Guidelines for the management of severe traumaticbrain injury, fourth edition. Neurosurgery, 80(1), 6-15.doi:10.1227/NEU.0000000000001432.8. Giardino, N. D., Friedman, S. D., & Dager, S. R.(2007). Anxiety, respiration and cerebral bloodflow: Implications for functional brain imaging.Comprehensive Psychiatry, 48(2), 103-112.9. Davis, D. P., Heister, R., Poste, J. C., Hoyt, D. B., Ochs, M.,& Dunford, J. V. (2005). Ventilation patterns in patients with severe traumatic brain injury following paramedic rapid sequence intubation. Neurocritical Care, 2(2),165-171. 10. Spaite, D. W., Bobrow, B. J., Keim, S. M., Barnhart, B.,Chikani, V., Gaither, J. B., . . . Hu, C. (2019). Association of statewide implementation of the prehospital traumatic brain injury treatment guidelines with patient survival following traumatic brain injury: The excellence inprehospital injury care (epic) study. JAMA Surgery,e191152-e191152. doi:10.1001/jamasurg.2019.1152.11. Poste, J. C., Davis, D. P., Ochs, M., Vilke, G. M.,Castillo, E. M., Stern, J., & Hoyt, D. B. (2004). Airmedical transport of severely head-injured patientsundergoing paramedic rapid sequence intubation.Air Medical Journal, 23(4), 36-40. doi:https://doi.org/10.1016/j.amj.2004.04.006.12. Shutter, L. A., & Narayan, R. K. (2008). Blood pressuremanagement in traumatic brain injury. Annals ofEmergency Medicine, 51(3, Supplement), S37-S38.doi:https:///10.1016/j.annemergmed.2007.11.013.13. Cormio, M., Robertson, C. S., & Narayan, R. K. (1997).Secondary insults to the injured brain. Journal ofClinical Neuroscience, 4(2), 132-148. doi:https://doi.org/10.1016/S0967-5868(97)90062-X.14. Manley, G. (2001). Hypotension, hypoxia, and headinjury: Frequency, duration, and consequences.Archives of Surgery, 136(10), 1118-1123.15. Spaite, D. W., Hu, C., Bobrow, B. J., Chikani, V., Barnhart,B., Gaither, J. B., . . . Sherrill, D. (2017). The effect ofcombined out-of-hospital hypotension and hypoxia on mortality in major traumatic brain injury. Annalsof Emergency Medicine, 69(1), 62-72. doi:10.1016/j.annemergmed.2016.08.007.8。
Dipyridamole_PDE抑制剂_58-32-2_Apexbio
特别声明
产品仅用于研究, 不针对患者销售,望谅解。 每个产品具体的储存和使用信息显示在产品说明书中。ApexBio 产品在推荐的条件下是稳定 的。产品会根据不同的推荐温度进行运输。许多产品短期运输是稳定的,运输温度不同于长 期储存的温度。我们确保我们的产品是在保持试剂质量的条件下运输的。收到产品后,按照 产品说明书上的要求进行储存。
ApexBio Technology
产品说明书
化学性质
产品名: Cas No.: 分子量: 分子式:
Dipyridamole 58-32-2 504.63 C24H40N8O4
产品名: Dipyridamole 修订日期: 6/30/2016
ቤተ መጻሕፍቲ ባይዱ
化学名: SMILES: 溶解性: 储存条件: 一般建议:
运输条件:
生物活性
靶点 : 信号通路: 产品描述: Dipyridamole 参考文献:
>15.6mg/mL in DMSO
Store at -20°C
For obtaining a higher solubility , please warm the tube at 37°C and shake it in the ultrasonic bath for a while.Stock solution can be stored below -20°C for several months.
2-[[2-[bis(2-hydroxyethyl)amino]-4,8-di(piperidin-1-yl)pyrimido[5,4d]pyrimidin-6-yl]-(2-hydroxyethyl)amino]ethanol
恩替卡韦说明书

恩替卡韦说明书【通用名】恩替卡韦片【商品名】博路定【性状】本品为薄膜衣片,除去包衣后显白色。
【规格】铝箔包装,0.5毫克,7片/盒【用途】本品用于肝胆胰用药或肝炎用药;适用于病毒复制活跃,血清转氨酶ALT持续升高或肝脏组织学显示有活动性病变的慢性乙型肝炎的治疗。
【用法用量】服用恩替卡韦应在专业医生指导下服用。
推荐剂量为:16岁以上青年和成人口服本品,0.5mg/天;建议本品空腹服用或餐前、餐后至少2个小时。
在肾功能不全的患者中,恩替卡韦口服清除率会随肌酐清除率的降低而降低,当肌酐清除率<50ml/分钟的患者应调整用药剂量;而肝功能不全患者无需调整用药剂量。
【耐药性】体外研究没有发现与恩替卡韦耐药相关的基因型或表型证据。
【不良反应】恩替卡韦治疗普遍出现的不良反应有:头痛、眩晕、疲劳、恶心等。
【禁忌事项】对恩替卡韦或制剂中任何成分过敏者禁用;妊娠、哺乳期妇女慎用。
【注意的事项】1.应在医生的指导下服用恩替卡韦,并对任何新出现的异常症状及合并用药情况及时告诉主管医生。
2.恩替卡韦不可擅自停药,因为擅自停药后可能会出现肝炎病情急速加重的情况,3.恩替卡韦服用后若出现过敏反应或服用期间若出现明显不适症状,应及时与医生联系,以便采取相应的措施;若出现耐药现象,应在专业医生的指导下改变治疗方法。
4.使用恩替卡韦治疗的患者并不能降低经性接触或污染血源传播HBV的危险性,因此,需要采取适当的防护措施。
【药物过量】据调查发现,在健康人群中单次给药达40毫克或连续14天多次给药20mg/天后,未观察到不良现象,建议:如果发生药物过量,须监测患者的毒性指标,必要时进行支持疗法。
【贮藏】需密封,15-30℃干燥处保存。
【通用名】恩替卡韦片【商品名】博路定【性状】本品为薄膜衣片,除去包衣后显白色。
【规格】铝箔包装,0.5毫克,7片/盒【用途】本品用于肝胆胰用药或肝炎用药;适用于病毒复制活跃,血清转氨酶ALT持续升高或肝脏组织学显示有活动性病变的慢性乙型肝炎的治疗。
SUBLOCADE 说明书
MEDICATION GUIDESUBLOCADE(SUB-lo-kade) (buprenorphine extended-release) injection, for subcutaneous use, (CIII)What is the most important information I should know about SUBLOCADE?•Because of the serious risk of potential harm or death from self-injecting SUBLOCADE into a vein (intravenously), it is only available through a restricted program called the SUBLOCADE REMS Program.•SUBLOCADE is not available in retail pharmacies.•Your SUBLOCADE injection will only be given to you by a certified healthcare provider.•SUBLOCADE contains a medicine called buprenorphine. Buprenorphine is an opioid that can cause serious and life-threatening breathing problems, especially if you take or use certain other medicines or drugs.•Talk to your healthcare provider about naloxone. Naloxone is a medicine that is available to patients for the emergency treatment of an opioid overdose. If naloxone is given, you must call 911 or get emergency medical help right away to treat overdose or accidental use of an opioid.•SUBLOCADE may cause serious and life-threatening breathing problems. Get emergency help right away if you:•feel faint•feel dizzy•are confused•Feel sleepy or uncoordinated •have blurred vision•have slurred speech•are breathing slower than normal •cannot think well or clearlyDo not take certain medicines during treatment with SUBLOCADE. Taking other opioid medicines, benzodiazepines, alcohol, or other central nervous system depressants (including street drugs) while on SUBLOCADE can cause severe drowsiness, decreased awareness, breathing problems, coma, and death.•In an emergency, have family members tell emergency department staff that you are physically dependent on an opioid and are being treated with SUBLOCADE.•You may have detectable levels of SUBLOCADE in your body for a long period after stopping treatment with SUBLOCADE.What is SUBLOCADE?SUBLOCADE is a prescription medicine used to treat adults with moderate to severe addiction (dependence) to opioid drugs (prescription or illegal) who:•have received treatment with an oral transmucosal (used under the tongue or inside the cheek) buprenorphine-containing medicine for 7 days and•are taking a dose that controls withdrawal symptoms for at least seven days.•SUBLOCADE is part of a complete treatment plan that should include counseling.Who should not take SUBLOCADE?Do not use SUBLOCADE if you are allergic to buprenorphine or any ingredient in the prefilled syringe (ATRIGEL® delivery system). See the end of this Medication Guide for a list of ingredients in SUBLOCADE.Before starting SUBLOCADE, tell your healthcare provider about all your medical conditions, including if you have:•trouble breathing or lung problems• a curve in your spine that affects your breathing •Addison’s disease •an enlarged prostate (men)•problems urinating•liver, kidney, or gallbladderproblems•alcoholism• a head injury or brainproblem•mental health problems•adrenal gland or thyroidgland problemsTell your healthcare provider if you are:•pregnant or plan to become pregnant. If you receive SUBLOCADE while pregnant, your baby may have symptoms of opioid withdrawal at birth that could be life-threatening if not recognized and treated. Talk to your healthcare provider if you are pregnant or plan to become pregnant.•breastfeeding or plan to breastfeed. SUBLOCADE can pass into your breast milk and harm your baby. Talk to your healthcare provider about the best way to feed your baby during treatment with SUBLOCADE. Monitor your baby for increased drowsiness and breathing problems if you breastfeed during treatment with SUBLOCADE.Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins and herbal supplements.How will I receive SUBLOCADE?•You will receive SUBLOCADE by your healthcare provider as an injection just under the skin (subcutaneous) of your stomach (abdomen). You will receive SUBLOCADE monthly (with at least 26 days between doses). •SUBLOCADE is injected as a liquid. After the injection, SUBLOCADE changes to a solid form called a depot. The depot may be seen or felt as a small bump under your skin at the injection site on your abdomen for several weeks. The depot will get smaller over time.•Do not try to remove the depot.•Do not rub or massage the injection site.•Try not to let belts or clothing waistbands rub against the injection site.•If you miss a dose of SUBLOCADE, see your healthcare provider to get your SUBLOCADE injection as soon as possible.What should I avoid while being treated with SUBLOCADE?•Do not drive, operate heavy machinery, or perform any other dangerous activities until you know how SUBLOCADE affects you. Buprenorphine can cause drowsiness and slow reaction times. SUBLOCADE can make you sleepy, dizzy, or lightheaded. This may happen more often in the first few days after your injection and when your dose is changed.•You should not drink alcohol or take prescription or over-the-counter medicines that contain alcohol during treatment with SUBLOCADE, because this can lead to loss of consciousness or even death.What are the possible side effects of SUBLOCADE?SUBLOCADE can cause serious side effects, including:•Trouble breathing. Taking other opioid medicines, benzodiazepines, alcohol, or other central nervous system depressants during treatment with SUBLOCADE can cause breathing problems that can lead to coma and death. •Sleepiness, dizziness, and problems with coordination.•Physical dependence.•Liver problems. Call your healthcare provider right away if you notice any of these symptoms:•your skin or the white part of your eyes turns yellow (jaundice)•dark or “tea-colored” urine•light colored stools (bowel movements) •loss of appetite•pain, aching, or tenderness on the right side of your stomach area•nausea•Your healthcare provider should do blood tests to check your liver before you start and during treatment with SUBLOCADE.•Allergic reaction. You may have a rash, hives, swelling of your face, wheezing, low blood pressure, or loss of consciousness. Call your healthcare provider or get emergency help right away.•Opioid withdrawal. Call your healthcare provider right away if you get any of these symptoms:•shaking•sweating more than normal •feeling hot or cold more than normal •runny nose•watery eyes •goose bumps •diarrhea •vomiting •muscle aches•Decrease in blood pressure. You may feel dizzy when you get up from sitting or lying down. •The most common side effects of SUBLOCADE include:•constipation •headache •vomiting•increase in liver enzymes•nausea •injection site itching •tiredness •injection site pain•SUBLOCADE may affect fertility in males and females. Talk to your healthcare provider if this is a concern for you. These are not all the possible side effects of SUBLOCADE.Call your doctor for medical advice about side effects. You may report side effects to the FDA at 1-800-FDA-1088. General information about SUBLOCADEMedicines are sometimes prescribed for purposes other than those listed in a Medication Guide. You can ask your doctor or pharmacist for information that is written for healthcare professionals.What are the ingredients in SUBLOCADE?Active ingredient: buprenorphineATRIGEL® delivery system: biodegradable 50:50 poly(DL-lactide-co-glycolide) polymer and a biocompatible solvent, N-methyl-2-pyrrolidone (NMP).© 2022, Indivior UK Limited. All Rights Reserved.SUBLOCADE® is a registered trademark of Indivior UK Limited.Manufactured by Curia Global Inc. Albany, NY 12203For more information, go to or call 1-877-782-6966.This Medication Guide has been approved by the U.S. Food and Drug Administration. Issued: 08/2022。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
博路定说明书【通用名】:恩替卡韦片【商品名】:博路定片【适应症】本品适用于病毒复制活跃,血清转氨酶ALT持续升高或肝脏组织学显示有活动性病变的慢性成人乙型肝炎的治疗。
【汉语拼音】EntikaweiPian【英文名】:Entecavir Tablets【化学名】:其化学名称为2-氨基-9-[(1S,3R,4S)-4-羟基-3-羟甲基-2-亚甲基环戊基]-1,9-二氢-6H-嘌呤-6-酮-水合物。
【成份】本品主要成分为:恩替卡韦。
【性状】本品为薄膜衣片,除去包衣后显白色。
【药理毒理】药理作用微生物学作用机制本品为鸟嘌呤核苷类似物,对乙肝病毒(HBV)多聚酶具有抑制作用。
它能够通过磷酸化成为具有活性的三磷酸盐,三磷酸盐在细胞内的半衰期为15小时。
通过与HBV多聚酶的天然底物三磷酸脱氧鸟嘌呤核苷竞争,恩替卡韦三磷酸盐能抑制病毒多聚酶(逆转录酶)的所有三种活性:(1)HBV多聚酶的启动;(2)前基因组mRNA逆转录负链的形成;(3)HBVDNA正链的合成。
恩替卡韦三磷酸盐对HBVDNA多聚酶的抑制常数(Ki)为μM。
恩替卡韦三磷酸盐对细胞的α、β、δDNA多聚酶和线粒体γDNA多聚酶抑制作用较弱,Ki值为18至于160μM。
抗病毒活性在转染了野生型乙肝病毒的人类HepG2细胞中,恩替卡韦抑50%病毒DNA合成所需浓度(EC50)为μM。
恩替韦对拉米夫定耐药病毒株(rtL180M,rtM204V)的EC50的中位值是μM(范围至μM),而恩替卡韦对在细胞培养液中生长的1型人类免疫缺陷(HIV)无临床相关活性(EC50>10μM)。
每天或每周一次使用本品能降低北美土拨鼠的长期研究表明,每周口服kg恩替卡韦(相当于人体的剂量)能将其中的3只土拨鼠的病毒DNA保持在不可测水平(病毒DNA水平<200拷贝/ml,PCR法)长达3年之久。
在任何使用该药治疗长达3年的动物中,未发现HBV多聚酶发生耐药相关性的变化。
耐药性体外研究在细胞试验中发现,拉米夫定耐药的病毒株对恩替卡韦怕显型敏感性降低8至30倍。
如果乙肝病毒多聚酶本来就存在对拉米夫定耐药的氨基酸置换(rtL180M和/或rtLM204V/I),再加上rtT184,rtS202或rtM250位点的置换变异,都会造成对恩替卡韦的显型敏感受性降低更多(>70倍。
)临床研究核苷类药物初治患者:81%的核苷类药物初治病人在口服恩替卡韦天48周后,病毒载量达到<300拷贝/mL。
HbeAg阳性(AI463022研究,n=219)或HbeAg阴性(AI463027研究,n=211)的核苷类药特初治患者在治疗48周后,基因型分析结果表明HBVDNA多聚酶的基因没有发生与表型耐药相关基因型变异。
在AI463022研究中,有2名病人发生了病毒学反弹(HBVDNA从最低上升1个log10),但没有发现与恩替卡韦耐药相关的基因型或表型证据。
拉米夫定治疗失效的患者:22%的拉米夫定失效病人在口服恩替卡韦天48周后,病毒载量达到<300拷贝/ml。
对血清HBVDNA在可测出水平的病人进行基因型分析,结果表明在原先就有拉米夫定耐药变异(rtL180M和/或rtM204/1)的病人中,有7%(13/189)的病人在48周出现rtI169,rtT184,rtS202和/或rtM250等位点与恩替卡韦耐药相关的置换变异。
在这13名发生变异的病人中,有3名病人在48周之发生了病毒学反弹(HBVDNA从最低点上≥1个log10),多数病人在48周后发生了病毒学反弹。
交叉耐药在抗乙肝病毒的核苷类似物药物中已发现有交叉耐药现象,在细胞试验中发现恩替卡韦对拉米夫定耐药(rtL180M和/或rtM204V/I)的病毒株的抑制作用比野生株减弱8至30倍。
恩替卡韦对阿德福韦耐药性变异(HBVDNA多聚酶rtN236T或rtA181V变异)的重组病毒也完全敏感,体外试验显示,从拉米夫定和恩替卡韦都失效的病人中分离出来的病毒株,对阿德福韦敏感,但对拉米夫定依然保持耐药性。
毒理研究遗传毒性在人类淋巴细胞培养的实验中,发现恩替卡韦是染色体断裂的诱导剂。
在Ames实验(使用伤寒杆菌,大肠杆菌,使用或不用代谢激活剂)、基因突变实验和叙利亚仓鼠胚胎细胞转染实验中,发现恩替卡韦不是突变诱导剂。
在大鼠的经口给药微核实验和DNA修复实验中,恩替卡韦也呈阴性。
生殖毒性在生殖毒性研究中,连续4周给予恩替卡韦,剂量最高达30mg/kg,在给药剂量超过人体最高推荐剂量天的90倍时,没有发现雄性和雌性大鼠的生育力受到影响。
在恩替卡韦的毒理学研究中,当剂量至人体剂量的35倍或以上时,发现啮齿类动物与狗出现了输精管的退行性变。
在猴子实验中,未发现睾丸的改变。
在大鼠和家兔的生殖毒性研究中,口服本品的剂量达200和13mg/kg/天,即相当于人体最高剂量天的28倍(对于大鼠)和212倍(对于家兔)时,没有发现胚胎和母体毒性。
在大鼠实验中,当母鼠的用药量相当于人体剂量3100倍时,观察到恩替卡韦对胚胎—胎鼠的毒性作用(重吸收)、体重降低、尾巴和脊椎形态异常和骨化水平降低(脊椎、趾骨和指骨)并观察到额外的腰椎和肋骨。
在家兔实验中,对雌兔的用药量为人体的日剂量的883倍时,观察到对胚胎—胎兔的毒性作用(吸收)、骨化水平降低(舌骨),并且第13根肋骨的发生率增加。
在对出生前和出生后大鼠口服恩替卡韦的研究中发现用药量大于人的日剂量的94倍未对后代产生影响。
恩替卡韦可从大鼠乳汁分泌。
致癌性在小鼠和大鼠口服恩替卡韦的长期致癌性研究中,药物暴露量大约分别是人类最高推荐剂量(每天)的42倍(大鼠)和35倍(小鼠)。
在上述研究中,恩替卡韦致癌性出现阳性结果。
在小鼠试验中,当剂量至人体剂量的3至40倍时,雄性或雌性小鼠的肺部腺瘤的发生率增加。
当剂量至人体剂量的40倍时,雄性或雌性小鼠的肺部肿瘤的发生率增加。
当剂量至人体剂量的3倍时,雄性小鼠的肺部腺瘤和肿瘤的发生率增加;当剂量致人体剂量的40倍时,雌性小鼠的肺部腺瘤和肿瘤的发生率增加。
小鼠先出现肺细胞增生,继而出现肺部肿瘤,但给予本品的大鼠、狗和猴中并未发现肺细胞增生,这提示在小鼠体内发生的肺部肿瘤可能具有种属特异性。
当剂量至人体剂量的42倍时,雄性小鼠的肝细胞肿瘤与混合瘤(肿瘤和腺瘤)的发生率增加。
当剂量至人体剂量的40倍时,雌性小鼠的血管性肿瘤(包括卵巢,子宫的血管瘤和脾脏的血管肉瘤)发生率增加。
在大鼠的试验中,当剂量至人体剂量的24倍时,雌性大鼠的肝细胞腺瘤的发生率增加,混合瘤(肿瘤和腺瘤)的发生率也增加。
当剂量至人体剂量的35倍和24倍时,分别在雄性大鼠和雌性大鼠身上发现有脑胶质瘤。
当剂量至人体剂量的4倍时,在雌性大鼠身上发现有皮肤纤维瘤。
目前尚不清楚本品啮齿类动物致癌性试验的结果能否预测本品对人体的致癌作用。
【药代动力学】吸收健康人群口服用药后,本品被迅速吸收,到小时达到峰浓度(Cmax)。
每天给药一次,6—10天后可达稳态,累积量约为两倍。
食物对口服吸收的影响进食标准高脂餐或低脂餐的同时口服本品会导致药物吸收的轻微延迟(从原来的小时变为—小时),Cmax降低44—46%,药时曲线下面积(AUC)降低18—20%。
因此,本品应空腹服用(餐前或餐后至少2小时)。
药代动力学资料表明,其表观分布容积超过全身液体量,这说明本品广泛分布于各组织。
体外实验表明本品与人血浆蛋白结合率为13%。
代谢和清除在给人和大鼠服用14C标记的恩替卡韦后,未观察到本品的氧化或乙酰化代谢物,但观察到少量II期代谢产物葡萄糖醛酸甙结合物和硫酸结合物。
恩替卡韦不是细胞色素P450(CYP450)酶系统的底物、抑制剂或诱导剂。
在达到血浆峰浓度后,血药浓度以双指数方式下降,达到终末清除半衰期约需128—149小时。
药物累积指数约为每天一次给药剂量的2倍,这表明其有效累积半衰期约为24小时。
本品主要以原形通过肾脏清除,清除率为给药量的62—73%。
肾清除率为360—471mL/min,且不依赖于给药剂量,这表明恩替卡韦同时通过肾小球滤过和网状小管分泌。
特殊人群性别:本品的药代动力学不因性别的不同面改变。
种族:本品的药代动力学不因种族的不同而改变。
老年人:一项评价年龄与本品药代动力学关系的研究(口服本品)显示老年人的AUC较健康年轻人升高%,这很可能是由于个体肾功能的差异所造成的。
老年人的用药剂量参看肾功能不全者的剂量调节。
肾功能不全在不同程度肾功能不全患者(无慢性乙型肝炎病毒感染),包括使用血液透析或持续性便携式腹膜透析(CAPD)治疗的患者中,单次给药本品后的药代动力学结果显示清除率随肌酐清除率的降低而下降。
单次给药本品4小时后,血液透析能清除约给药剂量的13%,给药7天后,CAPD治疗仅能清除约给药剂量的%。
肝功能不全在中度和重度肝功能不全(Child—Pugh分级B或C)患者(不包括慢性乙肝病毒感染患者)中,研究了单次给药后恩替卡韦的药代动力学情况,肝功能不全患者与健康对照人群的恩替卡韦的药代动力学情况相似。
因此,无需在肝功能不全患者中调节恩替卡韦的给药剂量。
肝移植后:目前尚不清楚本品在肝移植患者中的安全性和有效性。
在一个小型的研究中,在使用稳定剂量的环孢酶素A(n=5)或他克莫司(n=4)治疗HBV感染肝移植患者中,由于肾功能的改变,本品在体内的总量约为肾功能正常的健康人的两倍。
肾功能的改变是导致本品在这些病人中浓度增加的原因。
本品与环孢酶素A或他克莫司之间的药物动力学的相互作用尚未被评价。
这些患者在肝移植前、移植中使用本品或在肝移植后使用免疫抑制如环孢酶素A或他克莫司的同时使用本品都有可能影响肾功能,故必须仔细评价患者的肾功能。
儿童用药:尚无儿童使用该药的药代动力学数据。
【用法用量】患者应在有经验的医生指导下服用本品。
推荐剂量:成人和16岁以上青年口服本品,每天一次,每次。
拉米夫定治疗时病毒血症或出现拉米夫定耐药突变的患者为每天一次,每次两片)。
本品应空腹服用(餐前或餐后至少2小时)。
肾功能不全在肾功能不全的患者中,恩替卡韦的表现口服清除率随肌酐清除率的降低而降低(参见药代动力学:特殊人群)。
肌酐清除率<50ml/分钟的患者(包括接受血液透析或CAPD治疗的患者)应调整用药剂量。
见表7。
表7:肾功能不全患者恩替卡韦推荐剂量肌酐清除率(mL/min)通常剂量()拉米夫定治疗失效()≥50每日一次,每次每日一次,每次到<50每日一次,每次每日一次,每次到<30每日一次,每次每日一次,每次血液透析*或CAPD每日一次,每次每日一次,每次*血液透析后用药肝功能不全肝功能不全患者无需调整用药剂量。
治疗的时间关于本品的最佳治疗时间,以及长期的治疗结果的关系,如肝硬化、肝癌,目前尚未明了。