Reliable Diagnostics for Coronary Artery Disease
clia实验室合格证书

clia实验室合格证书
CLIA实验室合格证书是由美国临床实验室改进法案修正案(Clinical Laboratory Improvement Amendments,简称CLIA)所授权颁发的证书。
该证书是美国政府对所有用于健康评价或疾病诊断、预防或者治疗的测试人体样本的临床实验室强制执行的资格要求。
在美国,所有临床实验室必须通过CLIA的认证注册,才有权接收并处理血液、体液和组织等人体样本,以用于疾病的诊断、预防、评估和治疗,其提供的检测服务才能向美国政府的医疗保险和医疗补助计划收费。
CLIA认证的意义在于:
1.实验室质量管理体系符合国际权威机构的要求。
2.实验技术水平符合国际标准、检测方法具有可重复性。
3.信息分析和临床解读能力获得国际认可。
CLIA的证书分为三种(COC、COA、COR证书),均为2年效期。
(JACR)CAD-RADS_ 冠状动脉狭窄诊断标准

ORIGINAL ARTICLECAD-RADSä:Coronary ArteryDisease e Reporting and Data System.An Expert Consensus Document of the Society of Cardiovascular ComputedT omography(SCCT),the American College of Radiology(ACR)and the North American Society for Cardiovascular Imaging(NASCI).Endorsed by theAmerican College of CardiologyRicardo C.Cury,MD a,Suhny Abbara,MD b,Stephan Achenbach,MD c,Arthur Agatston,MD d, Daniel S.Berman,MD e,Matthew J.Budoff,MD f,Karin E.Dill,MD g,Jill E.Jacobs,MD h, Christopher D.Maroules,MD i,Geoffrey D.Rubin,MD j,Frank J.Rybicki,MD,PhD k,U.Joseph Schoepf,MD l,Leslee J.Shaw,PhD m,Arthur E.Stillman,MD n,Charles S.White,MD o, Pamela K.Woodard,MD p,Jonathon A.Leipsic,MD qa Miami Cardiac and Vascular Institute,Baptist Hospital of Miami,8900N Kendall Drive,Miami,FL,33176,United States.b Department of Radiology,5323Harry Hines Blvd,Dallas,TX,75390, United States.c Friedrich-Alexander-Universität,Erlangen-Nürnberg,Department of Car-diology,Ulmenweg18,90154,Erlangen,Germany.d Baptist Health Medical Grp,1691Michigan Avenue,Miami,FL,33139, United States.e Cedars-Sinai Med Center,8700Beverly Boulevard,Taper Building,Rm 1258,Los Angeles,CA,90048,United States.f1124W.Carson Street,Torrance,CA,90502,United States.g5841South Maryland Ave,MC2026,Chicago,IL,60637,United States. h550First Avenue,New York,NY,10016,United States.i Department of Radiology,5323Harry Hines Blvd,Dallas,TX,75390, United States.j2400Pratt Street,Room8020,DCRI Box17969,Durham,NC,27715, United States.k The Ottawa Hospital General Campus,501Smyth Rd,Ottawa,ON,CA K1H8L6,Canada.l25Courtenay Dr.,Charleston,SC,29425,United States.m1256Briarcliff Rd.NE,Rm529,Atlanta,GA,30324,United States. n1364Clifton Road,NE,Atlanta,GA,30322,United States.o University of Maryland,22S.Greene St.,Baltimore,MD,21201,United States.p Mallinckrodt Instit of Radiology,510S Kingshighway Blvd,St.Louis, MO,63110,United States.q Department of Radiology,St.Paul’s Hospital,2nd Floor,Providence Building,1081Burrard Street,Vancouver,BC,V6Z1Y6,United States. Corresponding author and reprints:Ricardo C.Cury,MD,Miami Cardiac and Vascular Institute,Baptist Hospital of Miami,8900N Kendall Drive, Miami,FL33176;e-mail:rcury@.ª2016Society of Cardiovascular Computed T omography and the American College of Radiology.Published by Elsevier Inc.All rights reserved.1546-1440/16/$36.00n /10.1016/j.jacr.2016.04.0241CONDENSED ABSTRACTCAD-RADS is a standardized reporting system for cor-onary CTA results on a per-patient basis.It is intended to improve communication of results to referring physicians in a consistent fashion,including recommendations for further management.The achieved standardization of reporting will benefit education,research,peer review and quality assurance and may ultimately result in improved quality of care.1.INTRODUCTIONCoronary CT Angiography(coronary CTA)has made substantial progress since the introduction of64-slice CT scanners approximately10years ago[1],both concerning imaging technology and clinical validation.In parallel, several professional societies have issued guidelines, expert consensus documents,and Appropriateness Criteria for coronary CTA[2-8].To maximize the clinical impact of coronary CTA,imaging protocols must be optimized with respect to image quality, diagnostic accuracy,and radiation dose.Training and interpretation standards are important.Finally, standardized reporting is helpful to decrease variability among practitioners and may provide further benefit by linking thefinal impression in the report with suggestions for further patient management.Otherfields in medical imaging(notably,breast imag-ing with BI-RADS)have introduced standardized reporting linked with actionable information to guide next steps in patient management[9].BI-RADS standardized reporting of screening mammograms allows clinicians to interpret the clinical relevance of reportedfindings and to take action. Moreover,BI-RADS facilitates collection of data for regis-tries and databases,allowing better tracking of individual patient outcomes with specific imagingfindings.Next to BI-RADS,standardized reporting has been introduced for several otherfields.They include,for example:n LI-RADSÔ(Liver Imaging Reporting and Data System)for standardization reporting in patients with chronic liver disease[10].n Lung-RADSÔ(Lung CT Screening Reporting and Data System)for standardization reporting of high-risk smokers undergoing CT lung screening[11].n PI-RADSÔ(Prostate Imaging Reporting and Data System)for multi-parametric MR imaging in the context of prostate cancer[12].The purpose of this document is to describe a stan-dardized reporting system for patients undergoing coronary CTA.The report system is named CAD-RADS(Coronary Artery Disease Reporting and Data System)and is applicable to coronary CTA in patients with suspected or known cor-onary artery disease either in the outpatient,inpatient or emergency department setting.It includes suggestions regarding further patient management,which,obviously will always need to be seen in light of the full clinical information available to the treating physician.For the specific setting of coronary CTA in patients with acute chest pain presenting to the emergency department,certain management recom-mendations have been reported previously[13,14].The goal of CAD-RADS,through standardization of report terminology for coronary CTA,is to improve communication between interpreting and referring physicians,facilitate research,and offer mechanisms to contribute to peer review and quality assurance,ultimately resulting in improvements to quality of care.Importantly, CAD-RADS does not substitute the impression section provided by the reading physician and should always be interpreted in conjunction with the more individual and patient-specific information found in the report.2.CLINICAL VALUE OF CORONARY CT ANGIOGRAPHYSeveral recent prospective trials have evaluated the clinical utility of coronary CTA and the relevance of CTfindingsE-mail addresses:Suhny.Abbara@(S.Abbara),Stephan. Achenbach@uk-erlangen.de(S.Achenbach),ArthurSAg@ (A.Agatston),bermand@(D.S.Berman),mbudoff@ (M.J.Budoff),kdill@(K.E.Dill),jill.jacobs@ (J.E.Jacobs),christopher.maroules@(C.D.Maroules), grubin@(G.D.Rubin),frybicki@toh.on.ca(F.J.Rybicki), schoepf@(U.J.Schoepf),lshaw3@(L.J.Shaw),aestill@ (A.E.Stillman),cwhite@(C.S.White),woodardp@mir. (P.K.Woodard),jleipsic@providencehealth.bc.ca(J.A.Leipsic). This document was approved by the American College of Radiology Board of Chancellors in March2016.Please cite this article in press as:Cury RC,et al.,CAD-RADS TM: Coronary Artery Disease e Reporting and Data System.An expert consensus document of the Society of Cardiovascular Computed Tomography(SCCT),the American College of Radiology(ACR)and the North American Society for Cardiovascular Imaging(NASCI). Endorsed by the American College of Cardiology.Journal of Cardio-vascular Computed Tomography(2016),/10.1016/ j.jcct.2016.04.005.Suggested secondary citation:Cury RC,et al.,CAD-RADS TM:Cor-onary Artery Disease e Reporting and Data System.An expert consensus document of the Society of Cardiovascular Computed Tomography(SCCT),the American College of Radiology(ACR)and the North American Society for Cardiovascular Imaging(NASCI). Endorsed by the American College of Cardiology.J Am Coll Radiol /10.1016/j.jacr.2016.04.024.2Journal of the American College of RadiologyVolume-n Number-n Month2016in the context of suspected stable coronary artery disease. They include the PROMISE[15]and SCOT-HEART [16]trials,which demonstrated that coronary CTA is clinically useful as an alternative to(PROMISE)or in addition to functional testing(SCOT-HEART).Four large randomized trials(CT-STAT,ACRIN-PA, ROMICAT II and CT-COMPARE)compared coronary CTA to the current standard of care in patients with acute chest pain[17-20].Complemented by“real world”implementation data[21,22],they consistently demonstrate the safety of a negative coronary CTA to identify patients for discharge from the emergency department.There are some limitations to the currently mentioned available studies(for example,their over-representation of low risk patients).Other situations,such as the use of coronary CTA in patients with known coronary artery disease,have not been evaluated in appropriate clinical trials.Hence,while fully taking into account the available data,this document is based on expert consensus.This includes the suggested categories for reporting but also the suggestions for further patient management,which need to be interpreted in the context of other clinical information that is available in any given patient.3.CAD-RADS REPORTING SYSTEM3.1.CAD-RADS CategoriesCAD-RADS categories depend on stenosis severity.For the grading of stenosis severity,a classification system suggested by the Society of Cardiovascular Computed Tomography is used(see Table1).Tables2and3list the categories of the CAD-RADS reporting system for stable chest pain(Table2)and acute chest pain(Table3).They range from CAD-RADS0(absence of atherosclerosis)to CAD-RADS5(presence of at least one total occlusion)in both settings.Categories should reflect the clinically most relevantfinding per patient.Online Figures1through9 provide examples of CAD-RADS categories and sub-categories.It is important to note that CAD-RADS classification is meant to be complementary to thefinal impression of the report,particularly because the report will provide specific information regarding the location and extent of coronary plaque and stenosis.CAD-RADS categories4and5require some further consideration.For CAD-RADS4,recommendations may vary depending on whether the left main or severe obstructive three-vessel disease(>70%)is affected or not. If a left main coronary artery stenosis greater than50%is suspected or if the examination demonstrates three-vessel obstructive disease,then further evaluation with invasive angiography and possible revascularization is recom-mended.For this reason,CAD RADS4is sub-divided into A and B:CAD RADS4A—Single-vessel or two-vessels demon-strating severe stenosis(70-99%).CAD RADS4B—This indicates presence of left main stenosis greater than50%or three-vessel obstructive disease(>70%).Further evaluation with ICA and possible revascularization is usually recommended.The clinical relevance of CAD-RADS5(total coronary occlusion)varies widely depending on the clinical context.It may be acute or chronic,and,in the context of chronic oc-clusion,factors such as lesion length,calcification particu-larly at the proximal cap,and degree of collateralization may be of relevance for management decisions(Online Fig.8).3.2.Patients With Known CADManagement recommendations with regard to patients with previously known CAD deserve special consideration.The main clinical benefit of coronary CTA is derived from its high sensitivity and negative predictive value.The positive pre-dictive value of coronary CTA is lower,and especially inter-mediate lesions may be overestimated regarding their relevance.Many patients with previously known CAD will include lesions that fall into this category,so that coronary CTA will need to be complemented by further tests.Addi-tionally,coronary CTA has low accuracy for diagnosis of in-stent restenosis,particularly in stents smaller than3.0mm diameter.Thus,the use of coronary CTA in patients with previously known CAD should be carefully considered. Management decisions derived from coronary CTA results depend on other clinicalfindings as well as the patient-specific previous history,and should be made on an individual basis.3.3.ModifiersCAD-RADS categories can be complemented by modi-fiers to indicate that a study is not fully evaluable or non-diagnostic(N)or to indicate the presence of stents(S), grafts(G),and vulnerable plaque(V).Degree of Luminal Diameter Stenosis T erminology 0%No visible stenosis 1-24%Minimal stenosis 25-49%Mild stenosis50-69%Moderate stenosis 70-99%Severe stenosis 100%OccludedJournal of the American College of Radiology3 Cury et al n Coronary Artery Disease e Reporting and Data SystemCoronary Stenosis Interpretation Investigation ManagementCAD-RADS00%(No plaque orstenosis)Documented absenceof CADNone-Reassurance.Consider non-atherosclerotic causes of chest painCAD-RADS11-24%—Minimalstenosis or plaquewith no stenosis*Minimal non-obstructive CADNone-Consider non-atherosclerotic causesof chest pain-Consider preventive therapy and riskfactor modificationCAD-RADS225-49%—Mildstenosis Mild non-obstructiveCADNone-Consider non-atherosclerotic causesof chest pain-Consider preventive therapy and riskfactor modification,particularly forpatients with non-obstructiveplaque in multiple segments.CAD-RADS350-69%stenosis Moderate stenosis Consider functionalassessment -Consider symptom-guided anti-ischemic and preventive pharmacotherapy as well as risk factor modification per guideline-directed care†-Other treatments should be considered per guideline-directed care†CAD-RADS4A—70-99%stenosisorB—Left main>50%or3-vesselobstructive(70%)disease Severe stenosis A:Consider ICA orfunctionalassessmentB:ICA is recommended-Consider symptom-guided anti-ischemic and preventivepharmacotherapy as well as riskfactor modification per guideline-directed care†-Other treatments(including optionsof revascularization)should beconsidered per guideline-directedcare†CAD-RADS5100%(totalocclusion)T otal coronaryocclusionConsider ICA and/orviability assessment-Consider symptom-guided anti-ischemic and preventivepharmacotherapy as well as riskfactors modification per guideline-directed care†-Other treatments(including optionsof revascularization)should beconsidered per guideline-directedcare†CAD-RADS N Non-diagnostic study Obstructive CADcannot be excluded Additional or alternative evaluation may be neededAll vessels greater than1.5mm in diameter should be graded for stenosis severity.CAD-RADS will not apply for smaller vessels(<1.5mm in diameter).CAD¼coronary artery disease;ICA¼invasive coronary angiography.MODIFIERS:If more than one modifier is present,the symbol“/”(slash)should follow each modifier in the following order:First:modifier N(non-diagnostic)Second:modifier S(stent)Third:modifier G(graft)Fourth:modifier V(vulnerability)*CAD-RADS1—This category should also include the presence of plaque with positive remodeling and no evidence of stenosis.†Guideline-directed care per ACC Stable Ischemic Heart Disease Guidelines(Fihn et al JACC2012)[25].4Journal of the American College of RadiologyVolume-n Number-n Month2016I.Modi fier N —Non-Diagnostic Study“N ”can be used as a modi fier or as a CAD-RADS category,depending on context.If the study is not fully diagnostic (ie,not all segments >1.5mm diameter can be interpreted with con fidence)and a stenosis is presentin a diagnostic segment,the highest stenosis should be graded in addition to the modi fier N if CAD-RADS is greater than 3.For example,a patient with moderate stenosis (50-69%)in one segment and one or more non-diagnostic remote segments should be graded as CAD-RADS 3/N (Online Fig.10)and notCAD-RADSCoronary Stenosis Interpretation ManagementCAD-RADS 00%ACS highly unlikely -No further evaluation of ACS is required.-Consider other etiologies.CAD-RADS 11-24%*ACS highly unlikely-Consider evaluation of non-ACS etiology,if normal troponin and no ECG changes.-Consider referral for outpatient follow-up for preventive therapy and risk factor modi fication.CAD-RADS 225-49%†ACS unlikely-Consider evaluation of non-ACS etiology,if normal troponin and no ECG changes.-Consider referral for outpatient follow-up for preventive therapy and risk factor modi fication.-If clinical suspicion of ACS is high or if high-risk plaque features are noted,consider hospital admission with cardiology consultation.CAD-RADS 350-69%ACS possible-Consider hospital admission with cardiology consultation,functional testing and/or ICA for evaluation and management.-Recommendation for anti-ischemic and preventivemanagement should be considered as well as risk factor modi fication.Other treatments should be considered if presence of hemodynamically signi ficant lesion.CAD-RADS 4A —70-99%orB —Left main >50%or 3-vesselobstructive diseaseACS likely-Consider hospital admission with cardiology consultation.Further evaluation with ICA and revascularization as appropriate.-Recommendation for anti-ischemic and preventivemanagement should be considered as well as risk factor modi fication.CAD-RADS 5100%(T otal occlusion)ACS very likely-Consider expedited ICA on a timely basis and revascularization if appropriate if acute occlusion ‡-Recommendation for anti-ischemic and preventivemanagement should be considered as well as risk factor modi fications.CAD-RADS N Non-diagnostic studyACS cannot be excludedAdditional or alternative evaluation for ACS is neededvessels greater than 1.5mm in diameter should be graded for stenosis severity.CAD-RADS will not apply for smaller vessels (<1.5mm in diameter).ACS ¼acute coronary syndrome;ICA ¼invasive coronary angiography.MODIFIERS:If more than one modi fier is present,the symbol “/”(slash)should follow each modi fier in the following order:First:modi fier N (non-diagnostic)Second:modi fier S (stent)Third:modi fier G (graft)Fourth:modi fier V (vulnerability)*CAD-RADS 1—This category should also include the presence of plaque with positive remodeling and no evidence of stenosis.†CAD-RADS 2—Modi fier 2/V can be used to indicate vulnerable/high-risk plaque.‡Unless the total coronary occlusion can be identi fied as chronic (through CT and clinical characteristics or patient history).Journal of the American College of Radiology5Cury et al n Coronary Artery Disease e Reporting and Data SystemN,since further evaluation is needed,possibly with functional imaging,and patient recommendations for anti-ischemic and preventive management apply. However,for a patient with no stenosis(zero),minimal (1-24%),or no more than mild stenosis(25-49%)in interpretable segments,CAD-RADS N should be used since Coronary CTA cannot be used to guide patient management and further evaluation to exclude obstructive coronary artery disease is still needed.II.Modifier S—Presence of a StentThe modifier“S”indicates the presence of at least one coronary stent anywhere in the coronary system.For example,if a patient has a patent stent in the proximal left anterior descending coronary artery(LAD)with no significant in-stent restenosis or occlusion and demonstrates mild non-obstructive disease(25-49%)in the left circumflex artery(LCX)and right coronary artery(RCA),the case would be classified as:CAD-RADS2/S.If a patient dem-onstrates significant in-stent restenosis of a stent in the proximal LAD,then the case would be classified as:CAD-RADS4A/S(Online Fig.11).Similarly,a non-stenotic stent in the LAD and a new severe stenosis in the RCA would be classified as CAD-RADS4A/S.Finally,if a stent were non-evaluable,the case would be classified as CAD-RADS N/S if there is no other stenosis greater than 50%in the coronary tree.Note:CAD-RADS was created to guide management recommendations,so it does not matter whether it is the stent or a non-stented vessel that has a severe stenosis.Rather,what matters is that the patient has a severe stenosis and needs further work-up. III.Modifier G—Presence of Coronary Bypass Grafts The modifier“G”indicates the presence of at least one coronary-artery bypass graft(Online Fig.12).A stenosis bypassed by a fully patent graft is not considered for the CAD-RADS classification.For example,if a patient has a graft to LAD,with absence of significant stenoses in the graft,distal anastomosis and run-off vessel,and demonstrates non-obstructive lesions(25-49%)in the LCX and RCA,in addition to the“expected”proximal LAD severe stenosis,then the case would be classified as:CAD-RADS2/G.If a patient demonstrates total occlusion of a saphenous vein graft(SVG)to the RCA,and a patent LIMA to LAD and SVG to LCX,then the case would be classified as:CAD-RADS5/G.The interpretation is that a total occlusion is present and further investigation and/or management may be required.IV.Modifier V—Presence of“Vulnerable”or High-Risk Plaque FeaturesData from recent coronary CTA studies have described vulnerable plaque characteristics that are inde-pendently associated with future ACS.They include positive remodeling,low-attenuation plaque,spotty calcification,and the napkin-ring sign[23,24].If a coronary plaque clearly demonstrates two or more high-risk features by coronary CTA,the modifier“V”(vulnerability)should be added(Online Figs.13and14). High-risk features include:low attenuation plaque(less than30Hounsfield Units),positive remodeling,spotty calcification,and the“napkin ring sign”(see Online Fig.13).For example,CAD RADS2/V should be used for a patient with diameter stenosis between25-49%and demon-strating plaque with two or more high-risk features(large non-calcified plaque,positive remodeling,spotty calci-fication,low HU values and napkin ring sign)(Online Fig.14).The features should be described,particularly in patients presenting to the emergency department with acute chest pain.There is not enough published data to guide the management of such patients.However, clinical and laboratory correlation and close observation is recommended.Consider hospital admission in high-risk clinical settings.If the patient is discharged,short-term clinical follow-up within a week is suggested in the outpatient setting with a cardiologist or primary care physician.Studies coded with CAD-RADS3/V(the presence of high risk plaque with50-69%diameter stenosis,excluding left main lesions)should prompt consideration for more aggressive management than studies coded with CAD-RADS3,partic-ularly in patients presenting to the emergency department with acute chest pain.This includes consideration of further testing with invasive coronary angiography instead of non-invasive functional testing.However,management decisions should ultimately be made on an individual basis taking into consideration all supporting clinical and laboratory data. V.If more than one modifier is present,the symbol“/”(slash)should follow each modifier in the following order:i.First:modifier N(non-diagnostic)ii.Second:modifier S(stent)iii.Third:modifier G(graft)iv.Fourth:modifier V(vulnerability)For example:i.Non-interpretable coronary stent without evi-dence of other obstructive coronary disease:Modifier S[CAD-RADS N/S6Journal of the American College of RadiologyVolume-n Number-n Month2016ii.Presence of stent and a new moderate stenosisshowing a plaque with high-risk features:Modifiers Sand V[CAD-RADS3/S/V(Online Fig.15) iii.Presence of stent,grafts and non-evaluable segments due to metal artifacts:Modifiers S andG[CAD-RADS N/S/Giv.Presence of patent LIMA to the LAD and expected occluded proximal d non-obstructive stenosis in the RCA and LCX.Modifier G[CAD-RADS2/G.v.For a patient with severe stenosis(70-99%)in onesegment and a non-diagnostic area in anothersegment,the study should be graded asCAD-RADS4/N.3.4.Presence of Other Cardiac or Extra-Cardiac FindingsPatients undergoing coronary CTA may demonstrate other significant,potentially significant or non-significant cardiac or extra-cardiacfindings.CAD-RADS is intended to focus solely on the classification of coronary artery ste-nosis and further management.However,other cardiac and extra-cardiacfindings of relevance should be reported in coronary CTA studies and should be mentioned in the report text.Specific follow-up and recommendations should be included depending on the pathology.Finally,Online Figure16provides a sample standardized reporting template for coronary CTA incorporating CAD-RADS coding.4.DISCUSSIONThe use of coronary CTA to assess patients with stable chest pain in the outpatient setting or acute chest pain presenting to the Emergency Department has been validated in various clinical trials.Major guidelines are incorporating the use of coronary CT angiography as appropriate for assessing low to intermediate risk patients presenting with chest pain. Decreasing the variation in reporting is one aspect that will contribute to wider dissemination in clinical practice,minimize error and to ultimately improve patient outcome.The main goal of the CAD-RADS classification system is to propose a reporting structure that provides consistent categories forfinal assessment,along with suggestions for further management.CAD-RADS is intended to be a“living document”that undergoes continued development to provide up-to-date, evidence based recommendations to achieve its goal of being a tool that imagers can use to communicate with clinicians and to convey concisefindings using unambiguous and standardized terminology.Next to its utilization in clinical reporting,CAD-RADS will allow reliable and reproducible data collection,storage and retrieval for future research trials and audits.Similar to other larger registries,such as the National Radiology Data Registry(NRDR)and National Cardio-vascular Data Registry(NCDR),CAD-RADS can provide the framework for standardize collection of coronary CTA reports across multiple sites for quality improvement and benchmarking.Further,it can provide the framework for collecting outcome data in each of several sub-categories of CAD-RADS,such as:1.Follow-up of disposition of patients with positivecoronary CTA results;2.Rate of downstream testing;3.Correlation with ICA;4.Rate of revascularization(percutaneous coronaryintervention and coronary artery by-pass graft surgery) 5.Major adverse cardiac events,including cardiovasculardeath and myocardial infarct.Therefore,it is strongly encouraged that every coronary CTA examination includes the CAD-RADS classification for afinal assessment.Residency and Fellowship trainees should be required to use the CAD-RADS terminology,assessment categories and management recommendations.Similar to BI-RADS,peer-reviewed radiology and cardiology journals may alsofind the CAD-RADS terminology useful for standardized classification of coro-nary CTA results,which in turn will further promote the use of CAD-RADS nationally and internationally.Finally,standardization in reports and management recommendations will not only improve the clarity of communication and comprehension of imaging results by all members of the clinical care team,but also will improve communication between humans and computer-based systems.This will allow the development of decision support technologies and serve as the basis for developing artificial intelligence algorithms.5.CONCLUSIONIn conclusion,CAD-RADS has been developed based on scientific data,expert guidance from leaders in cardiac im-aging and a multi-disciplinary effort involving radiology and cardiology societies(Society of Cardiovascular Computed Tomography,American College of Radiology,American College of Cardiology and North American Society of Cardiac Imaging).It is meant to be an evolving document that will undergo continuous updates as new data are ac-quired.The main goal of CAD-RADS is to create report standardization terminology for coronary CTA results,andJournal of the American College of Radiology7 Cury et al n Coronary Artery Disease e Reporting and Data System。
中国科学英文版模板
中国科学英文版模板1.Identification of Wiener systems with nonlinearity being piece wise-linear function HUANG YiQing,CHEN HanFu,FANG HaiTao2.A novel algorithm for explicit optimal multi-degree reduction of triangular surfaces HU QianQian,WANG GuoJin3.New approach to the automatic segmentation of coronary arte ry in X-ray angiograms ZHOU ShouJun,YANG Jun,CHEN WuFan,WANG YongTian4.Novel Ω-protocols for NP DENG Yi,LIN DongDai5.Non-coherent space-time code based on full diversity space-ti me block coding GUO YongLiang,ZHU ShiHua6.Recursive algorithm and accurate computation of dyadic Green 's functions for stratified uniaxial anisotropic media WEI BaoJun,ZH ANG GengJi,LIU QingHuo7.A blind separation method of overlapped multi-components b ased on time varying AR model CAI QuanWei,WEI Ping,XIAO Xian Ci8.Joint multiple parameters estimation for coherent chirp signals using vector sensor array WEN Zhong,LI LiPing,CHEN TianQi,ZH ANG XiXiang9.Vision implants: An electrical device will bring light to the blind NIU JinHai,LIU YiFei,REN QiuShi,ZHOU Yang,ZHOU Ye,NIU S huaibining search space partition and search Space partition and ab straction for LTL model checking PU Fei,ZHANG WenHui2.Dynamic replication of Web contents Amjad Mahmood3.On global controllability of affine nonlinear systems with a tria ngular-like structure SUN YiMin,MEI ShengWei,LU Qiang4.A fuzzy model of predicting RNA secondary structure SONG D anDan,DENG ZhiDong5.Randomization of classical inference patterns and its applicatio n WANG GuoJun,HUI XiaoJing6.Pulse shaping method to compensate for antenna distortion in ultra-wideband communications WU XuanLi,SHA XueJun,ZHANG NaiTong7.Study on modulation techniques free of orthogonality restricti on CAO QiSheng,LIANG DeQun8.Joint-state differential detection algorithm and its application in UWB wireless communication systems ZHANG Peng,BI GuangGuo,CAO XiuYing9.Accurate and robust estimation of phase error and its uncertai nty of 50 GHz bandwidth sampling circuit ZHANG Zhe,LIN MaoLiu,XU QingHua,TAN JiuBin10.Solving SAT problem by heuristic polarity decision-making al gorithm JING MingE,ZHOU Dian,TANG PuShan,ZHOU XiaoFang,ZHANG Hua1.A novel formal approach to program slicing ZHANG YingZhou2.On Hamiltonian realization of time-varying nonlinear systems WANG YuZhen,Ge S. S.,CHENG DaiZhan3.Primary exploration of nonlinear information fusion control the ory WANG ZhiSheng,WANG DaoBo,ZHEN ZiYang4.Center-configur ation selection technique for the reconfigurable modular robot LIU J inGuo,WANG YueChao,LI Bin,MA ShuGen,TAN DaLong5.Stabilization of switched linear systems with bounded disturba nces and unobservable switchings LIU Feng6.Solution to the Generalized Champagne Problem on simultane ous stabilization of linear systems GUAN Qiang,WANG Long,XIA B iCan,YANG Lu,YU WenSheng,ZENG ZhenBing7.Supporting service differentiation with enhancements of the IE EE 802.11 MAC protocol: Models and analysis LI Bo,LI JianDong,R oberto Battiti8.Differential space-time block-diagonal codes LUO ZhenDong,L IU YuanAn,GAO JinChun9.Cross-layer optimization in ultra wideband networks WU Qi,BI JingPing,GUO ZiHua,XIONG YongQiang,ZHANG Qian,LI ZhongC heng10.Searching-and-averaging method of underdetermined blind s peech signal separation in time domain XIAO Ming,XIE ShengLi,F U YuLi11.New theoretical framework for OFDM/CDMA systems with pe ak-limited nonlinearities WANG Jian,ZHANG Lin,SHAN XiuMing,R EN Yong1.Fractional Fourier domain analysis of decimation and interpolat ion MENG XiangYi,TAO Ran,WANG Yue2.A reduced state SISO iterative decoding algorithm for serially concatenated continuous phase modulation SUN JinHua,LI JianDong,JIN LiJun3.On the linear span of the p-ary cascaded GMW sequences TA NG XiaoHu4.De-interlacing technique based on total variation with spatial-t emporal smoothness constraint YIN XueMin,YUAN JianHua,LU Xia oPeng,ZOU MouYan5.Constrained total least squares algorithm for passive location based on bearing-only measurements WANG Ding,ZHANG Li,WU Ying6.Phase noise analysis of oscillators with Sylvester representation for periodic time-varying modulus matrix by regular perturbations FAN JianXing,YANG HuaZhong,WANG Hui,YAN XiaoLang,HOU ChaoHuan7.New optimal algorithm of data association for multi-passive-se nsor location system ZHOU Li,HE You,ZHANG WeiHua8.Application research on the chaos synchronization self-mainten ance characteristic to secret communication WU DanHui,ZHAO Che nFei,ZHANG YuJie9.The changes on synchronizing ability of coupled networks fro m ring networks to chain networks HAN XiuPing,LU JunAn10.A new approach to consensus problems in discrete-time mult iagent systems with time-delays WANG Long,XIAO Feng11.Unified stabilizing controller synthesis approach for discrete-ti me intelligent systems with time delays by dynamic output feedbac k LIU MeiQin1.Survey of information security SHEN ChangXiang,ZHANG Hua ngGuo,FENG DengGuo,CAO ZhenFu,HUANG JiWu2.Analysis of affinely equivalent Boolean functions MENG QingSh u,ZHANG HuanGuo,YANG Min,WANG ZhangYi3.Boolean functions of an odd number of variables with maximu m algebraic immunity LI Na,QI WenFeng4.Pirate decoder for the broadcast encryption schemes from Cry pto 2005 WENG Jian,LIU ShengLi,CHEN KeFei5.Symmetric-key cryptosystem with DNA technology LU MingXin,LAI XueJia,XIAO GuoZhen,QIN Lei6.A chaos-based image encryption algorithm using alternate stru cture ZHANG YiWei,WANG YuMin,SHEN XuBang7.Impossible differential cryptanalysis of advanced encryption sta ndard CHEN Jie,HU YuPu,ZHANG YueYu8.Classification and counting on multi-continued fractions and its application to multi-sequences DAI ZongDuo,FENG XiuTao9.A trinomial type of σ-LFSR oriented toward software implemen tation ZENG Guang,HE KaiCheng,HAN WenBao10.Identity-based signature scheme based on quadratic residues CHAI ZhenChuan,CAO ZhenFu,DONG XiaoLei11.Modular approach to the design and analysis of password-ba sed security protocols FENG DengGuo,CHEN WeiDong12.Design of secure operating systems with high security levels QING SiHan,SHEN ChangXiang13.A formal model for access control with supporting spatial co ntext ZHANG Hong,HE YePing,SHI ZhiGuo14.Universally composable anonymous Hash certification model ZHANG Fan,MA JianFeng,SangJae MOON15.Trusted dynamic level scheduling based on Bayes trust model WANG Wei,ZENG GuoSun16.Log-scaling magnitude modulated watermarking scheme LING HeFei,YUAN WuGang,ZOU FuHao,LU ZhengDing17.A digital authentication watermarking scheme for JPEG image s with superior localization and security YU Miao,HE HongJie,ZHA NG JiaShu18.Blind reconnaissance of the pseudo-random sequence in DS/ SS signal with negative SNR HUANG XianGao,HUANG Wei,WANG Chao,L(U) ZeJun,HU YanHua1.Analysis of security protocols based on challenge-response LU O JunZhou,YANG Ming2.Notes on automata theory based on quantum logic QIU Dao Wen3.Optimality analysis of one-step OOSM filtering algorithms in t arget tracking ZHOU WenHui,LI Lin,CHEN GuoHai,YU AnXi4.A general approach to attribute reduction in rough set theory ZHANG WenXiuiu,QIU GuoFang,WU WeiZhi5.Multiscale stochastic hierarchical image segmentation by spectr al clustering LI XiaoBin,TIAN Zheng6.Energy-based adaptive orthogonal FRIT and its application in i mage denoising LIU YunXia,PENG YuHua,QU HuaiJing,YiN Yong7.Remote sensing image fusion based on Bayesian linear estimat ion GE ZhiRong,WANG Bin,ZHANG LiMing8.Fiber soliton-form 3R regenerator and its performance analysis ZHU Bo,YANG XiangLin9.Study on relationships of electromagnetic band structures and left/right handed structures GAO Chu,CHEN ZhiNing,WANG YunY i,YANG Ning10.Study on joint Bayesian model selection and parameter estim ation method of GTD model SHI ZhiGuang,ZHOU JianXiong,ZHAO HongZhong,FU Qiang。
冠心病病人运动恐惧量表的汉化及信效度检验

冠心病病人运动恐惧量表的汉化及信效度检验虎银凤1,周丽琼1,刘瑞卿2,胡娜妞2,李转珍2*1.深圳大学附属华南医院,广东 518111;2.河南科技大学第一附属医院Chinesization of Fear of Activity in Patients with Coronary Artery Disease and its reliability and validity testHU Yinfeng, ZHOU Liqiong, LIU Ruiqing, HU Naniu, LI ZhuanzhenSouth China Hospital of Shenzhen University, Guangdong 518111 ChinaCorresponding Author LIZhuanzhen,E⁃mail:***********************Abstract Objective:To translate Fear of Activity in Patients with Coronary Artery Disease(Fact-CAD) and test its reliability and validity. Methods:Fact⁃CAD was translation according to the Brislin translation model.Provisional Chinese version of Fact⁃CAD was developed after cultural adaptation and pre-investigation.A total of 340 patients with coronary heart disease hospitalized in cardiovascular department of a tertiary grade A hospital in Luoyang city were selected as research subjects from February 22 to September 30,2021.Item of provisional Chinese version of Fact⁃CAD was analyzed,and reliability and validity was test.Results:The Chinese version of Fact⁃CAD was single dimensional scale,and its Cronbach's α coefficient was 0.982,the half reliability was 0.986, the retest reliability was 0.854,the item⁃level content validity index was from 0.83 to 1.00,scale⁃content validity index was 0.90.Exploratory factor analysis extracted one common factor with an eigenvalue of 15.484,and the variance contribution rate was 73.732%.Conclusions:The Chinese version of Fact⁃CAD has good reliability and validity,and can be used for assessing fear of activity in Chinese patients with coronary heart disease. Keywords coronary heart disease; fear of activity; Chinesization; reliability; validity; nursing摘要目的:对冠心病病人运动恐惧量表(Fact⁃CAD)进行汉化,并检验其信效度。
能谱CT_冠状动脉血管成像对糖尿病患者合并冠状动脉病变的诊断价值研究
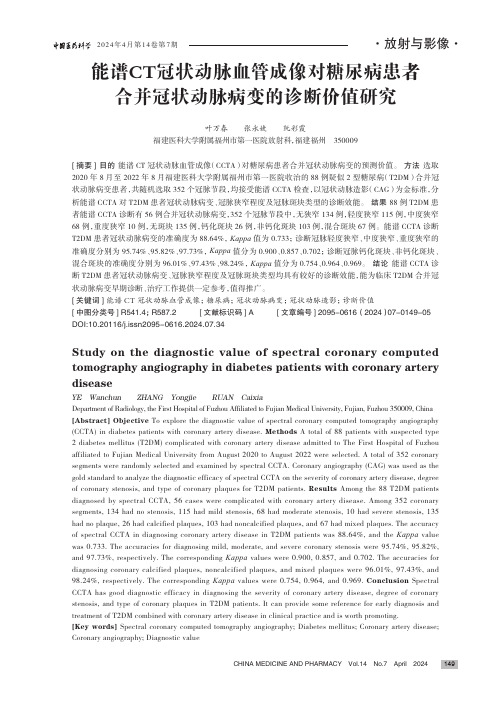
CHINA MEDICINE AND PHARMACY Vol.14 No.7 April 2024149能谱CT冠状动脉血管成像对糖尿病患者合并冠状动脉病变的诊断价值研究叶万春 张永婕 阮彩霞福建医科大学附属福州市第一医院放射科,福建福州 350009[摘要] 目的 能谱CT 冠状动脉血管成像(CCTA)对糖尿病患者合并冠状动脉病变的预测价值。
方法 选取2020年8月至2022年8月福建医科大学附属福州市第一医院收治的88例疑似2型糖尿病(T2DM)合并冠状动脉病变患者,共随机选取352个冠脉节段,均接受能谱CCTA 检查,以冠状动脉造影(CAG)为金标准,分析能谱CCTA 对T2DM 患者冠状动脉病变、冠脉狭窄程度及冠脉斑块类型的诊断效能。
结果 88例T2DM 患者能谱CCTA 诊断有56例合并冠状动脉病变,352个冠脉节段中,无狭窄134例,轻度狭窄115例,中度狭窄68例,重度狭窄10例,无斑块135例,钙化斑块26例,非钙化斑块103例,混合斑块67例。
能谱CCTA 诊断T2DM 患者冠状动脉病变的准确度为88.64%,Kappa 值为0.733;诊断冠脉轻度狭窄、中度狭窄、重度狭窄的准确度分别为95.74%、95.82%、97.73%,Kappa 值分为0.900、0.857、0.702;诊断冠脉钙化斑块、非钙化斑块、混合斑块的准确度分别为96.01%、97.43%、98.24%,Kappa 值分为0.754、0.964、0.969。
结论 能谱CCTA 诊断T2DM 患者冠状动脉病变、冠脉狭窄程度及冠脉斑块类型均具有较好的诊断效能,能为临床T2DM 合并冠状动脉病变早期诊断、治疗工作提供一定参考,值得推广。
[关键词] 能谱CT 冠状动脉血管成像;糖尿病;冠状动脉病变;冠状动脉造影;诊断价值[中图分类号] R541.4;R587.2 [文献标识码] A [文章编号] 2095-0616(2024)07-0149-05DOI:10.20116/j.issn2095-0616.2024.07.34Study on the diagnostic value of spectral coronary computedtomography angiography in diabetes patients with coronary artery diseaseYE Wanchun ZHANG Yongjie RUAN CaixiaDepartment of Radiology, the First Hospital of Fuzhou Affiliated to Fujian Medical University, Fujian, Fuzhou 350009, China [Abstract] Objective To explore the diagnostic value of spectral coronary computed tomography angiography (CCTA) in diabetes patients with coronary artery disease. Methods A total of 88 patients with suspected type 2 diabetes mellitus (T2DM) complicated with coronary artery disease admitted to The First Hospital of Fuzhou affiliated to Fujian Medical University from August 2020 to August 2022 were selected. A total of 352 coronary segments were randomly selected and examined by spectral CCTA. Coronary angiography (CAG) was used as the gold standard to analyze the diagnostic efficacy of spectral CCTA on the severity of coronary artery disease, degree of coronary stenosis, and type of coronary plaques for T2DM patients. Results Among the 88 T2DM patients diagnosed by spectral CCTA, 56 cases were complicated with coronary artery disease. Among 352 coronary segments, 134 had no stenosis, 115 had mild stenosis, 68 had moderate stenosis, 10 had severe stenosis, 135 had no plaque, 26 had calcified plaques, 103 had noncalcified plaques, and 67 had mixed plaques. The accuracy of spectral CCTA in diagnosing coronary artery disease in T2DM patients was 88.64%, and the Kappa value was 0.733. The accuracies for diagnosing mild, moderate, and severe coronary stenosis were 95.74%, 95.82%, and 97.73%, respectively. The corresponding Kappa values were 0.900, 0.857, and 0.702. The accuracies for diagnosing coronary calcified plaques, noncalcified plaques, and mixed plaques were 96.01%, 97.43%, and 98.24%, respectively. The corresponding Kappa values were 0.754, 0.964, and 0.969. Conclusion Spectral CCTA has good diagnostic efficacy in diagnosing the severity of coronary artery disease, degree of coronary stenosis, and type of coronary plaques in T2DM patients. It can provide some reference for early diagnosis and treatment of T2DM combined with coronary artery disease in clinical practice and is worth promoting.[Key words] Spectral coronary computed tomography angiography; Diabetes mellitus; Coronary artery disease; Coronary angiography; Diagnostic valueCHINA MEDICINE AND PHARMACY Vol.14 No.7 April 2024150据统计,2017年全球高达4.51亿人患有糖尿病,预计2045年全球糖尿病人数将超6.93亿人[1]。
小而密低密度脂蛋白胆固醇在糖尿病合并冠心病中的作用研究进展

小而密低密度脂蛋白胆固醇在糖尿病合并冠心病中的作用研究进展杨雨佳;李川;李莉【摘要】流行病学研究表明,糖尿病是心血管疾病的独立危险因素,糖尿病人群心血管病的发病率是非糖尿病人群的2倍;而2型糖尿病患者心血管疾病高发的原因目前公认的原因包括其所伴随的脂代谢紊乱;而多项国内外实验结果证明,冠状动脉粥样硬化的严重程度与血清中小而密低密度脂蛋白胆固醇(sdLDL-C)的水平呈正相关.因此,对sdLDL-C在2型糖尿病合并冠状动脉粥样硬化患者中的作用的阐述,有利于临床指导sdLDL-C对心血管疾病的预防和治疗.【期刊名称】《中国继续医学教育》【年(卷),期】2018(010)035【总页数】4页(P91-94)【关键词】小而密低密度脂蛋白;2型糖尿病;冠状动脉粥样硬化;脂代谢【作者】杨雨佳;李川;李莉【作者单位】中国医科大学第二临床学院,辽宁沈阳 110000;中国医科大学第二临床学院,辽宁沈阳 110000;中国医科大学附属盛京医院内分泌科,辽宁沈阳 110000【正文语种】中文【中图分类】R587流行病学研究表明,糖尿病是心血管疾病的独立危险因素,糖尿病人群心血管病的发病率是非糖尿病人群的2倍。
且众所周知,在2型糖尿病的多种并发症中,冠心病是2型糖尿病患者的主要致死原因。
国内外多项研究显示,导致2型糖尿病患者心血管疾病发病率如此高的原因并不仅仅是胰岛素和糖代谢的异常,目前比较公认的原因是2型糖尿病患者所伴随的脂代谢紊乱[1],其特点为高甘油三酯(TG)血症、低HDL-C及小密度LDL颗粒浓度升高[2]。
下面将对小而密低密度脂蛋白胆固醇在2型糖尿病合并冠心病患者中作用的研究进展做一综述。
1 2型糖尿病患者的血脂改变经大量研究验证,2型糖尿病血脂紊乱的主要原因是胰岛素抵抗。
机体的胰岛素受体或受体后缺陷,使糖不能被机体有效的利用,导致胰岛素的代偿性分泌增加,形成高胰岛素血症,进而使胰岛素外周组织对胰岛素的敏感性下降。
冠状动脉钙化的相关研究进展
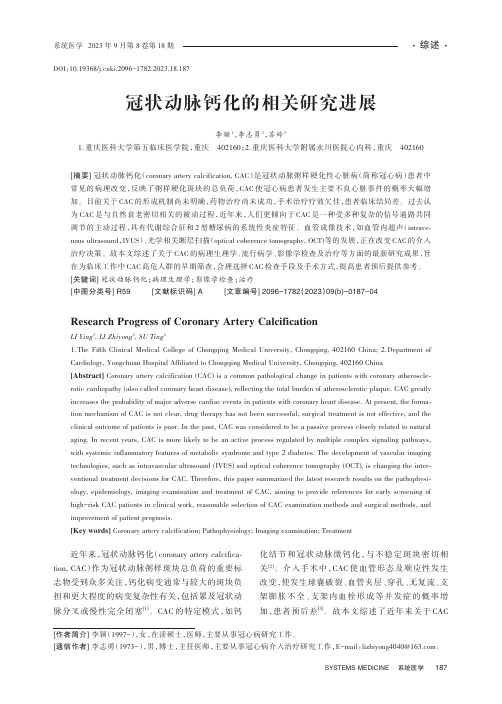
冠状动脉钙化的相关研究进展李颖1,李志勇2,苏婷21.重庆医科大学第五临床医学院,重庆402160;2.重庆医科大学附属永川医院心内科,重庆402160[摘要]冠状动脉钙化(coronary artery calcification, CAC)是冠状动脉粥样硬化性心脏病(简称冠心病)患者中常见的病理改变,反映了粥样硬化斑块的总负荷,CAC使冠心病患者发生主要不良心脏事件的概率大幅增加。
目前关于CAC的形成机制尚未明确,药物治疗尚未成功,手术治疗疗效欠佳,患者临床结局差。
过去认为CAC是与自然衰老密切相关的被动过程,近年来,人们更倾向于CAC是一种受多种复杂的信号通路共同调节的主动过程,具有代谢综合征和2型糖尿病的系统性炎症特征。
血管成像技术,如血管内超声(intrave⁃nous ultrasound,IVUS)、光学相关断层扫描(optical coherence tomography, OCT)等的发展,正在改变CAC的介入治疗决策。
故本文综述了关于CAC的病理生理学、流行病学、影像学检查及治疗等方面的最新研究成果,旨在为临床工作中CAC高危人群的早期筛查,合理选择CAC检查手段及手术方式,提高患者预后提供参考。
[关键词]冠状动脉钙化;病理生理学;影像学检查;治疗[中图分类号]R59 [文献标识码]A [文章编号]2096-1782(2023)09(b)-0187-04 Research Progress of Coronary Artery CalcificationLI Ying1, LI Zhiyong2, SU Ting21.The Fifth Clinical Medical College of Chongqing Medical University, Chongqing, 402160 China;2.Department of Cardiology, Yongchuan Hospital Affiliated to Chongqing Medical University, Chongqing, 402160 China [Abstract] Coronary artery calcification (CAC) is a common pathological change in patients with coronary atheroscle⁃rotic cardiopathy (also called coronary heart disease), reflecting the total burden of atherosclerotic plaque. CAC greatly increases the probability of major adverse cardiac events in patients with coronary heart disease. At present, the forma⁃tion mechanism of CAC is not clear, drug therapy has not been successful, surgical treatment is not effective, and the clinical outcome of patients is poor. In the past, CAC was considered to be a passive process closely related to natural aging. In recent years, CAC is more likely to be an active process regulated by multiple complex signaling pathways, with systemic inflammatory features of metabolic syndrome and type 2 diabetes. The development of vascular imaging technologies, such as intravascular ultrasound (IVUS) and optical coherence tomography (OCT), is changing the inter⁃ventional treatment decisions for CAC. Therefore, this paper summarized the latest research results on the pathophysi⁃ology, epidemiology, imaging examination and treatment of CAC, aiming to provide references for early screening of high-risk CAC patients in clinical work, reasonable selection of CAC examination methods and surgical methods, and improvement of patient prognosis.[Key words] Coronary artery calcification; Pathophysiology; Imaging examination; Treatment近年来,冠状动脉钙化(coronary artery calcifica⁃tion, CAC)作为冠状动脉粥样斑块总负荷的重要标志物受到众多关注,钙化病变通常与较大的斑块负担和更大程度的病变复杂性有关,包括累及冠状动脉分叉或慢性完全闭塞[1]。
药明奥测

品牌文化
愿景 让天下没有难诊的病 核心价值观 开放包容专心专注敢想敢拼因信得见 理念 勇·韧·耀
谢谢观看
2020年10月9日,药明奥测宣布与赛默飞世尔科技(以下简称“赛默飞”)和 Mayo Clinic合作开发的新型 冠状病毒抗体检测试剂盒 —— Thermo Scientific OmniPath COVID-19 Total Antibody ELISA,获得美国 食品药品监督管理局(FDA)紧急使用授权(EUA),并于赛默飞的美国和欧洲工厂投入生产 。
药明奥测聚焦临床、支付端痛点,凭借强大的商业资源整合能力,打造“诊·疗·药·险”生态圈,造福更 多患者及健康人群。
品牌规模
上海总部、研发中心、专业检测机构
药明奥测作为苏州市企业技术中心、苏州市企业工程技术研究中心,苏州工业园区上市苗圃企业,总部位于 上海,研发人员占比过半。旗下上海药明傲喆医学检验所(以下简称“医检所”)是专业从事临床检验服务的医 疗机构,具有医学检验实验室临床体液、血液专业,临床微生物学专业,临床化学检验专业,临床免疫、血清学 专业,临床细胞分子遗传学专业及病理科“5+1”学科及平台建设执业资质。医检所面积约3000平米,配备全球 先进的诊断设备,引进和转化Mayo Clinic临床检测项目,结合临床特检自主开发能力,打造创新型体外诊断服 务赋能平台。医检所应用与国际接轨的自动化信息系统,建立国际标准的质量管理体系,现已获得美国病理学家 协会(CAP)实验室认可,相关实验室技术能力和质量管理体系已达到世界先进水准,出具的检验报告符合国际质 量标准 。
苏州产业化基地
苏州药明泽康生物科技有限公司(简称药明泽康)总面积约 8,000m²,主要从事医疗器械和临床诊断试剂产品 的研发、注册、生产和销售以及临床诊断医学技术的开发、转让、咨询及服务。公司拥有资历深厚的研发团队, 专业的产品临床实验和注册团队,按照ISO建立生产质量管理体系。目前在质谱、病理和分子等多个技术平台上 开发诊断产品,并已有200+ 体外诊断试剂获得药监局批准,助力客户为患者提供精准诊断服务 。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Reliable Diagnostics for Coronary Artery DiseaseMatjaˇz Kukar University of Ljubljana,Faculty of Computer and Information Science,Trˇz aˇs ka25,SI-1001Ljubljana,Sloveniae-mail:matjaz.kukar@fri.uni-lj.siCiril Groˇs eljUniversity Medical Centre Ljubljana,Department for Nuclear Medicine,Zaloˇs ka7,SI-1525Ljubljana,Sloveniae-mail:ciril.groselj@kclj.si AbstractIn the past decades Machine Learning tools have been successfully used in several medical diag-nostic problems.While they often significantly outperform expert physicians(in terms of diagnostic accuracy,sensitivity,and specificity),they are mostly not being used in practice.One reason for this is that it is difficult to obtain an unbiased estimation of diagnosis’reliability.We discuss how reliability of diagnoses is assessed in medical decision making and propose a general framework for reliability estimation in Machine Learning,based on transductive inference.We compare our approach with the usual Machine Learning probabilistic approach as well as with classical step-wise diagnostic process where the reliability of diagnosis is presented as its post-test probability. The proposed transductive approach is evaluated in a practical problem of clinical diagnosis of the coronary artery disease.Significant improvements over existing techniques are achieved.Clinical decision-making is a complicated process based on experience,judgement,and reason-ing that should simultaneously integrate information from the medical literature and a variety of other sources,including quantitative results of clinical trials and,most importantly,diagnostic test results.Since no diagnostic test is perfect,thefinal decision–diagnosis of a condition in question –also carries a certain amount of imperfectness and therefore cannot be considered completely reliable.It is often crucial to know the magnitude of diagnosis’(un)reliability in order to minimize risks for the patient’s health or even life.In recent decades a Bayesian approach to integrating various test results withfindings from the patient’s history and physical examination has become increasingly popular,especially in a con-junction with stepwise diagnostic process.While the Bayesian calculation of post-test probabilities provides a physician with a quantitative assessment of diagnosis’reliability,it suffers from several problems.In this paper we propose a general strategy,a transductive reliability estimation,based on the Machine Learning(ML)paradigm.It can be used for detecting and selecting reliable diagnoses independently of the applied ML algorithms.The reasoning behind transductive approach is that in order to solve a more general task,resources may be wasted or compromises have to be made which would not have been necessary for solving only the problem at hand(i.e.to diagnose a patient vs. to diagnose the whole patient population).This common-sense principle reduces a more generalproblem of inferring a functional dependency on the whole of input space(inductive inference)to the problem of estimating the values of a function only at given points(transductive inference).The goal of our study was to determine whether it could be possible to increase number of re-liable diagnoses(both positive and negative)thus reducing unnecessary further diagnostic testing (rationalization of diagnostic procedure).We have successfully adapted this principle for estima-tion of diagnoses’reliability and compared it with post-test probability calculations of coronary artery disease.We managed to improve the specificity of reliable diagnoses by33%and sensitiv-ity by18%.We performed an extensive comparison with clinical diagnostic process and included enthusiastic physicians’responses to our results.In most clinical institutions the patients’data are stored in a central computer database.With time,more and more records that include confirmed diagnoses appear in the database.Such databases are frequently subject of retrospective studies.The patients in whom the outcome has already occurred are selected and analyzed,thus looking backward to assess potential risk factors and diagnostic principles.Retrospective studies naturallyfit in the ML application framework, which is becoming increasingly popular as a support tool in medical decision making.Having collected a set of patient descriptions with confirmed diagnoses,the task of a ML al-gorithm is to automatically generate a model(a description)of the given data with respect to the correct diagnosis.A set of possible diagnoses is used as a target for classification process.A gen-erated model can subsequently be used for risk factors’assessment and decision-making support. Unfortunately,only little work has been done in ML to assess reliability of individual decisions.2.1.Assessment of post-test probabilityIn past decades a Bayesian approach to integrating various test results withfindings from the patient’s history and physical examination has become increasingly popular.By this approach the post-test diagnostic probability is calculated from the pre-test probability(prevalence of a disease), diagnostic test’s outcome,sensitivity and specificity,thus providing a basis for a quantitative estima-tion of diagnosis’reliability.This approach is often used in a conjunction with stepwise diagnostic process,where diagnostic tests are performed sequentially until the post-test probability of a disease exceeds certain threshold,usually[1].While the Bayesian calculation of post-test probabili-ties provides a physician with a quantitative assessment of diagnosis’reliability,it has from several problems.Those include obtaining exact values for pre-test probabilities and diagnostic tests’sen-sitivity and specificity,as well as an unbiased test result and selection of conditionally independent (in Bayesian sense)diagnostic tests[3,8].2.2.Transductive reliability estimation in Machine LearningWe propose a general strategy,a transductive reliability estimation[4,5],for detecting and selecting reliable diagnoses independently of the applied ML algorithms.Basically,we have a two-step process,featuring an inductive step followed by a transductive step.An inductive step is just like an ordinary inductive learning process in Machine Learning.A Machine Learning algorithm is run on the training set,inducing a classifier.A selectedexample is taken from an independent dataset and classified using the induced classifier.An example,labelled with the classified class is included into the training set.A transductive step is almost a repetition of an inductive step.A Machine Learning al-gorithm is run on the changed training set,transducing a classifier.The same example as before is taken from the independent dataset and and classified using the transduced classi-fier.Both classifications(probability distributions)of the same example are compared and their difference(symmetric Kullback-Leibler divergence)is calculated,thus approximating the randomness deficiency.A classification–or a diagnosis–is considered reliable if the difference in probability distributions between the two above steps is small enough1.The idea behind transductive reliability estimation leverages two approaches.Thefirst one is the iid(identically independently distributed)assumption,usually used in statistical models and Machine Learning,and the second one is randomness deficiency[2,7].Basically,we estimate how much the randomness of the training set(in a Kolmogorov complexity sense)would change if it included a new example.2.3.Clinical diagnostics of coronary artery diseaseCoronary artery disease(CAD)is one of the most important cause of mortality in the world.It is caused by diminished bloodflow through coronary arteries due to stenosis or occlusion.CAD produces impaired function of the heart andfinally the necrosis of the myocardium(infarction). During the exercise the volume of the blood pumped to the body has to be increased,this causing the bloodflow through the coronary arteries to be increased as well.In a(low grade)CAD the bloodflow as perfusion of the myocardium is adequate at rest or during a moderate exercise,but insufficient during a severe exercise.Therefore,signs and symptoms of the disease develop only during the exercise.There are four diagnostic levels of CAD.1.Signs and symptoms of the disease are evaluated clinically and ECG is performed at rest.2.This is followed by sequential ECG testing during controlled exercises by gradually increas-ing the work load of the patient.3.If the previous test is not conclusive,or if additional information regarding the perfusion ofthe myocardium is needed,myocardial scintigraphy is performed at rest and during exercise.4.If an invasive therapy of the disease is contemplated,the diagnosis has to be confirmed byimaging of the coronary vessels(coronary angiography).In our study we used a dataset of327patients(250males,77females)with performed clinical and laboratory examinations,exercise ECG,myocardial scintigraphy and coronary angiography be-cause of suspected CAD.The features from the ECG an scintigraphy data were extracted manually by the clinicians(up to77attributes).In228cases the disease was angiographically confirmed and in99cases it was excluded.162patients had suffered from recent myocardial infarction.The patients were selected from a population of approximately4000patients who were examined at the Nuclear Medicine Department between1991and1994.We selected only the patients with com-plete diagnostic procedures(all four levels)[6].For determining the pre-test probability we applied a tabular calculation,consisting of three attributes(age,sex,type of chest pain),retrieved from[9].We performed all our experiments by using naive Bayesian classifier[4]as our ML tool of choice,since it usually performs very well in medical problems and can comprehensibly explain its classifications to the physicians.However,this does not mean that our approach is limited to this ML paradigm.In fact,many different ML approaches,such as decision trees,K-nearest neighbour and neural networks have been tested within the framework of transductive reliability estimations [5]and all of them performed well.3.1.Experiments in the clinical diagnostics of CADIn the stepwise diagnostic process we measured after each completed step the percentage(share) of reliable diagnoses(with the post-test probability over),and errors made in this process (percentage of incorrectly diagnosed patients with seemingly reliable diagnoses).We evaluated the problem in four different settings:Case1:Physicians.Stepwise diagnostic process is performed by physicians.Pre-test probabilities are obtained from literature.A boundary for reliable diagnoses is(post-test probability). Case2:Stepwise Machine Learning.Stepwise diagnostic process is performed by using a ML classifier(naive Bayesian classifier)for evaluation of each offirst three diagnostic levels.A boundary for reliable diagnoses is(post-test probability).Case3:Naive Bayes.Diagnostics with all attributes available on the third diagnostic level(my-ocardial scintigraphy)using naive Bayes classifier.A boundary for reliable diagnoses is(probability of the most probable class).Case4:Naive Bayes(transductive).Diagnostics with all attributes available on the third level using naive Bayesian classifier.Reliability of diagnosis is estimated with transductive method (Sec. 2.2).A boundary for reliable diagnoses is automatically calculated,using internal leave-one-out testing procedure.The experimental results are presented in Tab.1.In cases1and2(stepwise diagnostic process for physicians and naive Bayesian classifier)the performance in terms of reliable classifications was quite similar.In cases3and4we used all available attributes on the third diagnostic level(myocar-dial scintigraphy).In both cases we significantly outperformed physicians in terms of classification accuracy,sensitivity and specificity.Naive Bayesian classifier’s diagnoses’reliability was assessed by classifier’s probability(case3)and by transductive method(case4).The calculated boundary for reliable estimations was,which is quite close to for post-test probabilities.The overall results in case4are quite impressive.While the number of reliable classifications stays on the same high level as in case3(naive Bayes with all attributes),the total number of errors drops significantly below physicians’levels.In a direct comparison,naive Bayes(transductive)im-proved the number of reliable positive diagnoses by0.18(18%)and the number of reliable negative diagnoses even by0.33(33%)!The number of errors in positive diagnoses is slightly higher than the physicians’,while the number of errors in negative diagnoses dropped below0.04(4%)!For comparison of physicians’and transductive Bayes’performance a reliable ROC curves for positive and negative patients are depicted in Fig.2(a)and Fig.2(b).In both cases the ROC curve for transductive reliable estimations(marked ML)lies above the physician’s ROC curve and closer to the left top corner,that an ideal ROC curve should touch.In the problem of clinical diagnostics of CAD the physicians are mostly interested in increasing numbers of correctly diagnosed negative patients after the third diagnostic level(higher specificityparison between physicians’results and different ML approaches.Remarkable improvements achieved with transductive Bayesian classifier are emphasized.1.Physicians(post-test)0.850.850.860.720.030.460.082.Naive Bayes(post-test)0.890.910.830.790.050.460.033.Naive Bayes(class prob.)0.910.920.870.900.070.810.114.Naive Bayes(transductive)0.910.920.870.900.050.790.04T r u e r e l i a b l e p o s i t i v e r a t e (a)Reliable ROC curve on positive patients.(b)Reliable ROC curve on negative pa-tients.Figure parison of reliability estimations between physicians (post-test probabilities)and transductive reliability estimation.10%-15%less patients needing to perform coronary angiography test seems reasonable.We are aware that the results of the CAD study are obtained on a significantly restricted popula-tion and therefore may not be generally applicable to the normal population,i.e.to all the patients coming to the Nuclear Medicine Department.Further studies are in progress to verify our find-ings on larger population.In particular,on-line data gathering,advocated in our previous papers,has now at least partially entered everyday practice and may result in providing us with a more representative dataset in the near future.[1]G.A.Diamond and J.S.Forester.Analysis of probability as an aid in the clinical diagnosis of coronary arterydisease.New England Journal of Medicine ,300:1350,1979.[2] A.Gammerman,V .V ovk,and V .Vapnik.Learning by transduction.In Proceedings of theConference on Uncertainty in Artificial Intelligence ,pages 148–155,Madison,Wisconsin,1998.[3]L.Goldman and E.Braunwald.Primary Cardiology .W.B.Saunders Company,Philadelphia,Pennsylvania,1998.[4]M.Kukar.Making reliable diagnoses with machine learning:A case study.In Proc.European Conference onArtificial Intelligence in Medicine ,pages 65–74,Porto,Portugal,2001.[5]M.Kukar.Transductive reliability estimation for medical diagnosis.Artificial Intelligence in Medicine ,2002.Toappear.[6]M.Kukar,I.Kononenko,C.Groˇs elj,K.Kralj,and J.Fettich.Analysing and improving the diagnosis of ischaemicheart disease with machine learning.Artificial Intelligence in Medicine ,16(1):25–50,1999.[7]M.Li and P.Vit´a nyi.An introduction to Kolmogorov complexity and its applications .Springer-Verlag,New York,edition,1997.[8]M.Olona-Cabases.The probability of a correct diagnosis.In J.Candell-Riera and D.Ortega-Alcalde,editors,Nuclear Cardiology in Everyday Practice ,pages 348–357.Kluwer,1994.[9] puter-assisted interpretation of noninvasive tests for diagnosis of coronary artery disease.Car-diovasc.Rev.Rep.4,pages 367–375,1983.。