器官移植临床案例二
因器官移植引发法律案件(3篇)

第1篇一、引言近年来,随着医学技术的不断发展,器官移植手术已成为挽救无数患者生命的重要手段。
然而,在器官移植过程中,由于种种原因,引发了一系列法律纠纷。
本文将针对因器官移植引发的几起典型案例进行分析,探讨相关法律问题,以期对我国器官移植立法和司法实践提供借鉴。
二、案例分析1.案例一:器官捐献纠纷基本案情:患者甲因患有重症肝病,急需进行肝脏移植手术。
甲的家属在得知甲病情危重后,向当地红十字会提出器官捐献申请。
红十字会组织协调,在甲去世后,将甲的肝脏捐献给患者乙。
然而,甲的家属在得知乙的病情好转后,认为乙是故意拖延甲的治疗,导致甲死亡。
于是,甲的家属将乙及其所在医院告上法庭,要求赔偿损失。
法院判决:法院认为,甲的家属与乙之间不存在合同关系,乙并非故意拖延甲的治疗。
甲的死亡与乙的行为无直接因果关系。
因此,法院驳回了甲家属的诉讼请求。
2.案例二:器官移植中介纠纷基本案情:患者丙因患有尿毒症,急需进行肾脏移植手术。
丙的家属通过中介公司找到了合适的肾脏捐赠者丁。
然而,在移植手术过程中,中介公司未履行告知义务,导致丙在手术中发生意外。
丙的家属将中介公司告上法庭,要求赔偿损失。
法院判决:法院认为,中介公司作为专业机构,有义务向患者及其家属提供真实、全面的移植信息。
中介公司在此次事件中存在过错,应当承担相应的赔偿责任。
因此,法院判决中介公司赔偿丙家属一定数额的损失。
3.案例三:器官移植费用纠纷基本案情:患者戊因患有晚期癌症,急需进行肝脏移植手术。
戊的家属通过众筹平台筹集手术费用。
然而,在手术完成后,医院向戊家属索要高额手术费用。
戊家属认为医院收费标准过高,拒绝支付。
双方发生纠纷,戊家属将医院告上法庭。
法院判决:法院认为,医院在收费方面应当遵循合理、公正的原则。
在此次事件中,医院收费标准过高,损害了戊家属的合法权益。
因此,法院判决医院退还部分手术费用。
三、法律问题探讨1.器官捐献的法律效力我国《人体器官移植条例》规定,器官捐献应当遵循自愿、无偿的原则。
器官移植伦理

人体器官移植的历史
临床阶段——肾移植 肾移植 临床阶段 1960年,北医吴阶平教授开展国内首例 年 同种异体肾移植。 同种异体肾移植。 1972年,国内首例孪生兄弟肾移植在北 年 京友谊医院获得成功。 京友谊医院获得成功。
附属二院在东北三省率先开展肾脏移植手术,其技术处于国内先进行列, 附属二院在东北三省率先开展肾脏移植手术,其技术处于国内先进行列, 迄今已成功实施近500例,其中存活时间最长的患者已健康生活了二十年 迄今已成功实施近 例
【案例2】中国“盗窃”眼角膜案 案例 】中国“盗窃”
从供体中取出角膜
医大一院刘平教授正在进行角膜移植手术
1998年10月,北京某医院一名眼科医生 年 月 在准备为两位失去视力的病人移植角膜时, 在准备为两位失去视力的病人移植角膜时, 发现储存的角膜已经坏死。于是, 发现储存的角膜已经坏死。于是,他进入停 尸房,摘取了一女性尸体的角膜, 尸房,摘取了一女性尸体的角膜,然后为她 换上了义眼。此事没有告知死者家属, 换上了义眼。此事没有告知死者家属,也没 有获得家属同意。在火葬前, 有获得家属同意。在火葬前,家属发现死者 角膜已被摘除,后来将医生告上法庭, 角膜已被摘除,后来将医生告上法庭,控告 他犯盗尸罪。 他犯盗尸罪。
1997年附属二院普外科肝移植课题组成功为患者实施了肝脏移植手术 年附属二院普外科肝移植课题组成功为患者实施了肝脏移植手术 成为我省肝移植生存时间最长、 成为我省肝移植生存时间最长、国内生存质量最好的肝移植病人之一
2005年附属四院开展黑龙江省第一例经典原位非转流 年附属四院开展黑龙江省第一例经典原位非转流 同种肝移植, 同种肝移植,提高了我省在肝脏移植领域的治疗水平
人体器官移植的历史
临床阶段——肺移植 肺移植 临床阶段 1963年,哈代首先开展了同种异体肺移植 年
医学伦理案例分析
医学伦理案例分析医学伦理是指医学领域中涉及道德、价值观和法律规范的伦理问题。
在医学实践中,经常会遇到一些涉及伦理的案例,这些案例需要我们进行深入的分析和思考,以便做出正确的决策和处理。
下面,我们将就一些医学伦理案例进行分析。
案例一,医生隐瞒病情。
某位医生在诊断一名患者时发现,患者患有晚期癌症,预后不乐观。
医生决定不告诉患者真相,以免给患者带来精神上的伤害。
然而,这种做法引发了伦理上的争议。
一方面,医生有义务告知患者病情,让患者有权利知道自己的病情和治疗方案;另一方面,医生也应该考虑到患者的心理承受能力,避免过多的负面影响。
针对这个案例,我们需要权衡医生的职业道德和患者的权益。
在这种情况下,医生可以选择与患者进行沟通,了解患者的心理状态和意愿,然后再决定是否告知病情。
同时,医生也可以寻求其他医疗团队成员或专业的心理医生的意见,共同商讨最合适的决策。
案例二,器官捐献。
一名患者因患有严重的器官疾病,需要进行器官移植手术。
患者的家属同意捐献患者的器官,以挽救其他患者的生命。
然而,这也牵涉到伦理上的问题。
首先,患者本人是否在意愿书上表达了器官捐献的意愿?其次,家属是否真正理解并同意了器官捐献的意义和后果?在这个案例中,医生需要尊重患者和家属的意愿,但同时也需要确保患者的权益不受侵犯。
医生可以与家属进行深入的沟通,解释器官捐献的意义和程序,同时也需要尊重患者的意愿。
在整个过程中,医生需要做到真诚、耐心,并尊重患者和家属的决定。
案例三,医疗资源分配。
在一些医疗资源匮乏的地区,医生需要面对医疗资源分配的难题。
例如,一名急需手术的患者需要使用一台唯一的手术设备,而同时还有其他患者也需要使用这台设备。
医生需要如何决定分配这个医疗资源?在这种情况下,医生需要考虑到患者的病情严重程度、手术的紧急性、患者的生存机会等因素。
医生需要权衡每位患者的权益,同时也需要考虑到医疗资源的合理利用。
在这个过程中,医生需要做出公正、合理的决策,并尽量避免主观因素的影响。
关于器官移植的法律案例(3篇)

第1篇一、背景近年来,随着医疗技术的不断发展,器官移植已成为治疗某些疾病的有效手段。
然而,器官移植过程中涉及的伦理、法律问题也日益凸显。
本文将以某市首例活体肾脏移植案为例,分析器官移植法律案例。
二、案情简介2019年,某市居民李某因患有慢性肾功能衰竭,急需进行肾脏移植手术。
经检查,李某的配偶王某与李某的HLA配型相符,愿意无偿捐献肾脏。
在得知此消息后,李某及其家属感激不已,希望尽快进行移植手术。
然而,在移植手术前,李某及其家属向医院提出要求,希望王某在手术前进行医学伦理审查,以确保移植手术的合法性和合规性。
三、争议焦点1. 活体肾脏移植的合法性2. 医院在移植手术前的伦理审查义务3. 捐赠者与受赠者之间的权利义务关系四、案例分析1. 活体肾脏移植的合法性根据《中华人民共和国器官移植条例》第二条规定,器官移植是指将人体器官从捐献者体内取出,植入受者体内,以替代其原有功能的行为。
根据该条例,活体肾脏移植属于合法行为。
2. 医院在移植手术前的伦理审查义务《医疗机构管理条例》第三十八条规定,医疗机构应当建立健全伦理审查制度,对涉及伦理问题的诊疗活动进行审查。
在本案中,医院在移植手术前对王某进行了医学伦理审查,符合法律规定。
3. 捐赠者与受赠者之间的权利义务关系根据《中华人民共和国合同法》第三百九十七条规定,赠与的财产依法需要办理登记等手续的,应当办理有关手续。
在本案中,王某自愿捐赠肾脏,李某及其家属对王某表示感激,双方之间形成了赠与关系。
根据《中华人民共和国合同法》第三百九十八条规定,赠与人在赠与财产的权利转移之前可以撤销赠与。
在本案中,王某在手术前撤销了捐赠,但李某及其家属并未因此受到损失。
五、结论本案中,某市首例活体肾脏移植案在法律层面得到了妥善处理。
通过分析本案,我们可以得出以下结论:1. 活体肾脏移植在我国是合法的,但仍需遵守相关法律法规。
2. 医院在移植手术前应进行伦理审查,确保移植手术的合法性和合规性。
器官移植临床案例二
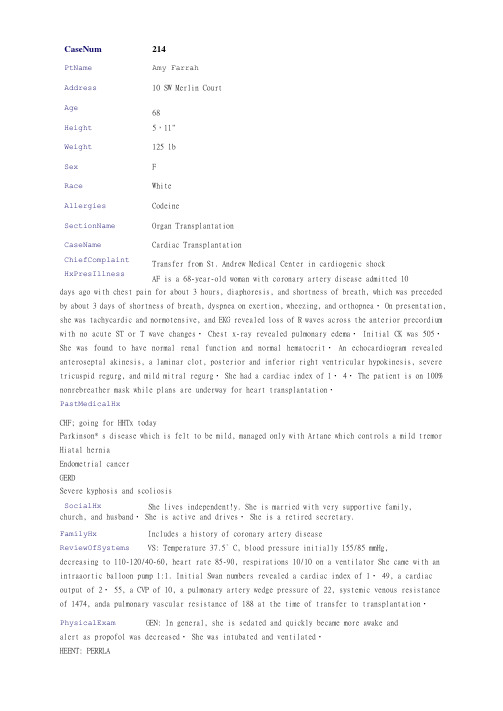
CaseNum214PtName Amy FarrahAddress10 SW Merlin CourtAge68Height5,11"Weight125 lbSex FRace WhiteAllergies CodeineSectionName Organ Transplantation CaseName Cardiac TransplantationChiefComplaint HxPresIllness Transfer from St. Andrew Medical Center in cardiogenic shockAF is a 68-year-old woman with coronary artery disease admitted 10days ago with chest pain for about 3 hours, diaphoresis, and shortness of breath, which was preceded by about 3 days of shortness of breath, dyspnea on exertion, wheezing, and orthopnea・On presentation, she was tachycardic and normotensive, and EKG revealed loss of R waves across the anterior precordium with no acute ST or T wave changes・ Chest x-ray revealed pulmonary edema・ Initial CK was 505・She was found to have normal renal function and normal hematocrit・An echocardiogram revealed anteroseptal akinesis, a laminar clot, posterior and inferior right ventricular hypokinesis, severe tricuspid regurg, and mild mitral regurg・ She had a cardiac index of 1・ 4・ The patient is on 100% nonrebreather mask while plans are underway for heart transplantation・PastMedicalHxCHF; going for HHTx todayParkinson* s disease which is felt to be mild, managed only with Artane which controls a mild tremor Hiatal herniaEndometrial cancerGERDSevere kyphosis and scoliosisSocialHx She lives independent!y. She is married with very supportive family, church, and husband・ She is active and drives・ She is a retired secretary.FamilyHx Includes a history of coronary artery diseaseReviewOfSystems VS: Temperature 37.5° C, blood pressure initially 155/85 mmHg,decreasing to 110-120/40-60, heart rate 85-90, respirations 10/10 on a ventilator She came with an intraaortic balloon pump 1:1. Initial Swan numbers revealed a cardiac index of 1・ 49, a cardiac output of 2・ 55, a CVP of 10, a pulmonary artery wedge pressure of 22, systemic venous resistance of 1474, anda pulmonary vascular resistance of 188 at the time of transfer to transplantation・PhysicalExam GEN: In general, she is sedated and quickly became more awake andalert as propofol was decreased・ She was intubated and ventilated・HEENT: PERRLACARDIOVASCULAR: SI, S2・ Balloon pump made heart sounds difficult to assess further・LUNGS: Bilateral crackles to bilateral bases but bilateral exchange throughout・ ABDOMEN: Bowel sounds were active・ Abdomen was soft・ There was no obvious hepatosplenomegaly・EXTREMITIES: Cool but pink・ Distal pulses were palpable・ There was no edema・LabsAndDxTests Sodium 137 mEq/LPotassium 3・ 6 mEq/LChloride 94 mEq/LHC0330 mEq/LBUN 28 mg/LCreatinine 1・1 mg/LMg 2 mg/dLWBC 7500/nim3Hematocrit 32. 7%Platelets 158 x 10VLDiagnosis Cardiogenic shock and heart transplantationRPhNotes New admit for heart transplantCaseNum214Que st Num Question2131When monitoring serum concentration of tacrolimus, the recommended a trough level is:AnswerChoiceA2-3 ng/mL. AnswerChoiceB5-15 ng/mL.AnsweirChoi ceC150-250 ng/mL・AnswerChoi ceD250-500 ng/mL・AnswerChoi ceE greater than 500 ng/mL・Correc tAnswer Explanation BFollowing oral administration, approximately 20% of the dose isabsorbed in the GI tract・ Tacrolimus concentration can be measured in both plasma and blood. Whole blood is the preferred method for measuring tacrolimus blood concentration・ Tacrolimus levels should be maintained in a range of 5-15 ng/mL・ Levels greater than 20 ng/mL have been associated with nephrotoxicity, neurotoxicity, and diabetogenicity・CompetencyStmt 1.2.6K-TypeCaseNum214Que st Num Question 2132Which of the following medications require close plasma therapeuticmonitoring?<br>I. aAzathioprine<br>II. 6Steroids<br>III. Tacrolimus AnswerChoi ceA I onlyAnswcrChoiceB III onlyAnswerChoi ceC I and II onlyAnswerChoi ceD II and III onlyAnswerChoi ceE I, II, and IIICorrec tAnswer Explanation BTacrolimus trough levels should be maintained in a range of 5-15ng/mL・ Clinical pharmacokinetic studies do not suggest a strong correlation between plasma concentration and pharmacodynamic properties of steroids and azathioprine・ Because of high interindividual variability and wider therapeutic indices in azathioprine and steroid plasma levels, therapeutic drug monitoring is not required in these agents・CompetencyStmt 1.2.6K-Type CaseNum K 214qid<br>3<br>4/ll<br>D429828<br>@<br>Fluconazole<br>12<br>100 mg po daily<br>0Que st Num Question 2133Which of the following is the dose-limiting toxicity of tacrolimus?<br>I・ Nephrotoxicity<br>II・ Alopecia<br>III・ Diarrhea AnswerChoi ceA I onlyAnswerChoi ceB III onlyAnswerChoi ceC I and II onlyAnswerChoi ceE I, II, and IIICorrec tAnswer Explanation AA variety of adverse drug reactions have been reported with the useof tacrolimus・ Evidence suggests that tacrolimus-induced adverse drug reactions are typically associated with a highblood concentration・ Alopecia and diarrhea have been reported in patients with low troughatacrolimus levels・CoapetencyStmt1・ 2・ 4K-TypeCaseNum214Que st Num Question 2134How would you monitor a patient taking tacrolimus? <br>I. Serumcreatinine, cardiac function tests<br>II・ Blood pressure, diabetes<br>III. Plasma therapeutic concentrationAnswerChoiccA I onlyAnswerChoi ccB III onlyAnswerChoi ceC I and II onlyAnswerChoi ceD II and III onlyAnswerChoi ceE I, II, and IIICorrec tAnswcr Explanation between plasmaEClinical pharmacokinetic studies do suggest a strong correlation concentration and toxicity of tacrolimus・ Plasma concentration oftacrolimus should be monitored very closely to avoid toxicity・ However, some patients may experience adverse drug reactions despite normal tacrolimus leve1・ Therefore, itis essential to monitor for blood pressure and diabetes following transplantation・CompctencyStmt 1.2.3K-TypeCaseNum214QuestNum Question<br>I・ patient* s2135The primary criteria for selecting an immunosuppressive drug is:> risk factors for acute rejection and infection・〈br〉II. efficacy andsafety・II. cost.AnswerChoi ceA I only AnswerChoi ccB III only AnswerChoi ccC I and II only AnswerChoi ccD II and III onlyCorrec tAnswer Explanation immunosuppressive immunosuppressive immunosuppressive limiting adverse immunosuppressiveCRisk factors of acute rejection, efficacy, and safety of therapy should all be considered before formulating an protocol for each individual patient・The focus of an protocol should be on decreasing the risk of acute rejection anddrug reactions・ Although the cost is important, cost of drugs are only 5% of the total cost of transplantation・CompetencyStmt 1. 1. 3 K-TypeCaseNum214Quest Num Question sirolimus・〈br>II.2136The most likely cause of hypertension in this patient is: <br>I・tacrolimus・ <br>III. prednisone・AnswerChoi ceA I only AnswerChoi ceB III only AnswerChoi ccC I and II only AnswerChoiceD II and III only AnswerChoi ceE I, II, and IIICorrec tAnswer Explanation DSeveral studies have shown that prednisone and tacrolimus canelevate blood pressure・ The long-term effect of sirolimus on blood pressure remains unknown, but recent data indicate that sirolimus has a limited effect on blood pressure・ Therefore, only II and III are correct・CompctcncyStmt 1.2.3K^TypeQuestionsirolimus therapy? Nephrotoxicity Which of the following clinical tests are used for monitoring <br>I・ WBC (white blood counts)<br>II・ Sirolimus level<br>III.AnswerChoi ceA I only AnswcrChoiccB III only AnswerChoi ccC I and II only AnswerChoi ceD II and III only AnswerChoi ceE I, II, and IIICorrec tAnswer Explanation CClinical pharmacokinetic studies suggest a strong correlationbetween plasma concentration of sirolimus and toxicity・ Plasma sirolimus concentrations should be monitored very closely to avoid toxicity・ However, some patients may develop hyperlipidemia and neutropenia despite normal sirolimus levels・ Nephrotoxicity is not a common complication of sirolimus therapy・Compc tencyStmt 1.2.3K-TypeCascNum214QuestNum Questionrange for a trough 2138When monitoring serum concentrations of sirolimus, the recommended level is:AnswcrChoiccA1-2 ng/mL・AnswerChoi ceB10-20 ng/mL・AnswerChoi ceC40-50 ng/mL・AnswerChoi ceD150-250 ng/mL・AnswcrChoiceE greater than 250 ng/mL・Correc tAnswer Explanation BLike other agents with narrow therapeutic windows, sirolimus levelsshould be monitored very closely to avoid acute rejection or toxicities・ Sirolimus levels should be maintained in a range of 10-20 ng/mL・Compe tcncyStmt 1.2.6K-TypeQuestion The most common cause(s) of post-transplant hyperlipidemia is: <br>I・ mycophenolate・〈br>II. sirolimus・〈br>III. prednisone.AnswcrChoiceA I onlyAnswerChoi ceB III onlyAnswerChoi ceC I and II onlyAnswerChoi ceD II and III onlyAnswerChoi ceE I, II, and IIICorrcc tAnswcr Explanation DHyperlipidemia developing after heart transplantation is nearlyuniversal, occurring in 70-80% of patients・ Although the exact pathogenesis of hyperlipidemia following transplantation is still being determined, several studies have shown that both prednisone and sirolimus are independent risk factors for the development of hyperlipidemia・CompetencyStmt 1. 3. 1K-TypeCaseNum214Que st Num Question 2140Which of the following immunosuppressive drugs is associated withcausing gingival hyperplasia?AnswerChoi ceA CyclosporineAnswerChoi ceB TacrolimusAnswerChoi ceC MycophenolateAnswerChoiccD Both cyclosporine and mycophenolate AnswerChoi ceE Cyclosporine and tacrolimusCorrec tAnswer Explanation AGingival hyperplasia has been attributed to the use of cyclosporineonly. Other commonly used drugs in transplant that might increase the risk of this cosmetic adverse reaction are Nifedipine and Dilantin・Compc tencyStmt 1.2.2K-Type214器官移植病人姓名:艾米•法拉地址:莫林院西南10号年龄:68 身高:156cm性别:女性种族:白人体重:57Kg过敏史:可待因主诉转移来自安德鲁医疗中心心源性休克。
活体亲属供肾移植二例报告
因而手 术成功率较高 , 排斥反应 较 肾 , 2供 者取 左 肾。硬 膜 外 麻 醉后 取 上 腹腹 直 肌 切 免疫抑制剂剂量 , 例 出现并发症机会也少 , 其长期存活率明显高于尸体 口, 剪开结肠旁沟侧后腹膜 , 肾脂肪囊 内注人生理盐水 少 , 10 +2 0ml %利 多 卡 因 2 , Oml游离 肾脏 , 露 肾蒂 , 暴 仔细 肾移植 。括体亲属供肾移植是解决国内目前供肾不足 如 分离肾动静脉 , 一步游离输尿管并在髂血管上方 4 的有效 途 径 。国外 活体 亲 属 供 肾移 植 较 普 遍 , 美 国 进 5 挪 6c 切断 。术 中充 分补 液 , 断 肾蒂前静 注速 尿 2 活体 亲 属 供 肾移 植 占肾移植 病例 的 2 %, 威 占 m 离 O 0 土耳 其达 8 %【 而我 国报 道较 少 【 。 5 , , m 及肝索 10n , g 0 a 待出现利尿现象后分 别切断 肾动 4 % , g
维普资讯
第 1卷 9
20 0 2年 第1 期 来自2月 湖南
医
学
W .9 N 6 1 o
20 02
Hum dcl o ma r n Me i u l aJ
活体 亲 属供 肾移 植 二 例报 告
朱 华 臣, 雷光前 , 钟发 平 , 周建辉 , 黄
中国湖 南 ( 湖南省 常德 市 第一人 民 医院 ,
[ 关键词 】 肾移植 ; 活俸供 肾 ; 近亲 [ 中圈分类号 】 R 1 ;692 [ 献标识码】 B [ 编号】 10 ~92 ( 0 }1 01 — 2 67R 9 文 文章 0 1 412 20 — 05 0 0
关于器官移植的法律案例(3篇)

第1篇案情简介:张某,男,45岁,因患有晚期肝硬化,急需进行肝脏移植手术。
李某,男,35岁,因意外事故不幸去世,其家属在悲痛之余,决定将李某的肝脏捐献给张某。
经过严格的医学评估和伦理审查,张某与李某的肝脏移植手术得以顺利进行。
然而,在术后一个月,张某突然出现严重的排斥反应,经抢救无效死亡。
张某的家属认为李某的肝脏存在质量问题,遂将李某的家属告上法庭,要求赔偿损失。
一、案件背景1. 器官移植的现状:随着医学技术的不断发展,器官移植已成为挽救众多患者生命的重要手段。
然而,器官供体严重短缺,器官分配不均等问题一直困扰着器官移植事业的发展。
2. 器官捐献的法律规定:根据《中华人民共和国器官移植条例》和《人体器官捐赠管理办法》,我国实行自愿、无偿、统一的器官捐献制度。
任何单位和个人不得买卖人体器官,不得利用人体器官进行商业广告宣传。
3. 器官移植的法律纠纷:器官移植涉及多个法律关系,包括器官捐献者、受赠者、医疗机构和医务人员等。
在器官移植过程中,可能会出现医疗事故、器官质量问题、伦理争议等问题,引发法律纠纷。
二、案件经过1. 器官捐献:李某因意外事故去世,其家属在悲痛之余,决定将李某的肝脏捐献给张某。
经医院评估,李某的肝脏符合移植条件。
2. 器官移植手术:在经过严格的医学评估和伦理审查后,张某与李某的肝脏移植手术得以顺利进行。
术后,张某的病情有所好转。
3. 排斥反应:术后一个月,张某突然出现严重的排斥反应,经抢救无效死亡。
张某的家属认为李某的肝脏存在质量问题,遂将李某的家属告上法庭。
三、争议焦点1. 器官质量问题:张某的家属认为李某的肝脏存在质量问题,导致张某在术后出现排斥反应,最终死亡。
2. 医疗机构的责任:张某的家属认为医院在器官移植过程中存在过错,未对器官进行严格检测,导致李某的肝脏存在质量问题。
3. 李某家属的责任:张某的家属认为李某的家属在器官捐献过程中存在过错,未对李某的身体健康状况进行充分了解,导致李某的肝脏存在质量问题。
肾移植手术的成功案例

肾移植手术的成功案例肾移植手术是一种常见的治疗终末期肾脏疾病的方法,成功的肾移植手术可以让患者恢复正常的肾功能,提高生活质量。
下面列举了十个成功的肾移植手术案例。
1. 张先生是一名患有多囊肾的患者,他的肾功能逐渐下降,最终进入了终末期肾脏疾病。
经过严格的筛选和配型,他成功接受了一位亲属的肾脏移植手术。
手术后,张先生的肾功能得到了很好的恢复,他现在能够正常工作和生活。
2. 李女士是一位年轻的肾脏捐赠者,她毅然决然决定捐献自己的一个肾脏给需要肾移植的患者。
经过手术后,李女士的身体恢复得很快,而接受了她肾脏的患者也顺利康复,两人现在都非常健康。
3. 王先生是一位患有先天性肾疾病的患者,他的肾功能非常差。
经过一段时间的等待,他终于等到了一位逝者的肾脏,成功进行了肾移植手术。
手术后,王先生的肾功能逐渐恢复,他现在能够正常工作和参加体育活动。
4. 赵女士是一名患有IgA肾病的患者,她的肾功能不断下降。
经过医生的评估和筛选,她成功接受了一个无关亲属的肾脏移植手术。
手术后,赵女士的肾功能得到了很好的恢复,她现在能够正常生活,不再需要进行透析治疗。
5. 杨先生是一位患有肾功能衰竭的患者,他的肾脏逐渐失去了正常的功能。
经过严格的匹配和配型,他成功接受了一位捐赠者的肾脏移植手术。
手术后,杨先生的肾功能明显改善,他的生活质量也得到了很大的提高。
6. 孙女士是一位年轻的肾脏捐赠者,她自愿捐献自己的一个肾脏给需要肾移植的患者。
经过手术后,孙女士的身体迅速恢复,而接受了她肾脏的患者也成功康复,两人现在都过上了健康的生活。
7. 刘先生是一位患有糖尿病肾病的患者,他的肾功能严重受损。
经过一段时间的等待,他终于等到了一位逝者的肾脏,成功进行了肾移植手术。
手术后,刘先生的肾功能得到了很好的恢复,他现在能够正常工作和参加社交活动。
8. 徐女士是一名患有遗传性肾病的患者,她的肾功能逐渐恶化。
经过医生的评估和筛选,她成功接受了一个无关亲属的肾脏移植手术。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
CaseNum214PtName Amy FarrahAddress10 SW Merlin CourtAge68Height5' 11"Weight125 lbSex FRace WhiteAllergies CodeineSectionName Organ TransplantationCaseName Cardiac TransplantationChiefComplaint Transfer from St. Andrew Medical Center in cardiogenic shock HxPresIllness AF is a 68-year-old woman with coronary artery disease admitted 10 days ago with chest pain for about 3 hours, diaphoresis, and shortness of breath, which was preceded by about 3 days of shortness of breath, dyspnea on exertion, wheezing, and orthopnea. On presentation, she was tachycardic and normotensive, and EKG revealed loss of R waves across the anterior precordium with no acute ST or T wave changes. Chest x-ray revealed pulmonary edema. Initial CK was 505. She was found to have normal renal function and normal hematocrit. An echocardiogram revealed anteroseptal akinesis, a laminar clot, posterior and inferior right ventricular hypokinesis, severe tricuspid regurg, and mild mitral regurg. She had a cardiac index of 1.4. The patient is on 100% nonrebreather mask while plans are underway for heart transplantation.PastMedicalHxCHF; going for HHTx todayParkinson's disease which is felt to be mild, managed only with Artane which controls a mild tremorHiatal herniaEndometrial cancerGERDSevere kyphosis and scoliosisSocialHx She lives independently. She is married with very supportive family, church, and husband. She is active and drives. She is a retired secretary.FamilyHx Includes a history of coronary artery diseaseReviewOfSystems VS: Temperature 37.5°C, blood pressure initially 155/85 mmHg, decreasing to 110-120/40-60, heart rate 85-90, respirations 10/10 on a ventilatorShe came with an intraaortic balloon pump 1:1. Initial Swan numbers revealed a cardiac index of 1.49, a cardiac output of 2.55, a CVP of 10, a pulmonary artery wedge pressure of 22, systemic venous resistance of 1474, anda pulmonary vascular resistance of 188 at the time of transfer to transplantation.PhysicalExam GEN: In general, she is sedated and quickly became more awake and alert as propofol was decreased. She was intubated and ventilated.HEENT: PERRLACARDIOVASCULAR: S1, S2. Balloon pump made heart sounds difficult to assess further. LUNGS: Bilateral crackles to bilateral bases but bilateral exchange throughout. ABDOMEN: Bowel sounds were active. Abdomen was soft. There was no obvious hepatosplenomegaly.EXTREMITIES: Cool but pink. Distal pulses were palpable. There was no edema. LabsAndDxTests Sodium 137 mEq/LPotassium 3.6 mEq/LChloride 94 mEq/LHCO330 mEq/LBUN 28 mg/LCreatinine 1.1 mg/LMg 2 mg/dLWBC 7500/mm3Hematocrit 32.7%Platelets 158 x 109/LDiagnosis Cardiogenic shock and heart transplantationRxRecordRPhNotes New admit for heart transplantCaseNum214QuestNum2131Question When monitoring serum concentration of tacrolimus, the recommended range for a trough level is:AnswerChoiceA2-3 ng/mL.AnswerChoiceB5-15 ng/mL.AnswerChoiceC150-250 ng/mL.AnswerChoiceD250-500 ng/mL.AnswerChoiceE greater than 500 ng/mL.CorrectAnswer BExplanation Following oral administration, approximately 20% of the dose is absorbed in the GI tract. Tacrolimus concentration can be measured in both plasma and blood. Whole blood is the preferred method for measuring tacrolimus blood concentration. Tacrolimus levels should be maintained in a range of 5-15 ng/mL. Levels greater than 20 ng/mL have been associated with nephrotoxicity, neurotoxicity, and diabetogenicity.CompetencyStmt 1.2.6K-TypeCaseNum214QuestNum2132Question Which of the following medications require close plasma therapeutic monitoring?<br>I.áAzathioprine<br>II.áSteroids<br>III. TacrolimusAnswerChoiceA I onlyAnswerChoiceB III onlyAnswerChoiceC I and II onlyAnswerChoiceD II and III onlyAnswerChoiceE I, II, and IIICorrectAnswer BExplanation Tacrolimus trough levels should be maintained in a range of 5-15 ng/mL. Clinical pharmacokinetic studies do not suggest a strong correlation between plasma concentration and pharmacodynamic properties of steroids and azathioprine. Because of high interindividual variability and wider therapeutic indices in azathioprine and steroid plasma levels, therapeutic drug monitoring is not required in these agents.CompetencyStmt 1.2.6K-Type KCaseNum214qid<br>3<br>4/11<br>D429828<br>@<br>Fluconazole<br>12<br>100 mg po daily<br>0QuestNum2133Question Which of the following is the dose-limiting toxicity of tacrolimus? <br>I. Nephrotoxicity<br>II. Alopecia<br>III. DiarrheaAnswerChoiceA I onlyAnswerChoiceB III onlyAnswerChoiceC I and II onlyAnswerChoiceD II and III onlyAnswerChoiceE I, II, and IIICorrectAnswer AExplanation A variety of adverse drug reactions have been reported with the use of tacrolimus. Evidence suggests that tacrolimus-induced adverse drug reactions are typically associated with a highblood concentration. Alopecia and diarrhea have been reported in patients with low troughátacrolimus levels.CompetencyStmt 1.2.4K-Type KCaseNum214QuestNum2134Question How would you monitor a patient taking tacrolimus? <br>I. Serum creatinine, cardiac function tests<br>II. Blood pressure, diabetes<br>III. Plasma therapeutic concentrationAnswerChoiceA I onlyAnswerChoiceB III onlyAnswerChoiceC I and II onlyAnswerChoiceD II and III onlyAnswerChoiceE I, II, and IIICorrectAnswer EExplanation Clinical pharmacokinetic studies do suggest a strong correlation between plasma concentration and toxicity of tacrolimus. Plasma concentration of tacrolimus should be monitored very closely to avoid toxicity. However, some patients may experience adverse drug reactions despite normal tacrolimus level. Therefore, it is essential to monitor for blood pressure and diabetes following transplantation.CompetencyStmt 1.2.3K-Type KCaseNum214QuestNum2135Question The primary criteria for selecting an immunosuppressive drug is: <br>I. patient's risk factors for acute rejection and infection.<br>II. efficacy and safety. <br>III. cost. AnswerChoiceA I onlyAnswerChoiceB III onlyAnswerChoiceC I and II onlyAnswerChoiceD II and III onlyAnswerChoiceE I, II, and IIICorrectAnswer CExplanation Risk factors of acute rejection, efficacy, and safety of immunosuppressive therapy should all be considered before formulating an immunosuppressive protocol for each individual patient. The focus of an immunosuppressive protocol should be on decreasing the risk of acute rejection and limiting adverse drug reactions. Although the cost is important, cost of immunosuppressive drugs are only 5% of the total cost of transplantation.CompetencyStmt 1.1.3K-Type KCaseNum214QuestNum2136Question The most likely cause of hypertension in this patient is: <br>I. sirolimus.<br>II. tacrolimus. <br>III. prednisone.AnswerChoiceA I onlyAnswerChoiceB III onlyAnswerChoiceC I and II onlyAnswerChoiceD II and III onlyAnswerChoiceE I, II, and IIICorrectAnswer DExplanation Several studies have shown that prednisone and tacrolimus can elevate blood pressure. The long-term effect of sirolimus on blood pressure remains unknown, but recent data indicate that sirolimus has a limited effect on blood pressure. Therefore, only II and III are correct.CompetencyStmt 1.2.3K-Type KeCaseNum214QuestNum2137Question Which of the following clinical tests are used for monitoring sirolimus therapy? <br>I. WBC (white blood counts)<br>II. Sirolimus level<br>III. Nephrotoxicity AnswerChoiceA I onlyAnswerChoiceB III onlyAnswerChoiceC I and II onlyAnswerChoiceD II and III onlyAnswerChoiceE I, II, and IIICorrectAnswer CExplanation Clinical pharmacokinetic studies suggest a strong correlation between plasma concentration of sirolimus and toxicity. Plasma sirolimus concentrations should be monitored very closely to avoid toxicity. However, some patients may develop hyperlipidemia and neutropenia despite normal sirolimus levels. Nephrotoxicity is not a common complication of sirolimus therapy.CompetencyStmt 1.2.3K-Type KCaseNum214QuestNum2138Question When monitoring serum concentrations of sirolimus, the recommended range for a trough level is:AnswerChoiceA1-2 ng/mL.AnswerChoiceB10-20 ng/mL.AnswerChoiceC40-50 ng/mL.AnswerChoiceD150-250 ng/mL.AnswerChoiceE greater than 250 ng/mL.CorrectAnswer BExplanation Like other agents with narrow therapeutic windows, sirolimus levels should be monitored very closely to avoid acute rejection or toxicities. Sirolimus levels should be maintained in a range of 10-20 ng/mL.CompetencyStmt 1.2.6K-TypeCaseNum214QuestNum2139Question The most common cause(s) of post-transplant hyperlipidemia is: <br>I. mycophenolate.<br>II. sirolimus.<br>III. prednisone.AnswerChoiceA I onlyAnswerChoiceB III onlyAnswerChoiceC I and II onlyAnswerChoiceD II and III onlyAnswerChoiceE I, II, and IIICorrectAnswer DExplanation Hyperlipidemia developing after heart transplantation is nearly universal, occurring in 70-80% of patients. Although the exact pathogenesis of hyperlipidemia following transplantation is still being determined, several studies have shown that both prednisone and sirolimus are independent risk factors for the development of hyperlipidemia. CompetencyStmt 1.3.1K-Type KCaseNum214QuestNum2140Question Which of the following immunosuppressive drugs is associated with causing gingival hyperplasia?AnswerChoiceA CyclosporineAnswerChoiceB TacrolimusAnswerChoiceC MycophenolateAnswerChoiceD Both cyclosporine and mycophenolateAnswerChoiceE Cyclosporine and tacrolimusCorrectAnswer AExplanation Gingival hyperplasia has been attributed to the use of cyclosporine only. Other commonly used drugs in transplant that might increase the risk of this cosmetic adverse reaction are Nifedipine and Dilantin.CompetencyStmt 1.2.2K-Type214 器官移植病人姓名:艾米·法拉地址:莫林院西南10号年龄:68身高:156cm性别:女性种族:白人体重:57Kg过敏史:可待因主诉转移来自安德鲁医疗中心心源性休克。