抗菌药物临床应用管理软件操作手册
抗菌药物临床应用操作规程与流程
抗菌药物临床应用操作规程与流程1. 背景随着抗菌药物的广泛应用,抗菌药物的合理使用和管理显得尤为重要。
为了确保患者的安全和有效治疗,制定本操作规程与流程,规范抗菌药物的临床应用。
2. 目的本操作规程与流程的目的是确保抗菌药物的临床应用符合科学、规范和安全的原则,以提高治疗效果,并减少抗菌药物的滥用和耐药性的发展。
3. 操作规程3.1 抗菌药物的选择和配方- 根据患者的病情和临床实验室的细菌培养和药敏结果,选择合适的抗菌药物进行治疗。
- 遵循抗菌药物使用的指南和标准剂量进行配方,不得越权使用或滥用抗菌药物。
3.2 抗菌药物的使用和监测- 必须经过临床医生的合理判断和授权,合理使用抗菌药物。
- 定期监测患者病情和疗效,评估抗菌药物的效果和需要调整的情况。
- 对于需要长期使用抗菌药物的患者,应定期进行血药浓度监测,避免剂量过高或过低。
3.3 抗菌药物的药品管理- 对抗菌药物进行分类管理,确保存放和使用的安全性和正确性。
- 抗菌药物的进货、发放和使用必须有相关部门的批准和监督。
- 定期检查抗菌药物的库存和过期情况,并及时处理过期药物。
4. 流程4.1 患者入院- 患者入院后,临床医生根据病情判断是否需要使用抗菌药物。
- 根据医生的处方,药剂师准备抗菌药物。
4.2 抗菌药物使用- 护士按照医嘱和药剂师提供的抗菌药物,进行患者的药物给予和记录。
- 定期监测患者的病情和临床实验室结果,及时调整药物治疗。
4.3 抗菌药物管理- 药剂师负责抗菌药物的分类管理和库存管理。
- 相关部门定期检查抗菌药物的管理情况和库存情况。
5. 总结本操作规程与流程是指导抗菌药物临床应用的重要文件,通过规范化和标准化的管理,可以提高抗菌药物的使用效果和安全性,减少滥用和耐药性的风险。
医院抗菌药物临床应用程序
医院抗菌药物临床应用程序
为规范抗菌药物的临床应用,根据《抗菌药物临床应用指导原则》、《卫生部办公厅关于抗菌药物临床应用管理有关问题的通知》、《抗菌药物临床应用管理办法》,结合我院实际,制订抗菌药物临床应用程序。
一、医疗机构和医务人员应当严格掌握使用抗菌药物预防感染的指证。
二、治疗感染要有明确的使用抗菌药物指证,使用抗菌药物前,尽可能取相关标本送微生物室培养。
三、预防感染、治疗轻度或者局部感染应当首选非限制使用级抗菌药物。
四、严重感染、免疫功能低下合并感染或者病原菌只对限制使用级抗菌药物敏感时,经上级医生查房确认后,方可选用限制使用级抗菌药物。
由具有相应处方权医师开具处方。
五、严格控制特殊使用级抗菌药物使用。
特殊使用级抗菌药物不得在门诊使用。
临床应用特殊使用级抗菌药物应当严格掌握用药指证,经科主任提出会诊申请,由抗菌药物管理小组指定的专业技术人员会诊同意后,由具有相应处方权医师开具处方。
特殊使用级抗菌药物会诊人员由具有抗菌药物临床应用经验的感染性疾病科、呼吸科、重症医学科、微生物检验科、药学部门等具有高级专业技术职务资格的医师、药师或具有高级专业技术职务任职资格的抗菌药物专业临床药师担任。
六、因抢救生命垂危的患者等紧急情况,医师可以越级使用抗菌药物。
越级使用抗菌药物应当在病程中详细记录用药指证,并应当于24小时内
补办越级使用抗菌药物的必要手续。
黄石医院抗菌药物使用手册

Minocycline
Imipenem
Glycylcyclines
Newer carbapenems Trinems
Penicillin Prontosil
Semi-synthetic penicillins & cephalosporins
Chloramphenicol Neomycin Polymixin Streptomycin Thiacetazone
12.4.10我院召开医药购销和医疗服 务中突出问题专项整治工作动员大会
用药之道:知己知彼
知药知病 百战不殆
知药不知病 祈天保佑 不知药不知病 危乎殆哉
知
药
抗感染药物发展简史
熟知所用药物:
抗菌谱 适应症 PK/PD 用法 不良反应
抗感染药物发展简史
1929 Alexander Fleming 发现青霉素
1929 1935-40 1940 1940-50 1953 1959 1960 1970 1980 1990A. FLEMING 发现青霉素 磺胺 分离提纯青霉素G成功,用于临床 链、氯、金、土、红、卡那、利福、多粘菌素 发现头孢菌素 提纯青霉素母核— 6-APA成功 半合成青霉素,发现三甲氧苄胺嘧啶(TMP) 头孢菌素迅速发展、半合成青霉素推出酰脲类 头孢发展到第三代,新型β-内酰胺类出现 喹诺酮类抗菌药崛起 头孢菌素、喹诺酮类进一步发展
Synthetic approaches
Newer macrolides & ketolides
Rifampicin
Rifapentine Semi-synthetic glycopeptides Semi-synthetic streptogramins
抗菌药物审批系统操作说明
抗菌药物审批系统操作说明
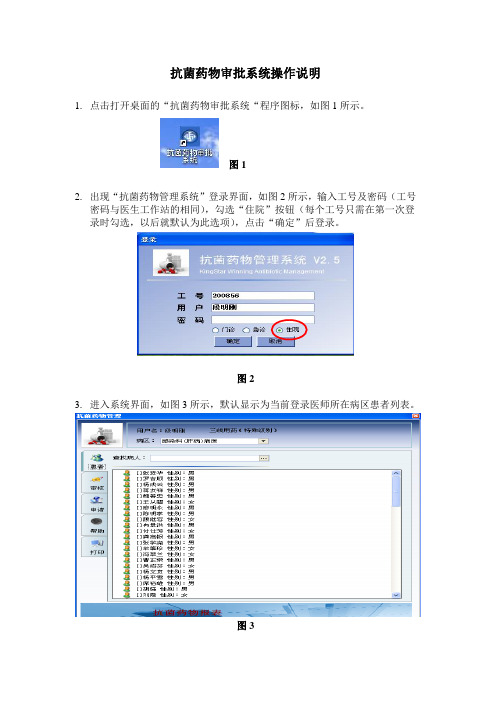
1.点击打开桌面的“抗菌药物审批系统“程序图标,如图1所示。
图1
2.出现“抗菌药物管理系统”登录界面,如图2所示,输入工号及密码(工号
密码与医生工作站的相同),勾选“住院”按钮(每个工号只需在第一次登录时勾选,以后就默认为此选项),点击“确定”后登录。
图2
3.进入系统界面,如图3所示,默认显示为当前登录医师所在病区患者列表。
图3
4.点击“审核”菜单,即出现抗菌药物审批界面,如图4所示。
图4
5. 双击需审批的记录,弹出“抗菌药物用药审核”界面,在审批意见栏中输入意见(此项为必填项)后,点击“通过”或“拒绝”按钮后即可。
图5。
抗菌药物临床应用管理培训(共60张PPT)
4、 G—杆菌:
大肠杆菌、痢疾杆菌、伤寒杆菌、肠杆菌、克 雷伯杆菌〔肺炎杆菌〕、奇异变形杆菌、吲哚阳 性变形杆菌、普鲁威登菌、沙雷菌、拟杆菌、 螺 旋杆菌、流感嗜血杆菌、百日咳杆菌、布氏杆菌 、肉芽肿夹膜杆菌、铜绿杆菌、军团菌、不动杆 菌、枸橼酸杆菌、耶森氏菌、霍乱弧菌、耐酸杆 菌〔结核杆菌、麻风杆菌〕。
〔二〕真菌
浅表部真菌:癣菌
深部真菌:
白色念珠菌、新型隐球菌、曲霉菌、毛 霉菌
大多数真菌为时机性致病菌,一般
具有免疫能力的寄生体不会被感染;只有
当宿主免疫力低下才导致疾病的发生。
〔三〕支原体、衣原体
支原体:肺炎支原体 衣原体:沙眼衣原体、鹦鹉衣原体
〔四〕螺旋体
克拉霉素与铋剂、甲硝唑联用治疗幽门螺杆菌感染。
对浓度依赖型抗菌药物可qd (重症感染者例外)。
1、时间依赖型抗菌药物
特点:
梅毒螺旋体〔青霉素有效〕 克拉霉素与铋剂、甲硝唑联用治疗幽门螺杆菌感染。
5减少护理工作量。 第四代头孢菌素抗菌谱及其特点
哌拉西林、阿莫西林、头孢曲Байду номын сангаас钠
雅司螺旋体 〔青霉素有效〕 特点,选择用药。
2、对各种β-内酰胺酶稳定性远较第二、三代
头孢哌酮最强〕及厌氧菌如脆弱拟杆
〔五〕立克次体
普氏立克次体:流行性斑疹伤寒 莫氏立克次体:地方性斑疹伤寒 埃里希体属微生物:Q热、战壕热 羌虫病立克次体:羌虫病
2、头孢菌素类〔二〕
第一代头孢菌素抗菌谱及特点
1、对需氧G+球菌,抗菌作用比第二代略强,显 著超过第三代,仅少数对G—有抗菌活性;头
孢唑林抗G—杆菌活性为此类中活性最强。
2、对各种β-内酰胺酶稳定性远较第二、三代 差,可被G—菌的β-内酰胺酶所破坏。
抗菌药物临床应用实施细则手册

抗菌药物临床应用实施细则手册目录1.医院关于进一步加强抗菌药物临床应用管理的通知 (1)2.医院抗菌药物临床应用分级管理办法及目录 (8)3.医院特殊使用抗菌药物临床应用规定及会诊专家名单 (12)4.医院抗菌药物处方/医嘱专项点评管理办法 (13)5.医院抗菌药物临床应用督查和奖惩细则 (15)6.抗菌药物临床应用管理办法(卫生部令第84号)............. 错误!未定义书签。
7.抗菌药物临床应用指导原则(2015年版) (24)8.卫生部2009年38号文内容摘要 (48)9.我院关于Ⅰ类切口预防性使用抗菌药物的管理规定 (48)10.《国家卫生计生委办公厅关于进一步加强抗菌药物临床应用管理遏制细菌耐药的通知》摘要 (49)11.建立碳青霉烯类抗菌药物以及替加环素使用专档管理的规定 (52)医院关于进一步加强抗菌药物临床应用管理的通知为落实《抗菌药物临床应用指导原则》(2015年版)、国家卫生计生委“关于进一步加强抗菌药物临床应用管理工作的通知(国卫办医发[2015]42号)”和“进一步改善医疗服务行动计划”有关要求,规范我院抗菌药物临床应用,保障医疗质量与安全,对我院进一步加强抗菌药物临床合理应用提出以下要求:一、严格落实抗菌药物临床应用管理有关法规要求,明确抗菌药物临床应用管理责任严格落实《医疗机构管理条例》、《处方管理办法》、《医疗机构药事管理规定》、《抗菌药物临床应用管理办法》、《医院处方点评管理规范(试行)》等法规规定,加强抗菌药物管理,明确工作职责,完善工作制度,细化工作流程,对抗菌药物品种、品规的遴选、采购、处方、调剂、临床应用和评价等各个环节进行全过程管理与监控。
严格落实抗菌药物管理责任,医院院长是抗菌药物临床合理应用的第一责任人,各临床科室主任是科室抗菌药物合理应用的第一责任人。
各临床科室以科主任负责制实现抗菌药物临床合理应用各项指标,把抗菌药物合理应用情况作为科室主任综合目标考核以及晋升、评先评优的重要指标。
护士抗生素管理工具包和综合用户指南说明书
2019 Toolkit and Comprehensive User Guide to Enhance Nursing Antibiotic Stewardship Activities: Nurses Take Antibiotic Stewardship Action InitiativeDespite discussions at the national level about the need to integrate nurses into antibiotic stewardship (AS) activities, there are limited tools and resources for Antimicrobial Stewardship Programs (ASPs), nursing, or hospital leadership to facilitate implementation of nurse-based AS interventions in acute care hospitals. This toolkit provides materials to:(a) engage front-line nurses in AS, (b) obtain leadership support to implement nurse-driven AS activities, and (c) implement a nurse-driven diagnostic stewardship intervention to improve urine and respiratory culturing practices and a penicillin allergy algorithm to improve penicillin allergy documentation.This toolkit and guide were developed by the Johns Hopkins University with collaboration from the Johns Hopkins Hospital Department of Antimicrobial Stewardship, with support from a U.S. Centers for Disease Control and Prevention (CDC)contract.ContributorsProject Development:Johns Hopkins University:Valeria Fabre, MDSara E. Cosgrove MD, MS Elizabeth Zink, MS, RN, CCNS, CNRN Lauren Rosales, BA, BSN-RN Ashley Pleiss, RN, BSN The Office of Antibiotic Stewardship, Centers for Disease Control and Prevention:Arjun Srinivasan, MDLauri Hicks, DOMelinda Neuhausser, PharmD, MPHProject Management:Alejandra B. Salinas, BS Research Program Coordinator George F. Jones IV, BS Research Program CoordinatorTable of ContentsIntroduction to the Emergent Role of Nursing in AS and Potential Outcomes of Nursing Involvement.. 3 Facilitator Guide to Obtain Support from Stakeholders (3)Implementation Checklist (4)Implementation Framework (4)Educational Material (5)Algorithms (6)Troubleshooting Guide (7)Additional Resources (7)References (8)Introduction to the Emergent Role of Nursing in AS and Potential Outcomes of Nursing InvolvementParticipation of nurses in Antibiotic Stewardship (AS) activities is recommended by the American Nurses Association and the Centers for Disease Control and Prevention [1]. However, there is a paucity of information on how or what nursing interventions lead to improved antibiotic use in acute care settings. Nurses have indicated that some activities that may impact antibiotic use (e.g., providing input on the necessity of bacterial cultures) are within their scope of practice [2]. While clinical pathways to optimize urine and respiratory culturing adopted by nurses in the long-term care (LTC) setting have improved patient care [3, 4], such approaches have not been employed in most acute care settings.In the hospital, most AS interventions occur after patients have microbiology cultures or infectious diagnostic tests sent and empiric antimicrobial therapy started, when the opportunity to review the necessity of microbiology cultures, or a Clostridioides difficile stool test or a patient’s antibiotic allergy history to ensure prompt receipt of the best empiric therapy has passed. Nurses generally interact with patients before the AS team and often before primary prescribers; thus, they are in a unique position to positively influence decisions about sending microbiology cultures, a C. difficile stool test and obtaining initial antibiotic allergy histories. Nurses have been instrumental in reducing hospital-acquired infections such as catheter-associated urinary tract infections (CAUTI) and central line-associated bloodstream infections (CLABSI) by implementation of checklists and bundle interventions.While bedside nurses are not responsible for prescribing antibiotics themselves, nurses can still play a role in AS. There are many proposed ways in which nurses can enhance AS activities [1, 5]. In this toolkit, we provide tools and resources to implement nurse-driven interventions aiming at (1) reducing unnecessary urine culture with the ultimate goal of reducing inappropriate antibiotic treatment of asymptomatic bacteriuria (ASB), (2) reducing unnecessary respiratory cultures with the ultimate goal of reducing inappropriate antibiotics for positive respiratory cultures without clinical evidence of bacterial pneumonia, (3) reducing unnecessary testing for C. difficile with the goal of reducing unnecessary treatment in patients who are likely colonized in who C. difficile antibiotic therapy may enhance toxin production at the same time of affecting the patient’s gut micro biota and (3) improving penicillin allergy documentation with the goal of increasing β–lactam use whenever possible and indicated.Facilitator Guide to Obtain Support from StakeholdersOne of the first steps in engaging front-line nurses in AS activities is to obtain support from both nursing and physician groups. We recommend starting the conversation with the unit manager to assess feasibility, learn about competing initiatives, understand unit priorities and define the best time to implement new initiatives. In some hospitals the unit manager may need toconsult/obtain approval with the director of nursing before any quality improvement project is initiated to ensure appropriate approvals are in place.The initial contact may be via electronic mail; however a follow up in-person meeting is strongly recommended.∙An email template to start the conversation with providers is provided here.∙An email template to start the conversation with nurses is provided here.∙Talking points regarding the importance of integration of nurses in AS are provided here:o The Role of the Bedside Nurse in AS Slide Decko The Role of the Bedside Nurse in AS ScriptImplementation ChecklistThis checklist will assist the individual considering to implement a nurse-driven AS intervention in ensuring all basic steps have been considered before launching the initiative.∙Checklist provided here.Implementation FrameworkIn order to integrate staff nurses into AS activities in a meaningful and sustainable way, nurses need to: a) learn the principles of AS and particular topics most relevant to them such as best culturing practices or obtaining accurate penicillin allergy histories, b) be able to communicate effectively with the rest of the medical team about these topics, and c) be familiar with an implementation framework. The Plan-Do-Study-Act cycle is a commonly used quality improvement framework that is an iterative process beginning with developing a plan to test a proposed improvement change (Plan), carrying out the test (Do), observing and learning from the consequences (Study), and determining what modifications should be made to the test (Act). Some advantages of adopting such framework include: opportunity to examine if the proposed change is leading to the desired improvement and opportunity to addresses concerns of those involved to prevent major setbacks.To assess the progress of the intervention, the team will need to think of how this will be tracked. In the case of microbiologic cultures, the team may be able to get a report from either the electronic medical record or from the microbiology laboratory. Temporal trends can be performed in Microsoft Excel (Microsoft Office Professional Plus 2016). Run charts and control charts present data over time and enable quick identification of variation that is unlikely due to chance (special-cause variation)[6]. Run charts display data over time with a median line that indicates the central tendency. Control charts have advantages over run charts in that they define expected variation in a process; they provide an upper and lower control limits defined by the distribution of the data with 3 standard deviations above or below the centerline.Additional discussion on how to best display and analyze data can be found here: ∙Introduction to Quality Improvement∙Displaying and Analyzing Quality Improvement DataAdditionally, depending on resources the team may want to review cases to provide feedback on appropriateness and ongoing inappropriate reasons for testing. Likewise for the penicillin allergy documentation improvement project, providing feedback on specific areas of documentation will be helpful for nurses to know where the gaps are (e.g., review some cases and report percentage of cases with non-specified skin rash).A more in-depth reading regarding a practical approach to integrate bedside nurses in AS can be found here:∙ A Practical Approach to Integrating Bedside Nurses into Antibiotic Stewardship Educational MaterialNurses have previously identified limited formal education on antibiotics and microbiology as a barrier to their participation in AS activities [7, 8]. In this toolkit, you will find four 15—30 minute topic-specific modules with accompanying scripts:•Urinary Tract Infection 101 for Nurseso Slide Decko Script•Pneumonia 101 for Nurseso Slide Decko Script•Penicillin Allergy 101 for Nurseso Slide Decko Script•Clostridioides difficile 101 for Nurseso Slide Decko ScriptThese presentations were developed for nurses; however, the materials can be used by other health care providers (e.g., physicians in training, medical students, medical assistants, respiratory therapists, occupational and/or physical therapy).Key points regarding urine and respiratory cultures and documentation of penicillin allergy have been summarized into one-page documents and are available here:∙Urine Cultures One Pager∙Respiratory Cultures One Pager∙Penicillin Allergy One PagerAlgorithmsPrior to algorithm implementation, a meeting should be held with nurses to ensure they understand the content of the algorithms and feel comfortable using them. The algorithms are intended for use by nurses primarily but not exclusively (the algorithms can be used by any healthcare provider with authority to document allergy histories and or order urine and respiratory cultures).Instructions for Urine Culture Algorithm Use•The algorithm can be found here.•This algorithm is for use in hospitalized adult patients with or without an indwelling urinary catheter.•The algorithm should not be used for the following patients: pregnant women and those undergoing urologic procedures associated with mucosal bleeding.•We recommend not using this algorithm for patients with neurogenic bladder given that symptoms in these patients may be unusual and not addressed in the algorithm or forpatients with renal transplant < 1 month since the role of treatment of ASB in the early post-transplant period remains under investigation.•An additional resource recommended for use in conjunction with this algorithm is the SBAR Tool (Situation-Background-Assessment-Recommendation) to aid nurses incommunicating their assessments to the respective ordering provider. The tool is alsoprovided in Additional Resources below.Instructions for Respiratory Culture Algorithm Use•The algorithm can be found here.•This algorithm is for use in hospitalized adult patients in intensive care units.•If the pathway in the algorithm ends in “do no collect a respiratory specimen for bacterial culture, communicate with ordering provider”, review the need for therespiratory culture with the rest of the primary team.•An additional resource recommended for use in conjunction with this algorithm is the SBAR Tool (Situation-Background-Assessment-Recommendation) to aid nurses incommunicating their assessments to the respective ordering provider. The tool is alsoprovided in Additional Resources below.Instructions for Penicillin Allergy Algorithm Use∙Use this algorithm for patients who report an allergy to penicillin and/or aminopenicillins (amoxicillin, ampicillin), or for patients who develop a reaction topenicillin during their hospital stay in order to accurately document the reaction type.∙The algorithm with pictures of most common skin reactions can be found here.o If utilizing this version, print in color for maximum impact. This algorithm contains a list of most common β-lactams to help your patient in recalling theantibiotic they were allergic to, or any β-lactams they have taken successfullysubsequent to their allergic episode.∙The same algorithm without pictures and can be printed in black and white and can be found here.The instructions for algorithm use are also available as attachments and are provided here: ∙Instructions for Urine Culture Algorithm Use∙Instructions for Respiratory Culture Algorithm Use∙Instructions for Penicillin Allergy Algorithm UseTroubleshooting GuideThis guide provides common scenarios with solutions that may be encountered when implementing a nurse-driven AS intervention. It outlines some barriers and solutions that may be encountered during the process of involving nurses in antibiotic stewardship activities. For an additional resource on implementation of nurse-driven stewardship interventions, refer to the article below (also present in Implementation Framework).∙Troubleshooting Guide∙ A Practical Approach to Integrating Bedside Nurses into Antibiotic Stewardship Additional Resources∙ A focus group guide to assess baseline knowledge and perceptions regarding antibiotic use and antibiotic stewardship.∙Progress report templates:o Urine Progress Report Templateo Respiratory Progress Report Templateo Penicillin Allergy Documentation Progress Report Template ∙ A logo for nurse antibiotic stewardship activities and initiatives:o Proud to be a Nurse Antibiotic Steward Logo∙SBAR Communication Tool∙Penicillin allergy materials for unit floor:o Interpretation guides to most commonly seen skin reactions to antibiotics:▪Skin Reaction Interpretation Form for Nurses▪Skin Reaction Interpretation Form for Patientso An assessment tool for nurses:Penicillin Allergy Assessment Tool for Nurseso Penicillin allergy documentation reminders to place on workstations:▪Penicillin Allergy Trigger for WorkstationsReferences1.White Paper: Redefining the Antibiotic Stewardship Team: Recommendations from theAmerican Nurses Association/Centers for Disease Control and Prevention Workgroup on the Role of Registered Nurses in Hospital Antibiotic Stewardship Practices. 2017.2.Carter EJ, Greendyke WG, Furuya EY, et al. Exploring the nurses' role in antibioticstewardship: A multisite qualitative study of nurses and infection preventionists. Am JInfect Control 2018; 46(5): 492-7.3.Carusone SC, Loeb M, Lohfeld L. A clinical pathway for treating pneumonia in thenursing home: part II: the administrators' perspective and how it differs from nurses'views. J Am Med Dir Assoc 2006; 7(5): 279-86.4.Zabarsky TF, Sethi AK, Donskey CJ. Sustained reduction in inappropriate treatment ofasymptomatic bacteriuria in a long-term care facility through an educationalintervention. Am J Infect Control 2008; 36(7): 476-80.5.Monsees EA, Tamma PD, Cosgrove SE, Miller MA, Fabre V. Integrating bedside nursesinto antibiotic stewardship: A practical approach. Infect Control Hosp Epidemiol 2019;40(5): 579-84.6.Brady PW, Tchou MJ, Ambroggio L, Schondelmeyer AC, Shaughnessy EE. QualityImprovement Feature Series Article 2: Displaying and Analyzing Quality ImprovementData. J Pediatric Infect Dis Soc 2018; 7(2): 100-3.7.Monsees E, Popejoy L, Jackson MA, Lee B, Goldman J. Integrating staff nurses inantibiotic stewardship: Opportunities and barriers. Am J Infect Control 2018; 46(7): 737-42.8.Greendyke WG, Carter EJ, Salsgiver E, et al. Exploring the Role of the Bedside Nurse inAntimicrobial Stewardship: Survey Results From Five Acute-Care Hospitals. InfectControl Hosp Epidemiol 2018; 39(3): 360-2.。
抗菌药物临床应用具体操作流程

抗菌药物临床应用具体操作流程下载温馨提示:该文档是我店铺精心编制而成,希望大家下载以后,能够帮助大家解决实际的问题。
文档下载后可定制随意修改,请根据实际需要进行相应的调整和使用,谢谢!并且,本店铺为大家提供各种各样类型的实用资料,如教育随笔、日记赏析、句子摘抄、古诗大全、经典美文、话题作文、工作总结、词语解析、文案摘录、其他资料等等,如想了解不同资料格式和写法,敬请关注!Download tips: This document is carefully compiled by theeditor.I hope that after you download them,they can help yousolve practical problems. The document can be customized andmodified after downloading,please adjust and use it according toactual needs, thank you!In addition, our shop provides you with various types ofpractical materials,such as educational essays, diaryappreciation,sentence excerpts,ancient poems,classic articles,topic composition,work summary,word parsing,copy excerpts,other materials and so on,want to know different data formats andwriting methods,please pay attention!一、抗菌药物临床应用具体操作流程1. 诊断和治疗计划制定1.1 病史采集1.1.1 询问患者病史,包括症状、体征、既往病史等1.1.2 进行体格检查,了解患者的病情1.1.3 采集必要的实验室检查结果,如血常规、尿常规、细菌培养等1.2 病原学检查1.2.1 根据病情需要,进行病原学检查,如细菌培养、病毒检测等1.2.2 确定病原体种类和药敏试验结果1.2.3 结合病原学检查结果,制定治疗计划2. 抗菌药物选择2.1 抗菌药物种类2.1.1 根据病原学检查结果,选择敏感的抗菌药物2.1.2 考虑药物的抗菌谱、药代动力学特性、副作用等因素2.1.3 避免使用耐药性高的抗菌药物2.2 抗菌药物剂量2.2.1 根据患者体重、年龄、病情等因素,确定抗菌药物剂量2.2.2 参考药物说明书和相关指南,制定合适的剂量2.2.3 注意药物的剂量调整,以避免药物过量或不足3. 抗菌药物给药途径3.1 口服给药3.1.1 选择合适的口服抗菌药物3.1.2 确定给药频率和给药时间3.1.3 注意药物的饮食禁忌和胃肠道反应3.2 静脉给药3.2.1 选择合适的静脉抗菌药物3.2.2 确定给药速度和给药时间3.2.3 注意药物的过敏反应和静脉炎等副作用3.3 局部给药3.3.1 选择合适的局部抗菌药物3.3.2 确定给药频率和给药时间3.3.3 注意药物的局部刺激和感染扩散等风险4. 用药监护4.1 血药浓度监测4.1.1 监测抗菌药物的血药浓度4.1.2 根据血药浓度结果,调整药物剂量和给药方案4.1.3 避免药物浓度过高或过低,影响治疗效果4.2 临床疗效评估4.2.1 评估患者的临床症状和体征改善情况4.2.2 根据治疗效果,调整用药方案4.2.3 及时停药或换药,避免药物滥用和耐药性产生5. 用药记录与报告5.1 用药记录5.1.1 记录患者的用药情况,包括药物名称、剂量、给药途径等5.1.2 记录患者的用药反应和副作用5.1.3 保持用药记录的完整性和准确性5.2 用药报告5.2.1 定期向上级医生汇报患者的用药情况5.2.2 反映患者的病情变化和治疗效果5.2.3 提出用药建议和调整方案注意事项:1. 在诊断和治疗计划制定阶段,要全面了解患者的病情,进行必要的检查,制定合理的治疗计划。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
抗菌药物临床应用管理系统操作手册(用户图解)
(第三版)
福州玖叁医药软件技术服务有限公司
http:\\ e_mail:
总工程师手机:魏峰松目录
第1章运行环境3
第2章合理用药指标5
第2.1节三级医院合理用药指标(部颁2011版)5
第2.2节抗菌药物品种用量DDDs排名(住院)6
第2.3节抗菌药物品种用量DDDs排名(门诊)6
第2.4节抗菌药物品种分类统计(住院)7
第2.5节抗菌药物品种分类统计(门诊)7
第2.6节抗菌药物DDDs科室排名(住院)8
第2.7节抗菌药物DDDs科室排名(门诊)8
第2.8节抗菌药物DDDs医生排名(住院)9
第2.9节抗菌药物DDDs医生排名(门诊)9
第2.10节抗菌药物用量DDDs/分类汇总(住院)10
第2.11节抗菌药物用量DDDs/分类汇总(门诊)10
第3章抗菌药物监测11
第3.1节抗菌药物库存供应监测11
第3.2节门诊抗菌药物处方监测11
第3.3节住院抗菌药物医嘱监测12
第3.4节住院病人联合用药监控12
第3.5节清洁手术预防用药监控13
第3.6节抗菌药物申请审批监控13
第3.7节抗菌药物申请使用说明14
第4章抗菌药物季报14
第4.1节医疗机构抗菌药物临床应用信息季报表(1)14 第4.2节医疗机构抗菌药物临床应用信息季报表(2)15 第5章抗菌药物自查15
第5.1节抗菌药物临床应用情况自查表115
第5.2节抗菌药物临床应用情况自查表216
第5.3节抗菌药物临床应用情况自查表316
第5.4节抗菌药物临床应用情况自查表417
第6章系统维护17
第6.1节系统运行参数设置17
第6.2节处方权调剂权管理18
第6.3节抗菌药物目录管理18
第6.4节国家基本药物目录字典19
第6.5节抗菌药物分类目录字典19
第6.6节抗菌药物DDD值目录字典20
第6.7节抗菌药物分级目录字典20
第6.8节手术预防用抗菌药物目录21
第6.9节质量问题分类字典维护21
第6.10节质控反馈信息字典维护22
第6.11节用户登陆口令修改22
第7章门诊医生工作站说明23
第8章住院医生工作站说明24
第1章运行环境
一、软件安装
服务器端:
本软件运行需要后台安装数据库和系统字典;数据库表结构建立脚本在:“表结构改变.txt”文件内,按照文件内数据在SQLPLUS下,复制粘帖该脚本即可看到执行结果,注意各角色连接需要的口令要与贵单位的口令一致。
系统字典的导入:请进入开发工具PB的“Database administrator”画板内打开各表,装入字典数据保存即可,相应的表和数据文本文件如下:ANTI_DRUG_LEVEL_LIST.TXT抗菌药物分级目录字典(国家)
ANTI_DRUG_CLASS_DICT.TXT抗菌药物分类目录字典(福建省)
ANTI_DRUG_DDD_LIST.TXT抗菌药物DDD值目录字典(国家)
NATI_ESSE_DRUG_LIST.TXT国家基本药物目录字典(国家)
OPER_PRUSE_ANTI_DURG_LIST.TXT手术预防用抗菌药物目录字典(国家)
QC_MSG_DICT.TXT质量问题分类字典(医院)
QA_EVENT_TYPE_DICT.TXT质控反馈信息字典(医院)
以上数据请计算机室专业技术人员(或数据库管理员)操作完成。
客户端:
只要将本软件复制到电脑任意目录内即可运行,运行环境需要的系统环境为:WINDOWS 2000或 WINDOWS XP ,需要PB9DLL动态连接库,需要ORACLE连接客户端软件支持。
一般用户电脑均已设置好动态库的默认目录和ORACLE客户端数据库连接培植。
二、软件授权
软件运行需要在“用户管理系统”内进行软件登记,登记程序名称为:“ANTIDRUG”,功能描述为:“抗菌药物临床应用管理系统”,系统授权大小分四级,说明如下:
1-查询报表(大等于1即可进行数据查询和统计)
2-质量控制(大等于2具备质量控制权限)
3-字典维护(大等于3可进行字典维护)
9-处方授权(权限等于9时可对医生或药师进行处方和分级授权)没有授权用户不能运行该程序。
三、软件设置
运行程序即进入系统登陆界面如下:
如输入的用户名和口令正确即进入系统,如系统数据库配置错误或口令错误即跳出数据库配置界面显示如下,你只要输入正确的数据库连接名称保存后再重新登陆即可进入。
更详细设置见:系统数据维护—>系统运行参数设置栏。
四、软件登陆
软件登陆成功即可看到如下图所示的五大菜单和35项功能。
第2章合理用药指标
第2.1节三级医院合理用药指标(部颁2011版)
合理用药统计指标以国家卫生部《三级综合医院医疗质量管理与控制指标》(2011年版)规定的“医疗机构合理用药指标”以及《抗菌药物临床应用专项整治活动评价表》内容(注*者)为准。
统计界面如下:(所有报表可以按某科室或某费别统计)
第2.2节抗菌药物品种用量DDDs排名(住院)
第2.3节抗菌药物品种用量DDDs排名(门诊)
第2.4节抗菌药物品种分类统计(住院)
第2.5节抗菌药物品种分类统计(门诊)
第2.7节抗菌药物DDDs科室排名(门诊)
第2.9节抗菌药物DDDs医生排名(门诊)
第2.10节抗菌药物用量DDDs/分类汇总(住院)
第2.11节抗菌药物用量DDDs/分类汇总(门诊)
第3章抗菌药物监测
第3.1节抗菌药物库存供应监测
第3.2节门诊抗菌药物处方监测
第3.3节住院抗菌药物医嘱监测
第3.4节住院病人联合用药监控+ 质控
第3.5节清洁手术预防用药监控
第3.6节抗菌药物申请审批监控
第3.7节抗菌药物申请使用说明
第4章抗菌药物季报
第4.1节医疗机构抗菌药物临床应用信息季报表(1)
第4.2节医疗机构抗菌药物临床应用信息季报表(2)
第5章抗菌药物自查
第5.1节抗菌药物临床应用情况自查表1
第5.3节抗菌药物临床应用情况自查表3
第6章系统维护
第6.1节系统运行参数设置
第6.2节处方权调剂权管理
第6.3节抗菌药物目录管理
第6.4节国家基本药物目录字典
第6.5节抗菌药物分类目录字典
第6.6节抗菌药物DDD值目录字典
第6.7节抗菌药物分级目录字典
第6.8节手术预防用抗菌药物目录
第6.9节质量问题分类字典维护
第6.10节质控反馈信息字典维护
第6.11节用户登陆口令修改
第7章门诊医生工作站说明
当输入药品处方时系统自动检查权限,权限不足和特殊使用级药品提示如下
没有处方权时的提示如下:
初级职称输入限制级药品时提示如下:
使用特殊使用级药品时提示如下:
第8章住院医生工作站说明
药品录入检索颜色提示:(特殊使用级红色,限制使用蓝色)
1,没有药品(处方)权限提示:
2,药品医嘱超越权限使用时提示:
3,医嘱录入界面提示说明:
越权医嘱:
新开越权医嘱在“注”栏显示“越”,医嘱保存后显示为:“申”,上级医生批准后显示为:“批”。
未批准越权医嘱护士不能转抄执行。
绿色通道:
将“医生说明栏”选择“先用后批”后则进入绿色通道,但仅限临时医嘱使用,改医嘱护士可以转抄执行,药房可以摆药,在上级医生审批栏也可看到,仍需要审批,24小时内没有审批或超过24小时审批,在抗菌药物监控软件均可质控。
特殊使用级药品越权使用须指定会诊专家:
选择:先用后批进入:绿色通道仅限:临时医嘱双击“注”栏填写
或查看申请表或
使说明表
“注”栏说明:
空白没有申请记录
“越”:为新开越权医嘱
“申”:为有申请单医嘱
“批”:为申请单已批准
特殊使用级的药品的“绿色通道”须会诊专家批准后,护士站才能执行,没有“绿色通道”的需会诊专家先批,本科领导再批准后才能到达护士站。
越权抗菌药物颜色提示为粉红色,审批完毕后颜色恢复正常。
查看或修改申请说明表:
如果直接填写“药品申请/说明表”或修改已经生成的“表格”请直接双际“注”
栏某行,则进入“药品申请/说明表”的编辑状态,可修改保存。
修改完毕请按“保存”按钮,可打印则,界面如下:
4,上级医生/会诊医生审批:
程序进入即提示否有待审批的越权医嘱:
进入审批界面如图示,未审批医嘱只能看到与自己权限相符合的医嘱,如果是本科全部批准可直接点击“全部批准”,如果只批准某条请选中,在右拦点击“会诊医师”则自动填写“会诊意见”:可以使用,并自动填写会诊日期;如果点击“科室领导”则自动填写“科室意见”:批准使用,并自动填写审批日期时间,点击“保存修改”,改条医嘱自动到“已审批”序列。
已经审批界面:点击自动填写”批准使用”及批准人和批
准时间
(科室意见可以修改)
点击会诊意见,自动填写”可以使用”及会诊
医师和会诊时间(会诊意见可以修改) 内容改变切记保存
各类手术预防使用抗菌药物目录提示:(所有抗菌药物目录)
(妇科手术可用抗菌药物目录)。