Cervical Screening Programme, England - 2012-13 Graphs
Incidence and mortality of cervical cancer in China2013

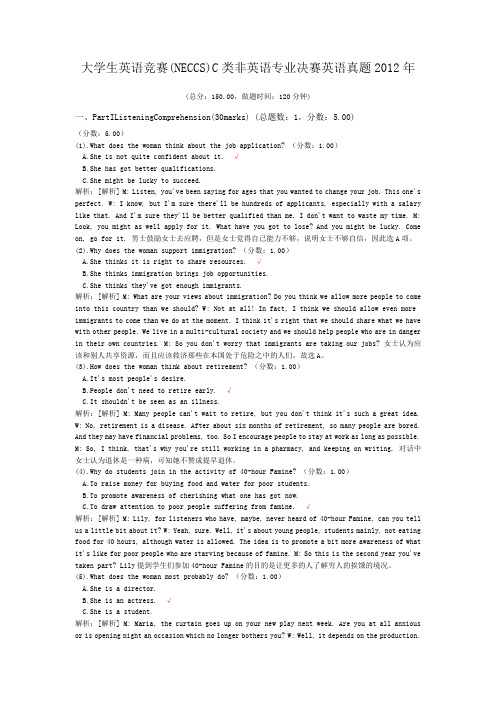
Incidence and mortality of cervical cancer in China, 2013Bingbing Song1,2*, Chao Ding3*, Wangyang Chen1,2, Huixin Sun1,2, Maoxiang Zhang1,2, Wanqing Chen31Tumor Prevention and Treatment Institute, Harbin Medical University, Harbin 150086, China; 2Heilongjiang Academy of Medical Sciences, Harbin 150086, China; 3National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100021, China*These authors contributed equally to this work.Correspondence to: Wanqing Chen, PhD. National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, No. 17 Panjiayuan South Lane, Chaoyang District, Beijing 100021, China. Email: chenwq@.AbstractObjective: Estimating the incidence and mortality rate of cervical cancer became necessary to establishprevention measures and healthy policies. The aim of this study was to estimate the updated incidence andmortality rate of cervical cancer in 2013 in China.Methods: According to the evaluation criteria developed by the National Central Cancer Registry of China, thedata submitted from 255 cancer registries met the required standards in 2013. Cervical cancer cases were retrievedfrom the national database and combined with the 2013 national population data. The age-standardized incidenceand mortality rates were based on the demographic structure of the national census 2000 and Segi’s worldpopulation.Results: In 2013, the estimated number of new cases and deaths from cervical cancer were 100,700 and 26,400,respectively. The crude incidence of cervical cancer was 15.17/100,000. The age-standardized incidence rates basedon the Chinese standard population (ASIRC) and the world standard population (ASIRW) were 11.30/100,000 and10.30/100,000, respectively. The incidence of cervical cancer in urban areas was 15.62/100,000 and the ASIRC was11.12/100,000. The incidence of cervical cancer in rural areas was 14.65/100,000 and the ASIRC was11.47/100,000. The mortality rate of cervical cancer was 3.98/100,000. The age-standardized mortality rates basedon the Chinese (ASMRC) and world standard populations (ASMRW) were 2.76/100,000 and 2.62/100,000,respectively. The mortality rate of cervical cancer in urban areas was 3.85/100,000 and in rural areas was4.14/100,000. Cervical cancer incidence and mortality increased with age. Urban areas had a higher incidence ofcervical cancer and lower mortality rates when compared with rural areas.Conclusions: Dynamic monitoring of cervical cancer incidence and mortality is the fundamental work ofcervical cancer prevention and control. Cervical cancer is a serious issue in women’s health, and preventionstrategies need to be enhanced, such as human papilloma virus (HPV) vaccination and screening programs.Keywords: Cervical cancer; cancer registration; epidemiologySubmitted Jul 24, 2017. Accepted for publication Aug 25, 2017.doi: 10.21147/j.issn.1000-9604.2017.06.01View this article at: https:///10.21147/j.issn.1000-9604.2017.06.01IntroductionOver the past 30 years, the increasing proportion of young women affected by cervical cancer has ranged from 10% to 40%. According to the World Health Organization and International Agency for Research on Cancer estimates (1),the year 2008 saw 529,000 new cases of cervical cancer globally. In developing countries, the number of new cases of cervical cancer was 452,000, and ranked second among malignancies in female patients. Conversely, the number of new cases of cervical cancer was 77,000 in developed countries, and ranked tenth among female malignancies.Original ArticlePer the Surveillance, Epidemiology, and End Results (SEER) data, the trend of both the incidence and mortality rate of cervical cancer showed a decline in the USA (2); however, the mortality rate showed an increasing trend in urban China (3). The highest incidence of cervical cancer was reported in Malawi and Zimbabwe, although the incidence is also high in parts of Central and South America. However, the incidence of cervical cancer was found to be lower in regions with a high human development index. The 5-year survival rate among women diagnosed with cervical cancer varies greatly from ≥70% in developed countries to <60% in low-income regions (4). Many factors such as social health inequities (5), place of residence, education (6), and human papilloma virus (HPV) vaccine coverage (7) have a strong impact on the incidence and survival rate of cervical cancer. Implementation of organized screening and prevention policies for cancer depends on high-quality cancer registry data. This study analyzed the incidence and mortality rate of cervical cancer based on the latest cancer registry data from whole country of China mainland in order to provide the updated epidemiological characteristic of cervical cancer for its prevention.Materials and methodsCancer registration in ChinaThe National Central Cancer Registry (NCCR), National Cancer Center is in charge of population-based cancer registry in China (8), collecting cancer registration data from local registries. In 2016, 347 registries submitted data to NCCR were distributed in 31 provinces, autonomous regions, municipalities, and groups of the Xinjiang Production and Construction Corps including 126 cities (urban areas) and 221 counties and county-level cities (rural areas). Finally, 255 cancer registries were qualified for analysis, including 88 urban cities and 167 rural counties. The 255 cancer registries covered a population of 226,494,490 (111,595,772 in urban and 114,898,718 in rural), including 114,860,339 men and 111,634,151 women, accounting for 16.65% of China population in the end of 2013.Evaluation of registration dataNCCR evaluated the registration data based on the Guidelines for Chinese Cancer Registration (2016) (9), quality control criteria for the Cancer Incidence in Five Continents Volume IX (10) from the International Agency for Research on Cancer/International Association of Cancer Registry (IARC/IACR) (11). These data were reviewed and checked using MS-FoxPro, MS-Excel, SAS and IARCcrg Tools (12). The comparability, validity and timeliness of data were evaluated by indicators, including of the percentage of cases with morphological verification (MV) (%), the percentage of death certificate only cases (DCO) (%), mortality-to-incidence ratio (M/I) and the percentage of the diagnosis of unknown basis (UB) (%). The M/I, MV%, DOC% and UB% were 0.27, 86.59%, 0.87% and 0.30, respectively, which was concluded by evaluating the quality of pooled data from all accepted registries. The quality of data from urban and rural is shown in Table 1.Statistical analysisThe incidence (mortality) rate, age-standardized incidence (mortality) rate, constituent ratio and cumulative rate of cervical cancer were calculated stratified by age, sex and area of residence. The standardized population used the sixth national census population in 2000 and Segi’s world population.ResultsIncidence of cervical cancerIn 2013, a total of 100,700 new cases of cervical cancer were estimated, accounting for 6.16% of malignancies in female patients. The crude incidence of cervical cancer was 15.17/100,000. The age-standardized incidence rates by Chinese standard population (ASIRC) and by world standard population (ASIRW) were 11.30/100,000 and 10.30/100,000, respectively, with a cumulative rate of 1.06% (0–74 years old). The crude incidence of cervical cancer, ASIRC and ASIRW were 15.62/100,000, 11.12/100,000, and 10.08/100,000 in urban areas, with a cumulative rate of 1.02% (0–74 years old), and 14.65/100,000, 11.47/100,000 and 10.54/100,000 in rural Table 1 Quality control indices of cervical cancer in China, 2013 Area M/I MV (%)DOC (%)UB (%) Overall0.2786.590.870.30 Urban areas0.2687.230.910.46 Rural areas0.2885.960.840.13M/I, mortality-to-incidence ratio; MV, cases identified via morphological verification; DOC, percentage of death certificate-only cases; UB, percentage of the diagnosis of unknown basis.472Song et al. 2013 cervical cancer burden in Chinaareas, with a cumulative rate of 1.11% (0–74 years old) (Table 2).Age-specific incidence of cervical cancerThe age-specific incidence of cervical cancer increased with age. The increase in incidence reached a peak (33.33/100,000) at age of 50, but decreased annually (11.86/100,000) at age ≥85 years. The incidence rates of cervical cancer were higher in urban areas than in rural areas among patients aged <50 years. The incidence rates of cervical cancer in urban areas were lower than that in rural areas among those aged≥50 years. The incidence of cervical cancer in urban and rural areas reached a peak at age≥45 years (34.24/100,000) and≥50 years (32.05/100,000), respectively (Figure 1).Mortality rate of cervical cancerIt was estimated that the number of deaths due to cervical cancer was 26,400 in 2013 and accounted for 3.21% of cancer-related deaths among female patients. The mortality rate of cervical cancer was 3.98/100,000. The age-standardized mortality rates by Chinese standard population (ASMRC) and by world standard population (ASMRW) were 2.76/100,000 and 2.62/100,000, respectively, with a cumulative rate of 0.29% (0–74 years old) in 2013. The crude mortality rate of cervical cancer, ASMRC and ASMRW were 3.85/100,000, 2.56/100,000, and 2.41/100,000 in urban areas, with a cumulative rate of 0.26% (0–74 years old), and 4.14/100,000, 2.99/100,000and 2.87/100,000 in rural areas, with a cumulative rate of 0.33% (0–74 years old) (Table 3).Age-specific mortality rate of cervical cancerThe age-specific mortality rate of cervical cancer was low over the ages of 0–29 years. After 30 years old, the mortality rate of cervical cancer increased gradually with age, and reached a peak at age ≥85 years (15.96/100,000). The age-specific mortality rates of cervical cancer in both urban and rural areas were not different at age ≥50 years. The age-specific mortality rate of cervical cancer in urban areas was higher than that in rural areas over the ages of ≥55 to ≥75 years. On the contrary, after age ≥80 years, this trend reversed (Figure 2).DiscussionAccording to previous studies, the trend of cervical cancer incidence remained consistent from 2003 to 2007. When compared with the year 2003, the crude incidences of cervical cancer in urban and rural areas increased by 70.03% and 51.00%, respectively (13). In the present study, the crude incidence of cervical cancer in China in 2013 was 15.17/100,000 and the ASIRC was 10.30/100,000, which was higher than that reported during 2003 to 2007. Moreover, the incidence rate increased by 52.29% when compared with 2009 (ASIRC: 7.42/100,000) (14). This could be explained by several reasons including aging of the national population, unhealthy lifestyles, and public healthTable 2 Incidence of cervical cancer in China, 2013Area New cases (×104)Crude rate (1/105)Ratio (%)ASIRC (1/105)ASIRW (1/105)Cumulative rate 0–74 (%)All areas10.0715.17 6.1611.3010.30 1.06Urban areas 5.5915.62 5.8411.1210.08 1.02Rural areas 4.4814.65 6.6211.4710.54 1.11 ASIRC, age-standardized incidence based on the Chinese standard population; ASIRW, age-standardized incidence based on world standard population.Table 3 Mortality rate of cervical cancer in China, 2013Area Death (×104)Crude rate (1/105)Ratio (%)ASMRC (1/105)ASMRW (1/105)Cumulative rate 0–74 (%)All areas 2.64 3.98 3.21 2.76 2.620.29Urban areas 1.38 3.85 3.10 2.56 2.410.26Rural areas 1.26 4.14 3.34 2.99 2.870.33 ASMRC, age-standardized mortality rate based on Chinese standard population; ASMRW, age-standardized mortality rate based on world standard population.Chinese Journal of Cancer Research, Vol 29, No 6 December 2017473programs (15). In addition, with the recent reform in China, national diversification of information, changes in ideas, and unsafe sexual behaviors may have led to an increase in HPV infection opportunities (16,17). Thus, the incidence of cervical cancer has been increasing annually.In order to prevent cervical cancer, the National Cervical Cancer Screening Program in Rural Areas launched by the government of China has been applied to women.Unfortunately, the large population coverage required and inequities of the technology yielded unsatisfactory benefits (18,19). Nonetheless, active prevention, early detection,and reasonable treatment are still important principles in cancer prevention and treatment (20).The mortality rate of cervical cancer in China increased annually from 2003 to 2007. The mortality rate of cervical cancer in urban and rural areas was increased by 32.43%and 3.01%, respectively, in 2007 when compared to 2003(13). The results of this study showed that the mortality rate of cervical cancer in the national cancer registration area in 2013 was 3.98/100,000, and the ASMRC was 2.76/100,000. This mortality rate in 2013 was higher than that in 2009 (mortality rate: 3.28/100,000; ASMRC:1.64/100,000) (14). Research shows that it is reasonable for a high incidence to be followed by high mortality rates:with the advances in diagnostic approaches and health awareness, new cases of cervical cancer are more frequently detected at the early stage (21,22).The incidence of cervical cancer in rural areas (3.98/100,000) was lower than that in urban areas (15.62/100,000); however, the mortality rate of cervical cancer in rural areas (4.14/100,000) was higher than that in urban areas (3.85/100,000). The high mortality rate of cervical cancer in rural areas may be related to the lack ofmedical resources, poor diagnosis and treatment conditions, low income, and treatment delays (22-24). In addition, the high incidence of cervical cancer in urban areas may be associated with the rapid economic development, being more receptive to new concepts, and changes in sexual behavior leading to increased opportunities for HPV infection.In our study, the incidence of cervical cancer peaked at group of age 45–54 years, and the mortality rate peaked at age ≥85 years. The incidence of HPV-positivity has steadily increased with age in China, peaking at 31–40 years (25).The period from HPV infection to carcinogenesis could contribute to the age at which incidence peaked. The relationship between HPV infection and cervical cancer has been identified by several laboratory and epidemiological investigations (26,27). HPV vaccination in high-income countries resulted in dramatic decreases in the incidence of HPV infection and associated cervical diseases (28). Our data could thus serve as guidelines to identify which patients as well as the proportion of those patients who would benefit from cervical cancer prevention and management efforts.ConclusionsChina is actively carrying out cervical cancer screening programs nationwide. However, the current incidence and mortality rates of cervical cancer continue to increase (29-31). Targeting the cause of cervical cancer could help prevent new cases (32,33). The cervical cancer prevention and control strategies should be tailored to the local conditions in the urban and rural areas. Efforts to promoteprimary prevention of cervical cancer have been carried outFigure 1Age-specific incidence of cervical cancer in China, 2013.Figure 2 Age-specific mortality of cervical cancer in China, 2013.474Song et al. 2013 cervical cancer burden in Chinain urban areas because of the high incidence of cervical cancer. The residents of urban areas may maintain a healthy lifestyle owing to the higher average education levels, and thus avoid risk factors of cervical cancer, thereby leading to a reduced incidence of cervical cancer. The high mortality rates of cervical cancer observed in rural areas require secondary and tertiary prevention programs, which involve early detection, early diagnosis, and early treatment, such as the National Cervical Cancer Screening Program in Rural Areas. Another approach is to effectively integrate urban and rural medical resources (34). These methods could improve the level of public health and enhance the diagnosis and treatment of cervical cancer in rural areas. Moreover, these efforts count as tertiary prevention, which can extend the life of patients with cervical cancer and reduce cervical cancer mortality.AcknowledgementsThis work was supported by CAMS Innovation Fund for Medical Sciences (CIFMS) (Grant No. 2016-12M-2-004)and Ministry of Science and Technology of China (Grant No. 2014FY121100).FootnoteConflicts of Interest : The authors have no conflicts of interest to declare.References Ferlay J, Shin HR, Bray F, et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 2010;127:2893-917.1.Lewis DR, Chen HS, Cockburn MG, et al. Early estimates of SEER cancer incidence, 2014. Cancer 2017;123:2524-34.2.Wang J, Bai Z, Wang Z, et al. Comparison of secular trends in cervical cancer mortality in China and the United States: an age-period-cohort analysis. Int J Environ Res Public Health 2016;13. pii: E1148.3.Ginsburg O, Bray F, Coleman MP, et al. The global burden of women’s cancers: a grand challenge in global health. Lancet 2017;389:847-60.4.Melan K, Janky E, Macni J, et al. Epidemiology and survival of cervical cancer in the French West-Indies:data from the Martinique Cancer Registry (2002-2011). Glob Health Action 2017;10:1337341.5.Vincerzevskiene I, Jasilionis D, Austys D, et cation predicts cervical cancer survival: a Lithuanian cohort study. Eur J Public Health 2017;27:421-4.6.Niccolai LM, Meek JI, Brackney M, et al. Declines in HPV-associated high-grade cervical lesions after introduction of HPV vaccines in Connecticut, US,2008-2015. Clin Infect Dis 2017.7.Chen W. Cancer statistics: updated cancer burden in China. Chin J Cancer Res 2015;27:1.8.Registry TNCC. Guideline for Chinese Cancer Registration. Beijing: Peking Union Medical College Press, 2004:48-50.9.Curado MP, Edwards B, Shin HR, et al. Cancer incidence in five continents, Volume IX. Lyon: IARC Scientific Publications, 2008.10.Bray F, Parkin DM. Evaluation of data quality in the cancer registry: principles and methods. Part I:comparability, validity and timeliness. Eur J Cancer 2009;45:747-55.11.Ferlay J, Burkhard C, Whelan S, et al. Check and conversion programs for cancer registries (IARC/IACR Tools for cancer Registries). IARC technical Report. Lyon: IARC, 2005.12.Li N, Zheng RS, Zhang SW, et al. An analysis of incidence and mortality of cervical cancer in China,2003-2007. Zhongguo Zhong Liu (in Chinese)2012;21:801-4.13.Ying Q, Xia QM, Zheng RS, et al. An analysis of incidence and mortality of cervical cancer in China,2009. Zhongguo Zhong Liu (in Chinese)2013;22:612-6.14.Bode AM, Dong Z, Wang H. Cancer prevention and control: alarming challenges in China. Natl Sci Rev 2016;3:117-27.15.Wu RF, Dai M, Qiao YL, et al. Human papillomavirus infection in women in Shenzhen City,People’s Republic of China, a population typical of recent Chinese urbanisation. Int J Cancer 2007;121:1306-11.16.Wagner M, Bennetts L, Patel H, et al. Global availability of data on HPV genotype-distribution in cervical, vulvar and vaginal disease and genotype-specific prevalence and incidence of HPV infection in females. Infect Agent Cancer 2015;10:13.17.Di JL, Rutherford S, Wu JL, et al. Knowledge of18.Chinese Journal of Cancer Research, Vol 29, No 6 December 2017475cervical cancer screening among health care workers providing services across different socio-economic regions of China. Asian Pac J Cancer Prev 2016;17:2965-72.Luo XM, Song L, Wu JL, et al. Analysis of the reported data of national rural cervical cancer screening project from 2012 to 2013, China.Zhonghua Yu Fang Yi Xue Za Zhi (in Chinese)2016;50:346-50.19.Practice Bulletin No. 168 Summary: Cervical Cancer Screening and Prevention. Obstet Gynecol 2016;128:923-5.20.Patra S, Upadhyay M, Chhabra P. Awareness of cervical cancer and willingness to participate in screening program: Public health policy implications.J Cancer Res Ther 2017;13:318-23.21.Koroukian SM, Bakaki PM, Htoo PT, et al. The Breast and Cervical Cancer Early Detection Program,Medicaid, and breast cancer outcomes among Ohio’s underserved women. Cancer 2017;123:3097-106.22.Kweon SS, Kim MG, Kang MR, et al. Difference of stage at cancer diagnosis by socioeconomic status for four target cancers of the National Cancer Screening Program in Korea: Results from the Gwangju and Jeonnam cancer registries. J Epidemiol 2017;27:299-304.23.Caldwell JT, Ford CL, Wallace SP, et al. Intersection of living in a rural versus urban area and race/ethnicity in explaining access to health care in the United States. Am J Public Health 2016;106:1463-9.24.Tang Y, Zheng L, Yang S, et al. Epidemiology and genotype distribution of human papillomavirus (HPV)25.in Southwest China: a cross-sectional five years study in non-vaccinated women. Virol J 2017;14:84.Park JY, Ngan HY, Park W, et al. Asian Society of Gynecologic Oncology International Workshop 2014.J Gynecol Oncol 2015;26:68-74.26.Walboomers JM, Jacobs MV, Manos MM, et al.Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol 1999;189:12-9.27.Aranda S, Berkley S, Cowal S, et al. Ending cervical cancer: A call to action. Int J Gynaecol Obstet 2017;138 Suppl 1:4-6.28.Chen W, Zheng R, Zeng H, et al. Annual report on status of cancer in China, 2011. Chin J Cancer Res 2015;27:2-12.29.Chen W, Zheng R, Zuo T, et al. National cancer incidence and mortality in China, 2012. Chin J Cancer Res 2016;28:1-11.30.Chen W, Zheng R, Zhang S, et al. Cancer incidence and mortality in China in 2013: an analysis based on urbanization level. Chin J Cancer Res 2017;29:1-10.31.Lea JS, Lin KY. Cervical cancer. Obstet Gynecol Clin North Am 2012;39:233-53.32.Haggar FA, Preen DB, Pereira G, et al. Cancer incidence and mortality trends in Australian adolescents and young adults, 1982-2007. BMC Cancer 2012;12:151.33.Woo RK, Skarsgard ED. Innovating for quality and value: Utilizing national quality improvement programs to identify opportunities for responsible surgical innovation. Semin Pediatr Surg 2015;24:138-40.34.Cite this article as: Song B, Ding C, Chen W, Sun H,Zhang M, Chen W. Incidence and mortality of cervical cancer in China, 2013. Chin J Cancer Res 2017;29(6):471-476. doi: 10.21147/j.issn.1000-9604.2017.06.01476Song et al. 2013 cervical cancer burden in China。
大学生英语竞赛(NECCS)C类非英语专业决赛英语真题2012年
大学生英语竞赛(NECCS)C类非英语专业决赛英语真题2012年(总分:150.00,做题时间:120分钟)一、PartIListeningComprehension(30marks) (总题数:1,分数:5.00)(分数:5.00)(1).What does the woman think about the job application? (分数:1.00)A.She is not quite confident about it. √B.She has got better qualifications.C.She might be lucky to succeed.解析:[解析] M: Listen, you've been saying for ages that you wanted to change your job. This one's perfect. W: I know, but I'm sure there'll be hundreds of applicants, especially with a salary like that. And I'm sure they'll be better qualified than me. I don't want to waste my time. M: Look, you might as well apply for it. What have you got to lose? And you might be lucky. Come on, go for it. 男士鼓励女士去应聘,但是女士觉得自己能力不够,说明女士不够自信,因此选A项。
(2).Why does the woman support immigration? (分数:1.00)A.She thinks it is right to share resources. √B.She thinks immigration brings job opportunities.C.She thinks they've got enough immigrants.解析:[解析] M: What are your views about immigration? Do you think we allow more people to come into this country than we should? W: Not at all! In fact, I think we should allow even more immigrants to come than we do at the moment. I think it's right that we should share what we have with other people. We live in a multi-cultural society and we should help people who are in danger in their own countries. M: So you don't worry that immigrants are taking our jobs? 女士认为应该和别人共享资源,而且应该救济那些在本国处于危险之中的人们,故选A。
XXX公卫考研真题-卫生综合1999-2013年(整理版)
XXX公卫考研真题-卫生综合1999-2013年(整理版)Anhui Medical University's 1999 XXX sciencesExam subject: Health ComprehensiveMajor: logy and Health Statistics。
XXX。
Maternal and Child Health and Family Planning。
n and Food XXXI。
n of XXX:1.Resident food structure2.Social norms of food hygiene3.Lead n4.Mercury toxicity tremors5.Geochemical diseases of logical origin6.XXX XXX7.Probability8.Confidence interval9.Life XXX10.n d11.Cohort12.Matching13.logy of nII。
Fill in the XXX:1.XXX _____.2.Pesticides that have been banned from n and use in China include _____.3.N-XXX。
of which _____ is the XXX.4.The public health issues related to melamine plastics are _____.5.XXX silicosis can be divided into _____.6.n XXX.7.The types of combined effects of environmental factors include _____.8.Meteorological factors。
including temperature。
2012年度职称英语“卫生类”新增阅读理解和完形填空全文翻译(3月3日)
2012年职称英语卫生类新增阅读理解第八篇 Eat Healthy"Clean your plate!" and "Be a member of the clean-plate -club!" Just about every kid in the US has heard this from a parent or grandparent. Often,it's accompanied by an appeal:" Just think about those starving orphans in Africa!" Sure, we should be grateful for every bite of food. Unfortunately, many people in the US take too many bites. Instead of staying "clean the plate", perhaps we should save some food for tomorrow.According to news reports, US restaurants are partly to blame for the growing bellies. A waiter puts a plate of food in front of each customer, with two to four times the amount recommended by the government, according to a USA Today story. Americans traditionally associate quantity with value and most restaurants try to give them that. They prefer to have customers complain about too much food rather than too little.Barbara Rolls, a nutrition professor at Pennsylvania State University, told USA Today that restaurant portion sizes began to grow in the 1970s, the same time that the American waistline began to expand.Health experts have tried to get many restaurants to serve smaller portions. Now, apparently,some customers are calling for this too. The restaurant industry trade magazine QSR reported last month that 57 percent of more than 4,000 people surveyed believe restaurants serve portions that are too large;23 percent had no opinion; 20 percent disagreed. But a closer look at the survey indicates that many Americans who can't afford fine dining still prefer large portions. Seventy percent of those earning at least $150,000 per year prefer smaller portions; but only 45 percent of those earning less than $25,000 want smaller.It's not that working class Americans don't want to eat healthy. It's just that,after long hours at low-paying jobs,getting less on their plate hardly seems like a good deal. They live from paycheck to paycheck ,happy to save a little money for next year's Christmas presents.词汇:orphan /''?:f?n] / n.孤儿belly /'beli/ n.肚子nutrition / nju:'tri??n / n.营养waistline / 'weistlain / n.腰围paycheck / 'pei't?ek / n.薪金支票注释:1. Be a member of the clean - plate club! 做清盘俱乐部的成员2. Just think about those starving orphans in Africa! 只要想想在非洲挨饿的孤儿们!3. take too many bites 吃得太多4. A Waiter puts a plate of food in front of each customer,with two to four times the amount recommended by the government, according to a USA Today story. 根据《今日美国》刊登的一个故事,服务员给每个顾客一盘饭菜,其量是政府推荐的2至4倍。
2012年6月研究生英语学位课统考(GET)真题试卷(题后含答案及解析)

2012年6月研究生英语学位课统考(GET)真题试卷(题后含答案及解析)题型有:1. LISTENING COMPREHENSION 2. VOCABULARY 3. CLOZE 4. READING COMPREHENSION 5. TRANSLATION 6. WRITINGLISTENING COMPREHENSIONSection A Directions: In this section, you will hear nine short conversations between two speakers. At the end of each conversation a question will be asked about what was said. The conversations and the questions will be read only once. Choose the best answer from the four choices given by marking the corresponding letter with a single bar across the square brackets on your machine-scoring Answer Sheet.听力原文:W: Larry, are you feeling OK? You’re so quiet at the party tonight.M: To be honest, whenever I go back to campus now, I feel really old—and all the students look so young! I feel out of place when I’m surrounded by students.Q: What does the man mean?1.A.He is pretty comfortable in this kind of setting.B.He is not at ease when seeing her.C.He is not used to the current surroundings.D.He rarely feels shy in unfamiliar places.正确答案:C解析:女士说:Larry,你没事吧?今晚的聚会上你那么安静。
首都医科大学附属北京妇产医院近40年宫颈癌发病特点及趋势分析

论著与临床研究首都医科大学附属北京妇产医院近40年宫颈癌发病特点及趋势分析苏丰丽,孔为民-作者单位:1_6北京,首都医科大学附属北京妇产医院妇瘤科作者简介:苏丰丽,首都医科大学硕士研究生在读,主治医师,主要研究方向为妇科肿瘤的基础与临床研究•通信作者,E-mail:****************.cn【摘要】目的探讨首都医科大学附属北京妇产医院近40年宫颈癌住院患者的发病特点及趋势的变化。
方法回顾性分析我院1979年1月至2018年12月期间收治的6 426例宫颈癌患者的病例资料,根据入院时间不同,划分为两组即1979 ~ 1998年组(前20年)和1999〜2018年组(后20年),统计分析两组不同年限的患者在发病年龄、肿瘤分期及病理类型方面的变化。
结果 1979〜1998年组纳入病例2 346例,1999 ~2018年组纳入病例4 〇8〇例。
19TO~ 1998年组宫颈癌发病年龄集中在55 ~64岁(占比42. 97%) ,1999 ~2018年组宫颈癌发病年龄集中在45 ~54岁(占比41. 08%)。
45 ~54岁的宫颈癌患者占比从20年前22. 04%升至41.08%,55 ~64岁组宫颈癌患者占比从2〇年前42.97%降至18. 21% , >65岁的老年人的宫颈癌占比由20年前的24•72%降至6.96%,差异均有统计学意义(^><0.05)。
在FIGO分期方面,早期宫颈癌(IA1-^A组期)占比由20年前的21. 82%升至52. 18% ,中晚期宫颈癌(IIB-IV期)占比由20年前的76. 94%降至41. 89%,差异有统计学意义(P <〇.〇5)。
在病理类型方面,均以鳞癌为主,但鱗癌由20年前的占比95. 01%降至80. 25%。
腺癌、特殊病理类型癌由20年前的占比3.37%、0. 68%升至17. 19%、1. 58%,差异均有统计学意义(P <0.05)。
Lee Hartwell 2012

JWS Grose Industrial Engine Reliability and Maintenance
• .
Fig. 19.4
19
Bartkova, J, etal Nature 434: 864 (2005)
Blood-Based Detection of Radiation Exposure in Humans Based on Novel Phospho-Smc1 ELISA Richard G. Ivey etal Radiation Research 175: 266 (2011)
Theory: Biomarkers for early detection of disease
Processes that monitor stress Assure accuracy to be identified
Are there checkpoints for:
4 Number of New Protein Analytes /yr
3
Traditional approaches have contributed all they can; we need new approaches / technologies.
2
1
0 1994
1996
1998
2000 Year
Jiao Tong 2012
Improving medicine with molecular diagnostics
Lee Hartwell
Better evidence for clinical intervention
• • • • • Identify those at risk for disease Identify those with early stage disease Identify effective treatment Know whether treatment was effective Detect early relapse
胆囊炎的诊治—老话题,新进展

胆囊炎的诊治—老话题,新进展胆囊炎的诊治——老话题,新进展流行病学胆囊结石全球患病率1丹麦6-13.1英国7.5-8.5法国13.9瑞典15挪威21.9意大利13.8罗马尼亚10.9西班牙9.7德国10.9-24.8中国6.3-12.1日本3.2印度6.1智利28.5秘鲁14.3巴西6.9苏丹5.2美国7.1-15在胆囊结石患者中,33%会出现急性胆囊炎发作2。
我国慢性胆囊炎、胆囊结石患病率为16.09%,占所有良性胆囊疾病的74.68%3。
胆囊结石是最常见的慢性胆囊炎危险因素,慢性结石性胆囊炎占所有慢性胆囊炎的90 %~95%3。
Datafrom:ThomsonReuters/globalepidemiologyinformation/ICD-9Code:574.2Calculusofgallbladderwithoutmentionofcholecystitis;gallstone(cholelithiasis)/referencesseeattachment AnnalsofEmergencyMedicine;V.28;No.3;9/96;p267中华消化杂志编辑委员会.中国慢性胆囊炎、胆囊结石内科诊疗共识意见(2014年,上海)胆囊炎的诊断慢性胆囊炎、胆囊结石3急性胆囊炎1-2症状发作性胆绞痛,与饮食有关,持续数小时后缓解消化不良并发症症状。
无症状胆囊结石。
阵发性右上腹或上腹部严重疼痛,至少持续15至30分钟,并放射至右侧背部或肩部,镇痛药可缓解体格检查右上腹压痛大多数患者可无任何阳性体征Murphy’s征右上腹包块、压痛、反跳痛或肌紧张辅助检查腹部超声是最常用、最有价值的检查CT有助于排除其他需要鉴别的疾病MRI主要用于鉴别急性和慢性胆囊炎MRCP可发现超声和CT不易检出的小结石肝胆管CCK-HIDA是评估胆囊排空的首选影像学检查首选腹部超声检查在临床强烈怀疑胆囊结石且腹部超声阴性的情况下,可实施超声内镜(或核磁共振)高度怀疑为急性胆囊炎的患者(发热、右上腹严重疼痛持续数小时以及右上腹压痛),可行CT检查JHepato l.2016Jul;65(1):146-81HepatobiliaryPancreatSci(2018)25:41–54JClinHepatol,Vol.31No.1.Jan.2015影像学诊断方法比较Meta分析提示,US对急性胆囊炎的诊断敏感性82%,特异性81%meta分析显示,对于慢性胆囊炎,腹部超声的敏感度为97%,特异度为95%,准确度为96%,阳性预测值为95%。