儿童贫血的治疗方法(英文版)
小儿贫血的护理措施

小儿贫血的护理措施引言小儿贫血是指血红蛋白水平低于正常范围的一种疾病,常见于儿童生长发育过程中。
贫血会导致儿童体内的氧供应不足,影响其生长与发育。
因此,对于患有小儿贫血的儿童,我们需要采取一系列的护理措施来改善他们的健康状况。
护理措施1. 了解病情首先,我们需要通过详细的病史询问和体检来了解患儿的病情。
同时,还要注意观察患儿的一些症状,如皮肤苍白、乏力、心悸等,以便及早发现并处理相关的问题。
2. 提供营养均衡的饮食饮食对于小儿贫血的治疗非常重要。
我们应该为患儿提供富含铁、叶酸和维生素B12的食物,如瘦肉、鸡蛋、红肉、豆类、动物肝脏等。
此外,还应避免患儿吃过多的含咖啡因的食物和饮料,因为咖啡因会影响铁的吸收。
3. 确保充足的睡眠睡眠是儿童健康发展的重要因素,对于患有贫血的儿童更为重要。
我们应该确保患儿有充足的睡眠时间,并保持规律的作息习惯。
此外,睡前可以进行一些放松的活动,如听音乐、阅读等,有助于改善患儿的睡眠质量。
4. 注重锻炼适度的锻炼可以增强儿童的体质,提高免疫力,改善贫血。
我们可以鼓励患儿多参加户外活动,如跑步、游泳、球类运动等。
同时,要注意适量,避免过度劳累。
5. 维持良好的卫生习惯良好的卫生习惯可以预防感染,减少疾病的发生。
我们应该教育患儿要常洗手,养成良好的饭前便后洗手习惯。
另外,还要注意饮食卫生,避免生食和不洁食物造成的感染。
6. 关注心理健康患有贫血的儿童可能会面临生长发育迟缓、体力不足等问题,对于他们的心理健康非常重要。
我们应该与他们建立良好的沟通,关心他们的情感需求,并给予积极的鼓励和支持。
此外,可以为患儿提供一些适合他们年龄的心理辅导,帮助他们更好地面对困难。
7. 定期随访和评估定期随访和评估是儿童贫血管理的重要环节。
我们应该根据医生的建议,定期带患儿进行血红蛋白水平和相关指标的检查,以便及时发现和处理问题。
结论小儿贫血是一种常见的儿童疾病,对儿童的发育有很大影响。
通过采取适当的护理措施,可以有效地改善患儿的贫血状况,提高他们的生活质量。
再生障碍性贫血文献英文版范文
再生障碍性贫血文献英文版范文Aplastic anemia is a blood disease that can be quite baffling for many. It's when your bone marrow doesn't produce enough new blood cells, leaving you feeling tired and weak. And, let's face it, nobody wants to feel that way.Imagine your body as a big factory, and your bone marrow is the part that makes all the new parts for your body. But with aplastic anemia, that factory isn't working properly. It's like the machines are broken or the raw materials aren't coming in. Your body starts to run out of the things it needs to keep going.Treatment for this can be a bit of a trial and error. Doctors might try different medicines to see what worksbest for you. It's kind of like playing a game of guesswork, but with your health at stake. Sometimes, it might take a while to find the right combo that helps.Living with aplastic anemia isn't easy. You have to beextra careful not to get sick or injured, because your body might not be able to heal as well as it used to. But it's not all doom and gloom. Many people with this condition are able to live normal lives, with the right support and care.In the end, it's important to remember that you're not alone in this. There are doctors, nurses, and other people who have been through this too, who are ready to help you get through it. And while it might be a tough journey, you can make it with the right attitude and support.。
贫血血常规报告英文版
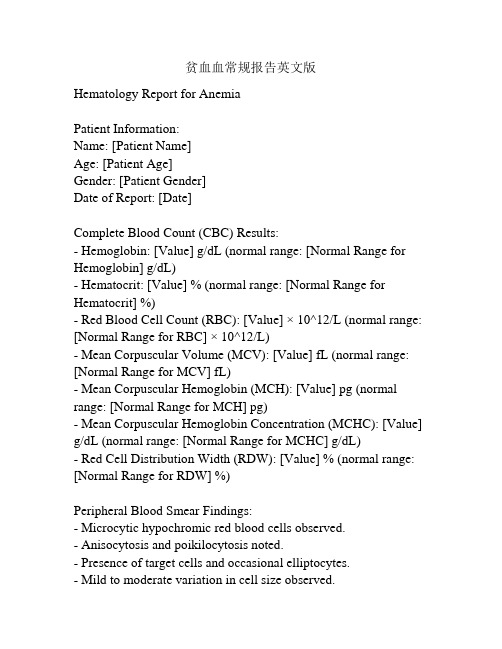
贫血血常规报告英文版Hematology Report for AnemiaPatient Information:Name: [Patient Name]Age: [Patient Age]Gender: [Patient Gender]Date of Report: [Date]Complete Blood Count (CBC) Results:- Hemoglobin: [Value] g/dL (normal range: [Normal Range for Hemoglobin] g/dL)- Hematocrit: [Value] % (normal range: [Normal Range for Hematocrit] %)- Red Blood Cell Count (RBC): [Value] × 10^12/L (normal range: [Normal Range for RBC] × 10^12/L)- Mean Corpuscular Volume (MCV): [Value] fL (normal range: [Normal Range for MCV] fL)- Mean Corpuscular Hemoglobin (MCH): [Value] pg (normal range: [Normal Range for MCH] pg)- Mean Corpuscular Hemoglobin Concentration (MCHC): [Value] g/dL (normal range: [Normal Range for MCHC] g/dL)- Red Cell Distribution Width (RDW): [Value] % (normal range: [Normal Range for RDW] %)Peripheral Blood Smear Findings:- Microcytic hypochromic red blood cells observed.- Anisocytosis and poikilocytosis noted.- Presence of target cells and occasional elliptocytes.- Mild to moderate variation in cell size observed.- Nucleated red blood cells not detected.Interpretation:The hematology report for the patient indicates the presence of microcytic hypochromic anemia. Low hemoglobin and hematocrit levels, as well as reduced red blood cell count (RBC), suggest a possible iron deficiency anemia.The mean corpuscular volume (MCV) is below the normal range, indicating smaller than normal red blood cells. Mean corpuscular hemoglobin (MCH) and mean corpuscular hemoglobin concentration (MCHC) are also reduced, further supporting the diagnosis of hypochromic anemia.The peripheral blood smear findings show microcytic cells with reduced color intensity (hypochromia). Additionally, anisocytosis (variation in cell size) and poikilocytosis (abnormal cell shapes) are present. The presence of target cells and occasional elliptocytes further supports the diagnosis of iron deficiency anemia.The absence of nucleated red blood cells suggests that the anemia is not due to increased destruction or ineffective production of red blood cells.Further investigation is needed to determine the underlying cause of the anemia, such as iron deficiency, chronic disease, or other nutritional deficiencies. Additional tests, medical history review, and possibly consultation with a hematologist or other specialists may be required for a comprehensive diagnosis and appropriate treatment.。
贫血--英文版
The aged patients or patients with vascular or cardiac diseases may not stand to milder anemia.
The level of anemia at which symptoms occur is highly variable among individuals as would be expected from the widely differing degrees of physical activity , physical conditioning , circulatory adequacy , and sensitivity or stoicism of the population.
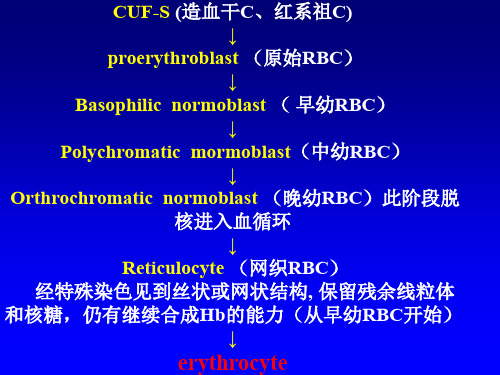
3 Production and maturation blockages of differentiating cells
DNA synthesis blockage : Vit B12, falic acid difficiencies, 嘌呤和嘧啶 metabolic defects→Megaloblastic anemia
★Classification
Morphologic classification
Type
MCV(um) MCH(PG) MCHC(%)
Diagnosis
Macrocytic >100
>32
Normocytic 80-100 26-32
Microcytic
<80
<26
32-35 Megaloblastic anemia
Classified accordind to the proliferative situations of BM
kdigo贫血指南

ESA初始治疗
纠正重度贫血(Hb<9g/dL)
强有力的证据(生活质量和输血) 安全性评估尚不充分
仅有一个临床试验(CESG, 1990)研究 CKD5D血透患者不同Hb目标值
严重贫血(Hb<9.5-11g/dL和>11g/dL)vs.安慰 剂
两组间生活质量无统计学差异
ESA初始治疗
肿瘤指南推荐合并活动性恶性肿瘤患者应 用ESA治疗时应提高警惕(尤其是可治愈的)
3.9.2 CKD非透析和CKD5PD患者,建议 皮下注射ESA。
3.10 建议根据CKD分期、治疗策略、有 效性、患者耐受性和喜好、ESA类型, 决定ESA治疗的频率。
ESA的用法
门诊和腹透患者:皮下注射 短效ESA:皮下注射优于静脉注射 长效ESA:皮下注射与静脉注射相当 CKD5HD患者一般更倾向于选择静脉注
副作用导致肿瘤的临床试验与TREAT的事 后分析一致
ESA的初始治疗时Hb>10g/dl,仍有部分患 者准备承担风险
有机会获得更好的生活质量vs.危害的风险
ESA的维持治疗
3.5 总体来说,成人CKD患者不建议应用ESAs 治疗维持Hb>11.5g/dl(115g/L)。
3.6 所有成人患者,不建议应用ESAs将Hb升 高至13.0g/dL(130g/L)。
ESA初始治疗
3.4.1 Hb≥10.0g/dL(≥100g/L)的成人非透 析患者,不建议开始ESA治疗。(2D)
3.4.2 Hb<10.0g/dL(<100g/L)的成人非透 析患者,建议需根据患者Hb下降程度、 需要输血的风险、ESA治疗的风险和贫血 导致的症状,决定是否开始ESA治疗。 (2C)
1999
2000
蛋白琥珀酸铁口服溶液
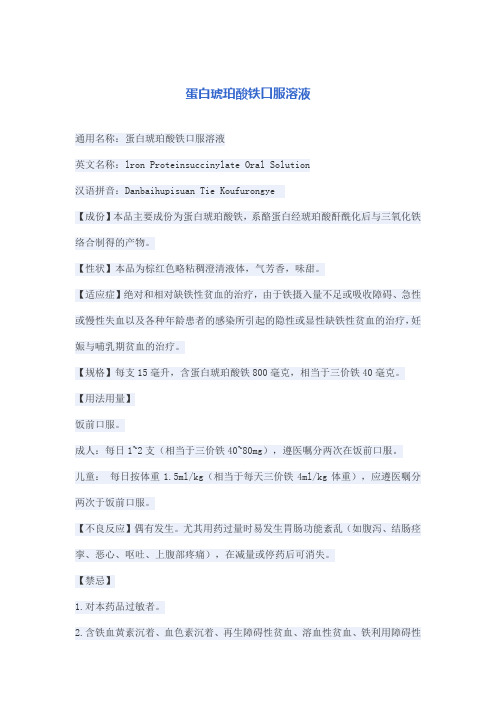
蛋白琥珀酸铁口服溶液通用名称:蛋白琥珀酸铁口服溶液英文名称:lron Proteinsuccinylate Oral Solution汉语拼音:Danbaihupisuan Tie Koufurongye【成份】本品主要成份为蛋白琥珀酸铁,系酪蛋白经琥珀酸酐酰化后与三氧化铁络合制得的产物。
【性状】本品为棕红色略粘稠澄清液体,气芳香,味甜。
【适应症】绝对和相对缺铁性贫血的治疗,由于铁摄入量不足或吸收障碍、急性或慢性失血以及各种年龄患者的感染所引起的隐性或显性缺铁性贫血的治疗,妊娠与哺乳期贫血的治疗。
【规格】每支15毫升,含蛋白琥珀酸铁800毫克,相当于三价铁40毫克。
【用法用量】饭前口服。
成人:每日1~2支(相当于三价铁40~80mg),遵医嘱分两次在饭前口服。
儿童:每日按体重1.5ml/kg(相当于每天三价铁4ml/kg体重),应遵医嘱分两次于饭前口服。
【不良反应】偶有发生。
尤其用药过量时易发生胃肠功能紊乱(如腹泻、结肠痉挛、恶心、呕吐、上腹部疼痛),在减量或停药后可消失。
【禁忌】1.对本药品过敏者。
2.含铁血黄素沉着、血色素沉着、再生障碍性贫血、溶血性贫血、铁利用障碍性贫血患者。
3.慢性胰腺炎合肝硬化患者。
【注意事项】1.在开始治疗前,应先找出产生贫血的原因。
2.本品尤其适用于妊娠与哺乳期妇女贫血的治疗。
3.本品不会影响病人的反应(驾驶及机器的操作)。
4.本品不会引起成瘾性,除了持续性出血、月经过多及怀孕外,不应服用本品超过六个月。
5.本品应放在孩子不能触及的地方。
【孕妇及哺乳期妇女用药】本品适用于妊娠与哺乳期妇女贫血的治疗。
【儿童用药】儿童每天按体重1.5ml/kg(相当于每天三价铁4ml/kg体重),应遵医嘱分两次于饭前口服。
【老年用药】未进行该项试验研究,且无可靠参考文献。
但预计不存在限制本品在老人使用的特殊问题。
【药物相互作用】铁衍生物可影响四环素类药品的吸收,应避免与其同时服用。
服用超过200mg维生素C可增加铁质的吸收,而跟制酸剂一起服用可降低铁质的吸收,氯霉素可延迟病人对本品的反应。
幼儿轻度贫血的指导及建议
幼儿轻度贫血的指导及建议
幼儿是成长发育阶段最重要的群体之一,而随着生活水平的提高
和快节奏的生活方式的出现,幼儿轻度贫血的情况也越来越普遍。
那么,面对幼儿轻度贫血,我们应该如何指导和建议呢?
首先,我们需要了解幼儿轻度贫血的症状。
幼儿轻度贫血的早期
症状多数比较难以察觉,但随着时间的推移,幼儿的视力、智力、免
疫力逐渐下降,容易产生疲劳、乏力、食欲不振等症状。
因此,家长
要密切观察幼儿的身体状况,及时发现问题。
接下来,针对幼儿轻度贫血,我们需要采取一些有效的建议和指导,以辅助幼儿摆脱轻度贫血的困扰。
1、增加幼儿的铁质摄入。
幼儿轻度贫血的主要原因之一就是缺乏
铁质,因此,家长应该注意给幼儿提供富含铁质的食品,如瘦肉、鸭肝、红枣等。
2、增加幼儿的维生素C摄入。
维生素C可以促进铁的吸收和利用,同时还可以保持身体的免疫力和抵抗力,因此,家长应该给幼儿多吃
新鲜的水果和蔬菜。
3、及时进行检查和治疗。
如果幼儿出现轻度贫血的症状,家长应
该及时带幼儿去医院进行检查和治疗,以排除其他疾病,并针对贫血
症状进行合理的治疗。
4、改善生活习惯。
家长应该帮助幼儿养成健康的生活习惯,如保
证充足的睡眠、合理的饮食、适度的运动等。
综上所述,幼儿轻度贫血并不可怕,只要家长能够及时发现问题,并采取相应的建议和指导,帮助幼儿增加铁质和维生素C的摄入,改
善生活习惯,那么幼儿的贫血症状就可以得到缓解,健康成长。
【疾病名】小儿α-地中海贫血【英文名】pediatricalphathalassaemia...
【疾病名】小儿α-地中海贫血【英文名】pediatric alpha thalassaemia【缩写】【别名】小儿α-地贫;小儿α-海洋性贫血;小儿α-珠蛋白生成障碍贫血;小儿α-库利氏贫血;小儿α-库利贫血Mediterranean anemia;小儿α-Mediterranean disease【ICD号】D56.0【概述】地中海贫血(alpha thalassaemia)(简称地贫)又称海洋性贫血(thalassemia),据全国医学名词审定委员会规定应称为“珠蛋白生成障碍贫血”。
是由于一种或多种珠蛋白肽链合成受阻或完全抑制,导致Hb成分组成异常,引起慢性溶血性贫血。
根据不同类型的珠蛋白基因缺失或缺陷,而引起相应的珠蛋链合成受抑制情况不同,可将地贫分为α-地中海贫血;β-地中海贫血,δ-地中海贫血、γ-地中海贫血及少见的β-地中海贫血;以前2种类型常见。
各类地中海贫血之间又可互相组合,可与各种异常Hb组合(如HbE/β地中海贫血),这一组疾病又称地中海贫血综合征。
均属常染色体不完全显性遗传。
α-地中海贫血(α-mediterranean anemia)是由于α-珠蛋白基因的缺失或功能缺陷(点突变)而导致α-珠蛋白链合成障碍所引起的一组溶血性贫血。
【流行病学】从地中海沿岸的意大利、希腊、马耳他、塞浦路斯到东南亚各国均是本病多发区。
在我国的广东、广西、海南、云南、贵州、四川及香港等地区常见,发病率达10%~14%,黄河以南至长江流域,台湾、福建及西藏等省(区)均有病例报道。
患者以汉族为多,亦可见于回、傣、壮、苗和布依等少数民族。
【病因】属常染色体不完全显性遗传。
α-珠蛋白基因位于16号染色体短臂(16P13.33~p13.11~pter),总长约29kb,包含7个连锁的α类基因或假基因。
1.α-基因缺失 每条染色体上各有一对控制合成α-链的α-基因,因此每个细胞内有4个α-基因,可发生不同程度(1~4个)基因异常:(1)α-地贫(α地贫):若其中一条染色体上缺失一个α-基因组,则受控的α-链的合成部分受抑制,称为α-地贫(α地贫)。
24章抗贫血药PPT优秀课件
• 思考题
• 1、铁剂、VB12、叶酸的适应症分别是什么? 铁剂应用时要注意哪些问题?
25
缺乏,可影响维生素B12吸收,而引起“恶性贫血”。
19
临床应用
主要用于恶性贫血及其他巨幼红细胞性 贫血,也可用于神经系统疾病(如神经炎、 神经萎缩、神经痛等) 、肝病、再生障碍 性贫血等 的辅助治疗。
不良反应 偶见过敏反应,严重者可致过敏性休克, 故不可滥用。
20
四、造血细胞生长因子
• 造血细胞生长因子是调节骨髓造血前体细胞 增生和分化的糖蛋白激素。现用于临床的造 血细胞生长因子有红细胞生成素、粒细胞集 落刺激因子、白介素Ⅱ等。
入胃内以结合残存的铁 。
10
• 同类药物 • 多糖铁复合物 商品名为力蜚能,作为
铁元素补充剂,可迅速提高血铁水平与 升高血红蛋白。本品吸收极佳,与硫酸 亚铁一样易被人体吸收。本品为有机铁 化合物,不含游离铁离子如Fe2+或 Fe3+,安全性高,不会导致游离铁离子 所引起的便秘、腹泻和恶心等消化道不 良反应。
胃癌)、慢性腹泻等胃肠道疾病 (3)慢性失血
如:消化性溃疡、月经过多、痔出血等 (4)红细胞大量破坏 如:疟疾、溶血 8
铁剂治疗缺铁性贫血,口服铁剂1 周即可使血液中网织红细胞增加, 10~14d达高峰,2~4周,血红蛋白明 显增加,但要使血红蛋白达到正常值, 常需1~3个月。为使体内铁贮存恢复正 常,待血红蛋白正常后尚需减半量继续 服药2~3月。
5
药理作用
铁是构成血红蛋白、肌红蛋白和金属 黄素蛋白酶等的重要原料。铁吸收到骨髓 后,进入骨髓幼红细胞,在线粒体内与原 卟啉结合形成血红素,再与珠蛋白结合成 为血红蛋白,进而发育为成熟的红细胞。 铁缺乏,血红蛋白合成减少,血液携氧能 力降低,引起全身组织器官的缺氧性损害 ,产生贫血的症状和体征,儿童严重缺铁 时会影响行为和学习能力。
儿童贫血(全英文)
2、extramedullary:when requirement of haemopoiesis increase,liver、spleen、 lymphadenectasis,hepatomegaly and splenomegaly, in circulating blood immature erythrocytes and granulocytes .
5、myelohaematopoiesis:
6mons Haematogenesis function emphasis, make various kinds of blood cells,unique hematogenic organ after birth.
Haematopoiesis postnatal
The criteria of anemia
Age
< 28 days 1~4 months 4~6 months 6 months~6 years 6~14 years
Hb concentration
blood characteristics – ages
red blood cells(RBC) and Hb Physiological haemolysis and anemia write blood cells(WBC) and classification 4-6 cross Platelets 150-250×109/L blood volume 8-10%
Red blood cell (RBC)
The wide range of hemoglobin concentration is accounted for by: Variation in how rapidly the umbilical cord is clamped. An infant’s position after delivery. If cord clamping is delayed and the baby is held lower than placenta, both hemoglobin and blood volume are increased by a placental transfusion.
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Evaluation
Hb electrophoresis Osmotic fragility, Morphology
Enzyme deficiencies
PK/G6PD screen, reduction of methemoglobin
Autoimmune
Coombs test
Microangiopathic PNH
Who has anemia?
•①. 1d, 130 g/L; •②. 1y, 130 g/L; •③. 2m, 95 g/L; •④. 2y, 95 g/L.
How to work up an anemic patient ?
• History: age, duration, diet, complaint • PE: pale, jaundice, hepatomegaly, thrill • CBC:
Normal children
The change of RBC and Hb
(180) 6 (150) 5 (120) 4 (90) 3 (60) 2 (30) 1
Hb RBC
birth 10d 2~3m
12y (age)
The Diagnostic Criteria
Age
Hb (g/L)
At birth
Posteriority
microangiopathic DIC/TTP/HUS mechanical heart valve
snake venoms
Differentiation of Hemolytic anemia
Diagnosis
Hemoglobinopathy Membrane disorder
Aplastic anemia
Vit B 12
Tumor infiltration
Folic acid
MDS
Differentiation of microcytic anemia
IDA
Sideroblastic Thalassemias Anemia
Chronic disease
serum iron
145
1-4 m
90
4-6 m
100
6 m -6 y
110
6-14 y
120
Who has anemia?
•①. 1d, 130 g/L√; •②. 1y, 130 g/L; •③. 2m, 95 g/L; •④. 2y, 95 g/L√.
2nd step:
Reticulocyte production index=?
1yr old boy:
Hb 7.8 g/dL;
Reticulocyte count 4.2%;
MCV 60.4fl, MCH 24.6 pg/L, MCHC 30.5%.
RPI ???
• RPI=[Ret (%)×(Patient Hb) / (Normal Hb)]
=4.2×7.8/15 = 2.2
ABO, Rh
transfusion
non-immune hemolysis
congenital
membrane defects (Hereditary spherocytosis)
Unstable hemoglobins (Thalassemias)
Enzyme deficiencies (G-6-PD)
3rd step: Size of RBC ?
• Iro • Lead poison • Sideroblastic
Anemia
• Chronic infections
Bone marrow disorder: Megaloblastic anemia:
Approach to Childhood Anemia
Important to Remember on Anemia
• Anemia is a clinical sign of disease. • It is not a single disease by itself. • Need to look for the underlying cause ! • Will we ignore a fever with out investigation? • Drug Administration depends on the cause.
• idiopathic pulmonary hemosiderosis
Hiatus hernia & Meckel diverticulum
Approach to anemia
N,
serum ferritin
N,
Hb electrophoresis
N
HbF/HbA2
N
N
4th step: immune-related ?
RPI>2
hemolysis
Coombs (+)
Coombs (-)
immune
non-immune
Primary
AIHA
Secondary
allogenic
Morphology, History,BUN/Cr Ham test, flow cytometry
Last but not least-Hemorrhage
• Peptic ulcer • Hiatus hernia • Meckel diverticulum • Parasitic infection • Pulmonary hemorrhage
1st step: Anemia?
Measurement Normal
RBC count 5 million/mm3
Hemoglobin (Hb) 15 g/dL
Hematocrit (Hct)
45%
Range
4.0 ~ 5.7 12 ~17 38 ~ 50
A x 3 = B x 3 = C - This is the rule of thumb
• Hb, Hct, RBC • MCV, MCH, MCHC • Ret & RPI (Reticulocyte production index):
RPI=Ret(%)×(Patient Hb)/(Normal Hb)
• Peripheral smear examination
Reticulocyte production index