2009-EASL-Management of cholestatic liver diseases
梗阻性黄疸围手术期护肝治疗

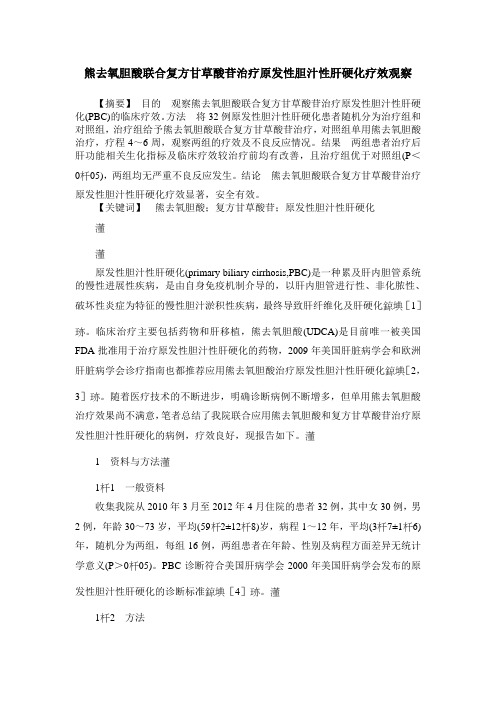
胆汁淤积诊断步骤
病史、体检
肝功能试验 ALP和GGT↑ B超、CT
胆管扩张
肝外胆汁淤积 手术、 内镜、 经皮介入 梗阻
胆管不扩张
肝内胆汁淤积 AMA/ANA
CT/ERCP/MRCP 无梗阻 肝活检
EASL Clinical Practice Guidelines: Management of cholestatic liver diseases, J Hepatol 2009;51:237-267 陆伦根,曾民德。胆汁淤积性肝病。人民卫生出版社 2008年
梗阻性黄疸的治疗
解除梗阻、迅速退黄、快速恢复肝功能
在减黄手术后和胆道引流围手术期解除梗阻的同时合 并使用保肝药物是必须的, ●有利于患者恢复肝功能 ●减少并发症的发生 ●对恶性梗阻性黄疸,有利于提高患者生存质量
及早解除梗阻是 基本治疗措施
非手术或手术治疗
维生素K吸收障碍
补充维生素K 保肝
合理选用药物治疗
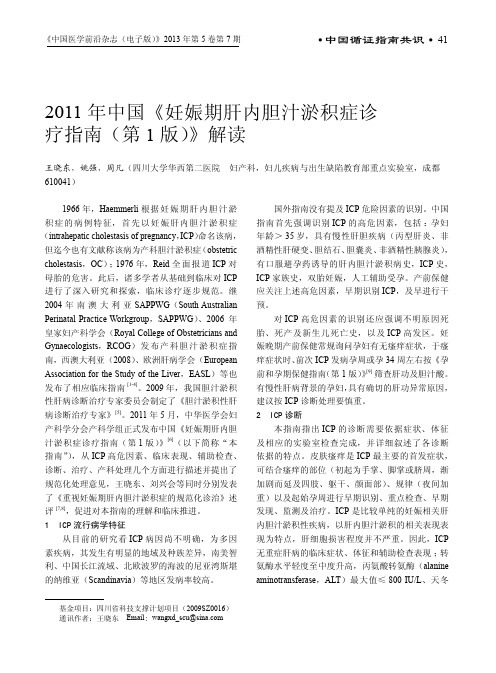
Prevalence according to etiology(%)
Prevalence according to diagnosis(%)
32%
8% 15% Cirrhosis PBC PSC CPH CAH
26%
26% Viral Alcoholic Drug related Autoimmune Cryptogenic
犬梗阻性胆管损伤
梗阻后炎症因子明显升高
犬梗阻性胆管损伤后肝脏功能和胆管局部病理学改变的研究
胆汁淤积的临床和生化表现
胆汁成分淤积表现
肝外表现
碱性磷酸酶升高 谷氨酰转肽酶升高 高胆红素血症 高结合胆红素血症 高胆固醇血症及黄色瘤形成 血清胆汁酸盐升高
安瓶幻灯

iStelle-术后极速修复系列
安
瓶
美国·艾思黛尔
目录
1. 美国iStelle(艾思黛尔)公司介绍
2. 中国总代理—万润时代公司介绍 3. 安瓶主要成分--干细胞信息素的来源及作用机理 4. 微脂囊包裹技术 5. 安瓶的主要成分、适用范围及使用方法。 6. 五年大样本临床观察及效果对比图。 7. iStelle(艾思黛尔)安瓶与竞品的比较 8. iStelle(艾思黛尔)系列介绍 9. 各类证书 10.小结
常见问题解答
iStelle(艾思黛尔)安瓶容量怎么才1.7ml,量太少了吧?
答: iStelle(艾思黛尔)安瓶的核心成份为高浓度的细胞信息素及玻尿酸,
具备高活性,同时应用了最先进的微脂囊技术,具有很强的透皮吸收功效, 使用1—2瓶完全可使术后肌肤得到很好的修复,如需要抑制瘢痕形成。需要 使用3个月左右。
术后第一天
40岁
女性
当日同时操作:水光针、5D
童颜术、自体血清填充三项. 术后第一天
美国·艾思黛尔
安瓶--同时做微整形三项效果
术后第三天
女士,40岁 同时操作:水光针、5D童颜术、 自体血清填充三项; 术后第三天。 术后7天淡妆出镜,接受采访
美国·艾思黛尔
安瓶—对儿童皮肤挫伤的修复对比
小朋友, 4岁,意外摔伤, 使用iStelle安瓶,每6小时涂 抹创面一次 48h完全结痂, 第5天结痂脱落,皮肤基本恢复 第6天皮肤完全恢复,没有一点
疤克:只能使用在完全愈合的伤口上,起到淡化疤痕的作用; 愈肤宁:主要为几聚糖(Chitosan),为含氨多糖,干燥后可形 成透明保护薄膜。 金扶宁 :主要成分重组人粒细胞巨噬细胞刺激因子,主要为消炎的功效,没有促 进伤口愈合及细胞再生的作用;
熊去氧胆酸联合复方甘草酸苷治疗原发性胆汁性肝硬化疗效观察
熊去氧胆酸联合复方甘草酸苷治疗原发性胆汁性肝硬化疗效观察【摘要】目的观察熊去氧胆酸联合复方甘草酸苷治疗原发性胆汁性肝硬化(PBC)的临床疗效。
方法将32例原发性胆汁性肝硬化患者随机分为治疗组和对照组,治疗组给予熊去氧胆酸联合复方甘草酸苷治疗,对照组单用熊去氧胆酸治疗,疗程4~6周,观察两组的疗效及不良反应情况。
结果两组患者治疗后肝功能相关生化指标及临床疗效较治疗前均有改善,且治疗组优于对照组(P<005),两组均无严重不良反应发生。
结论熊去氧胆酸联合复方甘草酸苷治疗原发性胆汁性肝硬化疗效显著,安全有效。
【关键词】熊去氧胆酸;复方甘草酸苷;原发性胆汁性肝硬化原发性胆汁性肝硬化(primary biliary cirrhosis,PBC)是一种累及肝内胆管系统的慢性进展性疾病,是由自身免疫机制介导的,以肝内胆管进行性、非化脓性、破坏性炎症为特征的慢性胆汁淤积性疾病,最终导致肝纤维化及肝硬化[1]。
临床治疗主要包括药物和肝移植,熊去氧胆酸(UDCA)是目前唯一被美国FDA批准用于治疗原发性胆汁性肝硬化的药物,2009年美国肝脏病学会和欧洲肝脏病学会诊疗指南也都推荐应用熊去氧胆酸治疗原发性胆汁性肝硬化[2,3]。
随着医疗技术的不断进步,明确诊断病例不断增多,但单用熊去氧胆酸治疗效果尚不满意,笔者总结了我院联合应用熊去氧胆酸和复方甘草酸苷治疗原发性胆汁性肝硬化的病例,疗效良好,现报告如下。
1资料与方法11一般资料收集我院从2010年3月至2012年4月住院的患者32例,其中女30例,男2例,年龄30~73岁,平均(592±128)岁,病程1~12年,平均(37±16)年,随机分为两组,每组16例,两组患者在年龄、性别及病程方面差异无统计学意义(P>005)。
PBC诊断符合美国肝病学会2000年美国肝病学会发布的原发性胆汁性肝硬化的诊断标准[4]。
12方法对照组给予UDCA(优思弗,德国福克大药厂)口服250 mg/次,3次/d。
2009年诺贝尔生理学医学奖

伊丽莎白-布莱克本和杰克-绍斯塔克 发现端粒的一种独特DNA序列能保护 染色体免于退化。卡罗尔-格雷德和 伊丽莎白-布莱克本确定了端粒酶, 端粒酶是形成端粒DNA的成分。这些 发现解释了染色体的末端是如何受到 端粒的保护的,而且端粒是由端粒酶 形成的。 如果端粒缩短了,细胞就会老化。
相反,如果端粒酶的活动显著,端粒 的长度也就能得以保持,并且细胞衰 老也将延后。癌细胞就是一个例子, 癌细胞被认为是具有永久生命力的。 相反,某些特定的遗传疾病,会出现 一些有缺陷的端粒酶这样的特征,导 致损害细胞。对此诺贝尔奖颁给这一 细胞基本机制的发现,这一发现有助 于新的治疗措施的发展。
端粒酶简介 1、概念: 端粒酶是一种 RNA与蛋白的复 合体,它以自 身RNA上的一个 片段为模板通 过逆转录合成 端粒重复序列, 并通过一
种RNA依赖性聚合酶(如逆转录酶)机制加 到染色体3’末端以延伸端粒。 2、组成:RNA(作为模板) 蛋白质(反转录酶) 3、作用机制: 在端粒DNA的复制时,端粒酶既有模板, 又有逆转录酶这两方面的作用。其与端粒3´ 端结合后,以其RNA为模板,经反转录延长 端粒,从而保护DNA双链末段免遭降解及相 互融合。
2009年诺贝尔生理学
或医学奖-授予解开 DNA谜团的研究
2009年10月5日诺贝尔瑞典卡罗林斯卡医学 院宣布,将2009年诺贝尔生理学或医学奖 授予美国加利福尼亚旧金山大学的伊丽莎 白·布莱克本(Elizabeth Blackburn)、美 国巴尔的摩约翰·霍普金医学院的卡罗尔格雷德(Carol Greider)、美国哈佛医学院 的杰克·绍斯塔克(Jack Szostak)以及霍 华德休斯医学研究所,以表彰他们发现了 端粒和端粒酶保护染色体的机理。
伊丽莎白·布莱克本因学术成就卓著曾 被美《时代》周刊评为年度全球最具影 响力的100个人物之一。布莱克本曾在 美国耶鲁大学任博士后研究员,并曾任 教于美国加利福尼亚大学伯克利分校, 自1990年开始担任美国加利福尼亚大学 旧金山分校生物学和生理学教授。
自身免疫性肝炎-原发性胆汁性胆管炎重叠综合征合并胃腺癌1例报告

/01 DOI:10.3969/j.issn.1001-5256.2023.05.022自身免疫性肝炎-原发性胆汁性胆管炎重叠综合征合并胃腺癌1例报告李力晨,汤绍辉暨南大学附属第一医院消化内科,广州510630通信作者:汤绍辉,tangshaohui206@163.com(ORCID:0000-0002-7217-1840)关键词:肝炎,自身免疫性;原发性胆汁性胆管炎;胃肿瘤;诊断基金项目:中央高校基本科研业务费专项资金(21622315)Autoimmunehepatitis-primarybiliarycholangitisoverlapsyndromewithgastricadenocarcinoma:AcasereportLILichen,TANGShaohui.(DepartmentofGastroenterology,TheFirstAffiliatedHospitalofJinanUniversity,Guangzhou510630,China)Correspondingauthor:TANGShaohui,tangshaohui206@163.com(ORCID:0000-0002-7217-1840)Keywords:Hepatitis,Autoimmune;PrimaryBiliaryCholangitis;StomachNeoplasms;DiagnosisResearchfunding:TheFundamentalResearchFundsfortheCentralUniversities(21622315)1 病例资料患者女性,72岁,因“反复腹痛1个月余”于2022年4月4日入本院。
2022年3月25日患者因鱼刺卡喉至当地医院就诊,行胃镜检查发现:胃角溃疡;食管静脉曲张(中度)。
胃镜下活检考虑早期癌,腹部CT考虑肝硬化可能。
患者为进一步诊治转入本院。
既往有中药服用史半年余,无烟酒嗜好,否认接触毒物、工业化学物品等。
2011 年中国《妊娠期肝内胆汁淤积症诊疗指南(第1 版)》解读
《中国医学前沿杂志(电子版)》2013年第5卷第7期41● 中国循证指南共识 ●2011年中国《妊娠期肝内胆汁淤积症诊疗指南(第1版)》解读王晓东,姚强,周凡(四川大学华西第二医院 妇产科,妇儿疾病与出生缺陷教育部重点实验室,成都 610041)基金项目:四川省科技支撑计划项目(2009SZ0016)通讯作者:王晓东 Email : wangxd_scu@1966年,Haemmerli 根据妊娠期肝内胆汁淤积症的病例特征,首先以妊娠肝内胆汁淤积症(intrahepatic cholestasis of pregnancy ,ICP )命名该病,但迄今也有文献称该病为产科胆汁淤积症(obstetric cholestasis ,OC );1976年,Reid 全面报道ICP 对母胎的危害。
此后,诸多学者从基础到临床对ICP 进行了深入研究和探索,临床诊疗逐步规范。
继2004年南澳大利亚SAPPWG (South Australian Perinatal Practice Workgroup ,SAPPWG )、2006年皇家妇产科学会(Royal College of Obstetricians and Gynaecologists ,RCOG )发布产科胆汁淤积症指南,西澳大利亚(2008)、欧洲肝病学会(European Association for the Study of the Liver ,EASL )等也发布了相应临床指南[1-4]。
2009年,我国胆汁淤积性肝病诊断治疗专家委员会制定了《胆汁淤积性肝病诊断治疗专家》[5]。
2011年5月,中华医学会妇产科学分会产科学组正式发布中国《妊娠期肝内胆汁淤积症诊疗指南(第1版)》[6](以下简称“本指南”),从ICP 高危因素、临床表现、辅助检查、诊断、治疗、产科处理几个方面进行描述并提出了规范化处理意见,王晓东、刘兴会等同时分别发表了《重视妊娠期肝内胆汁淤积症的规范化诊治》述评[7,8],促进对本指南的理解和临床推进。
Catalysis Letters 2009,131,1-2, 250-257
Propane Oxidative Dehydrogenation Over Ln–Mg–Al–O Catalysts (Ln 5Ce,Sm,Dy,Yb)Gheorghit ¸a Mitran ÆAdriana Urda ÆNathalie Tanchoux ÆFranc ¸ois Fajula ÆIoan-Cezar MarcuReceived:10March 2009/Accepted:4June 2009/Published online:23June 2009ÓSpringer Science+Business Media,LLC 2009Abstract Ln–Mg–Al mixed oxide catalysts (Ln =Ce,Sm,Dy,Yb)were prepared from layered double hydroxide precursors,characterized using XRD,N 2adsorption,TG-DTG,EDX,H 2-TPR and CO 2-TPD techniques and tested in the oxidative dehydrogenation of propane in the temperature range 450–600°C.For all the catalysts the conversion increases with increasing the reaction temper-ature while the propene selectivity decreases to the benefit of carbon oxides for Ce-based system and of cracking products for the others.The best yields in propene were obtained with Dy-and Sm–Mg–Al–O catalysts.No corre-lation between the reducibility of the rare-earth cation and the catalytic performances was observed.A linear corre-lation between the catalyst basicity and the propene selectivity was evidenced.Keywords Oxidative dehydrogenation ÁPropane ÁRare-earth oxides ÁLayered double hydroxides1IntroductionThe oxidative dehydrogenation of propane to propene is one of the potentially important catalytic processes for theeffective utilization of light alkanes and has been thor-oughly studied in recent times [1–14],propene being an important raw material for the production of polypropyl-ene,acrylonitrile,acrolein and acrylic acid.In spite of this high number of studies there is no up to now a sufficiently active and selective catalyst for the oxidative dehydroge-nation of propane to propene that could be used at indus-trial scale.Thus,the development of a catalyst with a sufficiently high activity and selectivity is highly desirable.Heterogeneous catalysts for this reaction typically con-tain vanadium and molybdenum as the critical elements [1–9].Among other oxide systems,those containing rare-earth oxides are also reported as active and selective [14–16].It has been shown that c -Al 2O 3-supported rare-earth oxides (Y,Dy,Tb,Yb,Ce,Tm,Ho and Pr)are reactive in propane oxidative dehydrogenation,but propene selectivi-ties were relatively low,namely under 40%[14].Taking into consideration the electron-donating character of the olefinic species,it was of interest to investigate whether the propene selectivity could be enhanced by increasing the catalyst basicity.For this reason we prepared Mg–Al mixed oxide-supported rare-earth oxides from layered double hydroxide (LDH)precursors and we studied their catalytic properties in the oxidative dehydrogenation of propane.The obtained results are presented in this paper.2Experimental 2.1Catalysts PreparationLn–Mg–Al–O (Ln =Ce,Sm,Dy,Yb)samples were pre-pared by coprecipitation of mixed metal nitrate solutions with an aqueous solution of NaOH (2M)at a constant pH of 10.Thus,an aqueous solution of Mg(NO 3)2Á6H 2O andG.Mitran ÁA.Urda ÁI.-C.Marcu (&)Department of Chemical Technology and Catalysis,Faculty of Chemistry,University of Bucharest,4-12,Blv.Regina Elisabeta,030018Bucharest,Romaniae-mail:marcu.ioan@unibuc.ro;ioancezar_marcu@ N.Tanchoux ÁF.FajulaInstitut Charles Gerhardt,UMR 5253CNRS/ENSCM/UM2/UM1,Mate´riaux Avance ´s pour la Catalyse et la Sante ´(MACS),Ecole Nationale Supe´rieure de Chimie,8,rue de l’Ecole Normale,34296Montpellier Cedex 5,FranceCatal Lett (2009)131:250–257DOI 10.1007/s10562-009-0057-1Al(NO3)3Á9H2O was contacted with the basic solution by dropwise addition of both solutions into a well-stirred beaker containing200cm3of rare-earth Ln nitrate solution at room temperature.Ln content,as atomic percent with respect to the cationic species,was equal to5and the Mg/Al atomic ratio was kept at3for all preparations.The addition of the alkaline solution and pH were controlled by pH-STAT Titrino(Metrohm).The precipitates formed were aged in their mother liquor overnight at80°C under stirring,separated by centrifugation,washed with deion-ized water until a pH of7and dried at80°C overnight. Dried samples were calcined in air at750°C during8h in order to form the corresponding mixed metal oxides which were used as catalysts.2.2Catalysts CharacterizationPowder X-Ray diffraction(XRD)spectra were obtained using a Siemens D5000Diffractometer and monochromatic Cu-K a radiation.They were recorded with0.02°(2h)steps over the3°–70°/angular range with1s counting time per step.The chemical composition of the samples was deter-mined by EDX microprobe on a Cambridge Stereoscan260 apparatus.The textural characterization was achieved using con-ventional nitrogen adsorption/desorption method,with a Micromeritics ASAP2010automatic analyzer.Prior to nitrogen adsorption,the samples were outgassed for8h at 523K.The thermal analysis(TG and DTG)was carried out using a Netzsch TG209device,in the following condi-tions:linear heating rate10°C min-1from room temper-ature to900°C,dynamic air atmosphere,Al2O3crucible, sample weight approximately20mg.Temperature-programmed desorption(TPD)of CO2was carried out using a Micromeritics Autochem model2910 instrument.Fresh calcined samples(100mg)were pre-treated in air at550°C before adsorption of the probe mol-ecule at100°C.During desorption,the sample was heated in a heliumflow(30mL min-1)at a ramp of10°C min-1.The amount of the probe molecule desorbed from the sample was estimated from the area under the peak after taking the thermal conductivity detector response into consideration.Hydrogen temperature-programmed reduction(H2-TPR) studies were carried out using a Micromeritics Autochem model2910instrument.Fresh calcined samples(100mg), placed in a U-shaped quartz reactor,were pretreated in air at 750°C before reduction.After cooling down to room tem-perature and introducing the reduction gas of3%H2/Ar,the sample was heated at a rate of10°C min-1from room temperature to800°C.The hydrogen consumption was estimated from the area under the peak after taking the thermal conductivity detector response into consideration. Calibration of TCD signal has been done with an Ag2O standard(Merck,reagent grade).Characterization of the samples has been performed before and,for some of them,after the catalytic test.2.3Catalytic TestingThe catalytic oxidative dehydrogenation of propane was carried out in afixed bed quartz tube down-flow reactor operated at atmospheric pressure.The internal diameter of the reactor tube was15mm.The catalyst was supported by quartz wool.The axial temperature profile was measured using an electronic thermometer placed in a thermowell centered in the catalyst bed.Quartz chips were used tofill the dead volumes before and after the catalyst bed to minimize potential gas-phase reactions at higher reaction temperatures.The gas mixture consisting of propane and air was fed into the reactor at a volume hourly space velocity(VHSV)in the range of3,000–12,000h-1.The reaction temperature was varied between450and600°C, the propane-to-oxygen molar ratio,between1and4,and the catalyst bed volume was always kept to1cm3.In a typical reaction run,the reactor was heated to the desired temperature in theflow of reactants.The system was allowed to stabilize for about1h at the reaction tempera-ture before thefirst product analysis was made.Each run was carried out over a period of2–3h.The reaction products were analyzed in a Clarus500Gas-Chromato-graph equipped with a thermal conductivity detector(TCD) using an alumina column and aflame ionization detector (FID)using a CTR I column.Propene,CO,CO2and cracking products(methane and ethylene)were the major products formed under the reac-tion conditions.Conversion of propane and product selec-tivities were expressed as mol%on a carbon atom basis. The carbon balance was in all runs higher than95%.3Results and Discussion3.1Catalysts CharacterizationThe XRD patterns of the prepared precursors andfinal cat-alysts are displayed in Figs.1and2,respectively.Poorly crystallized layered hydrotalcite-type structures(JCPDS 37-0630),as generally observed for multicationic LDH, were detected on all dried precipitated samples labeled LnMgAl-LDH.The interlayer distance003equal to ca.8A˚, was consistent with the presence of nitrates as interlayered [17].Some of the samples,as Ce-,Sm-and DyMgAl-LDH, displayed lines corresponding to poorly crystallized CeO2 (JCPDS75-0076)Sm(OH)3(JCPDS83-2036)and Dy2O3Propane Oxidative Dehydrogenation Over Ln–Mg–Al–O Catalysts251(JCPDS22-0612),respectively.On the other hand,samples calcined at750°C exhibited,in all cases,lines correspond-ing to the MgAlO mixed oxide phase with the periclase-like structure(JCPDS-ICDD4-0829)and lines corresponding to CeO2(JCPDS75-0076),Sm2O3(JCPDS15-0813),Dy2O3 (JCPDS22-0612)and Yb2O3(JCPDS41-1106)phases for Ce-,Sm-,Dy-and Yb–Mg–Al–O mixed oxides,respec-tively.We note that XRD patterns of the samples after the catalytic test remained practically unchanged.The chemical compositions of the samples reported in Table1show that the rare-earth content was slightly higher than the nominal value and the Mg/Al atomic ratio varied between2.9for Ce–Mg–Al–O and3.9for Yb–Mg–Al–O.The specific surface areas of the catalysts were high,in the range102–160m2g-1.They are also reported in Table1. All the catalysts displayed type IV nitrogen adsorption/ desorption isotherms,according to IUPAC classification, with a hysteresis loop characteristic of mesoporous materials [18]with a broad distribution of sizes.After the catalytic test, the specific surface areas of the catalysts remained practi-cally the same.The TG-DTG curves of YbMgAl-LDH precursor and of the corresponding oxide,Yb–Mg–Al–O,are presented in Fig.3.Thefirst weight loss in the TG-DTG curves of the HDL precursor(Fig.3a)is due to the elimination of loosely bound water and interlayer water molecules.The second weight loss is ascribed to the removal of hydroxyl groups in the metal hydroxide layers.The sample exhibited a net weight loss of43%up to900°C,with the second weight loss being larger than thefirst one.This is in accord with literature data for hydrotalcite-like materials[19–21]. In the case of the calcined oxide,the TG curve decreased continuously up to500°C but the DTG profile presented two well-defined signals at90and185°C and a broad signal in the range250–500°C(Fig.3b).The total weight loss for the calcined sample was smaller,namely15%.This may be due to the adsorption of water and carbon dioxide from the environmental air at the oxide surface and sug-gests that the catalyst must be activated in the reactor before the catalytic test at temperatures higher than500°C for cleaning its surface.The basicity of the catalysts was determined by tem-perature-programmed desorption of CO2(CO2-TPD),the profiles obtained being shown in Fig.4.These profiles were deconvoluted in three CO2desorption peaks,having the maximum in the range of175–185,225–250and300–340°C demonstrating that they have basic sites of different strengths:weak,moderate and strong.The total basicity was calculated according to the desorbed amount of CO2252G.Mitran et al.and summarized in Table1.The total basicity followed the order:Dy[Sm[Yb[Ce.TPR experiments have been carried out over all the mixed oxide samples prepared in order to study the redox properties of the catalysts.The TPR patterns of the catalysts are presented in Fig.5.All the samples displayed at high temperatures a large not well-defined pattern which was decomposed in two reduction peaks.These peaks must correspond to the reduction of the tetravalent cation(Ce) according to the equation:Ce4??Ce3?,and to the reduction of trivalent Ln3?cations according to the equa-tion:Ln3??Ln2?.The low-temperature peak could be attributed to the reduction of the rare-earth cationic species from the rare-earth oxide clusters,and the high-temperature peak,attributed to the reduction of rare-earth cationic species in the large crystalline rare-earth oxide particles. We note that for Sm–Mg–Al–O sample a well-defined low intensity peak was also observed before the large pattern.ItTable1Physico-chemical characteristics of the catalystsCatalyst SSA a(m2g-1)Chemical composition(%at.)by EDX bLn/(Ln?Mg?Al)atomic ratioMg/Al atomicratioTotal basicity(mmol CO2/g)Total H2consumption(mol H2/mol Ln)Ln Mg AlCe–Mg–Al–O157 1.721.17.2 5.6 2.9 1.630.13 Sm–Mg–Al–O160 1.826.07.1 5.2 3.6 2.180.12 Dy–Mg–Al–O102 1.521.37.0 5.1 3.1 2.520.18 Yb–Mg–Al–O142 1.925.3 6.5 5.6 3.9 1.960.19a Specific surface areab Oxygen in balancePropane Oxidative Dehydrogenation Over Ln–Mg–Al–O Catalysts253could be due to the reduction of the easily reducible samarium species from highly dispersed samarium oxide.These results suggest a non-uniform dispersion of the rare-earth oxide in the Mg–Al mixed oxide matrix.Assuming the reduction according to the equations above,0.5moles of H 2per mol of Ln would be necessary.The data from Table 1show that much lower quantities of H 2were experimentally consumed indicating that only a partial reduction of rare-earth cations occurred.3.2Catalytic Oxidative DehydrogenationFirstly blank tests have been done without a catalyst,the catalyst bed being replaced with quartz.Figure 6a shows that the non-catalytic oxidative conversion of propane is not significant in our testing conditions,at least at tem-peratures below 600°C,confirming that the contribution of the homogeneous reaction was negligible.The conversion of propane and the product selectivities as a function of reaction temperature for the reaction with propane–air mixtures at a total VHSV of 9,000h -1and a propane-to-oxygen molar ratio equal to 2,over the tested catalysts are depicted in Fig.6.For all the catalysts the conversion increased with increasing the reaction tempera-ture while the propene selectivity decreased to the benefit of CO x for Ce-based system and of cracking products for the other systems.We note that the Yb-based system wasnot254G.Mitran et al.active at temperatures lower than500°C.For the reaction at 500°C the catalytic activity followed the order:Dy[ Sm C Ce[Yb.The differences in conversions indicate the influence of the metallic properties on the rate-determining hydrogen abstraction by the catalysts[14].In the case of Ce–Mg–Al–O system,the sum of the selectivities of CO x and CH4was not equal to that of ethylene,as was the case with the other systems,but much higher within all the range of temperatures studied.This suggests that for Ce-based system,total oxidation products(CO x)were formed not only from C1species resulting from the cracking of propane,but also by the direct oxidation of propane or by further oxidation of propene.This was not the case for Sm-,Dy and Yb–Mg–Al–O catalysts.The apparent activation energies(E act)corresponding to the propane transformation on the different catalysts have been calculated(Table2)from the Arrhenius plots pre-sented in Fig.7.The activation energies increased fol-lowing the order Dy\Sm B Ce\Yb,in line with the observed variation of the catalytic activity.On the other hand,the values obtained for the activation energies fall within the usual range measured for propane oxidative dehydrogenation over oxide-based catalysts[22,23].The effect of the conversion on the selectivities has been studied for the reactions over all Ln–Mg–Al–O catalysts at 550°C and a propane-to-oxygen molar ratio equal to2,by varying the VHSV in the range3,000–12,000h-1(Fig.8).Table2Apparent activation energies corresponding to the propane transformation on the Ln–Mg–Al–O catalystsCatalyst E act(kcal mol-1)Ce–Mg–Al–O23.7Sm–Mg–Al–O23.2Dy–Mg–Al–O19.0Yb–Mg–Al–O27.3Propane Oxidative Dehydrogenation Over Ln–Mg–Al–O Catalysts255As expected,the selectivity to propene decreased in all cases with increasing conversion.The extrapolation to zero conversion results,for the reaction over Ce-based system, in non-zero selectivity for carbon oxides and cracking products indicating that they are also primary products formed simultaneously with propene.For the reaction over other Ln-based systems studied,the extrapolation to zero conversion results in zero carbon oxides selectivity and non-zero selectivity for cracking products showing that only the latter are also primary products,carbon oxides being not in this case.These results confirm that,among the catalysts studied,the parallel reaction of propane leading to carbon oxides is specific only for Ce-based system.On the other hand,the conversion-selectivity curves clearly showed that the oxidative dehydrogenation selec-tivity followed the order:Dy[Sm[Yb[Ce.The changes in the selectivities on the studied catalysts indicate the effect of Ln properties on the selectivity.The effect of the propane-to-air molar ratio on the oxi-dative dehydrogenation of propane over Dy-based catalyst is presented in Fig.9.The propane conversion strongly decreased when the propane-to-oxygen molar ratio increased from1to4.At the same time the selectivity to propene increased at the expense of cracking products and carbon oxides.These results could be explained by the decrease of the available oxygen related to the increase in the propane-to-oxygen ratio.Moreover,the observed decrease of the selectivity for cracking products can be explained taking into consideration that when the propane-to-oxygen molar ratio was increased keeping the total VHSV constant, the partial pressure of propane in the reaction mixture increased,cracking being thus disadvantaged.A linear correlation between the catalyst CO2-TPD basicity and the propene selectivity was observed as shown in Fig.10both for the reaction at500and550°C.The direct relationship found between surface basicity and propene selectivity can be accounted for by the electron-donating character of the olefinic species and the conse-quent easier desorption from a more basic surface,thus preventing further overoxidation into carbon oxides. Interestingly,the most selective catalysts proved the most active as well(Fig.6).We note that the Mg–Al mixed oxide-supported rare-earth oxides studied in this work exhibit better performance in terms of selectivity to propene than the c-Al2O3-sup-ported rare-earth oxides in Ref.[14],confirming the expected effect of magnesium.Finally,we note that no correlation between the H2-TPR reducibility of the rare-earth cation and the catalytic per-formances was observed,suggesting that the surface-adsorbed oxygen but not lattice oxygen species are involved in the reaction.A similar result was obtained by Al-Zahrani et al.[14]for c-Al2O3-supported rare-earth oxide catalysts by estimating the lattice oxygen reactivity from the reduction potential of the cation.256G.Mitran et al.4ConclusionsThe properties of basic Ln–Mg–Al mixed oxides catalysts for the ODH of propane have been investigated in the temperature range450–600°C.For all the catalysts the conversion increased with increasing the reaction temper-ature while the propene selectivity decreased.The best yields in propene were obtained with Dy-and Sm–Mg–Al–O systems,Dy-based catalyst being the most selective one. Increasing the propane-to-oxygen molar ratio from1to4 for Dy-based catalyst,the propane conversion decreased from8to2%but the propene selectivity increased from55 to75%at the expense of cracking products and carbon oxides.A linear correlation between the catalyst basicity and the propene selectivity was observed.On the other hand,no correlation between the H2-TPR reducibility of the rare-earth cation and the catalytic performances was observed.Acknowledgment This research was supported by the Romanian National University Research Council(CNCSIS)under the project ‘‘IDEI’’No.1906/2009.References1.D’Ippolito SA,Ban˜ares MA,Garcia Fierro JL,Pieck CL(2008)Catal Lett122:2522.Karakoulia SA,Triantafyllidis KS,Lemonidou AA(2008)MicroMeso Mater110:1573.Sugiyama S,Osaka T,Hirata Y,Sotowa KI(2006)Appl Catal A312:524.Dz´wigaj S,Gressel I,Grzybowska B,Samson K(2006)CatalToday114:2375.Koc SN,Gurdag G,Geissler S,Guraya M,Orbay M,Muhler M(2005)J Mol Catal A225:1976.Heracleous E,Machli M,Lemonidou AA,Vasalos IA(2005)JMol Catal A232:297.Ban˜ares MA,Khatib SJ(2004)Catal Today96:2518.Davies T,Taylor SH(2004)J Mol Catal A220:779.Zhaorigetu B,Li W,Xu H,Kieffer R(2004)Catal Lett94:12510.Wu Y,He Y,Chen T,Weng W,Wan H(2006)Appl Surf Sci252:522011.He Y,Wu Y,Chen T,Weng W,Wan H(2006)Catal Commun7:26812.Trionfetti C,Babich IV,Seshan K,Lefferts L(2006)Appl CatalA310:10513.Jibril BY(2005)Ind Eng Chem Res44:70214.Al-Zahrani SM,Jibril BY,Abasaeed AE(2003)Catal Lett85:5715.Buyevskaya OV,Wolf D,Baerns M(2000)Catal Today62:9116.Zhang W,Zhou X,Tang D,Wan H,Tsai K(1994)Catal Lett23:10317.Rives V,Ulibarri MA(1999)Coord Chem Rev181:6118.IUPAC Reporting physisorption data for gas/solid system(1985)Pure Appl Chem57:60319.Das J,Das D,Parida KM(2006)J Coll Int Sci301:56920.Tichit D,Das N,Coq B,Durand R(2002)Chem Mater14:153021.Parida KM,Das J(2000)J Mol Catal A Chem151:18522.Mattos ARJM,da Silva San Gil RA,Rocco MLM,Eon J-G(2002)J Mol Catal A178:22923.Male JL,Niessen HG,Bell AT,Tilley TD(2000)J Catal194:431Propane Oxidative Dehydrogenation Over Ln–Mg–Al–O Catalysts257。
2009诺贝尔生理及医学奖
生老病死,这或许是人类生命最为简洁的概括,但其中却蕴藏了无数的奥秘。获得2009年诺贝尔生理学或医学奖的三位美国科学家,凭借“发现端粒和端粒酶是如何保护染色体的”这一成果,揭开了人类衰老和罹患癌症等严重疾病的奥秘。 在生物的细胞核中,有一种易被碱性染料染色的线状物质,它们被称为“染色体”。正常人的体细胞有23对染色体,它们对人类生命具有重要意义,例如众所周知,决定男女性别的就是一对染色体。在染色体的末端部分有一个像帽子一样的特殊结构,这就是端粒。而端粒酶的作用则是帮助合成端粒,使得端粒的长度等结构得以稳定。 “染色体携有遗传信息。端粒是细胞内染色体末端的‘保护帽’,它能够保护染色体,而端粒酶在端粒受损时能够恢复其长度。”获奖者之一的伊丽莎白·布莱克本介绍说:“伴随着人的成长,端粒逐渐受到‘磨损’。于是我们会问,这是否很重要?而我们逐渐发现,这对人类而言确实很重要。” 卡罗林斯卡医学院发布的新闻公报说,这三位科学家的发现“解释了端粒如何保护染色体的末端以及端粒酶如何合成端粒”。借助他们的开创性工作,人们知道,端粒不仅与染,端粒变短,细胞就老化。相反,如果端粒酶活性很高,端粒的长度就能得到保持,细胞的老化就被延缓。 不过需要指出的是,近年来陆续有研究发现,端粒和染色体等虽然与细胞老化有关,进而影响衰老,但并非唯一的因素,“生命衰老是一个非常复杂的进程,它有许多不同的影响因素,端粒仅仅是其中之一”。 “这是有关人类衰老、癌症和干细胞等研究的谜题拼图中重要的一片,”新闻公报说,“他们的发现使我们对细胞的理解增加了新的维度,清楚地显示了疾病的机理,并将促使我们开发出潜在的新疗法。”
PBC临床对症治疗及“亚临床”PBC的研究进展
㊃综述㊃d o i:10.3969/j.i s s n.1671-8348.2021.22.033网络首发h t t p s://k n s.c n k i.n e t/k c m s/d e t a i l/50.1097.R.20210924.0542.002.h t m l(2021-09-24)P B C临床对症治疗及 亚临床 P B C的研究进展*程苕莼1,李民2,李晗1,刘一村1综述,卞兆连2ә审校(1.南通大学医学院,江苏南通226001;2.南通大学附属南通第三医院消化内科,江苏南通226001)[摘要]原发性胆汁性胆管炎(P B C)是一种以肝内小胆管非化脓性炎症为特征的器官特异性自身免疫性疾病㊂早期干预治疗对P B C患者的预后及生活质量提升都有极为重要的作用,但由于疾病本身临床表现的非典型性及各种肝内㊁肝外常见并发疾病的干扰,如何对P B C患者进行早期诊断仍是目前临床上亟待解决的问题㊂该文结合最新研究进展,对经典P B C的临床表现及对症处理进行归纳和总结,重点讨论了如何对 亚临床 P B C患者诊断处理,以期为该疾病的早期鉴别与治疗提供依据㊂[关键词]原发性胆汁性胆管炎;临床表现;对症治疗[中图法分类号] R320[文献标识码] A[文章编号]1671-8348(2021)22-3927-04C l i n i c a l s y m p t o m a t i c t r e a t m e n t o f p r i m a r y b i l i a r y c h o l a n g i t i s a n dr e s e a r c h p r o g r e s s o f"s u b c l i n i c a l"P B C*C H E N G S h a o c h u n1,L I M i n2,L I H a n1,L I U Y i c u n1,B I A N Z h a o l i a n2ә(1.M e d i c a l C o l l e g e,N a n t o n g U n i v e r s i t y,N a n t o n g,J i a n g s u226001,C h i n a;2.D e p a r t m e n t o f G a s t r o e n t e r o l o g y,A f f i l i a t e d N a n t o n g T h i r d H o s p i t a l o f N a n t o n gU n i v e r s i t y,N a n t o n g,J i a n g s u226001,C h i n a)[A b s t r a c t] P r i m a r y b i l i a r y c h o l a n g i t i s(P B C)i s a n o r g a n-s p e c i f i c a u t o i mm u n e d i s e a s e c h a r a c t e r i z e d b y n o n-s u p p u r a t i v e i n f l a mm a t i o n o f t h e s m a l l b i l e d u c t s i n t h e l i v e r.E a r l y i n t e r v e n t i o n t h e r a p y i s o f g r e a t i m p o r-t a n c e t o t h e p r o g n o s i s a n d q u a l i t y o f l i f e i n t h e P B C p a t i e n t s.H o w e v e r,d u e t o t h e a t y p i c a l c l i n i c a l m a n i f e s t a-t i o n s o f t h e d i s e a s e i t s e l f a n d t h e i n t e r f e r e n c e o f v a r i o u s c o mm o n i n t r a h e p a t i c a n d e x t r a h e p a t i c c o m p l i c a t i o n s, h o w t o m a k e e a r l y d i a g n o s i s o f P B C p a t i e n t s i s s t i l l a n u r g e n t c l i n i c a l p r o b l e m t o b e s o l v e d.T h i s r e v i e w c o m-b i n e s t h e l a t e s t r e s e a r c h p r o g r e s s t o s u mm a r i z e t h e c l i n i c a l m a n i f e s t a t i o n s a n d s y m p t o m a t i c t r e a t m e n t o f c l a s-s i c P B C,f o c u s i n g o n h o w t o d i a g n o s e a n d t r e a t t h e p a t i e n t s w i t h"s u b c l i n i c a l"P B C,h o p i n g t o p r o v i d e a b a s i s f o r t h e e a r l y i d e n t i f i c a t i o n a n d t r e a t m e n t o f t h e d i s e a s e.[K e y w o r d s]p r i m a r y b i l i a r y c h o l a n g i t i s;c l i n i c a l m a n i f e s t a t i o n s;s y m p t o m a t i c t r e a t m e n t随着我国临床医师对原发性胆汁性胆管炎(p r i-m a r y b i l i a r y c h o l a n g i t i s,P B C)认识的增加,自身抗体和肝活检等技术的广泛开展,该病的检出率明显上升,已经成为我国非病毒性肝病的重要组成部分㊂熊去氧胆酸(u r s o d e o x y c h o l i c a c i d,U D C A)作为食品药品监督管理局批准的一线药物,近40年来在P B C的治疗中占据了绝对的主导地位㊂多项研究表明长期服用U D C A可改善P B C患者肝脏生化指标㊁肠道菌群及脑缺血缺氧,同时具有延缓组织学进展及提高无移植生存率的作用[1-2]㊂其他关于P B C的药物治疗较为有限,临床治疗更倾向于在原发病治疗的基础上对一些临床症状进行干预,改善患者生活质量和预后[3-4]㊂早期P B C患者的临床表现并不典型,无力和瘙痒是最常见的初始症状,治疗目标包括缓解症状㊁减少或推迟并发症㊁延长患者寿命等㊂早期对P B C患者进行干预治疗可以改善患者预后及生活质量,因此,本文归纳总结了P B C的一些临床表现及对症处理方法,以期为P B C的鉴别和对症治疗提供依据㊂根据血清碱性磷酸酶(a l k a l i n e p h o s p h a t a s e, A L P)升高和抗线粒体抗体(a n t i-m i t o c h o n d r i a l a n t i-b o d y,AMA)阳性可对大多数P B C患者进行临床诊断,但该诊断标准并没有囊括P B C表现的全部范围㊂7293重庆医学2021年11月第50卷第22期*基金项目:国家自然科学基金项目(81600449);江苏省 青年医学人才 项目(Q N R C2016400)㊂作者简介:程苕莼(1997-),在读硕士,主要从事自身免疫性肝病方面的研究㊂ә通信作者,E-m a i l:b i a n z h a o l i a n1998@163.c o m㊂Copyright©博看网 . All Rights Reserved.AMA是诊断P B C灵敏度和特异度最高的血清抗体,尤其以AMA-M2亚型诊断价值最高,但5%~10% P B C患者的AMA为阴性[5]㊂具有典型肝内胆汁淤积生化变化及肝活检符合P B C的病理特征,但AMA 为阴性的患者被定义为AMA阴性P B C患者㊂抗糖蛋白210(g p210)抗体及抗核蛋白体100(s p100)抗体对AMA阴性P B C患者的诊断具有重要意义,2018年美国肝病研究协会指南推荐将g p210抗体或s p100抗体阳性作为AMA阴性P B C患者的诊断标准之一[6]㊂研究人员发现,AMA阴性的女性患者更容易合并自身免疫疾病,在预后和生存方面,AMA阴性患者也比阳性患者差,因此,对AMA阴性的P B C患者进行早期诊断尤为重要[5]㊂在A L P异常的P B C患者中,AMA被认为是高度特异性(ȡ95%)的,无须进行肝活检就可以可靠地诊断P B C[7],但到目前为止,还没有大规模的前瞻性研究来评估在缺乏P B C临床指征的情况下AMA的具体意义㊂对于血清AMA阳性而A L P水平正常者是否存在胆管损伤㊁是否会进展为P B C㊁是否需要早期U D C A治疗㊁是否需要肝穿刺以明确诊断及如何确定肝穿刺时机等是目前的研究重点㊂1 P B C患者瘙痒㊁乏力症状的治疗有20%~70%的P B C患者存在瘙痒症状,并且瘙痒程度与某些实验室指标的异常程度,疾病的持续时间及组织学严重程度无关[8-9]㊂瘙痒的病理生理机制可能与胆汁酸和胆汁盐的积累,内源性阿片受体的失衡,自身抗体水平,性腺皮质类固醇等有关[10-11]㊂尽管U D C A是P B C治疗的核心药物,但是其对瘙痒症状的改善无明显帮助[12]㊂胆汁酸结合树脂作为治疗瘙痒的一线药物,具有丰富的临床经验佐证和良好的安全性,是目前唯一被批准用于治疗胆汁淤积性瘙痒的药物[13]㊂利福平作为二线治疗药物,在治疗慢性胆汁淤积继发性瘙痒方面卓有成效,特别是对不能耐受或对胆汁酸结合受体应答不佳的瘙痒症患者作用良好㊂纳曲酮是阿片类药物的拮抗剂,作为治疗胆汁淤积性瘙痒的三线药物,其在P B C中控制瘙痒的功效已在2项随机对照试验中得到证实[14]㊂舍曲林和加巴喷丁属于选择性5-羟色胺再摄取抑制剂,作为胆汁淤积性瘙痒的经验治疗药物,通常在瘙痒患者对其他药物无反应的情况下应用[15]㊂在一项小型安慰剂对照试验中,舍曲林已被证明可有效改善患者瘙痒症状,但其缓解瘙痒与其抗抑郁作用无关[16]㊂目前,需要更多的多中心安慰剂对照试验对加巴喷丁的安全性及有效性进行验证㊂乏力是另一种常见症状,会影响约80%的P B C 患者,其主要生物学特征包括白天嗜睡和自主神经系统功能障碍[17-19]㊂有研究表明,乏力通常与焦虑症㊁抑郁症和睡眠障碍同时发生,被患者视为最影响生活质量的症状[20-22]㊂与常规疲劳不同,P B C所引起的乏力与运动无关,不能通过休息来缓解,并且其严重程度与疾病的组织学阶段和自身抗体水平无关[23-24]㊂尽管P B C患者乏力的具体机制尚未被完全阐明,但研究人员认为,结构性脑异常,自主神经系统功能异常,心理因素及周围肌肉线粒体功能异常程度等可能在发病机制中占很大比例[25-28]㊂目前尚无针对P B C乏力的特定治疗方法,临床评估应先从排除可能引起乏力的其他疾病(如贫血,甲状腺功能减退和抑郁)开始㊂如果乏力症状严重影响了患者的日常生活,可以尝试使用莫达非尼(一种批准用于发作性睡病的兴奋剂)来帮助患者缓解虚弱症状[29-30]㊂2 亚临床 P B C的临床特征AMA阳性而A L P正常,并且肝活检符合P B C 肝组织诊断者被定义为 亚临床 P B C患者㊂法国一项多中心㊁前瞻性队列研究发现,在AMA阳性但A L P正常的人群中,5年内P B C的发生率仅为16%[31]㊂G U L AMHU S E I N等[32]的研究成果佐证了上述发现:在P B C患者的一级亲属中,单纯AMA阳性者随访8年后无一例发展为P B C㊂但与上述发现不同的是,M I T C H I S O N等[33]曾对29例AMA阳性而A L P正常者进行了肝脏活检,发现27例患者显示了P B C的组织学特征㊂M E T C A L F等[34]在1996年同样对一组由29例无症状的AMA阳性患者组成的队列进行了研究,肝活检筛查发现24例患者的组织学病变与P B C相符㊂在平均17.8年的随访期间, 76%的患者出现P B C症状,83%的患者肝脏检查显示胆汁淤积㊂然而,没有患者发展为门脉高压或肝硬化,也没有患者死于P B C,研究人员指出这些患者的疾病进展非常缓慢㊂一项来自瑞士的队列研究发现, 80%AMA阳性且A L P水平正常的患者具有典型的或与P B C相一致的肝脏组织学表现㊂同时该项研究发现在22例接受U D C A治疗的 亚临床 P B C患者中有14例在治疗前谷氨酰转肽酶(g a mm a-g l u t a m y l-t r a n s f e r a s e,G G T)水平高于正常值,提出了G G T可以作为 亚临床 P B C患者潜在的生物标志物[35]㊂G E R U S S I等[36]进行的大型国际研究也报告了G G T 水平在预测P B C肝移植或死亡中的可靠预后价值㊂这些结果的差异可能是由于各项研究所使用的技术和诊断阈值及筛查人群的类型㊁年龄和性别结构不同造成的,因此,对于单纯AMA阳性患者,是否需要行肝活检进一步明确诊断,目前尚缺乏足够的临床证据,仍然需要多中心㊁前瞻性的大样本研究进一步明确㊂8293重庆医学2021年11月第50卷第22期Copyright©博看网 . All Rights Reserved.近期上海仁济医院的研究人员在60例AMA阳性而A L P正常的试验组中发现了49例 亚临床 P B C 患者,并且其存在明显胆管反应及胆管细胞衰老的表现,但轻于典型P B C组,提示 亚临床 P B C患者确实存在一定程度的胆管损伤㊂AMA阳性可在患者出现临床症状㊁生化异常和组织学变化之前出现,及早行AMA检查可及时发现患者并有助于检测有P B C家族史的人群[37]㊂同时建议该类患者尤其AMAȡ1ʒ320和A L P>0.475U L N者及时进行肝穿刺活检术,以明确诊断[38]㊂进一步的随访发现所有接受U D C A 治疗的 亚临床 P B C患者均未出现症状或肝功能持续异常,证明了终身服用U D C A的临床指南可能也同样适用于 亚临床 P B C患者㊂而日本之前的一项全国范围研究比较了早期P B C患者治疗组(U D C A在诊断后1年内开始)和延期/不治疗组(U D C A在诊断后1年开始或未给予U D C A治疗)的总生存率㊁失代偿症状的发生率和非肝脏相关病死率,发现延迟/不接受U D C A治疗并不影响早期P B C患者终点事件的发生率[39]㊂并且提出早期P B C患者可能不需要U D C A的及时治疗干预,而是受益于 观察和等待 的治疗方法㊂尽管这里研究的早期对象是指那些无症状㊁A L P<1.67ˑ正常上限㊁正常胆红素和肝脏组织学处于Ⅰ~Ⅱ期的患者,但是其与 亚临床 P B C患者肯定存在一定的交叉性㊂仁济医院及日本研究结果之间的差异性值得进一步深究与挖掘㊂ 亚临床 P B C患者的疾病进展非常缓慢,而仁济医院的研究随访时间不足且样本量较小,可能并没有追踪到研究对象出现生化学异常㊂而来自日本的大数据研究在样本的选择上存在一定问题,延迟/不进行U D C A治疗组的患者明显更年轻,且A L P水平更低,另外一些U D C A治疗中断的患者被错误地记录为从未接受过U D C A治疗,这些可能对研究结果产生了一定的影响㊂具体这种 亚临床 P B C患者是否需要在诊断初期即进行U D C A治疗仍然值得商榷,需要更加有效和持续时间和更长的临床试验进行辅助判断㊂P B C作为典型的肝脏特异的自身免疫性疾病,肝内免疫失衡是其重要发病机制,目前尚不能被完全治愈㊂该病的发作具有隐匿性,早期难以被发现㊂掌握P B C患者的临床特点对疾病的诊断和预后具有重要的指导意义㊂参考文献[1]T A N G R,W E I Y,L I Y,e t a l.G u t m i c r o b i a lp r o f i l e i s a l t e r e d i n p r i m a r y b i l i a r y c h o l a n g i t i sa n d p a r t i a l l y r e s t o r e d a f t e r U D C A t h e r a p y[J].G u t,2018,67(3):534-541.[2]H A R M S M,V A N B U U R E N H,C O R P E C HO T C,e t a l.U r s o d e o x y c h o l i c a c i d t h e r a p y a n d l i v e r t r a n s p l a n t-f r e e s u r v i v a l i n p a t i e n t s w i t h p r i m a-r y b i l i a r y c h o l a n g i t i s[J].J H e p a t o l,2019,71(2):357-365.[3]S H A H R A,K OWD L E Y K V.M e c h a n i s m s a n d t r e a t m e n t s o f p r u r i t u s i n p r i m a r y b i l i a r y c h o l a n g i t i s[J].S e m i n L i v e r D i s,2019,39(2): 209-220.[4]G A T S E L I S N K,G O E T J C,Z A C HO U K,e ta l.F a c t o r s A s s o c i a t e d w i t h p r o g r e s s i o n a n d o u t c o m e s o f e a r l y s t a g e p r i m a r yb i l i a r yc h o l a n-g i t i s[J].C l i n G a s t r o e n t e r o l H e p a t o l,2020,18(3):684-692.[5]C A R E Y E J,A L I A H,L I N D O R K D.P r i m a r yb i l i a r yc i r r h o s i s[J].L a n c e t,2015,386(10003): 1565-1575.[6]L I N D O R K,B OW L U S C,B O Y E R J,e t a l.P r i-m a r y b i l i a r y c h o l a n g i t i s:2018p r a c t i c e g u i d a n c e f r o m t h e A m e r i c a n a s s o c i a t i o n f o r t h e s t u d y o f l i v e r d i s e a s e s[J].H e p a t o l o g y,2019,69(1):394-419.[7]E u r o p e a n A s s o c i a t i o n f o r t h e S t u d y o f t h e L i v-e r.E A S L c l i n i c a l p r a c t i c e g u i d e l i n e s:m a n a g e-m e n t o f c h o l e s t a t i c l i v e r d i s e a s e s[J].J H e p a t o l, 2009,51(2):237-267.[8]R I S H E E,A Z A R M A,B E R G A S A N V.I t c h i n p r i m a r y b i l i a r y c i r r h o s i s:a p a t i e n t s'p e r s p e c t i v e[J].A c t a D e r m V e n e r e o l,2008,88(1):34-37.[9]K R E M E R A E,N AM E R B,B O L I E R R,e t a l. P a t h o g e n e s i s a n d m a n a g e m e n t o f p r u r i t u s i n P B C a n d P S C[J].D i g D i s,2015,33S u p p l2: 164-175.[10]C A R R I O N A F,R O S E N J D,L E V Y C.U n d e r-s t a n d i n g a n d t r e a t i n g p r u r i t u s i n p r i m a r y b i l i a r-y c h o l a n g i t i s[J].C l i n L i v e r D i s,2018,22(3): 517-532.[11]T R I V E D I H D,L I Z A O L A B,T A P P E R E B,e ta l.M a n a g e m e n t o f P r u r i t u s i n p r i m a r yb i l i a r yc h o l a n g i t i s:a n a r r a t i v e r e v i e w[J].A m J M e d, 2017,130(6):744.e1-744.e7.[12]N E V E N S F,A N D R E O N E P,MA Z Z E L L A G,e t a l.A p l a c e b o-c o n t r o l l e d t r i a l of o b e t i c h o l i ca c i d i n p r i m a r yb i l i a r yc h o l a n g i t i s[J].N E n g l JM e d,2016,375(7):631-643.9293重庆医学2021年11月第50卷第22期Copyright©博看网 . All Rights Reserved.[13]I N V E R N I Z Z I P,F L O R E A N I A,C A R B O N EM,e t a l.P r i m a r y b i l i a r y c h o l a n g i t i s:a d v a n c e si n m a n a g e m e n t a n d t r e a t m e n t o f t h e d i s e a s e[J].D i g L i v e r D i s,2017,49(8):841-846.[14]T E R G R,C O R O N E L E,S O R DÁJ,e t a l.E f f i-c a c y a nd s a fe t y of o r a l n a l t r e x o n e t r e a t m e n t f o rp r u r i t u s o f c h o l e s t a s i s,a c r o s s o v e r,d o u b l eb l i n d,p l ac e b o-c o n t r o l l ed s t u d y[J].J He p a t o l,2002,37(6):717-722.[15]E u r o p e a n A s s o c i a t i o n f o r t h e S t u d y o f t h e L i v-e r.E A S L c l i n i c a l p r a c t i c e g u i d e l i n e s:t h e d i a g-n o s i s a n d m a n a g e m e n t o f p a t i e n t s w i t h p r i m a r yb i l i a r yc h o l a n g i t i s[J].J H e p a t o l,2017,67(1): 145-172.[16]MA Y O M,H A N D E M I,S A L D A N A S,e t a l.S e r t r a l i n e a s a f i r s t-l i n e t r e a t m e n t f o r c h o l e s-t a t i c p r u r i t u s[J].H e p a t o l o g y,2007,45(3): 666-674.[17]N E WT O N J L,G I B S O N G J,T OM L I N S O NM,e t a l.F a t i g u e i n p r i m a r y b i l i a r y c i r r h o s i s i sa s s o c i a t e d w i t h e x c e s s i v e d a y t i m e s o m n o l e n c e[J].H e p a t o l o g y,2006,44(1):91-98. [18]J O N E S D E,N E WT O N J L.A n o p e n s t u d y o fm o d a f i n i l f o r t h e t r e a t m e n t o f d a y t i m e s o m n o-l e n c e a n d f a t i g u e i n p r i m a r y b i l i a r y c i r r h o s i s[J].A l i m e n t P h a r m a c o l T h e r,2007,25(4): 471-476.[19]N E WT O N J L,HU D S O N M,T A C H T A T Z I SP,e t a l.P o p u l a t i o n p r e v a l e n c e a n d s y m p t o ma s s o c i a t i o n s o f a u t o n o m i c d y s f u n c t i o n i n p r i-m a r y b i l i a r y c i r r h o s i s[J].H e p a t o l o g y,2007,45(6):1496-1505.[20]M E L L S G F,P E L L S G,N E WT O N J L,e t a l.I m p a c t o f p r i m a r y b i l i a r y c i r r h o s i s o n p e r c e i v e dq u a l i t y o f l i f e:t h e U K-P B C n a t i o n a l s t u d y[J].H e p a t o l o g y,2013,58(1):273-283.[21]S T A N C A C M,B A C H N,K R A U S E C,e t a l.E-v a l u a t i o n o f f a t i g u e i n U.S.p a t i e n t s w i t h p r i-m a r y b i l i a r y c i r r h o s i s[J].A m J G a s t r o e n t e r o l, 2005,100(5):1104-1109.[22]T A L WA L K A R J A,D O N L I N G E R J J,G O S-S A R D A A,e t a l.F l u o x e t i n e f o r t h e t r e a t m e n to f f a t i g u e i n p r i m a r y b i l i a r y c i r r h o s i s:a r a n-d o m i ze d,d o u b l e-b l i n d c o n t r o l l e d t r i a l[J].D i gD i s S c i,2006,51(11):1985-1991.[23]B JÖR N S S O N E,S I M R E N M,O L S S O N R,e ta l.F a t i g u e i s n o t a s p e c i f i c s y m p t o m i n p a t i e n t sw i t h p r i m a r y b i l i a r y c i r r h o s i s[J].E u r J G a s-t r o e n t e r o l H e p a t o l,2005,17(3):351-357.[24]C H A L I F O U X S L,K O N Y N P G,C HO I G,e ta l.E x t r a h e p a t i c M a n i f e s t a t i o n s o f p r i m a r yb i l i-a r y c h o l a n g i t i s[J].G u t L i v e r,2017,11(6):771-780.[25]J O N E S D E,G R A Y J C,N E WT O N J.P e r-c e i v ed f a t i g ue i s c o m p a r a b l e b e t w e e n d if f e r e n td i se a s e g r o u p s[J].Q J M,2009,102(9):617-624.[26]L E E J Y,D A N F O R D C J,T R I V E D I H D,e ta l.T r e a t m e n t o f f a t i g u e i n p r i m a r yb i l i a r yc h o l a n g i t i s:a s y s t e m a t i c r e v i e w a nd me t a-a n a l-y s i s[J].D i g D i s S c i,2019,64(8):2338-2350.[27]K H A N N A A,L E I G H T O N J,L E E WO N G L,e t a l.S y m p t o m s of P B C-P a t h o p h y s i o l og y a n dm a n a g e m e n t[J].B e s t P r a c t R e s C l i n G a s t r o e n-t e r o l,2018,34:41-47.[28]Y A G I M,T A N A K A A,A B E M,e t a l.S y m p-t o m s a n d h e a l t h-r e l a t e d q u a l i t y o f l i f e i n J a p a-n e s e p a t i e n t s w i t h p r i m a r y b i l i a r y c h o l a n g i t i s[J].S c i R e p,2018,8(1):12542.[29]H A R D Y T,MA C D O N A L D C,J O N E S D E,e ta l.A f o l l o w-u p s t u d y o f m o d a f i n i l f o r t h e t r e a t-m e n t o f d a y t i m e s o m n o l e n c e a n d f a t i g u e i n p r i-m a r y b i l i a r y c i r r h o s i s[J].L i v e r I n t,2010,30(10):1551-1552.[30]I A N G A N S,D E J O N G H M,K A P L A N M M.M o d a f i n i l i n t h e t r e a t m e n t o f d e b i l i t a t i n g f a-t i g u e i n p r i m a r y b i l i a r y c i r r h o s i s:a c l i n i c a l e x-p e r i e n c e[J].D i g D i s S c i,2009,54(10):2242-2246.[31]D A H L Q V I S T G,G A O U A R F,C A R R A T F,e ta l.L a r g e-s c a l e c h a r a c t e r i z a t i o n s t u d y o f p a-t i e n t s w i t h a n t i m i t o c h o n d r i a l a n t ib o d i e s b u tn o n e s t a b l i s h e d p r i m a r y b i l i a r y c h o l a n g i t i s[J].H e p a t o l o g y,2017,65(1):152-163.[32]G U L AMHU S E I N A,J U R A N B,A T K I N S O NE,e t a l.L o w i n c i d e n c e o f p r i m a r y b i l i a r y c i r-r h o s i s(P B C)i n t h e f i r s t-d e g r e e r e l a t i v e s o fP B C p r o b a n d s a f t e r8y e a r s o f f o l l o w-u p[J].L i v e r I n t,2016,36(9):1378-1382.[33]M I T C H I S O N H,B A S S E N D I N E M,H E N D RI C K A,e t a l.P o s i t i v e a n t i m i t o c h o n d r i a l a n t i-b o d y b u t n o r m a l a l k a l i n e p h o s p h a t a s e:i s t h i sp r i m a r y b i l i a r y c i r r h o s i s[J].H e p a t o l o g y,1986,6(6):1279-1284.(下转第3936页)0393重庆医学2021年11月第50卷第22期Copyright©博看网 . All Rights Reserved.[27]N E G R O N I A,C O L A N T O N I E,P I E R D OM E NI C O M,e t a l.R I P3a n d p M L K L p r o m o t e n e c-r o p t o s i s-i n d u c e d i n f l a mm a t i o n a n d a l t e r m e m-b r a n e p e r m e a b i l i t y i n i n t e s t i n a l e p i t h e l i a lc e l l s[J].D i g L i v e r D i s,2017,49(11):1201-1210.[28]L E E K H,K A N G T B.T h e m o l e c u l a r l i n k s b e-t w e e n c e l l d e a t h a n d i n f l a mm a s o m e[J].C e l l s, 2019,8(9):1057.[29]陈鑫.超高分辨率显微成像研究M L K L依赖的细胞坏死机制[D].厦门:厦门大学,2013.[30]S HU L G A N,P A S T O R I N O J G.G R I M-19-m e-d i a te d t r a n s l o c a t i o n of S T A T3t o m i t o c h o n d r i a i s n e c e s s a r y f o r T N F-i n d u c e d n e c r o p t o s i s[J].JC e l l S c i,2012,125(12):2995-3003.[31]K I M H,Z AM E L R,B A I X H,e t a l.I s c h e m i a-r e p e r f u s i o n i n d u c e s d e a t h r e c e p t o r-i n d e p e n d e n tn e c r o p t o s i s v i a c a l p a i n-S T A T3a c t i v a t i o n i n a l u n g t r a n s p l a n t s e t t i n g[J].A m J P h y s i o l L u n gC e l l M o l P h y s i o l,2018,315(4):595-608.[32]S M I T H A D,L U C,P A Y N E D,e t a l.A u t o c r i n eI L6-m e d i a t e d a c t i v a t i o n o f t h e S T A T3-D NMTa x i s s i l e n c e s t h e T N Fα-R I P1n e c r o p t o s i s p a t h-w a y t o s u s t a i n s u r v i v a l a n d a c c u m u l a t i o n o fm y e l o i d-d e r i v e d s u p p r e s s o r c e l l s[J].C a n c e rR e s,2020,80(15):3145-3156.[33]WA N G S,N I H M,D O R K O K,e t a l.I n c r e a s e dh e p a t i c r e c e p t o r i n t e r a c t i n g p r o t e i n k i n a s e3e x-p r e s s i o n d u e t o i m p a i r e d p r o t e a s o m a l f u n c t i o n s c o n t r i b u t e s t o a l c o h o l-i n d u c e d s t e a t o s i s a n d l i v-e r i n j u r y[J].O n c o t a r g e t,2016,7(14):17681-17698.[34]Z H A N G L,WA N G X,C H E N S,e t a l.M e d i u m-c h a i n t r i g l y c e r ide s a t t e n u a t e l i v e r i n j u r y i n l i-p o p o l y s a c c h a r i d e-c h a l l e n g e d p i g s b y i n h i b i t i n gn e c r o p t o t i c a n d i n f l a mm a t o r y s i g n a l i n g p a t h-w a y s[J].I n t J M o l S c i,2018,19(11):3697.[35]Z HU A N G Y,X U H C,S H I N D E P V,e t a l.F r a g i l e X m e n t a l r e t a r d a t i o n p r o t e i n p r o t e c t sa g a i n s t t u m o u r n e c r o s i s f a c t o r-m e d i a t e d c e l ld e a t h a n d l i v e r i n j u r y[J].G u t,2020,69(1):133-145.[36]C H E N L,C A O Z,Y A N L,e t a l.C i r c u l a t i n g r e-c e p t o r-i n t e r a c t i n g p r o t e i n k i n a s e3a r e i n c r e a s ed i n H B V p a t ie n t s w i t h a c u t e-o n-c h r o n i c l i v e rf a i l u r e a n d a r e a s s o c i a t e d w i t h c l i n i c a l o u t c o m e[J].F r o n t P h y s i o l,2020,11:526.(收稿日期:2021-02-18修回日期:2021-07-08)(上接第3930页)[34]M E T C A L F J,M I T C H I S O N H,P A L M E R J,e ta l.N a t u r a l h i s t o r y o f e a r l y p r i m a r yb i l i a r yc i r-r h o s i s[J].L a n c e t,1996,348(9039):1399-1402.[35]T E R Z I R O L I B E R E T T A-P I C C O L I B,S T I R N I-MA N N G,M E R T E N S J,e t a l.P r i m a r y b i l i a r y c h o l a n g i t i s w i t h n o r m a l a l k a l i n e p h o s p h a t a s e:an e g l e c t e d c l i n i c a l e n t i t y c h a l l e n g i n g c u r r e n tg u i d e l i n e s[J].J A u t o i mm u n,2020,116: 102578.[36]G E R U S S I A,B E R N A S C O N I D,O'D O N N E L LS,e t a l.M e a s u r e m e n t o f g a mm a g l u t a m y l t r a n s f e r a s e t o d e t e r m i n e r i s k o f l i v e r t r a n s p l a n-t a t i o n o r d e a t h i n p a t i e n t s w i t h p r i m a r y b i l i a r y c h o l a n g i t i s[J].C l i n G a s t r o e n t e r o l H e p a t o l, 2021,19(8):1688-1697.[37]H E A T H C O T E E.M a n a g e m e n t o f p r i m a r y b i l-i a r y c i r r h o s i s.T h e A m e r i c a n a s s o c i a t i o n f o r t h e s t u d y o f l i v e r d i s e a s e s p r a c t i c e g u i d e l i n e s[J].H e p a t o l o g y,2000,31(4):1005-1013.[38]S U N C,X I A O X,Y A N L,e t a l.H i s t o l o g i c a l l yp r o v e n AMA p o s i t i v e p r i m a r y b i l i a r y c h o l a n g i-t i s b u t n o r m a l s e r u m a l k a l i n e p h o s p h a t a s e:i sa l k a l i n e p h o s p h a t a s e t r u l y a s u r r o g a t e m a r k e r[J].J A u t o i mm u n,2019,99:33-38.[39]T A N A K A A,H I R O H A R A J,N A K A N O T,e ta l.E f f e c t o f d e f e r r e d o r n o t r e a t m e n t w i t h u r-s o d e o x y c h o l i c a c i d i n p a t i e n t s w i t h e a r l y p r i m a-r yb i l i a r yc h o l a n g i t i s[J].H e p a t o l R e s,2018,48(9):727-734.(收稿日期:2021-03-18修回日期:2021-07-28)6393重庆医学2021年11月第50卷第22期Copyright©博看网 . All Rights Reserved.。
内镜下减重手术治疗肥胖的研究进展
内镜下减重手术治疗肥胖的研究进展文志勇;刘志平;文剑波【摘要】肥胖在当今社会逐渐成为危害人类健康的重要因素.在治疗肥胖症方面,饮食控制、运动和传统的内科疗法均难以获得稳定的减肥疗效,而外科手术创伤大、改变解剖结构,难以重复及影响美观,难以满足现代人的要求.随着内镜技术的发展,通过自然腔道(口腔-胃)实施减重手术显示出其独特优势.根据内镜下手术的原理,可分为:胃限制性手术、胃-空肠旁路途径、胃空间占用性手术.目前国内实施内镜下减重手术很少.本文对此三种术式、所需内镜装置及国内外应用效果作一综述,以期更多临床医师及群众了解内镜下减重手术的优势.【期刊名称】《赣南医学院学报》【年(卷),期】2018(038)003【总页数】6页(P265-270)【关键词】肥胖症;内镜手术;减重手术【作者】文志勇;刘志平;文剑波【作者单位】赣南医学院,江西赣州341000;赣南医学院基础医学院,江西赣州341000;赣南医学院第六临床学院,江两萍乡337000【正文语种】中文【中图分类】R723.14近年来,随着世界经济的发展,饮食与生活习惯的改变,肥胖症在全球越来越普遍,2012年我国5省市18~60岁肥胖状况调查显示,超重为28.9%,肥胖为6.3%,肥胖趋势明显,成为影响居民健康的重要疾患[1],国外一项2007~2012美国肥胖流行调查显示39.96%男性,29.74%女性为超重,35.04%男性、36.84%女性为肥胖[2],而肥胖相关的高血压、高血脂、糖尿病等越来越被重视[3]。
在治疗肥胖症方面,饮食控制、运动和传统的内科疗法均难以获得稳定的减肥疗效,而外科减重手术难以满足效果及美观的追求,临床上逐渐开展的内镜下减重手术,具有更小创伤,可逆性及可重复性等优势,内镜下减重手术最早可追溯到上世纪80年代在胃内安放自由浮动的橡胶球囊,但在减重效果及并发症都难以达到满意效果,本世纪初随着内镜技术发展及对现有装备进行改进,在狭小胃内空间进行的操作越来越多,overstitch、IOP、endocinch操作系统都能在胃内进行缝合,国内实施减重手术很少。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
EASL Clinical Practice Guidelines:Management of cholestatic liver diseasesEuropean Association for the Study of the Liver *Keywords :Primary biliary cirrhosis;Primary sclerosing cholangitis;Overlap syndrome;Immunoglobulin G4-associated cholangitis;Drug-induced cholestatic liver disease;Genetic cholestatic liver disease;Cholestatic liver diseases in pregnancy;Intrahepatic cholestasis of pregnancy;Fatigue;Pruritus 1.IntroductionEASL Clinical Practice Guidelines (CPG)on the management of cholestatic liver diseases define the use of diagnostic,therapeutic and preventive modalities,including non-invasive and invasive procedures,in the management of patients with cholestatic liver diseases.They are intended to assist physicians and other health-care providers as well as patients and interested individ-uals in the clinical decision-making process by describing a range of generally accepted approaches for the diagnosis,treatment and prevention of specificcholestatic liver diseases.The clinical care for patients with cholestatic liver diseases has advanced considerably during recent decades thanks to growing insight into pathophysiological mechanisms and remarkable meth-odological and technical developments in diagnostic procedures as well as therapeutic and preventive approaches.Still,various aspects in the care of patients with cholestatic disorders remain incompletely resolved.The EASL CPG on the management of cholestatic liver diseases aim to provide current recommendations on the following issues:Diagnostic approach to the cholestatic patient. Diagnosis and treatment of primary biliary cirrhosis (PBC).Diagnosis and treatment of PBC–autoimmune hepatitis (AIH)overlap syndrome.Diagnosis and treatment of primary sclerosing cho-langitis (PSC).Diagnosis and treatment of PSC–AIH overlap syndrome.Diagnosis and treatment of immunoglobulin G4-associated cholangitis (IAC).0168-8278/$36.00Ó2009Published by Elsevier B.V.on behalf of the European Association for the Study of the Liver.doi:10.1016/j.jhep.2009.04.009*EASL Office,7rue des Battoirs,1205Geneva,Switzerland.Tel.:+41228070360;fax:+41223280724.E-mail address:easloffice@easloffice.euAbbreviations:AIH,autoimmune hepatitis;AIP,autoimmune pancreatitis;AMA,antimitochondrial antibodies;AP,alkaline phosphatase in serum;ASMA,anti-smooth muscle antibodies;BRIC,benign recurrent intrahepatic cholestasis;CCA,cholangiocarcinoma;CF,cystic fibrosis;CFALD,cystic fibrosis-associated liver disease;CPG,Clinical Practice Guidelines;CT,computed tomography;DILI,drug-induced liver injury;EASL,European Association for the Study of the Liver;ERCP,endoscopic retrograde cholangiopancreatography;EUS,endoscopic ultrasound;FDG-PET,(18F)-fluoro-deoxy-D -glucose positron emission tomography;FXR,farnesoid X receptor;c GT,c -glutamyltranspeptidase in serum;HCC,hepatocellular carci-noma;IAC,immunoglobulin G4-associated cholangitis;IAIHG,International Autoimmune Hepatitis Group;IBD,inflammatory bo-wel disease;IgG,immunoglobulin G in serum;IgG4,immunoglobulin G4in serum;MRCP,magnetic resonance cholangiopancreatography;NASH,non-alcoholic steatohepatitis;PBC,primary biliary cirrhosis;PDC-E2,E2subunit of the pyruvate dehydrogenase complex;PSC,primary sclerosing cholangitis;PIIINP,procollagen-3-aminoterminal propeptide;UC,ulcerative colitis;ULN,upper limit of normal;US,ultrasound.Contributors:Clinical Practice Guidelines Panel:Ulrich Beuers,Kirsten M.Boberg,Roger W.Chapman,Olivier Chazouille`res,Pietro Invernizzi,David E.J.Jones,Frank Lammert,Albert Pare`s,Michael Trauner;Reviewers:Antonio Benedetti,Peter L.M.Jansen,Hanns-Ulrich Marschall,James Neuberger,Gustav Paumgartner,RaoulPoupon,Jesu´s Prieto./locate/jhepDiagnosis and treatment of drug-induced cholestatic liver diseases.Diagnosis and treatment of genetic cholestatic liver diseases.Diagnosis and treatment of cholestatic liver diseases in pregnancy.Treatment of extrahepatic manifestations of chole-static liver diseases.A panel of experts selected by the EASL Governing Board in May2008wrote and discussed these guidelines between June and November2008.These guidelines have been produced using evidence from PubMed and Cochra-ne database searches before1October,2008.Where pos-sible,the level of evidence and recommendation are cited (Tables1a,1b).The evidence and recommendations in these guidelines have been graded according to the Grad-ing of Recommendations Assessment Development and Evaluation(GRADE system)[1].The strength of recom-mendations thus reflects the quality of underlying evi-dence which has been classified in one of three levels: high[A],moderate[B]or low-quality evidence[C].The GRADE system offers two grades of recommendation: strong[1]or weak[2](Table1b).The CPG thus consider the quality of evidence:the higher,the more likely a strong recommendation is warranted;the greater the variability in values and preferences,or the greater the uncertainty, the more likely a weaker recommendation is warranted.Where no clear evidence exists,guidance is based on the consensus advice of expert opinion in the literature and the writing committee.2.Diagnostic approach to cholestasisCholestasis is an impairment of bile formation and/or bileflow which may clinically present with fatigue,pru-ritus and,in its most overt form,jaundice.Early bio-chemical markers in often asymptomatic patients include increases in serum alkaline phosphatase(AP) and c-glutamyltranspeptidase(c GT)followed by conju-gated hyperbilirubinemia at more advanced stages.Cho-lestasis may be classified as intrahepatic or extrahepatic. Intrahepatic cholestasis may result from hepatocellular functional defects or from obstructive lesions of the intrahepatic biliary tract distal from bile canaliculi.Cho-lestasis may also be related to mixed mechanisms in dis-eases such as lymphoma[2].By convention,cholestasis is considered chronic if it lasts>6months.Most chronic cholestatic diseases are purely intrahepatic,whereas sclerosing cholangitis may affect small and large intrahe-patic and/or extrahepatic bile ducts.Asymptomatic patients are generally identified when routine laboratory tests are being performed or during work-up for another disease when an increase is noted in the serum level of AP and/or c GT.Isolated serum c GT elevation has little specificity for cholestasis,and may also result from enzyme induction in response to alcohol or drug intake. Isolated serum AP elevation is seen in cholestatic liver diseases including certain rare disorders(e.g.,progres-sive familial intrahepatic cholestasis(PFIC)1&2,bile acid synthesis defects),but may also result from rapid bone growth(e.g.,in children),bone disease(e.g., Paget’s disease),or pregnancy.The cut-offlevels of serum AP and c GT requiring diagnostic work-up are debated:AP levels higher than1.5times the upper limit of normal(ULN)and c GT levels>3ÂULN have been proposed.The differential diagnosis of cholestatic disor-Table1aCategories of evidence.Grade EvidenceI Randomized controlled trialsII-1Controlled trials without randomizationII-2Cohort or case-control analytic studiesII-3Multiple time series,dramatic uncontrolled experimentsIII Opinions of respected authorities,descriptive epidemiologyTable1bEvidence grading(adapted from the GRADE system[1]).Evidence NotesHigh quality Further research is very unlikely to change our confidence in theestimate of effectAModerate quality Further research is likely to have an important impact on ourconfidence in the estimate of effect and may change the estimateBLow quality Further research is very likely to have an important impact on ourconfidence in the estimate of effect and is likely to change theestimate.Any change of estimate is uncertainCRecommendationStrong Factors influencing the strength of the recommendation includedthe quality of the evidence,presumed patient-important outcomes,and cost1Weak Variability in preferences and values,or more uncertainty.Recommendation is made with less certainty,higher cost orresource consumption 2238European Association for the Study of the Liver/Journal of Hepatology51(2009)237–267ders can be wide(Table2).Nevertheless,thefirst critical step is to differentiate intra-and extrahepatic cholestasis.Careful patient history and physical examination are essential in the diagnostic process and may provide valu-able information so that an experienced clinician can pre-dict the nature of cholestasis in many cases[3].Presence of extrahepatic diseases has to be recorded.A thorough occupational and drug history is imperative and any med-ications taken within6weeks of presentation may be incriminated(and discontinued);this includes herbal medicines,vitamins and other substances.A history of fever,especially when accompanied by rigors or right upper quadrant abdominal pain is suggestive of cholangi-tis due to obstructive diseases(particularly choledocholi-thiasis),but may be seen in alcoholic disease and rarely, viral hepatitis.A history of prior biliary surgery also increases the likelihood that biliary obstruction is present. Finally,a family history of cholestatic liver disease sug-gests a possibility of a hereditary disorder.Some chole-static disorders are observed only under certain circumstances(e.g.,pregnancy,childhood,liver trans-plantation,HIV-infection),and may require specific investigations that are not relevant in other populations.Abdominal ultrasonography is usually thefirst step to exclude dilated intra-and extrahepatic ducts and mass lesions because it is rather sensitive and specific, non-invasive,portable and relatively inexpensive.Its disadvantages are that itsfindings are operator-depen-dent and abnormalities of bile ducts such as those observed in sclerosing cholangitis may be missed.Fur-thermore,the lower common bile duct and pancreas are usually not well puted tomography of the abdomen is less interpreter-dependent,but is asso-ciated with radiation exposure and may be not as good as ultrasound at delineating the biliary tree.If bile duct abnormalities are present,further work-up depends on the presumed cause.From a purely diagnostic perspective,magnetic resonance cholangiopancreatogra-phy(MRCP)is a safe option to explore the biliary tree.Its accuracy for detecting biliary tract obstruction approa-ches that of endoscopic retrograde cholangiopancreatog-raphy(ERCP)when performed in experienced centres with state-of-the-art technology.Endoscopic ultrasound (EUS)is equivalent to MRCP in the detection of bile duct stones and lesions causing extrahepatic obstruction and may be preferred to MRCP in endoscopic units.Extrahepatic biliary obstruction may be caused by stones,tumours,cysts,or strictures.The gold standard for visualizing the biliary tract and treating extrahepatic biliary obstruction is endoscopic retrograde cholangio-pancreatography(ERCP),but even in experienced hands it carries a significant complication rate(pancrea-titis in3–5%of cases;when combined with sphincterot-omy,bleeding2%,cholangitis1%,procedure-related mortality0.4%[4]).Thus,when extrahepatic obstruction is considered and the need for endoscopic intervention is unclear,MRCP or EUS should be performed in order to avoid ERCP if it is not needed[3].If imaging studies do not demonstrate mechanical obstruction,a diagnosis of intrahepatic cholestasis can be reasonably made.However,in an individual whose history suggests an extrahepatic cause(like early pancre-atic or ampullary carcinoma),clinical judgment should Table2bCauses of intrahepatic cholestasis in infancy and childhood[2]. Metabolic disease–with biliary tract involvement:a1-antitrypsin storage disease,cysticfibrosis–without biliary tract involvement:galactosemia,tyrosinemia,fatty acid oxidation defects,lipid and glycogen storage disorders,peroxisomal disorders–specific defects in biliary function:disorders of bile acid biosynthesis and conjugationdisorders of canalicular secretion(PFIC)Paucity of bile ducts–syndromic:Alagille syndrome(Jagged1defect)–non-syndromicDuctal plate malformationsInfections:bacterial,viralToxic:parenteral nutrition,drugsIdiopathic neonatal hepatitisCirrhosis(any cause)Table2aCauses of intrahepatic cholestasis in adulthood.Hepatocellular cholestasisSepsis-,endotoxemia-induced cholestasisCholestatic variety of viral hepatitisAlcoholic or non-alcoholic steatohepatitisDrug-or parenteral nutrition-induced cholestasisGenetic disorders:e.g.,BRIC,PFIC,ABCB4deficiency,intrahepaticcholestasis of pregnancy(ICP),erythropoietic protoporphyriaMalignant infiltrating disorders:e.g.,hematologic diseases,metastaticcancerBenign infiltrating disorders:e.g.,amyloidosis,sarcoidosis hepatis andother granulomatoses,storage diseasesParaneoplastic syndromes:e.g.,Hodgkin disease,renal carcinomaDuctal plate malformations:e.g.,congenital hepaticfibrosisNodular regenerative hyperplasiaVascular disorders:e.g.,Budd–Chiari syndrome,veno-occlusivedisease,congestive hepatopathyCirrhosis(any cause)Cholangiocellular cholestasisPrimary biliary cirrhosis(AMA+/AMAÀ)Primary sclerosing cholangitisOverlap syndromes of PBC and PSC with AIHIgG4-associated cholangitisIdiopathic adulthood ductopeniaDuctal plate malformations:biliary hamartoma,Caroli syndromeCysticfibrosisDrug-induced cholangiopathyGraft vs.host diseaseSecondary sclerosing cholangitis:e.g.,due to various forms ofcholangiolithiasis,ischemic choangiopathies(hereditary hemorragictelangiectasia,polyarteritis nodosa and other forms of vasculitis),infectious cholangitis related to AIDS and other forms ofimmunodepression,etc.European Association for the Study of the Liver/Journal of Hepatology51(2009)237–267239be pursued and repeat ultrasound or another imaging procedure should be performed[3].When extrahepatic obstruction has been reasonably excluded,further work-up of intrahepatic cholestasis (Table2)depends on the clinical setting.In adult patients with chronic intrahepatic cholesta-sis,the next step is testing for serum antimitochondrial antibodies(AMA)since the diagnosis of PBC,which is the major cause of small-duct biliary diseases[5], can be made with confidence in a patient with high-titer AMA(P1/40)and a cholestatic serum enzyme profile in the absence of an alternative explanation[6].A liver biopsy may still be appropriate in selected patients.If AMA and PBC-specific antinuclear antibodies(ANA) are negative,MRCP(in a specialized centre)may be the next diagnostic step for most patients with chronic intrahepatic cholestasis of unknown cause.Subsequently,a liver biopsy should be performed when the diagnosis is still unclear.Particular attention to the condition of bile ducts is critical in the histologic evaluation and a biopsy of adequate quality should con-tain P10portalfields because of the high degree of sam-pling variability in patients with small bile duct disease. Biopsyfindings should be classified under(i)disordersinvolving bile ducts(for typical biliary lesions,see Table 3)the main causes being AMA-negative PBC,isolated small duct PSC,ABCB4deficiency,sarcoidosis,idio-pathic ductopenia or prolonged drug-induced cholesta-sis;(ii)disorders not involving bile ducts,the main causes being a variety of storage or infiltrative liver dis-eases,hepatic granulomas(without cholangitis),nodular regenerative hyperplasia,peliosis,sinusoidal dilatation and cirrhosis;and(iii)hepatocellular cholestasis with only minimal histologic abnormalities as observed in benign recurrent intrahepatic cholestasis(BRIC),estro-gen or anabolic steroid therapy,sepsis,total parenteral nutrition or as a paraneoplastic phenomenon.A general algorithm for evaluating the adult patient with cholestasis is presented in Fig.1.Recommendations1.A detailed history and physical examination areessential(III/C1).2.Ultrasound is thefirst-line non-invasive imaging pro-cedure in order to differentiate intra-from extrahe-patic cholestasis(III/C1).3.Testing for serum antimitochondrial antibodies(AMA)is mandatory in adults with chronic intrahe-patic cholestasis(III/C1).4.Magnetic resonance cholangiopancreatography(MRCP)is the next step to be considered in patients with unexplained cholestasis(III/C1).5.Endoscopic ultrasound(EUS)is an alternative toMRCP for evaluation of distal biliary tract obstruc-tion(II-2/B1).6.Diagnostic endoscopic retrograde cholangiopancrea-tography(ERCP)should be reserved for highly selected cases(II-2/A1).If the need for a therapeutic maneuver is not anticipated,MRCP or EUS should be preferred to ERCP because of the morbidity and mortality related to ERCP(II-2/A1).7.A liver biopsy should be considered in patients withotherwise unexplained intrahepatic cholestasis and a negative AMA test(III/C1).8.Genetic testing for ABCB4(encoding the canalicularphospholipid export pump),when available,should be considered in patients with a negative AMA test and biopsyfindings that might be compatible with PBC or PSC.3.Primary biliary cirrhosis(PBC)3.1.Diagnosis of PBCPatients with PBC may present with symptoms as fatigue,pruritus and/or jaundice,but the majority of them are asymptomatic at diagnosis.Atfirst presenta-tion,very few patients present in advanced stage of dis-ease and with complications of portal hypertension (ascites,hepatic encephalopathy or esophageal variceal bleeding).Currently,a diagnosis of PBC is made with confidence on a combination of abnormal serum liver tests(elevation of AP of liver origin for at least6 months)and presence of AMA(P1:40)in serum[6]. The diagnosis is confirmed by disclosing characteristic histological features offlorid bile duct lesions. Table3Typical biliary lesions and their main causes(liver transplant setting excluded)[2].1.Nonsuppurative destructive cholangitisPrimary biliary cirrhosisPrimary sclerosing cholangitisAutoimmune hepatitisDrug-induced cholangitisSarcoidosisABCB4deficiency(Hepatitis C,B,E)2.Fibrous obliterative cholangitisPrimary sclerosing cholangitisSecondary sclerosing cholangitisIgG4-associated cholangitisSarcoidosis3.Other cholangitis(unusual)Malignant cholangitisLymphoma(Hodgkin or non-Hodgkin)Systemic mastocytosisLangerhans cell histiocytosisNeutrophilic cholangitis:neutrophilic dermatosis4.Ductal plate malformationsBiliary hamartomas(von Meyenburg complexes)Caroli syndromeCongenital hepaticfibrosis240European Association for the Study of the Liver/Journal of Hepatology51(2009)237–267AMA-positive individuals with normal AP carry a high risk to develop PBC during follow-up [7].boratory testsBiochemical markers:Serum AP and c GT are raised in PBC;serum aminotransferases (ALT,AST)and con-jugated bilirubin can also be elevated,but are not diag-nostic.Patients with normal AP and c GT,but with serological stigmata of PBC,should be reassessed clini-cally and biochemically at annual intervals.Patients with PBC typically present elevated levels of immuno-globulin M.Serum cholesterol is commonly elevated like in other cholestatic conditions.Alterations in prothrom-bin time,serum albumin and conjugated bilirubin are observed only in advanced disease.Immunological markers:The diagnostic hallmark of PBC is the presence of AMA,which are detected in serum of more than 90%of affected individuals;the spec-ificity of AMA in PBC is greater than 95%[8].AMA reactivity is classically studied byimmunofluorescenceFig.1.Diagnostic approach to cholestasis in adult patients.Abbreviations:US,ultrasound;CT,computed tomography;AMA,antimitochondrial antibodies;ANA,antinuclear antibodies;MRCP,magnetic resonance cholangiopancreatography;ERCP,endoscopic retrograde cholangiopancreatog-raphy;PBC,primary biliary cirrhosis;SC,sclerosing cholangitis.European Association for the Study of the Liver /Journal of Hepatology 51(2009)237–267241and considered positive at a titre P1/40[9].The identifi-cation of the molecular mitochondrial target antigens has allowed the setting up of immunoenzymatic assays with recombinant proteins that raise the sensitivity and specificity of the test.If available,anti-AMA-M2(anti-PDC-E2)may be a useful alternative.Non-specific anti-nuclear antibodies(ANA)are found in at least30%of PBC sera.However,ANA directed against nuclear body or envelope proteins such as anti-Sp100and anti-gp210 which present as multiple[6–12]nuclear dots and perinu-clear rims,respectively,at indirect immunofluorescence staining show a high specificity for PBC(>95%)and can be used as markers of PBC when AMA are absent. Their sensitivity,however,is low.3.1.2.HistologyA liver biopsy is no longer regarded as mandatory to make a diagnosis of PBC in patients with a cholestatic serum enzyme pattern and serum AMA.It may,how-ever,be useful for assessment of the activity and staging of the disease.Histological staging of PBC(stages1–4) has been proposed by Ludwig et al.[10]and Scheuer [11]according to the degree of bile duct damage,inflam-mation andfibrosis.Focal duct obliteration with granu-loma formation has been termed theflorid duct lesion, and is judged almost pathognomonic for PBC when present.The liver is not uniformly involved,and features of all four stages of PBC can co-exist simultaneously in a single biopsy.The most advanced histological features should be used for histological staging.3.1.3.ImagingAbdominal ultrasound examination is indicated in all patients with elevation of serum AP and c GT to disclose intrahepatic or extrahepatic bile duct dilatation(see above)or focal liver lesions.There are no specific fea-tures of PBC on ultrasound;in particular the biliary tree appears normal.Ultrasoundfindings in advanced PBC resemble those seen in other forms of cirrhosis.Recommendations1.A diagnosis of PBC can be made with confidence inadult patients with otherwise unexplained elevation of AP and presence of AMA(P1:40)and/or AMA type M2.A liver biopsy is not essential for the diagnosis of PBC in these patients,but allows activity and stage of the disease to be assessed (III/A1).2.A liver biopsy is needed for the diagnosis of PBC inthe absence of PBC specific antibodies.A liver biopsy may also be helpful in the presence of disproportion-ally elevated serum transaminases and/or serum IgG levels to identify additional or alternative processes (III/C1).3.AMA-positive individuals with normal serum livertests should be followed with annual reassessment of biochemical markers of cholestasis(III/C2).3.2.Treatment of PBC3.2.1.Ursodeoxycholic acid(UDCA)Over the past two decades,increasing evidence has accumulated indicating that ursodeoxycholic acid (UDCA;13–15mg/kg/d)is the treatment of choice for patients with PBC based on placebo-controlled trials and more recent long-term case-control studies.UDCA has been demonstrated to exert anticholestatic effects in various cholestatic disorders.Several potential mecha-nisms and sites of action of UDCA have been unraveled in clinical and experimental studies which might explain its beneficial effects.Their relative contribution to the anticholestatic action of UDCA might depend on the type of the cholestatic injury.In early-stage PBC,pro-tection of injured cholangiocytes against the toxic effects of bile acids might prevail,and stimulation of impaired hepatocellular secretion by mainly posttranscriptional mechanisms including stimulation of synthesis,targeting and apical membrane insertion of key transporters might be relevant in more advanced cholestasis[12].In addition,stimulation of ductular alkaline choleresis and inhibition of bile acid-induced hepatocyte and cho-langiocyte apoptosis can have a certain role for the ben-eficial effect of UDCA in PBC[12].UDCA has been demonstrated to markedly decrease serum bilirubin,AP,c GT,cholesterol and immunoglob-ulin M levels,and to ameliorate histological features in patients with PBC in comparison to placebo treatment [13–17]although no significant effects on fatigue or pru-ritus were observed in these large trials.Moreover,long-term treatment with UDCA delayed the histological progression of the disease in patients in whom treatment was started at an early stage[17,18].Still,a clear-cut beneficial effect of UDCA on survival has not been shown in any of the studies mentioned above,probably due to the limited number of patients and the limited observation periods too short for a slowly progressing disease.A beneficial effect of UDCA on survival has only been demonstrated in a combined analysis of the raw data from the French,Canadian and Mayo cohorts followed up for4years[19].In this analysis,UDCA treatment was associated with a significant reduction in the likelihood of liver transplantation or death.This benefit was seen in patients with moderate and severe disease but not in those with mild disease(serum biliru-bin concentration<1.4mg/dL(24l mol/L),stage I or II histologic change)in whom progression to end-stage disease did not occur during the4-year period of obser-vation[19].The affirmative results on survival have been chal-lenged by meta-analyses which included a majority of242European Association for the Study of the Liver/Journal of Hepatology51(2009)237–267studies of up to two years’duration and trials using UDCA doses which are today known to be ineffective [20,21].Inclusion of trials which have a duration of three months to two years for a disease with an estimated duration of one to two decades without intervention may be suited to analyze biochemical effects of medical treatment,but certainly carries a risk to dilute the infor-mation needed for a well-based survival analysis.There-fore,it was not surprising that meta-analyses which excluded studies of short duration(less than24months) and those that used an ineffective dose of UDCA(less than10mg/kg/d)concluded that long-term UDCA sig-nificantly improved transplant-free survival and delayed histologic progression in early-stage patients[22,23].Recent reports have demonstrated the favorable effects of UDCA on long-term survival in patients with PBC receiving standard doses(13–15mg/kg/d)[24]over10–20years.Treatment with UDCA led to a transplant-free survival similar to that of a healthy control population matched for age and gender in patients with early-stage disease[25,26]and to improved survival in comparison to the estimated survival at the start of treatment as calcu-lated by the Mayo risk score for PBC[25–27].Interest-ingly,a‘‘good biochemical response”to UDCA defined as a decrease in AP>40%of pretreatment levels or nor-malization at one year(‘‘Barcelona criteria”)was associ-ated with an excellent95%transplant-free survival at14 years of follow-up,similar to that predicted for the stan-dardized population[27].The prognostic impact of the ‘‘Barcelona criteria”was confirmed in a large indepen-dent cohort of PBC patients for which a serum bilirubin 61mg/dL(17l mol/L),AP63ÂULN,and AST62ÂULN(‘‘Paris criteria”)after one year of treatment even better identified those with a good long-term prognosis of a90%(vs.51%)ten year transplant-free survival[28]. Thus,additional therapeutic options for those patients failing to reach a‘‘good biochemical response”under UDCA are warranted.3.2.2.Corticosteroids and other immunosuppressive agentsPrednisolone improved serum liver tests and histolog-ical features,but markedly worsened bone mineral den-sity in patients with PBC[29]prohibiting its long-term use in PBC.In combination with UDCA(10mg/kg/ d),prednisolone(10mg/d,9months)exerted beneficial effects on various features of liver histology in early-stage PBC in comparison to UDCA alone[30].Budesonide in combination with UDCA showed favorable results on biochemical and histological param-eters in early-stage disease[31,32],but not late-stage dis-ease[33,34].Studies with a longer follow-up using the combination of budesonide and UDCA in patients with early-stage disease not adequately responding to UDCA alone are warranted to confirm its safety and its effect on postponing or preventing the need for liver transplanta-tion.Development of portal vein thrombosis probably related to short-term budesonide administration was reported in stage4patients with portal hypertension [34].Thus,budesonide should not be administered to cir-rhotic patients.Other immunosuppressive agents like azathioprine [35],cyclosporine A[36],methotrexate[37–39],chloram-bucil[40]and mycophenolate mofetil[41]proved to be marginally effective,ineffective or potentially harmful during long-term administration and cannot be recom-mended for standard treatment in PBC.3.2.3.Anti-fibrotic agentsColchicine was inferior to UDCA in the treatment of PBC[42]and did not,when combined with UDCA in comparison to UDCA alone[43],significantly improve symptoms,serum liver tests,serum markers offibrosis, or histological features.Thus,addition of colchicine to UDCA currently cannot be recommended in the treat-ment of PBC.D-Penicillamine is not effective in PBC and can be associated with severe side effects[44,45].3.2.4.Other drugsMalotilate[46],thalidomide[47],silymarin[48]and atorvastatin[49]were not effective in the treatment of PBC.Sulindac[50]and the peroxisome proliferator-acti-vated receptor a(PPAR a)agonist,bezafibrate[51] improved some serum liver tests in limited groups of patients with an incomplete response to UDCA,and bezafibrate deserves further studies.Tamoxifen[52] decreased AP levels in two women who were taking it after surgery for breast cancer.Antiretroviral strategies have also been tested in PBC:Lamivudine alone or in combination with zidovu-dine(Combivir)was associated with minor clinical and biochemical effbivir was also associated with improvement of some histological features,but thisfind-ing needs confirmation in randomized studies[53].3.2.5.Liver transplantationLiver transplantation has dramatically improved sur-vival in patients with late-stage PBC.Indications are not different from those of patients with other etiologies of liver failure[54]:decompensated cirrhosis with an unac-ceptable quality of life or anticipated death within a year due to treatment-resistant ascites and spontaneous bacterial peritonitis,recurrent variceal bleeding,enceph-alopathy or hepatocellular carcinoma.Severe,treat-ment-resistant pruritus may merit consideration for transplantation.Patients should be referred to a liver transplant center for assessment when their bilirubin approaches6mg/dL(103l mol/L),the Mayo risk score is P7,8,and the MELD score is>12at the latest.Survival rates above90%and80–85%at one andfive years,respectively,have been reported by many centersEuropean Association for the Study of the Liver/Journal of Hepatology51(2009)237–267243。