肺炎克雷伯菌研究进展
儿童耐药肺炎克雷伯杆菌研究进展

儿童耐药肺炎克雷伯杆菌研究进展1. 引言1.1 儿童耐药肺炎克雷伯杆菌研究进展概述儿童耐药肺炎克雷伯杆菌是近年来临床上越来越严重的问题,其治疗变得愈发困难。
随着抗生素的过度使用和滥用,这些细菌对药物的耐药性逐渐增加,给儿童健康带来了巨大的威胁。
对儿童耐药肺炎克雷伯杆菌的研究变得尤为重要。
本文将首先介绍耐药肺炎克雷伯杆菌的研究现状,包括该菌株在临床上的表现和对各种抗生素的耐药情况。
将探讨儿童耐药肺炎的流行病学特点,包括发病率和传播途径等方面。
然后,将深入研究耐药肺炎克雷伯杆菌的致病机制,从分子水平解析该菌菌株的病理生理特点。
接着,将探讨目前治疗儿童耐药肺炎克雷伯杆菌的现状,包括常用的抗生素和联合用药的策略。
将提出预防儿童耐药肺炎克雷伯杆菌的策略,包括加强卫生监管和提倡合理使用抗生素等措施。
通过本文的探讨,希望能够深入了解儿童耐药肺炎克雷伯杆菌的研究进展,为临床治疗提供更加科学的依据,为未来的研究提供新的思路和方法。
2. 正文2.1 耐药肺炎克雷伯杆菌的研究现状耐药肺炎克雷伯杆菌(Acinetobacter baumannii)是目前临床上常见的一种耐药细菌,在医院感染中占据较大比例。
随着抗生素的滥用和过度使用,耐药肺炎克雷伯杆菌的研究也变得愈发重要。
1. 耐药性机制研究:研究人员通过分析耐药肺炎克雷伯杆菌的基因组,探究其耐药性的机制,包括多药耐药的相关基因、耐药突变等。
这有助于深入了解该菌株的抗药性并制定更有效的治疗策略。
2. 流行病学调查:针对不同地区、不同医院及患者群体进行耐药肺炎克雷伯杆菌的流行病学调查,找出其传播途径、耐药性变化趋势,并及时采取干预措施。
3. 抗菌药物的研发:针对耐药肺炎克雷伯杆菌的特点,寻找新型抗菌药物或组合疗法,以应对其耐药性的挑战。
通过以上研究进展,我们不仅能更深入了解耐药肺炎克雷伯杆菌的特点和致病机制,也为未来治疗和预防该细菌感染提供了更为全面的参考和指导。
希望未来能有更多针对耐药肺炎克雷伯杆菌的研究取得突破,为临床诊疗提供更多有效的手段。
儿童耐药肺炎克雷伯杆菌研究进展
儿童耐药肺炎克雷伯杆菌研究进展引言:肺炎克雷伯杆菌(Pseudomonas aeruginosa)是一种常见的耐药细菌,它在医院感染和治疗中造成了许多问题。
而在儿童中感染的耐药肺炎克雷伯杆菌尤为令人担忧,因为儿童的免疫系统尚未完全发育,抗菌药物的选择也更加有限。
对儿童耐药肺炎克雷伯杆菌的研究进展至关重要,可以为临床治疗提供更为有效的策略和方案。
近年来,针对儿童耐药肺炎克雷伯杆菌的研究取得了一些重要进展,下面将对相关研究进行简要介绍和总结。
一、耐药机制的研究耐药肺炎克雷伯杆菌对抗菌药物的耐药性主要来源于其多重耐药机制。
研究人员通过分析这些机制,希望找到有效的途径来克服这些耐药性。
近期的研究发现,儿童耐药肺炎克雷伯杆菌的耐药机制与成人可能有所不同,这为针对儿童感染的治疗提供了新的视角。
通过对儿童耐药肺炎克雷伯杆菌的耐药机制进行深入研究,可以为研发新型抗菌药物提供更为有效的方向。
二、治疗策略的优化针对儿童耐药肺炎克雷伯杆菌的治疗策略一直是研究的热点之一。
近年来,有许多新的临床试验和研究致力于寻找更为有效的治疗策略。
联合用药治疗、靶向治疗和免疫治疗等都成为研究的焦点。
而一些新型抗菌药物的研发也为治疗提供了新的选择。
通过对治疗策略的优化,可以为儿童耐药肺炎克雷伯杆菌的治疗提供更为有效的手段。
三、感染控制的研究除了治疗策略的优化,感染控制也是重要的研究方向之一。
通过研究感染源的识别和传播途径,可以有效地减少儿童耐药肺炎克雷伯杆菌的传播和感染。
针对感染控制策略的研究也在不断深入,寻找更为有效的控制措施和手段,以降低儿童的感染风险。
结语:随着对儿童耐药肺炎克雷伯杆菌研究的深入,我们对其治疗和控制的策略也有了更为清晰的认识。
这只是一个开端,仍需要更多的研究和实践来进一步完善这些策略。
我们相信,在不久的将来,对儿童耐药肺炎克雷伯杆菌的研究会取得更多的突破,为儿童的健康提供更为有效的保障。
肺炎克雷伯菌耐药基因近年国内研究进展
KPN中同时携带多种B.内酰胺酶基 因十分常见。国内报道的同时携带多种B .内酰胺酶丛因的有昆uJJ(3种)、深圳与南 京(4种),常州(6种)。国内KPN完整p 内酰胺酶基凶系统研究报道仍鲜见。
和新的氨基糖苷类修饰酶基因aac(6’)一b— Suzhou型。后来黄支密等又从阴沟肠 杆菌中查出aac(6。)一b.Suzhou型。
5耐药基因载体
耐药基因载体都是可移动的遗传元 件(mobile genetic elements),包括质粒、 转座子、整合子。近年来,国外大量文献 报道质粒、转座子和整合子可介导各种 耐药基因。获得质粒、转座予和整合子 的细菌可表现为多重耐药。
质粒是染色体DNA之外的DNA 分子,多数情况下为环状圆形。F质粒, 又称致育因子(fertility factor)。它含有 的traA基因可编码性毛,是细菌接合 (conjugation)关键部件.F质粒接合型质 粒。traA越凶为F质粒的边f擘标记。
收稿日期:2008.09.1l (责任编辑:孙海儿)
医学文稿中缩略语使用须知
·编读往来·
文题一般不使用缩略语,正文内也尽量不用。必须使Jf】绵略.i籍时,于首次fIj现}Jj先叙述中文,然后括号注出英文全称及 其缩略语,后两者用“。”分开,如该缩略语已公知,也可不注出j£英文全称。缩略语不宜移行。
(本刊编辑部)
万方数据
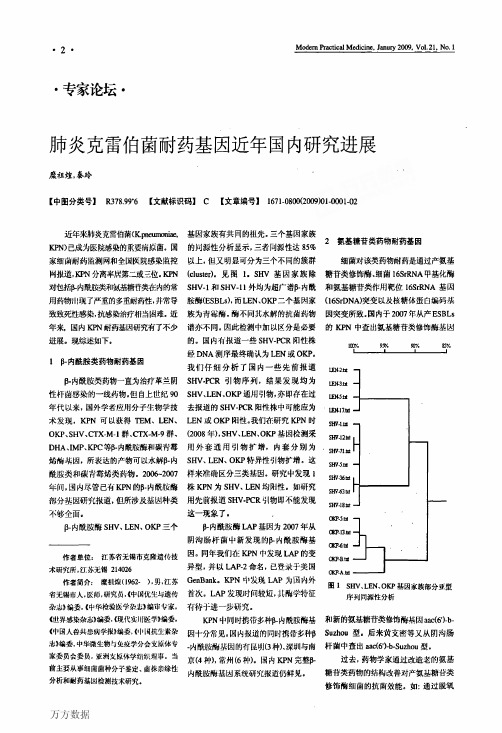
饰作用的新氨基精苷类修饰酶aac(6')- I b.Cr型;还发现了能使喹诺酮类药物 外排的qepA基因。但国内尚缺乏关于 KPN上述基因系统的研究报道。
4广谱抗菌药物耐药基因
四环素、氯霉素、磺胺为广谱抗荫药 物,作为老药已不作为临床一线药物使 用。但上述药物可用作医用敷料,或用 于涂布于进入人体导管的表面,其目的 均为预防感染。在革兰阴性菌中四环 素、氯霉素、磺胺耐药基因分别为tetA/ tetB、catB/emlA、sul、dfrA、dfrB基因。 KPN四环素、氯霉素、磺胺耐药基因研 究尚缺乏。
肺炎克雷伯菌耐药机制研究进展
中华医院感染学杂志2007年第17卷第4期
·479·
酶有从染色体编码向质粒编码转移的趋势。因质粒介导的 AmpC酶多见于无或只有不健全AmpC染色体的细菌种属 中,如克雷伯菌属,所以质粒介导的AmpC酶在克雷伯菌属 耐药机制中日渐重要[5]。
质粒介导的AmpC酶与ESBLs的区别在于后者对青霉 素,如头孢菌素类抗菌药物均耐药,但可以被克拉维酸等争 内酰胺酶抑制剂所抑制,而AmpC酶则B一内酰胺酶抑制剂对 其均无作用,而且质粒型AmpC酶可通过接合、转化、转导等 途径将耐药性传递给其他菌引起的感染发生与流行,当应用 广谱头孢菌素时,还能将突变株筛选出来[5]。所以,近年来, 由此类酶引起的难治性感染日渐突出,已是临床关注的焦 点。但这方面的研究有待于深入。
1耐药现状
近年来,肺炎克雷伯菌的耐药率已显著上升,对四代头 孢菌素B一内酰胺酶抑制剂复合物也呈升高趋势。目前,在西 班牙肺炎克雷伯菌对三代头孢的耐药率为20%,美国肺炎克 雷伯菌对三代头孢的耐药率约占20%,我国克雷伯菌属对三 代头孢的耐药率为29%~47%[1]。
产超广谱B_内酰胺酶(ESBLs)是肺炎克雷伯菌产生耐 药的主要机制。自从1994年第1例SHV-ESBLs在中国报 道以后,在这个国家,ESBLs发生率一直上升。如何治疗产 ESBLs菌已是临床一大治疗难点。在中国ESBLs主要是 CTX_M型,包括CTx_M-3、CTX-M-9、CTX-M-13、CTX-M一 14、CTX-M-18。最近几年,一些新型CTX-M型B一内酰胺酶 也已经报道,包括CTX-M-22、CTX-M-24、CTx_M-29、CTX- M一32,流行的主要原因是三代头孢菌素的广泛应用;另外一 个原因,TOHO-I、CTX-M-2、CTX-M-3、CTx-M一14通过国 际旅游,从邻国(日、韩)传到中国Cz]。
高毒力肺炎克雷伯菌的研究进展
山 东 化 工 收稿日期:2019-09-19基金项目:黑龙江省卫生计生委科研课题(课题编号2018-291);佳木斯大学校长创新创业基金项目(项目编号XZFY2018-43)作者简介:席健峰(1992—),江苏连云港人,在读硕士研究生,从事细菌耐药机制方向的研究,E-mail:1017341923@qq.com;通信作者:王勇,E-mail:15331878255@163.com;邹佳贺,E-mail:447012334@qq.com。
高毒力肺炎克雷伯菌的研究进展席健峰1,刘效伊2,姜良勇1,李 强1,邹佳贺3 ,王 勇1(1.佳木斯大学附属第一医院,黑龙江佳木斯 154003;2.深圳市龙岗区妇幼保健院,广东深圳 518172;3.佳木斯市中心医院,黑龙江佳木斯 154003)摘要:近年来肺炎克雷伯菌逐渐成为仅次于大肠埃希菌引起医院感染的重要病原菌,根据该菌的毒力不同,可将该菌分为高毒力肺炎克雷伯菌和普通肺炎克雷伯菌。
经研究发现,hvKP的毒力因子包括:荚膜多糖,菌毛,脂多糖和铁的摄入。
随着肺炎克雷伯菌碳青霉烯酶KPC、NDM等的水平播,已经出现了碳青霉烯耐药的高毒力肺炎克雷伯菌(cr-hvKP)。
本文将对hvKP的相关毒力基因及耐药相关情况作具体介绍。
关键词:肺炎克雷伯菌;毒力因子;耐药中图分类号:R446.5 文献标识码:A 文章编号:1008-021X(2019)24-0054-03ResearchProgressonHighlyVirulentKlebsiellaPneumoniaeXiJianfeng1,LiuXiaoyi2,JiangLiangyong1,LiQiang1,ZouJiahe3 ,WangYong1(1.FirstAffiliatedHospitalofJiamusiUniversity,Jiamusi 154003,China;2.LonggangDistrictMaternalandChildHealthHospital,Shenzhen 518172,China;3.JiamusiCentralHospital,Jiamusi 154003,China)Abstract:Inrecentyears,KlebsiellapneumoniaehasbecomeanimportantpathogenafterhospitalinfectioncausedbyEscherichiacoli.Accordingtothevirulenceofthebacteria,thebacteriacanbedividedintohighlytoxicKlebsiellapneumoniaeandCommonKlebsiellapneumoniae.StudieshavefoundthatthevirulencefactorsofhvKPinclude:capsularpolysaccharide,pili,lipopolysaccharideandironintake.WiththehorizontalsowingofK.pneumoniaecarbapenemaseKPC,NDM,etc.carbapenem-resistantandhighlyvirulentKlebsiellapneumoniae(cr-hvKP)hasemerged.ThisarticlewillintroducetherelatedvirulencegenesanddrugresistancerelatedtohvKP.Keywords:klebsiellapneumoniae;virulencefactor;drugresistance 肺炎克雷伯菌(KP)是一种极为常见的病原菌,它属于肠杆菌科克雷伯氏菌属,其所导致的疾病在克雷伯氏菌属中居于首位。
肺炎克雷伯菌疫苗研究进展
灭活病原微生物,然后以灭活的病原菌诱导机体免 疫 应 答,
从而达到预防感染的目 的。IWC 由 于 病 原 菌 本 身 的 部 分 结
构的内毒性及安全性问 题, 目 前 尚 未 运 用 于 临 床。2013 年
Sun 等
制备了 KP 灭 活 全 菌 疫 苗, 但 研 究 发 现 KP 携 带
[
11]
重基础疾病及免疫功 能 低 下 患 者 其 更 易 罹 患 该 病 原 菌 感 染
行病学研究显示:KP 分离株对氨曲南和头孢他啶的耐药率
包括产 β
-内酰胺 酶、 氨 基 糖 苷 钝 化 酶、 染 色 体 变 异、 质 粒
及整合子介导、外 膜 孔 蛋 白 缺 失、 靶 位 改 变、 生 物 膜 形 成
分别达到了55 4% 和55 7% [7]。KP 的 耐 药 机 制 复 杂 多 样,
主要引起社区获 得 性 肝 脓 肿、 脑 膜 炎、 重 症 肺 炎、 眼 内 炎
及机制尚不清楚,尚有待人们去探索研究。
如所周知,KP 可引起多种感染,如肺部感染、尿路感
染、腹腔感染、手术 部 位 感 染 甚 至 血 流 感 染 等, 而 在 有 严
41
KP 细 胞 毒 素 (Kl
ebs
i
e
l
l
a cy
t
o
t
ox
i
ns, KCTs)
的s
i
tA 蛋白对细胞存在明显 的 毒 性 作 用,s
i
tA 是 在 肠 杆 菌
KCTs是致病 KP 的重要毒力因子,在宿主应激状态下表达
节转运蛋白基因,其 表 达 水 平 随 着 细 菌 培 养 条 件 的 变 化 而
KP 免疫,从 而 达 到 预 防 或 控 制 KP 感 染 的 目 的。 本 文 就
肺炎克雷伯菌耐药基因近年国内研究进展
DH I 、 C等D内酰胺酶和碳 肯霉 刚 外 套 通 用 引 物 扩 增 , 内 套 分 别 为 A、MP KP 一
烯 陷丛 囚 ,所 表 达 的产 物 可 以水 8内 S 一 HV、 E O L N、 KP特异性引物扩J 。这 f _ ! } 酰 胺 类 和 碳 青 霉 烯 类 药 物 。2 0 ~ 0 7 样 来 准 确 区分 三 类 基 。研 究 发现 1 0 6 2 0 N HV、 E 均 性 。如 研 究 LN " f, 内尽 管 已有 K N 的B内酰 胺 牌 株 KP 为 S l O囡 q P 一
川药物 L现 了严 重 的多重 耐药 - 常 导 胺 酶 ( S L )而 L N、 P二个 基 因家 (6 r NA) l 5 H, : 并 E B s, E OK 1SD 突变 以及核糖体蛋 白编码
致致死性感染 , 抗感染治疗 当困难。近 族 为 青 霉 酶 。 不 同其 水解 的抗 菌 药 物 因突 变 所 致 。 酶 国内 于 2 0 年 从 产 E B s 07 S L
・
2 ・
M o e nP a tc l e iie a uy 2 0 Vo . 1 No. d r rcia dcn ,J n r 0 9, 12 , M 1
・
专家论坛 ・
肺炎克雷伯菌耐药基 因近年 国内研 究进展
糜祖 煌, 秦玲
【 中图 分 类 号 】 R 7 . 【 献 标 识 码 】 C 【 章 编 号 】 17 —8 02 0 )10 0 —2 3 8 96 9 文 文 6 100 (0 90 —0 10
《』 I界感染杂志》 』 = 编委,现代实川医学》 《 编委, 《i ・ 幽人兽共忠病学报》 一 编委, 《…司抗生岽杂 志》 编委 ,
2023肺炎克雷伯菌多黏菌素耐药机制的研究进展
2023肺炎克雷伯菌多黏菌素耐药机制的研究进展近年来,碳青霉烯耐药肺炎克雷伯菌临床分离率不断增加,导致多黏菌素成为治疗多重耐药肺炎克雷伯菌感染的重要防线,但随着多黏菌素的使用增多,其耐药率也逐渐升高。
肺炎克雷伯菌多黏菌素耐药机制多种多样,以外膜修饰脂多糖为主。
参与这一过程的基因除位于染色体上的双组份系统夕万。
々2、PmrAB、b"18及负性调控跨膜蛋白∕77gM基因外,质粒携带的移动性多黏菌素耐药基因力”也能介导外膜修饰。
其中,mg加基因变异对多黏菌素耐药起关键作用。
本文主要阐述肺炎克雷伯菌多黏菌素耐药机制,以更好遏制肺炎克雷伯菌多黏菌素耐药发生。
肺炎克雷伯菌属肠杆菌目,在人类细菌性感染的病原体中居于前3位【1】。
中国细菌耐药监测网显示2023年1—12月临床分离株中肺炎克雷伯菌对美罗培南及亚胺培南耐药率分别为24.2%和22.6%β碳青霉炸酶,如肺炎克雷伯菌碳青霉烯酶(K1ebsie11apneumoniae Carbapenemase,KPC)、新德里金属B内酰胺酶(NewDe1himeta11o-β-1actamase,NDM)、OXA-48等播散使得碳青霉焙类抗菌药物无法用于治疗碳青霉烯类耐药肺炎克雷伯菌(Carbapenemresistant K1ebsie11apneumoniae,CRKP)o新型B内酰胺类抑制剂的抗菌药物如头抱他D定/阿维巴坦对于产NDM的CRKP无效,产KPC-2的CRKP感染在使用头抱他咤/阿维巴坦治疗的过程中可因KPC-2变异致治疗失败,多黏菌素可作为治疗CRKP的最后手段【2】,但随着多黏菌素在临床使用增加,耐药率明显升高【21。
2019年一项较为全面的数据统计发现,临床分离肺炎克雷伯菌多黏菌素耐药率分别为4.0%(亚洲)、3.5%(南美洲)、3.2%(欧洲)、2.4%(非洲)、0.8%(北美洲)。
其中,亚洲较2014—2018年有明显的增长趋势[3〕。
肺炎克雷伯菌抗生素耐药性的研究进展
文章编号:1001-8689(2020)06-0540-05肺炎克雷伯菌抗生素耐药性的研究进展罗可人 唐军(四川大学华西第二医院儿科/出生缺陷与相关妇儿疾病教育部重点实验室,成都 610041)摘要:肺炎克雷伯菌的耐药问题日益严重,给临床治疗带来了严峻挑战。
本文总结了近年来的相关研究,阐述了肺炎克雷伯菌对多种抗生素的耐药机制及分子特征,以及肺炎克雷伯菌耐药性与毒力之间可能存在的联系,希望能给临床实践带来新视角和新选择。
关键词:肺炎克雷伯菌;耐药;毒力中图分类号:R978.1 文献标志码:A Progress in antibiotic resistance of Klebsiella pneumoniaeLuo Ke-ren and Tang Jun(Department of Pediatrics, West China Second University Hospital, Key Laboratory of Birth Defects and Related Diseases of Women andChildren (Sichuan University), Ministry of Education, Chengdu 610041)Abstract The resistance of Klebsiella pneumoniae is becoming more and more serious, which brings severe challenges to clinical treatment. This article summarizes related research in recent years, and elaborates the resistance mechanism, molecular characteristics of Klebsiella pneumoniae to various antibiotics, and the possible relationship between Klebsiella pneumoniae resistance and virulence with the hope to bring clinical practice new perspectives and new choices.Key words Klebsiella pneumoniae ; Drug resistance; Virulence收稿日期:2019-12-13作者简介:罗可人,女,生于1994年,在读博士研究生,主要从事新生儿相关研究,E-mail:********************通讯作者,E-mail:******************。
儿童耐药肺炎克雷伯杆菌研究进展
儿童耐药肺炎克雷伯杆菌研究进展儿童耐药肺炎克雷伯杆菌(MDR-AB)是目前临床上越来越常见的一种耐药菌株,它对多种抗生素表现出抗药性,给临床治疗带来了挑战。
在过去的几年里,针对儿童耐药肺炎克雷伯杆菌的研究取得了一些进展,主要集中在病因、流行病学特征和治疗方案等方面。
关于儿童耐药肺炎克雷伯杆菌的病因研究表明,MDR-AB感染主要通过呼吸道传播,而机械通气、住院时间延长、免疫抑制等因素是感染的危险因素。
一些研究还发现儿童耐药肺炎克雷伯杆菌感染与其他医院获得性感染的共同因素存在一定的相关性,提示了交叉感染和传播的可能性。
针对儿童耐药肺炎克雷伯杆菌的流行病学特征研究发现,MDR-AB的流行趋势呈逐渐增长的趋势,且呈现出多样性和多样化。
不同地区和医疗机构间的流行菌株差异较大,这可能与不同地区的使用抗菌药物方针、感染控制措施和病人流行状况等有关。
儿童耐药肺炎克雷伯杆菌的流行病学特征也与不同基因型的菌株相关,一些基因型与高耐药性的MDR-AB 菌株相关联。
关于儿童耐药肺炎克雷伯杆菌的治疗方案研究主要集中在药物疗法和预防控制措施上。
药物疗法方面,学者们发现仅使用单一抗生素治疗儿童耐药肺炎克雷伯杆菌感染的疗效不佳,而联合应用抗生素或采用其他治疗方案,如药物切换或静脉用药,可能会提高治疗效果。
预防控制措施方面,一些研究表明,MDR-AB的感染控制需要综合性的策略,包括严格执行手卫生、合理使用抗生素、加强环境清洁、加强感染控制培训和教育等。
儿童耐药肺炎克雷伯杆菌的研究进展为我们提供了更好地了解和应对这一问题的方法和策略。
目前的研究还远远不够,我们需要继续深入研究相关的病因机制、流行病学特征和治疗方案,以便更有效地预防和控制这一感染的传播。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
J OURNAL OF C LINICAL M ICROBIOLOGY,Aug.2007,p.2723–2725Vol.45,No.8 0095-1137/07/$08.00ϩ0doi:10.1128/JCM.00015-07Evaluation of Methods To Identify the Klebsiella pneumoniaeCarbapenemase in EnterobacteriaceaeᰔK.F.Anderson,*D.R.Lonsway,J.K.Rasheed,J.Biddle,B.Jensen,L.K.McDougal,R.B.Carey,A.Thompson,S.Stocker,B.Limbago,and J.B.PatelCenters for Disease Control and Prevention,Division of Healthcare Quality Promotion,Atlanta,GeorgiaReceived3January2007/Returned for modification13February2007/Accepted6June2007The Klebsiella pneumoniae carbapenem(KPC)-lactamase occurs in Enterobacteriaceae and can conferresistance to all-lactam agents including carbapenems.The enzyme may confer low-level carbapenemresistance,and the failure of susceptibility methods to identify this resistance has been reported.Automatedand nonautomated methods for carbapenem susceptibility were evaluated for identification of KPC-mediatedresistance.Ertapenem was a more sensitive indicator of KPC resistance than meropenem and imipenemindependently of the method used.Carbapenemase production could be confirmed with the modified Hodgetest.Carbapenems are commonly used to treat infections caused by multidrug-resistant Enterobacteriaceae.In the United States and other locations,an increasingly common mechanism of carbapenem resistance is the Klebsiella pneumoniae carbapen-emase(KPC)(2,10,15,18,19,24,26,27).The KPC-lacta-mase occurs most commonly in K.pneumonia e,but it has also been reported sporadically in other species of Enterobacteria-ceae(Klebsiella oxytoca,Enterobacter spp.,Escherichia coli,Sal-monella spp.,Citrobacter freundii,and Serratia spp.)and Pseudomonas aeruginosa(4,10–12,17,23,28).The KPC en-zyme confers resistance to all-lactam agents including peni-cillins,cephalosporins,monobactams,and carbapenems(1,21, 27,28).Some isolates containing KPC demonstrate low-level carbapenem resistance,but when combined with other cellular changes,such as porin loss,the carbapenem MIC increases (21,26).The gene encoding the KPC enzyme is usuallyflanked by transposon-related sequences and has been identified on conjugative plasmids;therefore,the potential for dissemina-tion is significant(17,26–28).Several outbreaks of KPC-pro-ducing bacteria have occurred in the northeast United States (2,26).Isolates that acquired this enzyme are usually resistant to several other classes of antimicrobial agents used as treat-ment boratory identification of KPC-producing clinical isolates will be critical for limiting the spread of this resistance mechanism.The failure of automated susceptibility testing systems to detect KPC-mediated resistance was previ-ously noted(5,22).We evaluated commonly used susceptibility testing methods to identify the most sensitive conditions for KPC detection with31 KPC-producing Enterobacteriaceae isolates(25of K.pneumoniae, 2of K.oxytoca,1of E.coli,1of Enterobacter spp.,1of Citrobacter freundii,and1of Salmonella spp.).These were isolated from different patients who were hospitalized in13different healthcare institutions from seven different states:Maryland(one),NewJersey(two),New York(four),Pennsylvania(two),Michigan (two),Missouri(one),and North Carolina(one).The presence of blaKPCwas determined using previously described oligonucleo-tide primers and cycling conditions(27).Enzyme activity was demonstrated in all isolates by isoelectric focusing(6,16).To measure the specificity of methods to detect KPC-medi-ated resistance,45isolates(26of K.pneumoniae,9of K.oxy-toca,and10of E.coli)were chosen for testing.All45isolateswere negative for blaKPCby PCR.These isolates were submit-ted to the CDC for reference susceptibility ing the reference broth microdilution(BMD)method,all isolates met the CLSI extended-spectrum-lactamase(ESBL)screening test criteria;that is,they demonstrated reduced susceptibility to at least one extended-spectrum cephalosporin(7,8).Twenty-six isolates were positive by the CLSI ESBL broth confirmatory test, and the other isolates were presumed to have another broad-spectrum-lactamase or other mechanism of cephalosporin resistance.Five isolates were nonsusceptible to a carbapenem (imipenem,meropenem,or ertapenem)by BMD.Since two of the isolates were ESBL producers by BMD and the other three isolates produced an AmpC-type enzyme as demonstrated by isoelectric focusing and PCR(20),it is likely that the mechanism of reduced carbapenem susceptibility is a combination of a cepha-loporinase and porin loss(3,9,13).Meropenem,imipenem,and ertapenem susceptibilities were determined by BMD using cation-adjusted Mueller-Hinton broth in panels that were prepared in-house(7),disk diffusion(Becton Dickinson,Sparks,MD)(8),Etest(AB Biodisk,Piscataway,NJ), Microscan Autoscan using the NM32panel(Dade Behring,West Sacramento,CA),and the Vitek2test using the AST GN14card (bioMe´rieux,Durham,NC).Susceptibility testing of meropenem and imipenem was performed with the Phoenix test using the NEG MIC30panel or NEG MIC112panel(Becton Dickinson, Sparks,MD),the Vitek Legacy test using the GNS-122and GNS-127panels(bioMe´rieux,Durham,NC),and the Sensititre Auto Reader using the GN2F panel(Trek Diagnostics,West Lake, OH).All methods were performed according to the manufactur-ers’recommendations.Quality control testing of susceptibility*Corresponding author.Mailing address:Centers for Disease Con-trol and Prevention,Mail Stop G-08,1600Clifton Road NE,Atlanta,GA30333.Phone:(404)639-2824.Fax:(404)639-1381.E-mail:ebi2@.ᰔPublished ahead of print on20June2007.2723 on August 19, 2015 by guest / Downloaded fromtesting methods was performed with Escherichia coli ATCC 25922and Pseudomonas aeruginosa ATCC 27853.Two criteria were evaluated for detection of KPC-mediated resistance:(i)an inter-mediate or resistant susceptibility to a carbapenem or (ii)a car-bapenem MIC of Ͼ1g/ml (see Table 1).Overall,reference BMD was the most sensitive method for the identification of KPC-mediated carbapenem resistance (Table 1).An interpretation of intermediacy or resistance for any of the three carbapenems tested (meropenem,imipenem,and ertapenem)demonstrated greater than 90%sensitivity.For disk diffusion,Etest,Vitek 2,and MicroScan greater than 90%sensitivity was achieved only when ertapenem was tested.When interpreting the results for the disk diffusion test and the Etest,it was important to recognize the presence of small colonies growing inside the zone of inhibition.Meropenem and imipenem susceptibility demonstrated poor sensitivity for methods other than BMD.However,the specificity of mero-penem and imipenem susceptibility testing was higher than that for ertapenem susceptibility testing regardless of test method.For nearly all methods (i.e.,those demonstrating a specificity of Ն89%),the specificity errors occurred with one or more of the five isolates that were nonsusceptible to carbap-enem by a mechanism other than carbapenemase production.It is important that these are not specificity errors in measuring carbapenem susceptibility but rather errors in the detection of carbapenemase production.Using the criterion of a carbapenem MIC of Ͼ1g/ml,the sensitivity of detecting KPC-mediated resistance increased for ertapenem,meropenem,and imipenem with only small changes in specificity.Meropenem susceptibility testing dem-onstrated greater than 90%sensitivity by BMD and MicroScan whereas imipenem susceptibility testing was at least 90%sen-sitive by BMD,Etest,Vitek 2,and MicroScan.The modified Hodge test (Fig.1)was also evaluated for detection of KPC-mediated resistance (14).This is a pheno-typic test which could be used to determine if reduced suscep-tibility to carbapenems is mediated by a carbapenemase.The test was performed as described by Lee et al.(14),and it demonstrated 100%sensitivity and specificity for detection of KPC activity.We tested a limited number of isolates in this study.Theactual sensitivity and specificity of these methods in any given laboratory will depend upon the prevalent mechanisms of -lactam resistance in the laboratory’s patient population.Considering the potential clinical impact of carbapenemase-producing isolates,laboratories should consider testing for ertapenem susceptibility since it was the most sensitive indica-tor of KPC activity regardless of method.Ertapenem is not available on panels from all manufacturers;laboratories that cannot test ertapenem on their current system may consider using the ertapenem disk diffusion test,which was a sensitiveTABLE 1.Performance of susceptibility testing methods for detecting KPC-mediated resistanceMethodSensitivity (%)/specificity (%)of:Intermediate or resistant susceptibility result aCarbapenem MIC of Ͼ1g/mlMeropenemImipenemErtapenemMeropenemImipenemErtapenemReference BMD 94/9894/9397/89100/93100/93100/89Etest58/9655/9690/8484/9190/89100/84Disk diffusion 71/9642/9697/87NA b NA NA Vitek Legacy 52/9855/96NA d NA c NA c NA d Vitek 248/9671/9694/9371/9394/8994/89MicroScan 84/9874/96100/89100/93100/93NA c Phoenix 61/9881/96NA d 74/9687/93NA d Sensititre42/9829/96NA d 81/96NA c NA da Interpretive criteria were based upon CLSI criteria.bNA,not applicable.cNot applicable because the MIC range tested was not low enough (e.g.,lowest dilution tested was either 2g/ml or 4g/ml)for the identification of a carbapenem MIC of Ͼ1g/ml.dNot applicable because ertapenem was not available on apanel.FIG.1.The modified Hodge test Mueller-Hinton agar plate was inoculated with a 1:10dilution of a 0.5McFarland suspension of E.coli ATCC 25922and streaked for confluent growth using a swab.A 10-g imipenem disk was placed in the center,and each test isolate was streaked from the disk to the edge of the plate.Isolate A is a KPC producer and positive by the modified Hodge test.Isolates B,C,D,and E do not produce a carbapenemase and are negative by the test.2724NOTESJ.C LIN .M ICROBIOL .on August 19, 2015 by guest/Downloaded fromindicator for the presence of the KPC enzyme in this study and a study by Bratu et al.(5).The KPC enzyme also hydrolyzes extended-spectrum cephalosporins;therefore,screening for reduced susceptibility to carbapenems could be limited to iso-lates that are resistant to these cephalosporins (e.g.,ceftazi-dime,ceftriaxone,and cefotaxime).Alternatively,meropenem and imipenem susceptibility could be used to detect KPC-mediated resistance if an elevated but susceptible MIC (MIC of Ͼ1g/ml)is applied.However,it should be noted that this MIC cutoff was applied only to Klebsiella spp.and E.coli in this study.Other species of Enterobacteriaceae have higher wild-type carbapenem MICs (),and so this strategy may not be appropriate.No method demonstrated 100%specificity for carbapene-mase activity.In the United States,where metallo--lactama-ses are uncommon,the most likely alternative mechanism of carbapenem resistance is the combination of an ESBL or AmpC-type enzyme with porin loss (3,9,13).A report by Woodford et al.(25)noted that nonsusceptibility to ertapenem is not specific for carbapenemase production,especially when carbapenemase production is uncommon.Also,the authors noted that for isolates with noncarbapenemase mechanisms,ertapenem resistance does not necessarily predict resistance to other carbapenems.In this study,the modified Hodge test was a useful method for confirming carbapenemase production.Alternatively,a laboratory could confirm the carbapenemase with PCR for the bla KPC gene,which has the added benefit of confirming which enzyme is present.It is important for laboratories to be vigilant about the iden-tification of emerging KPC resistance in their institution.Strat-egies for laboratory identification of this resistance will likely have to be reviewed and adjusted as this mechanism is further investigated.REFERENCES1.Alba,J.,Y.Ishii,K.Thomson,E.S.Moland,and K.Yamaguchi.2005.Kinetics study of KPC-3,a plasmid-encoded class A carbapenem-hydrolyzing -lactamase.Antimicrob.Agents Chemother.49:4760–4762.2.Bradford,P.A.,S.Bratu,C.Urban,M.Visalli,N.Mariano,ndman,J.J.Rahal,S.Brooks,S.Cebular,and J.Quale.2004.Emergence of carbapenem-resistant Klebsiella species possessing the class A carbapenem-hydrolyzing KPC-2and inhibitor-resistant TEM-30-lactamases in New York City.Clin.Infect.Dis.39:55–60.3.Bradford,P.A.,C.Urban,N.Mariano,S.J.Projan,J.J.Rahal,and K.Bush.1997.Imipenem resistance in Klebsiella pneumoniae is associated with the combination of ACT-1,a plasmid-mediated AmpC -lactamase,and the loss of an outer membrane protein.Antimicrob.Agents Chemother.41:563–569.4.Bratu,S.,ndman,M.Alam,E.Tolentino,and J.Quale.2005.Detec-tion of KPC carbapenem-hydrolyzing enzymes in Enterobacter spp.from Brooklyn,New York.Antimicrob.Agents Chemother.49:776–778.5.Bratu,S.,M.Mooty,S.Nichani,ndman,C.Gullans,B.Pettinato,U.Karumudi,P.Tolaney,and J.Quale.2005.Emergence of KPC-possessing Klebsiella pneumoniae in Brooklyn,New York:epidemiology and recommen-dations for detection.Antimicrob.Agents Chemother.49:3018–3020.6.Bush,K.,and S.B.Singer.1989.Effective cooling allows sonication to be used for liberation of -lactamases from gram-negative bacteria.J.Antimi-crob.Chemother.24:82–84.7.Clinical and Laboratory Standards Institute.2006.Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically,7th ed.Approved standard M7-A7.Clinical and Laboratory Standards Institute,Wayne,PA.8.Clinical and Laboratory Standards Institute.2006.Performance standards for antimicrobial disk susceptibility tests,9th ed.Approved standard M2-A9.Clinical and Laboratory Standards Institute,Wayne,PA.9.Crowley,B.,V.J.Benedi,and A.Domenech-Sanchez.2002.Expression ofSHV-2-lactamase and of reduced amounts of OmpK36porin in Klebsiella pneumoniae results in increased resistance to cephalosporins and carbapen-ems.Antimicrob.Agents Chemother.46:3679–3682.10.Deshpande,L.M.,P.R.Rhomberg,H.S.Sader,and R.N.Jones.2006.Emergence of serine carbapenemases (KPC and SME)among clinical strains of Enterobacteriaceae isolated in the United States medical centers:report from the MYSTIC program (1999–2005).Diagn.Microbiol.Infect.Dis.56:367–372.11.Hong,T.,E.S.Moland,B.Abdalhamid,N.D.Hanson,J.Wang,C.Sloan,D.Fabian,A.Farajallah,J.Levine,and K.S.Thomson.2005.Escherichia coli :development of carbapenem resistance during therapy.Clin.Infect.Dis.40:e84–e86.12.Hossain,A.,M.J.Ferraro,R.M.Pino,R.B.Dew III,E.S.Moland,T.J.Lockhart,K.S.Thomson,R.V.Goering,and N.D.Hanson.2004.Plasmid-mediated carbapenem-hydrolyzing enzyme KPC-2in an Enterobacter sp.Antimicrob.Agents Chemother.48:4438–4440.13.Kaczmarek,F.M.,F.Dib-Hajj,W.Shang,and T.D.Gootz.2006.High-level carbapenem resistance in a Klebsiella pneumoniae clinical isolate is due to the combination of bla ACT-1-lactamase production,porin OmpK35/36inser-tional inactivation,and down-regulation of the phosphate transport porin PhoE.Antimicrob.Agents Chemother.50:3396–3406.14.Lee,K.,Y.Chong,H.B.Shin,Y.A.Kim,D.Yong,and J.H.Yum.2001.Modified Hodge and EDTA-disk synergy tests to screen metallo--lacta-mase-producing strains of Pseudomonas and Acinetobacter species.Clin.Microbiol.Infect.7:88–91.15.Lomaestro,B.M.,E.H.Tobin,W.Shang,and T.Gootz.2006.The spread of Klebsiella pneumoniae carbapenemase-producing K.pneumoniae to upstate New York.Clin.Infect.Dis.43:e26–e28.16.Matthew,M.,and A.M.Harris.1976.Identification of -lactamases by analytical isoelectric focusing:correlation with bacterial taxonomy.J.Gen.Microbiol.94:55–67.17.Miriagou,V.,L.S.Tzouvelekis,S.Rossiter,E.Tzelepi,F.J.Angulo,and J.M.Whichard.2003.Imipenem resistance in a Salmonella clinical strain due to plasmid-mediated class A carbapenemase KPC-2.Antimicrob.Agents Chemother.47:1297–1300.18.Naas,T.,P.Nordmann,G.Vedel,and C.Poyart.2005.Plasmid-mediated carbapenem-hydrolyzing -lactamase KPC in a Klebsiella pneumoniae isolate from France.Antimicrob.Agents Chemother.49:4423–4424.19.Navon-Venezia,S.,I.Chmelnitsky,A.Leavitt,M.J.Schwaber,D.Schwartz,and Y.Carmeli.2006.Plasmid-mediated imipenem-hydrolyzing enzyme KPC-2among multiple carbapenem-resistant Escherichia coli clones in Is-rael.Antimicrob.Agents Chemother.50:3098–3101.20.Perez-Perez,F.J.,and N.D.Hanson.2002.Detection of plasmid-mediated AmpC -lactamase genes in clinical isolates by using multiplex PCR.J.Clin.Microbiol.40:2153–2162.21.Smith Moland,E.,N.D.Hanson,V.L.Herrera,J.A.Black,T.J.Lockhart,A.Hossain,J.A.Johnson,R.V.Goering,and K.S.Thomson.2003.Plasmid-mediated,carbapenem-hydrolysing -lactamase,KPC-2,in Klebsiella pneu-moniae isolates.J.Antimicrob.Chemother.51:711–714.22.Tenover,F.C.,R.K.Kalsi,P.P.Williams,R.B.Carey,S.Stocker,D.Lonsway,J.K.Rasheed,J.W.Biddle,J.E.McGowan,Jr.,and B.Hanna.2006.Carbapenem resistance in Klebsiella pneumoniae not detected by au-tomated susceptibility testing.Emerg.Infect.Dis.12:1209–1213.23.Villegas,M.V.,K.Lolans,A.Correa,J.N.Kattan,J.A.Lopez,and J.P.Quinn.2007.First identification of Pseudomonas aeruginosa isolates produc-ing a KPC-type carbapenem-hydrolyzing -lactamase.Antimicrob.Agents Chemother.51:1553–1555.24.Villegas,M.V.,K.Lolans,A.Correa,C.J.Suarez,J.A.Lopez,M.Vallejo,and J.P.Quinn.2006.First detection of the plasmid-mediated class A carbapenemase KPC-2in clinical isolates of Klebsiella pneumoniae from South America.Antimicrob.Agents Chemother.50:2880–2882.25.Woodford,N.,J.W.Dallow,R.L.Hill,M.F.Palepou,R.Pike,M.E.Ward,M.Warner,and D.M.Livermore.2007.Ertapenem resistance among Kleb-siella and Enterobacte r submitted in the UK to a reference laboratory.Int.J.Antimicrob.Agents 29:456–459.26.Woodford,N.,P.M.Tierno,Jr.,K.Young,L.Tysall,M.F.Palepou,E.Ward,R.E.Painter,D.F.Suber,D.Shungu,L.L.Silver,K.Inglima,J.Kornblum,and D.M.Livermore.2004.Outbreak of Klebsiella pneumoniae producing a new carbapenem-hydrolyzing class A -lactamase,KPC-3,in a New York medical center.Antimicrob.Agents Chemother.48:4793–4799.27.Yigit,H.,A.M.Queenan,G.J.Anderson,A.Domenech-Sanchez,J.W.Biddle,C.D.Steward,S.Alberti,K.Bush,and F.C.Tenover.2001.Novel carbapenem-hydrolyzing -lactamase,KPC-1,from a carbapenem-resistant strain of Klebsiella pneumoniae .Antimicrob.Agents Chemother.45:1151–1161.28.Yigit,H.,A.M.Queenan,J.K.Rasheed,J.W.Biddle,A.Domenech-Sanchez,S.Alberti,K.Bush,and F.C.Tenover.2003.Carbapenem-resistant strain of Klebsiella oxytoca harboring carbapenem-hydrolyzing -lactamase KPC-2.Antimicrob.Agents Chemother.47:3881–3889.V OL .45,2007NOTES 2725on August 19, 2015 by guest/Downloaded from。