依诺肝素钠说明书翻译
肝素钠使用说明书
肝 素钠 注射液 说 明书
渭仔细阅读说明书并在医师指导下使用 【 药品名称 】 通 用名称 :肝 素钠 注射液 英文 名称 :Heparin Sodium I翊 ectiOn 汉语拼音 :Gansuna Zhuslleye 1成 份】 本 品主要成份为 :肝 素钠 。肝素钠 系 自猪 的肠粘膜或牛肺 中提取精制 的 一 种硫 酸氨基葡聚糖 的钠 盐 。属黏 多糖 类物质 。平均分子量 1200O。 辅料为 :2。 5‰ 苯酚 。 【 性状 1 本 品为无色或淡黄色的澄 明液体 。 1适 应症 1
)、
;
(1)本 品与下列药物合用 ,可 加重出血危险。 ①香豆素及其衍生物 ,可 导致严重的因子 Ⅸ缺乏而致出血 ②阿司匹林及非甾体消炎镇痛药 ,包 括 甲芬那酸 、水杨酸等均能抑制血小板 功能 ,并 能诱发胃肠道溃疡出血 ③双嘧达莫 、右旋糖酐等可能抑制血小板功能 ④肾上腺皮质激素、促肾上腺皮质激素等易诱发胃肠道溃疡出血 ⑤其他尚有利尿酸 、组织纤溶酶原激活物(卜 PA)、 尿激酶 、链激酶等。 (2)肝 素并用碳酸氢钠 、乳酸钠等纠正酸中毒的药物可促进肝素的抗凝作用。 (3)肝 素与透明质酸酶混合注射 ,既 能减轻肌注痛 ,又 可促进肝素吸收。但肝素 可抑制透明质酸酶活性 ,故 两者应临时配伍使用 ,药 物混合后不宜久置 。 (⑶ 肝素可与胰岛素受体作用 9从 而改变胰岛素的结合和作用。已有肝素致低血 —ˉ ~ 糖的报道。 ~ˉ _ _ (5)下 列药物与本 品有配伍禁忌 :卡 那霉素 、阿米卡星 、柔红霉素 、乳糖酸红霉
1。
; ;
; ;
1药 物相互作用】
i
素 、硫酸庆大霉素 、氢化考 的松琥珀酸钠 、多粘菌素 B、 阿霉素 、要布霉素 、万古霉 丙嗪 、异丙嗪 、麻醉性镇痛药 。 素 、头孢孟 多 、头孢氧哌唑 、头孢 噻吩钠 、氯喹 `氯 (f9l甲 巯咪唑 、丙硫氧嘧啶 与本 品有 协同作用 。 【 药物过量 1 本 品过量可致 自发性 出血倾 向。肝素过量时可用 1%的 硫酸鱼精蛋 白溶液缓 l曼 滴 注 ,如 此可中和肝素作用 。每 1mg鱼 精 蛋 白可 中和 100U的 肝素钠 。 【 药理毒理 1 曲于本 品具有带强 负电荷 的理化 特性 ,能 干扰血凝过程 的许 多环节 9在 体 内外都 其 有抗凝血作 用。 作用机制 比较复杂 ,主 要通过与抗凝血酶 ⅢlAT-Ⅲ )结 合 ,而 增强 后者对活化 的 Ⅱ、Ⅸ 、X、 Ⅺ 和 Ⅻ 凝血 因子 的抑制作用 。其 后果涉及阻止血小板凝 集 和破坏 ,妨 碍凝血激活酶 的形 成 ;阻 止凝血酶原变为凝 血酶 ;抑 制凝 血酶 ,从 而妨碍 ∷ 纤维蛋 白原变成纤维蛋 白。 【 药代动力学Ⅱ 本 品 田服不吸收 ,皮 下 、肌 内或静注吸收 良好 。但 80%肝 素与 血浆 白蛋 白相结 合 ,部 分被 血细胞吸附 ,部 分可弥散到 血管外组织 间隙 。曲于分子量较大 9不 能通过 胸膜 、 肾脏排泄 ,其 中少量 以原形 腹膜和胎盘组织 。本 品主要在 网状 内皮 系统代谢 ” 00U/kg时 ”fl″ 分别 排 出 1静 注后其排泄取决于给药剂量 。当 1次 给予 100Байду номын сангаас 娴 0或 息 2.5小 时和 5小 时 。 慢性肝肾功能不全及过度肥胖者 ,代 谢 排泄延迟 ,有 蓄 为 1小 时 、 积可能 ;本 品起效时 间与给药方式有关 ,静 注 即刻发挥最大抗凝 效应 ,钽 个体差异较 血浆 内肝素浓度不受 大 ,皮 下注射 因吸收个体 差异较大 ,故 总体持续时 间明显延长 。 透析 的影 响。 【 贮藏 1 遮光 ,密 闭 ,在 阴凉处 (不 超过 ⒛ C)保 存 。 【 包装 1 安瓿瓶装 ,10支 /盒 。 【 有效期】 冗 个月 【 执行标准】 《 中国药典》 ⒛ 10年 版 二 部 【 批准文号Ⅱ 国药准字 H32022088 【 生产企业】 企业 名称 :常 州千红生化制药股份有限公 司 生产地址 :江 苏 省常州市新北区黄河西路 192号 邮政编码 :213032 电话 号码 :(0519)85156015 85156凼 9 传真 号码 :(0519)8515⑾ 18 址 :http://w叩慨 q1怼 ∞m。 cn 网
克赛产品说明书(Clexane insert-4.1)
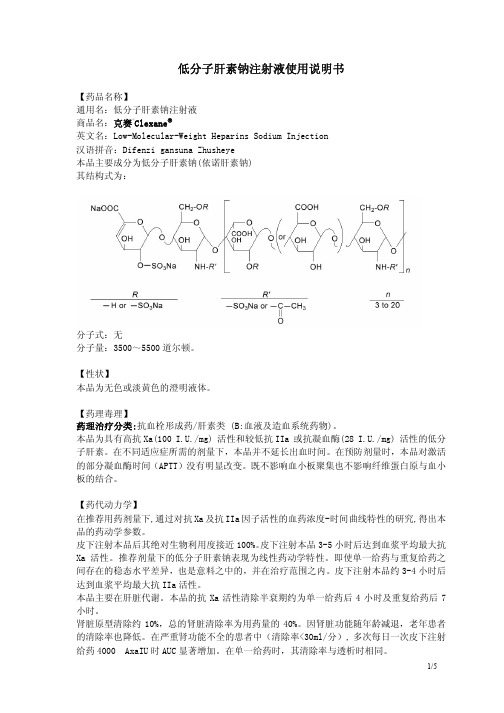
低分子肝素钠注射液使用说明书【药品名称】通用名:低分子肝素钠注射液商品名:克赛®Clexane英文名:Low-Molecular-Weight Heparins Sodium Injection汉语拼音:Difenzi gansuna Zhusheye本品主要成分为低分子肝素钠(依诺肝素钠)其结构式为:分子式:无分子量:3500~5500道尔顿。
【性状】本品为无色或淡黄色的澄明液体。
【药理毒理】药理治疗分类:抗血栓形成药/肝素类 (B:血液及造血系统药物)。
本品为具有高抗Xa(100 I.U./mg) 活性和较低抗IIa 或抗凝血酶(28 I.U./mg) 活性的低分子肝素。
在不同适应症所需的剂量下,本品并不延长出血时间。
在预防剂量时,本品对激活的部分凝血酶时间(APTT)没有明显改变。
既不影响血小板聚集也不影响纤维蛋白原与血小板的结合。
【药代动力学】在推荐用药剂量下,通过对抗Xa及抗IIa因子活性的血药浓度-时间曲线特性的研究,得出本品的药动学参数。
皮下注射本品后其绝对生物利用度接近100%。
皮下注射本品3-5小时后达到血浆平均最大抗Xa 活性。
推荐剂量下的低分子肝素钠表现为线性药动学特性。
即使单一给药与重复给药之间存在的稳态水平差异,也是意料之中的,并在治疗范围之内。
皮下注射本品约3-4小时后达到血浆平均最大抗IIa活性。
本品主要在肝脏代谢。
本品的抗Xa活性清除半衰期约为单一给药后4小时及重复给药后7小时。
肾脏原型清除约10%,总的肾脏清除率为用药量的40%。
因肾脏功能随年龄减退,老年患者的清除率也降低。
在严重肾功能不全的患者中(清除率<30ml/分), 多次每日一次皮下注射给药4000 AxaIU时AUC显著增加。
在单一给药时,其清除率与透析时相同。
【适应症】- 2000 AXa IU 和4000 AXa IU注射液:•预防静脉血栓栓塞性疾病 (预防静脉内血栓形成) ,特别是与骨科或普外手术有关的血栓形成。
依诺肝素钠注射液
依诺肝素钠注射液依诺肝素钠注射液是一种静脉注射用药物,被广泛用于临床上,用于预防和治疗深静脉血栓形成和肺栓塞。
它含有肝素钠作为主要活性成分,具有抗凝和抗血栓的作用。
肝素是一种糖蛋白多糖,它通过增强抗凝血酶活性,从而降低血液的凝血能力。
依诺肝素钠注射液通过与抗凝血酶形成复合物,抑制凝血酶的形成和活性,从而阻止血栓的形成。
同时,依诺肝素钠注射液还能抑制凝血因子Xa的活性,起到抗Xa活性的作用。
依诺肝素钠注射液主要用于以下情况的预防和治疗:1. 高危患者预防深静脉血栓形成:依诺肝素钠注射液可用于术后高危患者,如髋、膝关节置换手术、骨折手术等。
它可以通过减少血栓的形成,降低术后深静脉血栓形成的风险。
2. 治疗已存在的深静脉血栓形成:依诺肝素钠注射液可以用于治疗深静脉血栓形成,通过抑制血栓的进一步扩展和减少血栓的形成,从而缓解症状,减少并发症的发生。
3. 治疗肺栓塞:肺栓塞是一种危及生命的疾病,依诺肝素钠注射液可用于治疗肺栓塞。
它可以抑制血栓的形成和进一步扩展,从而减轻肺栓塞引起的症状,改善患者的生存率和预后。
依诺肝素钠注射液的使用方法一般为静脉注射,剂量根据患者的体重、病情以及所需的治疗目标而定。
通常情况下,成人的推荐剂量为每日0.5mg/kg,分为2次给药。
使用依诺肝素钠注射液时需要注意以下事项:1. 依诺肝素钠注射液属于处方药物,必须在医生的指导下使用。
2. 依诺肝素钠注射液可能引起出血,使用过程中需要密切观察患者的出血情况,如果发生出血,应立即停药并就医。
3. 依诺肝素钠注射液与其他抗凝血药物同时使用时可能增加出血的风险,患者在使用其他抗凝血药物时应告知医生。
4. 依诺肝素钠注射液可能与其他药物发生相互作用,患者在使用其他药物时应告知医生,以防发生不良反应。
依诺肝素钠注射液是一种可靠有效的抗凝血药物,在临床上被广泛应用。
它通过抑制凝血酶的形成和活性,阻止血栓的形成和进一步扩展,达到预防和治疗深静脉血栓形成和肺栓塞的目的。
伊诺肝素钠

HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use Lovenox safely and effectively. See full prescribing information for Lovenox.Lovenox® (enoxaparin sodium injection) for subcutaneous and intravenous useInitial U.S. Approval: 1993WARNING : SPINAL/EPIDURAL HEMATOMASee full prescribing information for complete boxed warning . • Enoxaparin use in patients undergoing spinal/epidural anesthesia or spinal puncture increases the risk of spinal or epidural hematoma, which may cause long-term or permanent paralysis (5.5) • Risk is increased by:o Indwelling epidural catheters for analgesia (5.5) o Drugs affecting hemostasis [e.g., nonsteroidal anti-inflammatory drugs, platelet inhibitors, anticoagulants] (5.5, 7)o Traumatic or repeated spinal or epidural puncture (5.5)-----------------------RECENT MAJOR CHANGES ------------------Indications and Usage (1.4), 5/2007 Dosage and Administration (2) 5/2007ST-segment Elevation Myocardial Infarction Warnings and Precautions (5.2) 5/2007 Percutaneous coronary revascularization procedures------------------INDICATIONS AND USAGE -------------------Lovenox is a low molecular weight heparin [LMWH] indicated for:• Prophylaxis of deep vein thrombosis (DVT) in abdominalsurgery, hip replacement surgery, knee replacement surgery, or medical patients with severely restricted mobility during acute illness (1.1)• Inpatient treatment of acute DVT with or without pulmonaryembolism (1.2)• Outpatient treatment of acute DVT without pulmonaryembolism. (1.2)• Prophylaxis of ischemic complications of unstable angina andnon-Q-wave myocardial infarction [MI] (1.3)• Treatment of acute ST-segment elevation myocardialinfarction [STEMI] managed medically or with subsequent percutaneous coronary intervention [PCI] (1.4)-------------------DOSAGE AND ADMINISTRATION--------------Indication Standard Regimen (2.1, 2.3) Severe RenalImpairment (2.2)DVT prophylaxis in abdominal surgery 40 mg SC once daily 30 mg SC once daily DVT prophylaxis in knee replacement surgery30 mg SC every 12 hours 30 mg SC once daily DVT prophylaxis in hip replacement surgery 30 mg SC every 12 hours or 40 mg SConce daily30 mg SC once daily DVT prophylaxis in medical patients 40 mg SC once daily 30 mg SC once daily Inpatient treatment of acute DVT with or without pulmonary embolism 1 mg/kg SC every 12 hours or 1.5 mg/kg SC once daily (with warfarin)1 mg/kg SC once daily Outpatient treatment acute DVT without of hours (with warfarin) g SC oncedaily pulmonary embolism 1 mg/kg SC every 12 1 mg/k Unstable angina and g SC once non-Q-wave MI 1 mg/kg SC every 12hours (with aspirin) 1 mg/k daily Acute STEMI in patients <75 years of CI, see 1)] hours with aspirin) by g SC once daily age[For dosing insubsequent P Dosage andAdministration (2.30 mg single IV bolus plus a 1 mg/kg SC dose followed by 1 mg/kg SC every 12 30-mg single IV bolus plus a 1 mg/kgSC dose followed 1 mg/k Acute STEMI in patients ≥75 years of 12 hours (no bolus) daily (no bolus) age0.75 mg/kg SC every 1 mg/kg SC once Do not use as intramuscular injection.For subcutaneous use, do not mix with other injections or fusions. --------------------DOSAGE FORMS AND STRENGTHS-------- • 60 mg/0.6 mL, 80 mg/0.8AINDICATIONS ----------------- i-platelet) oval5.3) arin or other LMWHs (5.6)notMultiple-dose formulations contain benzyl alcohol (5.8) --- adverse reactions (>1%) were bleeding, anemia, rombocytopenia, elevation of serum aminotransferase, diarrhea, ADVERSE REACTIONS, contact nofi-aventis at 1-800-633-1610 or FDA at 1-800-FDA-1088 or /medwatch. in--100mg/mL concentration (3.1):• Prefilled syringes: 30 mg/0.3 mL, 40 mg/0.4 mLGraduated prefilled syringes:mL,100 mg/1 mL• Multiple-dose vial: 300 mg/3 mL 150mg/mL concentration (3.2):• Graduated prefilled syringes: 120 mg/0.8 mL, 150 mg/1 mL------------------------------CONTR• Active major bleeding (4.1)Thrombocytopenia with a positive in vitro test for ant • antibody in the presence of enoxaparin sodium (4.2 Hypersensitivity to enoxaparin sodium (4.3)•• Hypersensitivity to heparin or pork products (4.4)-----------------------WARNINGS AND PRECAUTIONS ----------• Use caution in conditions with increased risk of hemorrhage(5.1)• Obtain hemostasis at the puncture site before sheath rem after percutaneous coronary revascularisation (5.2)• Use caution with concomitant medical conditions (• Use caution in case of history of heparin-inducedthrombocytopenia (5.4)• Monitor thrombocytopenia of any degree closely (5.5) •Do not exchange with hep • Pregnant women with mechanical prosthetic heart valves adequately studied (5.7)•• Periodic blood counts recommended (5.9)-----------------------------ADVERSE REACTIONS ----------------Most common th and nauseaTo report SUSPECTED sa w-----------------------------DRUG INTERACTIONS ----- hich may enhance hemorrhage risk prior to itiation of Lovenox or conduct close clinical and laboratory --------------Discontinue agents w in monitoring (5.9, 7).----------------USE IN SPECIFIC POP ------ULATIONS ------------ patients with• Hepatic Impairment (8.8)• Low-weight patients: Observe for signs of bleeding (8.9)• Severe renal impairment: Adjust dose for creatinine clearance <30 mL/min (2.2)See 17 for PATIENT COUNSELING INFORMATIONRevised: [m/year]WARNIN 1 INDIC ction)2 NGTHSon 4 5 ures ty with Other Heparinswith Mechanical Prosthetic Heart7 CTIONS8 USE IN SPECIFIC POPULATIONS8.1 Pregnancyical Prosthetic Heart Valves ent 11 12 LOGY13 OLOGYlity 14 Acute ardialections or subsections omitted from the full prescribing ation are not listedFULL PRESCRIBING INFORMATION: CONTENTS* G - SPINAL / EPIDURAL HEMATOMAS ATIONS AND USAGEProphylaxis of deep vein thrombosis in patients1.1 undergoing surgery and in medical patients with severely restricted mobility during acute illness Treatment of acute deep vein thrombosis1.2 1.3 Prophylaxis of ischemic complications of unstableangina and non-Q-wave myocardial infar 1.4 Treatment of acute ST-segment Elevation Myocardial Infarction (STEMI DOSAGE AND ADMINISTRATION2.1 Adult dosage 2.2 Renal impairment2.3 Geriatric patients with acute STEMI 2.4 Administration3 3.1 100-mg/mL concentrati DOSAGE FORMS AND STRE 3.2 150-mg/mL concentration CONTRAINDICATIONSWARNINGS AND PRECAUTIONS5.1 Increased risk of Hemorrhage5.2 Percutaneous coronary revascularization proced 5.3 Use of Lovenox with Concomitant Medical Conditions 5.4 History of heparin-induced thrombocytopenia 5.5 ThrombocytopeniaInterchan 5.6 geabili 5.7 Pregnant Women Valves5.8 Benzyl alcohol 5.9 Laboratory tests6 6.1 Clinical StudiesADVERSE REACTIONS6.2 Post-marketing experience DRUG INTERA 8.3 Nursing Mothers 8.4 Pediatric Use 8.5 Geriatric Use8.6 Patients with Mechan 8.7 Renal impairment 8.8 Hepatic impairm 8.9 Low-weight Patients 10 OVERDOSAGE DESCRIPTIONCLINICAL PHARMACO 12.1 Mechanism of Action 12.2 Pharmacodynamics 12.3 PharmacokineticsNONCLINICAL TOXIC 13.1 Carcinogenesis, Mutagenesis, Impairment of Ferti 13.2 Animal ToxicologyICAL TRIALS EX CLIN PERIENCE14.1 Prophylaxis of deep vein thrombosis followingabdominal surgery14.2 Prophylaxis of deep vein thrombosis following Hip orKnee Replacement surgeryProphylaxis of deep vein thr 14.3 ombosis in MedicalPatients with Severely Restricted Mobility during Illness14.4 Treatment of acute deep vein thrombosis with orwithout pulmonary embolism14.5 Prophylaxis of ischemic complications in unstableangina and non-Q-wave myocardial infarction14.6 Treatment of acute ST-segment Elevation Myoc Infarction (STEMI)16 HOW SUPPLIED/STORAGE AND HANDLING 17 PATIENT COUSELING INFORMATION*S inform12FULL PRESCRIBING INFORMATIONWARNING: SPINAL / EPIDURAL HEMATOMAS3When neuraxial anesthesia (epidural/spinal anesthesia) or spinal puncture is employed, 4patients anticoagulated or scheduled to be anticoagulated with low molecular weight 5heparins or heparinoids for prevention of thromboembolic complications are at risk of 6developing an epidural or spinal hematoma which can result in long-term or permanent 7paralysis.89The risk of these events is increased by the use of indwelling epidural catheters for 10administration of analgesia or by the concomitant use of drugs affecting hemostasis such as 11non steroidal anti-inflammatory drugs (NSAIDs), platelet inhibitors, or other 12anticoagulants. The risk also appears to be increased by traumatic or repeated epidural or 13spinal puncture.1415Monitor patients for signs and symptoms of neurological impairment. If neurologic 16compromise is noted, urgent treatment is necessary.1718Consider the potential benefit versus risk before neuraxial intervention in patients 19anticoagulated or to be anticoagulated for thromboprophylaxis [see Warnings and 20Precautions (5.1) and Drug Interactions (7)].2122232425262728293031323334353637383940414243 1 INDICATIONS AND USAGE1.1Prophylaxis of deep vein thrombosisLovenox is indicated for the prophylaxis of deep vein thrombosis, which may lead to pulmonary embolism:•in patients undergoing abdominal surgery who are at risk for thromboembolic complications [see Clinical Trials Experience 14.1].•in patients undergoing hip replacement surgery, during and following hospitalization.•in patients undergoing knee replacement surgery.•in medical patients who are at risk for thromboembolic complications due to severely restricted mobility during acute illness.1.2Treatment of Acute Deep Vein ThrombosisLovenox is indicated for:•the inpatient treatment of acute deep vein thrombosis with or without pulmonary embolism, when administered in conjunction with warfarin sodium;•the outpatient treatment of acute deep vein thrombosis without pulmonary embolism when administered in conjunction with warfarin sodium.1.3Prophylaxis of Ischemic Complications of Unstable Angina and Non-Q-wave Myocardial InfarctionLovenox is indicated for the prophylaxis of ischemic complications of unstable angina and non-Q-wave myocardial infarction, when concurrently administered with aspirin.44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 1.4 Treatment of acute ST- segment Elevation Myocardial Infarction (STEMI)Lovenox has been shown to reduce the rate of the combined endpoint of recurrent myocardial infarction or death in patients with acute STEMI receiving thrombolysis and being managed medically or with Percutaneous Coronary Intervention (PCI).2 DOSAGE AND ADMINISTRATIONAll patients should be evaluated for a bleeding disorder before administration of Lovenox, unless the medication is needed urgently. Since coagulation parameters are unsuitable for monitoring Lovenox activity, routine monitoring of coagulation parameters is not required [see Warnings and Precautions (5.9)].For subcutaneous use, Lovenox should not be mixed with other injections or infusions. For intravenous use (i.e., for treatment of acute STEMI), Lovenox can be mixed with normal saline solution (0.9%) or 5% dextrose in water.Lovenox is not intended for intramuscular administration.2.1 Adult DosageAbdominal Surgery: In patients undergoing abdominal surgery who are at risk for thromboembolic complications, the recommended dose of Lovenox is 40 mg once a day administered by SC injection with the initial dose given 2 hours prior to surgery. The usual duration of administration is 7 to 10 days; up to 12 days administration has been administered in clinical trials. 65 66 67 68 69 70Hip or Knee Replacement Surgery: In patients undergoing hip or knee replacement surgery, the recommended dose of Lovenox is 30 mg every 12 hours administered by SC injection. Provided that hemostasis has been established, the initial dose should be given 12 to 24 hours after surgery. For hip replacement surgery, a dose of 40 mg once a day SC, given initially 12 (±3) hours prior to surgery, may be considered. Following the initial phase of thromboprophylaxis in hip replacement surgery patients, it is recommended that continued prophylaxis with Lovenox 40 mg once a day is administered by SC injection for 3 weeks. The usual duration of administration is 7 to 10 days; up to 14 days administration has been administered in clinical trials. 71 72 73 74 75 76 77 78 79 80Medical Patients During Acute Illness: In medical patients at risk for thromboembolic complications due to severely restricted mobility during acute illness, the recommended dose of Lovenox is 40 mg once a day administered by SC injection. The usual duration of administration is 6 to 11 days; up to 14 days of Lovenox has been administered in the controlled clinical trial. 81 82 83 84 85 86Treatment of Deep Vein Thrombosis With or Without Pulmonary Embolism: In outpatient treatment , patients with acute deep vein thrombosis without pulmonary embolism who can be 87 88treated at home, the recommended dose of Lovenox is 1 mg/kg every 12 hours administered SC. In inpatient (hospital) treatment , patients with acute deep vein thrombosis with pulmonary embolism or patients with acute deep vein thrombosis without pulmonary embolism (who are not candidates for outpatient treatment), the recommended dose of Lovenox is 1 mg/kg every 12 hours administered SC or 1.5 mg/kg once a day administered SC at the same time every day. In both outpatient and inpatient (hospital) treatments, warfarin sodium therapy should be initiated when appropriate (usually within 72 hours of Lovenox). Lovenox should be continued for a minimum of 5 days and until a therapeutic oral anticoagulant effect has been achieved (International Normalization Ratio 2.0 to 3.0). The average duration of administration is 7 days; up to 17 days of Lovenox administration has been administered in controlled clinical trials. 89 90 91 92 93 94 95 96 97 98 99 100Unstable Angina and Non-Q-Wave Myocardial Infarction: In patients with unstable angina or non-Q-wave myocardial infarction, the recommended dose of Lovenox is 1 mg/kg administered SC every 12 hours in conjunction with oral aspirin therapy (100 to 325 mg once daily). Treatment with Lovenox should be prescribed for a minimum of 2 days and continued until clinical stabilization. The usual duration of treatment is 2 to 8 days; up to 12.5 days of Lovenox has been administered in clinical trials. [See Warnings and Precautions (5.2) and Clinical Trials Experience (14.5)]. 101 102 103 104 105 106 107 108Treatment of acute ST-segment Elevation Myocardial Infarction: In patients with acute ST-segment Elevation Myocardial Infarction, the recommended dose of Lovenox is a single IV bolus of 30 mg plus a 1 mg/kg SC dose followed by 1 mg/kg administered SC every 12 hours (maximum 100 mg for the first two doses only, followed by 1 mg/kg dosing for the remaining doses). Dosage adjustments are recommended in patients ≥75 years of age [see Dosage and Administration (2.3)]. 109 110 111 112 113 114 115 116 117 118 119 120 121 122 123 124 125 126 127 128 129 130 131 132When administered in conjunction with a thrombolytic (fibrin-specific or non-fibrin specific), Lovenox should be given between 15 minutes before and 30 minutes after the start of fibrinolytic therapy. All patients should receive acetylsalicylic acid (ASA) as soon as they are identified as having STEMI and maintained with 75 to 325 mg once daily unless contraindicated. In the pivotal clinical study, the Lovenox treatment duration was 8 days or until hospital discharge, whichever came first. An optimal duration of treatment is not known, but it is likely to be longer than 8 days.For patients managed with Percutaneous Coronary Intervention (PCI): If the last Lovenox SC administration was given less than 8 hours before balloon inflation, no additional dosing is needed. If the last Lovenox SC administration was given more than 8 hours before balloon inflation, an IV bolus of 0.3 mg/kg of Lovenox should be administered [see Warnings and Precautions (5.2)].2.2 Renal ImpairmentAlthough no dose adjustment is recommended in patients with moderate (creatinine clearance 30-50 mL/min) and mild (creatinine clearance 50-80 mL/min) renal impairment, all such patients should be observed carefully for signs and symptoms of bleeding.133 134 135 136 137 The recommended prophylaxis and treatment dosage regimens for patients with severe renal impairment (creatinine clearance <30 mL/min) are described in Table 1 [see Use in SpecificPopulations (8.6) and Clinical Pharmacology (12.3)].Table 1Dosage Regimens for Patients with Severe Renal Impairment(creatinine clearance <30mL/minute)Indication DosageRegimen Prophylaxis in abdominal surgery 30 mg administered SC once dailyProphylaxis in hip or knee replacement surgery 30 mg administered SC once dailyProphylaxis in medical patients during acute illness 30 mg administered SC once dailyInpatient treatment of acute deep vein thrombosis withor without pulmonary embolism, when administered inconjunction with warfarin sodium1 mg/kg administered SC once dailyOutpatient treatment of acute deep vein thrombosiswithout pulmonary embolism, when administered inconjunction with warfarin sodium1 mg/kg administered SC once dailyProphylaxis of ischemic complications of unstableangina and non-Q-wave myocardial infarction, whenconcurrently administered with aspirin1 mg/kg administered SC once dailyTreatment of acute ST-segment Elevation MyocardialInfarction in patients <75 years of age30 mg single IV bolus plus a 1 mg/kgSC dose followed by 1 mg/kgadministered SC once daily.Treatment of acute ST-segment Elevation MyocardialInfarction in geriatric patients ≥75 years of age1 mg/kg administered SC once daily(no initial bolus)138 139140 141 142 143 144 145 146 147 148 149 150 151 152 153 154 155 2.3 Geriatric patients with acute ST-Elevation Myocardial InfarctionFor treatment of acute ST-segment Elevation Myocardial Infarction in geriatric patients ≥75 years of age, do not use an initial IV bolus. Initiate dosing with 0.75 mg/kg SC every 12 hours (maximum 75 mg for the first two doses only, followed by 0.75 mg/kg dosing for the remaining doses)[see Use in Specific Populations (8.5) and Clinical Pharmacology (12.3)].No dose adjustment is necessary for other indications in geriatric patients unless kidney function is impaired [see Dosage and Administration (2.2)].2.4 AdministrationLovenox is a clear, colorless to pale yellow sterile solution, and as with other parenteral drug products, should be inspected visually for particulate matter and discoloration prior to administration.The use of a tuberculin syringe or equivalent is recommended when using Lovenox multiple-dose vials to assure withdrawal of the appropriate volume of drug.156157 158 159 160 161 162 163 Lovenox must not be administered by intramuscular injection. Lovenox is intended for use under the guidance of a physician.For subcutaneous administration, patients may self-inject only if their physicians determine that it is appropriate and with medical follow-up, as necessary. Proper training in subcutaneous injection technique (with or without the assistance of an injection device) should be provided. Subcutaneous Injection Technique: Patients should be lying down and Lovenox administered by deep SC injection. To avoid the loss of drug when using the 30 and 40 mg prefilled syringes, do not expel the air bubble from the syringe before the injection. Administration should be alternated between the left and right anterolateral and left and right posterolateral abdominal wall. The whole length of the needle should be introduced into a skin fold held between the thumb and forefinger; the skin fold should be held throughout the injection. To minimize bruising, do not rub the injection site after completion of the injection.164 165 166 167 168 169 170171 172 173 174 175 176 177 178 Lovenox prefilled syringes and graduated prefilled syringes are available with a system that shields the needle after injection.1. Remove the needle shield by pulling it straight off the syringe (see Figure A). If adjusting the dose is required, the dose adjustment must be done prior to injecting the prescribed dose to the patient.Figure A179 180181 182 183 184 2. Inject using standard technique, pushing the plunger to the bottom of the syringe (see FigureB).Figure B185 186187 188 3. Remove the syringe from the injection site keeping your finger on the plunger rod (see FigureC).189Figure C190 191 192 193 194 195 196198199 200 201 2024. Orient the needle away from you and others, and activate the safety system by firmly pushing the plunger rod. The protective sleeve will automatically cover the needle and an audible “click” will be heard to confirm shield activation (see Figure D).Figure D1975. Immediately dispose of the syringe in the nearest sharps container (see Figure E).Figure E203 204 205 206 207 208 209 210 211 212 213NOTE:• The safety system can only be activated once the syringe has been emptied.• Activation of the safety system must be done only after removing the needle from the patient’s skin.• Do not replace the needle shield after injection. • The safety system should not be sterilized.Activation of the safety system may cause minimal splatter of fluid. For optimal safety activate the system while orienting it downwards away from yourself and others.Intravenous (Bolus) Injection Technique: For intravenous injection, the multiple-dose vial should be used. Lovenox should be administered through an intravenous line. Lovenox should not be mixed or co-administered with other medications. To avoid the possible mixture of Lovenox with other drugs, the intravenous access chosen should be flushed with a sufficient amount of saline or dextrose solution prior to and following the intravenous bolus administration of Lovenox to clear the port of drug. Lovenox may be safely administered with normal saline solution (0.9%) or 5% dextrose in water.214 215 216 217 218 219 220 221222223 224 225 226 227 228 229 230 231 232 233 234 235 236 237 238 239 240 241 242 243 244 245 246 247 248 249 250 251 252 253 254 255 256 257 258 259 260 261 262 263 264 265 266 3 DOSAGE FORMS AND STRENGTHSLovenox is available in two concentrations:3.1 100 mg per mL-Prefilled Syringes 30 mg / 0.3 mL, 40 mg / 0.4 mL-Graduated Prefilled Syringes 60 mg / 0.6 mL, 80 mg / 0.8 mL, 100 mg / 1 mL-Multiple-Dose Vials 300 mg / 3 mL3.2 150 mg per mL-Graduated Prefilled Syringes 120 mg / 0.8 mL, 150 mg / 1 mL4 CONTRAINDICATIONS•Active major bleeding.•Thrombocytopenia associated with a positive in vitro test for anti-platelet antibody in the presence of enoxaparin sodium.•Known hypersensitivity to enoxaparin sodium (e.g., pruritus, urticaria, anaphylactoid reactions) [see Adverse Reactions (6.2)].•Known hypersensitivity to heparin or pork products.•Known hypersensitivity to benzyl alcohol (which is in only the multi-dose formulation of Lovenox).5 WARNINGS AND PRECAUTIONS5.1 Increased Risk of HemorrhageCases of epidural or spinal hematomas have been reported with the associated use of Lovenox and spinal/epidural anesthesia or spinal puncture resulting in long-term or permanent paralysis. The risk of these events is higher with the use of post-operative indwelling epidural catheters or by the concomitant use of additional drugs affecting hemostasis such as NSAIDs[see boxed Warning, Adverse Reactions (6.2) and Drug Interactions (7)].Lovenox should be used with extreme caution in conditions with increased risk of hemorrhage, such as bacterial endocarditis, congenital or acquired bleeding disorders, active ulcerative and angiodysplastic gastrointestinal disease, hemorrhagic stroke, or shortly after brain, spinal, or ophthalmological surgery, or in patients treated concomitantly with platelet inhibitors.Major hemorrhages including retroperitoneal and intracranial bleeding have been reported. Some of these cases have been fatal.Bleeding can occur at any site during therapy with Lovenox. An unexplained fall in hematocrit or blood pressure should lead to a search for a bleeding site.5.2Percutaneous coronary revascularization proceduresTo minimize the risk of bleeding following the vascular instrumentation during the treatment of unstable angina, non-Q-wave myocardial infarction and acute ST-segment elevation myocardial267 268 269 270 271 272 273 274 275 276 277 278 279 280 281 282 283 284 285 286 287 288 289 290 291 292 293 294 295 296 297 298 299 300 301 302 303 304 305 306 307 308 309 310 311 infarction, adhere precisely to the intervals recommended between Lovenox doses. It is important to achieve hemostasis at the puncture site after PCI. In case a closure device is used, the sheath can be removed immediately. If a manual compression method is used, sheath should be removed 6 hours after the last IV/SC Lovenox. If the treatment with enoxaparin sodium is to be continued, the next scheduled dose should be given no sooner than 6 to 8 hours after sheath removal. The site of the procedure should be observed for signs of bleeding or hematoma formation [see Dosage and Administration (2.1)].5.3 Use of Lovenox with Concomitant Medical ConditionsLovenox should be used with care in patients with a bleeding diathesis, uncontrolled arterial hypertension or a history of recent gastrointestinal ulceration, diabetic retinopathy, and hemorrhage.5.4 History of Heparin-induced ThrombocytopeniaLovenox should be used with extreme caution in patients with a history of heparin-induced thrombocytopenia.5.5ThrombocytopeniaThrombocytopenia can occur with the administration of Lovenox.Moderate thrombocytopenia (platelet counts between 100,000/mm3 and 50,000/mm3) occurred at a rate of1.3% in patients given Lovenox, 1.2% in patients given heparin, and 0.7% in patients given placebo in clinical trials.Platelet counts less than 50,000/mm3 occurred at a rate of 0.1% in patients given Lovenox, in 0.2% of patients given heparin, and 0.4% of patients given placebo in the same trials. Thrombocytopenia of any degree should be monitored closely. If the platelet count falls below 100,000/mm3, Lovenox should be discontinued. Cases of heparin-induced thrombocytopenia with thrombosis have also been observed in clinical practice. Some of these cases were complicated by organ infarction, limb ischemia, or death [see Warnings and Precautions (5.4)].5.6 Interchangeability with Other HeparinsLovenox cannot be used interchangeably (unit for unit) with heparin or other low molecular weight heparins as they differ in manufacturing process, molecular weight distribution, anti-Xa and anti-IIa activities, units, and dosage. Each of these medicines has its own instructions for use.5.7 Pregnant Women with Mechanical Prosthetic Heart ValvesThe use of Lovenox for thromboprophylaxis in pregnant women with mechanical prosthetic heart valves has not been adequately studied. In a clinical study of pregnant women with mechanical prosthetic heart valves given enoxaparin (1 mg/kg twice daily) to reduce the risk of thromboembolism, 2 of 8 women developed clots resulting in blockage of the valve and leading to maternal and fetal death. Although a causal relationship has not been established these deaths may have been due to therapeutic failure or inadequate anticoagulation. No patients in the。
肝素钠说明书
肝素钠注射液说明书请仔细阅读说明书并在医师指导下使用【药品名称】通用名称:肝素钠注射液英文名称:heparin sodium lnjection 汉语拼音:gansuna zhusheye 【成份】本品主要成份为肝素钠。
肝素钠系自猪或牛的肠黏膜中提取的硫酸氨基葡聚糖的钠盐,属黏多糖类物质。
辅料为:苯酚、注射用水。
【性状】本品为无色至淡黄色的澄明液体。
【适应症】用于防治血栓形成或栓塞性疾病(如心肌梗塞、血栓性静脉炎、肺栓塞等);各种原因引起的弥漫性血管内凝血(dic);也用于血液透析、体外循环、导管术、微血管手术等操作中及某些血液标本或器械的抗凝处理。
【规格】 2ml:12500单位【用法用量】(1)深部皮下注射:首次5000~10000单位,以后每8小时8000~10000单位或每12小时15000~20000单位;每24小时总量约30000~40000单位,一般均能达到满意的效果。
(2)静脉注射:首次5000~10000单位,之后,或按体重每4小时100单位/kg,用氯化钠注射液稀释后应用。
(3)静脉滴注:每日20000~40000单位,加至氯化钠注射液1000mi中持续滴注。
滴注前可先静脉注射5000单位作为初始剂量。
(4)预防性治疗:高危血栓形成病人,大多是用于腹部手术之后,以防止深部静脉血栓。
在外科手术前2小时先给5000单位肝素皮下注射,但麻醉方式应避免硬膜外麻醉,然后每隔8~12小时5000单位,共约7日。
【不良反应】毒性较低,主要不良反应是用药过多可致自发性出血,故每次注射前应测定凝血时间。
如注射后引起严重出血,可静注硫酸鱼精蛋白进行急救。
偶可引起过敏反应及血小板减少,常发生在用药初5~9天,故开始治疗1个月内应定期监测血小板计数。
偶见一次性脱发和腹泻。
尚可引起骨质疏松和自发性骨折。
肝功能不良者长期使用可引起抗凝血酶-iii耗竭而血栓形成倾向。
【禁忌】对肝素过敏、有自发出血倾向者、血液凝固迟缓者(如血友病、紫癜、血小板减少)、溃疡病、创伤、产后出血者及严重肝功能不全者禁用。
依诺肝素

商品名:克赛/Clexane英文名:Enoxaparin通用名:依诺肝素【理化特性】成分及含量:每个注射器:20mg40mg60mg80mg100mg依诺肝素钠:20mg40mg60mg80mg100mg加注射用水至0.2ml0.4ml0.6ml0.8ml 1.0ml剂型:无菌无致热源可注射液,已预装入注射器。
药理治疗分类抗栓剂/低分子肝素 (B:血液,造血器官)【药理作用】药效动力学特性:本品为具有高活性抗Xa(100 I.U./mg)作用和低活性抗IIa 或抗凝血酶(28 I.U./mg)作用的低分子肝素. 在不同适应证所需的剂量下, 本品并不延长出血时. 在预防剂量时, 本品对APTT没有明显改变. 既不影响血小板聚集也不影响纤维蛋白原与血小板的结合.药代动力学特性:药代动力学参数源于对血浆中抗Xa因子活性的研究.生物利用度:皮下注射本品可迅速并完全被吸收, 本品的生物利用度接近95%.分布:皮下注射本品3小时后达最大血浆活性. 抗Xa活性存在于血管内.生物转化:本品主要在肝脏代谢.消除:使用40 mg 本品时其抗Xa 活性的半衰期约为4.4小时. 使用60mg 或 80mg 本品时约为4小时.排泄:本品经尿排出. 在老年患者中消除半衰期略延长.赋形剂成分:注射用水【适应证】-20 mg和40 mg注射液:.预防静脉栓塞性疾病 (防止静脉内血栓形成) 尤其是与某些手术有关的栓塞.用于血液透析体外循环中,防止血栓形成-60 mg, 80 mg和100 mg注射液:.治疗深静脉血栓形成.治疗急性不稳定性心绞痛及非Q波心肌梗死,与阿司匹林同用【用法及用量】1 mg依诺肝素产生相当于100 I.U抗Xa活性为预防及治疗目的而使用依诺肝素时应采用深部皮下注射给药,用于血液透析体外循环时为血管内途径给药禁止肌肉内注射皮下用药须知:预装药液注射器可供直接使用。
在注射之前勿将注射器内的气泡排出。
应于患者平躺后进行注射。
肝素钠注射液说明书
请仔细阅读说明书并在医师指导下使用【药品名称】通用名称:肝素钠注射液英文名称:Heparin Sodium lnjection汉语拼音:Gansuna Zhusheye【成份】本品主要成份为肝素钠。
肝素钠系自猪或牛的肠黏膜中提取的硫酸氨基葡聚糖的钠盐,属黏多糖类物质。
辅料为:苯酚、注射用水。
【性状】本品为无色至淡黄色的澄明液体。
【适应症】用于防治血栓形成或栓塞性疾病(如心肌梗塞、血栓性静脉炎、肺栓塞等);各种原因引起的弥漫性血管内凝血(DIC);也用于血液透析、体外循环、导管术、微血管手术等操作中及某些血液标本或器械的抗凝处理。
【规格】2ml:12500单位【用法用量】(1)深部皮下注射:首次5000~10000单位,以后每8小时8000~10000单位或每12小时15000~20000单位;每24小时总量约30000~40000单位,一般均能达到满意的效果。
(2)静脉注射:首次5000~10000单位,之后,或按体重每4小时100单位/kg,用氯化钠注射液稀释后应用。
(3)静脉滴注:每日20000~40000单位,加至氯化钠注射液1000mI中持续滴注。
滴注前可先静脉注射5000单位作为初始剂量。
(4)预防性治疗:高危血栓形成病人,大多是用于腹部手术之后,以防止深部静脉血栓。
在外科手术前2小时先给5000单位肝素皮下注射,但麻醉方式应避免硬膜外麻醉,然后每隔8~12小时5000单位,共约7日。
【不良反应】毒性较低,主要不良反应是用药过多可致自发性出血,故每次注射前应测定凝血时间。
如注射后引起严重出血,可静注硫酸鱼精蛋白进行急救。
偶可引起过敏反应及血小板减少,常发生在用药初5~9天,故开始治疗1个月内应定期监测血小板计数。
偶见一次性脱发和腹泻。
尚可引起骨质疏松和自发性骨折。
肝功能不良者长期使用可引起抗凝血酶-III耗竭而血栓形成倾向。
【禁忌】对肝素过敏、有自发出血倾向者、血液凝固迟缓者(如血友病、紫癜、血小板减少)、溃疡病、创伤、产后出血者及严重肝功能不全者禁用。
肝素钠说明书

肝素钠说明书肝素钠说明书1. 药品信息- **药品名称:** 肝素钠- **药品成分:** 肝素钠- **药理作用:** 肝素钠是一种抗凝血药物,具有抑制凝血酶活性的作用,可预防和治疗血栓病变等血液凝固性疾病。
2. 适应症肝素钠适用于以下病症:- 静脉血栓形成和肺栓塞的预防和治疗;- 高危患者的血栓形成风险降低;- 血栓溶解治疗的辅助用药。
3. 药品剂型和规格肝素钠有以下剂型和规格:- **注射剂:** 2500IU/0.2ml,5000IU/0.2ml,10000IU/0.4ml,20000IU/0.8ml。
4. 使用方法- **给药途径:** 皮下注射或静脉注射。
- **剂量和使用频率:** 根据患者的体重、病情和遗传因素等因素确定剂量和使用频率。
一般情况下,成人的剂量为100IU/kg体重,每日2-3次。
5. 禁忌症和注意事项肝素钠的禁忌症包括以下情况:- 对本品过敏者禁用;- 活动性出血病例;- 急性脑血管疾病;- 结肠憩室出血。
使用肝素钠时需要注意以下事项:- 遵循医生的建议和给药指导;- 密切监测患者的凝血时间,避免出现出血或血栓等不良反应;- 注意与其他药物的相互作用,特别是抗血小板药物和抗凝血药物;- 孕妇、哺乳期妇女和儿童使用时需谨慎。
6. 不良反应肝素钠可能出现的不良反应包括:- 出血:皮下出血、黏膜出血、肌肉出血等;- 过敏反应:皮疹、荨麻疹、呼吸困难、血压下降等;- 骨质疏松:长期使用可能导致骨质疏松。
7. 药物相互作用肝素钠可能与以下药物相互作用:- 抗血小板药物:使用肝素钠时需注意增加出血风险;- 抗凝血药物:与肝素钠联合使用时需谨慎监测凝血时间。
8. 注意事项- 肝素钠需储存在阴凉干燥的地方,避免阳光直射;- 儿童需在成人监护下使用此药;- 药品过期后不得使用。
以上是对肝素钠的简要说明,如需进一步了解该药品,请遵循医生的指导和咨询药师。
*请注意:以上信息仅供参考,具体用药请遵循医生的指导。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
核准日期:2009年8月12日修改日期:依诺肝素钠注射液说明书请仔细阅读说明书并在医师指导下使用警示语:椎管内血肿。
当实施椎管内麻醉(脊麻和硬膜外麻醉)或椎管穿刺时应注意,使用低分子肝素或肝素类物质预防血栓并发症的病人,有可能引起椎管内血肿,导致长期甚至永久性瘫痪,以上事件很少发生。
放置硬膜外导管或反复硬膜外穿刺,合并使用影响止血功能的药物,如非甾体类抗炎药(NSAIDs)、血小板抑制剂或其它抗凝药物等,血肿发生率可能会更高。
此种情况,应监测病人神经损害的症状和体征,如发现有可能损伤神经,应紧急处理。
医生在对此类病人实施椎管内干预(麻醉或穿刺)时,应进行利弊权衡。
【药品名称】通用名称:依诺肝素钠注射液商品名称:克赛®Clexane英文名称:Enoxaparin Sodium Injection汉语拼音:Yinuogansuna Zhusheye【成份】化学名称:依诺肝素钠(低分子肝素钠)化学结构式:分子量:3500至5500道尔顿辅料:注射用水【性状】本品为无色或淡黄色的澄明液体。
【适应症】2000 Axa IU 和4000 Axa IU注射液:•预防静脉血栓栓塞性疾病(预防静脉内血栓形成) ,特别是与骨科或普外手术有关的血栓形成。
6000 Axa IU, 8000 Axa IU 和10000 Axa IU注射液:• 治疗已形成的深静脉栓塞,伴或不伴有肺栓塞,临床症状不严重,不包括需要外科手术或溶栓剂治疗的肺栓塞。
• 治疗不稳定性心绞痛及非Q波心肌梗死,与阿司匹林合用。
• 用于血液透析体外循环中,防止血栓形成。
• 治疗急性ST段抬高型心肌梗死,与溶栓剂联用或同时与经皮冠状动脉介入治疗(PCI)联用。
【规格】(1)0.2ml :2000 AxaIU (2)0.4ml: 4000 AxaIU (3)0.6ml: 6000 AxaIU (4)0.8ml :8000 AxaIU (5)1.0ml :10000 AxaIU【用法用量】预防静脉血栓栓塞性疾病,治疗深静脉栓塞,治疗不稳定性心绞痛及非Q波心肌梗死时应采用深部皮下注射给予依诺肝素;血液透析体外循环时为血管内途径给药;对于ST段抬高型急性心肌梗死,初始的治疗为静脉注射,随后改为皮下注射治疗。
本品为成人用药禁止肌内注射每毫升注射液含10000 AxaIU,相当于100mg依诺肝素。
每毫克(0.01ml)依诺肝素约等于100 AxaIU。
皮下注射技术:根据患者体重调整依诺肝素的注射剂量,注射前需将多余量排出,而在注射之前无需排出注射器内的气泡。
预装药液注射器可供直接使用。
应于患者平躺后进行注射。
应于左、右腹壁的前外侧或后外侧皮下组织内交替给药。
注射时针头应垂直刺入皮肤而不应成角度,在整个注射过程中,用拇指和食指将皮肤捏起,并将针头全部扎入皮肤皱折内注射。
只用于治疗ST段抬高型急性心肌梗死的静脉注射技术:通过静脉通路给予依诺肝素,不能与其他药物混合或同时注射。
为避免依诺肝素与其他药物混合,应在给予依诺肝素的前后,使用足量的生理盐水或葡萄糖溶液冲洗静脉通路以清除其它药物。
依诺肝素和0.9%生理盐水或5%葡萄糖溶液合用是安全的。
•初始3000AxaIU的静脉给药对于初始3000AxaIU的静脉给药,用预填充的依诺肝素,注射器内保留3000AxaIU (0.3ml),排出多余的液体。
可将3000AxaIU的剂量直接注射入静脉血管内。
•冠脉血管成形术的额外静脉负荷剂量:如果最后一次皮下给药在囊球扩张前8小时以上,冠脉血管成形术患者需要额外的30AxaIU/kg静脉给药。
为了确保该小注射量的准确性,推荐稀释药物至300AxaIU/ml。
为了得到300AxaIU的溶液,使用6000AxaIU的预填充依诺肝素钠注射液,推荐使用50ml输液袋[使用例如生理盐水(0.9%)或5%葡萄糖溶液]进行如下操作:用注射器从输液袋中取出30ml溶液弃除。
注入全部6000AxaIU依诺肝素钠预填充注射液到剩余20ml溶液的输液袋中。
轻轻混合输液袋中药物。
用注射器吸取所需的稀释液用于静脉注射。
稀释完全后,根据如下公式计算[稀释体积ml=患者体重kg*0.1]或用下表得出所需注射液的体积。
推荐在使用前制备稀释液。
一般建议由于肝素有诱导血小板减少症(HIT)的风险,因此治疗期间需常规监测血小板计数。
应严格遵循推荐剂量或遵医嘱。
• 在外科患者中,预防静脉血栓栓塞性疾病当患者有中度血栓形成危险时(如腹部手术),本品推荐剂量为2000 AxaIU (0.2 ml) 或4000 AxaIU (0.4 ml), 每日一次皮下注射。
在普外手术中,应于术前2小时给予第一次皮下注射,当患者有高度血栓形成倾向时(如矫形外科手术),本品推荐剂量为术前12小时开始给药,每日一次皮下注射4000 AxaIU (0.4 ml)。
在蛛网膜下腔/硬膜外麻醉及经皮冠脉腔内成形术时,应特别注意给药间隔,见特殊警告。
依诺肝素治疗一般应持续7至10天。
某些患者适合更长的治疗周期,若患者有静脉栓塞倾向,应延长治疗至静脉血栓栓塞危险消除且患者不需卧床为止。
在矫形外科手术中,连续3周,每日一次给药4000 AxaIU是有益的。
•在内科治疗患者中,预防静脉血栓栓塞性疾病依诺肝素推荐剂量为每日一次皮下给药4000 AxaIU (0.4 ml)。
依诺肝素治疗最短应为6天,直至患者不需卧床为止,最长为14天。
•治疗深静脉栓塞,伴或不伴有肺栓塞,临床症状不严重任何不确定的深静脉血栓应通过适当的检查尽快确诊。
用法和剂量:依诺肝素可用于皮下每日一次注射150 AxaIU/kg或每日两次100 AxaIU/kg。
当患者为复杂性栓塞性疾病时,推荐每日两次给药100 AxaIU/kg。
在体重高于100kg或低于40kg的患者中,依诺肝素的剂量尚无评价。
对于体重高于100kg 的患者,依诺肝素的疗效可能轻微降低。
对于体重低于40kg的患者,出血的风险可能增加。
对于这些病人必须进行特殊的临床监测。
深静脉血栓治疗期间:除非有禁忌,依诺肝素应尽早替换为口服抗凝药治疗。
依诺肝素治疗应该不超过10天,包括达到口服抗凝药治疗效果所需时间,除非不能达到目的(见4.4部分使用注意事项:血小板监测)。
因此应尽早使用口服抗凝药治疗。
•治疗不稳定性心绞痛及非Q波心梗皮下注射依诺肝素推荐剂量为每次100 AxaIU/kg,每12小时给药一次,应与阿司匹林同用(推荐剂量:最小负荷剂量为160mg,之后每日一次口服75至325 mg )。
一般疗程为2至8天,直至临床症状稳定。
•用于血液透析体外循环中,防止血栓形成推荐剂量为100 Axa IU/kg。
对于有高度出血倾向的血液透析患者,应减量,即双侧血管通路给予依诺肝素50 Axa IU/kg或单侧血管通路给予75Axa IU/kg。
应于血液透析开始时,在动脉血管通路给予依诺肝素钠。
上述剂量药物的作用时间一般为4小时。
然而,当出现纤维蛋白环时,应再给予50至100 Axa IU/kg的剂量。
•与溶栓剂联用或同时与经皮冠状动脉介入治疗(PCI)联用,治疗急性ST段抬高型心肌梗死在初始静脉注射给予3000 AxaIU后的15分钟内皮下给药100 AxaIU/kg,随后每隔12小时皮下注射一次100 AxaIU/kg(最初两次皮下注射剂量最大为10 000AxaIU).首剂依诺肝素应在溶栓治疗前15分钟至溶栓治疗(无论是否有纤维蛋白特异性)后30分钟之间给予。
推荐疗程为8天,或使用至出院(未到8天)。
合并用药:应在症状出现后尽早给予阿司匹林,维持剂量为每日口服75至325 mg,至少30天,除非有其它指征。
行冠脉血管成形术患者:如果最后一次依诺肝素皮下注射是在球囊扩张前不到8小时,则不需再次给药.如果最后一次依诺肝素皮下注射是在球囊扩张前8小时以上,则需静脉给予30AxaIU/kg 剂量的依诺肝素。
为了提高给药剂量的准确性,推荐将药物稀释到300Axa IU/ml(见只用于治疗ST段抬高型急性心肌梗死的静脉注射技术部分的描述)。
75岁或以上的患者,在治疗ST段抬高型急性心肌梗死时不应给予静脉负荷剂量注射。
应给予每隔12小时皮下注射75AxaIU/kg剂量(最初两次注射最大剂量为7500 AxaIU 剂量)。
【不良反应】已有超过15 000名患者在临床研究中接受依诺肝素治疗,由此对依诺肝素进行了评估。
包括在1776名有血栓栓塞性并发症风险的骨科或腹部手术患者中用于预防深静脉血栓;在1169名严重活动受限的急性内科疾病患者中用于预防深静脉血栓;559名用于治疗伴有或不伴有肺栓塞的深静脉血栓患者;1578名用于治疗不稳定性心绞痛及非Q波心梗(MI)患者;10 176名用于治疗急性ST段抬高型心肌梗死(STEMI)患者。
在这些临床试验期间,依诺肝素钠的用法用量根据适应症的不同而有所不同。
手术后的或严重活动受限的急性内科疾病患者,用于预防深静脉血栓的依诺肝素钠给药剂量为40 mg 皮下注射每日1次。
在伴有或不伴有肺栓塞(PE)的深静脉血栓(DVT)的治疗中,患者接受每12小时1次1 mg/kg 皮下注射依诺肝素,或每日1次1.5 mg/kg皮下注射依诺肝素。
在治疗不稳定性心绞痛和非Q波心肌梗死的临床研究中,依诺肝素钠的剂量为每12小时1次1 mg/kg皮下注射,在急性ST段抬高型心肌梗死的临床研究中,依诺肝素钠给药方案为30 mg静脉快速给药,随后每12小时1次1 mg/kg皮下注射。
这些临床研究中观察到的及上市后经验报告的不良反应如下:发生率的定义如下:非常常见(≥ 1/10);常见(≥ 1/100 到< 1/10);不常见(≥1/1000 到< 1/100);罕见(≥ 1/10,000 到<1/1,000)和非常罕见(< 1/10,000)。
在临床试验中没有观察到,但是在上市后经验报告中出现的不良事件列为“罕见”。
出血在临床研究中,出血是最常见的不良反应。
包括大出血,最高在4.2%的患者中报告(手术患者1)。
其中一些为致死性病例。
与其它抗凝药物一样,伴有以下危险因素时,可能发生出血:有出血倾向的器官损伤、介入性操作或与影响凝血的药物联合用药(请参见[注意事项]和[相互作用])。
*:如血肿、注射部位之外的瘀斑、伤口血肿、血尿、鼻出血和胃肠道出血。
此外的上市后经验:1在手术患者中,出血栓栓塞性并发症被认为是严重的:(1)如果出血导致了显著的临床事件,或(2)如果合并出现血红蛋白下降≥2 g/dL或输注2个单位或以上的血液制品。
腹膜后出血和颅内出血一直被认为是严重的出血。
罕见:在蛛网膜下腔/硬膜外麻醉或脊髓穿刺时使用依诺肝素钠,已经报告了硬膜外血肿(或神经轴索血肿)病例。