盐酸米诺环素软膏(派丽奥)的说明书
盐酸米诺环素软膏---邹平中心医院--朱汉越
通用名:盐酸米诺环素软膏商品名称:派丽奥适应症:牙科用抗生素制剂,用于改善敏感菌所致牙周炎的各种症状。
用法用量:每周给药一次,4周为1个疗程。
贮藏:遮光,密闭保存。
派丽奥牙科用软膏是治疗牙周炎的局部用药,每克含有20mg盐酸二甲胺四环素(minoeyeline hydrochloride,有效成分)。
该药膏置于专用注射器中,没支注射器含有0.5g,可以直接施用于感染部位的牙周袋内。
本药对牙龈卟啉菌为主的一系列牙周病原菌有强力的抗菌作用,对治疗牙周炎有优良的临床效果。
药品特色1.药品直接施用(Drug Delivery System DDS)一般认为,口腔内给药最大的问题是在牙周部位保持有效的浓度,派丽奥牙科用软膏是一种牙周袋内直接给药疗效肯定的药品。
2.每周一次给药由于本药为缓解制剂,只需每周给药一次即足以维持治疗浓度。
3.高效灭细菌派丽奥牙科用软膏含有抗牙周炎病原菌的广谱药物-盐酸二甲胺四环素。
派丽奥牙科用软膏抑制牙周病原菌的成长,使牙龈更加健康。
使用本药后的药敏性试验表明不存在处于本药作用范围的耐性细菌或不敏感的细菌。
4.优异临床表现派丽奥牙科软膏不仅缓解炎症,如疼痛、红肿、出血和流脓,而且使牙周袋的深度变浅。
5.一次性使用派丽奥牙科软膏是一次性使用品,为了防止医院内交叉感染,每支注射器只限给1位患者使用一次。
6.不良反应少药品上市监察中,对3291位病人进行了评估,其中39位2病人(占百分之1.19)出现了不良反应,只要不良反应为施药时胀痛(34位病人,占百分之1.03)。
牙周用药派丽奥基本问题详细补充说明:牙周用药-派丽奥基本问题详细补充,希望对大家的临床用药有所帮助。
1、派丽奥的缓释机理?(派丽奥软膏与龈沟内的水分发生水合作用,形成网孔样被膜,不同直径大小的药物微分子球按不同时间缓慢、持续释放,小微分子球先释放出来)2、一支派丽奥有多少克?其中活性成分占多少?(0.5g每支,活性成分10mg,占2%)3、盐酸米诺环素是属于广谱抗生素药物还是窄谱抗菌药物?(广谱)4、如何判断派丽奥已经失效?(药物颜色变深、变棕色)5、派丽奥的有效成分?(盐酸二甲胺四环素/盐酸米诺环素)6、通常来讲一支派丽奥能够用于多少牙齿?(10颗牙左右)7、派丽奥生产商(日本Sunstar株式会社)8、派丽奥一般用于牙周袋深度几毫米以上(4毫米以上)9、派丽奥一个疗程多长时间,使用几次?(使用四次,效果显著,每周一次,共一个月)10、牙周基础治疗包括(洁治、深刮、药物治疗、松动牙固定等)11、派丽奥在牙周袋中保持有效浓度的时间(一周,168小时)12、派丽奥的禁忌证(禁忌证:对四环素过敏的患者不得使用)13、派丽奥为何不能应用于孕妇、哺乳期妇女和儿童(怀孕或可能怀孕的妇女使用本药品的安全性尚未确定,儿童使用本药品的安全性尚未确定(没有经过临床试验检验)14、注入派丽奥后产生疼痛的原因(药物从冰箱里取出没有放至室温,过冷刺激牙龈;上药速度过快压力过大;牙周组织处于急性炎症期等)15、派丽奥适应证(牙周炎(处于活动、或急性期)、牙周脓肿(急性、慢性)、慢性牙周炎(初诊时PD>5mm)、冠周炎、牙周手术、种植体周围炎(早期)、干槽症等)16、派丽奥用药前注意事项1)在使用本药前应把药物处于室温状态,以防止上药时冷刺激引起的疼痛。
盐酸米诺环素ARESTIN FDA说明书
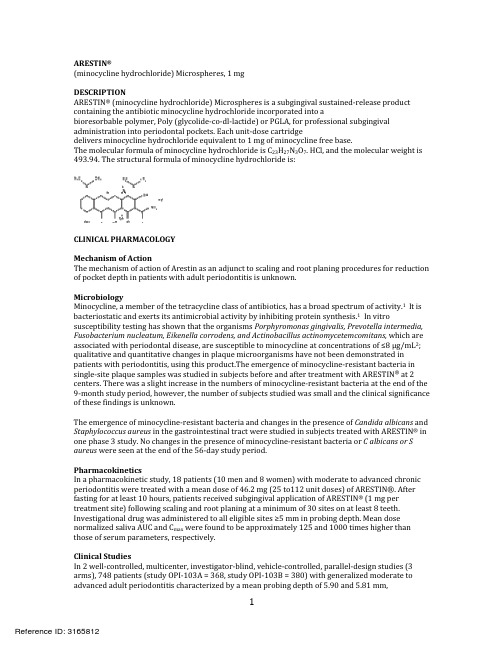
ARESTIN®(minocycline hydrochloride) Microspheres, 1 mgDESCRIPTIONARESTIN® (minocycline hydrochloride)Microspheres is a subgingival sustained‐release product containing the antibiotic minocycline hydrochloride incorporated into abioresorbable polymer, Poly (glycolide‐co‐dl‐lactide) or PGLA, for professional subgingivalpockets. Each unit‐dose cart dgeadministration into periodontal ridelivers minocycline hydrochloride equivalent to 1 mg of minocycline free base.The molecular formula of minocycline hydrochloride is C23H27N3O7. HCl, and the molecular weight is 493.94. The structural formula of minocycline hydrochloride is:CLINICAL PHARMACOLOGYMechanism of ActionThe mechanism of action of Arestin as an adjunct to scaling and root planing procedures for reduction of pocket depth in patients with adult periodontitis is unknown.MicrobiologyMinocycline, a member of the tetracycline class of antibiotics, has a broad spectrum of activity.1 It is bacteriostatic and exerts its antimicrobial activity by inhibiting protein synthesis.1 In vitro susceptibility testing has shown that the organisms Porphyromonas gingivalis,Prevotella intermedia, Fusobacterium nucleatum,Eikenella corrodens,and Actinobacillus actinomycetemcomitans, which are associated with periodontal disease, are susceptible to minocycline at concentrations of≤8 µg/mL2; qualitative and quantitative changes in plaque microorganisms have not been demonstrated in patients with periodontitis,using this product.The emergence of minocycline‐resistant bacteria in single‐site plaque samples was studied in subjects before and after treatment with ARESTIN® at2 centers. There was a slight increase in the numbers of minocycline‐resistant bacteria at the end of the 9‐month study period, however, the number of subjects studied was small and the clinical significance of these findings is unknown.The emergence of minocycline‐resistant bacteria and changes in the presence of Candida albicans and Staphylococcus aureus in the gastrointestinal tract were studied in subjects treated with ARESTIN® in one phase 3 study. No changes in the presence of minocycline‐resistant bacteria or C albicans or S aureus were seen at the end of the 56‐day study period.PharmacokineticsIn a pharmacokinetic study, 18 patients (10 men and 8 women) with moderate to advanced chronic periodontitis were treated with a mean dose of 46.2 mg (25 to112 unit doses) of ARESTIN®. After fasting for at least 10 hours, patients received subgingival application of ARESTIN® (1 mg per treatment site)following scaling and root planing at a minimum of 30 sites on at least 8 teeth. Investigational drug was administered to all eligible sites ≥5 mm in probing depth. Mean dose normalized saliva AUC and C max were found to be approximately 125 and 1000 times higher than those of serum parameters, respectively.Clinical StudiesIn 2 well‐controlled, multicenter, investigator‐blind, vehicle‐controlled, parallel‐design studies (3 arms), 748 patients (study OPI‐103A = 368, study OPI‐103B = 380) with generalized moderate to advanced adult periodontitis characterized by a mean probing depth of 5.90 and 5.81 mm,respectively, were enrolled. Subjects received 1 of 3 treatments: (1) scaling and root planing, (2) scaling and root planing + vehicle (bioresorbable polymer, PGLA), and (3) scaling and root planing + ARESTIN®. To qualify for the study, patients were required to have 4 teeth with periodontal pockets of 6 to 9 mm that bled on probing. However, treatment was administered to all sites with mean probing depths of 5mm or greater. Patients studied were in good general health. Patients with poor glycemic control or active infectious diseases were excluded from the studies. Retreatment occurred at 3 and 6 months after initial treatment, and any new site with pocket depth ≥5 mm also received treatment. Patients treated with ARESTIN® were found to have statistically significantly reduced probing pocket depth compared with those treated with SRP alone or SRP +vehicle at9 months after initial treatment, as shown in Table 1.Table1:Probing Pocket Depth at Baseline and Change in Pocket Depth at 9 Months From 2 Multicenter US Clinical TrialsTime Study OPI‐103A (N=368) Study OPI‐103B (N=380)SRP+ SRP+SRP+ SRP SRP + SRP+Alone Vehicle ARESTIN® Alone Vehicle ARESTIN®n=124 n=123 n=121 n=126 n=126 n=128PD (mm) at Baseline 5.88 5.91 5.88 5.79 5.82 5.81 [Mean ± SE] ±0.04 ±0.04 ±0.04 ±0.03 ±0.04 ±0.04PD (mm) Change from Baseline ‐1.04 ‐0.90 ‐1.20*†† ‐1.32 ‐1.30 ‐1.63**††at 9 Months ±0.07 ±0.54 ±0.07 ±0.07 ±0.07 ±0.07 [Mean ±SE]SE = standard error; SRP = scaling and root planing; PD= pocket d e pth.Significantly different from SRP *(P ≤0.05); **(P ≤0.001).Significantly different from SRP + vehicle †(P ≤0.05); ††(P ≤0.001).In these 2 studies, an average of29.5 (5‐114), 31.7 (4‐137), and 31 (5‐108) sites were treated at baseline in the SRP alone, SRP + vehicle, and SRP+ ARESTIN® groups, respectively. When these studies are combined, the mean pocket depth change at 9 months was ‐1.18 mm, ‐1.10 mm, and ‐1.42 mm for SRP a l one, SRP + vehicle, and SRP+ ARESTIN®, respectively.Table2: Numbers (percentage) of Pockets Showing a Change of Pocket Depth ≥2 mm at9 Months From 2 Multic e nt e r US Clinical TrialsStudy OPI‐103A Study OPI‐103BSRP SRP + SRP + SRP SRP + SRP +Alone Vehicle ARESTIN®Alone Vehicle ARESTIN®Pockets 1046 927 1326 1692 1710 2082≥2 mm (31.1%) (25.7%) (36.5%) (42.2%) (40.0%) (51.0%) (% of total)Pockets 417 315 548 553 524 704≥3 mm (12.4%) (8.7%) (15.1%) (13.8%) (12.3%) (17.3%) (% of total)SRP + ARESTIN® resulted in a greater percentage of pockets showing a change ofPD ≥2 mm and ≥3 mm compared to SRP alone at9 months, as shown in Table 2.Table3:Mean Pocket Depth Changes (SE) in Subpo p ulations, Studies 103A and103B CombinedSRP SRP + SRP +Alone Vehicle ARESTIN®Smokers n = 91 n = 90 n = 90‐0.96 (± 0.09) mm ‐0.98 (± 0.07) mm ‐1.24 (± 0.09) mm** o ers n = 159 n = 159 Nonsm k n = 159‐1.31 (± 0.06) mm ‐1.17 (± 0.07) mm ‐1.53 (± 0.06) mm**Patients >50 YOA n = 21 n = 81 n = 107‐1.07 (± 0.09) mm ‐0.92 (±0.08) mm ‐1.42 (±0.08)mm**Patients ≥50 YOA n = 167 n = 168 n = 142‐1.24 (±0.06) mm ‐1.19 (±0.06) mm ‐1.43 (±0.07) mm* Patients With CV Disease n = 36 n = 29 n = 36‐0.99 (±0.13) mm ‐1.06 (± 0.14) mm ‐1.56 (±0.14) mm** Patients W/O CV Disease n = 214n = 220 n = 213‐1.22 (±0.06) mm‐1.11 (±0.05) mm ‐1.40 (±0.06) mm**SRP = scaling and root planing; YOA= years of age; CV = cardiovascular.*SRP vs SRP +ARESTIN®P ≤0.05; **SRP vs SRP+ ARESTIN®P ≤0.001.In both studies, the following patient subgroups were prospectively analyzed: smokers, patients over and under 50 years of age, and patients with a previous history of cardiovascular disease. The results of the combined studies are presented in Table 3.In smokers, the mean reduction in pocket depth at 9 months was less in all treatment groups than in nonsmokers, but the reduction in mean pocket depth at 9 months with SRP + ARESTIN® was significantly greater than with SRP +vehicle or SRP alone.Table4:Mean Pocket Depth Change in Patients With Mean Baseline PD ≥5 mm,≥6 mm, and ≥7 mm at 9 Months From 2 Multicenter US Cli n cal Tria si lStudy OPI‐103A Study OPI‐103BMean Baseline Pocket DepthSRPAloneSRP +VehicleSRP +ARESTIN®SRPAloneSRP +VehicleSRP +ARESTIN®≥5 mm(n) ‐1.04 mm ‐0.09 mm(124) (123)‐1.20 mm*(121)‐1.32 mm(126)‐1.30 mm(126)‐1.63 mm*(128)≥6 mm (n) ‐0.91 mm ‐0.77 mm(34) (46)‐1.40 mm*(45)‐1.33 mm(37)‐1.46 mm(40)*‐1.69 mm(25)≥7 mm ‐1.10 mm ‐0.46 mm ‐1.91 mm ‐1.72 mm ‐1.11 mm ‐2.84 mm(n) (4) (5) (3) (3) (3) (2)*Statistically significant comparison between SRP +ARESTIN® and SRP alone.The combined data from these 2 studies also show that for pockets 5 mm to 7 mm at baseline, greater reductions in pocket depth occurred in pockets that were deeper at baseline.INDICATIONS AND USEARESTIN® is indicated as an adjunct to scaling and root planing procedures for reduction of pocket depth in patients with adult periodontitis.ARESTIN® may be used as part of a periodontal maintenance program which includes good oral hygiene, and scaling and root planing.CONTRAINDICATIONSARESTIN® should not be used in any patient who has a known sensitivity to minocycline or tetracyclines.WARNINGSTHE USE OF DRUGS OF THE TETRACYCLINE CLASS DURING TOOTH DEVELOPMENT (LAST HALF OF PREGNANCY, INFANCY, AND CHILDHOOD TO THE AGE OF 8 YEARS) MAY CAUSE PERMANENT DISCOLORATION OF THE TEETH (YELLOW‐GRAY BROWN). This adverse reaction is more common during long‐term use of the drugs, but has been observed following repeated short‐term courses. Enamel hypoplasia has also been reported. TETRACYCLINE DRUGS, THEREFORE, SHOULD NOT BE USED IN THIS AGE GROUP, OR IN PREGNANT OR NURSING WOMEN,UNLESS THE POTENTIAL BENEFITS ARE CONSIDERED TO OUTWEIGH THE POTENTIAL RISKS. Results of animal studies indicate that tetracyclines cross the placenta, are found in fetal tissues, and can have toxic effects on the developing fetus (often related to retardation of skeletal development). Evidence of embryotoxicity has also been noted in animals treated early in pregnancy. If any tetracyclines are used during pregnancy, or if the patient becomes pregnant while taking this drug, the patient should be apprised of the potential hazard to the fetus. Photosensitivity manifested by an exaggerated sunburn reaction has been observed in some individuals taking tetracyclines. Patients apt to be exposed to direct sunlight or ultraviolet light should be advised that this reaction can occur with tetracycline drugs, and treatment should be discontinued at the first evidence of skin erythema.PRECAUTIONSHypersensitivity ReactionsHypersensitivity reactions that included, but were not limited to anaphylaxis, angioneurotic edema, urticaria, rash, swelling of the face and pruritus have been reported with the use of ARESTIN®. Some of these reactions were serious. Post‐marketing cases of anaphylaxis and serious skin reactions such as Stevens‐Johnson syndrome and erythema multiforme have been reported with oral minocycline.Autoimmune SyndromesTetracyclines, including oral minocycline, have been associated with the development of autoimmune syndromes including a Lupus‐like syndrome manifested by arthralgia, myalgia,rash, and swelling. Sporadic cases of serum sickness have presented shortly after oral minocycline use, manifested by fever, rash, arthralgia, and malaise. In symptomatic patients, liver function tests, ANA, CBC,and other appropriate tests should be performed to evaluate the patients. No further treatment with ARESTIN®should be administered to the patient.The use of ARESTIN® in an acutely abscessed periodontal pocket has not been studied and is not recommended.While no overgrowth by opportunistic microorganisms, such as yeast, were noted during clinical studies, as with other antimicrobials, the use of ARESTIN® may result in overgrowth of nonsusceptiblemicroorganisms including fungi. The effects of treatment for greater than 6 months has not been studied.ARESTIN® should be used with caution in patients having a history of predisposition to oral candidiasis. The safety and effectiveness of ARESTIN®has not been established for the treatment of periodontitis in patients with coexistent oral candidiasis. ARESTIN® has not been clinically tested in immunocompromised patients (such as those immunocompromised by diabetes, chemotherapy, radiation therapy, or infection with HIV).If superin ect on is suspected, appropriate measures should bf i e taken.ARESTIN has not been clinically tested in pregnant women.®ARESTIN® has not been clinically tested for use in the regeneration of alveolar bone, either in preparation for or in conjunction with the placement of endosseous (dental)implants or in the treatment of failing implants.Information for PatientsAfter treatment, patients should avoid chewing hard, crunchy, or sticky foods (i.e., carrots, taffy, and gum) with the treated teeth for 1 week, as well as avoid touching treated areas. Patients should also postpone the use of interproximal cleaning devices around the treated sites for 10 days after administration of ARESTIN®. Patients should be advised that although some mild to moderate sensitivity is expected during the first week after SRP and administration of ARESTIN®, they should notify the dentist promptly if pain, swelling, or other problems occur. Patients should be notified to inform the dentist if itching, swelling, rash, papules, reddening, difficulty breathing, or other signs and symptoms of possible hypersensitivity occur.Carcinogenicity,Mutagenicity,Impairment of FertilityDietary administration of minocycline in long‐term tumorigenicity studies in rats resulted in evidence of thyroid tumor production. Minocycline has also been found to produce thyroid hyperplasia in rats and dogs. In addition, there has been evidence of oncogenic activity in rats in studies with a related antibiotic, oxytetracycline (i.e., adrenal and pituitary tumors). Minocycline demonstrated no potential to cause genetic toxicity in a battery of assays which included a bacterial reverse mutation assay (Ames test), an in vitro mammalian cell gene mutation test (L5178Y/TK+/‐ mouse lymphoma assay), an in vitro mammalian chromosome aberration test, and an in vivo micronucleus assay conducted in ICR mice.Fertility and general reproduction studies have provided evidence that minocycline impairs fertility in male rats.Teratogenic Effects: Pregnancy Category D. (See WARNINGS)Labor and DeliveryThe effects of tetracyclines on labor and delivery are unknown.Nursing MothersTetracyclines are excreted in human milk.Because of the potential for serious adverse reactions in nursing infants from the tetracyclines, a decision should be made whether to discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother. (See WARNINGS)Pediatric UseSince adult periodontitis does not affect children, the safety and effectiveness of ARESTIN® in pediatric patients cannot be established.ADVERSE REACTIONSThe most frequently reported nondental treatment‐emergent adverse events in the3 multice n ter US trials were headache, infection, flu syndrome, and pain.Table5: Adverse Events(AEs) Reported in ≥3% of the Combined Clinical Trial Population of 3 Multicenter US Trials by Treatment GroupNumber (%) of Patients Treatment‐emergent AEsTotal Number of AEs 987Periodontitis16.3%Tooth Disorder 12.3%Tooth Caries9.9%Dental Pain9.9%Gingivitis9.2%Headache9.0%Infection7.6%Stomatitis6.4%Mouth Ulceration 5.0%Flu Syndrome5.0%Pharyngitis4.3%Pain4.3%Dyspepsia SRPAloneN=250SRP +VehicleN=249SRP +ARESTIN®N=423 62.4% 71.9% 68.1%543 58925.6% 28.1%12.0% 13.7%9.2% 11.2%8.8% 8.8%7.2% 8.8%7.2% 11.6%8.0% 9.6%8.4% 6.8%1.6% 3.2%3.2% 6.4%3.2% 1.6%4.0% 1.2%2.0% 0 4.0%Infection Dental 4.0% 3.6%3.8%Mucous Membrane Disorder 2.4% 0.8% 3.3%The change in clinical attachment levels was similar across all study arms, suggesting that neither the vehicle nor ARESTIN® compromise clinical attachment.DOSAGE AND ADMINISTRATIONARESTIN® is provided as a dry powder, packaged in a unit‐dose cartridge with a deformable tip (see Figure 1), which is inserted into a spring‐loaded cartridge handle mechanism (see Figure 2) to administer the product.The oral health care professional removes the disposable cartridge from its pouch and connects the cartridge to the handle mechanism (see Figures 3‐4). ARESTIN® is a variable dose product, dependent on the size, shape, and number of pockets being treated. In US clinical trials, up to 122 unit‐dose cartridges were used in a single visit and up to 3 treatments, at 3‐month intervals, were administered in pockets with pocket depth of 5 mm or greater.Figure 1 Figure 2Figure 3 Figure 4The administration of ARESTIN® does not require local anesthesia. Professional subgingival administration is accomplished by inserting the unit‐dose cartridge to the base of the periodontal pocket and then pressing the thumb ring in the handle mechanism to expel the powder while gradually withdrawing the tip from the base of the pocket. The handle mechanism should be sterilized between patients. ARESTIN® does not have to be removed, as it is bioresorbable, nor is an adhesive or dressing required.HOW SUPPLIEDARESTIN® (minocycline hydrochloride)Microspheres, 1 mg is supplied as follows:• 1 unit‐dose cartridge with desiccant in a heat‐sealed, foil‐laminated pouch (NDC 65976‐100‐01)• 12 unit‐dose cartridges in 1 tray with desiccant in a heat‐sealed, foil‐laminated, resealable pouch (NDC 65976‐100‐24). There are 2 pouches in each boxEach unit‐dose cartridge contains the product identifier "OP‐1."Storage ConditionsStore at 20° to 25°C (68° to 77°F)/60% RH: excursions permitted to15° to 30°C (59° to 86°F). Avoid exposure to excessive heat.Rx onlyManufactured for OraPharma, Inc.5 Walnut Grove DriveHorsham, PA 19044For m o re information call 1‐866‐ARESTIN (1‐866‐273‐7846)REFERENCES:1. Stratton CW, Lorian V. Mechanisms of action of antimicrobial agents: general principles and mechanisms for selected classes of antibiotics. In:Antibiotics in Laboratory Medicine. 4th ed. Baltimore, Md: Williams and Wilkins; 1996. 2. Slots J, Rams TE. Antibiotics in periodontal therapy: adva n ta g es and dis a dvantages. J Clin Periodontol. 1990;17:479‐493.U.S. Pat. Nos. 6,682,3487,699,609AUS‐INS‐XXXXXXXXX。
盐酸米诺环素胶囊说明书
盐酸米诺环素胶囊盐酸米诺环素胶囊使用说明书•【药品名称】通用名称:盐酸米诺环素胶囊英文名称:Minocycline Hydrochloride Capsules•【成份】盐酸二甲胺四环素•【性状】本品为胶囊剂。
•【适应症】本品适用于因葡萄球菌、链球菌、肺炎球菌、淋病奈瑟菌、痢疾杆菌、大肠埃希菌、克雷伯氏菌、变形杆菌、绿脓杆菌、梅毒螺旋体及衣原体等对本品敏感的病原体引起的下列感染:1.败血症、菌血症。
2.浅表性化脓性感染:毛囊炎、脓皮症、扁桃体炎、肩周炎、泪囊炎、牙龈炎、外阴炎、创伤感染、手术后感染等。
3.深部化脓性疾病:乳腺炎、淋巴管(结)炎、颌下腺炎、骨髓炎、骨炎。
4.急慢性支气管炎、喘息型支气管炎、支气管扩张、支气管肺炎、细菌性肺炎、异型肺炎、肺部化脓症。
5.痢疾、肠炎、感染性食物中毒、胆管炎、胆囊炎。
6.腹膜炎。
7.肾盂肾炎、肾盂炎、肾盂膀胱炎、尿道炎、膀胱炎、前列腺炎、附睾炎、宫内感染、淋病。
8.中耳炎、副鼻窦炎、颌下腺炎。
9.梅毒。
•【规格】按米诺环素计:(1)50mg(5万单位)(2)100mg(10万单位)•【用法用量】口服。
成人首次剂量为0.2g,以后每12小时服用本品0.1g,或每6小时服用50mg。
•【不良反应】1.菌群失调:本品引起菌群失调较为多见。
轻者引起维生素缺乏,也常可见到由于白色念珠菌和其他耐药菌所引起的二重感染。
亦可发生难辨梭菌性假膜性肠炎。
2.消化道反应:食欲不振、恶心、呕吐、腹痛、腹泻、口腔炎、舌炎、肛门周围炎等;偶可发生食管溃疡。
3.肝损害:偶见恶心、呕吐、黄疸、脂肪肝、血清氨基转移酶升高、呕血和便血等,严重者可昏迷而死亡。
4.肾损害:可加重肾功能不全者的肾损害,导致血尿素氮和肌酐值升高。
5.影响牙齿和骨发育:本品可沉积于牙齿和骨中,造成牙齿黄染,并影响胎儿、新生儿和婴幼儿骨骼的正常发育。
6.过敏反应:主要表现为皮疹、荨麻疹、药物热、光敏性皮炎和哮喘等。
罕见全身性红斑狼疮,若出现,应立即停药并作适当处理。
派丽奥软膏治疗急性局限型智齿冠周炎的疗效观察
派丽奥软膏治疗急性局限型智齿冠周炎的疗效观察目的:观察派丽奥软膏(盐酸米诺环素软膏)治疗急性局限型智齿冠周炎的临床效果及不良反应。
方法:120例临床诊断为急性局限型智齿冠周炎的病人随机分为两组,治疗组在常规冲洗后局部使用派丽奥软膏,对照组在常规冲洗后局部使用碘甘油,用药后4 d观察疗效及不良反应。
治疗期间停用其他抗生素类药物。
结果:治疗组的治愈率(46.77%)、显效率(82.25%)均显著高于对照组(25.00%,55.00%),且未发现明显不良反应。
结论:派丽奥软膏治疗急性局限型智齿冠周炎安全、有效。
标签:药物治疗;智齿冠周炎;盐酸米诺环素冠周炎是口腔科常见疾病,临床上以下颌智齿冠周炎多见,智齿冠周炎如治疗不及时常扩散引起颌面部蜂窝组织炎、间隙感染等严重并发症[1]。
临床上多采用局部冲洗、上药,结合全身使用抗生素治疗。
本研究应用派丽奥软膏(主要成分为盐酸米诺环素)治疗急性局限型下颌智齿冠周炎,效果良好,报道如下:1资料与方法1.1一般资料选择临床确诊为急性局限型智齿冠周炎122例,男66例,女56例,年龄17~49岁。
临床表现为智齿冠周软组织红肿,有盲袋,袋内有炎性渗出或溢脓,疼痛剧烈。
不伴有间隙感染,无明显全身症状,无系统性疾病及1周内未用过抗生素类药物。
无扩散至间隙感染,无明显全身症状。
随机分为两组,其中,治疗组62例,对照组60例。
治疗组与对照组患者性别、年龄、病情分布等经统计学分析无显著性差异,具有可比性。
1.2方法用3%双氧水和生理盐水交替冲洗,干棉球擦干,派丽奥注入盲袋底,充盈。
治疗组患者的冠周组织用1%的碘酊消毒后,用探针轻轻分离龈瓣,排出分泌物,再用3%双氧水及生理盐水反复交替冲洗冠周及盲袋,至渗出液清亮为止,隔湿,擦干,将派丽奥软膏在冠周及盲袋底轻轻注入,直至袋口有软膏溢出,嘱患者1 h内不漱口,第4天复诊观察并记录疗效。
对照组用3%双氧水和生理盐水交替冲洗,干棉球擦干,将碘甘油导入冠周及盲袋,嘱患者1 h内不漱口,第2、3天复诊,以同样的方法处理1次,第4天观察疗效。
盐酸米诺环素软膏与碘甘油治疗智齿冠周炎的疗效比较
盐酸米诺环素软膏与碘甘油治疗智齿冠周炎的疗效比较【摘要】目的比较盐酸米诺环素软膏与碘甘油在治疗急性智齿冠周炎中的疗效。
方法对120例急性发作的智齿冠周炎,随机分为治疗组和对照组两组。
常规冠周冲洗后,治疗组将盐酸米诺环素软膏注入冠周龈袋或者盲袋内;对照组冠周龈袋或者盲袋内置入10%碘合剂。
5 d后复诊评价疗效。
结果治疗组的显效率和总有效率均较对照组高(P<0.01),无不良反应发生。
盐酸米诺环素软膏的疗效明显高于碘甘油组。
结论相对碘甘油,采用盐酸米诺环素软膏进行急性智齿冠周炎的治疗,具有一定的优越性。
【关键词】智齿冠周炎;盐酸米诺环素软膏;碘甘油智齿冠周炎是指智齿(第三磨牙) 萌出不全或阻生时,牙冠周围软组织发生的炎症,临床上以下颌智齿冠周炎多见,是口腔临床中的常见病、多发病[1]。
常规的治疗手段为局部冲洗、上药,结合静脉使用抗生素消炎治疗。
作者采用盐酸米诺环素软膏治疗智齿冠周炎,与碘甘油局部用药在治疗智齿冠周炎中的应用效果进行了比较,报告如下。
1 资料与方法1.1 一般资料2006~2011年诊断为急性冠周炎患者120例。
男56例,女64例,年龄18~45岁,平均30岁。
其中下颌第三磨牙近中阻生42例,颊侧阻生50例,垂直阻生28例。
临床表现为智齿冠周软组织红肿,疼痛,冠周龈袋或者盲袋内有炎性渗出物或溢脓,无扩散至间隙感染、无明显全身症状。
未使用过抗生素或此前做过局部治疗。
采用随机化数字表法进行排序,随机分为两组,其中治疗组62例,对照组58例。
实验组与对照组患者性别、年龄、病情分布等经统计学分析无显著性差异,两组构成均衡具有可比性。
1.2 材料2 %“ 盐酸米诺环素软膏” 牙科用软膏(商品名:派丽奥,日本S U N ,S T AR株式会社生产),对四环素过敏者禁用。
1.3 治疗方法冠周软组织以碘伏消毒后,用探针分离盲袋,排出炎性渗出液或脓液,用生理盐水和3%双氧水反复局部冲洗,隔湿。
治疗组将派丽奥软膏轻轻注入冠周及盲袋内,直到药物溢出为止;3 d后重复治疗1次,5 d 复诊。
派丽奥软膏治疗慢性牙周炎的临床疗效观察
派丽奥软膏治疗慢性牙周炎的临床疗效观察作者:李瑶徐静舒张玉皓来源:《中国医药导报》2008年第02期[摘要] 目的:评价派丽奥牙科用软膏治疗慢性牙周炎的临床效果。
方法:采用随机分组的方法,以单纯基础治疗者为对照组,评价将派丽奥牙周袋内用药辅助治疗牙周炎的疗效。
记录基线、用药后1、4和8周的菌斑指数(PLI)、牙龈出血指数(BI)和牙周探诊深度(PD),对数据进行统计学处理。
结果:实验组和对照组在基线时各临床指标无显著性差异(P>0.05),经龈下刮治及根面平整术后1周,实验组与对照组比较,基线PLI、BI、PD均有显著改善(P<0.05);辅助用药后,实验组与对照组比较,PLI 在用药后1 周有显著性差异,而4、8周则无显著性差异(P>0.05);BI 在用药后1周无显著性差异(P>0.05),但用药后4 周及8 周有显著性差异(P<0.05);PD 在用药后1、4 及8 周均有显著性差异(P<0.05)。
结论:牙周炎治疗以机械的洁、刮治疗为基础,派丽奥牙科用软膏局部辅助用药能够提高牙周炎治疗的效果。
[关键词] 牙周炎;派丽奥牙科用软膏;牙周治疗[中图分类号] R781.4 [文献标识码]A [文章编号]1673-7210(2008)01(b)-052-02牙周病是由牙菌斑中的微生物所引起的牙周支持组织的慢性感染性疾病,可导致牙周支持组织的炎症、牙周袋形成、附着丧失、牙槽骨吸收,最后可导致牙松动拔除,它是我国成年人牙齿丧失的首位原因,是口腔两大类疾病之一,在世界范围内均有较高的患病率,在我国的患病率更高,居于龋病之上[1],近年来,发病率呈逐渐增高的趋势[2]。
牙周病是局部感染性疾病,细菌及其产物是牙周病的主要致病因素。
用机械的方法去除牙体上的菌斑和牙石,是牙周炎的常规基础治疗方法。
而对与牙周病发生发展有关的特异性细菌的控制,正愈来愈受到临床医师的重视。
派丽奥牙科用软膏(又名盐酸米诺环素软膏)是一种治疗牙周炎的广谱抗菌缓释制剂。
米诺环素辅助治疗牙周炎前后牙龈卟啉单胞菌的定量检测

米诺环素辅助治疗牙周炎前后牙龈卟啉单胞菌的定量检测万君;李秋红;王如;韩焱;薄志坚【摘要】Objective Using the TaqMan Real -time PCR to compare between the scaling and root planting treatment (SRP) and SPR with minocycline hydrochloride for detection and quantification of Porphyromonas gingivalis (Pg) taken from subgingival plaque in moderate or severe chronic periodontitis .Methods We collected 50 cases of moderate to severe periodontitis patients , every patient's teeth were divided into two groups according to randomized control trial design as non-drug therapy (only SPR) and drug therapy (after SPR putting minocycline hydrochloride into periodontal pocket ).To measure the Index at baseline before SPR .1 and 3 months after SPR or SPR and drug treatment , subgingival plaque sam-ples were collected and detected and quantified by the measurements of TaqMan Real -time PCR.To analyze the data u-sing SPSS 11.5 software.Results (1) Constitution ratio of Pg of the two groups: before the treatment, the data of two groups were 68%;after treatment 1 month the SPR group was 30%, SPR with minocycline was 28%, 3 month the SPR group was 24%, SPR with minocycline was 22%, after treatment 1 month and 3 month were reduced comparing with the one before treatment, the result was statistically significant (P<0.05).Constitution ratio of Pg of the two groups after treatment 3 month was below the one of 1 months after treatment , the result was no statistically significant ( P>0.05) . Constituent ratio of Pg between the two groups showed no difference before and afterthe treatment 1 and 3 mouths,the result was no statistically significant (P>0.05).(2)The relationship between constituent ratio of Pg and the clinical index such as PD, BI and AL showed positive correlation, the result was statistically significant (P<0.05).Conclusion Periodontal disease whichis treated by SPR treatment or SPR with minocycline hydrochloride will reduce the number of Pg in subgingi -val plaque , and can maintain a therapeutic effect in three months .the SRP treatment plays a critical role and the improve-ment of clinical treatment effect using minocycline hydrochloride shows no obvious .%目的:对在基础治疗辅助米诺环素治疗慢性牙周炎前后,实时定量检测龈下菌斑中牙龈卟啉单胞菌( porphyromonas gingivalis ,Pg)占总细菌构成比。
派丽奥治疗牙周炎临床效果分析

派丽奥治疗牙周炎临床效果分析发布时间:2023-05-23T12:11:05.261Z 来源:《医师在线》2023年1月1期作者:李雪[导读]派丽奥治疗牙周炎临床效果分析李雪(徐州医科大学附属口腔医院;江苏徐州221000)【摘要】目的:探究对牙周炎患者实施派丽奥治疗的临床效果。
方法:自2018年8月到2019年8月入组90例牙周炎患者统计,组别:抽取对照组与实验组,前者碘甘油治疗,后者经派丽奥治疗,统计指标为有效性与治疗前后牙周情况等。
结果:治疗前,两组患者牙周指标无对比意义,P>0.05;对照组、实验组治疗后SBI、GI、PLI、MD、PD指标对比后者优于前者,实验组总有效人数多于对照组,P<0.05。
结论:对牙周炎患者实施派丽奥治疗后临床疗效得到明显改善,在短时间内恢复其牙齿功能,保证牙龈健康状态。
【关键词】牙周炎;派丽奥;临床疗效牙周炎是临床上确诊率较高的口腔疾病之一,临床对该病的治疗多采取机械化治疗去除牙结石与牙菌斑,但随着病情进展,患者的牙周袋深度增加,传统治疗方案难以保证良好的疗效[1]。
在随着医学水平的进步,临床逐步提出药物化学疗法干预,对其患病牙龈、牙齿使用局部缓释药治疗,充分改善患者的临床症状,恢复患者的口腔健康状态。
派丽奥是临床上应用较为广泛的口腔疾病治疗辅助药物之一,其可遇水变硬形成网孔状的被膜,从而保证牙周袋内药物的缓释,持续周期在一周以上。
上文收集90例牙周炎患者分析,统计经不同方案干预后患者的治疗有效性与牙周指标变化,具体内容汇报见下文。
1、资料与方法1.1临床数据择取2018年8月到2019年8月入组90例牙周炎患者探究,评估为实验组与对照组,前者男女患者例数比值为20:25,年龄在25-65岁区间,均值数据为(45.24±1.33)岁,后者女男患者例数比值为22:23,年龄在26-64岁区间,均值数据为(45.13±1.41)岁。
对年龄、性别基础资料比对无显著差异,汇总其年龄、性别等比较无显著差异,统计学无意义,P>0.05。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
盐酸米诺环素软膏(派丽奥)的说明书
日常生活中所说的五官是指眼鼻口耳喉,但是中医当中所说的五官却不是这么简单的了。
很多医院就设有五官科,但是如果细分的话可以分为耳鼻喉科和眼科,这些都是属于五官科的范畴。
目前治疗五官类疾病往往采用药物进行治疗,今天,我们为您推荐一种叫做盐酸米诺环素软膏(派丽奥)的药物,它对于五官疾病治疗效果显著。
【药品名称】
通用名称:盐酸米诺环素软膏
商品名称:盐酸米诺环素软膏(派丽奥)
英文名称:Minocycline Hydrochloride Ointment
拼音全码:YanSuanMiNuoHuanSuRuanGao(PaiLiAo)
【主要成份】7一二甲胺四环素。
【性状】本药为淡黄色软膏,无臭、味苦。
充填在口腔用注射器内。
【适应症/功能主治】改善对本品具有药敏性的牙龈卟啉菌、中间型普氏、产黑色素普氏菌、腐蚀埃肯菌、核梭杆菌、二氧化碳噬纤维菌、伴放线放线杆菌所致牙周炎(慢性边缘性牙周炎)的各种症状。
【规格型号】0.5g*5支
【用法用量】洁治或龈下刮治后,将软膏注满患部牙周袋内,每周一次,连续用四次,效果最好。
本品为一次性用品。
【不良反应】调查了使用本药的227颗牙齿中有4颗牙认为有局部刺激,都是在牙周袋内注射后即刻出现的,随即消失属于一过性的。
在使用本药病例中,经一般血液检查的148例中,均未发现异常现象。
【禁忌】对四环素类抗生素有过敏史的患者。
【注意事项】1.过敏反应必须注意观察,一旦出现过敏征兆(搔
痒,发红,肿胀,丘疹,水泡等)即停止用药。
2.局部如出现耐药性或不敏感菌所致的感染症应停止用药。
3.只限用于牙科。
4.使用时:1)用药前去除软垢,龈上菌斑及牙石。
2)为了使药物充满牙周袋,需将注射器的头部轻插至牙周袋底部。
3)注药后不得立即漱口及进食。
5.注药时,患部可能出现一时刺激或疼痛,缓慢注药可明显减轻此症状。
6.如症状不见改善,应改用其他疗法。
【儿童用药】尚不明确。
【老年患者用药】尚不明确。
【孕妇及哺乳期妇女用药】对孕妇及哺乳期妇女用药的安全性尚未肯定。
因此必须断定治疗上有益性超过危险性时方可用药。
【药物相互作用】如与其他药物同时使用可能会发生药物相互作用,详情请咨询医师或药师。
【药物过量】本药的注射器中含药量很少,过量使用的可能性很小。
但是万一过量摄取,要进行洗胃以及随即处置。
没有特异的解毒剂。
【药理毒理】
1.盐酸二甲胺四环素对葡萄球菌、肺炎杆菌等革兰阳性菌以及大肠杆菌、克雷杆菌、肠杆菌等革兰氏阴性菌具有广谱抗菌作用。
其作用机理为阻止细菌的蛋白合成而发挥抗菌作用。
2.盐酸二甲胺四环素能明显抑制与破坏牙周组织和形成牙周袋
有关的胶原酶的活性水平。
【药代动力学】
1.牙周袋内浓度给牙周炎患者的牙周袋内注入本药,每个牙齿约0.05ml(盐酸二甲胺四环素1.3mg效价)注药后牙周袋的药物浓度可维持长时间,168小时(7天)后仍有0.1μg/ml。
2.血清中浓度健康成人一次投入本药0.5g,血清中盐酸二甲胺四环素最高浓度为0.19μg/ml,达峰时间为2小时。
给牙周炎患者每次0.5g,每周一次,共用四周,第一次及第四次用药后4小时,血清中盐酸二甲胺四环素浓度约0.1μg/ml,但第四次用药前未检查出。
【贮藏】密封。
【包装】10mg(效价)/0.5g/支*5支/盒。
【有效期】24 月
【批准文号】H20100244
【生产企业】Sunstar INC Japan(日本)
看完上面的内容,您对于盐酸米诺环素软膏(派丽奥)这种五官类药物有了一个比较全面的了解了吗?五官是人们心灵的窗户,外表的健康与否直接跟内心挂钩,因此,大家要重视五官疾病的治疗,及时服用药物可以有效治愈五官疾病。