Intravenous Paraquat Poisoning
阿维菌素与有机磷农药混配中毒的临床研究

于接触组(JP<O.01),混配农药中毒高于有机磷农药中 毒组(P<0.01),两者比较差异有统计学意义(P< 0.0I)。提示有机磷中毒和混配后农药巾毒均可产生全 身炎症反应,进一步说明全身炎症反应是各种中毒危重 症中不可忽视的问题。
eonl州¥Oll phnsphorus pesticide.and search for∞effective detoxification method.Methods The
study of 59 cases with acute poisoning by
hybrid biolo画eal pesticide almrn∞tin mixed organophosphons pesticide.and the blood biochemical index,eholinemerase,plasma inflammatory
与第3组比较,差异无统汁学意义(P>0.05)。CHE 活性测定、CRP与APACHE II评分3组问,差异有统
有不同程度的眼部症状,用氯霉素眼药后第2 d均缓 计学意义(P<O.01)。
解。第2、第3组均以有机磷中毒症状为主,第3组临床 表1 实验室数据比较(i±s)
。。.
“”’
“
第1 d
CHE活性(U/1.) 第2 tl
出现焦虑、烦躁、嗜睡、精神抑郁、惊厥、共济失调,甚评分的分值差异有统计学意义,与姜红等…研究结果相
至昏迷等神经系统症状¨。】。阿维菌素经皮毒性较
符。这与国内外一些学者对危重病评价中的研究结果
小,对眼睛及皮肤的刺激性较大。尤其对眼睛角膜呵 相符p。81,表明该评分能预测中毒患者的预后。③CRP
造成不可逆的损伤。有机磷农药与阿维菌素混配后是一种非常敏感的炎症和组织损伤标记物¨1。由于有
血必净注射液对急性百草枯中毒患者的多器官保护作用

2005
ⅣAⅣG沌,ZH以。胁挖. E聊rgP,王掣D印口疗僦疗t D,Sk挖∥行g胁印i缸z D,吼i咒口
to【)ecember patients).
201 O
were
randomly
divided
into
treatment
group
(18 patients)and control group(17 treatment group,besides intravenous drip, twice
。297。
病史。入院后按随机原则分为对照组(17例)和治疗 组(18例),两组患者的年龄、服药量、服药后至就诊
时间、发生急性呼吸窘迫综合征(ARDS)和多器官
比较(表2):与对照组比较,治疗组3 d时血浆 MDA水平低于对照组,7 d时二者比较差异仍有统
计学意义(均P<0.05);治疗组治疗3、7、14 d时血
I、Ⅱ型上皮细胞被破坏,肺泡间隔内大量中性粒细 胞浸润,形成广泛的肺泡炎。此后逐渐出现广泛肺泡
1.3检测指标及方法:①动态监测动脉血氧饱和度 (SaO。)、肾功能、肝功能、心肌酶学;②2个或2个
以上器官功能障碍,无干预情况下不能维持内环境
稳定的为MODS,比较两组患者的病死率;③检测 血浆丙二醛(MDA)和超氧化物歧化酶(SOD)水平, 严格按照试剂盒说明书操作。 1.4统计学方法:应用SPSS 16.o统计软件处理数 据。计量资料以均数土标准差(z士s)表示,组间比较 采用成组设计t检验;计数资料比较采用影检验; 尸<O.05为差异有统计学意义。
保护胃肠道黏膜及大剂量糖皮质激素治疗,并尽早
行血流灌流(HP),每日3 h,连用5 d。治疗组在以上 3讨论
去甲肾上腺素在百草枯中毒致肺纤维化小鼠模型中的作用研究
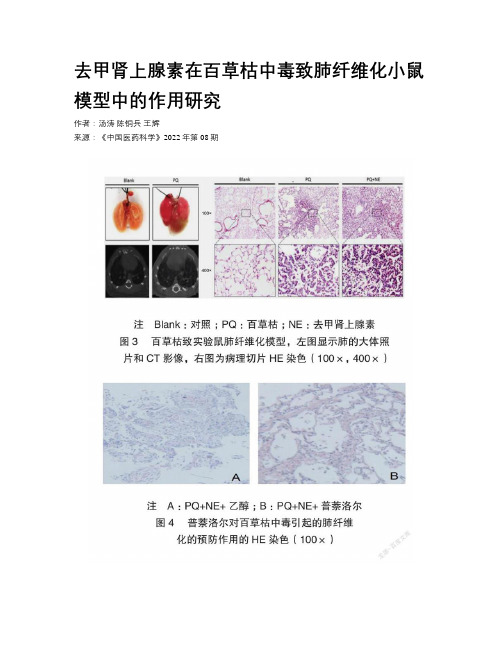
去甲肾上腺素在百草枯中毒致肺纤维化小鼠模型中的作用研究作者:汤涛陈铜兵王辉来源:《中国医药科学》2022年第08期[摘要]目的探讨去甲肾上腺素(NE)在百草枯中毒导致肺纤维化中的作用。
方法选取苏州大学附属第三医院急诊科收治的41例百草枯中毒患者和6只实验小鼠的血浆,實验组和对照组小鼠各3只,实验组用百草枯处理,高效液相色谱电化学法检测血浆中 NE 浓度。
采用微渗透泵构建小鼠模型,实验组9只,对照组小鼠3只,实验组用百草枯加 NE 处理,对照组仅用百草枯处理。
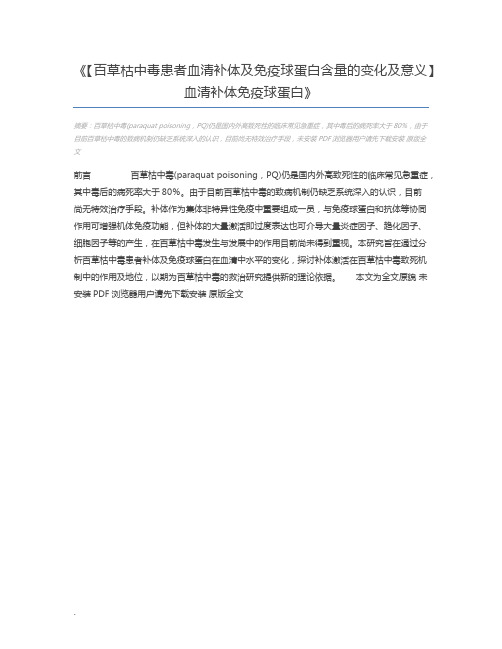
模拟 NE 受体阻断剂普萘洛尔对百草枯中毒引起的肺纤维化模型,实验组和对照组小鼠各18只,实验组用百草枯加 NE 加普萘洛尔处理,对照组中普萘洛尔换成等量的乙醇。
结果研究显示百草枯中毒患者的 NE 水平显著提高,而中毒实验小鼠 NE 并没有提高。
体外细胞实验显示, NE 在体外可诱导人肺泡Ⅱ型上皮细胞发生上皮间质转化,从而协同百草枯中毒致肺纤维化,小鼠实验发现实验组用 NE 处理的小鼠肺纤维化程度高于对照组。
普萘洛尔实验显示,实验组加了普萘洛尔后百草枯中毒小鼠的肺纤维化程度明显低于对照组。
结论 NE 可能是导致临床百草枯中毒致肺纤维化疗效不佳的重要原因,普萘洛尔在临床上对百草枯中毒所致的肺纤维化有一定的预防作用。
[关键词]百草枯;肺纤维化;去甲肾上腺素;间质转化;普萘洛尔[中图分类号] R965 [文献标识码] A [文章编号]2095-0616(2022)08-0027-05The study on effect of norepinephrine in mouse models of pulmonary fibrosis induced by paraquat poisoningTANG Tao CHEN Tongbing WANG HuiDepartment of Pathology,the First People’s Hospital of Changzhou, Jiangsu, Changzhou 213003, China[Abstract] Objective To investigate the effect of norepinephrine in pulmonary fibrosis induced by paraquat poisoning. Methods The plasma of 41 paraquat poisoning patients who were admitted to the emergency department of the Third Affiliated Hospital of Soochow University and plasma of 6 experimental mice were selected, with 3 mice each in the experimental group and the control group. The experimental group was treated with paraquat, and the high-performance liquid chromatographywith electrochemical detection was used to determine the concentration of norepinephrine in plasma.A micro-osmotic pump was used to construct a mouse model, with 9 mice in the experimental group and 3 mice in the control group. The experimental group was treated with paraquat plus norepinephrine, and the control group was treated with paraquat only. A model of pulmonary fibrosis induced by paraquat poisoning with propranolol, a norepinephrine receptor blocker, was established. There were 18 mice in each of the experimental group and the control group. The experimental group was treated with paraquat plus norepinephrine plus propranolol, and propranolol in the control group was replaced with the same amount of ethanol. Results The study showed that the level of norepinephrine in paraquat poisoned patients was significantly increased, while it did not increase in poisoned experimental mice. In vitro cell experiments showed that norepinephrine induced epithelial-mesenchymal transition in human alveolar type Ⅱ epithelial cells in vitro, thereby cooperating with paraquat poisoning to induce pulmonary fibrosis. Experiments in mice found that the degree of pulmonary fibrosis in mice treated with norepinephrine in the experimental group was higher than that in the control group. The propranolol experiment showed that the degree of pulmonary fibrosis in the paraquat poisoned mice in the experimental group with addition of propranolol was significantly lower than that of the control group. Conclusion Norepinephrine may be an important reason for the poor efficacy of clinical pulmonary fibrosis induced by paraquat poisoning. Propranolol has a certain clinical preventive effect on pulmonary fibrosis induced by paraquat poisoning.[Key words] Paraquat; Pulmonary fibrosis; Norepinephrine; Mesenchymal transition; Propranolol百草枯(paraquat, PQ)中毒是较常见的农药中毒之一,毒性可累及全身多个脏器,但主要以肺为靶器官,早期临床表现为急性肺损伤,后期可出现肺泡内和肺间质纤维化[1-2]。
血必净注射液疗百草枯中毒患者疗效观察

department had admitted 49
poisoning.We randomly
divided these patients into two only
one
groups had received the routine
treatment,and
observed
group had
received the additional
周的动脉血气,肝功能,肾功能,死亡率的变化及趋势,并将两组进行比较。
结果
血必净治疗组与常规治疗组患者相比较,前者不同时间段的血肌酐、黄疸指 数水平明显低于对照组。血必净治疗组患者的动脉血氧分压的下降水平和速度远 较对照组平缓。血必净治疗组患者各个时间段及总死亡率远较对照组低。
结论
在常规规范化治疗的基础上使用血必净可以明显改善百草枯中毒患者的 肝、肾功能损伤,减轻急性肺损害,降低患者的死亡率。
指导教师签名:
日
期:
基一
・论文・
血必净注射液治疗百草枯中毒患者疗效观察
刖吾 百草枯(Paraquat,PQ),是吡啶类除草剂,有效成分为:1.1—4.4-二联吡啶。 是目前全世界使用最广泛的除草剂之一,皮肤接触,呼吸道吸入和口服均可造成 中毒,且百草枯中毒无特殊解毒剂。人口服致死量为30—40mg/kg【11。百草枯中毒 患者大多有急性肝、肾功能衰竭,急性肺泡炎和不可逆转的肺纤维化等重要脏器 损害,死亡率极高。血必净是一种新型的中药注射液,药理证明,活血化瘀药能 改善微循环,减少血小板聚集,减少炎性渗出,改善局部血液循环,增强网状内 皮细胞的吞噬和吸附能力。此外,还有研究显示,血必净具有强效抗内毒素作 用,提高超氧化物歧化酶活性,调节过高或过低的免疫反应‘21。 本文通过对我院急诊科从2007年1月至tJ2009年3月收治入院治疗的49位的百草 枯中毒患者使用血必净注射液治疗的疗效分析,观察血必净治疗对百草枯毒患者
血必净注射液联合乙酰半胱氨酸对急性百草枯中毒肝肾损伤的作用

血必净注射液联合乙酰半胱氨酸对急性百草枯中毒肝肾损伤的作用龚升玄;魏书堂【期刊名称】《西北药学杂志》【年(卷),期】2024(39)1【摘要】目的探讨血必净注射液联合乙酰半胱氨酸(acetylcysteine,AC)对急性百草枯中毒(acute paraquat poisoning,APP)肝肾损伤的作用。
方法回顾性分析救治的80例APP患者的临床资料,按治疗方式不同分为AC组(n=39,常规治疗联合AC)、联合组(n=41,在AC组治疗的基础上加用血必净注射液)。
比较2组治疗前、治疗2周后呼吸指标[动脉血氧分压(PaO_(2))、氧合指数]、炎症因子水平[白细胞介素-6(interleukin-6,IL-6)、转化生长因子β_(1)(transforming growth factor-β_(1),TGF-β_(1))]和肝肾功能指标[丙氨酸氨基转移酶(glutamic pyruvic transaminase,GPT)、天冬氨酸氨基转移酶(glutamic oxaloacetic transaminase,GOT)、血肌酐(serum creatinine,Scr)和肾小球滤过率(estimated glomerular filtration rate,eGFR)],并观察预后。
结果治疗后,2组PaO_(2)、氧合指数和eGFR均较治疗前明显升高(P<0.05),且联合组均明显高于AC组(P<0.05);治疗后,2组血清IL-6、TGF-β_(1)水平和GPT、GOT、Scr均较治疗前明显降低(P<0.05),且联合组均明显低于AC组(P<0.05);联合组1个月内脏器功能衰竭发生率(32.56%vs.56.41%)、病死率(60.98%vs.82.05%)均明显低于AC组(P<0.05)。
结论血必净注射液联合AC治疗APP,可明显减轻肝肾损伤,有效抑制炎症反应,显著提高患者的存活率。
【百草枯中毒患者血清补体及免疫球蛋白含量的变化及意义】 血清补体免疫球蛋白
《【百草枯中毒患者血清补体及免疫球蛋白含量的变化及意义】
血清补体免疫球蛋白》
摘要:百草枯中毒(paraquat poisoning,PQ)仍是国内外高致死性的临床常见急重症,其中毒后的病死率大于80%,由于
目前百草枯中毒的致病机制仍缺乏系统深入的认识,目前尚无特效治疗手段,未安装PDF浏览器用户请先下载安装原版全
文
前言百草枯中毒(paraquat poisoning,PQ)仍是国内外高致死性的临床常见急重症,其中毒后的病死率大于80%。
由于目前百草枯中毒的致病机制仍缺乏系统深入的认识,目前
尚无特效治疗手段。
补体作为集体非特异性免疫中重要组成一员,与免疫球蛋白和抗体等协同
作用可增强机体免疫功能,但补体的大量激活即过度表达也可介导大量炎症因子、趋化因子、
细胞因子等的产生,在百草枯中毒发生与发展中的作用目前尚未得到重视。
本研究旨在通过分
析百草枯中毒患者补体及免疫球蛋白在血清中水平的变化,探讨补体激活在百草枯中毒致死机
制中的作用及地位,以期为百草枯中毒的救治研究提供新的理论依据。
本文为全文原貌未
安装PDF浏览器用户请先下载安装原版全文
.。
PQP诊治专家共识与规范(协和)

HD+HP 住院几天后,症状好转,血PQ浓度0.03mg/L 8.29右肺移植 9.1(术后48h,出现中毒症状后21天)血PQ浓度0.2mg/L,较前升高7倍
9.3(术后4d,出现中毒症状后23天)移植肺出现渗出性病变,肺活检考虑PQ损害 ECMO+HP+间断HD
9.12(术后13d,出现中毒症状后32天)血PQ水平很低
百草枯中毒诊治共识与规范
河北医科大学第二医院急诊科 田英平
急性百草枯中毒诊治专家共识
• 我国急性中毒第一个急诊同道的共识 • 中国急诊医师协会,中国急救医学 ,2013,33(6):484-489 • 共识与指南?所知有限,为共识。 • 共识讨论两年余,共识可否成为规范? • 尚有距离!
共识解读与规范
坚持了服毒量分级依据 服毒量判断困难与局限 通常一口按致死量处理是合适的 血尿毒检的意义与现实距离
分级标准的认同共识
轻型 摄入百草枯的量<20毫克/kg体重 中重型 摄入百草枯量>20 ~40毫克/kg体重 暴发型 摄入百草枯的量>40毫克/kg体重
分级标准的原意与解读
指导治疗,判断预后 防止过度医疗,避免医源性损害 存在局限性:服毒量如何判断
• • • • • • 背景与现状 毒代动力学与 毒理机制 诊断与鉴别诊断 救治措施与原则 知情告知与预后 协会责任与呼吁
规范之PQ中毒命名
命名:急性百草枯中毒(acute paraquat poisoning,APQ),慢性罕见,以示警 觉。 有慢性中毒吗?巴金森病与PQ有关?
诊断之规范
• 必须进行鉴别诊断:毒检方法有局限性 • 疑似诊断、临床诊断、临床确诊界定了 条件。 • 诊断共识应成为规范
共识对诊断条件界定
(完整版)药学英语专业词汇
(完整版)药学英语专业词汇一、药物分类及命名1. 抗生素(Antibiotics)青霉素(Penicillin)头孢菌素(Cephalosporins)大环内酯类(Macrolides)2. 抗病毒药物(Antiviral Drugs)抗流感病毒药物(Antiviral for Influenza)抗艾滋病病毒药物(Antiviral for HIV)3. 抗肿瘤药物(Anticancer Drugs)化疗药物(Chemotherapeutic Agents)靶向治疗药物(Targeted Therapy Drugs)4. 心血管系统药物(Cardiovascular Drugs)抗高血压药物(Antihypertensive Drugs)抗心绞痛药物(Antianginal Drugs)抗心律失常药物(Antiarrhythmic Drugs)5. 消化系统药物(Gastrointestinal Drugs)抗胃溃疡药物(Antigastric Ulcer Drugs)止泻药物(Antidiarrheal Drugs)泻药(Laxatives)6. 中枢神经系统药物(Central Nervous System Drugs)抗抑郁药物(Antidepressants)抗精神病药物(Antipsychotic Drugs)镇痛药物(Analgesics)二、药物剂型及给药途径1. 剂型(Dosage Forms)片剂(Tablets)胶囊(Capsules)注射剂(Injections)2. 给药途径(Routes of Administration)口服(Oral)肌内注射(Intramuscular)静脉注射(Intravenous)三、药物作用及不良反应1. 药物作用(Pharmacological Actions)抗菌作用(Antibacterial Action)抗病毒作用(Antiviral Action)镇痛作用(Analgesic Action)2. 不良反应(Adverse Reactions)过敏反应(Allergic Reactions)胃肠道反应(Gastrointestinal Reactions)肝脏毒性(Hepatotoxicity)四、药学专业英语词汇1. 药理学(Pharmacology)药物代谢(Drug Metabolism)药物动力学(Pharmacokinetics)药效学(Pharmacodynamics)2. 药剂学(Pharmaceutics)制剂工艺(Preparation Technology)药物稳定性(Drug Stability)药物质量控制(Drug Quality Control)3. 药物化学(Medicinal Chemistry)药物合成(Drug Synthesis)药物结构(Drug Structure)药物设计(Drug Design)本文档旨在帮助药学专业学生和从业者掌握药学英语专业词汇,提高专业英语水平,为学术交流和临床实践提供便利。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
IntroductionPesticide poisoning is common in Taiwan, and a sui-cide attempt is the most common reason for pesticide exposure.1Oral ingestion is the most common pathway of poisoning.1Herbicide is a type of pesticide, and paraquat is a widely used herbicide. Patients with para-quat exposures have a high mortality rate in Taiwan.1Paraquat is highly toxic to humans after oral inges-tion. The initial clinical features of paraquat ingestion include oral ulcer, nausea, vomiting and diarrhea. The patient will usually die from multiorgan failure, such as metabolic acidosis, depression of myocardial and respiratory function with pulmonary fibrosis, and renal or hepatic failure. To the best of our knowledge, intra-venous paraquat poisoning is rare,2–6and the clinical presentation and prognosis of such a scenario would appear to be quite different from that of oral inges-tion.2–6Only 1 case of survival has been reported.4Herein, we present a patient who attempted suicide by means of intravenous paraquat injection.Case ReportThis 28-year-old male was an intravenous drug abuser.He had attempted suicide several times previously,and had received treatment for major depression. He diluted 10mL of 24% paraquat solution with normal saline and injected it into a superficial vein in his left forearm. Whilst the toxic substance was infusing, the skin along the infused vessel developed an erythema-tous appearance and the injection site became painful.The patient was quickly sent to our emergency depart-ment,approximately 2 hours post-exposure. At this time, the patient’s consciousness was clear and he had vital signs with a pulse of 74beats/min, a respiratory rate of 23breaths/min, and blood pressure of 101/65mmHg. He had low body temperature (34.9°C).T he abnormal physical findings for this young man were left arm erythema and induration. Initial complete blood counts and biochemical data, including elec-trolytes, liver- and renal-function tests, revealed nor-mal results, and subsequent urinalysis did not reveal any abnormalities. The patient’s arterial blood-gas ass-essment displayed a PaO 2of 120mmHg in room air.A qualitative urine test confirmed the presence of para-quat, and plasma paraquat concentration (6 hours after injection) was 2.38μg/mL.The patient received 6 consecutive 8-hour sessions of hemoperfusion with activated charcoal; thereafter,urine paraquat level became negative. Intravenous cyclophosphamide treatment (1g) and parenteral pulse therapy with 1g methylprednisolone daily for 3 daysCASE REPORTIntravenous Paraquat PoisoningHuan-Wen Chen 1, Tse-Kai Tseng 2, Liang-Wen Ding 3*Departments of 1Internal Medicine and 2Radiology, and 3Division of Critical Care Medicine,Department of Emergency and Critical Care Medicine, Lotung Poh-Ai Hospital, Yi-Lan, Taiwan, R.O.C.Paraquat is a substance that is highly poisonous to humans. Oral ingestion is the most common pathway of poisoning.Intravenous paraquat poisoning is rare and is strongly associated with attempted suicide. The clinical presentations of such a scenario would appear to be quite different from those of oral ingestion. Herein,we present a case of an intra-venous drug abuser who injected paraquat in an effort to commit suicide. He received hemoperfusion and intravenous cyclophosphamide treatment and parenteral pulse therapy with methylprednisolone. Nevertheless,he suffered from dys-pnea at around 48 hours post-exposure. His condition improved transiently,but he eventually died from severe hypoxia.The findings from our case and those of previously reported cases indicate the grave prognosis and lack of effective management of intravenous paraquat poisoning. [J Chin Med Assoc 2009;72(10):547–550]Key Words:hemoperfusion,herbicide,intravenous poisoning,paraquat,suicide*Correspondence to: Dr Liang-Wen Ding,Division of Critical Care Medicine,Department of Emergency and Critical Care Medicine,Lotung Poh-Ai Hospital,83,Nan Chang Street,Lotung,Yilan 265,Taiwan,R.O.C.E-mail: dinglw@●Received: April 6,2009●Accepted: September 16,2009were undertaken at the same time as hemoperfusion. T he erythematous change, pain and induration of the patient’s left arm progressed gradually. Some blis-ters appeared 4 days after poisoning (Figure 1). The patient suffered from dyspnea around 48 hours post-exposure, and his respiratory rate was 32 breaths/min. At this time, his arterial blood gas displayed a PaO2 value of 49.8mmHg in room air. Follow-up chest X-ray revealed increasing infiltration over bilateral lower-lung fields (Figure 2). Intubation with mechan-ical ventilator support was then performed for acute hypoxic respiratory failure. The patient’s dyspnea sub-sided gradually, and the hypoxemia and chest X-ray results (Figure 3) also appeared to reverse following hemoperfusion and methylprednisolone pulse therapy. Unfortunately, the patient complained of dyspnea on the 10th day of admission. The degree of hypoxemia (PaO2of 51.6mmHg) worsened. At this time, chest X-ray revealed the presence of diffuse fibrotic changes (Figure 4). Pulse therapy was therefore repeated with 1g/day of methylprednisolone for 3 consecutive days in an attempt to suppress the inflammation. In addition, we prescribed oral dexamethasone sub-sequent to the pulse steroid therapy. Although he received this aggressive management, the hypoxemia progressed. On the 21st day subsequent to paraquat poisoning, our patient eventually died from severe hypoxemia.Figure 1.Four days following paraquat poisoning. Several vesi-cles featuring erythematous and indurated changes have devel-oped around the paraquat-infused vessel in the patient’s forearm.Figure 2.Chest radiograph of the patient taken on the 3rd day ofhospitalization shows ill-defined alveolar infiltration predominantin bilateral lower-lung fields with patch consolidation in the rightmiddle lobe of the lung.Figure 4.Chest radiography taken on the 10th day of hospitaliza-tion demonstrates diffuse fibrotic change and reticulonodularopacities in bilateral lungs.Figure 3.Chest radiography taken on the 5th day of hospitaliza-tion depicts great improvement in the patient’s lungs (comparedwith Figure 2).DiscussionParaquat (1,1Ј-dimethyl-4,4Ј-dipyridylium) is an effec-tive herbicide; it is highly toxic to humans and most animals. Unintentional and intentional oral ingestion are the most common pathways of paraquat poisoning in humans. According to a search of the related litera-ture, intravenous paraquat injection is extremely rare.MEDLINE was searched from 1966 to 2008 for cases of intravenous paraquat poisoning in the English-language literature. Only 6 cases were found.2–6The available medical data for the 6 patients and our patient (total, 7 cases) are summarized in Table 1.The symptoms in patients with poisoning include local and systemic toxicological effects. The local clin-ical presentations of intravenous paraquat poisoning differ from those of oral poisoning. Patients with oral paraquat ingestion suffer from oral ulcers, hemoptysis and gastrointestinal (GI) symptoms such as nausea,vomiting, diarrhea and GI bleeding.7T hese symp-toms are caused by direct mucosal irritation.7Patients with intravenous paraquat poisoning do not have direct mucosal irritation, but they might have some GI symptoms such as nausea and vomiting,2,5,6which may be explained by the systemic effect of paraquat on the central nervous system.5Patients with intravenous poisoning have local skin or vessel symptoms.2,5,6In our patient, the injection site developed an erythema-tous condition, and tissue swelling was initially apparent around the site of the injected vessel. T hen, several vesicles of varying sizes appeared. Such findings have also been reported by Hsu et al.5The skin presentation may be explained by local reaction due to the occur-rence of trivial extravasation of paraquat solution to adjacent soft tissue, and/or by local blood-vessel injury,such as phlebitis, related specifically to paraquat injec-tion. The systemic toxicological effects, such as renal hepatic or pulmonary damage, come later than local effects, and are suspected to be dose-dependent and lethal.7The systemic toxicological effects are also sus-pected to have faster onset in patients with intravenous poisoning than in patients with oral ingestion.5,6Although there is no definitive treatment for para-quat poisoning, patients with oral paraquat poisoning require immediate treatment that includes: (1) pre-venting GI absorption; (2) increasing plasma elimina-tion; and (3) preventing pulmonary damage.7Several methods are suggested to prevent pulmonary dam-age, including immunosuppressive therapy, vitamin E,deferoxamine, and N -acetylcysteine.7Although there is a lack of good evidence of the clinical efficacy of immunosuppressive therapy with glucocorticoids and cyclophosphamide in a systematic review,8a current meta-analysis suspects that immunosuppressive therapy is likely to decrease lung fibrosis and mortality.9No treatment protocol was suggested for patients of intra-venous paraquat poisoning. Because of the limited number of cases (Table 1), there are no existing treat-ment protocols to improve the grave outcome for patients with paraquat injection.Proudfoot et al were the first to suggest that paraquat concentration-time ratio before treatmentTable 1.Summary of clinical manifestations and outcomes of patients with intravenous paraquat poisoningPlasma paraquat Predictive Patients Age Sex concentration (μg/mL) survival Management Outcome(yr)(hours after injection)rate (%)*Harley et al 224FNANAForced diuresis +Died after 20 dascorbic acid +superoxide dismutase +α-tocopherol +steroid Hendy et al 342M 2.3 (4)30–50Hemoperfusion ×2SurvivedFernandez et al 421M 0.62 (6)50–70Hemoperfusion +propranolol Died after 15 d Hsu et al 535F 18 (5)<10Hemoperfusion ×2+Died after 4 dcyclophosphamide +pulse therapyHsu et al 537M 19.6 (1)<10Hemoperfusion ×2+Died after 5 dcyclophosphamide +pulse therapy Choi et al 631F 21 (10)<10Hemoperfusion ×2Died after 3 d Present case 28M 2.38 (6)20–30Hemoperfusion ×6+Died after 21 dcyclophosphamide +repeated pulse therapy*According to the formula of Hart et al.12could predict the outcome of poisoning.10Several prediction methods were developed. Five methods were compared in a large cohort study, and these methods are likely to be accurate in predicting death for patients with paraquat poisoning.11Hart et al created a nomogram with 6 concentration-time curves of about 10–90% survival probability,12and the nomo-gram is easy to use in the emergency department. Sawada et al presented a severity index of paraquat poisoning (SIPP) which was calculated according to the serum level of paraquat,13and the serum concen-trations were lower than plasma concentration.7We could not calculate the SIPP because we only have the plasma paraquat concentrations of the 6 patients with intravenous paraquat from published reports. Jones developed an equation to predict the probability of survival for any specific time,14but it is too complex to be of practical use in the emergency department. Because paraquat enters the body more rapidly by intravenous injection than by oral exposure, the prog-nosis of intravenous paraquat poisoning might be worse than that of oral poisoning. We tried to predict the mortality rate of the 6 patients with intravenous paraquat according to the formula of Hart et al,12and 5 of the 6 patients were considered to have a very high mortality rate (Table 1).2–6Six of the 7 patients (including the present case) did not survive after aggressive treatment (Table 1).2–6Only 1 miraculous case survived from severe pulmonary damage due to paraquat administered intravenously and orally.2The predictive mortality method according to the formula of Hart et al12seems to be suitable for use with cases of intravenous paraquat. However, as there is an inade-quate number of cases who survived, we cannot test the survival prediction ability of Hart et al’s nomogram.In conclusion, intravenous paraquat poisoning is rare, and patients may manifest with a variety of symp-toms including initial dermal changes. These symptoms often appear immediately subsequent to paraquat injection. The prognosis of intravenous paraquat poi-soning is graver than that of oral poisoning. Further experimental and clinical trials are required to search for an effective treatment for patients suffering from intravenous paraquat poisoning.References1.Yang CC, Deng JF. Pattern of acute pesticide poisoning inTaiwan. J To xico l Clin To xico l2003;41:523. (XXII Inter-national Congress of the European Association of Poison Centres and Clinical Toxicologists, Rome, Italy.)2.Harley JB, Grinspan S, Root RK. Paraquat suicide in a youngwoman: results of therapy directed against the superoxide radi-cal. Yale J Biol Med1977;50:481–8.3.Hendy MS, Williams PS, Ackrill P. Recovery from severe pul-monary damage due to paraquat administered intravenously and orally. Thorax1984;39:874–5.4.Fernandez P, Bermejo AM, Lopez-Rivadulla M, Cruz A,Rodriguez E, Otero A. A fatal case of parenteral paraquat poi-soning. Forensic Sci Int1991;49:215–24.5.Hsu HH, Chang CT, Lin JL. Intravenous paraquat poisoning-induced multiple organ failure and fatality: a report of two cases. J Toxicol Clin Toxicol2003;41:87–90.6.Choi Y, Cho K, Yoon S, Lee H, Choi Y. A case of paraquatintoxication caused by intravenous injection. Am J Emerg Med 2008;26:836.e3–4.7.Dinis-Oliveira RJ, Duarte JA, Sánchez-Navarro A, Remião F,Bastos ML, Carvalho F. Paraquat poisonings: mechanisms of lung toxicity, clinical features, and treatment. Crit Rev Toxicol 2008;38:13–71.8.Eddleston M, Wilks MF, Buckley NA. Prospects for treatmentof paraquat-induced lung fibrosis with immunosuppressive drugs and the need for better prediction of outcome: a system-atic review. QJM2003;96:809–24.9.Agarwal R, Srinivas R, Aggarwal AN, Gupta D. Immuno-suppressive therapy in lung injury due to paraquat poisoning:a meta-analysis. Singapore Med J2007;48:1000–5.10.Proudfoot AT, Stewart MS, Levitt T, Widdop B. Paraquat poi-soning: significance of plasma–paraquat concentrations. Lancet 1979;2:330–2.11.Senarathna L, Eddleston M, Wilks MF, Woollen BH,Tomenson JA, Roberts DM, Buckley NA. Prediction of out-come after paraquat poisoning by measurement of the plasma paraquat concentration. QJM2009;102:251–9.12.Hart TB, Nevitt A, Whitehead A. A new statistical approach tothe prognostic significance of plasma paraquat concentrations.Lancet1984;2:1222–3.13.Sawada Y, Yamamoto I, Hirokane T, Nagai Y, Satoh Y, UeyamaM. Severity index of paraquat poisoning. Lancet1988;1:1333.14.Jones AL, Elton R, Flanagan R. Multiple logistic regressionanalysis of plasma paraquat concentrations as a predictor of out-come in 375 cases of paraquat poisoning. QJM1999;92:573–8.。