CCL2 recruitment of IL-6-producing CD11b+ monocytes
猪IL-2和IL-6的原核表达及多克隆抗体的制备
白 IM 、 G、g 主 要 发 挥 体 液 免 疫 功 能 , 可 以 g I I A, g 也
促进 P HA 或 刀 豆 球 蛋 白 A 激 活 的 T 细 胞 增 殖 生
体菌 E.oiDH5 cl a及 表达 菌 E cl B 2 ( E ) .oi L 1 D 3 和
Roet( E ) 表 达 载 体 p T 0 st D 3 、 a E 3 a均为 山东省 滨 州 畜 牧 兽 医研究 院 实验 室 保存 ; TI一 p L 2和 p I 一 T L 6为 山东省滨 州 畜 牧 兽 医研 究 院王 金 良研 究 员 构 建 保 存 。其他试 剂均为进 口或 国产分 析纯 。
关键 词 : 白细胞介 素 2 猪 白细胞 介素 6 原核 表达 ; 猪 ; ; 多克隆抗体
中 图分 类 号 : 8 8 2 ; 8 2 4 ¥ 5 . 8 ¥ 5 . 文 献标 识 码 : A 文章 编 号 : 0 75 3 ( 0 0 0 — 0 00 1 0 —0 8 2 1 ) 20 6 —5
自细胞介素 ( tre kn I ) 由免疫细 胞和某 i el i , 是 n u I 些非免疫 细胞经刺 激后转 录表达 和分泌 的一 类小 分 子多肽或糖 蛋 白的 生 物活性 物质 , 机 体 内重 要 的 是 细胞因子之 一 。其在 体 内能激 活 和调节 免疫 活性细 胞, 对免疫应 答 的产 生 和调 节 具 有重 要 作 用 。 白细 胞介 素 2 I — ) 白细胞 介索 6 I一 ) (L Z 和 (I 6 是机体 重要 的
免疫 调 节 因 子 , 有 多 种 生 物 学 活性 。I一 具 I 2属 于
R st ( E ) o et D 3 进行 了表 达 , a 其后 提取包 涵体 , 纯化 复 性后 免疫 家兔制 备 了兔抗 猪 I 一 、L 6的多 克隆抗 L2 I 一
类风湿关节炎患者血清IL-6、IL-17表达及其意义分析
生命科学仪器 2023年第21卷/第6期生命科学-医药卫生139作者简介:冷俊,出生年月:1985年2月,性别:男,学历:硕士研究生,职称:副主任技师,研究方向:主要从事临床免疫㊁分子检测工作,邮箱:c o l d d o g 19852000@126.c o m 通讯作者:周晔,出生年月:1973年3月,性别:女,学历:本科,职称:主管技师,研究方向:主要从事临床生化㊁免疫检测工作,邮箱:c m j yk 5590@126.c o m 类风湿关节炎患者血清I L -6、I L -17表达及其意义分析冷 俊 林 豪 周 晔*(上海健康医学院附属崇明医院检验科,上海202150)摘要 目的:通过开展回顾性分析,观察血清白细胞介素-6(I L-6)㊁白细胞介素-17(I L-17)在类风湿关节炎(R A )患者中的表达及其意义,为R A 早期诊疗提供新思路㊂方法:回顾性分析,采集我院2019年7月至2022年7月收治的110例R A 患者基线资料,依据D A S 28评分系统评估R A 患者病情活动度并分为稳定组(D A S 28评分ɤ3.2分)与进展组(D A S 28评分>3.2分),观察两组患者血清I L -6㊁I L -17表达情况,并分析上述血清表达与疾病活动度的关系㊂结果:入组110例R A 患者经D A S 28评分系统评估显示,高度活动37例,平均得分(7.21ʃ1.52)分,中度活动度32例,平均得分(4.12ʃ0.67)分,低度活动度41例,平均得分(2.15ʃ0.52)分;与稳定组相比,进展组血清I L -6㊁I L -17表达均较高,D A S 28平均得分较稳定组高(P<0.05),组间其他资料对比(P>0.05);建立L o g i s t i c 回归模型,结果显示,血清I L-6㊁I L-17表达与R A 患者疾病活动度有关,且血清I L-6(O R=1.176,95%C I :1.028~1.346)㊁I L -17(O R=1.117,95%C I :1.044~1.196)过表达是导致R A 患者疾病进展的危险因素(P <0.05);绘制R O C 曲线显示,血清I L -6㊁I L -17表达单独及联合预测R A 患者疾病活动度的A U C 均>0.80,预测价值较理想㊂结论:血清I L -6㊁I L -17表达与R A 患者疾病活动度密切相关,血清I L -6㊁I L -17过表达是导致R A 患者疾病进展的重要因素㊂关键词 类风湿关节炎;白细胞介素-6;白细胞介素-17;疾病活动度;相关性A n a l y s i s o f s e r u m I L -6a n d I L -17e x p r e s s i o n a n d t h e i r s i gn i f i c a n c e i n p a t i e n t s w i t h r h e u m a t o i d a r t h r i t i s L E N G J u n ,L I N H a o ,Z H O U Y e *(D e p a r t m e n t o f C l i n i c a l L a b o r a t o r y ,C h o n g m i n g H o s p i t a l A f f i l i a t e d t o S h a n gh a i U n i v e r s i t y o f M e d i c i n e a n d H e a l t h S c i e n c e s ,S h a n gh a i 202150,C h i n a )ʌA b s t r a c t ɔO b je c t i v e :T o o b s e r v e t h e e x p r e s s i o n of s e r u m i n t e r l e u k i n -6(I L-6)a n d i n t e r l e u k i n -17(I L-17)i n p a t i e n t s w i t h r h e u m a t o i d a r t h r i t i s (R A )a n d t h e i r s ig n i f i c a n c e b y c o n d u c t i n g a r e t r o s p e c t i v e a n a l ys i s .M e t h o d s :R e t -r o s p e c t i v e a n a l y s i s w a s p e r f o r m e d t o c o l l e c t b a s e l i n e d a t a f r o m 110R A p a t i e n t s a d m i t t e d t o o u r h o s pi t a l f r o m F e b -r u a r y 2020t o F e b r u a r y 2023,a n d t o a s s e s s t h e d i s e a s e a c t i v i t y o f R A p a t i e n t s a c c o r d i n g t o t h e D A S 28s c o r i n g s y s -t e m a n d d i v i d e t h e m i n t o s t a b l e g r o u p (D A S 28s c o r e ɤ3.2)a n d p r o g r e s s i v e g r o u p (D A S 28s c o r e >3.2),a n d t o o b s e r v e t h e e x p r e s s i o n o f s e r u m I L -6a n d I L -17i n b o t h g r o u p s a n d a n a l y z e T h e r e l a t i o n s h i p be t w e e n t h e a b o v e s e r u m e x p r e s s i o n a n d d i s e a s e a c t i v i t y w a s a n a l y z e d .R e s u l t s :T h e r e s u l t s of 110R A p a t i e n t s e n r o l l e d i n t h eg r o u pw e r e e v a l u a t e d b y t h e D A S 28s c o r i n g s y s t e m ,w h i c h s h o w e d t h a t 37p a t i e n t s w e r e h i g h l y ac t i v e w i t h a m e a n s c o r e o f (7.21ʃ1.52),32p a t i e n t s w e r e m ode r a t e l y a c t i v e w i t h a m e a n s c o r e of (4.12ʃ0.67),a n d 41p a t i e n t s w e r e h y -p o a c t i v e w i t h a m e a n s c o r e o f (2.15ʃ0.52);c o m p a r e d w i t h t h e s t a b l eg r o u p ,s e r u m I L -6a n d I L -17e x pr e s s i o n s w e r e h i g h e r i n t h e p r o g r e s s i v e g r o u p ,a n d t h e m e a n D A S 28s c o r e w a s h i g h e r i n t h e p r o g r e s s i v e g r o u p .C o m pa r e d w i t h t h e s t ab l e g r o u p ,t h e m e a n sc o r e o f D A S 28w a s h i g h e r t h a n t h a t o f t h e s t a b l e g r o u p (P <0.05),a n d o t h e r i n -f o r m a t i o n w a s c o m p a r e d b e t w e e n g r o u p s (P >0.05);l o g i s t i c r e gr e s s i o n m o d e l s w e r e e s t a b l i s h e d ,a n d t h e r e s u l t s s h o w e d t h a t s e r u m I L -6a n d I L -17e x p r e s s i o n w e r e r e l a t e d t o d i s e a s e a c t i v i t yi n R A p a t i e n t s ,a n d s e r u m I L -6a n d I L -17o v e r e x p r e s s i o n w a s a r i s k f a c t o r f o r d i s e a s e p r o g r e s s i o n i n R A p a t i e n t s (O R>1,P <0.05);p l o t t i n gR O C c u r v e s s h o w e d t h a t t h e A U C o f s e r u m I L -6a n d I L -17e x pr e s s i o n a l o n e a n d i n c o m b i n a t i o n t o p r e d i c t d i s -生命科学-医药卫生生命科学仪器 2023年第21卷/第6期140e a s e a c t i v i t yi n R A p a t i e n t s w a s >0.80,w h i c h w a s a g o o d p r e d i c t i v e v a l u e .C o n c l u s i o n :S e r u m I L -6a n d I L -17e x p r e s s i o n a r e c l o s e l y r e l a t e d t o d i s e a s e a c t i v i t y i n R A p a t i e n t s ,a n d s e r u m I L -6a n d I L -17o v e r e x pr e s s i o n i s a n i m p o r t a n t f a c t o r l e a d i n g t o d i s e a s e p r o gr e s s i o n i n R A p a t i e n t s .ʌK e y wo r d s ɔR h e u m a t o i d a r t h r i t i s ;i n t e r l e u k i n -6;i n t e r l e u k i n -17;d i s e a s e a c t i v i t y ;c o r r e l a t i o n 中图分类号:R 684.3 文献标识码:A D O I :10.11967/2023211232类风湿关节炎(R h e u m a t o i d a r t h r i t i s ,R A )是以对称性㊁侵蚀性为特征的自身免疫性疾病,患者主要表现为掌指关节㊁腕关节㊁足部小关节等出现肿痛㊁功能障碍等不可逆性表现,严重者可致畸[1-2]㊂R A 的发病与遗传㊁环境等密切相关,但针对R A 具体发病机制尚无确切定论,但确定的是单纯的遗传因素尚不能全面解释复杂的免疫介导性疾病,也提示遗传因素在R A 疾病发病㊁进展过程中的尚存在局限性,同时提示临床环境因素在R A 疾病介导过程中的重要性[3-5]㊂血清I L -6与I L -17在R A 患者中的表达及其在机体中的特殊意义,能否为R A 疾病诊疗或病情评估等方面提供新的启示,这些目前尚不得知,且临床尚未发现有关研究,鉴于此,本研究通过开展回顾性分析,观察血清I L -6㊁I L-17在R A 患者中的表达及其意义,为R A 早期诊疗提供新思路㊂具示如下㊂1 资料与方法1.1 一般资料:回顾性分析,采集我院2019年7月至2022年7月收治的R A 患者基线资料(对于R A 疾病活动度不同的患者,按照疾病活动程度均衡抽样),纳入对象均需满足如下条件:纳入标准:①符合‘2018中国类风湿关节炎诊疗指南“[6]中类风湿关节炎的诊断标准;②研究涉及资料㊁实验室检查等均保存完善㊂排除标准:①入组前3个月内有服用抗感染㊁抗炎等可能对血清I L-6㊁I L-17表达有影响的药物;②合并其他风湿免疫性疾病;③合并活动感染性疾病;④伴重要脏器功能衰竭患者㊂本研究经上述纳入条件筛选后最终入组110例R A 患者,其中男性27例,女性83例㊂1.2 方法1.2.1 疾病活动度评估方法:依据D A S 28评分系统[7]评估R A 患者病情活动度,判定细则:所有患者入院后均查体,内容主要包括:肿胀关节数㊁压痛关节数与血沉㊂①压痛关节数:双侧膝关节㊁肩关节㊁肘关节㊁腕关节㊁掌指关节共计28个关节,记录关节被动活动或触痛时的关节数㊂②肿胀关节数:记录上述关节肿胀的数量㊂1.2.2 实验室指标检测方法:采集患者空腹周静脉血5m l ,高速离心后(半径15c m ,3000r/m i n ,离心20m i n),采用酶联免疫吸附法检测血清中I L -6㊁I L -17㊂全自动多功能酶联免疫分析仪产自日本T a K a R a 公司,试剂盒均由海源叶生物科技有限公司提供㊂采用魏氏法检测红细胞沉降率㊂1.3 统计学方法:采用S P S S 24.0软件进行数据处理,全部计量资料均经S h a p i r o -W i l k 正态性检验,符合正态分布的资料以x ʃs 表示,组间比较采用独立样本t 检验;计数资料用%表示,采用χ2检验,各指标之间采用双变量S p e a r m a n 直线相关性分析,采用L o gi s t i c 回归分析血清I L-6㊁I L-17表达与R A 患者疾病活动度之间的关系;绘制受试者工作曲线(R O C ),检验血清I L-6㊁I L-17在R A 患者疾病活动度的预测价值;P <0.05为差异具有统计学意义㊂2 结果2.1 疾病活动度情况:入组110例R A 患者经D A S 28评分系统评估显示,高度活动37例,平均得分(7.21ʃ1.52)分,中度活动度32例,平均得分(4.12ʃ0.67)分,低度活动度41例,平均得分(2.15ʃ0.52)分㊂2.2 两组基线资料㊁实验室指标比较:与稳定组患者相比,进展组患者血清I L-6㊁I L-17表达均较高,D A S 28平均得分较稳定组高,差异有统计学意义(P <0.05),组间其他资料对比,差异无统计学意义(P >0.05)㊂见表1㊂2.3 血清I L -6㊁I L -17表达与R A 患者疾病活动度的L o g i s t i c 回归分析:将R A 患者血清I L-6㊁I L-17表达作为协变量,疾病活动度情况作为因变量(1=进展,0=稳定),经二元回归分析后将2.2中全部资料纳入,建立多元L o gi s t i c 回归模型,结果显示,血清I L-6㊁I L-17表达与R A 患生命科学仪器 2023年第21卷/第6期生命科学-医药卫生141者疾病活动度有关,且血清I L-6㊁I L-17过表达是导致R A 患者疾病进展的危险因素(O R>1,P<0.05)㊂见表2㊂表1 两组基线资料㊁实验室指标比较资料进展组(n =69)稳定组(n =41)统计值P 性别(n ,%)男20(28.99)7(17.07)女49(71.01)34(82.93)χ2=1.9710.160年龄[(x ʃs ,岁)]42.56ʃ4.8542.25ʃ5.15t =0.3170.752病程[(x ʃs,月)]42.15ʃ10.1545.25ʃ13.15t =1.3850.169I L -17[(x ʃs ,n g /L )]36.12ʃ12.5618.25ʃ7.88t =8.194<0.001I L -6[(x ʃs ,p g/m L )]110.25ʃ40.2040.10ʃ5.58t =11.090<0.001D A S 28平均得分[(x ʃs,分)]5.78ʃ1.752.15ʃ0.52t =12.926<0.001表2 血清I L -6㊁I L -17表达与R A 患者疾病活动度的L o gi s t i c 回归分析变量B S .E W a l s P O R 值95%置信区间上限下限常量-10.2572.59215.664<0.0010.000--I L -60.1620.0695.5820.0181.1761.0281.346I L -170.1110.03510.2310.0011.1171.0441.1962.4 血清I L -6㊁I L -17表达预测R A 患者疾病活动度的效能分析:将R A 患者血清I L-6㊁I L-17表达分别作为检验变量,疾病活动度情况作为状态变量(1=进展,0=稳定),绘制R O C 曲线(见图1),结果显示,血清I L-6㊁I L-17表达单独及联合预测R A 患者疾病活动度的A U C 均>0.80,预测价值较理想㊂依据R O C 曲线得出血清I L-6㊁I L -17的c u t -o f f 值分别为27.380(p g/m L )㊁7.345(n g/L ),在该c u t -o f f 值水平下,取敏感度与特异性㊂见表3㊂图1 血清I L -6㊁I L -17表达预测R A 患者疾病活动度的R O C 曲线图3 讨论R A 主要起始于某种细胞持续的活化状态,这种状态可引起机体关节㊁器官中自身免疫与免疫复合物的表达,R A 最先累及滑膜,常由充血㊁肿胀引起免疫细胞浸润,伴随病情进展主要经历非特异性炎症触发初始阶段㊁T 细胞活化引起扩增阶段与慢性炎症阶段,其中慢性炎症阶段往往伴随I L -6㊁I L -1㊁肿瘤坏死因子-α等细胞因子诱发的组织损伤与慢性免疫反应[8]㊂I L -6是由T 细胞㊁单核巨噬细胞等诸多细胞产生的具有较强刺激作用的多效应细胞,主要介导机体内免疫应答与细胞的生长㊁分化[9]㊂刘肃等[10]人研究中通过对比健康成人与R A 患者的血清炎性细胞因子发现,R A 患者的血清C 反应蛋白㊁I L-18㊁I L-6显著高于健康成人,该结果提示血清C 反应蛋白㊁I L-18㊁I L-6与R A 的发生相关㊂I L-17是由T h 17细胞生成的前炎症细胞因子,在体内主要生物学机制表现为:①通过刺激角质细胞㊁成纤维细胞㊁上皮细胞等释放I L-8㊁I L-6等参与炎症反应;②诱导人成纤维细胞表达细胞间粘附分子-1,继而促进T 细胞增殖㊁分化;③协同诸多细胞放大炎症状态与反应程度[11]㊂单核细胞在炎症的刺激下产生大量的I L-6,I L-6与其受体相结合,经过多次分化后形成的结合体会影响酪氨酸蛋白激酶1㊁2,最终导致患者体内释放大量T N F-&a l ph a ;㊁I L -17等细胞因子,诱发关节炎㊂与此同时,I L -6也是肝细胞的刺激因子,在炎症影响下,I L -6能够诱导S A A 等急性期的反应蛋白合成,尤其会使c -反应蛋白水平大幅提高㊂C 反应蛋白直接参与了炎症等疾病,具有复杂的生物生命科学-医药卫生生命科学仪器 2023年第21卷/第6期142活性,与补体的相互作用会直接影响宿主对炎症的反应㊂除此之外,I L-6还可以使多种免疫球蛋白形成类风湿因子,导致R A 患者滑膜内抗体沉积现象严重,损害R A 患者关节功能,导致患者病情加剧㊂且血清I L-6㊁I L-17过表达是导致R A 患者疾病进展的危险因素,临床考虑可将其作为R A 患者疾病进展的评估指标㊂为验证上述猜想,研究经绘制R O C 曲线显示血清I L -6㊁I L-17表达单独及联合预测R A 患者疾病活动度的A U C 均>0.80,预测价值较理想,且相关性分析显示,R A 患者I L -6㊁I L-17表达与D A S 28系统得分之间呈正相关,提示血清I L -6㊁I L -17在R A 疾病进展过程中均有参与㊂分析原因可能为:1)I L-6:I L-6通过诱导I L-1㊁I L -17㊁I L -2等炎症因子大量释放,扩大炎症范围,加重炎症破坏程度;诱导B 淋巴细胞,促使其释放大量类风湿因子与免疫球蛋白;加速效应T细胞活化,抑制T 细胞调节作用;I L-6高表达促进大量血管内皮生长因子产生,滑膜腔内内皮生长因子过表达,内皮细胞因此加速分化㊁迁移过程,血管通透性改变,为关节内血管翳的形成提供便利条件;加速破骨细胞分化㊁增殖,引起关节损伤,加速病情进展㊂2)I L-17:缩短滑膜成纤维细胞与破骨细胞活化㊁增殖过程,继而加速关节软骨的破坏程度,参与病情进展;上调肿瘤坏死因子㊁I L -1等与炎症相关的因子分泌,且I L-17与I L-1存在交叉调控,间接加重关节破坏与受损程度;刺激核刺因子受体及其配体表达,导致骨保护蛋白与核刺因子受体及其配体间的平衡,加重骨质破坏;提高滑膜成纤维细胞基质金属蛋白酶与软骨细胞表达,强化胶原酶活性,抑制胶原与软骨蛋白多糖合成并加速其降解,强化单核细胞对软骨基质的损害程度,加速疾病进展过程[12,13]㊂综上所述,血清I L-6㊁I L-17表达与R A 患者疾病活动度密切相关,血清I L-6㊁I L-17过表达是导致R A 患者疾病进展的重要因素,临床可通过针对血清I L -6㊁I L -17过表达患者,及时采取针对性干预手段,旨在控制患者病情进展,为临床治疗争取时间窗㊂但本研究采取回顾性分析,且血清I L -6㊁I L-17表达仅选取入院次日晨起空腹状态下,并未对患者血清I L-6㊁I L-17表达进行动态观察分析,导致研究结论存在偏倚,未来还需开展动态㊁连续的血清指标跟踪调查,旨在挖掘血清I L-6㊁I L-17在R A 疾病诊疗中的更多可能性㊂参考文献[1]D e m o r u e l l e M K ,W i l s o n T M ,D e a n e K D .L u n g in f l a mm a -t i o n i n t h e p a t h o g e n e s i s o f r h e u m a t o i d a r t h r i t i s [J ].I mm u n o l R e v ,2020,294(1):124-132.[2]谌虹焰,张明媚,陈杏,等.骨关节炎患者膝关节滑膜组织的基因表达谱分析[J ].川北医学院学报,2021,36(4):425-428.[3]石娇,吴东明,李静,等.痛风性关节炎中I L-1β/C a s p a s e -1介导的细胞焦亡的作用研究[J ].成都医学院学报,2020,15(1):19-22.[4]J a r l b o r g M ,G a b a y C .S y s t e m i c e f f e c t s o f I L-6b l o c k a d e i n r h e u m a t o i d a r t h r i t i s b e y o n d t h e j o i n t s [J ].C yt o k i n e ,2022,149(6):155742.[5]S a r a i v a A ,P e r e s R ,V e r a s F ,e t a l .C i t r u l l i n a t e d h u m a n f i b r i n -o g e n t r i g g e r s a r t h r i t i s t h r o u g h a n i n f l a mm a t o r y r e s po n s e m e -d i a t e d b y I L-23/I L-17i mm u n e a x i s .[J ].I n t I mm u n o p-h a r m a c o l ,2021,101(10):108363.[6]中华医学会风湿病学分会.2018中国类风湿关节炎诊疗指南[J ].中华内科杂志,2018,57(4):1242-251.[7]程国华,郝晓娟,姜敏.类风湿关节炎患者P L R ,N L R ,I L-27水平检测及其与疾病活动度的相关性[J ].海南医学,2023,34(1):19-21.[8]S c h e r e r H U ,D i a n e V ,T o e s R .F r o m r i s k t o c h r o n i c i t y :e v o -l u t i o n o f a u t o r e a c t i v e B c e l l a n d a n t i b o d y r e s po n s e s i n r h e u m a -t o i d a r t h r i t i s [J ].N a t r e v R h e u m a t o l ,2022,18(7):371-383.[9]吴旭,姚勐炜,郭震.关节液中T N F -αI L-6和I L-8水平与创伤性关节炎患者X 线分级和关节功能的相关性分析[J ].河北医学,2020,26(2):290-294.[10]刘肃,张鑫,王春生.类风湿性关节患者血清炎性细胞因子水平及其临床意义分析[J ].基因组学与应用生物学,2018,37(9):4100-4105.[11]邓燕群,刘翠玉,尹志华,等.类风湿关节炎患者血清中I L-17表达及I L-17F 基因位点r s 763780多态性分析[J ].中国免疫学杂志,2020,36(2):222-225.[12]廖发科,廖元军,胡秀年.膝关节骨性关节炎患者I L-6水平变化以及N F A T 1对I L -6作用机制研究[J ].中国骨与关节损伤杂志,2022,37(2):139-143.[13]S h a f r a n I H ,A l a s t i F ,S m o l e n J S ,e t a l .I m pl i c a t i o n o f b a s e -l i n e l e v e l s a n d e a r l y c h a n ge s of C -r e a c t i v e p r o t e i n f o r s u b s e -qu e n t c l i n i c a l o u t c o m e s o f p a t i e n t s w i t h r h e u m a t o i d a r t h r i t i s t r e a t e d w i t h t o c i l i z u m a b [J ].A n n R h e u m D i s ,2020,79(7):874-882.。
白介素—6(IL—6)测定试剂盒(荧光免疫层析法)产品技术要求瑞辉
医疗器械产品技术要求编号:
白介素-6(IL-6)测定试剂盒(荧光免疫层析法)
2.性能指标
2.1.物理性状
2.1.1.外观
试剂卡外观平整,材料附着牢固;
样本稀释液为无色透明液体,无悬浮物及沉淀物;
2.1.2.净含量
样本稀释液净含量应在标示值的 90%-110%之间;
稀释液标示值:300μl。
2.1.
3.膜条宽度
膜条宽度应不小于 3.9mm。
2.1.4.液体移行速度
液体移行速度应不低于 25mm/min。
2.2.最低检出限
最低检出限≤3pg/ml。
2.3 .线性范围
试剂的线性范围为(3-1000)pg/ml,在此线性范围内,线性相关系数 r 应不小于 0.990。
2.4.测量精密度
2.4.1.重复性
用质控品重复测试,所得结果的变异系数(CV)≤15%;
2.4.2.批间差
用质控品重复测试 3 个批号的试剂盒,所得结果的变异系数(CV)≤15%。
2.5.准确度
回收率在 85%-115%之间。
第 1 页共1 页。
4.01 降钙素原 ∕ 白介素-6测定试剂盒(荧光免疫层析法)技术要求

医疗器械产品技术要求编号:降钙素原/白介素-6测定试剂盒(荧光免疫层析法)1 产品型号/规格及其划分说明1.1 型号型号:型号G、型号Q。
1.2 规格1人份/盒,2人份/盒,3人份/盒,5人份/盒,10人份/盒,20人份/盒,25人份/盒,30人份/盒,40人份/盒,50人份/盒,100人份/盒,200人份/盒。
1.3 产品型号/规格划分说明产品型号划分主要根据产品注册单元进行划分,其中型号G由检测卡、样本缓冲液组成;型号Q由检测卡、样本缓冲液、质控物组成。
规格划分主要根据产品单人份铝箔包装的检测卡装量来进行规格划分。
产品形式由产品型号和规格组合形成。
产品型号/规格划分类型(例子)2 性能指标2.1 物理检查2.1.1 外观试剂盒各组分齐全、完整,包装无破损;液体组分澄清、无漏液;标签牢固,内容清晰、准确。
质控物应外观均匀,形成完整的冻干品,复溶后清亮,无浑浊及沉淀。
2.1.2 液体移行速度液体移行速度应不小于10mm/min。
2.2 线性2.2.1 PCT项目试剂盒项目PCT线性在0.1ng/mL~50.0ng/mL范围内,线性相关系数|r|应≥0.990。
2.2.2 IL-6项目试剂盒项目IL-6线性在3.0pg/mL~4000.0pg/mL范围内,线性相关系数|r|应≥0.990。
2.3 准确性2.3.1 PCT项目测定回收率应在85%~115%范围内。
2.3.2 IL-6项目用IL-6国际标准品配制的准确性校准品或经标化的准确性校准品进行检测,其检测结果的相对偏差应在±15.0%范围内。
注:国家、省质量监督抽检和风险监测、第三方仲裁检验时应采用国家/国际标准品。
2.4 检出限试剂盒项目PCT检出限不高于0.05ng/mL,项目IL-6检出限不高于1.5pg/mL。
2.5 重复性试剂盒项目PCT和IL-6每个项目的重复性变异系数(CV)不高于10%。
2.6 批间差试剂盒项目PCT和IL-6每个项目的批间变异系数(CV)不高于15%。
胃癌与胃溃疡患者血清白介素6表达及意义
胃癌与胃溃疡患者血清白介素6表达及意义白介素6(IL-6)是一种由多种细胞产生的蛋白质,可以促进细胞生长、增殖和分化,对于免疫和炎症反应的调节起着重要作用。
研究表明,IL-6在许多肿瘤中都具有促进增殖和转移的作用,包括胃癌。
而在胃溃疡的发病过程中,IL-6也被认为是一种炎症介质,参与了炎症反应和溃疡的形成。
研究人员通过检测胃癌和胃溃疡患者的血清中IL-6的表达水平,发现在这两种疾病的患者中,IL-6的表达水平明显升高。
尤其是在胃癌患者中,IL-6的表达水平与肿瘤的大小、浸润深度、淋巴结转移和临床分期等因素密切相关。
这种差异性的表达水平提示了IL-6在胃癌和胃溃疡的发病过程中可能起着重要的作用。
研究发现,高表达的IL-6与胃癌和胃溃疡患者的预后密切相关。
在胃癌患者中,IL-6的高表达水平往往伴随着肿瘤的快速生长、侵袭和转移,预后差;而在胃溃疡患者中,IL-6的高表达与溃疡的复发和转化为癌症的风险增加相关。
IL-6的表达水平对于胃癌和胃溃疡的早期诊断也具有重要的意义。
通过检测IL-6的表达水平,可以帮助医生及时发现患者的病情变化,提高早期诊断的准确性和敏感性。
在治疗方面,IL-6的高表达水平也为个体化治疗提供了重要的依据。
针对IL-6的高表达,可以设计针对性的靶向治疗方案,提高治疗效果,减少不必要的毒副作用。
针对IL-6的抑制剂也成为胃癌和胃溃疡治疗中的新颖研究方向。
胃癌和胃溃疡患者血清白介素6的高表达水平提示了这种蛋白对于疾病的发生发展具有重要意义。
通过对IL-6的研究,可以更好地理解胃癌和胃溃疡的病理生理过程,为早期诊断和个体化治疗提供重要依据。
未来的研究方向与展望在未来的研究中,人们可以进一步探究IL-6在胃癌和胃溃疡发病机制中的作用,深入了解其与其他信号通路的交互关系,为新药的研发和临床治疗提供更多的靶点和策略。
人们还可以进一步探索IL-6在胃癌和胃溃疡的临床诊断和预后评估中的价值,探讨其与其他临床指标的关联,构建更为全面的评估体系。
白介素6检测标准操作程序

白介素6检测标准操作程序1检验目的本试剂盒用于体外定量测定人血清和(或)血浆中的白介素6(IL-6)。
2检验原理及方法夹心法。
测定总时长18分钟。
1.第1次孵育:30L样本、生物素化的白介素6特异性单克隆抗体一起孵育,形成抗原一抗体复合物。
2.第2次孵育:添加包被链霉亲合素的磁珠微粒进行孵育,复合体与磁珠通过生物素和链霉亲合素的作用结合。
3.将反应液吸入测量池中,通过电磁作用将磁珠吸附在电极表面,未与磁珠结合的物质通过ProCell/ProCell M被去除。
给电极加以一定的电压,使复合体化学发光,并通过光电倍增器测量发光强度;4.通过由2点校准生成的分析仪专有的校准曲线和通过试剂条码或电子条形码提供的主曲线来确定结果。
3性能特征3.1检测范围:1.5-5000pg/mL3.2精密度:根据CLSI(临床实验室标准委员会)的方案(EP5-A2),使用Elecsys 试剂、混合人血清和 CLSI(临床和实验室标准化学会)修改协议(EP5-A)规定的质控品确定精密度:每天2次重复共21天;MODULAR ANALYTICSE170分析仪的批内精密度,n=84。
所得结果如下Cobas e 411 分析仪e)可重复性=批内精密度3.3分析特异性/干扰下列物质不会对Elecsys白介素-6检测(浓度范围10-200pg/mL)造成明显的交叉反应。
4标本4.1检测标本:血清和血浆(肝素锂、肝素钠、EDTA和柠檬酸钠抗凝)是推荐使用的样本类型。
尚未验证其他抗凝剂能否适用。
4.2采集及处理:在进行离心操作前需让血清样本完全凝结(凝结时间不小于1小时)。
所有的待测样本在测试前均应进行离心操作。
顶部含脂质的离心样本,需转移澄清、无脂质的部分到新的样本管中。
在测试前,确保已去除了残余的纤维蛋白和细胞类物质。
应小心处理患者样本,避免交叉污染。
在测试前,确保患者样本、校准品、质控品均已平衡至环境温度(20-25°C)。
白介素6(IL-6)测定试剂盒(磁微粒化学发光法)产品技术要求利德曼生化
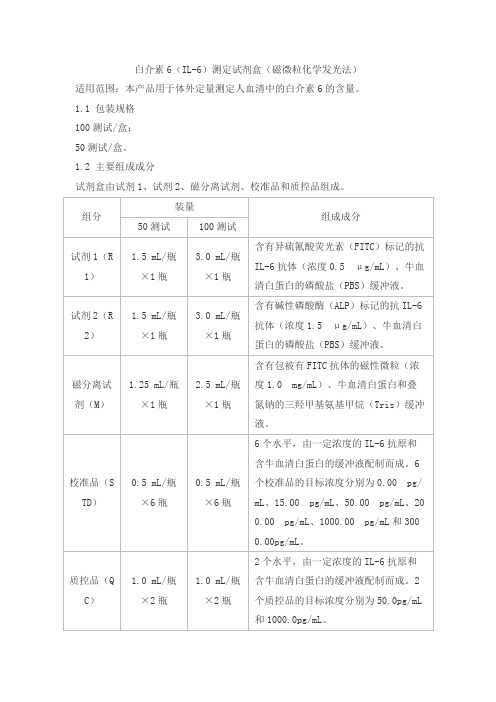
白介素6(IL-6)测定试剂盒(磁微粒化学发光法)适用范围:本产品用于体外定量测定人血清中的白介素6的含量。
1.1 包装规格100测试/盒;50测试/盒。
1.2 主要组成成分试剂盒由试剂1、试剂2、磁分离试剂、校准品和质控品组成。
注:校准品和质控品浓度具有批特异性,具体数值见瓶标签。
2.1外观2.1.1试剂盒各组分应齐全、完整、液体无渗漏;2.1.2磁分离试剂摇匀后为均匀悬浊液,无明显凝集;2.1.3液体组分应无沉淀或絮状物;2.1.4包装标签应清晰,易识别。
2.2准确度用国际标准品NIBSC 1st 89/548,配制浓度约为200.00pg/mL(允许偏差为±20.0%)作为样本检测,其测量结果的相对偏差在±15.0%范围内。
2.3空白限应不大于1.50 pg/mL。
2.4线性在[2.00,3000.00]pg/mL的测量范围内,试剂盒的相关系数r应≥0.9900。
2.5重复性用(50.00±10.00)pg/mL和(1000.00±200.00)pg/mL的样本各重复检测10次,变异系数(CV)应不大于10.0%。
2.6批间差用三个批号的试剂盒分别检测(50.00±10.00)pg/mL和(1000.00±200.00)pg/mL的样本,其批间变异系数应≤15%。
2.7质控品的赋值有效性质控品的测量值应在质控范围内。
2.8 稳定性试剂盒2℃~8℃保存有效期为12个月,在有效期满后检测试剂盒的准确度、空白限、线性、重复性、质控品的赋值有效性,应符合2.2、2.3、2.4、2.5、2.7的要求。
2.9 分析特异性测定浓度为50.00ng/mL的白介素1α( IL-1α)、50.00ng/mL的白介素1β( IL-1β)、50.00ng/mL的白介素2(IL-2)、50.00ng/mL的白介素4(IL-4)样本,测定结果≤3.00pg/mL。
血清IL-6水平在小鼠术后早期内植物感染中的筛查作用

2 7 5
文章编号 :1 0 0 1 . 8 6 8 9 ( 2 0 1 3 ) 0 4 - 0 2 7 5 — 0 5
血 清I L . 6 水平在小鼠术后早期 内植物感 染 中的筛查作用
姚海1 刘涛1 王信 李平・ 周 园东 朱勇军3 张健1 , ’
Ab s t r a c t Ob j e c t i v e A mo u s e mo d e l o f e a r l y p o s t o p e r a t i v e i mp l a n t i n f e c t i o n wa s d e v e l o p e d t o c o mp a r e
we r e e q u a l l y d i v i d e d i n t o A, B,C a n d D g r o u p a t r a n d o m. Af t e r l o c a t i n g t h e f e mo r a l t r o c h l e a r g r o o v e , t h e r i g h t
2 De p a r t me n t o f S p i n e , he t Af il f i a t e d Ho s p i al t o f Zu n y i Me d i c a l Co l l e g e , Zu n y i 5 6 3 0 0 0 ;
3 De p a r t me n t o f Or t h o p e d i c s , t h e Ni n e t h P e o p l e ’ S H o s p i t a l o f C h o n g q i n g , C h o n g q i n g 4 0 0 7 0 0 )
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
CCL2recruitment of IL-6-producing CD11b +monocytes to the draining lymph nodes during the initiation of Th17-dependent B cell-mediated autoimmunityYing Bai*1,2,6,Ruolan Liu*2,DeRen Huang 3,Antonio La Cava 4,Yi-yuan Tang 1,Yoichiro Iwakura 5,Denise I.Campagnolo 2,Timothy L.Vollmer 2,Richard M.Ransohoff 3and Fu-Dong Shi 1,21Institute of Neuroinformatics and Laboratory for Brain and Mind,Dalian University of Technology,Dalian,China2Barrow Neurological Institute,St.Joseph's Hospital and Medical Center,Phoenix,AZ,USA 3Neuroinflammation Research Center,Department of Neurosciences,Lerner Research Institute,Cleveland Clinic Foundation,Cleveland,OH,USA4Division of Rheumatology,David Geffen School of Medicine,University of California,Los Angeles,CA,USA5Center for Experimental Medicine,Institute of Medical Science,University of Tokyo,Tokyo,Japan6Division of Neurology,Xin Hua Hospital,Dalian University,Dalian,ChinaThe development and function of Th17cells are influenced in part by the cytokines TGF-b ,IL-23and IL-6,but the mechanisms that govern recruitment and activity of Th17cells during initiation of autoimmunity remain poorly defined.We show here that the development of autoreactive Th17cells in secondary lymphoid organs in experimental autoimmune myasthenia gravis –an animal model of human myasthenia gravis –is modulated by IL-6-producing CD11b +cells via the CC chemokine ligand 2(CCL2).Notably,acetylcholine receptor (AChR)-reactive Th17cells provide help for the B cells to produce anti-AChR antibodies,which are responsible for the impairment of the neuromuscular transmission that contributes to the clinical manifestations of autoimmunity,as indicated by a lack of disease induction in IL-17-deficient mice.Thus,Th17cells can promote humoral autoimmunity via a novel mechanism that involves CCL2.Key words:Autoantibodies ÁCCL2ÁMyasthenia gravis ÁTh17Supporting Information available onlineIntroductionHelper CD4+T cells that are characterized by the production of IL-17are commonly called Th17cells [1–6].Th17cells have features that are distinct from those of both Th1and Th2lineages.For example,TGF-b and IL-6are required for the generation ofTh17cells,and IL-23supports the survival and expansion of these cells [1–8].Recent data also suggest that IL-6and TGF-b drive initial lineage commitment of Th17cells,whereas IL-23mediates the full acquisition of pathogenic function of Th17cells [9].Studies in several experimental models have indicated that IL-17is a major mediator of tissue inflammation and autoimmunedisease*These authors contributed equally to this work.Correspondence:Dr.Fu-Dong Shi e-mail:Fu-Dong.Shi@[4–6],but the cellular source of the cytokines and chemokines required for Th17development and recruitment during initiation of autoimmunity have not been investigated as yet.The CC chemokine ligand2(CCL2),initially known as monocyte chemoattractant protein1(MCP-1),is expressed by inflammatory cells at sites of tissue injury[10–13].CCL2directs the migration of monocytes,dendritic cells,NK cells and T cells, and coordinates inflammatory responses during infection[13]. Here we tested the possibility that CCL2-mediated homing of monocytes may affect Th17cells in a mouse model of human myasthenia gravis(MG),the experimental autoimmune MG (EAMG)model.In MG and EAMG,the cardinal sign of weakness is mediated by circulating IgG autoantibodies to the acetylcholine receptor(AChR)or to other muscular antigens at the neuromus-cular junction[14,15].We show here that CCL2plays a critical role in coordinating cognate interactions among IL-6-producing CD11b+cells,auto-reactive Th17cells,and B cells.These interactions appear critical in the genesis of autoantibodies and in subsequent development of EAMG.ResultsExpression of CCL2in EAMGIn C57BL/6(B6)mice,EAMG presents as a protracted,progressive form of muscular weakness[16].This presentation differs from the bi-phasic form of this disease characterized by early muscular inflammatory infiltration in Lewis rats[17].Since the expression of CCL2can be important for the pathogenesis of EAMG in the Lewis rat model[18],we measured CCL2levels in EAMG B6mice at the sites of injections as well as in secondary lymphoid organs (lymph nodes and spleen).By ELISA,CCL2was hardly detectable in naïve mice(0.03Æ0.02pg/mg tissue).However,CCL2 expression was elevated in AChR/CFA-injected mice at the sites of immunization,in lymph nodes,and in spleens(Fig.1).CCL2-deficient mice developed mild muscular weakness upon induction of EAMGTo investigate directly whether CCL2contributes to the develop-ment of EAMG,we immunized CCL2–/–mice and control B6mice with AChR in CFA.Muscular weakness characteristic of MG was apparent in control mice around day14post immunization(p.i.), and became severe after booster immunizations on days30and 60,when the clinical score maximized at2.5Æ0.3.By contrast, no signs of muscular weakness were observed until day25p.i.in the CCL2–/–mice,and their disease remained mild(maximal clinical score of0.6Æ0.2,p<0.01)even after booster immuniza-tions(Fig.2A).Also,the CCL2–/–mice had less muscle AChR loss compared to control mice(Fig.2B).Thus,CCL2–/–mice are developed milder behavioral and histological disease after the induction of EAMG.B cell and autoantibody responses in CCL2–/–miceIn MG and EAMG,major immune effectors of the disease process at the neuromuscular junctions are circulating IgG autoantibodies reactive to AChR,whereas the cellular inflammatory infiltrates in the muscles are sparse and not considered essential for the impaired neuromuscular transmission,both in humans and mice [16,19,20].Therefore,we measured anti-murine AChR IgG(and related isotypes)in CCL2–/–mice and control miceimmunized L2expression in EAMG.C57BL/6(B6)mice were injectedwith AChR in CFA and sacrificed3or7days later.Tissues from theinjection sites as well as from spleens and lymph nodes were preparedas homogenates.The content of CCL2in the supernatant wasquantified by ELISA(n=4mice/group.*p<0.05).L2–/–mice are less susceptible to the induction of EAMG.B6mice and CCL2–/–mice were immunized with AChR/CFA on days0,30and60to induce EAMG.(A)Animals were then evaluated every2–3daysfor characteristic muscle weakness as described in Materials andmethods.(B)Loss of muscle AChR content.The muscle tissues wereremoved from the mice in(A)at the termination of experiments and thepercentage loss of muscle AChR was quantified.All results areexpressed as mean values+SD.**p<0.01.with pared with controls,CCL2–/–mice had only a marginal reduction of total anti-AChR IgG levels (p <0.06)(Fig.3A).Although the levels of anti-AChR IgG1and IgG2a were similar in the two groups,the amounts of anti-AChR IgG2b were markedly lower in the CCL2–/–mice (p <0.01)(Fig.3A).The same results were obtained for anti-torpedo AChR IgG in AChR-immunized control and CCL2–/–mice (control vs .CCL2–/–mice:IgG, 1.6Æ0.5vs .0.7Æ0.2,p =0.42;IgG2b, 1.2Æ0.2vs .0.3Æ0.1,p =0.008).CCL2exerts its function through its receptor CCR2in vivo [11,13].CCR2expression has been recently described on B cells and influences B cell functions [21,22].To determine whether the altered autoantibody response in CCL2–/–mice could be linked to CCR2expression on B cells,we purified B cells from control mice and CCL2–/–mice for studies of proliferation and production of antibodies.As shown in Fig.3B,B cells from control mice and from CCL2–/–mice proliferated at a similar extent after BCR and CD40cross-linking.The number of plasma cells generated from control and CCL2–/–B cells after BCR stimuli were similar (Fig.3C),and so were the levels of total IgG and IgG2b released from plasma cells (Fig.3D).Thus,CCL2deficiency does not impair the capacity of B cells to proliferate,differentiate into plasma cells,or release IgG antibodies.Although the intrinsic features of antibody responses are preserved in CCL2–/–mice,it is possible that CCL2–/–B cells may have an altered capacity in migration during the immune response,since B cells express CCR2.To examine this possibility,we quantified CD19+B cells in several peripherallymphoid organs (spleen and lymph nodes)during the course of EAMG.There was no significant alteration in B cell percentage and numbers between control mice and CCL2–/–mice (Supporting Information Fig.1).It was thus unlikely that the observed phenotype of EAMG in CCL2–/–mice was due to the defects in B cell migration.Impaired Th17responses in CCL2–/–miceThe altered levels of IgG autoantibodies in the AChR-primed CCL2–/–mice,associated with an intact B cell proliferation and differentiation,led us to investigate the phenotype of T cells in this model.In the absence of CCL2,T cell proliferation was not significantly altered,as reflected by CFSE dilution experiments (Supporting Information Fig.2).Nonetheless,the preferential reduction of the levels of anti-AChR IgG2b suggested altered Th cell L2plays a role in the development of both Th2and Th1cells [11,23].In our model,IFN-c production by CD4+T and CD8+T cells in response to AChR stimulation was marginally impaired in CCL2–/–mice (Fig.4A and B;Supporting Information Fig.3),and both CCL2–/–mice and controls produced similar amounts of IL-4(Fig.4D and E).Since the cytokine IL-17is an important mediator of tissue inflammation and Th17cells are important in the pathogenesis of several autoimmune conditions [1–6],we tested the role oftheseFigure 3.B cells are functionally intact in the CCL2–/–L2–/–mice and control mice were immunized with AChR/CFA as described in Materials and methods .(A)Serum samples were collected from mice as decribed in Fig.2at the termination of the experiments.Anti-AChR IgG antibodies and IgG isotypes were determined by ELISA (n =16–18)on AChR-coated plates.Mice were sacrificed on day 14p.i.,and lymph nodes cells were cultured with or without B-cell stimuli.(B)Proliferation of B cells measured as [3H]thymidine incorporation.(C)Plasma cell differentiation after polyclonal B cell stimulation measured by FACS.(D)Antibody production in the culture supernatants of plasma cells from spleen (left bars)and lymph nodes (right bars)(n =4/group).All results are expressed as mean values ÆSD.**p <0.01.cells in EAMG,because it is not known how and/or whether Th17cells contribute to this disease.We first compared Th17cell responses to AChR between wild-type (B6)and CCL2–/–T cells.Interestingly,CCL2–/–T cells failed to mount an effective Th17response to AChR (Fig.4A and C).To determine whether CCL2–/–T cells have intrinsic defects in Th17differentiation,we sorted CD4+CD44+T cells from control mice and CCL2–/–mice and cultured them in the presence or absence of IL-6and TGF-b for 48h.Levels of IL-17were similar for control T cells and CCL2–/–T cells (8834Æ322vs .8923Æ202ng/mL),showing that CCL2–/–Tcells do not have an intrinsic defect in Th17differentiation.The failure in mounting Th17cells in CCL2–/–mice must thus derive from other factors.CCL2modulates the homing of CD11b +cells to lymphoid organsPhenotypic commitment of Th17cells is dependent on IL-6[1–6].To study the mechanism underlying the impaired generation of Th17cells in AChR-immunized CCL2–/–mice,we quantified IL-6in several cell types of EAMG mice.As shown in Fig.5A,CD11b +cells and,to a lesser degree,CD11c +cells were the predominant sources of IL-6.The production of IL-6in the supernatants from cultured spleen and lymph node cells of CCL-2–/–mice was significantly lower than that of controls (Fig.5B).Since CCL2–/–mice had low levels of IL-6,a cytokine mainly produced by CD11b +cells,we sought to address whether CCL2deficiency altered the homing of CD11b +cells to lymph nodes or spleens,i.e .,causing a secondary reduction of IL-6production.We found no significant difference in the numbers and percentages of CD4+,CD8+,NK1.1+CD3–(NK cells)or NK1.1+CD3+(NKT)cells in lymph nodes of control mice and CCL2–/–mice (Supporting Information Fig.4).However,the numbers of CD11b +and CD11b +CD11c +cell populations were reduced in spleens (Fig.5C)and the lymph nodes of CCL2–/–mice (Supporting Information Fig.5).These data suggested that CCL2deficiency may interfere with homing of CD11b +cells and CD11b +CD11c +cells to peripheral lymphoid organs,which in turn reduces IL-6avail-ability for development of Th17cells.IL-6–/–mice fail to mount AChR-induced Th17responsesIn a previous study,IL-6–/–mice were found resistant to the induction of EAMG [24].Our current data taken in the content of recent findings [9]suggest that the resistance to EAMG could derive from faulty development of Th17cells.Since this could be secondary to IL-6deficiency,we measured autoantigen-induced Th17responses in IL-6–/–mice immunized with AChR/CFA.Consistent with previous reports [24],IL-6–/–mice wereresistantFigure 4.Th17responses are impaired in the CCL2–/–mice.Splenocytes from B6and CCL2–/–mice immunized with AChR/CFA were harvested at day 7–14p.i.and stimulated with10l g/mL AChR in culture medium for 3–5days.For intracellular cytokine staining,cells were restimulated with PMA/ionomycin/brefeldin A for further 5h,then IFN-c -,IL-4-,and IL-17-producing cells were detected by flow cytometry as described in Materials and methods .Results were shown in representative plots from three separate experiments (n =4–6mice/group)and bar graphs for summary data.(A–C)AChR-induced IFN-c and IL-17production by CD4+cells.(D,E)AChR-induced IL-4production by CD4+cells.**p <0.01.to the induction of EAMG.Importantly,IL-6–/–mice had impaired capacity to mount AChR-induced production of IL-17in CD4+cells,while IFN-c production was not altered significantly (Fig.6).These results indicate a role of IL-6in the development of Th17cells and not Th1responses in EAMG.IL-17facilitates autoantibody responses and clinical EAMG independently of IFN-cNext,we injected recombinant IL-17into AChR-primed mice during the T cell priming period,and then compared the outcome to that of mice given only PBS injections.Significantly,recipients of IL-17developed severe EAMG and elevated titers of AChR-specific IgG and IgG2b,as compared to controls (Fig.7A and B).We and others [25–27]have previously found that the development of EAMG is not dramatically altered by IFN-cdeficiency.To investigate whether the effects of IL-17on EAMG were related to or depended on IFN-c ,we treated IFN-c –/–mice with IL-17during EAMG induction,using the same regimen used for the B6mice.We found that IFN-c –/–mice and controls responded with elevated anti-AChR antibody production and clinical EAMG at similar magnitudes (Fig.7C and D).These data indicate that IL-17rather than IFN-c influences humoral autoimmune responses in EAMG.IL-17restores EAMG severity of CCL2–/–mice to that of wild-type miceIf the failure to mount autoreactive Th17responses contributes to milder EAMG in the CCL2–/–mice,provision of exogenous IL-17to CCL2–/–mice should reverse this phenotype.To test this hypothesis,we treated CCL2–/–mice with IL-17or PBS attheFigure L2controls homing of IL-6-producing CD11b +cells.B6and CCL2–/–mice were immunized with AChR/CFA to induce EAMG and sacrificed on day 7–14p.i.(A)Production of IL-6by CD4+cells,NK1.1+cells,CD11c +cells and CD11b +cells from B6mice was quantified by intracellular IL-6staining.(B)IL-6released from draining lymph nodes was measured in B6mice as well as CCL-2–/–mice by ELISA (n =4–7each/group).(C,D)Single-cell suspensions of spleen were stained with PE-Cy7-labeled anti-mouse CD11b and allophycocyanin-labeled anti-mouse CD11c before analysis by FACSAria using Diva software.Results represent three independent experiments with reproducible outcomes.**p <0.01.time of induction of pared with PBS-treated CCL2–/–mice that exhibited milder EAMG,AChR-primed CCL2–/–mice treated with IL-17exhibited early onset of muscular weakness (median day of onset:13Æ2vs .27Æ4)that progressed to severe weakness over time (maximum severity 2.6Æ0.3vs .1.5Æ0.2,Fig.7E).Treatment with IL-17elicited higher anti-AChR IgG and prominent IgG2b responses (Fig.7F).These data indicate that defective Th17responses contribute to the reduced severity of muscular weakness in the CCL2–/–mice.Autoreactive Th17cells drive IgG2b antibody response in vivoTransfer of myasthenogenic lymphocytes from humans with MG or from EAMG mice results in clinical EAMG [28,29].We isolated CD4+cells from control mice and CCL2–/–for transfer into RAG1–/–deficient mice (which are devoid of intrinsic T and B cells)[30].The transferred CD4+cells preferentially produced Th17in control mice but not in CCL2–/–mice.Naive B220+B cells were co-transferred into the RAG1–/–recipient mice.At 2weeks following immunization with AChR/CFA,production of anti-AChR IgG and IgG isotypes were evaluated.Mice receiving T cells from CCL2–/–mice had marginally reduced levels of total anti-AChR IgG and significantly reduced levels of IgG2b (Table 1),compared to mice receiving T cells from control EAMG mice.Mice receiving T cells from CCL2–/–mice scarcely developed behavioral signs of EAMG (Table 1).In control experiments,transferred control CD4+cells maintained the Th17phenotype in the recipient mice (percentages of IL-17+CD4+cells:7.2Æ1.6%(control)vs . 1.3Æ0.2%(CCL2–/–),p <0.01).Collectively,these data suggest that auto-reactive Th17cells help B cells to produce pathogenic antibodies,particularly the IgG2b subtype.IL-17-deficient mice develop mild EAMGTo further elucidate the role of IL-17/Th17in EAMG,we immunized control mice and IL-17–/–mice with AChR and CFA and monitored the development of pared to control mice,IL-17–/–mice exhibited significantly milder EAMG,as reflected by evaluation of muscular weakness (Table 2).Produc-tion of IgG2b was impaired in the IL-17–/–mice (Table 2).Table L2–/–CD4+T cells are poor helpers for B cells a)Source of T cells No.of T cells No.of mice/group Disease inci-dence (%)Loss of muscle AChR Mean maximal severity of EAMG (ÆSD)Anti-AChR IgG b)(OD 405)Anti-AChR IgG2b b)(OD 405)B65Â1066(6/6)10053.3Æ12.7% 1.87Æ0.22 1.84Æ0.23 1.21Æ0.20CCL2–/–5Â1067(1/7)14.318.4Æ9.6%0.13Æ0.07*1.03Æ0.300.31Æ0.06*a)CD4+cells were enriched and purified from AChR and CFA primed control mice and CCL2–/–mice and were co-transferred with 5Â106B220+B cells into RAG1–/–recipient mice.b)Muscle weakness was monitored for 55days following cell transfer,sera were collected at the termination of experiments for anti-AChR antibody ELISA.Loss of muscle AChR was quantified by RIA.*p <0.05.Figure 6.AChR-primed IL-6–/–mice fail to mount Th17responses.B6and IL-6–/–were immunized with AChR/CFA as described in Fig.1.Mice were sacrificed on day 7–14p.i.Production of IL-17and IFN-c by cultured spleen cells in response to AChR stimulation (10l g/mL)was measured by intracellular cytokine staining.(A)Expression of CD4vs.intracellular IL-17(upper panel)and IFN-c (lower panel)was compared within this gate.Representative plots are from one of three experiments using 2–3mice/group.(B,C).CD4+cells expressing IFN-c or IL-17in control mice and IL-6–/–mice (n =4–6/group).*p <0.05.DiscussionThis study implicates Th17responses in B cell-dependent (auto)immunity,and establishes a novel role for CCL2in the development of Th17responses.Increasing evidence supports the role of Th17cells in several models of inflammation and autoimmunity.Here we show that the chemokine CCL2,which is elevated during inflammation,is required for the recruitment of IL-6-producing CD11b +cells involved in the generation of autoreactive Th17cells in EAMG.Our model implies that in the lymph node CD11b +APC can produce IL-6to polarize Th cells toward a Th17phenotype,and then the Th17cells can provide help to B cells for the production of pathogenic IgG2b antibodies mediating functional blockade at the neuromuscular junction.It has long been known that autoimmune diseases such as EAMG are associated with elevated production of proinflamma-Table 2.IL-17–/–mice exhibit mild EAMG with reduced incidence a)MiceNo.of mice/group Disease inci-dence (%)Loss of muscle AChR Mean maximal severity of EAMG (ÆSD)Anti-AChR IgG (OD 405)Anti-AChR IgG2b (OD 405)B68(7/8)88%47.6Æ9.2% 1.64Æ0.33 1.91Æ0.34 1.35Æ0.41IL-17–/–4(0/4)010.0Æ2.3%0.09Æ0.05**0.94Æ0.200.22Æ0.03**a)Mice were immunized with AChR and CFA.Muscle weakness was monitored for 35days following the immunization,and sera were collected at this time for anti-AChR antibody ELISA.Loss of muscle AChR was quantified by RIA.**p <0.01.Figure 7.Role of IL-17in EAMG.Groups of B6(A,B),IFN-c –/–(C,D)and CCL-2–/–(E,F)mice were immunized with AChR/CFA and received IL-17or PBS starting at the date of immunization (see Material and methods ).Determination of development of EAMG (A,C,E)and production of anti-AChR antibodies (B,D,F)(n =8/group).*p <0.05,**p <0.01.tory mediators by several cell types.However,the understanding of the intermediate events between immunogenic exposure to autoantigen and subsequent downstream activation of pathogenic immune response has been limited.We found that CCL2-deficient mice developed milder behavioral and histological disease following the induction of EAMG.This result was surprising because monocyte infiltrates,the hallmark of CCL2action,are not prominent in EAMG muscle[24]. This defect was not caused by impaired function of autoreactive B cells,which remained intrinsically intact in the absence of CCL2. However,their capacity to produce anti-AChR IgG antibody,in particular IgG2b,was drastically reduced following immunization. Incidentally,IgG2b is highly myasthenogenic[31].The involvement of CCL2in several experimental models of inflammation and autoimmunity is well established,and appears to partly depend on the ability of this chemokine to direct the inflammatory influx to target organs and to promote Th1and/or Th2cells[10–13].The autoimmune model of EAMG differs from the other systems studied for at least two reasons.First,the muscular weakness characteristic of EAMG is primarily mediated by anti-AChR IgG antibodies produced by autoreactive B cells[19]. Second,because the inflammatory infiltrates are sparse and unrelated to the neuromuscular junctions in EAMG,their contribution to muscular weakness,if any,is likely minute[19]. As such,the B cell-mediated autoimmune process of EAMG, associated with limited inflammation,may represent a system with unique characteristics for studying the immune role of CCL2 independently of inflammation in tissue.We report that the regulation of the immune response to AChR by CCL2is sufficient to alter the magnitude of the symptoms of EAMG,yet CCL2does not directly affect the function of autoreactive B cells in EAMG,as indicated by the fact that upon BCR-cross-linking,CCL2–/–B cells proliferated efficiently,differ-entiated into plasma cells,and released antibodies at a level comparable with controls.Rather,an altered function of Th17cells was most likely responsible for the observed impaired autoanti-body response.CCL2has been reported to affect both Th1and Th2cells[11, 23].We add to this list Th17cells.We think that since we used B6 mice,which are a Th1-prone strain(and immunization with CFA further drove Th1responses),CCL2might have had limited effects on Th2cells in this system.On the other hand,the production of autoantibodies to AChR is clearly a T cell-driven process,which must rely in part on Th1responses,given our finding of preferential IgG2b autoantibodies[32].Although earlier work had indicated that ectopic expression of IFN-c at the neuromus-cular junction provoked MG-like disease[33],our current understanding of the role of IFN-c in EAMG is far from conclusive. For example,mice deficient of IFN-c[25]or IFN-c receptor[26] are resistant to EAMG,yet some groups have shown that IFN-c deficiency may not significantly alter the course of disease[27, 34].Thus,while Th1responses may possibly play a role in the disease depending on the experimental system used,the question arises on whether other inflammatory cytokine(s)with potent pro-pathogenic effects,such as IL-17,are required for the expression of EAMG.We found that AChR-primed CCL2–/–mice failed to mount an effective Th17response,which correlated with an impaired anti-AChR IgG2b response associated with milder disease.The failure to mount productive Th17responsiveness most likely came from impaired homing of the IL-6-producing CD11+cells to the secondary lymphoid organs,as CCL2–/–T cells maintained the capacity to produce IL-17after stimulation.Also,AChR-primed IL-6–/–mice had significantly reduced autoantigen-reactive Th17 responses,and IL-17injection enhanced both the humoral response to AChR and clinical EAMG in B6mice as well as in the IFN-c–/–mice.Finally,CCL2–/–CD4+T cells failed to help B cells to produce disease inducing IgG2b.It has been reported that IL-6–/–mice had impaired anti-AChR IgG2b response upon immunization with AChR[24].The question arises as whether the impaired IgG2b response is due to the lack of IL-6,or altered IL-17response in IL-6–/–mice,or both.Injection of IL-17can partially restore the capacity to mount an IgG2b response in IL-6–/–mice and reestablish susceptibility to the induction of EAMG in these mice.These results emphasized the importance of IL-17in the generation of IgG2b response and the expression of clinical EAMG.Th17cells express CCR2[35].It is plausible that abnormal migration of Th17cells in the CCL2–/–mice also contributes to the mild muscular weakness in this strain.This possibility is currently under investigation.We have not examined the development of EAMG in CCR2–/–mice.Several published works have shown that CCR2–/–mice are resistant to experimental autoimmune diseases,including the B cell-dominant lupus model[36,37].These observations support our current findings and emphasize the importance of CCR2-CCL2 pathway in the development of autoimmunity.The present study focused on the role of CCL2in recruiting IL-6-producing cells capable of promoting generation of auto-reactive Th17responses in B cell-dependent(auto)immunity.We found,further,that Th17plays a central role in humoral immunity in EAMG.We propose that inflammation associated with immunization recruits CD11b+mononuclear phagocytes to lymph nodes,a phenomenon that depends on CCL2.In the lymph nodes of wild-type mice,APC present the autoantigen to Th0cells and make IL-6,in conjunction with other cytokines including TGF-b and IL-23,which polarizes Th cells toward a Th17phenotype.The Th17cells are then required as helpers for the production of high titers of pathogenic anti-AChR IgG2b antibodies from B cells.In the light of new finding by Hsu et al.[38],IL-17may also promote the development of germinal centers.Antibodies to AChR are ultimately responsible for the block at the neuromuscular junction that leads to muscular weakness.It will be important to address next whether CCL2may be a specific therapeutic target to modulate clinical MG.MiceC57BL/6(B6)mice deficient of MCP-1(MCP-1–/–)[11],IL-6 (IL-6–/–),IFN(IFN-c–/–)and RAG(RAG-c–/–)[30]were purchased from The Jackson Laboratory(Bar Harbor,ME).IL-17–/–mice were provided by Dr.Yoichiro Iwakura[5].All mutant mice had been backcrossed to those of the B6background for at least ten generations.Only female mice of7–8weeks of age(at the initiation of the experiments)were used.All mice were bred and maintained in pathogen-free conditions at the animal facilities of the Barrow Neurological Institute in accordance with the Institutional Animal Care and Use Committee regulations.Antigens and peptidesAChR was purified from the electric organs of Torpedo californica (Pacific Biomarine,Venice,CA)by affinity chromatography on a a-cobratoxin-agarose resin(Sigma,St.Louis,MO)[39,40].The isolated product was pure as judged by SDS-PAGE.The AChR a146–162(LGIWTYDGTKVSISPES)peptide was synthesized by Biosynthesis Inc.(Lewisville,TX).Induction,clinical and laboratory evaluation of EAMGMice were injected subcutaneously(s.c.)between the shoulders and back with20l g AChR in CFA in a total volume of100l L. After1month,all mice were boosted once with20l g AChR in IFA s.c.at four sites on shoulders and thighs[38,39].The mice were observed every other day in a blinded fashion for signs of muscle weakness characteristic of EAMG.Clinical manifestations of EAMG were graded from0to3[39]:0,no definite muscle weakness;1+, normal strength at rest but weak with chin on the floor and inability to raise the head after exercise consisting of 20consecutive paw grips;2+,as grade1+and weakness at rest; and3+,moribund,dehydrated,paralyzed.To verify the myasthenic nature of the weakness,we injected i.p.edrophonium chloride(Reversol;Organon,West Orange,NJ),a cholinesterase inhibitor that immediately increases the strength of mice that have clinical EAMG.To further verify the extent of EAMG,we quantified the muscle AChR content by radioimmunoassay using125I-labeled a-bungarotoxin,(Amersham Corp.,Arlington Heights,IL)[27].IL-17injectionRecombinant murine IL-17was purchased from eBioscience(San Diego,CA).At EAMG induction,mice received daily1l g IL-17(in PBS)/mouse i.p.for7consecutive days.Control mice received equal volumes of PBS.Measurement of anti-AChR IgG antibodiesAnti-murine AChR IgG antibodies and anti-torpedo AChR IgG antibodies were detected by ELISA as described previously[39, 40].Briefly,microtiter plates(Corning Glass Works,Corning,NY) were coated with100l L/well murine AChR(0.5l g/mL)or torpedo AChR(2l g/mL)at4 C overnight.After blocking with 10%FBS,serum samples were added and incubated for2h at room temperature.Plates were then incubated for2h with biotinylated rabbit anti-mouse IgG,IgG1,IgG2a,and IgG2b (Invitrogen,Carlsbad,CA),followed by alkaline phosphatase-conjugated ABC reagent(Dakopatts;R&D systems,Minneapolis, MN),and color developed with p-nitrophenyl phosphate.Results were expressed as OD at405nm.CCL2ELISAThe s.c.injection sites and draining lymph nodes were removed from sacrificed control mice and CCL2–/–mice,weighed, homogenized in lysis buffer(PBS with1mM PMSF,0.01mg/ mL aprotinin,and0.01mg/mL leupeptin),sonicated,and centrifuged.The supernatant was assayed for CCL2immunor-eactivity by ELISA(Quantikine;R&D systems,Minneapolis,MN) following the manufacturer's instructions[12].B cell proliferation and differentiationTo determine the extent of B cell proliferation,105purified CD20+CD27+B cells were cultured in96-well round-bottom plates and stimulated with24l g/mL goat-anti-mouse IgM alone or in combination with5l g/mL anti-mouse CD40[41].After 3–5days of culture,[3H]thymidine was added to the culture for additional18h.[3H]Thymidine uptake was measured using a liquid scintillation counter.In some experiments,stimulated and control cultures were stained after various intervals with anti-CD19PerCP-Cy5.5(1D3)and allophycocyanin-conjugated anti-CD138(281–2)to visualize plasma cells,which were identified as CD19low/–CD138+cells[42].Plasma cell differentiation in AChR-primed control mice and CCL2–/–micePurified B cells from lymph nodes were either left unstimulated or stimulated with a combination of anti-CD40and IgM.After6days of culture,B cells were identified as CD19+and plasma cells as CD19low/–CD138+.。