病理图谱2
正常肝脏与肝脏胆管病理组织切片彩色图谱大全
正常肝脏与肝脏胆管病理组织切片彩色图谱大全肝小叶( hepatic lobule)是肝的基本结构单位,呈多角棱柱体,长约2mm,宽约1mm, 人的肝小叶间结缔组织很少,相邻肝小叶常连成-片,分界不清(图15-7,图15-8)。
肝小叶中央有一条沿其长轴走行的中央静脉( central vein) ,周園是大致呈放射状排列的肝索和肝血窦。
门管区:位相邻肝小叶间,为三角形或椭圆形结缔组织小区,内含伴行小叶间动脉、小叶间静脉和小叶间胆管。
有时在肝小叶间的结缔组织中可见一条单独的静脉即小叶下静脉。
小叶间胆管由单层立方或柱状上皮围成。
图13-10肝门管区图示壁厚腔小的是小叶间动脉(※)、壁薄腔大的是小叶间静脉(★),单层立方上皮构成,核深蓝色圆形的是小叶间胆管(↑)。
天马波波胆小管( bile canaliculus) 是相邻两个肝细胞之间局部胞膜凹陷形成的微细管道,在肝板内连接成网。
靠近胆小管的相邻肝细胞膜形成由紧密连接、桥粒等组成的连接复合体,可封闭胆小管周围的细胞间隙,防止胆汁外溢至细胞间或窦周隙。
当肝细胞发生变性、坏死或胆道堵塞而内压增大时,胆小管的正常结构被破坏,胆汁则溢人窦周隙,继而进人肝血窦,导致机体出现黄疸。
相邻肝小叶之间呈三角形或椭圆形的结缔组织小区,称门管区( portal area) , 每个肝小叶周围有3 ~4个门管区。
门管区内有小叶间静脉、小叶间动脉和小叶间胆管。
小叶间静脉是门静脉的分支,管腔较大而不规则,管壁薄;小叶间动脉是肝动脉的分支,管腔小,管壁相对较厚。
小叶间胆管管壁为单层立方上皮,它们向肝门方向汇集,最后形成左、右肝管出肝。
在非门管区的小叶间结缔组织中,还有单独走行的小叶下静脉,由中央静脉汇集形成,它们在肝门部汇集为肝静脉。
胆小管胆囊分底、体、颈三部分,颈部连胆囊管。
胆囊壁由黏膜、肌层和外膜三层组成。
黏膜有许多高而分支的皱襞突人腔内。
胆囊收缩排空时,皱襞高大而分支;胆囊充盈扩张时,皱襞减少变矮。
(仅供参考)动脉粥样硬化病理图谱

中年人增厚的内膜
中性粒细胞在内皮上的黏附(1)
中性粒细胞在内皮上的黏附
重度钙化动脉粥样硬化
粥瘤处细胞增殖及细胞外基质形成
粥瘤破裂(1)
粥瘤破裂(2)
粥瘤破裂(3)
粥瘤破裂(4)粥瘤破裂(来自)粥瘤破裂(6)粥瘤破裂(7)
粥瘤破裂
粥瘤纤维化
粥瘤纤维帽形成
粥瘤与纤维帽(1)
冠状动脉的血栓再通(1)
冠状动脉的血栓再通
冠状动脉粥样硬化
冠状动脉粥样硬化横切面
门克伯格正中动脉钙化性动脉粥样硬化
内膜平滑肌细胞增殖(1)
内膜平滑肌细胞增殖(2)
内膜平滑肌细胞增殖
泡沫细胞
染色的脂核
少量脂纹沉积的主动脉
肾脏内的胆固醇栓塞
肾脏增生性动脉粥样硬化
完整内皮下的早期脂纹
电镜下的巨噬细胞趋化至内皮下
电镜下的早期脂纹
动脉壁上的CD-68的表达
动脉壁上的ICAM-1的表达
动脉壁上的VCAM-1的表达
动 脉 内 膜 成 肌 纤 维 胞 破 坏
动 脉 内 膜 成 肌 纤 维 胞 增 殖
动脉粥样硬化
复杂性粥瘤
钙化的粥样硬化性冠状动脉
冠脉脂纹
冠状动脉斑块内出血
动脉粥样硬化病理图谱
HE染色下的中期脂纹
斑块钙化(1)
斑块钙化
斑块广泛钙化
伴糖尿病的肾脏玻璃样的动脉粥样硬化
薄纤维帽(1)
薄纤维帽(2)
不同程度动脉粥样硬化的主动脉
带血栓斑的动脉粥样硬化
带有血栓的冠状动脉粥样硬化
胆固醇裂缝
胆固胆醇固裂醇隙裂隙
电镜下的单核巨噬细胞黏附在内皮上
粥瘤与纤维帽
粥瘤中的淋巴细胞浸润(1)
医学培训教材 病理切片图谱
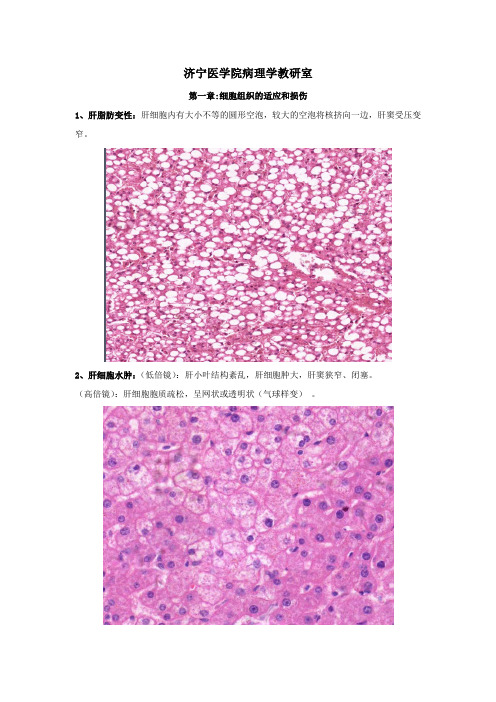
济宁医学院病理学教研室第一章:细胞组织的适应和损伤1、肝脂肪变性:肝细胞内有大小不等的圆形空泡,较大的空泡将核挤向一边,肝窦受压变窄。
2、肝细胞水肿:(低倍镜):肝小叶结构紊乱,肝细胞肿大,肝窦狭窄、闭塞。
(高倍镜):肝细胞胞质疏松,呈网状或透明状(气球样变)。
第二章:损伤修复肉芽组织:皮肤损伤(形成溃疡),溃疡底部部分坏死组织,炎细胞浸润。
肉芽组织描述基本同上。
结缔组织出血、水肿哦那个,可见较多新生的毛细血管(与创面垂直生长)及成纤维细胞,各种炎细胞。
(高倍镜):(1)新生毛细血管:有内皮细胞组成的管腔,有尚未形成管腔的内皮细胞(标注),毛细血管的生长多与创面垂直。
(2)成纤维细胞(标注):胞质淡染、多突起,胞核呈卵圆形,结构较疏松透亮,有1-2个核仁,少数细胞呈梭形,胞核稍致密。
第三章:局部血液循环障碍1、混合血栓:(血栓)由珊瑚状血小板梁及纤维素、红细胞及中性粒细胞构成(血栓内可见粉红色分枝状血小板梁,小梁表面有中性粒细胞粘附,小梁之间为红细胞和纤维素)。
2、肝淤血:(低倍镜):肝小叶结构尚存,中央静脉及肝窦扩张,充满红细胞,部分肝小叶之间淤血区相互连接,形成淤血带。
(高倍镜):肝细胞受压萎缩,部分肝细胞内见大小不等空泡(脂肪变性)。
3、慢性肺淤血:(低倍镜):肺泡壁毛细血管扩张、充血,肺泡腔内见棕褐色心力衰竭细胞及少量红细胞。
(高倍镜):“心力衰竭细胞”体积大,圆形,胞质内含有棕褐色颗粒。
4、肾凝固性坏死:镜下见淡染区为坏死组织,坏死组织区域内细胞核溶解消失,但肾小球和肾小管的轮廓依然保存。
正常与坏死组织之间为炎性反应带(中性粒细胞浸润)坏死区第四章:炎细胞(炎性息肉)各种炎细胞:(1)嗜中性粒细胞:细胞为圆形(直径10~12),核呈分叶状(2~3叶),胞质淡染,呈淡粉红色,并含有浅紫色嗜天青颗粒。
(2)大单核细胞:细胞为圆形,体积较大(直径14~20),核呈肾形、马蹄形或不规则形,着色较浅,胞质丰富,呈灰蓝色,内含淡紫色噬天青颗粒。
病理学图谱 实验二局部血液循环障碍

造成空气栓塞的主要途径有:
(1)动脉管路连接不紧或有裂缝,空气随之进入血液 (2)输液走空未及时发现 (3)回血操作时失误或血泵失控,气体进入体内 (4)空气监测器失灵,有气体时未报警
空气栓塞的处理要点:
(1)解除进气的因素 (2)立即给氧 (3)让病人取头低左侧卧位,使空气进入右心室,当血循环到 右心室,气泡会随氧气溶解到血液中 (4)空气较多时,影响到心脏排血,要行右心室穿刺 (5)必要时送高压氧舱治疗 (6)对症处理
6、 慢性肝淤血
肝血窦高度淤血、出血,肝细胞变性萎缩。
6、 慢性肝淤血
高倍镜下示扩张充血的中央静脉
6、 慢性肝淤血
淤血区周边的肝细胞有轻重不等的脂肪变性
7 、混合血栓
低倍镜下示混合血栓由血小板小梁和大量红细胞 组成
血栓形成示意图
7、 混合血栓
箭头示白色血栓,其他区域为红色血栓
7、 混合血栓
5、肺淤血水肿
肺泡间隔增宽,肺泡壁血管扩张充血,肺泡间隔及肺泡 腔内见心衰细胞
5、 肺淤血水肿
箭头示心力衰竭细胞,胞浆内含大量棕黄色的含铁血 黄素颗构
箭头示中央静脉
6、 慢性肝淤血
切面呈红黄相间,如槟榔条纹,故称槟榔肝
6、 慢性肝淤血
低倍镜下示:肝小叶结构模糊,中央静脉和血窦高 度扩张,充血
实验二 局部血液循环障碍 内容
一 理论复习 充血,淤血,出血,血栓,栓塞,梗死.
二 镜下标本 肺淤血水肿(5号切片) 慢性肝淤血(6号切片) 混合血栓 (7号切片)
三 大体标本
四 空气栓塞实验
5、肺淤血水肿
正常肺组织结构
5、肺淤血水肿
肺泡间隔增宽,肺泡间隔及肺泡腔内见淡红色水肿液 及心衰细胞
兽医病理学原色图谱
参考文献 :
【】 O i i , ia .e c bo[ ,0 4 9 :— 2 1 l er S Pj nCV t r il]2 0 ,91 1. v a o Mio J f1 Srw B E Zm r a , Ali , . 病 学 [ . 9版 . 2 t , imem nJJD' l r S 等 猪 a ae M1 第
5 6
养猪 S N R D C IN( WIEP O U TO 4 )
2 l 0O
达 1 ~ m;在巧克力培养基上 2 . 2m 5 4h长 出可见菌 3 讨 论 与小 结 落 ,8h菌落直径 可达 1 m左右; 4 m 在麦康 凯培养基 31 副猪嗜血杆菌是一种 多形态革兰 氏阴性细小杆 . 上不生长。 菌, 形状从球杆状到细丝状, 新分离菌株 多呈细丝状,
( 辑: 编 富春 妮 )
兽 医病理学原色 图谱 本书是 由中国畜牧兽医学会病理学分会理事 长 陈怀涛教 授组织 我 国 8 位 兽医病 理学专 家编 8 著 的兽 医病理 学的权威 专著,其 内容涵盖基础病 理和疾病病理 , 共选用 图片 23 1幅。基础病理主 6
要展示最基本 的病理形态变化 。疾病病 理包括猪、
禽 、 、 、 、 、 等 的主 要传染病 、 牛 羊 兔 犬 猫 寄生虫病 、 营养代谢病 、 中毒病及其他疾病 , 每种 疾病都附 以 图片 , 理论 结合实际 , 具有很高 的学术价值 , 是学 习兽 医病理学 必备的权威专著 。 全书 6 4页,精装 ,由中国农业 出版社 20 年 9 9 08 月出版。本刊服务部精品书 目编号 10号 。 0
北京: 中国农业大学出版社 ,0 84 7 4 6 20 :0 — 1.
新药毒理实验动物组织病理学图谱_11840095

[General Information]书名=新药毒理实验动物组织病理学图谱作者=苏宁 姚全胜主编 苏宁 姚全胜 陈平圣等参编页数=144SS号=11840095出版日期=2005年05月第1版前言目录 上篇 系统组织病理图第一章 心脏和大动脉第一节 心脏(heart)第二节 大动脉(large artery)第二章 消化系统第一节 口腔(oral tissues)第二节 消化管(digestive tract)第三节 消化腺(digestive glands)第三章 呼吸系统第一节 鼻腔(nasa cavity)第二节 气管和支气管(trachea and bronchus)第三节 肺脏(pulmonary)第四章 泌尿系统第一节 肾脏(kidney)第二节 膀胱(urinary bladder)第五章 雄性生殖系统第一节 睾丸(testis)第二节 附睾(epididymis)第三节 前列腺(prostate gland)第四节 精囊(seminal vesicule)第六章 雌性生殖系统第一节 卵巢(ovary)第二节 子宫(uterus)第三节 阴道(vagina)第四节 乳腺(mammary gland)第七章 神经系统第一节 大脑(cerebrum)第二节 小脑(cerebellum)第三节 脑干与脊髓(brain stem and spinal cord)第四节 视神经(optic nerve)第五节 坐骨神经(ischiatic nerve)第八章 淋巴造血系统第一节 脾脏(spleen)第二节 胸腺(thymus)第三节 淋巴结(lymph node)第四节 胸骨及骨髓(thorax and bone marrow)第五节 股骨及骨髓(femoris and bone marrow)第九章 内分泌系统第一节 甲状腺和甲状旁腺(thyroid and parathyroid)第二节 肾上腺(adrenals)第三节 垂体(hypophysis) 下篇 动物模型及药物刺激实验组织病理图第一章 常见的动物模型组织病理图第一节 异丙肾上腺素致大鼠心肌损伤模型第二节 四氯化碳诱发大鼠肝损伤模型第三节 脂肪肝模型第四节 氨基半乳糖实验性大鼠肝炎模型第五节 四氯化碳诱导的大鼠肝纤维化模型第六节 异种血清诱导的大鼠肝纤维化模型第七节 小鼠支气管肺炎模型第八节 急性呼吸窘迫综合征家兔模型第九节 链脲菌素复制大鼠糖尿病肾病模型第十节 牛磺胆酸钠盐复制大鼠胰腺炎模型第十一节 豚鼠胆囊炎模型第十二节 氯化高汞致小鼠急性肾损伤模型第十三节 大鼠肾功能衰竭模型第十四节 幽门结扎法致大鼠胃溃疡模型第十五节 乙酸法致大鼠胃溃疡模型第十六节 豚鼠溃疡性结肠炎模型第十七节 大鼠化脓性脑膜炎模型第十八节 电凝大鼠大脑中动脉致脑缺血模型第十九节 大鼠自体血致脑水肿模型第二十节 大鼠前列腺炎模型第二十一节 丙酸睾丸酮致大鼠前列腺增生模型第二十二节 化学致癌剂诱发大鼠乳腺癌模型第二十三节 乳腺增生动物模型第二十四节 大鼠慢性盆腔炎模型第二十五节 大鼠子宫平滑肌瘤模型第二十六节 大鼠骨质疏松症模型第二十七节 骨折模型的复制及愈合第二十八节 大鼠佐剂性关节炎模型第二章 药物刺激试验组织病理图第一节 家兔耳缘静脉刺激试验第二节 颊黏膜刺激试验第三节 家兔阴道黏膜刺激试验第四节 肌肉刺激试验第五节 眼刺激性试验附录:动物的自发性病变。
肾脏病理图谱(原创)
FROM:http://library.m /WebPath/REN AHTML/REN ALIDX.htm lMade by chenxh9905, copyright is reserved.Renal Pathology Index Normal and Incidental Findings1.Normal adult kidney, gross2.Normal adult kidney, cross section, gross3.Simple renal cyst, gross4.Double ureters, gross5.Horseshoe kidney, grossObstructive and Vascular diseases6.GIF animation of urinary tract lithiasis7.Hydronephrosis from obstruction by calculus, gross8.Staghorn calculus, gross9.Hydronephrosis, severe, gross10.Hydronephrosis with calculus at ureteropelvic junction, gross11.Ureteropelvic junction obstruction, gross12.Hydroureter and hydronephrosis, gross13.Atrophy of one kidney, gross14.Renal vein thrombosis, gross15.Acute renal infarction, gross16.Acute renal infarction, gross17.Acute renal infarction, microscopic18.Massive renal infarction, grossInfectious and Inflammatory Diseases19.Acute cystitis of bladder, gross20.Bladder hypertrophy and calculus with obstruction from nodular hyperplasia ofprostate, gross21.Ureteritis cystica, gross22.Renal abscess, gross23.Renal microabscesses, gross24.Renal microabscesses, gross25.Acute pyelonephritis, medium power microscopic26.Acute pyelonephritis, high power microscopic27.Renal papillary necrosis, gross28.Candida pyelonephritis, high power microscopic, PAS stain29.Chronic pyelonephritis, low power microscopic30.Chronic pyelonephritis, high power microscopic31.Xanthogranulomatous pyelonephritis, gross32.Xanthogranulomatous pyelonephritis, microscopicInterstitial Diseases33.Acute tubular necrosis, diagram34.Acute tubular necrosis with ischemia, microscopic35.Acute tubular necrosis with ethylene glycol poisoning, microscopic36.Drug-induced acute interstitial nephritis, microscopic37.Urate nephropathy, gross38.Uric acid crystals, polarized, microscopic39.Wegener granulomatosis with vasculitis, low power microscopic40.Wegener granulomatosis with vasculitis, high power microscopic41.Polyarteritis nodosa with vasculitis, microscopic42.Hyaline thrombus in glomerulus with thrombotic thrombocytopenic purpura (TTP),microscopic43.Hemolytic-uremic syndrome with fibrin thrombi in glomerulus, microscopic44.Benign nephrosclerosis, gross45.Malignant nephrosclerosis, gross46.Malignant nephrosclerosis with fibrinoid necrosis, microscopic47.Hyperplastic arteriolitis with hypertension, microscopic48.Nodular glomerulosclerosis, microscopic49.Nodular glomerulosclerosis and hyaline arteriolosclerosis, microscopic, PAS stain50.Diffuse glomerulosclerosis, microscopic, PAS stain51.End stage renal disease, gross52.End stage renal disease, microscopic53.Diabetic kidneys, renal transplant with chronic rejection, gross54.Acute transplant rejection, gross55.Acute tubulointerstitial cellular rejection, microscopic56.Chronic vascular rejection of kidney, microscopicCystic Diseases57.Normal term infant kidneys, external, gross58.Normal fetal kidneys, cut surface, gross59.Recessive polycystic kidney disease, gross60.Recessive polycystic kidney disease, cut surface, gross61.Recessive polycystic kidney disease, microscopic62.Congenital hepatic fibrosis in recessive polycystic kidney disease, microscopic63.Multicystic renal dysplasia, gross64.Multicystic renal dysplasia, grossparison of recessive polycystic renal disease and multicystic renal dysplasia,gross66.Multicystic renal dysplasia, microscopic67.Dominant polycystic kidney disease, gross68.Dominant polycystic kidney disease, gross69.Dominant polycystic kidney disease, gross70.Polycystic change with chronic renal dialysis, gross71.Renal cell carcinoma arising in dialysis-induced cystic change, gross72.Multiple simple renal cysts, grossNeoplasms73.Urothelial carcinoma of bladder, gross74.Urothelial carcinoma of bladder, gross75.Urothelial carcinoma of renal pelvis, gross76.Urothelial carcinoma of renal pelvis, gross77.Urothelial carcinoma, low power microscopic78.Urothelial carcinoma, high power microscopic79.Urothelial carcinoma in situ, high power microscopic80.Renal cell carcinoma, gross81.Renal cell carcinoma, gross82.Renal cell carcinoma, gross83.Renal cell carcinoma with renal vein invasion, gross84.Renal cell carcinoma, microscopic85.Metastases to kidney, gross86.Wilms tumor of kidney, gross87.Wilms tumor of kidney, low power microscopic88.Wilms tumor of kidney, high power microscopic89.Angiomyolipoma of kidney, gross90.Angiomyolipoma of kidney, microscopic91.Medullary fibroma (renomedullary interstitial cell tumor) of kidney, grossGlomerulonephritis92.Normal glomerulus, microscopic93.Normal glomerulus, microscopic, PAS stain94.Normal glomerulus, diagram95.Minimal change disease (MCD), electron micrograph96.Focal segmental glomerulosclerosis (FSGS), microscopic97.Focal segmental glomerulosclerosis (FSGS), microscopic, Trichrome stain98.Post-streptococcal glomerulonephritis, low power microscopic99.Post-streptococcal glomerulonephritis, high power microscopic100.Post-streptococcal glomerulonephritis, granular immune deposits, immunofluorescence microscopy101.Post-streptococcal glomerulonephritis, electron micrograph102.Membranous glomerulonephritis, microscopic103.Membranous glomerulonephritis, microscopic, Jones silver stain104.Membranous glomerulonephritis, immune deposits, immunofluorescence microscopy105.Membranous glomerulonephritis, electron micrograph106.Rapidly progressive glomerulonephritis with crescents, microscopic107.Rapidly progressive glomerulonephritis with crescents, microscopic108.Rapidly progressive glomerulonephritis with crescents, fluorescence microscopy109.Goodpasture syndrome with antiglomerular basement membrane antibody, immunofluorescence microscopy110.IgA nephropathy (Berger disease), microscopic111.IgA nephropathy (Berger disease), immunofluorescence microscopy112.Membranoproliferative glomerulonephritis, microscopic113.Membranoproliferative glomerulonephritis, microscopic, silver stain114.Membranoproliferative glomerulonephritis, type I, electron micrograph115.Membranoproliferative glomerulonephritis, type II, electron micrograph116.Membranoproliferative glomerulonephritis, type II, immunofluorescence microscopy117.Lupus nephritis, high power microscopic118.Hereditary nephritis (Alport syndrome), microscopic119.Chronic glomerulonephritis, gross1.Normal adult kidney, grossHere is a normal adult kidney. The capsule has been removed and a pattern of fetal lobulations still persists, as it sometimes does. The hilum at the mid left contains some adipose tissue. At the lower right is a smooth-surfaced, small, clear fluid-filled simple renal cyst. Such cysts occur either singly or scattered around the renal parenchyma and are not uncommon in adults.2.Normal adult kidney, cross section,grossIn cross section, this normal adult kidney demonstrates the lighter outer cortex and the darker medulla, with the renal pyramids into which the collecting ducts coalesce and drain into the calyces and central pelvis.3.Simple renal cyst, grossHere is a much larger simple renal cyst of the upper pole. Other smaller cysts are also scattered around the kidney. The ureter exits south on the left. Such a large renal cyst would be seen on a radiographic imaging procedure, but could probably be distinguished from a neoplasm by its uniform fluid density and thin wall. Such simple cysts are unlikely to compromise renal function.4.Double ureters, grossDouble ureters are seen exiting from each kidney and extending to the bladder that has been opened. A small segment of aorta is seen between the normal, smooth-surfaced kidneys. A partial or complete duplication of one or both ureters occurs in about 1 in 150 persons. There is a potential for obstructive problems due to the abnormal flow of urine and the entrance of two ureters into the bladder in close proximity, but most of the time this is an incidental finding (except to a urologist).5.Horseshoe kidney, grossHere is a "horseshoe" kidney. This is a congenital anomaly that most often occurs in association with other anomalies or syndromes with specific genetic defects such as trisomy 18. However, it can also occur as an isolated anomaly. The possible problem here is that the ureters take an abnormal course across the "bridge" of renal tissue and this can lead to partial obstruction with hydronephrosis.The passage of a calculus (stone) through the urinary tract is diagrammed here. Calculi form when there is increased excretion of solutes such as calcium and when urine alkalinity, acidity, stasis, and/or concentration are favorable. The most common varieties of calculi are:FrequencyType of StoneCalcium oxalate (or75%phosphate)Magnesium ammonium12%phosphate (struvite, or"triple phosphate")Uric acid6%Cystine1%Other6%6.GIF animation of urinary tract lithiasisStones containing calcium are far more frequent than other types, and about half the time occur when there is hypercalciuria. Only about 10% of the time do they appear as a consequence of hypercalcemia. The struvite stones are also known as "infection" stones because bacteria suchas Proteus that split urea to ammonia favor their formation. Uric acid stones may be seen inassociation with gout, but often are not, and may just reflect increased precipitation of urates in an acid urine. Rare cystine stones also form in acid urine.Urinary tract calculi are usually unilateral and about 1 to 3 mm in size. Their passage is marked by intense abdominal or back or flank pain. This pain can be paroxysmal, known as renal or ureteral "colic". Hematuria may also be present. Larger stones that cannot pass may produce hydronephrosis or hydroureter.7.Hydronephrosis from obstruction by calculus, grossThere was a large renal calculus (stone) that obstructed the calyces of the lower pole of this kidney, leading to a focal hydronephrosis (dilation of the collecting system). The stasis from the obstruction and dilation led to infection. The infection with inflammation is characterized by the pale yellowish-tan areas next to the dilated calyces with hyperemic mucosal surfaces. The upper pole is normal and shows good corticomedullary demarcations.8.Staghorn calculus, grossSometimes a very large calculus nearly fills the calyceal system, with extensions into calyces that give the appearance of a stag's (deer) horns. Hence, the name "staghorn calculus". Seen here is a horn-like stone extending into a dilated calyx, with nearly unrecognizable overlying renal cortex from severe hydronephrosis and pyelonephritis. Nephrectomy may be performed because the kidney is non-functional and serves only as a source for infection.9.Hydronephrosis, severe, grossHere is a kidney with much more advanced hydronephrosis in which there is only a thin rim of remaining renal cortex. Such a kidney is non-functional and a source for ongoing infection. If this process is unilateral, then the problem originates from the ureteral orifice up to the pelvis. In this case, a large "staghorn" calculus (so named because the prominent projections of the stone into the calyces resemble deer antlers) was present that filled up the pelvis and calyceal system. If this process were bilateral, then the problem would originate in the bladder trigone or urethra (or the prostate around the urethra) or some process (such as a large neoplasm) that could impinge on both ureters.10.Hydronephrosis with calculus at ureteropelvic junction, grossThe arrow points to the culprit in this case of hydronephrosis--a ureteral calculus caught at the ureteropelvic junction. This kidney demonstrates marked hydronephrosis with nearly complete loss of cortex. Such a kidney would be non-functional. If the other kidney had sufficient function, then renal failure will not ensue. There is sufficient renal reserve capacity that it is possible to survive with half of a normal kidney.There is scarring of this kidney from chronic obstruction and pyelonephritis. The renal pelvis is markedly dilated, but the ureter is not, indicating that the point of obstruction is the ureteropelvic junction.A long-standing obstruction (probably congenital) at the ureteral orifice through which the metal probe passes led to the marked hydroureter and hydronephrosis seen here. In the intravenous urogram below, note the dilation of the right ureter, compared to the normal left ureter. This patient had vesicoureteral reflux. Such obstructive processes increase the risk for urinary tract infection.There is one relatively normal-sized kidney with a granular surface and a few scattered, shallow cortical scars. The other kidney shows atrophy because of renal arterial occlusion. Such a situation can lead to hypertension (Goldblatt kidney).The white arrow marks a renal vein thrombus. There are a host of etiologies for renal vein thrombosis, including trauma, compression by neoplasms, renal vein invasion by renal cell carcinoma, and nephrotic syndrome with membranous glomerulonephritis.This is an acute renal infarction. Note the wedge shape of this zone of coagulative necrosis resulting from loss of blood supply with resultant tissue ischemia that produces the pale infarct. The small amount of blood supply from the capsule supplies the immediate subcortical zone. The remaining cortex is congested, as is the medulla.This acute renal infarction is pale, typical of coagulative necrosis. It is roughly wedge-shaped. Renal infarctions usually result from embolization of cardiac valvular vegetations or a portion of cardiac mural thrombus. Sometimes a renal arterial vasculitis can lead to infarction.This is the microscopic appearance of an acute renal infarct. At the far right is normal kidney, then to the left of that hyperemic kidney that is dying, then to the left of that pale pink infarcted kidney in which both tubules and glomeruli are dead.Acute renal arterial obstruction in this case led to massive renal infarction in which the entire cortex is pale yellow, with medullary hemorrhage.This bladder at autopsy has been opened to reveal areas of hyperemia of the mucosa. This is acute cystitis.The markedly enlarged prostate seen here has not only large lateral lobes, but a very large median lobe as well that obstructs the prostatic urethra and led to chronic urinary tract obstruction. As a result, the bladder became both enlarged and hypertrophied as it had to work against the obstruction with every episode of urination. That is why the surface of the bladder appears trabeculated. Note also that a yellowish-brown calculus formed in the bladder.The small bumps seen here over the ureteral mucosa are called ureteritis cystica and represent cystic areas of glandular metaplasia resulting from inflammation. They are more commonly seen in the bladder, where they are called cystitis cystica.In the lower pole of this kidney is a 1 cm pale yellow abscess. Infections can reach the kidney either by ascending up the urinary tract (from a bladder infection, for example) or by hematogenous spread with sepsis. This lone abscess was probably hematogenous in origin.The surfaces of both kidneys demonstrate multiple microabscesses from hematogenous spread of a bacterial infection. The microabscesses have yellow centers and prominent hyperemic borders.The cut surface of the kidney reveals many small yellowish microabscesses in both cortex and medulla. This type of pyelonephritis is most typical for hematogenous dissemination of infection to the kidney, rather than the more typical ascending urinary tract infection.This is an ascending bacterial infection leading to acute pyelonephritis. Numerous PMN's are seen filling renal tubules across the center and right of this picture.At high magnification, many neutrophils are seen in the tubules and interstitium in a case of acute pyelonephritis. The neutrophils can collect in the distal tubules and be passed in urine as WBC casts.The pale white areas involving some or all of many renal papillae are areas of papillary necrosis. This is an uncommon but severe complication of acute pyelonephritis, particularly in persons with diabetes mellitus. Papillary necrosis may also accompany analgesic nephropathy.[Image courtesy of Dr. John Nicholls, Hong Kong University]This PAS stain of a renal papilla with a portion of transitional lining epithelium at the lower right demonstrates many budding cells and pseudohyphae of Candida albicans. Fungal urinary tract infections are much less common than bacterial infections, but both are likely to be ascending infections, having originated in the lower urinary tract, typically bladder.The large collection of chronic inflammatory cells here is in a patient with a history of multiple recurrent urinary tract infections. This is chronic pyelonephritis.Both lymphocytes and plasma cells are seen in this case of chronic pyelonephritis. It is not uncommon to see lymphocytes accompany just about any chronic renal disease: glomerulonephritis, nephrosclerosis, pyelonephritis. However, the plasma cells are most characteristic for chronic pyelonephritis.Sometimes long-standing renal infection may be localized and form a mass-like lesion. This is a disease known as xanthogranulomatous pyelonephritis. It is uncommon, but may mimic a neoplasm.The microscopic appearance of xanthogranulomatous pyelonephritis shows many pale to foamy macrophages from breakdown of renal parenchyma with ongoing inflammation.These diagrams illustrate acute tubular necrosis. The distribution of the areas of necrosis is more segmental with ischemic injuries, while toxic injuries result in more diffuse proximal tubular injury.The epithelium of the tubules seen here is ragged from undergoing necrosis with acute tubular necrosis (ATN) from ischemia. In this case, heart failure with hypotension precipitated the ATN.The tubular vacuolization and tubular dilation here is a result of the toxic effect of ethylene glycol poisoning. This is representative of acute tubular necrosis (ATN), which has many causes. ATN resulting from toxins usually has diffuse tubular involvement, whereas ATN resulting from ischemia (as in profound hypotension from cardiac failure) has patchy tubular involvement.In this case of drug-induced interstitial nephritis, there are some scattered eosinophils, along with neutrophils and mononuclear cells in the inflamed interstitium. The classic example of this occurs occasionally with methicillin, but can occur with a variety of drugs such as thiazide diuretics and the H2 blocker cimetidine. The immune mechanism may be either type I or type IV hypersensitivity.This is chronic urate nephropathy with pale yellowish tan tophaceous deposits in the medulla. There is also an acute urate nephropathy that can occur with a "lysis" syndrome reulting from massive cellular necrosis of leukemia or lymphoma cells with chemotherapy. The metabolic breakdown of the cell nuclei yields large amounts of urate which, when excreted, plug renal tubules.Chronic urate nephropathy leads to deposition of uric acid crystals in the interstitium, forming tophi with surrounding foreign body inflammation, mononuclear cell infiltrates, and fibrosis. The long, needle-shaped crystals form the pale mass shown here at high magnification. Patients with hyperuricemia may also have nephrolithiasis with uric acid stones.This is a renal biopsy at low magnification in which there is a focal lesion centered around a blood vessel. Thus, a vasculitis is present. The one glomerulus at the lower center appears normal. An adequate renal biopsy should contain at least 6 glomeruli so that there is less chancethat focal lesions will be missed. Renal biopsies are often performed with ultrasound guidance.At high power, the vasculitis is seen to involve a renal artery branch. This is a necrotizing granulomatous vasculitis. In this case, the anti-neutrophil cytoplasmic autoantibody (ANCA) serology was positive and a diagnosis of Wegener granulomatosis was made. This patient also had pulmonary involvement with this disease.Here is a vasculitis of a renal arterial branch. Lymphocytes are scattered in and around the vessel. This happens to be the classic form of polyarteritis nodosa (PAN), a systemic vasculitisthat most often affects the kidneys. The ANCA serology is often negative.A small platelet-fibrin thrombus is seen in a glomerular capillary above the arrow. This occurred in a patient with thrombotic thrombocytopenic purpura (TTP). This rare coagulopathy mainly affects kidneys, heart, and brain with small arteriolar thrombi. Acute renal failure can occur. The classic pentad of fever, acute renal failure, neurologic changes, thrombocytopenia, and microangiopathic hemolytic anemia is often present. TTP results from a congenital or more often acquired defect in the ADAMTS-13 metalloproteinase enzyme that cleaves vonWillebrand factor (vWF) multimers, and the large multimers lead to abnormal platelet aggregation. TTP overlaps with hemolytic uremic syndrome (HUS) that may be precipitated by verotoxins from such organisms as E. coli (type O157:H7) that cause endothelial injury.Very similar to thrombotic thrombocytopenic purpura (TTP) is hemolytic-uremic syndrome (HUS). The two conditions may be difficult to tell apart. HUS can be a leading cause for acute renal failure in children. Ingestion of foods, such as poorly cooked ground beef, introduces a verotoxin-producing E. coli infection into the GI tract. Such strains are often identified by serotyping, typically type O157:H7. A bloody diarrhea is followed in a few days by renal failure caused by endothelial injury from the toxin, leading to the characteristic fibrin thrombi in glomerular and interstitial capillaries. Most patients recover in a few weeks with supportive dialysis.Here is an example of renal vascular disease known as benign nephrosclerosis. The smaller arteries in the kidney have become thickened and narrowed. Hyaline arteriolosclerosis with hypertension or diabetes mellitus is usually present. This leads to patchy ischemic atrophy with focal loss of parenchyma that gives the surface of the kidney the characteristic granular appearance as seen here.In malignant nephrosclerosis, the kidney demonstrates focal small hemorrhages. This is often due to an accelerated phase of essential hypertension in which blood pressures are very high (such as 300/150 mm Hg).Malignant hypertension leads to fibrinoid necrosis of small renal arteries as shown here. The damage to the arteries leads to formation of pink fibrin--hence the term "fibrinoid".Thickening of the arterial wall with malignant hypertension also is associated with a hyperplastic arteriolosclerosis (hyperplastic arteriolitis). This arteriole has an "onion skin" appearance.This is nodular glomerulosclerosis (the Kimmelstiel-Wilson lesion) of diabetes mellitus. Nodules of pink hyaline material form in regions of glomerular capillary loops in the glomerulus. This is due to a marked increase in mesangial matrix from damage as a result of non-enzymatic glycosylation of proteins.This is a PAS stain of nodular glomerulosclerosis(Kimmelstiel-Wilson disease) in a patient with long-standing diabetes mellitus. Note also the markedly thickened arteriole at the lower right which is typical for the hyaline arteriolosclerosis that is seen in diabetic kidneys as well.This PAS stain demonstrates diffuse glomerulosclerosis associated with long-standing diabetes mellitus. There is an increase in mesangial matrix, a slight increase in mesangial cellularity, and capillary basement membrane thickening. These changes gradually advance until the entire glomerulus is sclerotic.The end result of many renal diseases -- whether they are renal vascular diseases, glomerulonephritis, or chronic pyelonephritis--is end stage renal disease (ESRD). In ESRD, the kidneys are small bilaterally, as shown here. This condition is associated with chronic renal failure, and the patient's blood urea nitrogen (BUN) and serum creatinine continue to increase. Chronic renal failure can be treated by dialysis or by kidney transplantation, as shown here.The microscopic appearance of the "end stage kidney" is similar regardless of cause, which is why a biopsy in a patient with chronic renal failure yields little useful information. The cortex is fibrotic, the glomeruli are sclerotic, there are scattered chronic inflammatory cell infiltrates, and the arteries are thickened. Tubules are often dilated and filled with pink casts and give an appearance of "thyroidization."In this case, severe atherosclerosis in a patient with diabetes mellitus led to severe aortic atherosclerosis with renal arterial stenosis as well as nephrosclerosis and nodular glomerulosclerosis of the kidneys. The end stage renal disease was treated with renal transplantation. The transplant kidney is placed in the pelvis because this is technically easier and there is usually no point in trying to remove the native kidneys. In this case, the patient developed chronic rejection and that is why focal hemorrhages are seen in the kidney that is slightly swollen. A radiographic study would show decreased renal blood flow in the transplant kidney.This kidney was removed because of acute transplant rejection. Note the swollen and hemorrhagic appearance of this entire kidney.Seen here is acute tubulointerstitial cellular rejection of a renal transplant. This can occur days to months to years following transplantation. Both CD4 and CD8 lymphocytes participate in this rejection reaction. The immunosuppressive drugs such as cyclosporine given to counteract the rejection may lead to nephrotoxicity with similar changes as well.This is chronic vascular rejection of a renal transplant, which has a poor prognosis. Note the thickened arteries with intimal fibrosis and chronic inflammation. These changes gradually occur over months in affected patients.These are normal term infant kidneys. Note the presence of fetal lobulations and the smooth cortical surfaces with some attached adipose tissue.These fetal kidneys (from a gestation estimated at 25 weeks in the second trimester) demonstrate a normal cut surface. Note the pelvis and the calyces. Note the well-defined corticomedullary junctions.This infant died soon after premature birth at 23 weeks gestation from pulmonary hypoplasia as aresult of oligohydramnios. The oligohydramnios resulted from markedly diminished fetal urine output as a consequence of polycystic kidney disease. Note the bilaterally enlarged kidneys that nearly fill the abdomen below the liver. The histologic appearance in this case, coupled with the gross appearance., was consistent with autosomal recessive polycystic kidney disease (ARPKD).Here is a cut section of a kidney with autosomal recessive polycystic kidney disease (ARPKD). Note that the cysts are fairly small but uniformly distributed throughout the parenchyma so that the disease is usually symmetrical in appearance, with both kidneys markedly enlarged. The recurrence risk for this disease is, of course, 25% because of the autosomal recessive inheritance pattern. Affected babies usually do not survive long. This disorder is linked to an abnormal fibrocystin protein produced by the PKHD1 gene.。
内镜医师学病理知识(八)结肠腺癌病理诊断图谱
内镜医师学病理知识(八)结肠腺癌病理诊断图谱大肠癌是消化道最常见的癌。
它是男性和女性第三大常见癌,也是全世界癌症死亡的第三大原因。
结肠直肠癌分为三个主要的解剖区域:右结肠、左结肠和直肠。
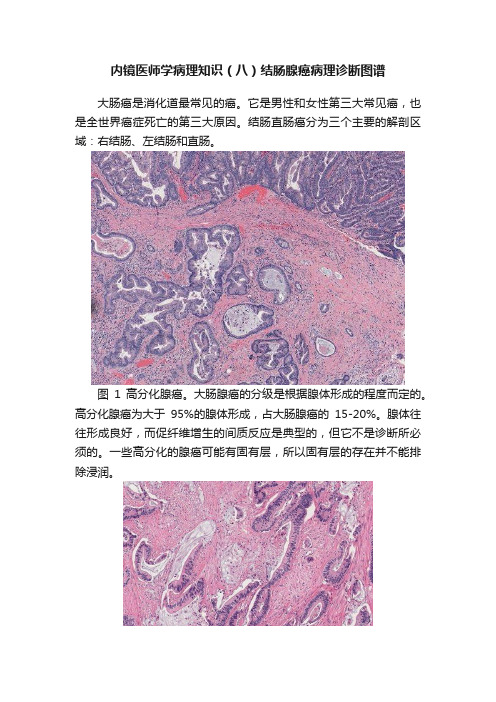
图1 高分化腺癌。
大肠腺癌的分级是根据腺体形成的程度而定的。
高分化腺癌为大于95%的腺体形成,占大肠腺癌的15-20%。
腺体往往形成良好,而促纤维增生的间质反应是典型的,但它不是诊断所必须的。
一些高分化的腺癌可能有固有层,所以固有层的存在并不能排除浸润。
图2 中分化腺癌。
中分化腺癌是最常见的结直肠腺癌,占所有病例的60%至70%。
肿瘤累及50-95%的腺体,腺体往往比高分化腺癌的腺体组织更紊乱,并常充满坏死的碎片(“脏性坏死”)。
图3 中分化腺癌伴脏性坏死。
结直肠癌常见腔内坏死(本例所示)。
中分化腺癌典型的腺体分化程度和细胞异型性。
图4 中分化结肠腺癌。
大多数浸润性结直肠腺癌都与促结缔组织增生性间质反应有关(本例所示)。
有些低异型度大肠腺癌也有例外,特别是与炎症性肠病相关的低异型度管状腺癌。
图5 中分化腺癌,本例腺体紧密地排列在一起,但是肿瘤仍然>50%的腺体形成,应该被认为是中分化腺癌。
图6 低分化腺癌。
低分化腺癌的腺体形成<50%。
大约15-20%的大肠腺癌分化较差。
肿瘤可以由肿瘤细胞、浸润巢或单个浸润细胞组成。
低分化腺癌预后较差。
本例肿瘤是以单个细胞的形式浸润的。
图7 低分化腺癌。
分化差的腺癌也可能以不规则岛的形式浸润。
在本例中,肿瘤岛被包埋在结缔组织增生间质中,仅形成局灶性腺体。
图8 低分化腺癌。
低分化腺癌也可以形成肿瘤生长的实性区域。
本例肿瘤显示明显的细胞异型性与拉长的肿瘤细胞。
本例细胞异型性的程度通常大于中分化腺癌,支持低分化腺癌。
图9 胶样(黏液)腺癌。
黏液腺癌约占大肠腺癌的10%。
肿瘤由黏液池和恶性上皮组成;超过50%的肿瘤必须有粘液样结构才能被认为是黏液腺癌。
大多数黏液腺癌是微卫星稳定的(MSS),但黏液腺癌比传统腺癌有更高的微卫星不稳定性(MSI-H)。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
25
肾小管上皮钙化无明显组织结构,细粒状 或块状钙盐沉着
26
宫颈腺上皮鳞形化生红:化生的鳞状上皮 正常宫颈粘膜上皮
细胞为单层柱状, 胞质空亮 分化成熟的鳞状上皮 代替了分化成熟的 柱状上皮
27
流行性脑脊髓膜炎
灰白色脓性渗出物沿 脑沟及血管分布
28
绿:平滑肌细胞 呈编制状 排列
6
子宫平滑肌肉瘤
黑:核分裂象 红:肉瘤细胞
7
心肌褐色萎缩
心脏颜色变深
8
脑萎缩
红箭头:变深的脑沟 蓝:变窄的脑回
9
肾压迫性萎缩
红:肾实质受压萎缩变薄 蓝:肾盂肾盏扩张
10
脾包膜玻璃样变性
被膜增厚,半透明 似糖衣,又称糖衣脾
11
肝脂肪变性 肝脏颜色变黄,黄油软大轻
非霍奇金淋巴瘤
绿:B细胞淋巴瘤 箭头所示就是瘤细胞
1
霍奇金淋巴瘤
红:R-S细胞 细胞体积大,核大,嗜酸性 粗大红染的核仁 背景细胞明显(各种炎细胞)
2
霍奇金淋巴瘤
镜影细胞
3
乳腺纤维腺瘤
红:增生的纤维组织 绿:增生的导管
4
乳腺纤维腺瘤
红:肌上皮 蓝:增生的纤维组织 绿:乳腺导管或腺泡上皮
5
子宫平滑肌瘤
血浆蛋白渗透 到血管内膜,血 均质红染,血管 变窄
21
肝细胞坏死
蓝:核碎裂 红:核溶解 绿:核固缩
22
脑液化性坏死 坏死灶内细胞、基质均溶解 呈疏松网状,结构消失
23
肉芽组织
绿:新生毛细血管 红:成纤维细胞 蓝:浸润的炎症细胞
24
Байду номын сангаас
皮肤一期愈合
红:新生胶原与表面平行 排列致密 蓝:正常上皮鳞状上皮 基底部的钉角消失
12
脑液化性坏死
坏死区组织酶解性液化 呈破棉絮状
13
肺干酪样坏死
坏死区淡黄,奶酪样
14
脚干性坏疽
干燥,皱缩成黑色,坏死区域 小,有明显分界
15
皮肤一期愈合 组织破坏少,创缘整齐,易 对合,无感染,形成瘢痕小
16
骨折愈合
红:骨折断端 绿:纤维性骨痂和骨性骨痂 的交替时期(纤维性骨痂是灰白色 半透明,骨性骨痂为不透明的 钙盐沉积)
17
心肌褐色萎缩
红:心肌纤维变细 细胞核两端可见 棕褐色的脂褐素 绿:萎缩心肌纤维之间很宽的 间隙
18
肝脂肪变性
肝细胞内脂肪空泡
19
肾贫血性梗死(凝固性坏死)
红:肾小管 上皮细胞 坏死但小管 轮廓尚存
蓝:肾小球 细胞坏死,核 溶解消失但 轮廓尚存
20
肾细动脉玻璃样变性
动脉管壁增厚 呈红染均质无 结构玻变