Dulera哮喘新药FDA说明书(英文)
盐酸度洛西汀FDA说明书(英文)
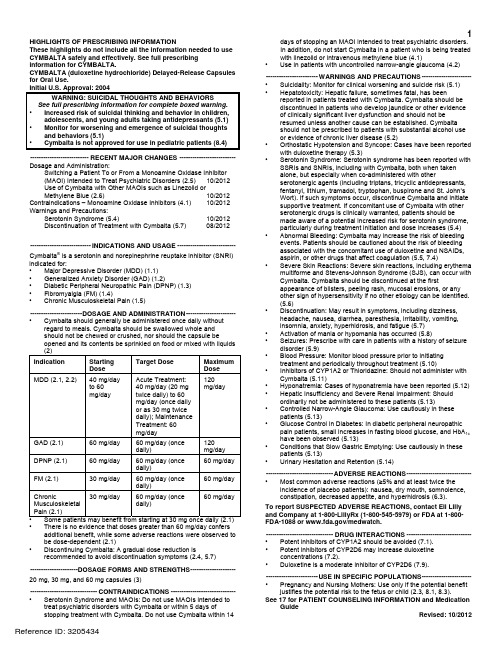
1HIGHLIGHTS OF PRESCRIBING INFORMATIONdays of stopping an MAOI intended to treat psychiatric disorders.These highlights do not include all the information needed to use In addition, do not start Cymbalta in a patient who is being treated CYMBALTA safely and effectively. See full prescribing with linezolid or intravenous methylene blue (4.1) information for CYMBALTA. •Use in patients with uncontrolled narrow-angle glaucoma (4.2)CYMBALTA (duloxetine hydrochloride) Delayed-Release Capsules for Oral Use.Initial U.S. Approval: 2004WARNING: SUICIDAL THOUGHTS AND BEHAVIORS See full prescribing information for complete boxed warning. • Increased risk of suicidal thinking and behavior in children,adolescents, and young adults taking antidepressants (5.1) • Monitor for worsening and emergence of suicidal thoughtsand behaviors (5.1) • Cymbalta is not approved for use in pediatric patients (8.4) ---------------------------RECENT MAJOR CHANGES --------------------------Dosage and Administration:Switching a Patient To or From a Monoamine Oxidase Inhibitor (MAOI) Intended to Treat Psychiatric Disorders (2.5) 10/2012 Use of Cymbalta with Other MAOIs such as Linezolid or Methylene Blue (2.6) 10/2012 Contraindications – Monoamine Oxidase Inhibitors (4.1) 10/2012 Warnings and Precautions: Serotonin Syndrome (5.4) 10/2012 Discontinuation of Treatment with Cymbalta (5.7) 08/2012 ----------------------------INDICATIONS AND USAGE ---------------------------Cymbalta ® is a serotonin and norepinephrine reuptake inhibitor (SNRI) indicated for: • Major Depressive Disorder (MDD) (1.1) • Generalized Anxiety Disorder (GAD) (1.2)• Diabetic Peripheral Neuropathic Pain (DPNP) (1.3)• Fibromyalgia (FM) (1.4)• Chronic Musculoskeletal Pain (1.5)------------------------DOSAGE AND ADMINISTRATION-----------------------• Cymbalta should generally be administered once daily withoutregard to meals. Cymbalta should be swallowed whole andshould not be chewed or crushed, nor should the capsule beopened and its contents be sprinkled on food or mixed with liquids (2) Indication Starting Dose Target DoseMaximumDose MDD (2.1, 2.2)40 mg/day to 60 mg/day Acute Treatment: 40 mg/day (20 mg twice daily) to 60 mg/day (once daily or as 30 mg twice daily); Maintenance Treatment: 60 mg/day 120 mg/day GAD (2.1) 60 mg/day 60 mg/day (once daily) 120mg/day DPNP (2.1) 60 mg/day 60 mg/day (once daily) 60 mg/day FM (2.1)30 mg/day 60 mg/day (once daily) 60 mg/day Chronic Musculoskeletal Pain (2.1)30 mg/day 60 mg/day (once daily) 60 mg/day • Some patients may benefit from starting at 30 mg once daily (2.1) • There is no evidence that doses greater than 60 mg/day confersadditional benefit, while some adverse reactions were observed to be dose-dependent (2.1) • D iscontinuing Cymbalta: A gradual dose reduction isrecommended to avoid discontinuation symptoms (2.4, 5.7) ----------------------DOSAGE FORMS AND STRENGTHS---------------------20 mg, 30 mg, and 60 mg capsules (3)-------------------------------CONTRAINDICATIONS ------------------------------• Serotonin Syndrome and MAOIs: Do not use MAOIs intended totreat psychiatric disorders with Cymbalta or within 5 days ofstopping treatment with Cymbalta. Do not use Cymbalta within 14------------------------WARNINGS AND PRECAUTIONS -----------------------• Suicidality: Monitor for clinical worsening and suicide risk (5.1) • Hepatotoxicity: Hepatic failure, sometimes fatal, has been reported in patients treated with Cymbalta. Cymbalta should be discontinued in patients who develop jaundice or other evidence of clinically significant liver dysfunction and should not be resumed unless another cause can be established. Cymbalta should not be prescribed to patients with substantial alcohol use or evidence of chronic liver disease (5.2)• Orthostatic Hypotension and Syncope: Cases have been reportedwith duloxetine therapy (5.3)• Serotonin Syndrome: Serotonin syndrome has been reported withSSRIs and SNRIs, including with Cymbalta, both when taken alone, but especially when co-administered with other serotonergic agents (including triptans, tricyclic antidepressants, fentanyl, lithium, tramadol, tryptophan, buspirone and St. John’s Wort). If such symptoms occur, discontinue Cymbalta and initiate supportive treatment. If concomitant use of Cymbalta with other serotonergic drugs is clinically warranted, patients should be made aware of a potential increased risk for serotonin syndrome, particularly during treatment initiation and dose increases (5.4) • Abnormal Bleeding: Cymbalta may increase the risk of bleedingevents. Patients should be cautioned about the risk of bleeding associated with the concomitant use of duloxetine and NSAIDs, aspirin, or other drugs that affect coagulation (5.5, 7.4)• Severe Skin Reactions: Severe skin reactions, including erythemamultiforme and Stevens-Johnson Syndrome (SJS), can occur with Cymbalta. Cymbalta should be discontinued at the firstappearance of blisters, peeling rash, mucosal erosions, or any other sign of hypersensitivity if no other etiology can be identified. (5.6)• Discontinuation: May result in symptoms, including dizziness,headache, nausea, diarrhea, paresthesia, irritability, vomiting, insomnia, anxiety, hyperhidrosis, and fatigue (5.7) • Activation of mania or hypomania has occurred (5.8)• Seizures: Prescribe with care in patients with a history of seizuredisorder (5.9)• Blood Pressure: Monitor blood pressure prior to initiatingtreatment and periodically throughout treatment (5.10)• Inhibitors of CYP1A2 or Thioridazine: Should not administer withCymbalta (5.11)• Hyponatremia: Cases of hyponatremia have been reported (5.12) • Hepatic Insufficiency and Severe Renal Impairment: Should ordinarily not be administered to these patients (5.13)• Controlled Narrow-Angle Glaucoma: Use cautiously in thesepatients (5.13)• Glucose Control in Diabetes: In diabetic peripheral neuropathicpain patients, small increases in fasting blood glucose, and HbA 1c have been observed (5.13)• Conditions that Slow Gastric Emptying: Use cautiously in these patients (5.13)• Urinary Hesitation and Retention (5.14)-------------------------------ADVERSE REACTIONS------------------------------• Most common adverse reactions (≥5% and at least twice theincidence of placebo patients): nausea, dry mouth, somnolence, constipation, decreased appetite, and hyperhidrosis (6.3). To report SUSPECTED ADVERSE REACTIONS, contact Eli Lilly and Company at 1-800-LillyRx (1-800-545-5979) or FDA at 1-800-FDA-1088 or /medwatch.-------------------------------DRUG INTERACTIONS ------------------------------• Potent inhibitors of CYP1A2 should be avoided (7.1). • Potent inhibitors of CYP2D6 may increase duloxetineconcentrations (7.2).• Duloxetine is a moderate inhibitor of CYP2D6 (7.9). ------------------------USE IN SPECIFIC POPULATIONS-----------------------• Pregnancy and Nursing Mothers: Use only if the potential benefitjustifies the potential risk to the fetus or child (2.3, 8.1, 8.3).See 17 for PATIENT COUNSELING INFORMATION and MedicationGuide Revised: 10/20122FULL PRESCRIBING INFORMATION: CONTENTS*WARNING: SUICIDAL THOUGHTS AND BEHAVIORS1 INDICATIONSANDUSAGE1.1 Major Depressive Disorder1.2 Generalized Anxiety Disorder1.3 Diabetic Peripheral Neuropathic Pain1.4 F ibromyalgia1.5 Chronic Musculoskeletal Pain2 DOSAGEANDADMINISTRATION2.1 I nitialTreatment2.2 M aintenance/Continuation/ExtendedTreatment2.3 Dosing in Special Populations2.4 D iscontinuingCymbalta2.5 Switching a Patient To or From a Monoamine OxidaseInhibitor (MAOI) Intended to Treat Psychiatric Disorders2.6 Use of Cymbalta with Other MAOIs such as Linezolid orMethylene Blue3 DOSAGE FORMS AND STRENGTHS4 CONTRAINDICATIONS4.1 Monoamine Oxidase Inhibitors (MAOIs)4.2 U ncontrolledNarrow-AngleGlaucoma5 WARNINGSANDPRECAUTIONS5.1 Suicidal Thoughts and Behaviors in Adolescents andYoung Adults5.2 H epatotoxicity5.3 Orthostatic Hypotension and Syncope5.4 S erotoninSyndrome5.5 A bnormalBleeding5.6 Severe Skin Reactions5.7 Discontinuation of Treatment with Cymbalta5.8 Activation of Mania/Hypomania5.9 S eizures5.10 Effect on Blood Pressure5.11 Clinically Important Drug Interactions5.12 H yponatremia5.13 Use in Patients with Concomitant Illness5.14 Urinary Hesitation and Retention5.15 L aboratoryTests6 ADVERSEREACTIONS6.1 Clinical Trial Data Sources6.2 Adverse Reactions Reported as Reasons forDiscontinuation of Treatment in Placebo-Controlled Trials6.3 Most Common Adverse Reactions6.4 Adverse Reactions Occurring at an Incidence of 5% orMore Among Duloxetine-Treated Patients in Placebo-Controlled Trials6.5 Adverse Reactions Occurring at an Incidence of 2% orMore Among Duloxetine-Treated Patients in Placebo-Controlled Trials6.6 Effects on Male and Female Sexual Function6.7 Vital Sign Changes6.8 W eightChanges6.9 L aboratoryChanges6.10 E lectrocardiogramChanges6.11 Other Adverse Reactions Observed During thePremarketing and Postmarketing Clinical Trial Evaluationof Duloxetine6.12 Postmarketing Spontaneous Reports7 DRUGINTERACTIONS7.1 Inhibitors of CYP1A27.2 Inhibitors of CYP2D67.3 Dual Inhibition of CYP1A2 and CYP2D67.4 Drugs that Interfere with Hemostasis (e.g., NSAIDs,Aspirin, and Warfarin)7.5 L orazepam7.6 T emazepam7.7 Drugs that Affect Gastric Acidity7.8 Drugs Metabolized by CYP1A27.9 Drugs Metabolized by CYP2D67.10 Drugs Metabolized by CYP2C97.11 Drugs Metabolized by CYP3A7.12 Drugs Metabolized by CYP2C197.13 Monoamine Oxidase Inhibitors (MAOIs)7.14 S erotonergicDrugs7.15 A lcohol7.16 C NSDrugs7.17 Drugs Highly Bound to Plasma Protein8 USE IN SPECIFIC POPULATIONS8.1 P regnancy8.2 Labor and Delivery8.3 N ursingMothers8.4 P ediatricUse8.5 G eriatricUse8.6 G ender8.7 S mokingStatus8.8 R ace8.9 H epaticInsufficiency8.10 Severe Renal Impairment9 DRUGABUSEANDDEPENDENCE9.2 A buse9.3 D ependence10 OVERDOSAGE10.1 Signs and Symptoms10.2 M anagementofOverdose11 DESCRIPTION12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.2 P harmacodynamics12.3 P harmacokinetics13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility14 CLINICAL STUDIES14.1 Major Depressive Disorder14.2 Generalized Anxiety Disorder14.3 Diabetic Peripheral Neuropathic Pain14.4 F ibromyalgia14.5 Chronic Musculoskeletal Pain16 HOW SUPPLIED/STORAGE AND HANDLING16.1 H owSupplied16.2 S torage17 PATIENT COUNSELING INFORMATION17.1 Information on Medication Guide17.2 Suicidal Thoughts and Behaviors17.3 M edicationAdministration17.4 Continuing the Therapy Prescribed17.5 H epatotoxicity17.6 A lcohol17.7 Orthostatic Hypotension and Syncope17.8 S erotoninSyndrome17.9 A bnormalBleeding17.10 Severe Skin Reaction17.11 Discontinuation of Treatment17.12 Activation of Mania or Hypomania17.13 Seizures17.14 Effects on Blood Pressure17.15 Concomitant Medications17.16 Hyponatremia17.17 Concomitant Illnesses17.18 Urinary Hesitancy and Retention17.19 Pregnancy and Breast Feeding17.20 Interference with Psychomotor Performance* Sections or subsections omitted from the full prescribing information are not listed.FULL PRESCRIBING INFORMATIONWARNING: SUICIDAL THOUGHTS AND BEHAVIORSAntidepressants increased the risk of suicidal thoughts and behavior in children, adolescents, and young adults in short-term studies. These studies did not show an increase in the risk of suicidal thoughts and behavior with antidepressant use in patients over age 24; there was a reduction in risk with antidepressant use in patients aged 65 and older [see Warnings and Precautions (5.1)].In patients of all ages who are started on antidepressant therapy, monitor closely for worsening, and for emergence of suicidal thoughts and behaviors. Advise families and caregivers of the need for close observation and communication with the prescriber [see Warnings and Precautions (5.1)].Cymbalta is not approved for use in pediatric patients [see Use in Specific Populations (8.4)].USAGEAND1 INDICATIONS1.1 Major Depressive DisorderCymbalta is indicated for the treatment of major depressive disorder (MDD). The efficacy of Cymbalta was established in four short-term and one maintenance trial in adults [see Clinical Studies (14.1)].A major depressive episode (DSM-IV) implies a prominent and relatively persistent (nearly every day for at least 2 weeks) depressed or dysphoric mood that usually interferes with daily functioning, and includes at least 5 of the following 9 symptoms: depressed mood, loss of interest in usual activities, significant change in weight and/or appetite, insomnia or hypersomnia, psychomotor agitation or retardation, increased fatigue, feelings of guilt or worthlessness, slowed thinking or impaired concentration, or a suicide attempt or suicidal ideation.AnxietyDisorder1.2 GeneralizedCymbalta is indicated for the treatment of generalized anxiety disorder (GAD). The efficacy of Cymbalta was established in three short-term trials and one maintenance trial in adults [see Clinical Studies (14.2)].Generalized anxiety disorder is defined by the DSM-IV as excessive anxiety and worry, present more days than not, for at least 6 months. The excessive anxiety and worry must be difficult to control and must cause significant distress or impairment in normal functioning. It must be associated with at least 3 of the following 6 symptoms: restlessness or feeling keyed up or on edge, being easily fatigued, difficulty concentrating or mind going blank, irritability, muscle tension, and/or sleep disturbance.1.3 Diabetic Peripheral Neuropathic PainCymbalta is indicated for the management of neuropathic pain (DPNP) associated with diabetic peripheral neuropathy [see Clinical Studies (14.3)].1.4 FibromyalgiaCymbalta is indicated for the management of fibromyalgia (FM) [see Clinical Studies (14.4)].PainMusculoskeletal1.5 ChronicCymbalta is indicated for the management of chronic musculoskeletal pain. This has been established in studies in patients with chronic low back pain (CLBP) and chronic pain due to osteoarthritis [see Clinical Studies (14.5)].2 DOSAGE AND ADMINISTRATIONCymbalta should be swallowed whole and should not be chewed or crushed, nor should the capsule be opened and its contents sprinkled on food or mixed with liquids. All of these might affect the enteric coating. Cymbalta can be given without regard to meals.Treatment2.1 InitialMajor Depressive Disorder — Cymbalta should be administered at a total dose of 40 mg/day (given as 20 mg twice daily) to 60 mg/day (given either once daily or as 30 mg twice daily). For some patients, it may be desirable to start at 30 mg once daily for 1 week, to allow patients to adjust to the medication before increasing to 60 mg once daily. While a 120 mg/day dose was shown to be effective, there is no evidence that doses greater than 60 mg/day confer any additional benefits. The safety of doses above 120 mg/day has not been adequately evaluated [see Clinical Studies (14.1)].Generalized Anxiety Disorder — For most patients, the recommended starting dose for Cymbalta is 60 mg administered once daily. For some patients, it may be desirable to start at 30 mg once daily for 1 week, to allow patients to adjust to the medication before increasing to 60 mg once daily. While a 120 mg once daily dose was shown to be effective, there is no evidence that doses greater than 60 mg/day confer additional benefit. Nevertheless, if a decision is made to increase the dose beyond 60 mg once daily, dose increases should be in increments of 30 mg once daily. The safety of doses above 120 mg once daily has not been adequately evaluated [see Clinical Studies (14.2)].Diabetic Peripheral Neuropathic Pain — The recommended dose for Cymbalta is 60 mg administered once daily. There is no evidence that doses higher than 60 mg confer additional significant benefit and the higher dose is clearly less well tolerated [see Clinical Studies (14.3)]. For patients for whom tolerability is a concern, a lower starting dose may be considered.Since diabetes is frequently complicated by renal disease, a lower starting dose and gradual increase in dose should be considered for patients with renal impairment [see Dosage and Administration (2.3), Use in Specific Populations (8.10), and Clinical Pharmacology (12.3)].Fibromyalgia — The recommended dose for Cymbalta is 60 mg administered once daily. Treatment should begin at 30 mg once daily for 1 week, to allow patients to adjust to the medication before increasing to 60 mg once daily. Some patients may respond to the starting dose. There is no evidence that doses greater than 60 mg/day confer additional benefit, even in patients who do not respond to a 60 mg dose, and higher doses are associated with a higher rate of adverse reactions [see Clinical Studies (14.4)].Chronic Musculoskeletal Pain — The recommended dose for Cymbalta is 60 mg once daily. Dosing may be started at 30 mg for one week, to allow patients to adjust to the medication before increasing to 60 mg once daily. There is no evidence that higher doses confer additional benefit, even in patients who do not respond to a 60 mg dose, and higher doses are associated with a higher rate of adverse reactions [see Clinical Studies (14.5)].Treatment2.2 M aintenance/Continuation/ExtendedMajor Depressive Disorder — It is generally agreed that acute episodes of major depression require several months or longer of sustained pharmacologic therapy. Maintenance of efficacy in MDD was demonstrated with Cymbalta as monotherapy. Cymbalta should be administered at a total dose of 60 mg once daily. Patients should be periodically reassessed to determine the need for maintenance treatment and the appropriate dose for such treatment [see Clinical Studies (14.1)].Generalized Anxiety Disorder — It is generally agreed that episodes of generalized anxiety disorder require several months or longer of sustained pharmacological therapy. Maintenance of efficacy in GAD was demonstrated with Cymbalta as monotherapy. Cymbalta should be administered in a dose range of 60-120 mg once daily. Patients should be periodically reassessed to determine the continued need for maintenance treatment and the appropriate dose for such treatment [see Clinical Studies (14.2)].Diabetic Peripheral Neuropathic Pain — As the progression of diabetic peripheral neuropathy is highly variable and management of pain is empirical, the effectiveness of Cymbalta must be assessed individually. Efficacy beyond 12 weeks has not been systematically studied in placebo-controlled trials.Fibromyalgia — Fibromyalgia is recognized as a chronic condition. The efficacy of Cymbalta in the management of fibromyalgia has been demonstrated in placebo-controlled studies up to 3 months. The efficacy of Cymbalta was not demonstrated in longer studies; however, continued treatment should be based on individual patient response.Chronic Musculoskeletal Pain — The efficacy of Cymbalta has not been established in placebo-controlled studies beyond 13 weeks.2.3 Dosing in Special PopulationsHepatic Insufficiency — It is recommended that Cymbalta should ordinarily not be administered to patients with any hepatic insufficiency [see Warnings and Precautions (5.13) and Use in Specific Populations (8.9)].Severe Renal Impairment — Cymbalta is not recommended for patients with end-stage renal disease or severe renal impairment (estimated creatinine clearance <30 mL/min) [see Warnings and Precautions (5.13) and Use in Specific Populations (8.10)].Elderly Patients — No dose adjustment is recommended for elderly patients on the basis of age. As with any drug, caution should be exercised in treating the elderly. When individualizing the dosage in elderly patients, extra care should be taken when increasing the dose [see Use in Specific Populations (8.5)].Pregnant Women — There are no adequate and well-controlled studies in pregnant women; therefore, Cymbalta should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus [see Use in Specific Populations (8.1)].Lilly maintains a pregnancy registry to monitor the pregnancy outcomes of women exposed to Cymbalta while pregnant. Healthcare providers are encouraged to register any patient who is exposed to Cymbalta during pregnancy by calling the Cymbalta Pregnancy Registry at 1-866-814-6975 or by visiting Nursing Mothers — Because the safety of duloxetine in infants is not known, nursing while on Cymbalta is not recommended [see Use in Specific Populations (8.3)].2.4 D iscontinuingCymbaltaSymptoms associated with discontinuation of Cymbalta and other SSRIs and SNRIs have been reported. A gradual reduction in the dose rather than abrupt cessation is recommended whenever possible [see Warnings and Precautions (5.7)].2.5 Switching a Patient To or From a Monoamine Oxidase Inhibitor (MAOI) Intended to Treat PsychiatricDisordersAt least 14 days should elapse between discontinuation of an MAOI intended to treat psychiatric disorders and initiation of therapy with Cymbalta. Conversely, at least 5 days should be allowed after stopping Cymbalta before starting an MAOI intended to treat psychiatric disorders [see Contraindications (4.1)].2.6 Use of Cymbalta with Other MAOIs such as Linezolid or Methylene BlueDo not start Cymbalta in a patient who is being treated with linezolid or intravenous methylene blue because there is an increased risk of serotonin syndrome. In a patient who requires more urgent treatment of a psychiatric condition, other interventions, including hospitalization, should be considered [see Contraindications (4.1)].In some cases, a patient already receiving Cymbalta therapy may require urgent treatment with linezolid or intravenous methylene blue. If acceptable alternatives to linezolid or intravenous methylene blue treatment are not available and the potential benefits of linezolid or intravenous methylene blue treatment are judged to outweigh the risks of serotonin syndrome in a particular patient, Cymbalta should be stopped promptly, and linezolid or intravenous methylene blue can be administered. The patient should be monitored for symptoms of serotonin syndrome for 5 days or until 24 hours after the last dose of linezolid or intravenous methylene blue, whichever comes first. Therapy with Cymbalta may be resumed 24 hours after the last dose of linezolid or intravenous methylene blue [see Warnings and Precautions (5.4)].The risk of administering methylene blue by non-intravenous routes (such as oral tablets or by local injection) or in intravenous doses much lower than 1 mg/kg with Cymbalta is unclear. The clinician should, nevertheless, be aware of the possibility of emergent symptoms of serotonin syndrome with such use [see Warnings and Precautions (5.4)].3 DOSAGE FORMS AND STRENGTHSCymbalta is available as delayed release capsules:20 mg opaque green capsules imprinted with “Lilly 3235 20mg”30 mg opaque white and blue capsules imprinted with “Lilly 3240 30mg”60 mg opaque green and blue capsules imprinted with “Lilly 3237 60mg”60 mg opaque green and blue capsules imprinted with “Lilly 3270 60mg”4 CONTRAINDICATIONS4.1 Monoamine Oxidase Inhibitors (MAOIs)The use of MAOIs intended to treat psychiatric disorders with Cymbalta or within 5 days of stopping treatment with Cymbalta is contraindicated because of an increased risk of serotonin syndrome. The use of Cymbalta within 14 days of stopping an MAOI intended to treat psychiatric disorders is also contraindicated [see Dosage and Administration (2.5) and Warnings and Precautions (5.4)].Starting Cymbalta in a patient who is being treated with MAOIs such as linezolid or intravenous methylene blue is also contraindicated because of an increased risk of serotonin syndrome [see Dosage and Administration (2.6) and Warnings and Precautions (5.4)].4.2 Uncontrolled Narrow-Angle GlaucomaIn clinical trials, Cymbalta use was associated with an increased risk of mydriasis; therefore, its use should be avoided in patients with uncontrolled narrow-angle glaucoma [see Warnings and Precautions (5.13)].PRECAUTIONS5 WARNINGSAND5.1 Suicidal Thoughts and Behaviors in Adolescents and Young AdultsPatients with major depressive disorder (MDD), both adult and pediatric, may experience worsening of their depression and/or the emergence of suicidal ideation and behavior (suicidality) or unusual changes in behavior, whether or not they are taking antidepressant medications, and this risk may persist until significant remission occurs. Suicide is a known risk of depression and certain other psychiatric disorders, and these disorders themselves are the strongest predictors of suicide. There has been a long-standing concern, however, that antidepressants may have a role in inducing worsening of depression and the emergence of suicidality in certain patients during the early phases of treatment.Pooled analyses of short-term placebo-controlled trials of antidepressant drugs (SSRIs and others) showed that these drugs increase the risk of suicidal thinking and behavior (suicidality) in children, adolescents, and young adults (ages 18-24) with major depressive disorder (MDD) and other psychiatric disorders. Short-term studies did not show an increase in the risk of suicidality with antidepressants compared to placebo in adults beyond age 24; there was a reduction with antidepressants compared to placebo in adults aged 65 and older.The pooled analyses of placebo-controlled trials in children and adolescents with MDD, obsessive compulsive disorder (OCD), or other psychiatric disorders included a total of 24 short-term trials of 9 antidepressant drugs in over 4400 patients. The pooled analyses of placebo-controlled trials in adults with MDD or other psychiatric disorders included a total of 295 short-term trials (median duration of 2 months) of 11 antidepressant drugs in over 77,000 patients. There was considerable variation in risk of suicidality among drugs, but a tendency toward an increase in the younger patients for almost all drugs studied. There were differences in absolute risk of suicidality across the different indications, with the highest incidence in MDD. The risk of differences (drug vs placebo), however, were relatively stable within age strata and across indications. These risk differences (drug-placebo difference in the number of cases of suicidality per 1000 patients treated) are provided in Table 1.Table 1Age Range Drug-Placebo Difference in Number of Cases ofSuicidality per 1000 Patients TreatedIncreases Compared to Placebo<18 14 additional cases18-24 5 additional cases Decreases Compared to Placebo25-64 1 fewer case≥65 6 fewer casesNo suicides occurred in any of the pediatric trials. There were suicides in the adult trials, but the number was notsufficient to reach any conclusion about drug effect on suicide.It is unknown whether the suicidality risk extends to longer-term use, i.e., beyond several months. However, thereis substantial evidence from placebo-controlled maintenance trials in adults with depression that the use ofantidepressants can delay the recurrence of depression.All patients being treated with antidepressants for any indication should be monitored appropriately andobserved closely for clinical worsening, suicidality, and unusual changes in behavior, especially during the initialfew months of a course of drug therapy, or at times of dose changes, either increases or decreases.The following symptoms, anxiety, agitation, panic attacks, insomnia, irritability, hostility, aggressiveness,impulsivity, akathisia (psychomotor restlessness), hypomania, and mania, have been reported in adult and pediatricpatients being treated with antidepressants for major depressive disorder as well as for other indications, both psychiatricand nonpsychiatric. Although a causal link between the emergence of such symptoms and either the worsening ofdepression and/or the emergence of suicidal impulses has not been established, there is concern that such symptomsmay represent precursors to emerging suicidality.Consideration should be given to changing the therapeutic regimen, including possibly discontinuing themedication, in patients whose depression is persistently worse, or who are experiencing emergent suicidality or symptomsthat might be precursors to worsening depression or suicidality, especially if these symptoms are severe, abrupt in onset,or were not part of the patient’s presenting symptoms.If the decision has been made to discontinue treatment, medication should be tapered, as rapidly as is feasible,but with recognition that discontinuation can be associated with certain symptoms [see Dosage and Administration (2.4)and Warnings and Precautions (5.7) for descriptions of the risks of discontinuation of Cymbalta].Families and caregivers of patients being treated with antidepressants for major depressive disorder orother indications, both psychiatric and nonpsychiatric, should be alerted about the need to monitor patients for the emergence of agitation, irritability, unusual changes in behavior, and the other symptoms described above, as well as the emergence of suicidality, and to report such symptoms immediately to health care providers. Such monitoring should include daily observation by families and caregivers. Prescriptions for Cymbalta should bewritten for the smallest quantity of capsules consistent with good patient management, in order to reduce therisk of overdose.Screening Patients for Bipolar Disorder — A major depressive episode may be the initial presentation of bipolardisorder. It is generally believed (though not established in controlled trials) that treating such an episode with anantidepressant alone may increase the likelihood of precipitation of a mixed/manic episode in patients at risk for bipolardisorder. Whether any of the symptoms described above represent such a conversion is unknown. However, prior toinitiating treatment with an antidepressant, patients with depressive symptoms should be adequately screened todetermine if they are at risk for bipolar disorder; such screening should include a detailed psychiatric history, including afamily history of suicide, bipolar disorder, and depression. It should be noted that Cymbalta (duloxetine) is not approvedfor use in treating bipolar depression.5.2 HepatotoxicityThere have been reports of hepatic failure, sometimes fatal, in patients treated with Cymbalta. These cases havepresented as hepatitis with abdominal pain, hepatomegaly, and elevation of transaminase levels to more than twenty times the upper limit of normal with or without jaundice, reflecting a mixed or hepatocellular pattern of liver injury. Cymbalta should be discontinued in patients who develop jaundice or other evidence of clinically significant liver dysfunction and should not be resumed unless another cause can be established.Cases of cholestatic jaundice with minimal elevation of transaminase levels have also been reported. Otherpostmarketing reports indicate that elevated transaminases, bilirubin, and alkaline phosphatase have occurred in patientswith chronic liver disease or cirrhosis.Cymbalta increased the risk of elevation of serum transaminase levels in development program clinical trials. Livertransaminase elevations resulted in the discontinuation of 0.3% (89/29,435) of Cymbalta-treated patients. In mostpatients, the median time to detection of the transaminase elevation was about two months. In placebo-controlled trials in any indication, for patients with normal and abnormal baseline ALT values, elevation of ALT >3 times the upper limit of normal occurred in 1.37% (132/9611) of Cymbalta-treated patients compared to 0.49% (35/7182) of placebo-treated patients. In placebo-controlled studies using a fixed dose design, there was evidence of a dose response relationship for ALT and AST elevation of >3 times the upper limit of normal and >5 times the upper limit of normal, respectively.。
美国FDA批准哮喘药Advair Diskus首个仿制药上市
美国FDA批准哮喘药Advair Diskus首个仿制药上市夏训明(编译)【摘要】葛兰素史克(Glaxo SmithKline)公司的哮喘/慢性阻塞性肺病治疗药物Advair Diskus的专利到期,该药是复方药,有效成分为丙酸氟替卡松(fluticasone propionate,CAS登记号为80474-14-2)和沙美特罗(salmeterol,CAS登记号为89365-50-4),剂型为吸入性粉剂。
美国FDA于2019年1月30日批准该药的首个非专利仿制药(通用名药物)上市,适用症为用于4岁及以上患者治疗哮喘病,也可用于慢性阻塞性肺病(chronic obstructive pulmonary disease,COPD)患者治疗气流受限及减轻病情加重。
【期刊名称】《广东药科大学学报》【年(卷),期】2019(035)001【总页数】1页(P96-96)【关键词】美国FDA;哮喘药;仿制药;FDA批准;上市;salmeterol;慢性阻塞性肺病;pulmonary【作者】夏训明(编译)【作者单位】【正文语种】中文【中图分类】R95葛兰素史克(Glaxo SmithKline)公司的哮喘/慢性阻塞性肺病治疗药物AdvairDiskus的专利到期,该药是复方药,有效成分为丙酸氟替卡松(fluticasone propionate,CAS登记号为80474-14-2)和沙美特罗(salmeterol,CAS登记号为89365-50-4),剂型为吸入性粉剂。
美国FDA于2019年1月30日批准该药的首个非专利仿制药(通用名药物)上市,适用症为用于4岁及以上患者治疗哮喘病,也可用于慢性阻塞性肺病(chronic obstructive pulmonary disease,COPD)患者治疗气流受限及减轻病情加重。
此次,仿制药巨头Mylan公司获准生产和销售3种不同剂量的Advair Diskus仿制药。
哮喘治疗药物及使用说明

哮喘治疗药物及使用说明哮喘是一种慢性炎症性疾病,通常由特定的刺激物引起,导致气道收缩和炎症反应。
对于患有哮喘的病人来说,正确的药物治疗是非常重要的,可以帮助他们控制病情和减少哮喘发作的频率。
本文将介绍一些常用的哮喘治疗药物以及使用说明。
1. 类固醇吸入剂(ICS)类固醇吸入剂是一种主要用于控制哮喘症状的药物。
它通过减少气道炎症和肿胀来减轻哮喘的症状。
ICS的使用方法通常是通过口腔吸入剂或吸入器来进行。
患者需要按照医生的指示使用,并遵循正确的使用方法。
ICS通常需要长期使用,持续控制哮喘的症状。
2. 快速救济药物快速救济药物,例如沙丁胺醇,也称为短效β2受体激动剂(SABA),主要用于缓解哮喘发作时的紧迫感和气喘。
这些药物通过扩张气道上的平滑肌来缓解哮喘症状。
患者应该在发作时使用快速救济药物,并按照医生的建议使用正确的剂量。
3. 长效β2受体激动剂(LABA)长效β2受体激动剂通常与类固醇吸入剂联合使用,用作哮喘的控制药物。
LABA通过扩张气道上的平滑肌,帮助患者更好地控制病情。
与快速救济药物不同,LABA的作用持续时间较长,可以提供更持久的症状缓解。
LABA通常需要长期服用,但是不能用于单独治疗哮喘。
4. 白三烯受体拮抗剂(LTRA)白三烯受体拮抗剂是一种用于控制哮喘的药物,主要用于防治冷气过敏和运动诱发的哮喘。
这些药物通过阻断白三烯受体来减少炎症反应和气道收缩。
患者应该按照医生的建议正确使用LTRA,并且了解副作用以及潜在的药物相互作用。
5. 抗胆碱能药物抗胆碱能药物作为一种用于缓解气道痉挛和减少分泌物的常用药物,对于某些哮喘患者来说也是一种有效的治疗选择。
然而,对于患有狭窄性青光眼等相关疾病的患者来说,使用抗胆碱能药物需要特别谨慎,并在医生的指导下进行。
总结起来,在哮喘的治疗过程中,患者可以根据病情严重程度和医生的建议来使用不同的药物。
对于轻度哮喘,ICS可能是唯一需要的治疗药物。
对于中重度哮喘,类固醇吸入剂通常需要与快速救济药物或LABA联合使用。
FDA英文药品说明书规定项目中英对照
FDA英文药品说明书规定项目中英对照--------------------------------------------------------------------------------药品说明书旧称description,instruction,direction.今称insert,package insert美国FDA规定其应包括十项。
一.drug names(药物名称)1.通常每种药物有三个名字(1)proprietary name(商品名称)(2)popular name(俗名)(3)chemical name(化学名)2.说明书标题多用商品名其右上角标有R者,表示registered trademark(注册商标)二.description(性状)(常用description,introduction,composition)包括药品的chemical structure(化学结构)、chemical composition(化学成分)、physical and chemical properties(物理和化学性质)三.clinical pharmacology(临床药理学)常用的还有:clinical data(临床数据)、clinical experience(临床经验)、clinical use(临床应用)、clinical observation(临床观察)、clinical effect(临床疗效)、clinical discussion(临床讨论)、mode of mechanism of action(临床机理及途径)、pharmacological actions(药理作用)、therapeutical actions(治疗作用)、bacteriology(细菌学)、microbiology(微生物学)、physiology(生理学)、toxicology(毒理学)四.indications and usage(适应证和用法)常用标题:indications,major indications,clinical indications,principal indications,condications,uses,treatment五.contraindications(禁忌证)1.常用标题contraindications,restriction on use(限制使用)2.常用词(组)pregnant women孕妇women of childbeating age育龄妇女be hypersensitive to 对......过敏者allergic reaction变态反应lactation,early infancy乳期heart,cardiac,myocardial心脏,心脏的,心肌的kidney,renal肾,肾脏的liver,hepatic肝,肝脏的insufficiency,impairment机能不全damage,danger,failure损伤,危险,衰?BR>六.precautions(注意事项)常用标题:causions,remark,note,notice,attention,awakening, N.B.七.warnings(警告)常用标题:additional warnings(告戒事项)八.adverse reactions(不良反应)常用标题:side reaction(副反应)、untoward reaction(不良反应)、toxicity reaction(毒性反应)、anaphylactic reaction(过敏反应)、side effects,by-effects,after effects,undesirable effects(副作用)、double infection(双重感染)九.overdosage(用药过量)常用标题:treatment of overdosage(用药过量的治疗)十.dosage and administration(剂量用法)1.常用标题:administration procedure,method for administration,method of use,direction for use,how to use,recommendation,reconstitution(用法)posology,dosage(剂量)application and dosage,usage and dosage(用法与剂量)clinical application(临床应用)2.mode of administration(给药方式)intramuscularly肌肉注射intragluteally臀肌注射intraarterially动脉注射intravenously静脉注射intrathecally鞘内注射intracerebeospinally脑脊髓腔注射orally口服parentarally肠道外给药locally局部给药subconjunctivally结膜下给药sublingually舌下给药submucously黏膜下给药现各大药厂的说明书,项目远远超过十项,如:1.animal pharmacology and animal toxicology(动物药理学和动物毒理学)2.absorption and excretion(吸收和排泄)3.tolerance(耐受性)4.drug interactions(药物相互作用)5.storage and duration of efficacy(贮藏与失效期)6.packages(包装)7.advantages(优点)8.references(参考文献)9.further information(补充说明)10.manufacturer(生产者)。
SUBLOCADE 说明书
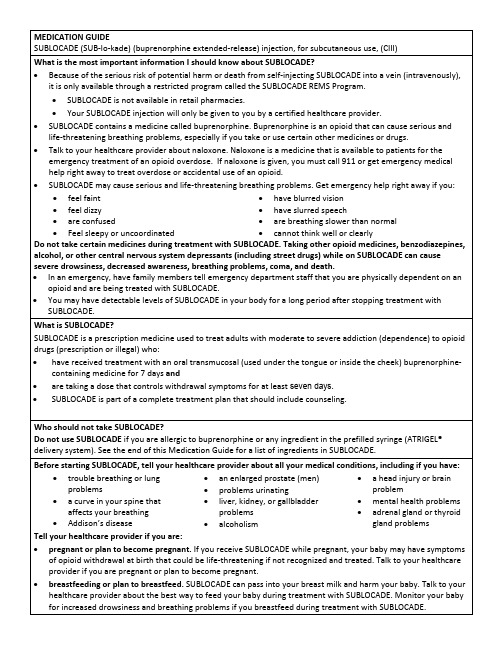
MEDICATION GUIDESUBLOCADE(SUB-lo-kade) (buprenorphine extended-release) injection, for subcutaneous use, (CIII)What is the most important information I should know about SUBLOCADE?•Because of the serious risk of potential harm or death from self-injecting SUBLOCADE into a vein (intravenously), it is only available through a restricted program called the SUBLOCADE REMS Program.•SUBLOCADE is not available in retail pharmacies.•Your SUBLOCADE injection will only be given to you by a certified healthcare provider.•SUBLOCADE contains a medicine called buprenorphine. Buprenorphine is an opioid that can cause serious and life-threatening breathing problems, especially if you take or use certain other medicines or drugs.•Talk to your healthcare provider about naloxone. Naloxone is a medicine that is available to patients for the emergency treatment of an opioid overdose. If naloxone is given, you must call 911 or get emergency medical help right away to treat overdose or accidental use of an opioid.•SUBLOCADE may cause serious and life-threatening breathing problems. Get emergency help right away if you:•feel faint•feel dizzy•are confused•Feel sleepy or uncoordinated •have blurred vision•have slurred speech•are breathing slower than normal •cannot think well or clearlyDo not take certain medicines during treatment with SUBLOCADE. Taking other opioid medicines, benzodiazepines, alcohol, or other central nervous system depressants (including street drugs) while on SUBLOCADE can cause severe drowsiness, decreased awareness, breathing problems, coma, and death.•In an emergency, have family members tell emergency department staff that you are physically dependent on an opioid and are being treated with SUBLOCADE.•You may have detectable levels of SUBLOCADE in your body for a long period after stopping treatment with SUBLOCADE.What is SUBLOCADE?SUBLOCADE is a prescription medicine used to treat adults with moderate to severe addiction (dependence) to opioid drugs (prescription or illegal) who:•have received treatment with an oral transmucosal (used under the tongue or inside the cheek) buprenorphine-containing medicine for 7 days and•are taking a dose that controls withdrawal symptoms for at least seven days.•SUBLOCADE is part of a complete treatment plan that should include counseling.Who should not take SUBLOCADE?Do not use SUBLOCADE if you are allergic to buprenorphine or any ingredient in the prefilled syringe (ATRIGEL® delivery system). See the end of this Medication Guide for a list of ingredients in SUBLOCADE.Before starting SUBLOCADE, tell your healthcare provider about all your medical conditions, including if you have:•trouble breathing or lung problems• a curve in your spine that affects your breathing •Addison’s disease •an enlarged prostate (men)•problems urinating•liver, kidney, or gallbladderproblems•alcoholism• a head injury or brainproblem•mental health problems•adrenal gland or thyroidgland problemsTell your healthcare provider if you are:•pregnant or plan to become pregnant. If you receive SUBLOCADE while pregnant, your baby may have symptoms of opioid withdrawal at birth that could be life-threatening if not recognized and treated. Talk to your healthcare provider if you are pregnant or plan to become pregnant.•breastfeeding or plan to breastfeed. SUBLOCADE can pass into your breast milk and harm your baby. Talk to your healthcare provider about the best way to feed your baby during treatment with SUBLOCADE. Monitor your baby for increased drowsiness and breathing problems if you breastfeed during treatment with SUBLOCADE.Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins and herbal supplements.How will I receive SUBLOCADE?•You will receive SUBLOCADE by your healthcare provider as an injection just under the skin (subcutaneous) of your stomach (abdomen). You will receive SUBLOCADE monthly (with at least 26 days between doses). •SUBLOCADE is injected as a liquid. After the injection, SUBLOCADE changes to a solid form called a depot. The depot may be seen or felt as a small bump under your skin at the injection site on your abdomen for several weeks. The depot will get smaller over time.•Do not try to remove the depot.•Do not rub or massage the injection site.•Try not to let belts or clothing waistbands rub against the injection site.•If you miss a dose of SUBLOCADE, see your healthcare provider to get your SUBLOCADE injection as soon as possible.What should I avoid while being treated with SUBLOCADE?•Do not drive, operate heavy machinery, or perform any other dangerous activities until you know how SUBLOCADE affects you. Buprenorphine can cause drowsiness and slow reaction times. SUBLOCADE can make you sleepy, dizzy, or lightheaded. This may happen more often in the first few days after your injection and when your dose is changed.•You should not drink alcohol or take prescription or over-the-counter medicines that contain alcohol during treatment with SUBLOCADE, because this can lead to loss of consciousness or even death.What are the possible side effects of SUBLOCADE?SUBLOCADE can cause serious side effects, including:•Trouble breathing. Taking other opioid medicines, benzodiazepines, alcohol, or other central nervous system depressants during treatment with SUBLOCADE can cause breathing problems that can lead to coma and death. •Sleepiness, dizziness, and problems with coordination.•Physical dependence.•Liver problems. Call your healthcare provider right away if you notice any of these symptoms:•your skin or the white part of your eyes turns yellow (jaundice)•dark or “tea-colored” urine•light colored stools (bowel movements) •loss of appetite•pain, aching, or tenderness on the right side of your stomach area•nausea•Your healthcare provider should do blood tests to check your liver before you start and during treatment with SUBLOCADE.•Allergic reaction. You may have a rash, hives, swelling of your face, wheezing, low blood pressure, or loss of consciousness. Call your healthcare provider or get emergency help right away.•Opioid withdrawal. Call your healthcare provider right away if you get any of these symptoms:•shaking•sweating more than normal •feeling hot or cold more than normal •runny nose•watery eyes •goose bumps •diarrhea •vomiting •muscle aches•Decrease in blood pressure. You may feel dizzy when you get up from sitting or lying down. •The most common side effects of SUBLOCADE include:•constipation •headache •vomiting•increase in liver enzymes•nausea •injection site itching •tiredness •injection site pain•SUBLOCADE may affect fertility in males and females. Talk to your healthcare provider if this is a concern for you. These are not all the possible side effects of SUBLOCADE.Call your doctor for medical advice about side effects. You may report side effects to the FDA at 1-800-FDA-1088. General information about SUBLOCADEMedicines are sometimes prescribed for purposes other than those listed in a Medication Guide. You can ask your doctor or pharmacist for information that is written for healthcare professionals.What are the ingredients in SUBLOCADE?Active ingredient: buprenorphineATRIGEL® delivery system: biodegradable 50:50 poly(DL-lactide-co-glycolide) polymer and a biocompatible solvent, N-methyl-2-pyrrolidone (NMP).© 2022, Indivior UK Limited. All Rights Reserved.SUBLOCADE® is a registered trademark of Indivior UK Limited.Manufactured by Curia Global Inc. Albany, NY 12203For more information, go to or call 1-877-782-6966.This Medication Guide has been approved by the U.S. Food and Drug Administration. Issued: 08/2022。
中英双语的药品说明书

中英双语的药品说明书药品说明书是一种专业化的文档,旨在向患者提供关于特定药物的详细信息,包括药物的配方、适应症、用法用量、不良反应、禁忌症、警告和注意事项等。
以下是一个关于药品说明书的双语参考内容。
药品说明书一、药品名称中文名称:[药品名称]英文名称:[Drug Name]二、成分中文名称:[主要成分]英文名称:[Active Ingredient]作用:[描述主要成分的功效及作用]三、适应症中文名称:[适应症]英文名称:[Indications]【中文描述用药适应症】【英文描述用药适应症】四、用法用量中文名称:[用法用量]英文名称:[Dosage and Administration]【中文描述正确用药的方法和剂量】【英文描述正确用药的方法和剂量】五、不良反应中文名称:[不良反应]英文名称:[Adverse Reactions]【中文描述可能引起的不良反应,包括常见和罕见的不良反应】【英文描述可能引起的不良反应,包括常见和罕见的不良反应】六、禁忌症中文名称:[禁忌症]英文名称:[Contraindications]【中文描述使用该药物的禁忌症】【英文描述使用该药物的禁忌症】七、警告和注意事项中文名称:[警告和注意事项]英文名称:[Warnings and Precautions]【中文描述使用该药物时需要特别注意的事项,包括特殊人群的用药注意事项】【英文描述使用该药物时需要特别注意的事项,包括特殊人群的用药注意事项】八、儿童用药指导中文名称:[儿童用药指导]英文名称:[Pediatric Use]【中文描述使用该药物给儿童用药的特殊指导】【英文描述使用该药物给儿童用药的特殊指导】九、孕妇和哺乳期妇女用药指导中文名称:[孕妇和哺乳期妇女用药指导]英文名称:[Use in Pregnant and Nursing Women]【中文描述使用该药物给孕妇和哺乳期妇女用药的特殊指导】【英文描述使用该药物给孕妇和哺乳期妇女用药的特殊指导】十、药物相互作用中文名称:[药物相互作用]英文名称:[Drug Interactions]【中文描述该药物与其他药物及物质的相互作用】【英文描述该药物与其他药物及物质的相互作用】十一、药物过量中文名称:[药物过量]英文名称:[Overdosage]【中文描述该药物过量使用的症状和处理方法】【英文描述该药物过量使用的症状和处理方法】十二、贮藏中文名称:[贮藏]英文名称:[Storage]【中文描述正确的药物贮藏方式和条件】【英文描述正确的药物贮藏方式和条件】十三、包装中文名称:[包装]英文名称:[Presentation]【中文描述药物的包装形式和包装材料】【英文描述药物的包装形式和包装材料】十四、有效期中文名称:[有效期]英文名称:[Expiry Date]【中文描述药物的有效期】【英文描述药物的有效期】十五、说明书修订日期中文名称:[说明书修订日期]英文名称:[Revision Date]【中文描述说明书的修订日期】【英文描述说明书的修订日期】以上是药品说明书的双语参考内容,用于提供给患者详细了解特定药物的信息。
美FDA修改伐仑克林说明书
参考 文献 :
【 郑志华.07 1 】 20 年下半年广东省医院用药情况分析Ⅱ. 日药学 , 0 , ( )8 — 6 】今 2 81 2 :5 8 0 8 [郑志华. 08 2 】 20 年一季度广东省医院用药情况分析U. 日药学,0 81 ()9 - 6 】今 20 , 4 :5 9 8
ቤተ መጻሕፍቲ ባይዱ
0 1, . )而对照组患者却轻度升 高。谷 甾醇 0 血症 患者 胆 固醇 生物 合成途 径中众 多酶
生命和 健康 的主 要疾病之 一。高胆 固醇
血症是动脉 粥样硬化 的危 险因 素 ,容 易 诱发 动脉 粥样硬化和 冠心病 。E ei b zt e mi
类的活性降低 , 他汀类药物 常常无 效。然
引起 L L R功 能异 常 , D— 导致 病情 严 重 、 难 以控 制 。G ge等将 5 an O例 H F 患 oH
醇 的过 度吸收和 肝排泄胆 固醇 、植 物 固 醇 的减 少 ,从而 导致血浆 和组织 中谷 甾 醇和 油菜甾醇 的浓度增加 以及过早 发生 的动脉粥样硬化 。通过在 一项多中心、 双 盲 、随机 、对照 试验 中,Me S n等研究 了 eei b 对谷 甾醇血症 患者 的疗效 。治 zt e mi
4 E ei b z t e的 不 良反 应 mi
口服 ee mie后 ,少 数 患者 出现 zt b i 疼痛 、痉挛 和无 力 的肌 肉失 调症状 、 血
样 具有 良好 的治疗 作用 。
具有 良好 的疗效 。E emb 的不 良反应 z iie t 很轻 , 与安慰剂类似 。 zt ie Ee mb 临床应用 i 的时间不长 , 内的研 究资料相 对匮乏 , 国 仍需进一步 的研 究 。
TECFIDERA FDA说明书(英文)
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use TECFIDERA safely and effectively. See full prescribing information for TECFIDERA.TECFIDERA™ (dimethyl fumarate) delayed-release capsules, for oral useInitial U.S. Approval: 2013-------INDICATIONS AND USAGE------- TECFIDERA is indicated for the treatment of patients with relapsing forms of multiple sclerosis (1)-------DOSAGE AND ADMINISTRATION-------∙Starting dose: 120 mg twice a day, orally, for 7 days (2)∙Maintenance dose after 7 days: 240 mg twice a day, orally (2)∙Swallow TECFIDERA capsules whole and intact. Do not crush, chew, or sprinkle capsule contents on food (2)∙Take TECFIDERA with or without food (2)-------DOSAGE FORMS AND STRENGTHS-------Delayed-release capsules: 120 mg and 240 mg (3)-------CONTRAINDICATIONS-------None (4)-------WARNINGS AND PRECAUTIONS------- TECFIDERA may cause lymphopenia. A recent CBC should be available before initiating treatment with TECFIDERA. A CBC is recommended annually, and as clinically indicated. Consider withholding treatment in patients with serious infections. (5.1, 6.1)-------ADVERSE REACTIONS-------Most common adverse reactions (incidence ≥10% and ≥2% placebo) were flushing, abdominal pain, diarrhea, and nausea (6.1)To report SUSPECTED ADVERSE REACTIONS, contact Biogen Idec at 1-800-456-2255 or FDA at 1-800-FDA-1088 or /medwatch.-------USE IN SPECIFIC POPULATIONS-------∙Pregnancy: based on animal data, may cause fetal harm (8.1)See 17 for PATIENT COUNSELING INFORMATION and FDA- approved patient labelingRevised: 03/2013FULL PRESCRIBING INFORMATION: CONTENTS*1 INDICATIONS AND USAGE2 DOSAGE AND ADMINISTRATION 2.1 Dosing Information2.2 Blood Test Prior to Initiation of Therapy3 DOSAGE FORMS AND STRENGTHS4 CONTRAINDICATIONS5 WARNINGS AND PRECAUTIONS5.1 Lymphopenia5.2 Flushing6 ADVERSE REACTIONS6.1 Clinical Trials Experience8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.3 Nursing Mothers8.4 Pediatric Use8.5 Geriatric Use11 DESCRIPTION 12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.2 Pharmacodynamics12.3 Pharmacokinetics13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility13.2 Animal Toxicology and/or Pharmacology14 CLINICAL STUDIES16 HOW SUPPLIED/STORAGE AND HANDLING17 PATIENT COUNSELING INFORMATION17.1 Dosage17.2 Flushing and Gastrointestinal (GI) Reactions17.3 Pregnancy and Pregnancy Registry17.4 Lymphocyte Counts* Sections or subsections omitted from the full prescribing information are not listedFULL PRESCRIBING INFORMATION1 INDICATIONS AND USAGETECFIDERA is indicated for the treatment of patients with relapsing forms of multiple sclerosis.2 DOSAGE AND ADMINISTRATION2.1 Dosing InformationThe starting dose for TECFIDERA is 120 mg twice a day orally. After 7 days, the dose should be increased to the maintenance dose of 240 mg twice a day orally. TECFIDERA should be swallowed whole and intact. TECFIDERA should not be crushed or chewed and the capsule contents should not be sprinkled on food. TECFIDERA can be taken with or without food. Administration with food may reduce the incidence of flushing [see Clinical Pharmacology (12.3)].2.2 Blood Test Prior to Initiation of TherapyA recent complete blood cell count (CBC) (i.e., within 6 months) is recommended before initiation of therapy to identify patients with pre-existing low lymphocyte counts.3 DOSAGE FORMS AND STRENGTHSTECFIDERA is available as hard gelatin delayed-release capsules containing 120 mg or 240 mg of dimethyl fumarate. The 120 mg capsules have a green cap and white body, printed with “BG-12 120 mg” in black ink on the body. The 240 mg capsules have a green cap and a green body, printed with “BG-12 240 mg” in black ink on the body.4 CONTRAINDICATIONSNone.5 WARNINGS AND PRECAUTIONS5.1 LymphopeniaTECFIDERA may decrease lymphocyte counts [see Adverse Reactions (6.1)]. In the MS placebo controlled trials, mean lymphocyte counts decreased by approximately 30% during the first year of treatment with TECFIDERA and then remained stable. Four weeks after stopping TECFIDERA, mean lymphocyte counts increased but did not return to baseline. Six percent (6%) of TECFIDERA patients and <1% of placebo patients experienced lymphocyte counts <0.5x109/L (lower limit of normal 0.91x109/L). The incidence of infections (60% vs 58%) and serious infections (2% vs 2%) was similar in patients treated with TECFIDERA or placebo, respectively. There was no increased incidence of serious infections observed in patients with lymphocyte counts <0.8x109/L or 0.5x109/L.Before initiating treatment with TECFIDERA, a recent CBC (i.e., within 6 months) should be available. A CBC is recommended annually, and as clinically indicated. Withholding treatment should be considered in patients with serious infections until the infection(s) is resolved. TECFIDERA has not been studied in patients with pre-existing low lymphocyte counts.5.2 FlushingTECFIDERA may cause flushing (e.g., warmth, redness, itching, and/or burning sensation). In clinical trials, 40% of TECFIDERA treated patients experienced flushing. Flushing symptoms generally began soon after initiating TECFIDERA and usually improved or resolved over time. In the majority of patients who experienced flushing, it was mild or moderate in severity. Three percent (3%) ofpatients discontinued TECFIDERA for flushing and <1% had serious flushing symptoms that were not life-threatening but led to hospitalization. Administration of TECFIDERA with food may reduce the incidence of flushing.6 ADVERSE REACTIONSThe following important adverse reactions are described elsewhere in labeling: Lymphopenia, Flushing [see Warnings and Precautions (5.1, 5.2)].6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.The most common adverse reactions (incidence ≥10% and ≥2% more than placebo) for TECFIDERA were flushing, abdominal pain, diarrhea, and nausea.Adverse Reactions in Placebo-Controlled TrialsIn the two well-controlled studies demonstrating effectiveness, 1529 patients received TECFIDERA with an overall exposure of 2244 person-years [see Clinical Studies (14)].The adverse reactions presented in the table below are based on safety information from 769 patients treated with TECFIDERA 240 mg twice a day and 771 placebo-treated patients.Table 1:Adverse Reactions in Study 1 and 2 reported for TECFIDERA 240 mg BIDat ≥ 2% higher incidence than placeboTECFIDERAN=769% Placebo N=771%Blood and Lymphatic System DisordersLymphopenia 2 <1 Gastrointestinal DisordersAbdominal pain Diarrhea Nausea Vomiting Dyspepsia 181412951011953Vascular DisordersFlushing 40 6 Skin and Subcutaneous Tissue DisordersPruritus RashErythema 885431InvestigationsAlbumin urine presentAspartate aminotransferase increased 6442GastrointestinalTECFIDERA caused GI events (e.g., nausea, vomiting, diarrhea, abdominal pain, and dyspepsia). The incidence of GI events was higher early in the course of treatment (primarily in month 1) and usually decreased over time in patients treated with TECFIDERA compared with placebo. Four percent (4%) of patients treated with TECFIDERA and less than 1% of placebo patients discontinued due to gastrointestinal events. The incidence of serious GI events was 1% in patients treated with TECFIDERA.Hepatic TransaminasesAn increased incidence of elevations of hepatic transaminases in patients treated with TECFIDERA was seen primarily during the first six months of treatment, and most patients with elevations had levels < 3 times the upper limit of normal (ULN). Elevations of alanine aminotransferase and aspartate aminotransferase to ≥ 3 times the ULN occurred in a small number of patients treated with both TECFIDERA and placebo and were balanced between groups. There were no elevations in transaminases ≥3 times the ULN with concomitant elevations in total bilirubin > 2 times the ULN. Discontinuations due to elevated hepatic transaminases were < 1% and were similar in patients treated with TECFIDERA or placebo.EosinophiliaA transient increase in mean eosinophil counts was seen during the first 2 months of therapy.Adverse Reactions in Placebo-Controlled and Uncontrolled StudiesIn placebo-controlled and uncontrolled clinical studies, a total of 2513 patients have received TECFIDERA and been followed for periods up to 4 years with an overall exposure of 4603 person-years. Approximately 1162 patients have received more than 2 years of treatment with TECFIDERA. The adverse reaction profile of TECFIDERA in the uncontrolled clinical studies was consistent with the experience in the placebo-controlled clinical trials.8 USE IN SPECIFIC POPULATIONS8.1 PregnancyPregnancy Category CThere are no adequate and well-controlled studies in pregnant women. In animals, adverse effects on offspring survival, growth, sexual maturation, and neurobehavioral function were observed when dimethyl fumarate (DMF) was administered during pregnancy and lactation at clinically relevant doses. TECFIDERA should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.In rats administered DMF orally (25, 100, 250 mg/kg/day) throughout organogenesis, embryofetal toxicity (reduced fetal body weight and delayed ossification) were observed at the highest dose tested. This dose also produced evidence of maternal toxicity (reduced body weight). Plasma exposure (AUC) for monomethyl fumarate (MMF), the major circulating metabolite, at the no-effect dose is approximately three times that in humans at the recommended human dose (RHD) of 480 mg/day. In rabbits administered DMF orally (25, 75, and 150 mg/kg/day) throughout organogenesis, embryolethality and decreased maternal body weight were observed at the highest dose tested. The plasma AUC for MMF at the no-effect dose is approximately 5 times that in humans at the RHD.Oral administration of DMF (25, 100, and 250 mg/kg/day) to rats throughout organogenesis and lactation resulted in increased lethality, persistent reductions in body weight, delayed sexual maturation (male and female pups), and reduced testicular weight at the highest dose tested. Neurobehavioral impairment was observed at all doses. A no-effect dose for developmental toxicity was not identified. The lowest dose tested was associated with plasma AUC for MMF lower than that in humans at the RHD.Pregnancy RegistryThere is a pregnancy registry that monitors pregnancy outcomes in women exposed to TECFIDERA during pregnancy. Encourage patients to enroll by calling 1-800-456-2255.8.3 Nursing MothersIt is not known whether this drug is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when TECFIDERA is administered to a nursing woman.8.4 Pediatric UseSafety and effectiveness in pediatric patients have not been established. 8.5 Geriatric UseClinical studies of TECFIDERA did not include sufficient numbers of patients aged 65 and over to determine whether they respond differently from younger patients. 11 DESCRIPTIONTECFIDERA contains dimethyl fumarate which is also known by its chemical name, dimethyl (E) butenedioate, (C 6H 8O 4). It has the following structure:HHOOOODimethyl fumarate is a white to off-white powder that is highly soluble in water with a molecular mass of 144.13. TECFIDERA is provided as hard gelatin delayed-release capsules for oral administration, containing 120 mg or 240 mg of dimethyl fumarate consisting of the following inactive ingredients: microcrystalline cellulose, silicified microcrystalline cellulose, croscarmellose sodium, talc, silica colloidal silicon dioxide, magnesium stearate, triethyl citrate, methacrylic acid copolymer - Type A, methacrylic acid copolymer dispersion, simethicone (30% emulsion), sodium lauryl sulphate, and polysorbate 80. The capsule shell, printed with black ink, contains the following inactive ingredients: gelatin, titanium dioxide, FD&C blue 1; brilliant blue FCF, yellow iron oxide and black iron oxide. 12 CLINICAL PHARMACOLOGY 12.1 Mechanism of ActionThe mechanism by which dimethyl fumarate (DMF) exerts its therapeutic effect in multiple sclerosis is unknown. DMF and the metabolite, monomethyl fumarate (MMF), have been shown to activate the Nuclear factor (erythroid-derived 2)-like 2 (Nrf2) pathway in vitro and in vivo in animals and humans. The Nrf2 pathway is involved in the cellular response to oxidative stress. MMF has been identified as a nicotinic acid receptor agonist in vitro .12.2 PharmacodynamicsPotential to prolong the QT intervalIn a placebo controlled thorough QT study performed in healthy subjects, there was no evidence that dimethyl fumarate caused QT interval prolongation of clinical significance (i.e., the upper bound of the 90% confidence interval for the largest placebo-adjusted, baseline-corrected QTc was below 10 ms).12.3 PharmacokineticsAfter oral administration of TECFIDERA, dimethyl fumarate undergoes rapid presystemic hydrolysis by esterases and is converted to its active metabolite, monomethyl fumarate (MMF). Dimethyl fumarate is not quantifiable in plasma following oral administration of TECFIDERA. Therefore all pharmacokinetic analyses related to TECFIDERA were performed with plasma MMF concentrations. Pharmacokinetic data were obtained in subjects with multiple sclerosis and healthy volunteers.AbsorptionThe median T max of MMF is 2-2.5 hours. The peak plasma concentration (C max) and overall exposure (AUC) increased approximately dose proportionally in the dose range studied (120 mg to 360 mg). Following administration of TECFIDERA 240 mg twice a day with food, the mean C max of MMF was 1.87 mg/L and AUC was 8.21 mg.hr/L in MS patients.A high-fat, high-calorie meal did not affect the AUC of MMF but decreased its Cmax by 40%. The T max was delayed from 2.0 hours to 5.5 hours. In this study, the incidence of flushing was reduced by approximately 25% in the fed state.DistributionThe apparent volume of distribution of MMF varies between 53 and 73 L in healthy subjects. Human plasma protein binding of MMF is 27-45% and independent of concentration.MetabolismIn humans, dimethyl fumarate is extensively metabolized by esterases, which are ubiquitous in the gastrointestinal tract, blood, and tissues, before it reaches the systemic circulation. Further metabolism of MMF occurs through the tricarboxylic acid (TCA) cycle, with no involvement of the cytochrome P450 (CYP) system. MMF, fumaric and citric acid, and glucose are the major metabolites in plasma.EliminationExhalation of CO2 is the primary route of elimination, accounting for approximately 60% of the TECFIDERA dose. Renal and fecal elimination are minor routes of elimination, accounting for 16% and 1% of the dose respectively. Trace amounts of unchanged MMF were present in urine.The terminal half-life of MMF is approximately 1 hour and no circulating MMF is present at 24 hours in the majority of individuals. Accumulation of MMF does not occur with multiple doses of TECFIDERA.Specific PopulationsBody weight, gender, and age do not require dosage adjustment.No studies have been conducted in subjects with hepatic or renal impairment. However, neither condition would be expected to affect exposure to MMF and therefore no dosage adjustment is necessary.Drug Interaction StudiesNo potential drug interactions with dimethyl fumarate or MMF were identified in in vitro CYP inhibition and induction studies, or in P-glycoprotein studies. Single doses of interferon beta-1a or glatiramer acetate did not alter the pharmacokinetics of MMF. Aspirin, when administered approximately 30 minutes before TECFIDERA, did not alter the pharmacokinetics of MMF.13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of FertilityCarcinogenesisCarcinogenicity studies of dimethyl fumarate (DMF) were conducted in mice and rats. In mice, oral administration of DMF (25, 75, 200, and 400 mg/kg/day) for up to two years resulted in an increase in nonglandular stomach (forestomach) and kidney tumors: squamous cell carcinomas and papillomas of the forestomach in males and females at 200 and 400 mg/kg/day; leiomyosarcomas of the forestomach at 400 mg/kg/day in males and females; renal tubular adenomas and carcinomas at 200 and 400 mg/kg/day in males; and renal tubule adenomas at 400 mg/kg/day in females. Plasma MMF exposure (AUC) at the highest dose not associated with tumors in mice (75 mg/kg/day) was similar to that in humans at the recommended human dose (RHD) of 480 mg/day.In rats, oral administration of DMF (25, 50, 100, and 150 mg/kg/day) for up to two years resulted in increases in squamous cell carcinomas and papillomas of the forestomach at all doses tested in males and females, and in testicular interstitial (Leydig) cell adenomas at 100 and 150 mg/kg/day. Plasma MMF AUC at the lowest dose tested was lower than that in humans at the RHD.MutagenesisDimethyl fumarate (DMF) and monomethyl fumarate (MMF) were not mutagenic in the in vitro bacterial reverse mutation (Ames) assay. DMF and MMF were clastogenic in the in vitro chromosomal aberration assay in human peripheral blood lymphocytes in the absence of metabolic activation. DMF was not clastogenic in the in vivo micronucleus assay in the rat.Impairment of FertilityIn male rats, oral administration of DMF (75, 250, and 375 mg/kg/day) prior to and throughout the mating period had no effect on fertility; however, increases in non-motile sperm were observed at the mid and high doses. The no-effect dose for adverse effects on sperm is similar to the recommended human dose (RHD) of 480 mg/day on a body surface area (mg/m2) basis.In female rats, oral administration of DMF (20, 100, and 250 mg/kg/day) prior to and during mating and continuing to gestation day 7 caused disruption of the estrous cycle and increases in embryolethality at the highest dose tested. The highest dose not associated with adverse effects (100 mg/kg/day) is twice the RHD on a mg/m2 basis.Testicular toxicity (germinal epithelial degeneration, atrophy, hypospermia, and/or hyperplasia) was observed at clinically relevant doses in mice, rats, and dogs in subchronic and chronic oral toxicity studies of DMF, and in a chronic oral toxicity study evaluating a combination of four fumaric acid esters (including DMF) in rats.13.2 Animal Toxicology and/or PharmacologyKidney toxicity was observed after repeated oral administration of dimethyl fumarate (DMF) in mice, rats, dogs, and monkeys. Renal tubule epithelia regeneration, suggestive of tubule epithelial injury, was observed in all species. Renal tubular hyperplasia was observed in rats with dosing for up to two years. Cortical atrophy and interstitial fibrosis were observed in dogs and monkeys at doses above 5 mg/kg/day. In monkeys, the highest dose tested (75 mg/kg/day) was associated with single cell necrosis and multifocal and diffuse interstitial fibrosis, indicating irreversible loss of renal tissue and function. In dogs and monkeys, the 5 mg/kg/day dose was associated with plasma MMF exposures less than or similar to that in humans at the recommended human dose (RHD).A dose-related increase in incidence and severity of retinal degeneration was observed in mice following oral administration of DMF for up to two years at doses above 75 mg/kg/day, a dose associated with plasma MMF exposure (AUC) similar to that in humans at the RHD.14 CLINICAL STUDIESThe efficacy and safety of TECFIDERA were demonstrated in two studies (Studies 1 and 2) that evaluated TECFIDERA taken either twice or three times a day in patients with relapsing-remitting multiple sclerosis (RRMS). The starting dose for TECFIDERA was 120 mg twice or three times a day for the first 7 days, followed by an increase to 240 mg twice or three times a day. Both studies included patients who had experienced at least 1 relapse over the year preceding the trial or had a brain Magnetic Resonance Imaging (MRI) scan demonstrating at least one gadolinium-enhancing (Gd+) lesion within 6 weeks of randomization. The Expanded Disability Status Scale (EDSS) was also assessed and patients could have scores ranging from 0 to 5. Neurological evaluations were performed at baseline, every 3 months, and at the time of suspected relapse. MRI evaluations were performed at baseline, month 6, and year 1 and 2 in a subset of patients (44% in Study 1 and 48% in Study 2).Study 1: Placebo-Controlled Trial in RRMSStudy 1 was a 2-year randomized, double-blind, placebo-controlled study in 1234 patients with RRMS. The primary endpoint was the proportion of patients relapsed at 2 years. Additional endpoints at 2 years included the number of new or newly enlarging T2 hyperintense lesions, number of new T1 hypointense lesions, number of Gd+ lesions, annualized relapse rate (ARR), and time to confirmed disability progression. Confirmed disability progression was defined as at least a 1 point increase from baseline EDSS (1.5 point increase for patients with baseline EDSS of 0) sustained for 12 weeks.Patients were randomized to receive TECFIDERA 240 mg twice a day (n=410), TECFIDERA 240 mg three times a day (n=416), or placebo (n=408) for up to 2 years. The median age was 39 years, median time since diagnosis was 4 years, and median EDSS score at baseline was 2. The median time on study drug for all treatment arms was 96 weeks. The percentages of patients who completed 96 weeks on study drug per treatment group were 69% for patients assigned to TECFIDERA 240 mg twice a day, 69% for patients assigned to TECFIDERA 240 mg three times a day and 65% for patients assigned to placebo groups.TECFIDERA had a statistically significant effect on all of the endpoints described above and the 240 mg three times daily dose showed no additional benefit over the TECFIDERA 240 mg twice daily dose. The results for this study (240 mg twice a day vs. placebo) are shown in Table 2 and Figure 1.Table 2: Clinical and MRI Results of Study 1TECFIDERA240 mg BID Placebo P-valueClinical Endpoints N=410 N=408Proportion relapsing (primary endpoint) 27% 46% <0.0001Relative risk reduction 49%Annualized relapse rate Relative reduction 0.17253%0.364 <0.0001Proportion with disability progression Relative risk reduction 16%38%27% 0.0050MRI Endpoints N=152 N=165Mean number of new or newly enlarging T2 lesions over 2 yearsPercentage of subjects with no new or newly enlarging lesions2.645%1727%<0.0001TECFIDERA 240 mg BID Placebo P-valueNumber of Gd+ lesions at 2 years Mean (median)Percentage of subjects withlesions1lesion2lesions3 to4 lesions5 or more lesionsRelative odds reduction(percentage) 0.1 (0)93%5%<1%<1%90%1.8 (0)62%10%8%9%11%<0.0001Mean number of new T1 hypointenselesions over 2 years1.5 5.6 < 0.0001Figure 1: Time to 12-Week Confirmed Progression of Disability (Study 1)Study 2: Placebo-Controlled Trial in RRMSStudy 2 was a 2-year multicenter, randomized, double-blind, placebo-controlled study that also included an open-label comparator arm in patients with RRMS. The primary endpoint was the annualized relapse rate at 2 years. Additional endpoints at 2 years includedthe number of new or newly enlarging T2 hyperintense lesions, number of T1 hypointense lesions, number of Gd+ lesions, proportion of patients relapsed, and time to confirmed disability progression as defined in Study 1.Patients were randomized to receive TECFIDERA 240 mg twice a day (n=359), TECFIDERA 240 mg three times a day (n=345), an open-label comparator (n=350), or placebo (n=363) for up to 2 years. The median age was 37 years, median time since diagnosis was 3 years, and median EDSS score at baseline was 2.5. The median time on study drug for all treatment arms was 96 weeks. The percentages of patients who completed 96 weeks on study drug per treatment group were 72% for patients assigned to TECFIDERA 240 mg twice a day, 70% for patients assigned to TECFIDERA 240 mg three times a day and 64% for patients assigned to placebo groups.TECFIDERA had a statistically significant effect on the relapse and MRI endpoints described above. There was no statistically significant effect on disability progression. The TECFIDERA 240 mg three times daily dose resulted in no additional benefit over the TECFIDERA 240 mg twice daily dose. The results for this study (240 mg twice a day vs. placebo) are shown in Table 3.Table 3: Clinical and MRI Results of Study 2TECFIDERA240 mg BIDPlacebo P-valueClinical Endpoints N=359 N=363Annualized relapse rate Relative reduction 0.22444%0.401 <0.0001Proportion relapsingRelative risk reduction 29%34%41% 0.0020Proportion with disability progression Relative risk reduction 13%21%17% 0.25MRI Endpoints N=147 N=144Mean number of new or newly enlarging T2 lesions over 2 yearsPercentage of subjects with no new ornewly enlarging lesions5.127%17.412%<0.0001Number of Gd+ lesions at 2 yearsMean (median)Percentage of subjects with 0lesions1lesion2lesions3 to4 lesions5 or more lesionsRelative odds reduction(percentage) 0.5 (0.0)80%11%3%3%3%74%2.0 (0.0)61%17%6%2%14%<0.0001Mean number of new T1 hypointenselesions over 2 years3.0 7.0 <0.000116 HOW SUPPLIED/STORAGE AND HANDLINGTECFIDERA is available as hard gelatin delayed-release capsules in two strengths containing either 120 mg or 240 mg of dimethyl fumarate. The green and white 120 mg capsules are printed with “BG-12 120 mg” in black ink. The green 240 mg capsules are printed with “BG-12 240 mg” in black ink. TECFIDERA is available as follows:30-day Starter Pack, (NDC 64406-007-03):7-day bottle 120 mg capsules, quantity 1423-day bottle 240 mg capsules, quantity 46120 mg capsules:7-day bottle of 14 capsules (NDC 64406-005-01)240 mg capsules:30-day bottle of 60 capsules (NDC 64406-006-02)Store at 15°C to 30°C (59 to 86°F). Protect the capsules from light. Store in original container. Once opened, discard bottles of TECFIDERA after 90 days.17 PATIENT COUNSELING INFORMATIONSee FDA-approved patient labeling (Patient Information)17.1 DosageInform patients that they will be provided two strengths of TECFIDERA when starting treatment: 120 mg capsules for the 7 day starter dose and 240 mg capsules for the maintenance dose, both to be taken twice daily. Inform patients to swallow TECFIDERA capsules whole and intact. Inform patients to not crush, chew, or sprinkle capsule contents on food. Inform patients that TECFIDERA can be taken with or without food [see Dosage and Administration (2.1)].17.2 Flushing and Gastrointestinal (GI) ReactionsFlushing and GI reactions (abdominal pain, diarrhea, and nausea) are the most common reactions, especially at the initiation of therapy, and may decrease over time. Advise patients to contact their healthcare provider if they experience persistent and/or severe flushing or GI reactions, as taking TECFIDERA with food may help [see Adverse Reactions (6.1)].17.3 Pregnancy and Pregnancy RegistryInstruct patients that if they are pregnant or plan to become pregnant while taking TECFIDERA they should inform their physician.Encourage patients to enroll in the TECFIDERA Pregnancy Registry if they become pregnant while taking TECFIDERA. Advise patients to call 1-800-456-2255 for more information [see Use in Specific Populations (8.1)].17.4 Lymphocyte CountsInform patients that TECFIDERA may decrease lymphocyte counts. A recent blood test (i.e., within 6 months) should be available before they start therapy to identify patients with pre-existing low lymphocyte counts. Blood tests are also recommended annually, and as clinically indicated [see Warnings and Precautions (5.1), Adverse Reactions (6.1)].。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use DULERA safely and effectively. See full prescribing information for DULERA.DULERA® 100 mcg/5 mcg (mometasone furoate 100 mcg and formoterol fumarate dihydrate 5 mcg) Inhalation AerosolDULERA® 200 mcg/5 mcg (mometasone furoate 200 mcg and formoterol fumarate dihydrate 5 mcg) Inhalation AerosolFOR ORAL INHALATIONInitial U.S. Approval: 2010WARNING: ASTHMA-RELATED DEATHSee full prescribing information for complete boxed warning.∙ Long-acting beta2-adrenergic agonists (LABA), such as formoterol, one of the active ingredients in DULERA, increase the risk of asthma-related death. Data from a large placebo-controlled U.S.study that compared the safety of another LABA (salmeterol) or placebo added to usual asthma therapy showed an increase in asthma-related deaths in patients receiving salmeterol. This finding with salmeterol is considered a class effect of the LABA, including formoterol. Currently available data are inadequate to determine whether concurrent use of inhaled corticosteroids or other long-term asthma control drugs mitigates the increased risk of asthma-related death from LABA. Available data from controlled clinical trials suggest that LABA increase the risk of asthma-related hospitalization in pediatric and adolescent patients.∙ When treating patients with asthma, prescribe DULERA only for patients with asthma not adequately controlled on a long-term asthma control medication, such as an inhaled corticosteroid or whose disease severity clearly warrants initiation of treatment with both an inhaled corticosteroid and LABA. Once asthma control is achieved and maintained, assess the patient at regular intervals and step down therapy (e.g., discontinue DULERA) if possible without loss of asthma control, and maintain the patient on a long-term asthma control medication, such as an inhaled corticosteroid. Do not use DULERA for patients whose asthma is adequately controlled on low or medium dose inhaled corticosteroids. (1.1, 5.1)---------------------------RECENT MAJOR CHANGES --------------------------Warnings and Precautions, Coexisting Conditions (5.15) 07/2013 ---------------------------INDICATIONS AND USAGE---------------------------DULERA is a combination product containing a corticosteroid and a long- acting beta2-adrenergic agonist indicated for:∙Treatment of asthma in patients 12 years of age and older. (1.1) Important limitations:∙Not indicated for the relief of acute bronchospasm. (1.1)-----------------------DOSAGE AND ADMINISTRATION ----------------------For oral inhalation only.Treatment of asthma in patients ≥12 years: 2 inhalations twice daily of DULERA 100 mcg/5 mcg or 200 mcg/5 mcg. Starting dosage is based on prior asthma therapy. (2.2)---------------------DOSAGE FORMS AND STRENGTHS---------------------Inhalation aerosol containing a combination of mometasone furoate (100 or 200 mcg) and formoterol fumarate dihydrate (5 mcg) per actuation. (3)------------------------------CONTRAINDICATIONS -----------------------------∙Primary treatment of status asthmaticus or acute episodes of asthma requiring intensive measures. (4.1)∙Hypersensitivity to any of the ingredients of DULERA. (4.2)-----------------------WARNINGS AND PRECAUTIONS-----------------------∙Asthma-related death: Long-acting beta2-adrenergic agonists increase the risk. Prescribe only for recommended patient populations. (5.1)∙Deterioration of disease and acute episodes: Do not initiate in acutely deteriorating asthma or to treat acute symptoms. (5.2)∙Use with additional long-acting beta2-agonist: Do not use in combination because of risk of overdose. (5.3) ∙ Localized infections: Candida albicans infection of the mouth and throatmay occur. Monitor patients periodically for signs of adverse effects onthe oral cavity. Advise patients to rinse the mouth following inhalation.(5.4)∙ Immunosuppression: Potential worsening of existing tuberculosis, fungal,bacterial, viral, or parasitic infection; or ocular herpes simplex infections.More serious or even fatal course of chickenpox or measles can occur insusceptible patients. Use with caution in patients with these infectionsbecause of the potential for worsening of these infections. (5.5)∙ Transferring patients from systemic corticosteroids: Risk of impairedadrenal function when transferring from oral steroids. Taper patientsslowly from systemic corticosteroids if transferring to DULERA. (5.6)∙ Hypercorticism and adrenal suppression: May occur with very highdosages or at the regular dosage in susceptible individuals. If suchchanges occur, discontinue DULERA slowly. (5.7)∙ Strong cytochrome P450 3A4 inhibitors (e.g., ritonavir): Risk ofincreased systemic corticosteroid effects. Exercise caution when usedwith DULERA. (5.8)∙ Paradoxical bronchospasm: Discontinue DULERA and institutealternative therapy if paradoxical bronchospasm occurs. (5.9)∙ Patients with cardiovascular disorders: Use with caution because of betaadrenergic stimulation. (5.11)∙ Decreases in bone mineral density: Monitor patients with major riskfactors for decreased bone mineral content. (5.12)∙ Effects on growth: Monitor growth of pediatric patients. (5.13)∙ Glaucoma and cataracts: Monitor patients with change in vision or with ahistory of increased intraocular pressure, glaucoma, and/or cataractsclosely. (5.14)∙ Coexisting conditions: Use with caution in patients with aneurysm,pheochromocytoma, convulsive disorders, thyrotoxicosis, diabetesmellitus, and ketoacidosis. (5.15)∙ Hypokalemia and hyperglycemia: Be alert to hypokalemia andhyperglycemia. (5.16)------------------------------ADVERSE REACTIONS -----------------------------Most common adverse reactions (reported in ≥3% of patients) included:∙Nasopharyngitis, sinusitis and headache. (6.1)To report SUSPECTED ADVERSE REACTIONS, contact Merck Sharp& Dohme Corp., a subsidiary of Merck & Co., Inc., at 1-877-888-4231 orFDA at 1-800-FDA-1088 or /medwatch.------------------------------DRUG INTERACTIONS------------------------------∙ Strong cytochrome P450 3A4 inhibitors (e.g., ritonavir): Use withcaution. May cause increased systemic corticosteroid effects. (7.1)∙ Adrenergic agents: Use with caution. Additional adrenergic drugs maypotentiate sympathetic effects. (7.2)∙ Xanthine derivatives and diuretics: Use with caution. May potentiateECG changes and/or hypokalemia. (7.3, 7.4)∙ MAO inhibitors, tricyclic antidepressants, macrolides, and drugs thatprolong QTc interval: Use with extreme caution. May potentiate effect onthe cardiovascular system. (7.5)∙ Beta-blockers: Use with caution and only when medically necessary.May decrease effectiveness and produce severe bronchospasm. (7.6)∙ Halogenated hydrocarbons: There is an elevated risk of arrhythmias inpatients receiving concomitant anesthesia with halogenatedhydrocarbons. (7.7)-----------------------USE IN SPECIFIC POPULATIONS ----------------------∙ Hepatic impairment: Monitor patients for signs of increased drugexposure. (8.6)See 17 for PATIENT COUNSELING INFORMATION and MedicationGuide.Revised:XX/XXXX08/2013FULL PRESCRIBING INFORMATION: CONTENTS* 2 DOSAGEANDADMINISTRATION2.1 GeneralWARNING: ASTHMA-RELATED DEATH 2.2 DosingINDICATIONSANDUSAGE 3 DOSAGE FORMS AND STRENGTHS 14.1 S tatusAsthmaticus4.2 H ypersensitivity5 WARNINGS AND PRECAUTIONS5.1 A sthma-RelatedDeath5.2 Deterioration of Disease and Acute Episodes5.3 Excessive Use of DULERA and Use with Other Long-ActingBeta2-Agonists5.4 L ocalEffects5.5 I mmunosuppression5.6 Transferring Patients from Systemic Corticosteroid Therapy5.7 Hypercorticism and Adrenal Suppression5.8 Drug Interactions with Strong Cytochrome P450 3A4 Inhibitors5.9 Paradoxical Bronchospasm and Upper Airway Symptoms5.10 I mmediate Hypersensitivity Reactions5.11 Cardiovascular and Central Nervous System Effects5.12 Reduction in Bone Mineral Density5.13 Effect on Growth5.14 Glaucoma and Cataracts5.15 Coexisting Conditions5.16 Hypokalemia and Hyperglycemia6 ADVERSEREACTIONS6.1 Clinical Trials Experience6.2 P ostmarketingExperience7 DRUGINTERACTIONS7.1 Inhibitors of Cytochrome P450 3A47.2 A drenergicagents7.3 X anthinederivatives7.4 D iuretics7.5 Monoamine oxidase inhibitors, tricyclic antidepressants, anddrugs known to prolong the QTc interval7.6 Beta-adrenergic receptor antagonists7.7 H alogenatedHydrocarbonsFULL PRESCRIBING INFORMATION 8 USE IN SPECIFIC POPULATIONS8.1 P regnancy8.2 Labor and Delivery8.3 N ursingMothers8.4 P ediatricUse8.5 G eriatricUse8.6 H epaticImpairment10 OVERDOSAGE10.1 Signs and Symptoms10.2 Treatment11 DESCRIPTION12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.2 Pharmacodynamics12.3 Pharmacokinetics13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility13.2 Animal Toxicology and/or Pharmacology14 CLINICAL STUDIES14.1 Asthma16 HOW SUPPLIED/STORAGE AND HANDLING16.1 How Supplied16.2 Storage and Handling17 PATIENT COUNSELING INFORMATION17.1 A sthma-Related Death17.2 Not for Acute Symptoms17.3 Do Not Use Additional Long-Acting Beta2-Agonists17.4 Risks Associated With Corticosteroid Therapy17.5 Risks Associated With Beta-Agonist Therapy*Sections or subsections omitted from the full prescribing information are not listed.WARNING: ASTHMA-RELATED DEATHLong-acting beta2-adrenergic agonists (LABA), such as formoterol, one of the active ingredients in DULERA, increase the risk of asthma-related death. Data from a large placebo-controlled U.S. study that compared the safety of another long-acting beta2-adrenergic agonist (salmeterol) or placebo added to usual asthma therapy showed an increase in asthma-related deaths in patients receiving salmeterol. This finding with salmeterol is considered a class effect of the LABA, including formoterol. Currently available data are inadequate to determine whether concurrent use of inhaled corticosteroids or other long-term asthma control drugs mitigates the increased risk of asthma-related death from LABA. Available data from controlled clinical trials suggest that LABA increase the risk of asthma-related hospitalization in pediatric and adolescent patients. Therefore, when treating patients with asthma, DULERA should only be used for patients not adequately controlled on a long-term asthma control medication, such as an inhaled corticosteroid or whose disease severity clearly warrants initiation of treatment with both an inhaled corticosteroid and LABA. Once asthma control is achieved and maintained, assess the patient at regular intervals and step down therapy (e.g., discontinue DULERA) if possible without loss of asthma control, and maintain the patient on a long-term asthma control medication, such as an inhaled corticosteroid. Do not use DULERA for patients whose asthma is adequately controlled on low or medium dose inhaled corticosteroids. [See Warnings and Precautions (5.1).]1 I NDICATIONSANDUSAGE1.1 Treatment of AsthmaDULERA is indicated for the treatment of asthma in patients 12 years of age and older.Long-acting beta2-adrenergic agonists, such as formoterol, one of the active ingredients in DULERA, increase the risk of asthma-related death. Available data from controlled clinical trials suggest that LABA increase the risk of asthma-related hospitalization in pediatric and adolescent patients [see Warnings and Precautions (5.1)]. Therefore, when treating patients with asthma, DULERA should only be used for patients not adequately controlled on a long-term asthma control medication, such as an inhaled corticosteroid or whose disease severity clearly warrants initiation of treatment with both an inhaled corticosteroid and LABA. Once asthma control is achieved and maintained, assess the patient at regular intervals and step down therapy (e.g., discontinue DULERA) if possible without loss of asthma control, and maintain the patient on a long-term asthma control medication, such as an inhaled corticosteroid. Do not use DULERA for patients whose asthma is adequately controlled on low or medium dose inhaled corticosteroids.Important Limitation of UseDULERA is NOT indicated for the relief of acute bronchospasm.2 DOSAGEANDADMINISTRATION2.1 GeneralDULERA should be administered only by the orally inhaled route (see Instructions for Using DULERA in the Medication Guide). After each dose, the patient should be advised to rinse his/her mouth with water without swallowing.The cap from the mouthpiece of the actuator should be removed before using DULERA.DULERA should be primed before using for the first time by releasing 4 test sprays into the air, away from the face, shaking well before each spray. In cases where the inhaler has not been used for more than 5 days, prime the inhaler again by releasing 4 test sprays into the air, away from the face, shaking well before each spray.The DULERA canister should only be used with the DULERA actuator. The DULERA actuator should not be used with any other inhalation drug product. Actuators from other products should not be used with the DULERA canister.2.2 DosingDULERA should be administered as two inhalations twice daily every day (morning and evening) by the orally inhaled route. Shake well prior to each inhalation.The recommended starting dosages for DULERA treatment are based on prior asthma therapy.Table 1: Recommended Dosages for DULERAPrevious Therapy Recommended Dose Maximum Recommended DailyDoseInhaled medium dose corticosteroids DULERA 100 mcg/5 mcg, 2inhalations twice daily400 mcg/20 mcgInhaled high dose corticosteroids DULERA 200 mcg/5 mcg, 2inhalations twice daily800 mcg/20 mcgThe maximum daily recommended dose is two inhalations of DULERA 200 mcg/5 mcg twice daily. Do not use more than two inhalations twice daily of the prescribed strength of DULERA as some patients are more likely to experience adverse effects with higher doses of formoterol. If symptoms arise between doses, an inhaled short-acting beta2-agonist should be taken for immediate relief.If a previously effective dosage regimen of DULERA fails to provide adequate control of asthma, the therapeutic regimen should be re-evaluated and additional therapeutic options, e.g., replacing the current strength of DULERA with a higher strength, adding additional inhaled corticosteroid, or initiating oral corticosteroids, should be considered.The maximum benefit may not be achieved for 1 week or longer after beginning treatment. Individual patients may experience a variable time to onset and degree of symptom relief. For patients ≥12 years of age who do not respond adequately after 2 weeks of therapy, higher strength may provide additional asthma control.3 DOSAGE FORMS AND STRENGTHSDULERA is a pressurized metered dose inhaler that is available in 2 strengths.DULERA 100 mcg/5 mcg delivers 100 mcg of mometasone furoate and 5 mcg of formoterol fumarate dihydrate per actuation. DULERA 200 mcg/5 mcg delivers 200 mcg of mometasone furoate and 5 mcg of formoterol fumarate dihydrate per actuation.4 CONTRAINDICATIONS4.1 Status AsthmaticusDULERA is contraindicated in the primary treatment of status asthmaticus or other acute episodes of asthma where intensive measures are required.4.2 HypersensitivityDULERA is contraindicated in patients with known hypersensitivity to mometasone furoate, formoterol fumarate, or any of the ingredients in DULERA [see Warnings and Precautions (5.10)].5 WARNINGSPRECAUTIONSAND5.1 Asthma-Related DeathLong-acting beta2-adrenergic agonists, such as formoterol, one of the active ingredients in DULERA, increase the risk of asthma-related death. Currently available data are inadequate to determine whether concurrent use of inhaled corticosteroids or other long-term asthma control drugs mitigates the increased risk of asthma-related death from LABA. Available data from controlled clinical trials suggest that LABA increase the risk of asthma-related hospitalization in pediatric and adolescent patients. Therefore, when treating patients with asthma, physicians should only prescribe DULERA for patients with asthma not adequately controlled on a long-term asthma control medication, such as an inhaled corticosteroid or whose disease severity clearly warrants initiation of treatment with both an inhaled corticosteroid and LABA. Once asthma control is achieved and maintained, assess the patient at regular intervals and step down therapy (e.g., discontinue DULERA) if possible without loss of asthma control, and maintain the patient on a long-term asthma control medication, such as an inhaled corticosteroid. Do not use DULERA for patients whose asthma is adequately controlled on low or medium dose inhaled corticosteroids.A 28-week, placebo-controlled US study comparing the safety of salmeterol with placebo, each added to usual asthma therapy, showed an increase in asthma-related deaths in patients receiving salmeterol (13/13,176 in patients treated with salmeterol vs. 3/13,179 in patients treated with placebo; RR 4.37, 95% CI 1.25, 15.34). This finding with salmeterol is considered a class effect of the LABAs, including formoterol, one of the active ingredients in DULERA. No study adequate to determine whether the rate of asthma-related death is increased with DULERA has been conducted.Clinical studies with formoterol suggested a higher incidence of serious asthma exacerbations in patients who received formoterol fumarate than in those who received placebo. The sizes of these studies were not adequate to precisely quantify the differences in serious asthma exacerbation rates between treatment groups.5.2 Deterioration of Disease and Acute EpisodesDULERA should not be initiated in patients during rapidly deteriorating or potentially life-threatening episodes of asthma. DULERA has not been studied in patients with acutely deteriorating asthma. The initiation of DULERA in this setting is not appropriate. Increasing use of inhaled, short-acting beta2-agonists is a marker of deteriorating asthma. In this situation, the patient requires immediate re-evaluation with reassessment of the treatment regimen, giving special consideration to the possible need for replacing the current strength of DULERA with a higher strength, adding additional inhaled corticosteroid, or initiating systemic corticosteroids. Patients should not use more than 2 inhalations twice daily (morning and evening) of DULERA.DULERA is not indicated for the relief of acute symptoms, i.e., as rescue therapy for the treatment of acute episodes of bronchospasm. An inhaled, short-acting beta2-agonist, not DULERA, should be used to relieve acute symptoms such as shortness of breath. When prescribing DULERA, the physician must also provide the patient with an inhaled, short-acting beta2-agonist (e.g., albuterol) for treatment of acute symptoms, despite regular twice-daily (morning and evening) use of DULERA.When beginning treatment with DULERA, patients who have been taking oral or inhaled, short-acting beta2-agonists on a regular basis (e.g., 4 times a day) should be instructed to discontinue the regular use of these drugs.5.3 Excessive Use of DULERA and Use with Other Long-Acting Beta2-AgonistsAs with other inhaled drugs containing beta2-adrenergic agents, DULERA should not be used more often than recommended, at higher doses than recommended, or in conjunction with other medications containing long-acting beta2-agonists, as an overdose may result. Clinically significant cardiovascular effects and fatalities have been reported in association with excessive use of inhaled sympathomimetic drugs. Patients using DULERA should not use an additional long-acting beta2-agonist (e.g., salmeterol, formoterol fumarate, arformoterol tartrate) for any reason, including prevention of exercise-induced bronchospasm (EIB) or the treatment of asthma.5.4 Local EffectsIn clinical trials, the development of localized infections of the mouth and pharynx with Candida albicans have occurred in patients treated with DULERA. If oropharyngeal candidiasis develops, it should be treated with appropriate local or systemic (i.e., oral) antifungal therapy while remaining on treatment with DULERA therapy, but at times therapy with DULERA may need to be interrupted. Advise patients to rinse the mouth after inhalation of DULERA.5.5 ImmunosuppressionPersons who are using drugs that suppress the immune system are more susceptible to infections than healthy individuals. Chickenpox and measles, for example, can have a more serious or even fatal course in susceptible children or adults using corticosteroids. In such children or adults who have not had these diseases or who are not properly immunized, particular care shouldbe taken to avoid exposure. How the dose, route, and duration of corticosteroid administration affect the risk of developing a disseminated infection is not known. The contribution of the underlying disease and/or prior corticosteroid treatment to the risk is also not known. If exposed to chickenpox, prophylaxis with varicella zoster immune globulin (VZIG) or pooled intravenous immunoglobulin (IVIG) may be indicated. If exposed to measles, prophylaxis with pooled intramuscular immunoglobulin (IG) may be indicated. (See the respective package inserts for complete VZIG and IG prescribing information.) If chickenpox develops, treatment with antiviral agents may be considered.DULERA should be used with caution, if at all, in patients with active or quiescent tuberculosis infection of the respiratory tract, untreated systemic fungal, bacterial, viral, or parasitic infections; or ocular herpes simplex.5.6 Transferring Patients from Systemic Corticosteroid TherapyParticular care is needed for patients who are transferred from systemically active corticosteroids to DULERA because deaths due to adrenal insufficiency have occurred in asthmatic patients during and after transfer from systemic corticosteroids to less systemically available inhaled corticosteroids. After withdrawal from systemic corticosteroids, a number of months are required for recovery of hypothalamic-pituitary-adrenal (HPA) function.Patients who have been previously maintained on 20 mg or more per day of prednisone (or its equivalent) may be most susceptible, particularly when their systemic corticosteroids have been almost completely withdrawn. During this period of HPA suppression, patients may exhibit signs and symptoms of adrenal insufficiency when exposed to trauma, surgery, or infection (particularly gastroenteritis) or other conditions associated with severe electrolyte loss. Although DULERA may improve control of asthma symptoms during these episodes, in recommended doses it supplies less than normal physiological amounts of corticosteroid systemically and does NOT provide the mineralocorticoid activity necessary for coping with these emergencies.During periods of stress or severe asthma attack, patients who have been withdrawn from systemic corticosteroids should be instructed to resume oral corticosteroids (in large doses) immediately and to contact their physicians for further instruction. These patients should also be instructed to carry a medical identification card indicating that they may need supplementary systemic corticosteroids during periods of stress or severe asthma attack.Patients requiring systemic corticosteroids should be weaned slowly from systemic corticosteroid use after transferring to DULERA. Lung function (FEV1 or PEF), beta-agonist use, and asthma symptoms should be carefully monitored during withdrawal of systemic corticosteroids. In addition to monitoring asthma signs and symptoms, patients should be observed for signs and symptoms of adrenal insufficiency such as fatigue, lassitude, weakness, nausea and vomiting, and hypotension.Transfer of patients from systemic corticosteroid therapy to DULERA may unmask allergic conditions previously suppressed by the systemic corticosteroid therapy, e.g., rhinitis, conjunctivitis, eczema, arthritis, and eosinophilic conditions.During withdrawal from oral corticosteroids, some patients may experience symptoms of systemically active corticosteroid withdrawal, e.g., joint and/or muscular pain, lassitude, and depression, despite maintenance or even improvement of respiratory function.5.7 Hypercorticism and Adrenal SuppressionMometasone furoate, a component of DULERA, will often help control asthma symptoms with less suppression of HPA function than therapeutically equivalent oral doses of prednisone. Since mometasone furoate is absorbed into the circulation and can be systemically active at higher doses, the beneficial effects of DULERA in minimizing HPA dysfunction may be expected only when recommended dosages are not exceeded and individual patients are titrated to the lowest effective dose.Because of the possibility of systemic absorption of inhaled corticosteroids, patients treated with DULERA should be observed carefully for any evidence of systemic corticosteroid effects. Particular care should be taken in observing patients postoperatively or during periods of stress for evidence of inadequate adrenal response.It is possible that systemic corticosteroid effects such as hypercorticism and adrenal suppression (including adrenal crisis) may appear in a small number of patients, particularly when mometasone furoate is administered at higher than recommended doses over prolonged periods of time. If such effects occur, the dosage of DULERA should be reduced slowly, consistent with accepted procedures for reducing systemic corticosteroids and for management of asthma symptoms.5.8 Drug Interactions with Strong Cytochrome P450 3A4 InhibitorsCaution should be exercised when considering the coadministration of DULERA with ketoconazole, and other known strong CYP3A4 inhibitors (e.g., ritonavir, atazanavir, clarithromycin, indinavir, itraconazole, nefazodone, nelfinavir, saquinavir, telithromycin) because adverse effects related to increased systemic exposure to mometasone furoate may occur [see Drug Interactions (7.1) and Clinical Pharmacology (12.3)].5.9 Paradoxical Bronchospasm and Upper Airway SymptomsDULERA may produce inhalation induced bronchospasm with an immediate increase in wheezing after dosing that may be life-threatening. If inhalation induced bronchospasm occurs, it should be treated immediately with an inhaled, short-acting bronchodilator. DULERA should be discontinued immediately and alternative therapy instituted.5.10 Immediate Hypersensitivity ReactionsImmediate hypersensitivity reactions may occur after administration of DULERA, as demonstrated by cases of urticaria, flushing, allergic dermatitis, and bronchospasm.5.11 Cardiovascular and Central Nervous System EffectsExcessive beta-adrenergic stimulation has been associated with seizures, angina, hypertension or hypotension, tachycardia with rates up to 200 beats/min, arrhythmias, nervousness, headache, tremor, palpitation, nausea, dizziness, fatigue, malaise, and insomnia. Therefore, DULERA should be used with caution in patients with cardiovascular disorders, especially coronary insufficiency, cardiac arrhythmias, and hypertension.Formoterol fumarate, a component of DULERA, can produce a clinically significant cardiovascular effect in some patients as measured by pulse rate, blood pressure, and/or symptoms. Although such effects are uncommon after administration of DULERA at recommended doses, if they occur, the drug may need to be discontinued. In addition, beta-agonists have been reported to produce ECG changes, such as flattening of the T wave, prolongation of the QTc interval, and ST segment depression. The clinical significance of these findings is unknown. Fatalities have been reported in association with excessive use of inhaled sympathomimetic drugs.5.12 Reduction in Bone Mineral DensityDecreases in bone mineral density (BMD) have been observed with long-term administration of products containing inhaled corticosteroids, including mometasone furoate, one of the components of DULERA. The clinical significance of small changes in BMD with regard to long-term outcomes, such as fracture, is unknown. Patients with major risk factors for decreased bone mineral content, such as prolonged immobilization, family history of osteoporosis, or chronic use of drugs that can reduce bone mass (e.g., anticonvulsants and corticosteroids) should be monitored and treated with established standards of care.In a 2-year double-blind study in 103 male and female asthma patients 18 to 50 years of age previously maintained on bronchodilator therapy (Baseline FEV1 85%-88% predicted), treatment with mometasone furoate dry powder inhaler 200 mcg twice daily resulted in significant reductions in lumbar spine (LS) BMD at the end of the treatment period compared to placebo. The mean change from Baseline to Endpoint in the lumbar spine BMD was -0.015 (-1.43%) for the mometasone furoate group compared to 0.002 (0.25%) for the placebo group. In another 2-year double-blind study in 87 male and female asthma patients 18 to 50 years of age previously maintained on bronchodilator therapy (Baseline FEV1 82%-83% predicted), treatment with mometasone furoate 400 mcg twice daily demonstrated no statistically significant changes in lumbar spine BMD at the end of the treatment period compared to placebo. The mean change from Baseline to Endpoint in the lumbar spine BMD was -0.018 (-1.57%) for the mometasone furoate group compared to -0.006 (-0.43%) for the placebo group.5.13 Effect on GrowthOrally inhaled corticosteroids, including DULERA, may cause a reduction in growth velocity when administered to pediatric patients. Monitor the growth of pediatric patients receiving DULERA routinely (e.g., via stadiometry). To minimize the systemic effects of orally inhaled corticosteroids, including DULERA, titrate each patient’s dose to the lowest dosage that effectively controls his/her symptoms [see Use in Specific Populations (8.4)].5.14 Glaucoma and CataractsGlaucoma, increased intraocular pressure, and cataracts have been reported following the use of long-term administration of inhaled corticosteroids, including mometasone furoate, a component of DULERA. Therefore, close monitoring is warranted in patients with a change in vision or with a history of increased intraocular pressure, glaucoma, and/or cataracts [see Adverse Reactions (6)].5.15 Coexisting ConditionsDULERA, like other medications containing sympathomimetic amines, should be used with caution in patients with aneurysm, pheochromocytoma, convulsive disorders, or thyrotoxicosis; and in patients who are unusually responsive to sympathomimetic amines. Doses of the related beta2-agonist albuterol, when administered intravenously, have been reported to aggravate preexisting diabetes mellitus and ketoacidosis.5.16 Hypokalemia and HyperglycemiaBeta2-agonist medications may produce significant hypokalemia in some patients, possibly through intracellular shunting, which has the potential to produce adverse cardiovascular effects. The decrease in serum potassium is usually transient, not requiring supplementation. Clinically significant changes in blood glucose and/or serum potassium were seen infrequently during clinical studies with DULERA at recommended doses.。