ICU护理记录单模板
ICU护理文书书写

刻度 cm 更换敷料 回血情况 更换敷料 通畅情况
cm 输入情况回血情 更换敷料
回血情况 更换敷料回血情 况 更换敷料 通畅情况
□ 置留胃管
□ 引流管
日期
部位
深度
cm
通畅情况
深度
cm
通畅情况
深度
cm
通畅情况
通畅情况
通畅情况
通畅情况
护士签名
表格式护理记录单 版本3.2
二 护理记录单
其他监护及护理项目
体温单
传统纸质版
手绘记录,费时费力, 效率低,而且容易出错
进阶版 电子版体温单
颜值高,工作量减轻,但 效率仍不高,录入易出错
高级版 ——移动护理PDA
生命体征等测量后直接录 入系统,准确高效 ,工作 效率普遍提升60%
二 护理记录单
眉栏:床号姓名住院号。。。 生命体征:T/P/R/BP/SPO2/CVP。。。 趋势图、数字记录 神志 呼吸模式参数 摄入量 排出量 泵入药 静脉注射药 CRRT 各种评估内容等
二 护理记录单
护理评分 主要护理问题 护理计划 护理记录或病情记录
护理记录内容应当根据相关专科护理特点 在病情栏内如实记录病情观察情况、采取的护理措施和 实际效果
自定义项
表格式护理记录单 版本1
各种自定义项编号
ICU 护 理 记 录 单
床号 日期 2 姓名 生命体征 李* 性别 CVP 男 年龄 瞳 意 孔 65岁 ID 机械通气 1234567 入 量 ml 总 量 引流 通 性 项目 颜色 畅 状 胃管 N 咖啡 粘 稠 尿管 N 淡黄 清 亮 腹腔 N 暗红 血 性 量 出 量
重症监护室护理记录单

CARES 护理
敷 料
胃 管
/
营 养 管
部
位
IV通路
护
理
CARES 护理
内容说明:
(一)CARES 基础护理
B-Bath 沐浴
L-Linen 更换床单源自C-Cath 引流管护理SH-Shave 刮胡子
E-Eye 眼睛护理
SP-Shampoo 洗头
O-Oral 口腔护理
P-Pericare 会阴护理
S-Skin 皮肤护理
基
础 护 理
o
so √
约 束
s
CARES 护理
活
动
/
翻
身
/ 卧
位
CARES SESTRAINTS
ACTIVITY\TURNING\POSITION
DRESSING NG\FEEDING TUBE
CARES 护理
敷 料
胃 管
/
营 养 管
部
位
IV通路
护
理
CARES 护理
内容说明: (三)ACTIVTY / TURNING / POSITION 活动/翻身/卧位
4-Patient asleep with a brisk response to a light glabellar tap 入睡,可唤醒,轻扣眉间反应灵敏
NEURO SIGNS 神经系统
(二)Ramsay Scale Ramsay 分级 3-Patient responds to commands only 嗜睡,能听从指令 2-Patient cooperative,oriented and tranquil 合作,清醒安静 1-Patient anxious or agitated or both 焦虑,激动不安
病危护理记录单范文模板

病危护理记录单范文模板英文回答:A template for a critically ill nursing care record:Title: Critically Ill Nursing Care Record.Date: [Date]Patient Name: [Patient Name]Medical Condition: [Brief description of the patient's medical condition]Medical History: [Brief summary of the patient's medical history]1. Vital Signs:Blood Pressure: [Record the patient's blood pressurereadings]Heart Rate: [Record the patient's heart rate readings]Respiratory Rate: [Record the patient's respiratory rate readings]Temperature: [Record the patient's body temperature readings]2. Medications:Name of Medication: [Record the name of the medication] Dosage: [Record the dosage of the medication]Administration Route: [Record the route of administration]Time and Frequency: [Record the time and frequency of medication administration]3. Interventions:Oxygen Therapy: [Record the type and flow rate of oxygen therapy]Intravenous Therapy: [Record the type and rate of intravenous fluids]Wound Care: [Record the type of wound care performed]Pain Management: [Record the pain assessment and interventions]4. Nursing Assessments:Neurological Assessment: [Record the patient's level of consciousness, pupil size, and response to stimuli]Respiratory Assessment: [Record the patient's lung sounds, oxygen saturation, and respiratory effort]Cardiovascular Assessment: [Record the patient's heartsounds, peripheral pulses, and edema]Gastrointestinal Assessment: [Record the patient's bowel sounds, appetite, and bowel movements]5. Communication:Communication with the Patient: [Record any conversations or interactions with the patient]Communication with the Family: [Record any conversations or interactions with the patient's family]6. Other Observations:Skin Integrity: [Record any changes in the patient's skin condition]Urinary Output: [Record the patient's urine output]Laboratory Results: [Record any abnormal laboratory results]7. Plan of Care:Nursing Diagnosis: [Record the nursing diagnosis]Goals: [Record the goals for the patient's care]Interventions: [Record the nursing interventions to achieve the goals]Evaluation: [Record the evaluation of the patient's response to the interventions]中文回答:病危护理记录单范文模板:标题,病危护理记录单。
手术护理记录单

附件4X X X 医院手术护理及物品清点记录单日期:年月日手术护理记录(器械物品清点)单填写要求手术护理记录单填写说明一、书写原则:1、记录书写内容必须真实准确,包括病人姓名、性别、科室、床号、住院号、年龄、术前诊断、术前皮肤情况、手术开始时间、手术名称、出手术室时间。
2、手术护理记录单一律用蓝黑墨水笔填写,字迹清晰、工整,禁止涂改,不得采用刮、粘、涂等方法掩盖或去除原来的字迹。
3、时间书写方式应采用国际标准,例如:下午3点,应写成15:00。
二、各种基本资料栏内的填写:1、患者基本资料栏必须正确记录:姓名、性别、科室、床号、住院号、年龄、血型、手术间、术前诊断、术前皮肤情况、手术名称、出手术室时间、术后患者去向。
若术前有压疮,应仔细填写压疮部位、大小。
2、洗手、巡回护士接替时间按实际时间填写,护士必须签全名,并在相应栏上填明是关腔前还是关腔后。
3、手术体位:以实际摆放体位填写。
4、皮肤消毒液:在相应栏内打钩。
5、局麻手术时麻醉药品按术中使用情况在相应药品前打钩,并填上使用剂量。
6、消毒物品检测合格在相应栏内打钩。
7、术后患者去向与实际交接科室在相应栏内如实填写。
8、特殊物品放置位置:应于人形图上注明相应的代表符号,标示实际放置位置(压手、压腿“=”,手支架“→”、负极片“□”、输液部分“△”、引流管“○”等)。
9、止血带:使用止血带时,应注明使用的部位、压力、开始时间及结束时间。
(注明压力,充气时间、放气时间、再次充气时间,放气时间。
)10、术前、中是否放置导尿管,是否使用电刀,“是”在相应栏内打钩。
术毕皮肤情况应真实填写,若术前有压疮,术后皮肤情况未发生改变可写为“同前”。
11、术中、后是否送细菌培养、冰冻切片、病理标本,并在相应栏内注明送检个数,标本处理者签全名。
12、开腹前手术物品清点是否正确,“正确”在相应栏内打钩,查看手术包名称是否正确。
13、手术用品的计数:(1)应计数的用品有:器械、纱布、盐水垫、刀片、缝针、其它:花生米、棉球、脑棉等。
一般护理记录单书写范文

一般护理记录单书写范文护理记录单。
姓名,XXX 年龄,XX岁性别,男/女床号,XXX。
入院日期,XXXX年XX月XX日入院诊断,XXXXX。
护理日期,XXXX年XX月XX日护理记录人,XXX。
一、生命体征及一般情况:1. 体温,XX.X℃2. 脉搏,XX次/分3. 呼吸,XX次/分 4. 血压,XXX/XXXmmHg。
5. 意识,清醒/嗜睡/昏迷6. 饮食,正常/少食/禁食7. 排尿,正常/尿潴留/失禁。
8. 排便,正常/便秘/腹泻。
二、主要护理内容:1. 皮肤护理,清洁皮肤,保持干燥,定时翻身,预防压疮。
2. 导尿护理,定时更换尿袋,观察尿量和尿色,保持导尿通畅。
3. 饮食护理,根据医嘱给予适量饮食,观察饮食情况及进食量。
4. 睡眠护理,保持环境安静,营造舒适的睡眠环境,观察睡眠情况。
5. 洗浴护理,定时给予患者洗澡,保持个人卫生。
6. 康复训练,根据康复医师指导,进行康复训练,帮助患者康复。
7. 安全护理,保持环境整洁,防止跌倒和意外伤害。
8. 心理护理,与患者进行交流,关心患者的情绪变化,给予心理安慰。
三、特殊护理及注意事项:1. 给予特殊治疗,如雾化吸入、输液、换药等特殊治疗,观察治疗效果。
2. 观察病情变化,观察患者病情变化,及时报告医生。
3. 用药观察,观察患者用药情况及药物不良反应。
4. 定期复查,协助医生进行定期复查,如血常规、生化等检查。
四、护理记录:XXXX年XX月XX日。
患者生命体征平稳,无发热、心率正常,血压稳定。
患者精神状态良好,饮食进食情况良好,排尿排便正常。
皮肤无异常,导尿通畅,无不适感。
定时更换尿袋,观察尿量和尿色,保持导尿通畅。
睡眠良好,无不适感。
定时给予患者洗澡,保持个人卫生。
协助患者进行康复训练,患者情绪稳定,与患者交流良好,给予心理安慰。
患者安全意识良好,无意外伤害。
XXXX年XX月XX日。
患者生命体征平稳,无发热、心率正常,血压稳定。
患者精神状态良好,饮食进食情况良好,排尿排便正常。
一份完整icu护理记录单范文
一份完整icu护理记录单范文In the intensive care unit (ICU), the nursing documentation plays a crucial role in providing comprehensive and accurate information about the patient's condition, care provided, and response to interventions. This record serves as a legal document, communication tool, and reference for future care. In this article, I will provide a sample ICU nursing documentation to demonstrate the essential components and the importance of a well-documented record.Paragraph 1: Introduction and Patient InformationIn this ICU nursing documentation, I will present the case of Mr. John Doe, a 55-year-old male admitted to the ICU following a severe motor vehicle accident. The documentation begins with the patient's basic information, including name, age, gender, and admission date. It is essential to ensure the accuracy of this information to avoid any confusion or misidentification.Paragraph 2: Presenting Complaint and Medical HistoryMr. Doe was admitted to the ICU with complaints of severe chest pain, shortness of breath, and multiple fractures. His medical history includes hypertension, diabetes mellitus, and a previous myocardial infarction. It is crucial to incorporate the patient's presenting complaints and medical history to provide a comprehensive understanding of the patient's condition and potential risk factors.Paragraph 3: Assessment Findings and Vital SignsUpon admission, Mr. Doe's assessment findings revealed a conscious but anxious patient with labored breathing. His vital signs were as follows: heart rate 110 beats per minute, blood pressure 150/90 mmHg, respiratory rate 28 breaths per minute, oxygen saturation 90% on room air. These assessment findings and vital signs indicate the severity of the patient's condition and the need for immediate intervention.Paragraph 4: Nursing Interventions and ResponseNursing interventions implemented for Mr. Doe included administering supplemental oxygen via a nasal cannula, initiating cardiac monitoring, and providing pain management. The patient's response to these interventions was monitored closely. Within 30 minutes, the patient's oxygen saturation improved to 95% on a 2-liter nasal cannula, and his pain score decreased from 8/10 to 4/10. These positive responses demonstrate the effectiveness of the nursing interventions provided.Paragraph 5: Medications and Laboratory ResultsDuring Mr. Doe's ICU stay, various medications were administered, including intravenous morphine for pain control, sublingual nitroglycerin for chest pain, and insulin for glycemic control. Laboratory results showed an elevated troponin level, indicating myocardial injury. These medication administrations and laboratory results are vital to document as they guide further treatment decisionsand provide a comprehensive picture of the patient's condition.Paragraph 6: Collaborative Care and Discharge PlanningThroughout Mr. Doe's ICU stay, a multidisciplinary approach was adopted to ensure comprehensive care. This involved regular communication and collaboration with the medical team, respiratory therapists, physical therapists, and social workers. Discharge planning was initiated earlyto ensure a smooth transition to a lower level of care. The patient's family was also involved in the decision-making process, providing emotional support and educationregarding post-discharge care.In conclusion, a well-documented ICU nursing record is essential for providing comprehensive and accurate information about the patient's condition, care provided, and response to interventions. It serves as a legal document, communication tool, and reference for future care. By incorporating the patient's information, medical history, assessment findings, interventions, medicationadministration, and collaborative care, a complete ICU nursing documentation can be achieved, ensuring high-quality patient care and continuity of care.。
ICU护理记录单书写

在信息化、个性化和跨学科合 作的发展过程中,ICU护理记 录单书写面临着数据安全和隐 私保护、标准化和规范化建设 、医护人员素质和技能提升等 多方面的挑战。
THANK YOU
感谢聆听
神经系统预防措施
控制患者基础疾病、密切观察神经系统症状 、及时处理异常情况等。
并发症发生时的处理措施和效果评价
呼吸系统并发症处理
根据感染情况选用合适抗生素、加强呼吸道管理、调整机 械通气参数等,效果评价包括感染控制情况、呼吸功能改 善情况等。
循环系统并发症处理
针对心律失常类型选用合适抗心律失常药物、纠正电解质 紊乱、改善心功能等,效果评价包括心律失常控制情况、 心功能改善情况等。
血氧饱和度
通过指脉氧监测仪持续监测患者 的血氧饱和度,记录具体数值, 注意有无缺氧现象。
异常情况及处理措施
异常情况
在监测过程中发现任何生命体征异常,如高热、低血压、呼吸急促等,应立即记 录并报告医生。
处理措施
根据医嘱采取相应的处理措施,如给予退热药物、升压药物、吸氧等,同时密切 观察患者的病情变化,及时调整治疗方案。在护理记录单中详细记录处理措施的 执行情况和患者的反应。
未来发展趋势和挑战
信息化发展
个性化需求
跨学科合作
面临的挑战
随着医疗信息化的不断推进, 电子护理记录单将逐步取代纸 质护理记录单,实现实时、动 态、全面的患者信息记录和管 理。
随着患者需求的多样化,ICU 护理记录单需要更加关注患者 的个性化需求和心理状态,提 供更加人性化的护理服务。
未来ICU护理记录单书写将更 加注重与其他学科的交流和合 作,实现跨学科的综合治疗和 护理。
发生情况等。
心理护理及健康教育实施情况
ICU护理工作质量检查记录表
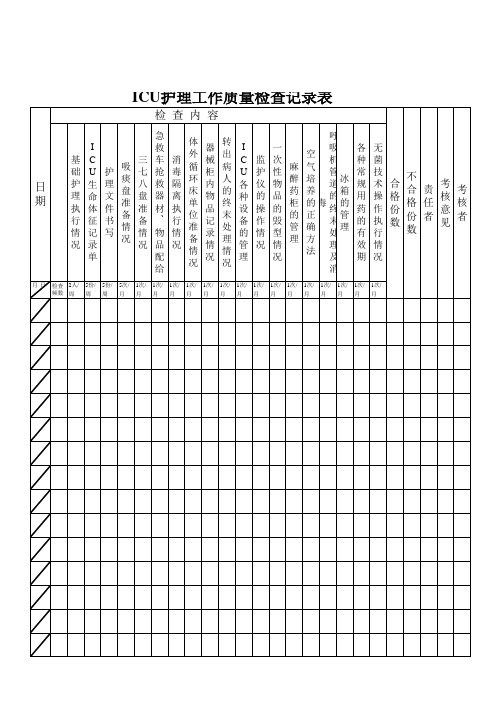
检 查 内 容
I C U 生 命 体 征 记 录 单
5份/ 周
日 期
基 础 护 理 执 行 情 况
护 理 文 件 书 写
吸 痰 盘 准 备 情 况
三 七 八 盘 准 备 情 况
急 救 车 抢 救 器 材 、 物 品 配 给
1次/ 月
消 毒 隔 离 执 行 情 况
体 外 循 环 床 单 位 准 备 情 况
月
1次/ 月
冰 箱 的 管 理
各 种 常 规 用 药 的 有 效 期
1次/ 月
无 菌 技 术 操 作 执 行 情 况
1次/ 月
不 合 考 合 责 考 格 核 格 任 核 份 意 份 者 者 数 见 数
日
检查 2人/ 频数 周
5份/ 周
5次/ 月
1次/ 月
1次/ 月
1次/ 月
1次/ 月
1次/ 月
1次/ 月
1次/ 月
器 械 柜 内 物 品 记 录 情 况
1次/ 月
转 出 病 人 的 终 末 处 理 情 况
1次/ 月
I C U 各 种 设 备 的 管 理
1次/ 月
监 护 仪 的 操 作 情 况
一 次 性 物 品 的 毁 型 情 况
1次/ 月
ቤተ መጻሕፍቲ ባይዱ
麻 醉 药 柜 的 管 理
空 气 培 养 的 正 确 方 法
呼 吸 机 管 道 的 终 末 处 理 及 消 毒
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
备注:
神志:1.清醒;2.嗜睡;3.意识模糊;4.昏睡;5.浅昏迷;6.深昏迷。
瞳孔反射:1.灵敏;2.迟钝;3.无。
人工气道方式:1.经口播管;2.气管切开;3.鼻插管;4.面罩。
吸氧方式:1.鼻塞;2.鼻导管;3.面罩;4.气管插管;5.气切导管。
呼吸音:用√表示清晰1.上低;2.下低;3.上痰鸣音;4.下痰鸣音;5其他。
静脉导管:1.外周;2.中心静脉(a颈内b锁骨下c股静脉);3.PlCC
管道:1、尿管;2.普通胃管;3.鼻肠管;4.T管;5.切口引流管;6.胸引管;7.腹腔引流管;8.其他通畅用√.
引流液颜色:1.血性;2.褐色;3.黄色;4.其他。
痰色:1.白粘痰;2.黄脓痰;3.稀薄粘痰;4.血性痰;5.粘痰略带血性。
痰量:1.少量;2.中等;3.大量。
约束末梢循环:1.良好;2.水肿;3.青紫:4.其他。
其他护理项目:1.洗头;2.换床单;3.换尿垫;4.换衣裤;5.协助进食水;6.面部清洁和梳头;7.足部清洁;8.趾/指甲护理。
约束部位:1.上肢;2.下肢;3.上下肢;4.胸部。
皮肤:用√完好,有问题请在病情中具体描述皮肤护理:1.气垫床;2.翻身q2h;3.局部皮肤换药(压疮评估见评估表)。