Int J Oncol Vol35 n2 page 393
肝细胞癌的立体定向放射治疗

carcinoma:anevidence⁃basedanalysis[J].AmJTransplant,2006,6(11):2644⁃2650.[15]LewandowskiRJ,KulikLM,RiazA,etal.Acomparativeanalysisoftransarterialdownstagingforhepatocellularcarcinoma:chemoembolizationversusradioembolization[J].AmJTransplant,2009,9(8):1920⁃1928.[16]LangH,SotiropoulosGC,DömlandM,etal.Liverresectionforhepatocellularcarcinomainnon⁃cirrhoticliverwithoutunderlyingviralhepatitis[J].BrJSurg,2005,92(2):198⁃202.[17]MajnoPE,LencioniR,MornexF,etal.Isthetreatmentofhepatocellularcarcinomaonthewaitinglistnecessary?[J].LiverTranspl,2011,17(suppl2):S98⁃S108.[18]ZimmermanMA,GhobrialRM,TongMJ,etal.Recurrenceofhepatocellularcarcinomafollowinglivertransplantation:areviewofpreoperativeandpostoperativeprognosticindicators[J].ArchSurg,2008,143(2):182⁃188.[19]HollebecqueA,DecaensT,BoleslawskiE,etal.Naturalhistoryandtherapeuticmanagementofrecurrenthepatocellularcarcinomaafterlivertransplantation[J].GastroenterolClinBiol,2009,33(5):361⁃369.(收稿日期:2015⁃05⁃04)DOI:10.3760/cma.j.issn.0253⁃3766.2015.09.004作者单位:200032上海,复旦大学附属中山医院放疗科通信作者:曾昭冲,Email:zeng.zhaochong@zs⁃hospital.sh.cn肝细胞癌的立体定向放射治疗曾昭冲ʌ主题词ɔ㊀癌,肝细胞;㊀放射疗法;㊀立体定向技术ʌSubjectwordsɔ㊀Carcinoma,hepatocellular;㊀Radiotherapy;㊀StereotaxicTechniques㊀㊀肝细胞癌是我国常见的恶性肿瘤,目前治疗小肝癌的手段为手术切除和射频消融,但仍有一部分患者不宜接受手术或射频消融㊂近年来,随着放疗技术的进步,立体定向放射治疗(stereotacticbodyradiationtherapy,SBRT)的临床应用逐渐增多,已有一些回顾性的研究显示,其对小肝癌的治疗效果与传统的外科手术或射频消融相当,可作为早期肝癌的根治性治疗手段之一㊂因此,肝癌的SBRT值得我们进一步研究和探索㊂一㊁基本概念1.定义:目前的SBRT是利用影像设备采集肿瘤及周围正常组织的图像,在治疗计划系统的配合下,利用立体定向原理和技术,对人体内肿瘤实施精确定位,将窄束放射线聚集于靶点,给予较大剂量照射,使肿瘤产生局灶性破坏,而正常组织受损伤的程度降到最低,达到根治性治疗的目的㊂肝癌的SBRT必须满足有四维CT的影像设备引导或肿瘤追踪系统㊁非常精确的患者体位固定㊁放疗前的个体化图像校正㊁放疗设备能聚焦到肿瘤而肿瘤之外的射线梯度下降快等条件㊂2.SBRT设备:肝癌的SBRT需要精确的放疗设备,诸如射波刀㊁螺旋断层放疗系统㊁旋转拉弧适形放疗技术(rapidArc⁃SBRT)以及带有CT的图像引导下的放疗设备等㊂射波刀的构造和原理是自动化机器人追踪,180ʎ非共面旋转㊂用射波刀治疗肝内肿瘤的最大特点是具有实时追踪肿瘤的能力㊂螺旋断层放疗系统是利用螺旋CT成像的逆原理进行放射治疗,原则上可以在人体内实现各种要求的剂量分布㊂其最大的优点是可同时照射多靶区,实现适形度非常高的剂量分布,治疗范围大,更适合中晚期肝癌的放射治疗㊂3.肝癌SBRT的优点:(1)就放疗效果而言,肝癌属于剂量依赖性肿瘤㊂而肝脏属于并联器官,一部分肝脏受到大剂量的放射损伤,未受到损伤的正常肝可以代偿性增生㊂(2)对远离重要器官或组织(如肠道)的肝脏肿瘤,放射治疗不会危及其他组织而导致并发症㊂(3)肝脏肿瘤会随呼吸运动,SBRT设备可有呼吸追踪功能,或限制腹部呼吸幅度,以减少正常肝脏的损伤㊂(4)SBRT可以大剂量低分割放疗,放疗时间可以缩短到1周以内,方便患者㊂二㊁肝细胞癌SBRT的效果1.安全性和毒副反应:目前有关肝细胞癌SBRT的报道,大多局限在安全性研究㊂SBRT的毒副反应轻微,绝大部分患者为1㊁2级毒副反应㊂在肝功能方面,多数文献报道,患者会出现轻中度的转氨酶升高或Child⁃Pugh肝功能评分上升2分[1⁃6],9.4%的患者会出现非致命性的放射性肝病[7],仅有1% 2%的患者会出现致死型放射性肝病[6,8⁃9]㊂少部分患者会出现胃肠道毒副反应,3㊁4级胃肠道毒副反应的发生率为2% 3%[8,10⁃11]㊂出现胃肠道放射性损伤的主要原因为肿瘤靠近胃肠道㊂有研究显示,肿瘤靠近肋骨,会出现肋骨骨折[12⁃13],或因皮肤及皮下肌肉受损伤,个别患者会出现胸壁疼痛[2]㊂亦有出现胆道狭窄的报道[12]㊂预防和减少严重毒副反应的关键是要求患者放疗前肝功能正常㊁正常肝体积>700cm3,如肿瘤靠近胃肠道,单次放疗剂量必须降低㊂如能达到以上要求,接受SBRT的患者则不会出现严重毒副反应㊂2.肿瘤反应:肿瘤退缩与放疗剂量有关㊂Facciuto等[14]的研究结果显示,肝细胞癌患者采用放疗剂量为30Gy㊁分2 4次完成方案治疗的有效率不足50%㊂Ibarra等[15]的研究结果显示,原发性肝癌患者的肿瘤体积较大,在放疗剂量偏低(7 15Gy,治疗3次,中位30Gy)的情况下,有效率仅为26%,放射野内的复发率却高达31.6%㊂Tekeda等[16]报道,巴塞罗那临床肝癌(BarcelonaClinicLiverCancer,BCLC)分期为A期或B期的肝细胞癌患者,采用放疗剂量35 40Gy㊁分5次完成方案治疗的3年局部控制率为92%㊂根据以往有关SBRT的报道,如给予患者40 60Gy的低分割剂量,美国癌症联合委员会(AmericanJointCommitteeonCancer,AJCC)分期为Ⅰ Ⅱ期患者的局部控制率可达90%左右,Ⅲ期及以上或BCLC分期为C期患者的局部控制率为60% 70%[1⁃17]㊂因此,在全肝耐受量可行的情况下,我们推荐,早期肝细胞癌的SBRT最好给予35 40Gy㊁分5次完成方案㊂3.生存情况:目前报道的小肝细胞癌SBRT的患者,大部分是外科手术或射频消融后复发者,少数为初始治疗者㊂对于复发患者,其预后不及初治患者好㊂Huang等[11]报道,36例复发肝细胞癌患者接受SBRT,并以同期不接受SBRT的患者作为对照,SBRT组和对照组各选28例患者作为配对比较,结果显示,SBRT组和对照组患者的2年生存率分别为72.6%和42.1%,差异有统计学意义(P=0.013)㊂单因素和多因素分析结果均显示,SBRT可以明显改善患者的生存状况㊂有研究显示,早期肝细胞癌患者接受SBRT的3年生存率约为70%[9,16];BCLC分期为A期者的5年生存率为58%[8],这与小肝癌患者接受外科手术切除的效果相当㊂4.等待移植:对于符合肝移植适应证的肝细胞癌患者,原位肝移植是最有效的治疗手段㊂但是,肝脏供体数量有限,许多患者在较长的肝源等待过程中发生肿瘤进展,从而失去最佳的治疗机会㊂因此,在肝源等待过程中延缓肿瘤进展的衔接治疗非常重要㊂美国Rochester大学医学中心和密西根WilliamBeaumont医院报道了18例移植前接受大分割SBRT的肝癌患者,中位放疗剂量为50Gy,分10次完成㊂10例患者的病灶出现病理性坏死,没有严重的胃肠道不良反应和放射性肝炎发生㊂其中12例患者在放疗后6.3个月的中位等待期内成功接受肝切除或肝移植术㊂在术后19.6个月的中位随访期内,所有患者均生存[4]㊂由此可见,大分割SBRT是肝癌患者等待肝移植前一种安全有效的衔接治疗方式,能够在移植前缩小或控制肿瘤,且能使患者的生存获益㊂三㊁SBRT的肿瘤剂量和正常组织受量关于SBRT的分割剂量和分割形式仍缺乏统一的认识㊂用L⁃Q模式把SBRT的低分割剂量换算为常规分割剂量,放疗剂量往往被高估㊂因此,不能简单地用L⁃Q模式换算㊂另外,我们尚需摸索肿瘤大小㊁放疗剂量与肿瘤控制率之间的关系㊂1.肿瘤的治疗量:SBRT的出发点就是肿瘤达到根治剂量的放疗,而周围正常组织受到放射损伤最小,且所用的分割次数最少㊂早期肝细胞癌的放疗剂量ȡ40Gy/次,共放疗5次,患者的3年局部控制率>90%㊂然而,还有很多因素限制肿瘤放疗剂量的提高,特别是正常肝的耐受量㊁肝脏的功能情况㊁肿瘤的大小㊁化疗或分子靶向治疗药物的应用㊁肿瘤周边正常组织等㊂2.正常组织耐受量:近年来,国外学者在肝癌SBRT中肿瘤病灶的放疗剂量㊁正常组织耐受量以及放疗毒副反应等方面进行了较多研究㊂Huang等[11]的研究结果显示,肝脏体积>700ml,平均照射剂量<15Gy;肾脏V16<33%(分4次照射时),V18<33%(分5次照射时);脊髓最大照射剂量<23Gy(分4次照射时),最大照射剂量<25Gy(分5次照射时);心脏最大照射剂量<32Gy(分4次照射时),最大照射剂量<35Gy(分5次照射时);胃V25<5ml(分4次照射时),最大照射剂量<29Gy(分4次照射时),V27<5ml(分5次照射时),最大照射剂量<31Gy(分5次照射时);小肠V23<5ml(分4次照射时);最大照射剂量<27Gy(分4次照射时);V25<5ml(分5次照射时);最大照射剂量<29Gy(分5次照射时);大肠V24<5ml(分4次照射时),最大照射剂量<28Gy(分4次照射时),V25<5ml(分5次照射时),最大照射剂量<29Gy(分5次照射时)㊂Sawrie等[18]收集了38个前瞻性临床研究,分析了SBRT肝癌的毒副反应,结果显示毒性较轻,但对肝细胞癌患者,因存在肝脏的基础疾病,放射性肝损伤的发生率稍高;而对于转移性肝癌出现放射性肝损伤者,其正常肝体积均<700ml,提示SBRT肝癌时,需保留足够多的正常肝脏组织㊂四㊁正常肝组织和肿瘤组织SBRT后的变化1.正常肝组织:由于每次SBRT的分割剂量大,肿瘤周围的正常肝组织受到的每次分割剂量也较大,其变化和常规分割照射时也不同㊂在CT上,放疗后正常肝组织早期为低密度变化,病理表现为肝窦内血流变慢,红细胞淤积在肝窦内,加上水肿㊁脂肪浸润,即使平扫,也呈低密度变化[19]㊂Olsen等[20]报道,15例肝癌患者的正常肝组织受照剂量为30Gy,在CT上能明显看到低密度影,病理上有明显的肝损伤条带,分为坏死区㊁纤维化区和静脉闭塞性病区(肝窦淤血㊁肝索紊乱)㊂放疗后2 6个月随访,肝体积缩小13% 30%,放疗剂量与体积缩小呈正相关㊂慢性肝损伤一般发生于放疗后6个月,CT上表现为静脉相高密度,为血管阻塞,中央静脉和肝窦纤维蛋白进行性沉积[17]㊂2.肿瘤组织:SBRT为大分割剂量,肿瘤细胞受到辐射死亡,肿瘤内的血管内皮细胞也受损,血管密闭,肿瘤血供减少,出现肿瘤坏死,CT或磁共振成像上表现为进行性缺乏血供,坏死的区域随时间推移不断升高㊂有研究显示,放疗后3㊁6㊁9和12个月随访,肿瘤坏死比例分别为59%㊁69%㊁81%和92%,但肿瘤体积缩小不明显㊂以实体瘤的疗效评价标准(responseevaluationcriteriainsolidtumor,RECIST)评价放疗效果,放疗后12个月完全缓解者占15%,以欧洲肝病学会(EuropeanAssociationfortheStudyoftheLiver,EASL)标准评价,完全坏死者占50%;RECIST标准评价为部分缓解9例,稳定1例,但以EASL标准评价则为完全缓解,明显的坏死在放疗结束后9个月出现[17]㊂因此,肝细胞癌SBRT的疗效评价EASL标准要优于RECIST标准㊂小肝癌采用SBRT安全有效,已经得到美国国家综合癌症网指南的推荐㊂但目前仍缺少高级别的循证医学证据,美国肿瘤放射治疗协作组织和国际原子能机构等组织,已经开展多项随机前瞻性多中心临床研究,相信在不久的将来会有更多的循证医学证据呈现㊂参考文献[1]CulletonS,JiangH,HaddadCR,etal.OutcomesfollowingdefinitivestereotacticbodyradiotherapyforpatientswithChild⁃PughBorChepatocellularcarcinoma[J].RadiotherOncol,2014,111(3):412⁃417.[2]YamashitaH,OnishiH,MatsumotoY,etal.Localeffectofstereotacticbodyradiotherapyforprimaryandmetastaticlivertumorsin130Japanesepatients[J].RadiatOncol,2014,9:112.[3]JungJ,YoonSM,KimSY,etal.Radiation⁃inducedliverdiseaseafterstereotacticbodyradiotherapyforsmallhepatocellularcarcinoma:clinicalanddose⁃volumetricparameters[J].RadiatOncol,2013,8:249.[4]KatzAW,ChawlaS,QuZ,etal.Stereotactichypofractionatedradiationtherapyasabridgetotransplantationforhepatocellularcarcinoma:clinicaloutcomeandpathologiccorrelation[J].IntJRadiatOncolBiolPhys,2012,83(3):895⁃900.[5]AndolinoDL,JohnsonCS,MaluccioM,etal.Stereotacticbodyradiotherapyforprimaryhepatocellularcarcinoma[J].IntJRadiatOncolBiolPhys,2011,81(4):e447⁃e453.[6]KwonJH,BaeSH,KimJY,etal.Long⁃termeffectofstereotacticbodyradiationtherapyforprimaryhepatocellularcarcinomaineligibleforlocalablationtherapyorsurgicalresection.Stereotacticradiotherapyforlivercancer[J].BMCCancer,2010,10:475.[7]LoCH,HuangWY,LeeMS,etal.Stereotacticablativeradiotherapyforunresectablehepatocellularcarcinomapatientswhofailedorwereunsuitablefortransarterialchemoembolization[J].EurJGastroenterolHepatol,2014,26(3):345⁃352.[8]JangWI,KimMS,BaeSH,etal.High⁃dosestereotacticbodyradiotherapycorrelatesincreasedlocalcontrolandoverallsurvivalinpatientswithinoperablehepatocellularcarcinoma[J].RadiatOncol,2013,8:250.[9]SanukiN,TakedaA,OkuY,etal.Stereotacticbodyradiotherapyforsmallhepatocellularcarcinoma:aretrospectiveoutcomeanalysisin185patients[J].ActaOncol,2014,53(3):399⁃404.[10]BibaultJE,DewasS,Vautravers⁃DewasC,etal.Stereotacticbodyradiationtherapyforhepatocellularcarcinoma:prognosticfactorsoflocalcontrol,overallsurvival,andtoxicity[J].PLoSOne,2013,8(10):e77472.[11]HuangWY,JenYM,LeeMS,etal.Stereotacticbodyradiationtherapyinrecurrenthepatocellularcarcinoma[J].IntJRadiatOncolBiolPhys,2012,84(2):355⁃361.[12]YoonSM,LimYS,ParkMJ,etal.Stereotacticbodyradiationtherapyasanalternativetreatmentforsmallhepatocellularcarcinoma[J].PLoSOne,2013,8(11):e79854.[13]ParkJH,YoonSM,LimYS,etal.Two⁃weekscheduleofhypofractionatedradiotherapyasalocalsalvagetreatmentforsmallhepatocellularcarcinoma[J].JGastroenterolHepatol,2013,28(10):1638⁃1642.[14]FacciutoME,SinghMK,RochonC,etal.Stereotacticbodyradiationtherapyinhepatocellularcarcinomaandcirrhosis:evaluationofradiologicalandpathologicalresponse[J].JSurgOncol,2012,105(7):692⁃698.[15]IbarraRA,RojasD,SnyderL,etal.Multicenterresultsofstereotacticbodyradiotherapy(SBRT)fornon⁃resectableprimarylivertumors[J].ActaOncol,2012,51(5):575⁃583.[16]TakedaA,SanukiN,EriguchiT,etal.Stereotacticablativebodyradiotherapyforpreviouslyuntreatedsolitaryhepatocellularcarcinoma[J].JGastroenterolHepatol,2014,29(2):372⁃379.[17]PriceTR,PerkinsSM,SandrasegaranK,etal.Evaluationofresponseafterstereotacticbodyradiotherapyforhepatocellularcarcinoma[J].Cancer,2012,118(12):3191⁃3198.[18]SawrieSM,FiveashJB,CaudellJJ.Stereotacticbodyradiationtherapyforlivermetastasesandprimaryhepatocellularcarcinoma:normaltissuetolerancesandtoxicity[J].CancerControl,2010,17(2):111⁃119.[19]HowellsCC,StinauerMA,DiotQ,etal.Normallivertissuedensitydoseresponseinpatientstreatedwithstereotacticbodyradiationtherapyforlivermetastases[J].IntJRadiatOncolBiolPhys,2012,84(3):e441⁃e446.[20]OlsenCC,WelshJ,KavanaghBD,etal.Microscopicandmacroscopictumorandparenchymaleffectsofliverstereotacticbodyradiotherapy[J].IntJRadiatOncolBiolPhys,2009,73(5):1414⁃1424.(收稿日期:2015⁃05⁃03)DOI:10.3760/cma.j.issn.0253⁃3766.2015.09.005作者单位:210009南京,江苏省肿瘤医院介入科通信作者:陈世晞,Email:chenshixi2007@126.com中国原发性肝癌介入治疗的现状与展望陈世晞ʌ主题词ɔ㊀癌,肝细胞;㊀化疗栓塞;㊀射频消融;㊀索拉菲尼;㊀p53基因ʌSubjectwordsɔ㊀Carcinoma,hepatocellular;㊀Chemoembolization;㊀Radiofrequencyablation;㊀Sorafenib;㊀p53gene㊀㊀从传统意义上讲,原发性肝癌的介入治疗大致可分为经血管的化疗栓塞术和非血管的经皮穿刺肿瘤消融术㊂中国的肝癌介入治疗已经历了20余年的发展历程㊂2011年,中国‘原发性肝癌诊疗规范“已将介入治疗列为无法手术切除肝细胞癌(hepatocellularcarcinoma,HCC)患者最常用的主要治疗方法,但从实质上看,肝癌的介入治疗尚未能超出姑息治疗的范畴㊂近年来的分子生物学研究表明,肝癌不仅是局部病变,更是全身性疾病㊂因此,除消灭肿瘤本身外,还需要想方设法去调变肿瘤,而机体和微环境具有强大的调变肿瘤的潜在能力㊂要提高肝癌治疗的总体疗效,必须依赖于综合治疗,这已成为业界的共识㊂介入治疗在肿瘤多学科治疗中的地位,也集中体现在原发性肝癌的综合治疗中㊂一㊁经肝动脉化疗栓塞术(transcatheterarterialchemoembolization,TACE)TACE是将栓塞物质(明胶海绵或者微球)与混于碘油中的化疗药物一起,经选择性动脉给药治疗肝癌的技术㊂20世纪80年代中后期,TACE开始用于中国HCC的治疗㊂早期阶段,TACE并不是一线的治疗选择㊂1995年,TheNewEnglandJournalofMedicine发表的一篇文章报道,在无法手术的肝癌患者中,TACE治疗虽然可以抑制肿瘤生长,但是也可引起急性肝功能衰竭,而且对比保守治疗并不延长肝癌患者的生存时间[1]㊂TACE的疗效因此受到广泛质疑,其应用也受到了很大冲击㊂2003年,Lancet发表的荟萃分析结果显示,TACE治疗HCC可使患者的总体生存获益,中期HCC患者的中位生存时间可延长20个月[2]㊂这项荟萃分析结果又重新奠定了TACE在不能手术切除肝癌患者治疗中的地位㊂随着介入放射学理论和技术的不断完善,以及栓塞材料和治疗技术的不断改进,TACE治疗后肝癌患者的生存率明显提高,已成为不能手术切除肝癌患者的首选治疗方案㊂迄今为止中国样本量最大的一组病例资料分析显示,TACE治疗肝癌患者的1㊁2㊁3年生存率分别为46.0%㊁11.8%和4.2%[3],低于吴孟超[4]报道的肝癌手术切除治疗的效果(1㊁3㊁5年生存率分别为62.5%㊁42.6%和27.5%),且远期疗效不甚理想㊂其主要原因可能是由于目前中国介入医师在TACE治疗的应用中,没有严格把握好适应证㊂但由于没有多中心㊁大样本的前瞻性随机对照研究结果,因此对TACE治疗方法的优势进行评价尚缺乏足够的证据㊂有学者对1978 2002年发表的随机对照研究进行系统性综述分析,比较TACE(7项研究,545例患者)与保守治疗对照(7项研究,898例患者)治疗HCC的效果,其中5项为蒽环类药物或顺铂方案为基础的TACE,2项研究结果提示,TACE治疗可使HCC患者的生存获益,1项研究确定了疗效是生存时间的独立预测指标㊂研究结果表明,中期HCC患者的自然中位生存时间约为16个月,而TACE治疗患者的中位生存时间可延长至20个月㊂上述2项提示TACE治疗可使患者生存获益的研究,分别采用蒽环类和顺铂进行TACE,均每年进行了3 4次TACE治疗[5]㊂但目前尚没有权威的荟萃分析结果能明确TACE中的最佳化疗药物和最佳复治时间㊂在最近的一项Ⅱ期临床试验中,TACE采用了含有多柔比星的缓释颗粒(又称载药微球),使接受治疗的HCC患者可以获得63%的疾病控制率㊂由于该缓释颗粒能使药物在1周内缓慢释放,因此该研究中大剂量(150mg)多柔比星给药所致的毒副。
前列腺癌诊治的几个热点问题

862 men localised CaP
randomised
Standard CFRT (64Gy/32f)
+
Escalated CFRT (74Gy/37f)
both with neo-adjuvant androgen suppression.
Endpoint of study: early toxicity
Int J Radiat Oncol Biol Phys. 2008 Jan 1;70(1):67-74.
v
What dose of external-beam radiation is high enough for prostate cancer?
1,530 men 3D-CRT
(Royal Marsden Scale) improved in both
groups from pre-androgen suppression to 6
months post-radiotherapy (p<0.001), but
bowel and sexual functioning deteriorated.
Lancet 355(9214): 1491-1498, 2000
内分泌治疗和手术治疗的联合
新辅助内分泌治疗(NHT) (术前内分泌治疗)
辅助内分泌治疗(AHT) (术后内分泌治疗)
复习有关文献后总结NHT的作用
使前列腺体积缩小 降低血清PSA值 使T2期降期,根治术后标本切缘阳性率
降低.延长T2期根治术后生化复发时间, 提高局部控制率,降低复发率,提高生存 率。 但对T3期患者,近远期疗效均不确定。
Vicini 荟萃分析了22项研究包括11297例前 列腺癌患者有关放射治疗剂量和疗效的关系
自噬及其与结直肠癌的发生和治疗

of叫tophagy觚d
chemot}Ie呷y肌d
radiothempy
are
stiU咖der debate.
【l【ey words】
Au婶ha影;colorectal rM砷las啪 mTOR激酶是氨基酸、A1’P和激素的感受器,对细胞 生长具有重要的调节作用,是自噬的负调控分子。 ②磷酸肌醇3一激酶(P13K)/AKT途径:I型P13K与 AKT相互作用抑制自噬,Ⅲ型P13K则与多种蛋白构 成复合体即Bcl-2-Beclin・1一Ⅲ型P13K一紫外线辐射抗 性相关基因(UV船dia£i伽resist卸ce一鹊sociated
own
pfoleills卸d
maintain
of-
and the subsequem recycle of ceUular products.Despite me cell
that autophagy
helps
s州v—
mecha-
al,exc鹤sive跏topha舒c绷lead to蛐tophagic
参考文献
[1]uallgc,FengP,Ku B,e£a1.Autophagic锄dtIlmom。哪ppressor黜一
ti“ty of
a
c眦in0眦肌d册lat鄂wit-l sho№ned
is
ove∞既p陀88ed in p砒ient叭rvival.
H印atog眦mntemlo盱,20lO,57(98):257粕1.
2
吲in等¨41报道结肠癌细胞在接受小剂量放疗
后可发生自噬,且自噬呈剂量依赖性,抑制自噬后,可 增加放疗细胞的死亡率,说明自噬是细胞产生放疗抵 抗的机制。5一Fu作用于结肠癌细胞株的体内外研究 证实,5-Fu本身可引起自噬和凋亡,自噬又可保护结 肠癌细胞免于凋亡,阻断自噬后细胞凋亡增加,抑制 肿瘤细胞生长的疗效提高,所以自噬是5.Fu抗瘤的 耐药机制¨5|。氯喹通过上调pH值,阻碍自噬体的 成熟而抑制自噬。氯喹作为增敏剂联合标准肿瘤治 疗方案治疗结直肠癌、肺癌、骨髓瘤等的I、Ⅱ期临床 试验正在进行中。
周疗在宫颈癌同步放化疗中的作用

周疗在宫颈癌同步放化疗中的作用唐郢;王冬;袁犁【摘要】Objective To evaluate the clinical efficacy and safety of chemotherapy weekly in the chemoradiotherapy of cervicalcancer.Methods Between Jan 2003 and Oct 2007,168 patients with stage Ⅲ B squamous cell carcinoma of the uterine cervix in Chongqing Cancer Hospital were divided into two groups randomly.The observationgroup,total 86 patients receiving radiotherapy concomitant with weekly cisplatin and taxol;the matched group,total 82 patients,receiving radiotherapy concomitant with cisplatin plus taxol every 3 weeks.There were no statistical difference in the clinical and pathological characteristics between the two groups. We compare the 5 years survival rate and side reaction of the two groups.Results The 5 years survival rate of the observation group and the matched group were respectively52.3%(45/86)and 42.7%(35/82),in which there was no significant difference (P >0.05).The response rate(CR+PR)were respectively 94.2%(81/86)and 92.7%(76/82)in the observation group and the matched group,in which there was no significant difference (P >0.05).Grade Ⅲ acute gastrointestinal toxicities (nausea and vomi-ting)in the matched group were exactly higher than that in the observation group [19.5%(16/82)vs.8.1% (7/86),P <0.05]. Moreover,Grade Ⅲ myelosuppression in the matched group were exactly higher than that in the observation group [20.7%(17/82) vs.9.3% (8/86),P <0.05].there were no significant difference of theincidence of the radiocystitis,radiation proctitis and radio-dermatitis between the two groups.But the Radiotherapy completion time in the matched group were exactly longer than that in the observation group [(61.12±6.71)days vs.(54.72±4.76)days,P <0.05].Conclusion The toxicity of the observation group was lower than the matched group.Moreover the efficacy of observation group is similar to the matched group.%目的:评价周疗在宫颈鳞癌同步放化疗中的作用。
原发性宫颈印戒细胞癌一例
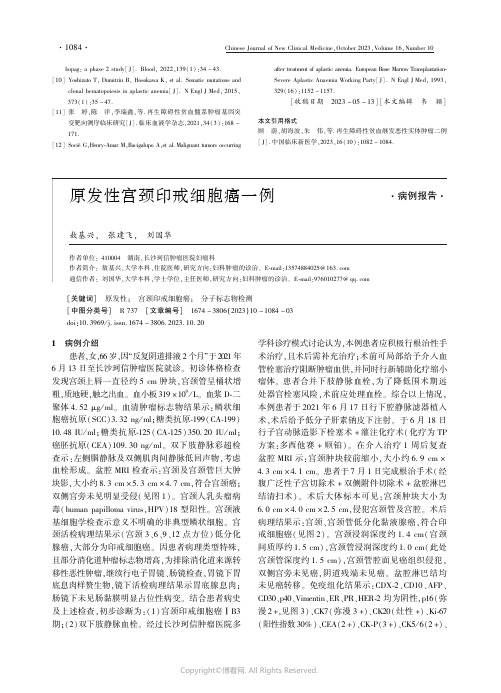
bopag:aphase2study[J].Blood,2022,139(1):34-43.[10]YoshizatoT,DumitriuB,HosokawaK,etal.Somaticmutationsandclonalhematopoiesisinaplasticanemia[J].NEnglJMed,2015,373(1):35-47.[11]张㊀婷,陈㊀洋,李瑞鑫,等.再生障碍性贫血髓系肿瘤基因突变靶向测序临床研究[J].临床血液学杂志,2021,34(3):168-171.[12]SociéG,Henry⁃AmarM,BacigalupoA,etal.Malignanttumorsoccurringaftertreatmentofaplasticanemia.EuropeanBoneMarrowTransplantation⁃SevereAplasticAnaemiaWorkingParty[J].NEnglJMed,1993,329(16):1152-1157.[收稿日期㊀2023-05-13][本文编辑㊀韦㊀颖]本文引用格式顾㊀蔚,胡海波,朱㊀伟,等.再生障碍性贫血继发恶性实体肿瘤二例[J].中国临床新医学,2023,16(10):1082-1084.㊀㊀[关键词]㊀原发性;㊀宫颈印戒细胞癌;㊀分子标志物检测㊀㊀[中图分类号]㊀R737㊀[文章编号]㊀1674-3806(2023)10-1084-03㊀㊀doi:10.3969/j.issn.1674-3806.2023.10.201 病例介绍患者,女,66岁,因 反复阴道排液2个月 于2021年6月13日至长沙珂信肿瘤医院就诊㊂初诊体格检查发现宫颈上唇一直径约5cm肿块,宫颈管呈桶状增粗,质地硬,触之出血㊂血小板319ˑ109/L㊂血浆D⁃二聚体4 52μg/ml㊂血清肿瘤标志物结果示:鳞状细胞癌抗原(SCC)3 32ng/ml;糖类抗原⁃199(CA⁃199)10 48IU/ml;糖类抗原⁃125(CA⁃125)350 20IU/ml;癌胚抗原(CEA)109 30ng/ml㊂双下肢静脉彩超检查示:左侧腘静脉及双侧肌肉间静脉低回声物,考虑血栓形成㊂盆腔MRI检查示:宫颈及宫颈管巨大肿块影,大小约8 3cmˑ5 3cmˑ4 7cm,符合宫颈癌;双侧宫旁未见明显受侵(见图1)㊂宫颈人乳头瘤病毒(humanpapillomavirus,HPV)18型阳性㊂宫颈液基细胞学检查示意义不明确的非典型鳞状细胞㊂宫颈活检病理结果示(宫颈3㊁6㊁9㊁12点方位)低分化腺癌,大部分为印戒细胞癌㊂因患者病理类型特殊,且部分消化道肿瘤标志物增高,为排除消化道来源转移性恶性肿瘤,继续行电子胃镜㊁肠镜检查,胃镜下胃底息肉样赘生物,镜下活检病理结果示胃底腺息肉;肠镜下未见肠黏膜明显占位性病变㊂结合患者病史及上述检查,初步诊断为:(1)宫颈印戒细胞癌ⅠB3期;(2)双下肢静脉血栓㊂经过长沙珂信肿瘤医院多学科诊疗模式讨论认为,本例患者应积极行根治性手术治疗,且术后需补充治疗;术前可局部给予介入血管栓塞治疗阻断肿瘤血供,并同时行新辅助化疗缩小瘤体㊂患者合并下肢静脉血栓,为了降低围术期远处器官栓塞风险,术前应处理血栓㊂综合以上情况,本例患者于2021年6月17日行下腔静脉滤器植入术,术后给予低分子肝素钠皮下注射㊂于6月18日行子宫动脉造影下栓塞术+灌注化疗术(化疗为TP方案:多西他赛+顺铂)㊂在介入治疗1周后复查盆腔MRI示:宫颈肿块较前缩小,大小约6 9cmˑ4 3cmˑ4 1cm㊂患者于7月1日完成根治手术(经腹广泛性子宫切除术+双侧附件切除术+盆腔淋巴结清扫术)㊂术后大体标本可见:宫颈肿块大小为6 0cmˑ4 0cmˑ2 5cm,侵犯宫颈管及宫腔㊂术后病理结果示:宫颈㊁宫颈管低分化黏液腺癌,符合印戒细胞癌(见图2)㊂宫颈浸润深度约1 4cm(宫颈间质厚约1 5cm),宫颈管浸润深度约1 0cm(此处宫颈管深度约1 5cm),宫颈管腔面见癌组织侵犯,双侧宫旁未见癌,阴道残端未见癌㊂盆腔淋巴结均未见癌转移㊂免疫组化结果示:CDX⁃2㊁CD10㊁AFP㊁CD30㊁p40㊁Vimentin㊁ER㊁PR㊁HER⁃2均为阴性,p16(弥漫2+,见图3)㊁CK7(弥漫3+)㊁CK20(灶性+)㊁Ki⁃67(阳性指数30%)㊁CEA(2+)㊁CK⁃P(3+)㊁CK5/6(2+)㊁㊃4801㊃ChineseJournalofNewClinicalMedicine,October2023,Volume16,Number10㊀㊀p53(灶5%+)㊂四项错配修复(mismatchrepair,MMR)蛋白:MSH2(+)㊁MSH6(+)㊁MLH1(+)㊁PMS2(+),提示pMMR状态(微卫星稳定状态)㊂综上,患者术后明确诊断为宫颈低分化印戒细胞癌ⅠB3期㊂患者术后接受了1周期TC方案(多西他赛+卡铂)全身静脉化疗,拟定补充盆腔外照射放疗[临床靶体积(CTV)包括:阴道残端㊁部分阴道㊁阴道旁组织㊁原宫旁及盆腔淋巴引流区,上界L4上缘,下界双侧闭孔下缘,95%计划靶体积(PTV),46Gy:2Gy/23F]㊂患者于2021年10月18日开始放疗,由于放疗过程中反复出现 尿频㊁尿急㊁尿痛 等副反应,患者拒绝继续放疗,因此实际仅执行5次放疗,未能完成全部照射计划㊂结束治疗后患者于长沙珂信肿瘤医院规律完成复查及随访,目前生化检查及影像学资料仍无疾病进展及复发证据㊂自患者初诊至2023年4月,总随访生存时间为22个月㊂㊀图1㊀患者宫颈肿块在盆腔MRI的影像学所见图2㊀患者术后组织病理学印戒细胞癌表现图(HEˑ50)图3㊀患者p16蛋白的免疫组化染色图(HEˑ50)2㊀讨论2 1㊀宫颈癌是我国最常见的女性生殖系统恶性肿瘤之一㊂在组织病理类型上,宫颈鳞癌最为常见且预后最好,约占80%;宫颈腺癌虽仅占15% 20%,但其恶性程度高,且近年来发生率呈上升趋势[1]㊂2014年世界卫生组织将宫颈黏液性腺癌分为胃型㊁肠型及印戒细胞型3种类型,其中以原发性宫颈印戒细胞癌(primarycervicalsignet⁃ringcellcarcinoma,PCSRCC)这类型最为罕见[2⁃3]㊂印戒细胞癌常见于消化道恶性肿瘤(比如胃癌),其余部位多为转移瘤㊂也有报道自肺癌㊁乳腺癌㊁阑尾癌㊁胆管癌或卵巢癌转移[4],而PCSRCC罕见[5⁃6]㊂自1990年报道PCSRCC以来[5],目前国内外已发表的文献较少,缺乏对PCSRCC的诊断及治疗经验㊂2 2㊀病理学诊断是宫颈印戒细胞癌诊断的金标准㊂绝大部分宫颈癌患者的症状为不规则阴道流血或性交后阴道流血,其主要病理类型为鳞癌㊂除上述症状外,部分宫颈腺癌患者还可出现不规则阴道排液㊂在已报道文献中,有2例主诉为 异常阴道排液 [7⁃8]㊂本例患者主诉 不规则阴道排液2个月 就诊,符合既往文献的报道㊂除此之外,PCSRCC患者在体格检查㊁实验室检验及MRI㊁CT等影像学检查等方面,与其他病理类型的宫颈癌患者比较并无特异性差异,增加了PCSRCC诊断的难度㊂2 3㊀基于病理诊断的结果,宫颈发现的印戒细胞癌必须与其他部位来源的转移瘤相鉴别[3],除了采用内镜手段排除胃肠道原发肿瘤之外(如本例患者),检测HPV的感染和生物标记蛋白的表达可为PCSRCC的鉴别诊断提供依据[7]㊂HPV16型和18型感染与宫颈癌发生最为密切[9],以往文献报道中,大部分PCSRCC患者为HPV18型阳性[4,7,9⁃11]㊂本例患者亦为HPV18型阳性,推测HPV18型感染可能与PCSRCC的发病及进展密切相关,但还需更多样本量研究证实㊂通过免疫组化检测生物标记蛋白表达量在分子层面为PCSRCC的鉴别诊断提供了重要依据㊂文献提示p16可作为一个重要的诊断标志物[7]㊂本例患者p16表达阳性且范围弥漫,阳性程度高㊂本例患者CK20为阳性表达,ER及PR为阴性表达,与文献[4,11⁃13]报道相符合㊂有文献指出CDX⁃2在PCSRCC中为阳性表达[8,13],而本例患者CDX⁃2为阴性㊂本例患者的CK7为阳性表达,有文献指出胃转移及乳腺转移的宫颈印戒细胞癌中CK7亦为阳性表达[7],故CK7无法作为鉴别肿瘤来源的分子标志物㊂本例检测了MMR标志物(MSH2㊁MSH6㊁MLH1㊁PMS2),因PCSRCC尚无有效的治疗方案,检查微卫星稳定状态㊁PDL1表达量㊁MMR标志物及肿瘤突变负荷等基因检测十分重要,为PCSRCC患者提供可能的免疫治疗选择㊂2 4㊀PCSRCC总体预后较差,从现有报道文献来看,预后与患者国际妇产科学联合(InternationalFederationofGynecologyandObstetrics,FIGO)分期相关[14]㊂PCSRCC的治疗主要依据鳞癌㊁腺癌㊁腺鳞癌3种病理类型的方案推荐[1]㊂文献显示,晚期患者疾病进展迅速,3例㊃5801㊃㊀㊀中国临床新医学㊀2023年㊀10月㊀第16卷㊀第10期Ⅳ期患者生存期均不到3个月[10⁃11],其中1例确诊后7周内死亡[11]㊂1例ⅢC期患者在接受姑息化疗后随访生存期超过半年[15]㊂大部分早期患者都接受了手术治疗,其中3例ⅠB期患者仅接受手术并未补充放化疗[9,11,16],仅接受手术的1例患者随访期内生存时间达25个月[16]㊂有2例ⅠB期患者接受了手术,术后辅助同步放化疗,生存期超过8年(其中1例生存期长达10年)[13,17]㊂本例患者FIGO分期为ⅠB期,手术前给予介入治疗及新辅助化疗以缩小瘤体,术后计划补充同步放化疗,但由于患者无法耐受未能完成所有巩固治疗计划,截至2023年4月,随访期内生存时间达22个月㊂2 5㊀PCSRCC的恶性程度高,预后差㊂由于病例较少,治疗手段和方案尚未形成专家共识㊂通过不断累积的案例报道,笔者认为通过HPV感染状态㊁分子标志物检测等手段,可为PCSRCC的诊断及鉴别诊断提供有力的依据㊂参考文献[1]彭巧华,吕卫国.2022年第1版‘NCCN子宫颈癌临床实践指南“解读[J].实用肿瘤杂志,2022,37(3):205-214.[2]赵东奇,李㊀淼,朱继红,等.原发性宫颈印戒细胞癌1例报告[J].西南国防医药,2021,31(2):181-182.[3]LazharH,SlaouiA,RostoumS,etal.Primarysignetringcellcarci⁃nomaofthecervix:aboutanuncommoncasereport[J].IntJSurgCaseRep,2023,105:107950.[4]WashimiK,YokoseT,NoguchiA,etal.Diagnosisofprimarypuresignet⁃ringcellcarcinomaofthecervix[J].PatholInt,2015,65(7):393-395.[5]MollUM,ChumasJC,MannWJ,etal.Primarysignetringcellcar⁃cinomaoftheuterinecervix[J].NYStateJMed,1990,90(11):559-560.[6]CardosiRJ,ReedyMB,VanNagellJR,etal.Neuroendocrinesignetringcelladenocarcinomaoftheendocervix[J].IntJGynecolCancer,1999,9(5):433-437.[7]GiordanoG,PizziS,BerrettaR,etal.Anewcaseofprimarysignet⁃ringcellcarcinomaofthecervixwithprominentendometrialandmyo⁃metrialinvolvement:immunohistochemicalandmolecularstudiesandreviewoftheliterature[J].WorldJSurgOncol,2012,10:7.[8]Su rez⁃PeñarandaJM,AbdulkaderI,Barón⁃DuarteFJ,etal.Signet⁃ringcellcarcinomapresentingintheuterinecervix:reportofaprimaryand2metastaticcases[J].IntJGynecolPathol,2007,26(3):254-258.[9]BalciS,SaglamA,UsubutunA.Primarysignet⁃ringcellcarcinomaofthecervix:casereportandreviewoftheliterature[J].IntJGynecolPathol,2010,29(2):181-184.[10]CracchioloB,KuhnT,HellerD.Primarysignetringcelladenocar⁃cinomaoftheuterinecervix arareneoplasmthatraisestheques⁃tionofmetastasistothecervix[J].GynecolOncolRep,2016,16:9-10.[11]SalV,KahramanogluI,TuranH,etal.Primarysignetringcellcarci⁃nomaofthecervix:acasereportandreviewoftheliterature[J].IntJSurgCaseRep,2016,21:1-5.[12]VerasE,SrodonM,NeijstromES,etal.MetastaticHPV⁃relatedcer⁃vicaladenocarcinomaspresentingwiththromboembolicevents(trous⁃seausyndrome):clinicopathologiccharacteristicsof2cases[J].IntJGynecolPathol,2009,28(2):134-139.[13]InsabatoL,SimonettiS,DeCecioR,etal.Primarysignet⁃ringcellcarcinomaoftheuterinecervixwithlongtermfollow⁃up:casereport[J].EurJGynaecolOncol,2007,28(5):411-414.[14]PurwotoG,NuryantoKH,WibowoTA,etal.Couldcombinationofradicalhysterectomyandradiationeffectiveinthetreatmentofpri⁃marycervicalsignetringcellcarcinoma?:ararecasereport[J].IntJSurgCaseRep,2022,94:107083.[15]MoritaniS,IchiharaS,KushimaR,etal.CombinedsignetringcellandglassycellcarcinomaoftheuterinecervixarisinginayoungJapanesewoman:acasereportwithimmunohistochemicalandhistochemicalanalyses[J].PatholInt,2004,54(10):787-792.[16]MayorgaM,García⁃ValtuilleA,Fern ndezF,etal.Adenocarcinomaoftheuterinecervixwithmassivesignet⁃ringcelldifferentiation[J].IntJSurgPathol,1997,5(3⁃4):95-100.[17]LoweryWJ,DifurioMJ,SundborgMJ,etal.Cervicalsignet⁃ringcellcarcinomapresentingasasynchronousprimarycarcinomawithuterineadenocarcinoma[J].MilMed,2009,174(2):212-213.[收稿日期㊀2023-07-29][本文编辑㊀韦㊀颖]本文引用格式敖基兴,张建飞,刘国华.原发性宫颈印戒细胞癌一例[J].中国临床新医学,2023,16(10):1084-1086.㊃6801㊃ChineseJournalofNewClinicalMedicine,October2023,Volume16,Number10㊀㊀。
国家药审中心发布《注册分类4、5.2类化学仿制药(口服固体制剂)生物等效性研究批次样品批量的一般要求

中国医药生物技术2018年10月第13卷第5期Chin Med Biotechnol, October 2018, V ol. 13, No. 5 451activated by angiogenic signals and is essential for capillary tube formation. Blood, 2001, 97(3):652-659.[28]Pasqualini R, Koivunen E, Kain R, et al. Aminopeptidase N is areceptor for tumor-homing peptides and a target for inhibiting angiogenesis. Cancer Res, 2000, 60(3):722-727.[29]Gao JJ, Xue X, Gao ZH, et al. LYP, a bestatin dimethylaminoethylester, inhibited cancer angiogenesis both in vitro, and in vivo.Microvasc Res, 2011, 82(2):122-130.[30]Li S, Wang F, Wang XY, et al. Effect of ubenimex combined withradiotherapy or chemotherapy on immune functions of malignant tumors: a meta-analysis. Pharma J Chin PLA, 2016, 32(5):462-465, 479. (in Chinese)李莎, 王芳, 王晓燕, 等. 乌苯美司联合放化疗对恶性肿瘤患者免疫功能影响的Meta分析. 解放军药学学报, 2016, 32(5):462-465, 479.[31]Meng H, Sun X, Nian JY, et al. Ubenimex combined withchemotherapy in the treatment of malignant tumor: a systematic review. China Pharm, 2017, 28(24):3387-3390. (in Chinese)孟慧, 孙旭, 念家云, 等. 乌苯美司联合化疗用于恶性肿瘤的系统评价. 中国药房, 2017, 28(24):3387-3390.[32]Shibuya K, Hayashi E, Abe F, et al. Enhancement of interleukin 1 andinterleukin 2 releases by ubenimex. J Antibiot (Tokyo), 1987, 40(3): 363-369.[33]Lkhagvaa B, Tani K, Sato K, et al. Bestatin, an inhibitor foraminopeptidases, modulates the production of cytokines and chemokinesby activated monocytes and macrophages. Cytokine, 2008, 44(3):386- 391.[34]Lv J, Zou L, Zhao L, et al. Leukotriene B4-leukotriene B4 receptoraxis promotes oxazolone-induced contact dermatitis by directing skin homing of neutrophils and CD8+ T cells. Immunology, 2015, 146(1):50-58.[35]Yamashita M, Wada H, Eguchi H, et al. A CD13 inhibitor, ubenimex,synergistically enhances the effects of anticancer drugs in hepatocellular carcinoma. Int J Oncol, 2016, 49(1):89-98.[36]Li W, Yao ZQ, Liu ZQ, et al. Clinical effect of ubenimex capsulescombined with SOX chemotherapy on treatment of advanced gastric cancer. Prog Mod Biomed, 2017, 17(23):4495-4497, 4470. (in Chinese)李炜, 姚忠强, 柳仲秋, 等. 乌苯美司胶囊联合SOX化疗对晚期胃癌患者的临床疗效研究. 现代生物医学进展, 2017, 17(23):4495- 4497, 4470.[37]Hirano T, Kizaki M, Kato K, et al. Enhancement of sensitivity bybestatin of acute promyelocytic leukemia NB4 cells to all- trans, retinoic acid. Leuk Res, 2002, 26(12):1097-1103.[38]Cao BS, Ji LY, Wang HX, et al. Effect of ubenimex, a CD13 inhibitor,on the chemosensitivity of A549 cells to cisplatin. Chin J Clin Oncol, 2012, 39(22):1778-1782. (in Chinese)曹宝山, 姬利延, 王荟霞, 等. CD13抑制剂乌苯美司对A549细胞顺铂敏感性的影响及其机制. 中国肿瘤临床, 2012, 39(22):1778- 1782.·信息站点·国家药审中心发布《注册分类4、5.2类化学仿制药(口服固体制剂)生物等效性研究批次样品批量的一般要求(试行)》为贯彻中共中央办公厅、国务院办公厅《关于深化审评审批制度改革鼓励药品医疗器械创新的意见》(厅字〔2017〕42 号)、国务院办公厅《关于改革完善仿制药供应保障及使用政策的意见》(国办发〔2018〕20 号)精神,促进仿制药研发,完善仿制药注册申请的技术标准,保证商业化生产批次样品与生物等效性研究批次样品质量与疗效的一致性,国家药审中心起草制定了《注册分类4、5.2 类化学仿制药(口服固体制剂)生物等效性研究批次样品批量的一般要求(试行)》,予以发布。
SCCA、NSE、CEA 联合检测对肺癌的诊断价值

SCCA、NSE、CEA 联合检测对肺癌的诊断价值王晓成;胡卫盟;徐晓明;赵志国【摘要】目的:研究鳞状细胞癌相关抗原(SCCA)、神经元烯醇化酶(NSE)、癌胚抗原( CEA)联合检测对肺癌的诊断价值,对临床诊治意义进行评估。
方法选取86例肺癌患者作为研究对象(肺癌组),其中小细胞肺癌29例,腺癌28例,鳞癌29例。
选取同期60例健康体检者作为正常组,抽取患者肘静脉血,采用电化学发光免疫法( ECLIA),检测患者血清中SCCA、CEA和NSE水平,对2组患者上述指标进行比较,对各组织类型肺癌血清肿瘤标记物的水平和阳性检测结果进行分析,并对联合检测和不同分期的各肺癌组血清肿瘤标记物的阳性率进行比较。
结果肺癌患者血清中3种肿瘤标记物水平均明显高于正常对照组( P <0.05),SCCA在鳞癌患者中水平最高( P <0.05),NSE在小细胞肺癌患者中水平最高( P <0.05),CEA在腺癌患者中水平最高( P <0.05)。
SCCA+CEA在非小细胞癌组中的双阳性率高于小细胞癌组( P <0.05)。
在小细胞癌患者中,血清NSE在广泛期患者的阳性率明显高于局限期患者( P <0.05);鳞癌组中,血清SCCA在转移期(Ⅲ+Ⅳ期)患者的阳性率明显高于局限期(Ⅰ+Ⅱ期)患者( P <0.05)。
腺癌组中,血清CEA在转移期(Ⅲ+Ⅳ期)患者中的阳性率明显高于局限期(Ⅰ+Ⅱ期)患者( P <0.05)。
结论多种肿瘤标记物联合检测有助于肺癌的诊断、并能指导临床进行肺癌组织学分型以及选择最佳的治疗方案。
【期刊名称】《河北医药》【年(卷),期】2015(000)022【总页数】3页(P3393-3395)【关键词】肺肿瘤;鳞状细胞癌相关抗原;神经元烯醇化酶;癌胚抗原【作者】王晓成;胡卫盟;徐晓明;赵志国【作者单位】067000 河北省承德市中心医院检验科;067000 河北省承德市中心医院检验科;067000 河北省承德市中心医院检验科;067000 河北省承德市中心医院检验科【正文语种】中文【中图分类】R734.2作者单位: 067000 河北省承德市中心医院检验科E-mail:*********************肺癌是我国常见的一种恶性肿瘤,近年调查发现其发病率为(48.83~56.2)/10万 [1,2],病死率为(25.1~31.93)/10万[3,4],严重威胁人类健康[5]。
HPV在宫颈炎_宫颈癌前病变_宫颈癌中的检测及意义分析

[7] Liu CY,Wu MC,Chen F,et al. A Large-scale genetic association study of esophageal adenocarcinoma risk [J]. Carcinogenesis, 2010,31( 7) : 1259-1263.
[5] Yousef F,Cardwell C,Cantwell MM,et al. The incidence of esophageal cancer and high-grade dysplasia in Barrett' s esophagus: a systematic review and meta-analysis[J]. Am J Epidemiol,2008, 168( 3) : 237-249.
·4550·
医学综述 2013 年 12 月第 19 卷第 24 期 Medical Recapitulate,Dec. 2013,Vol. 19,No. 24
[2] Kawasaki H,Altieri DC,Lu CD,et al. Inhibition of apoptosis by survivin predicts shorter survival rates in colorectal cancer[J]. Cancer Res,1998,58( 22) : 5071-5074.
[8] Dvorakova K,Payne CM,Ramsey L,et al. Apoptosis resistance in Barrett's esophagus: ex vivo bioassay of live stressed tissues[J]. Am J Gastroenterol,2005,100( 2) : 424-431.
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Abstract.Altered expression of microRNAs (miRNAs) has been detected in cancer, suggesting that these small non-coding RNAs can act as oncogenes or tumor suppressor genes. In the present study, we investigated the expression of miRNA-17-5p, miRNA-18a, miRNA-20a, miRNA-92a, miRNA-146a, miRNA-146b and miRNA-155 by real-time quantitative RT-PCR in a panel of melanocyte cultures and melanoma cell lines and explored the possible role of miRNA-155 in melanoma cell proliferation and survival. The analyzed miRNAs were selected on the basis of previous studies strongly supporting their involvement in cancer development and/or progression. We found that miRNA-17-5p, miRNA-18a, miRNA-20a, and miRNA-92a were overexpressed, whereas miRNA-146a, miRNA-146b and miRNA-155 were down-regulated in the majority of melanoma cell lines with respect to melanocytes. Ectopic expression of miRNA-155 significantly inhibited proliferation in 12 of 13 melanoma cell lines with reduced levels of this miRNA and induced apoptosis in 4 out of 4 cell lines analyzed. In conclusion, our data further support the finding of altered miRNA expression in melanoma cells and establish for the first time that miRNA-155 is a negative regulator of melanoma cell proliferation and survival.IntroductionMicroRNAs (miRNAs) are a class of small (~22-nt) non-coding RNAs, which play an important role in the negative regulation of gene expression (reviewed in refs. 1-5). They are present in plant and animal cells and are involved in numerous cellular processes, including apoptosis, proliferation, differentiation and metabolism (1-5).Genes coding for miRNAs (microRNA genes, miRs) are transcribed into primary transcripts, which are sequentially processed by the RNase III endonucleases Drosha and Dicer to release double-stranded, ~22-nt long fragments (reviewed in ref. 6). One strand of the miRNA duplex is subsequently incorporated into a ribonucleoprotein complex termed miRNA-induced silencing complex. In animal cells, single-stranded miRNAs bind to specific target mRNAs through partially complementary sequences, usually in the 3' untranslated region, and direct the miRNA-induced silencing complex to down-regulate gene expression by mRNA translational repression, which is frequently associated with mRNA decay (6).There is increasing evidence that miRs can be aberrantlyexpressed in cancer, suggesting that they may play a role as a novel class of oncogenes or tumor suppressor genes (reviewedin refs. 7-10). However, only a limited number of investigations have addressed the role of miRNA de-regulation in melanoma onset and progression (11-22).In the present study, we first used a sensitive real-time quantitative reverse transcription-PCR (qRT-PCR) assay toAltered expression of selected microRNAs in melanoma:Antiproliferative and proapoptotic activity of miRNA-155LAURETTA LEVATI1, ESTER ALVINO2, ELENA PAGANI1, DIEGO ARCELLI1, PATRIZIA CAPORASO1, SERGIO BONDANZA3, GIANPIERO DI LEVA4, MANUELA FERRACIN5, STEFANO VOLINIA4,6, ENZO BONMASSAR2,7, CARLO MARIA CROCE4and STEFANIA D'ATRI11Laboratory of Molecular Oncology, Istituto Dermopatico dell'Immacolata-IRCCS, Via dei Monti di Creta 104, I-00167 Rome;2Department of Medicine, Institute of Neurobiology and Molecular Medicine, National Council of Research, Via Fosso del Cavaliere 100, I-00133 Rome; 3Laboratory of Tissue Engineering and Cutaneous Physiopathology, Istituto Dermopatico dell'Immacolata-IRCCS, Via dei Monti di Creta 104, I-00167 Rome, Italy;4Department of Molecular Virology, Immunology and Medical Genetics and Comprehensive Cancer Center, Ohio State University, 460 West 12th Avenue, Columbus, OH 43210, USA; 5Department of Experimental and Diagnostic Medicine and Interdepartment Center for Cancer Research, University of Ferrara, Via Luigi Borsari 46;6DAMA, Data Mining for Microarray Analysis, Department of Morphology and Embryology, University of Ferrara, Via Fossato di Mortara 64/b, I-44100 Ferrara; 7Department of Neuroscience, School of Medicine,University of Rome ‘Tor Vergata’, Via Montpellier 1, I-00133 Rome, ItalyReceived February 24, 2009; Accepted April 29, 2009DOI: 10.3892/ijo_00000352_________________________________________Correspondence to:Dr Stefania D'Atri, Laboratory of MolecularOncology, Istituto Dermopatico dell'Immacolata-IRCCS, Via deiMonti di Creta 104, I-00167 Rome, ItalyE-mail: s.datri@idi.itKey words:microRNA, microRNA-155, melanoma, proliferation,apoptosisevaluate, in a panel of melanoma cell lines and normal melanocytes, the expression levels of seven miRNAs, namely miRNA-17-5p, miRNA-18a, miRNA-20a, miRNA-92a,miRNA-146a, miRNA-146b and miRNA-155. Actually,previous studies indicated that alterations in the expression of these miRNAs may have a role in cancer development and/or progression (7-10). Thereafter we focused our attention on miRNA-155, since it resulted markedly down-regulated in the majority of melanoma cell lines. In order to establish the possible biological significance of the low miRNA-155expression in melanoma, we investigated the effects of the ectopic expression of the miRNA on in vitro melanoma cell proliferation and apoptosis. Materials and methodsCell lines and normal melanocytes . Seventeen human melanoma cell lines were used in this study and cultured as previously described (23). GR-Mel and PNP-Mel were derived from primary melanomas, whereas the other cell lines were originated from metastatic lesions.Human melanocytes were isolated from normal skin biopsies of 10 different donors and cultured, as previously described (24).All biological material was obtained with the patient's informed consent and the study was conducted according to the Declaration of Helsinki Principles.Low molecular weight (LMW) RNA isolation and qRT-PCR analysis of miRNA expression . LMW RNA was isolated from melanocytes and melanoma cell lines using the mir Vana™miRNA isolation kit (Ambion, Austin, TX) according to the manufacturer's protocol. LMW RNA was quantified using the NanoDrop ND-1000 spectrophotometer (Thermo Fisher Scientific Inc, Waltham, MA).To evaluate the expression of U6 small nuclear RNA (snRNA) and mature miRNAs, the TaqMan®MicroRNA Reverse Transcription kit, the TaqMan Universal PCR Master Mix No AmpErase ®UNG and the TaqMan MicroRNA Assay for U6 snRNA and the selected miRNAs, all purchased from Applied Biosystems (Foster City, CA), were used. All experimental procedures were performed according to the manufacturer's protocols. One or 10 ng of LMW RNA were reverse transcribed in a final volume of 15 μl and qRT-PCR was done on an ABI PRISM 7000 Sequence Detection System (Applied Biosystems) in a final volume of 20 μl. All qRT-PCR reactions were run in duplicate. The expression of the miRNAs under investigation relative to miRNA-16 was determined using the formula 2-ΔC T , where ΔC T = (C TmiRNA - C TmiRNA-16) and C T (i.e. threshold cycle) indicates the fractional cycle number at which the amount of amplified target reaches a fixed threshold (25).Transfection . Pre-miR hsa-miR-155 miRNA Precursor (pre-miRNA-155) and Pre-miR miRNA Precursor Negative Control #1 (dsRNA-CTRL) were obtained from Ambion.To evaluate the effect of miRNA-155 on cell growth,melanoma cells were seeded into 24-well plates (Falcon,Becton and Dickinson Labware, Franklin Lakes, NJ) and allowed to adhere at 37˚C for 18 h. The cells were thentransfected with pre-miRNA-155 or dsRNA-CTRL. Trans-fection was performed using Oligofectamine or Lipofectamine 2000 (Invitrogen Corporation, Carlsbad, CA) in serum-free medium, according to the manufacturer's protocol. Additional controls consisted in melanoma cells left untreated or exposed to the transfection reagent only (mock-transfected cells). Three replica wells were used for each group. After 72 h of culture,the cells were subjected to a second transfection. Seventy-two hours later, the cells were harvested by trypsinization and cell growth was evaluated in terms of viable cell count.Transfection efficiency was evaluated using a fluorescein-labeled double-stranded RNA oligomer designated BLOCK-iT™fluorescent oligonucleotide (Invitrogen).Evaluation of apoptosis . Melanoma cells were plated in duplicate in 24-well plates and transfected with 100 nM pre-miRNA-155 or dsRNA-CTRL, as described above. Forty-eight hours after a single transfection procedure, apoptotic death was evaluated using the Cell Death Detection ELISA PLUS kit (Roche Diagnostics GmbH, Mannheim, Germany), according to the manufacturer's protocols. This kit allows the quantitative determination of mono- and oligonucleosomes that accumulate in the cytoplasm of cells undergoing apoptosis before plasma membrane breakdown. Signals were determined in a Microplate Reader 3550-UV (Bio-Rad, Hercules, CA). Data were expressed in terms of ‘Enrichment Factor’, calculated as the ratio between the adsorbance values of pre-miRNA-155-transfected cells and those of dsRNA-CTRL-transfected cells.Statistical analysis of qRT-PCR data . We performed two different statistical analyses to assess the significance of the differences in miRNA expression within a class of samples and between classes of samples.The statistical differences within a class of samples were determined using a customized script employing Bioconductor packages () and based on the R language (). In particular, we used ‘Permtest’ and ‘BootPR’ R-packages to perform t-test in conjunction with bootstrap analysis in order to determine which gene between U6 snRNA and miRNA-16 had the lowest variability among melanocytes. Fifty-thousand permutations were applied to the test in order to define the confidence limits and the corresponding significance thresholds. The statistical significance of the differential expression of U6 snRNA or miRNA-16 among the melanocytes was assessed by computing a P-value for each 2-CT value. No specific parametric form was assumed for the distribution of the test statistics. To determine the P-value, we used a permutation procedure in which the expression value of U6 snRNA or miRNA-16 was permuted 500,000 times, and for each permutation, two-sample t-statistics were computed for each value. The permutation P-value for a particular value is the proportion of the permutations (out of 500,000) in which the permuted test statistic exceeds the observed test statistic in absolute values.The same statistical analysis was applied to assess variability of miRNA-16 expression within the group of melanoma cell lines.The statistical significance of the differences in miRNA expression between melanoma cell lines and melanocytes was assessed by Student's t-test analysis performed on 2-ΔCT values.ResultsSelection of the internal control gene for the evaluation of miRNA expression by qRT-PCR. Previous studies showed that melanin inhibits RT-PCR (26). Therefore, to reduce melanin contamination and to enrich the miRNA content, we used column purified LMW RNA for qRT-PCR. U6 snRNA and miRNA-16 have been previously used as internal control genes to determine the relative expression of a large number of miRNAs in cell lines by qRT-PCR performed on total RNA (11,27). Therefore, preliminary experiments were carried out to select, between the two genes, the best internal control to be adopted for the present study.The first set of experiments showed that the 2-CT value of miRNA-16 was significantly higher (P<0.01 according to Student's t-test) than that of U6 snRNA in melanocytes isolated from normal skin biopsies of 10 different donors (data not shown). Moreover, t-test in conjunction with bootstrap analysis showed that variability of U6 snRNA expression among the different melanocyte samples was higher than that of miRNA-16 (i.e. P<0.01 or P<0.05 in 8 out of 10 samples in the case of U6 snRNA vs. no statistically significant variation in the case of miRNA-16, data not shown).In a subsequent set of experiments, the expression level of miRNA-16, in terms of 2-CT value, was determined in parallel in the 10 melanocyte samples and in 17 melanoma cell lines. The results of t-test in conjunction with bootstrap analysis confirmed that no significant differences existed in the expression of miRNA-16 within the group of melanocytes (Fig. 1). The same statistical analysis applied to melanoma cell lines identified three outliers (Fig. 1), indicating that de-regulation of miRNA-16 can occur in some melanomas. These 3 cell lines were then excluded from further analysis. Student's t-test analysis performed on miRNA-16 2-CT values relative to the remaining 14 melanoma cell lines and to the melanocytes showed no significant difference (Fig. 1). On these bases we selected miRNA-16 as the internal control gene for qRT-PCR assays.Expression of mature miRNAs in normal cultured melanocytes and melanoma cell lines. All qRT-PCR assays were performed using 1.33 μl of cDNA reverse transcribed from 1 ng of LMW RNA. However, the levels of miRNA-155 were found to be extremely low in melanoma cells. Therefore, the expression of this miRNA was evaluated using 1.33 μl of cDNA reverse transcribed from 10 ng of LMW RNA.As illustrated in Table I, all melanocyte samples expressed the miRNAs under investigation, being miRNA-146a the most expressed and miRNA-18a the less expressed miRNA in all samples.To identify miRNAs dysregulated in melanoma cell lines with respect to melanocytes, we performed Student's t-test analysis between the two groups (i.e. all melanoma cell lines vs. all melanocytes) and between each melanoma cell line and the group of melanocytes. When melanoma cell lines and melanocytes were compared as two groups, miRNA-17-5p, miRNA-18a, and miRNA-20a, which are encoded by the miR-17-92cluster, resulted overexpressed in the melanoma group (Table I). miRNA-92a, which is generated from the transcription of two different miRs(i.e. miR-92a-1in the miR-17-92cluster and miR-92a-2, in the miR-106a-363cluster) (reviewed in ref. 28) was also up-regulated in the melanoma group (Table I). In contrast, the expression of miRNA-146a, miRNA-146b and miRNA-155, was significantly reduced in the melanoma group with respect to that of melanocytes (Table I).When each melanoma cell line was compared with the melanocyte group, the four miRNAs encoded by the miR-17-92 cluster were up-regulated simultaneously in 9 cell lines. In contrast, miRNA-146a and miRNA-146b, were found to be concomitantly down-regulated in 10 melanomas and miRNA-155 resulted to be significantly reduced in 13 cell lines (Table I).Transfection of pre-miRNA-155 into melanoma cell lines inhibits proliferation. To investigate the biological significance of miRNA-155 down-regulation in melanoma cells, we decidedFigure 1. Expression levels of miRNA-16 in normal melanocytes and melanoma cell lines. Equal amounts (1.33 μl) of cDNA reverse transcribed from 1 ng of LMW RNA were used to determined by qRT-PCR the expression of miRNA-16 in normal skin melanocytes obtained from 10 different donors and in 17 melanoma cell lines. Data are expressed in terms of 2-CT x109. Each value represents the mean of six independent experiments, in which qRT-PCRs were run in duplicate. Bars, standard error of the mean. Among the melanoma group, three cell lines were found to be outliers (**P<0.01, according to t-test in conjunction with bootstrap analysis). The mean expression value for the melanocyte group was 155±8.13 and the mean expression value for the melanoma cell line group, not including CG-Mel, CR-Mel and MR-Mel, was 155±8.25.to assess the effect of ectopic expression of the miRNA on cell proliferation. To this end, all the melanoma cell lines were left untreated, mock-transfected or subjected to two sequential transfection procedures with 100 nM of a double-stranded RNA mimicking the endogenous precursor of miRNA-155(pre-miRNA-155) or with a double-stranded control RNA (dsRNA-CTRL). Cell growth was evaluated in terms of viable cell count 72 h after the second transfection.In preliminary experiments, the cell lines were transfected with either Oligofectamine or Lipofectamine 2000 and the BLOCK-iT™fluorescent oligonucleotide (100 nM) and assayed for transfection efficiency after 24 h. The cell lines were also subjected to two sequential transfections with the transfection reagents alone and assayed for proliferation 72 h after the second transfection. Based on the results of this set of experiments (data not shown), in 13 out of 14 cell lines we were able to select for the transfection reagent providing an acceptable transfection efficiency and minimal effects on proliferation (Table II and Fig. 2). In the remaining cell line (i.e. CT-Mel), we used Lipofectamine 2000 despite its marked inhibitory effect on cell growth because transfection efficiency with Oligofectamine was only 10%.The effects of pre-miRNA-155 transfection on melanoma cell growth are illustrated in Fig. 2. In 12 melanoma cell lines,growth inhibition induced by transfection of pre-miRNA-155was significantly higher than that observed in dsRNA-CTRL-transfected cells, with percentages of cell growth inhibition ranging between 30 and 98%. In the remaining cell lines (i.e. GR-Mel and PNM-Mel), no increase of cell growth inhibition was induced by pre-miRNA-155 transfection with respect to dsRNA-CTRL. Notably, GR-Mel, was the only cell line showing miRNA-155 levels comparable to those of melanocytes.To further assess the inhibitory activity of miRNA-155 on melanoma cell growth, a concentration-response curve was set up with CH-Mel, DR-Mel, GL-Mel and SK-Mel-28 cell lines.The results illustrated in Fig. 3 show that pre-miRNA-155,but not dsRNA-CTRL induced a concentration-dependent inhibition of cell growth.Table I. Expression of miRNAs in human normal melanocytes and melanoma cell lines.–––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––Melanoma cell lines showing Melanoma cell lines showingmiRNA Relative expression level (2-ΔCT )aup-regulation of the miRNAdown-regulation of the miRNA–––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––Melanocytes Melanoma P b No.c MC:NM Ratio d No.c MC:NM Ratio d–––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––17-5p 0.045±0.0020.132±0.020<0.0110 2.3-5.50-18a 0.016±0.0010.049±0.008<0.0110 2.1-6.40-20a 0.247±0.0100.449±0.054<0.0111 1.5-3.420.7-0.692a 0.227±0.0180.367±0.041<0.0110 1.3-3.110.5146a 2.057±0.142 1.189±0.169<0.010-100.8-0.2146b 1.770±0.1440.861±0.140<0.010-100.6-0.11550.069±0.0110.005±0.004<0.010-130.2-0.0004–––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––a The expression of miRNAs was determined by qRT-PCRs in melanocytes obtained from 10 different donors and in 14 melanoma cell lines.Values represent the mean ±standard error of the mean of the melanocyte or the melanoma group. For each melanocyte sample and melanoma cell line at least three independent experiments, in which qRT-PCRs were run in duplicate, were performed. b P, probability according to Student's t-analysis comparing miRNA expression values of melanocytes with those of melanoma cell lines.c Number of melanoma cell lines in which miRNA expression value was significantly higher or lower (P<0.05 according to Student's t-test analysis) than the mean expression value of the melanocyte group. d Range of the ratio between the mean expression value of each melanoma cell line (MC) and the mean expression value of the melanocyte group (NM).–––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––Figure 2. Ectopic expression of miRNA-155 inhibits melanoma cell growth.Melanoma cells were left untreated, mock-transfected or subjected to two sequential transfections with 100 nM pre-miRNA-155 or dsRNA-CTRL, as described under Materials and methods. Seventy-two hours after the second transfection, the cells were harvested by trypsinization and cell growth was evaluated in terms of viable cell count. Data are expressed in terms of percentage of growth inhibition of target cells transfected with pre-miRNA-155, or dsRNA-CTRL or mock-transfected with respect to the untreated cells. Each value represents the mean of at least three independent experiments performed with triplicate samples, with bars indicating standard error of the mean. **P<0.01, according to Student's t-test, comparing the percentages of cell growth inhibition of pre-miRNA-155-transfected cells with those of dsRNA-CTRL-transfected cells. Percentages were subjected to angular transformation in order to obtain normally distributed data.Thereafter, conventional standard error calculation and Student's t-test statistics were performed on converted data. However, the data are expressed in non-transformed percentages, following conversion of transformed data into the original values.Transfection of pre-miRNA-155 into melanoma cell lines induces apoptosis. To investigate whether the growth inhibitory effect of pre-miRNA-155 could be due, at least in part, to the triggering of apoptosis, experiments were performed on 4 different cell lines, that were subjected to a single transfection with 100 nM pre-miRNA-155 or dsRNA-CTRL and assayed for apoptosis 48 h later. Ectopic expression of miRNA-155 was able to induce apoptosis in all the 4 cell lines tested (Fig. 4). Moreover, apoptosis was particularly pronounced in the two cell lines in which transfection with pre-miRNA-155 was followed by strong cell growth suppression (i.e. CH-Mel and DR-Mel).DiscussionAberrant expression of the miR-17-92cluster or single components of the cluster, as well as of miR-146a, miR-146b and miR-155can have a role in tumorigenesis (7,8,10,28). To investigate whether these miRs could be deregulated in melanoma, we comparatively analyzed the expression levels of the corresponding mature miRNAs in a panel of human melanoma cell lines and cultured normal melanocytes. Notably, the qRT-PCR assays were performed on RNA preparations enriched for miRNAs, with conceivably reduced content of melanin. Moreover, the internal control gene (i.e. miRNA-16) was selected following an experimental survey of two candidate small RNA molecules largely used as reference gene transcripts. We found that miRNA-17-5p, miRNA-18a, miRNA-20a, and miRNA-92a were up-regulated, whereas miRNA-146a, miRNA-146b and miRNA-155 were down-regulated in the majority of the melanoma cell lines analyzed.We focused our attention on the biological role of miRNA-155, that was found, for the first time, to be a candidate gene able to control melanoma cell growth and survival. Indeed, we observed that enforced expression of miRNA-155 was able to inhibit proliferation and induce apoptosis in melanoma cells expressing low levels of this miRNA.In humans, miR-155resides within the BIC gene on chromosome 21 (7,8). High levels of miRNA-155 have been found in B-CLL, B-cell lymphomas, papillary tyroid carcinoma, breast cancer (7-10), pancreatic ductal adeno-carcinoma (29) and other tumors (30). Moreover, enforced expression of miRNA-155 is sufficient to trigger murine B lymphoma (7). On the other hand, miRNA-155 was reported to be expressed in healthy pancreas and essentially absent in endocrine pancreatic tumors (10). Moreover, the levels of this miRNA were found to be reduced in ovarian cancer (31). These findings suggest that miR-155can act either as oncogene or as tumor suppressor gene, depending on the cell background in which miRNA-155 is performing its specific target gene controlling function.Our results demonstrate that miRNA-155, which appears to be the most altered miRNA among those analyzed, is a negative regulator of melanoma cell growth. Actually, ectopic expression of miRNA-155 significantly inhibited proliferation in 12 out of 13 melanoma cell lines endowed with low miRNA-155 levels. In contrast, enforced expression of this miRNA did not affect the growth of GR-Mel cells, which display miRNA-155 levels comparable to those of melano-cytes. It must be noted that the transfection efficiency of GR-Mel cells was ~70-80%, thus eliminating the possibility that ineffective pre-miRNA-155 uptake might underlie the lack of response. Moreover, a concentration-dependent inhibitionTable II. Transfection efficiency and cell growth inhibition relative to the transfection reagent selected for melanoma cell lines.–––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––Transfection efficiency a Cell growth inhibition b Transfection reagent Cell line Range (%)Range (%)–––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––Oligofectamine CH-Mel80-9010-20CN-Mel80-905-10DR-Mel80-9010-20GL-Mel60-70<5WM-266-470-80<5 Lipofectamine 2000CL-Mel80-9010-20CT-Mel90-10060-70GR-Mel70-805-20M1470-8015-25PNM-Mel90-10015-20PNP-Mel80-905-15SK-Mel-2870-805-20SN-Mel80-9015-25397-Mel80-9015-25–––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––a Melanoma cells were seeded into 24-well plates, allowed to adhere at 37˚C for 18 h and then transfected with 100 nM BLOCK-iT™fluorescent oligonucleotide using Oligofectamine or Lipofectamine 2000. Transfection efficiency was evaluated 24 h after transfection using a fluorescence microscope (Axiovert 135, Zeiss, Oberkochen, Germany).b Melanoma cells were subjected to two sequential transfection procedures with the transfection reagent alone, as described in Materials and methods. Cell proliferation was evaluated 72 h after the second transfection.–––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––of cell growth was observed upon transfection of pre-miRNA-155 but not of dsRNA-CTRL, thus further supporting the specificity of the inhibitory effects of miRNA-155. Impairment of melanoma cell proliferation appears to be dependent, at least in part, on miRNA-155-mediated induction of apoptosis.Indeed, in 4 out of 4 cell lines tested ectopic expression of miRNA-155 caused significantly higher levels of apoptosis than ectopic expression of dsRNA-CTRL.Since miRNAs can regulate a large number of target genes,several algorithms have been developed to predict in silico the targets of selected miRNAs. We adopted the TargetScan (/) and PicTar (/) algorithms to identify putative miRNA-155 targets and found that 160 targets are predicted by both algorithms.Down-regulation of one or more of these target genes might be involved in miRNA-155-induced impairment of melanoma cell proliferation and survival. For instance, the MAP3K14genes code for nuclear factor-inducing kinase (NIK), which plays a central role in the activation of the non-canonical NF-κB pathway in response to a subset of NF-κB-inducing stimuli (reviewed in ref. 32). It has been shown that NIK expression and/or activity is significantly higher in melanoma cells than in normal melanocytes and that overexpression of a kinase-deficient mutant of NIK strongly reduces basal NF-κBFigure 4. Ectopic expression of miRNA-155 induces apoptosis in melanoma cells. CH-Mel, DR-Mel, SK-Mel-28 and 397-Mel cells were subjected to a single transfection procedure with 100 nM pre-miRNA-155 or dsRNA-CTRL,as described in Materials and methods. Forty-eight hours after transfection,the cytoplasmic amount of mono- and oligonucleosomes originated from apoptotic DNA degradation was quantified using an ELISA assay. Data areexpressed in terms of Enrichment Factor (EF), calculated as the ratio between the adsorbance value of pre-miRNA-155-transfected cells and that of dsRNA-CTRL-transfected cells, to which the arbitrary value of 1.0 was assigned. Each value represents the mean of at least four independent experiments. Bars, standard error of the mean. **P<0.01 and *P<0.05,according to Student's t-test, comparing the adsorbance values of pre-miRNA-155-transfected cells with those of dsRNA-CTRL-transfected cells.Figure 3. Ectopic expression of miRNA-155 induces a concentration-dependent inhibition of melanoma cell growth. CH-Mel (a), DR-Mel (b), GL-Mel (c) and SK-Mel-28 (d) cells were left untreated or subjected to two sequential transfections with the indicated concentrations of pre-miRNA-155 or dsRNA-CTRL, as describe under Materials and methods. Seventy-two hours after the second transfection, the cells were harvested by trypsinization and cell growth was evaluated in terms of viable cell count. Data are expressed in terms of percentage of growth inhibition of target cells transfected with pre-miRNA-155 or dsRNA-CTRL with respect to untreated cells. Each value represents the mean of at least three independent experiments performed with triplicate samples,with bars indicating standard error of the mean. Percentages were subjected to angular transformation in order to obtain normally distributed data. Thereafter,conventional standard error calculation was performed on converted data. However, the data are expressed in non-transformed percentages, following conversion of transformed data into the original values.。