2012 年ACS《癌症预防的营养与运动指南》解读
美国癌症学会(ACS)关于癌症预防的营养与身体活动指南推荐
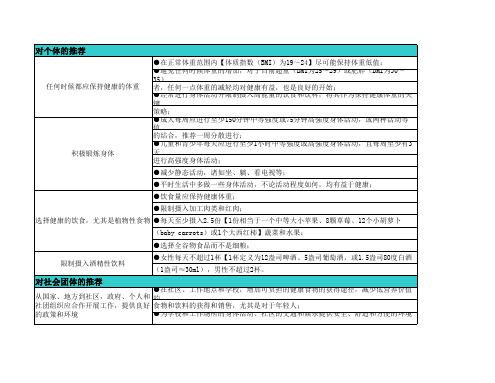
●在正常体重范围内【体质指数(BMI)为19~24】尽可能保持体重低值; ●避免任何时候体重的增加,对于目前超重(BMI为25~29)或肥胖(BMI为30~35) 任何时候都应保持健康的体重 者,任何一点体重的减轻均对健康有益,也是良好的开始; ●经常进行身体活动并限制摄入高能量的饮食和饮料,将其作为保持健康体重的关键 策略; ●成人每周应进行至少150分钟中等强度或75分钟高强度身体活动,或两种活动等值 的结合,推荐一周分散进行; 积极锻炼身体 ●儿童和青少年每天应进行至少1小时中等强度或高强度身体活动,且每周至少有3天 进行高强度身体活动; ●减少静态活动,诸如坐、躺、看电视等; ●平时生活中多做一些身体活动,不论活动程度如何,均有益于健康; ●饮食量应保持健康体重; ●限制摄入加工肉类和红肉; 选择健康的饮食,尤其是植物性食物 ●每天至少摄入2.5份【1份相当于一个中等大小苹果、8颗草莓、12个小胡萝卜 (baby carrots)或1个大西红柿】蔬菜和水果; ●选择全谷物食品而不是细粮; 限制摄入酒精性饮料 ●女性每天不超过1杯【1杯定义为12盎司啤酒、5盎司葡萄酒,或1.5盎司80度白酒 (1盎司≈30ml),男性不超过2杯。
对社会团体的推荐
从国家、地方到社区,政府、个人和 ●在社区、工作地点和学校,增加可负担的健康食物的获得途径,减少低营养价值的 社团组织应合作开展工作,提供良好 食物和饮料的获得和销售,尤其是对于年轻人; 的政策和环境
从国家、地方到社区,政府、个人和 社团组织应合作开展工作,提供良好 的政策和环境
●为学校和工作场所的身体活动、社区的交通和娱乐提供安全、舒适和方便的环境。
适量运动防癌抗癌的十大机理
适量运动防癌抗癌的十大机理作者:安然来源:《现代养生·上半月版》 2017年第11期安然运动锻炼何以能防癌抗癌?近些年来的运动医学研究、肿瘤实验研究和肿瘤病因调查等研究逐步揭示出了其中的奥妙,阐明了诸多新的机理。
1.运动锻炼能提高机体免疫功能,有利于防癌抗癌研究发现,癌细胞只有在逃脱人体免疫监视的时候才能生长和繁殖;如果一个人的免疫机制完整无缺,则任何癌症都不会发生;癌症患者如能维护与提高自身免疫功能,则能有效地抑制与战胜癌症。
研究证实,经常性地运动锻炼能有效提高自身免疫功能。
如运动可使体内T淋巴细胞、B淋巴细胞、吞噬细胞等免疫细胞明显增加,从而使机体的防癌抗癌能力增强。
运动还可使血液中的干扰素水平提高,而干扰素也是人体的免疫增强剂,有防癌抗癌的功效。
2.运动使人体吸入更多的氧气,富氧内环境有利抑制癌症运动能使人吸入比平时多几倍至几十倍的氧气。
人体吸氧量增多,呼吸频率加快,通过体内气体的频频交换,可排出更多的致癌毒素,降低癌症的发生几率;同时,癌细胞是一种厌氧细胞,它的生存、生长需要氧气不足的环境;氧气充足的体内环境,不适宜癌细胞的生长,因而更有利于抑制潜存于体内的癌症。
据德国运动医学家范·阿肯教授研究认为:“一个人每天获得氧气量比平时多8倍以上,可以预防癌症,即使得了癌症也能延长生命过程。
” 墨西哥肿瘤医师通过对100例癌症患者3年实验观察发现,每天进行2个小时氧气疗法,癌症患者的生存率可以从32%上升到88%。
3.运动促进血液循环,有利于阻止癌细胞“定居” 、“转移”运动时人体血液循环加快,此时癌细胞就好似湍流中的小沙子,不易“站住脚跟” ,因而不宜于癌细胞“定居” 形成扩散与转移;其在血流运行中,往往被免疫功能较强者的免疫细胞所消除。
4.运动可多出汗,能排出更多致癌物每次运动,都会排出比平时多得多的汗液。
通过多出汗,可使积存在体内的亚硝酸盐、丙酮、氯仿、硫、酚、锶、铅、汞和铍等致癌性毒物排出体外,避免致癌。
癌症患者的营养支持策略有哪些
癌症患者的营养支持策略有哪些癌症,这个令人闻之色变的词汇,给患者及其家庭带来了巨大的痛苦和挑战。
在与癌症的抗争中,患者的身体和心理都承受着巨大的压力,而营养支持在这个过程中起着至关重要的作用。
合理的营养支持不仅能够帮助患者维持良好的身体状态,增强抵抗力,还能提高治疗的耐受性和效果,改善生活质量。
那么,癌症患者的营养支持策略都有哪些呢?首先,我们要了解癌症患者的营养需求特点。
癌症本身以及治疗过程都会对患者的身体造成影响,导致营养需求发生改变。
癌症细胞的快速生长会消耗大量的能量和营养物质,同时治疗如化疗、放疗等可能引起恶心、呕吐、食欲不振、味觉改变、口腔溃疡等不良反应,影响患者的进食和消化吸收。
因此,癌症患者往往需要更多的蛋白质、热量、维生素和矿物质。
蛋白质是身体修复和维持正常功能所必需的营养素。
对于癌症患者来说,足够的优质蛋白质摄入尤为重要。
优质蛋白质的来源包括鱼、禽、蛋、瘦肉、豆类、奶制品等。
建议癌症患者在饮食中适当增加这些食物的比例,以满足身体对蛋白质的需求。
热量的充足供应也是关键。
由于癌症和治疗的影响,患者的身体代谢率可能会升高,消耗更多的能量。
如果热量摄入不足,患者可能会出现体重下降、身体虚弱等情况。
因此,需要根据患者的具体情况,计算出每天所需的热量,并通过合理的饮食搭配来提供。
维生素和矿物质对于维持身体的正常生理功能和免疫系统的健康也不可或缺。
例如,维生素 C、维生素 E、锌、硒等具有抗氧化作用,有助于减轻癌症治疗的副作用和增强身体的抵抗力。
富含这些营养素的食物包括新鲜的水果、蔬菜、坚果等。
在了解了癌症患者的营养需求特点后,我们来看看具体的营养支持策略。
饮食调整是基础。
尽量选择患者喜欢且易于消化吸收的食物。
食物的种类要丰富多样,以保证营养的均衡。
可以采用少食多餐的方式,增加进食的次数,减少每次进食的量,减轻胃肠道的负担。
对于食欲不振的患者,可以尝试在食物的色香味上下功夫,提高食物的吸引力。
运动抗癌的过去、现在与未来

Journal of Chengdu Sport University Vol.47No.2.2021成都体育学院学报2021年(第47卷)第2期DOI:10.15942/j.jcsu.2021.02.00l 运动抗癌的过去、现衽与未来朱为模摘要:近几十年的国内外研究,证明了运动在预防和治疗人类癌症中的积极作用。
运动在国外已经作为“协同药”进入癌症治疗的临床第一线,运动肿瘤学作为一门新兴学科也因此诞生和成长。
文章回顾了国内外运动抗癌发展史,分析了其发展现状,并对未来的研究主攻方向和实践中亟需解决的问题进行了展望与阐述。
关键词:运动是良药;运动处方;循证医学中图分类号:G804.3文献标志码:A文章编号:1001-9154(2021)02-0001-08癌症是因为异常细胞侵入其他组织,扩散至身体的其他部位并失控生长的疾病。
由于现代人不健康的生活方式(如抽烟、不运动、吃垃圾食品、压力大、肥胖等)和人口的老龄化,癌症在很多国家已经一跃成为人类的主要杀手之一。
过去得了癌症,临床医生通常是建议患者休息并避免体育锻炼或运动。
但从20世纪80年代起大量运动与癌症的研究让人们开始重新认识运动在癌症预防和治疗中的积极作用。
有关研究的数量也呈指数级增长,据统计,在过去10年中,已有数千项运动与癌症治疗的随机对照试验,多个大型流行病学和临床研究得以完成,所有这些都扩展了我们对这个领域的认知。
现在我们已经有足够科学证据来证明患有癌症的人能从运动中受益,一门新兴的癌症治疗学科即运动肿瘤学(Exercise Oncology)也应运而生。
随着研究的进一步深入,在不久的将来就可以像用药一样,精确地用运动来参与癌症的治疗和干预。
本文旨在通过对运动抗癌发展历史回顾,对未来发展的展望,以及对运动肿瘤学做的系统介绍,以期待更多的学者参与这个新学科的研究和实践,为人类战胜这个凶险的疾病共同奋斗。
1运动抗癌的过去1.1概念的提出:癌症病人创造了历史其实国外用运动来抗癌的历史并不很长。
癌症患者的临床运动指导
癌症患者的临床运动指导作者:唐玲琍来源:《中国保健营养》2019年第04期【摘 ;;;要】 ;;;早期筛查和早期诊治是某些类型癌症的医疗改进方案。
癌症治疗是个体化的,可以包括手术、放射治疗、化疗、激素治疗、靶向治疗,或者通常是这些疗法的结合。
癌症治疗通常会持续几个月甚至会持续数年。
尽管有更多的人治愈了他们的疾病,或者得到了更好的预后结果。
由于癌症或癌症的治疗,许多人经历了重大的生理和社会心理变化,这些变化会影响他们的生活质量,即对日常生活质量的感知或对整体幸福感的评估。
运动已被确定为一种干预措施,以解决治疗和其他方面的一些副作用。
运动作为一种处方药正在成为整个医学领域的常规。
许多与锻炼有关的问题:安全,生活质量,例如,肌肉和有氧健身。
或他们享受正常生活活动和一般福利的能力——已经用各种有效的量表对正在接受治疗或治疗结束后的癌症患者进行了评估。
有氧能力或有氧适应度衡量心肺系统的功能能力。
肌肉健康的结果包括力量测量,通常是上肢或下肢力量。
本指南对运动的定义来源于美国运动医学院:一种导致能量消耗增加的体育活动,包括有计划的或有组织的身体运动,在频率、强度和持续时间上系统地进行,旨在维持或增强与健康有关的结果。
【关键词】 ;;;癌症治疗;肌肉健康;生活质量;安全;锻炼【中图分类号】R197.3 ;;;【文献标识码】A ;;;【文章编号】1004-7484(2019)04-0077-02不同类型的运动和运动计划可以影响生活质量还有健身。
有氧运动影响心血管系统,主要依赖于氧气的作用。
阻力训练是力量训练,使用重量或弹性阻力带使肌肉超负荷,以提高力量和耐力。
运动项目可以有各种有氧和阻力运动的组合。
例如,频率或每周进行一种模式或类型的运动次数,可计算为每周3次有氧运动和每周2次抵抗运动。
持续时间练习的内容是每节课的锻炼分钟数,强度指在进行这项活动时所消耗的能量。
强度可以用心率、代谢当量,或在一项活动中消耗的氧气量。
家庭肠外营养指南解读完整版
家庭肠外营养指南解读完整版家庭肠外营养(HPN)是指在专业营养支持小组的指导下,让某些病情相对平稳且需要长期或较长期依赖肠外营养的特殊患者在家中实施肠外营养。
欧美国家开展HPN较早,目前应用比较普遍,而我国起步相对较晚,缺乏HPN规范标准,目前正在缓步发展中。
HPN不仅可以用于良性或恶性疾病所致的慢性肠衰竭(CIF)患者,还可用于终末期患者的姑息性营养治疗。
继2009、2016年之后,欧洲肠外肠内营养学会(ESPEN)在2023年又一次更新了家庭肠外营养治疗指南(以下简称《指南》)。
该指南从HPN的适应证、中心静脉血管通路装置(CVAD)和输液泵、静脉通路维护、营养剂、监测、管理等方面进行了规范。
为帮助相关人员更好地理解和应用,推动指南的有效实施,现对该指南进行解读。
1 指南修订的历程和意义2009年,ESPEN发布了第一份关于HPN的指南。
该指南由26项建议组成,推荐等级分为A/B/0/优质实践意见级(GPP)4级,其中10项基于证据,16项基于专家意见。
2016年,ESPEN发布了良性疾病所致CIF指南,其中包括11条HPN管理的建议、17条肠外营(PN)制剂的建议,以及22条关于预防和治疗中心静脉导管(CVC)相关并发症的建议。
这份指南的证据等级较2016年版本稍高,但其中仍有31条建议的证据等级极低,14条建议的证据等级低。
时至今日,这两版指南中的大多数建议依然有效,特别是涉及营养需求、代谢并发症和中心静脉血管通路装置管理的建议。
各学会和政府机构也提供了HPN的其他指南和标准,然而,一项系统评价显示,这些指南之间存在显著差异。
因此,2020年ESPEN发布了新版HPN指南,纳入自前版发布以来的新证据,强调了关于HPN安全给药的建议,并纳入患者的观点。
2023年发布的指南在其基础上,简短精确地指导临床实践,该指南不包括针对特定条件下患者营养需求的建议,更多的是在实践层面给予指导。
2 家庭肠外营养的适应证与其他HPN相关指南一样,本《指南》指出,HPN应用于无法通过口服和/或肠内途径满足其营养需求且可以在院外安全管理肠外营养的患者(GPP级,强烈共识,同意率95.8%),但本次《指南》对于HPN的适应证进行了更为详细的罗列举例和阐述,见图1。
2012 ACS 癌症预防的营养与运动指南
American Cancer Society Guidelines on Nutrition and Physical Activity for Cancer PreventionReducing the Risk of Cancer With Healthy Food Choicesand Physical ActivityLawrence H.Kushi,ScD1;Colleen Doyle,MS,RD2;Marji McCullough,ScD,RD3;Cheryl L.Rock,PhD,RD4;Wendy Demark-Wahnefried,PhD,RD5;Elisa V.Bandera,MD,PhD6;Susan Gapstur,PhD,MPH7;Alpa V.Patel,PhD8;Kimberly Andrews9;Ted Gansler,MD,MBA,MPH10and The American Cancer Society2010Nutrition andPhysical Activity Guidelines Advisory CommitteeAbstractThe American Cancer Society(ACS)publishes Nutrition and Physical Activity Guidelines to serve as a foundation for its communication,policy,and community strategies and,ultimately,to affect dietary and physical activity patterns among Americans.These Guidelines,published approximately every5years,are developed by a national panel of experts in cancer research,prevention,epidemiology,public health,and policy,and they reflect the most current scientific evidence related to dietary and activity patterns and cancer risk.The ACS Guidelines focus on recommen-dations for individual choices regarding diet and physical activity patterns,but those choices occur within a commu-nity context that either facilitates or creates barriers to healthy behaviors.Therefore,this committee presents recommendations for community action to accompany the4recommendations for individual choices to reduce can-cer risk.These recommendations for community action recognize that a supportive social and physical environment is indispensable if individuals at all levels of society are to have genuine opportunities to choose healthy behaviors.The ACS Guidelines are consistent with guidelines from the American Heart Association and the American Diabetes Association for the prevention of coronary heart disease and diabetes,as well as for general health promotion,as defined by the2010Dietary Guidelines for Americans and the2008Physical Activity Guidelines for Americans.CA Cancer J Clin2012;62:30–67.V C2012American Cancer Society.IntroductionThe Importance of Weight Control,Physical Activity,and Diet in Cancer Prevention For the great majority of Americans who do not use tobacco,the most important modifiable determinants of can-cer risk are weight control,dietary choices,and levels of physical activity.1,2One-third of the more than572,000 cancer deaths that occur in the United States each year can be attributed to diet and physical activity habits,includ-ing overweight and obesity,while another one-third is caused by exposure to tobacco products.2Although genetic susceptibility influences the risk of cancer,most of the variation in cancer risk across populations and among individuals is due to factors that are not inherited.3,4Behaviors such as avoiding exposure to tobacco products, 1Associate Director for Etiology and Prevention Research,Division of Research,Kaiser Permanente,Oakland,CA;2Director,Nutrition and Physical Activity, Cancer Control Science,American Cancer Society,Atlanta,GA;3Strategic Director,Nutritional Epidemiology,American Cancer Society,Atlanta,GA;4Professor,Department of Family and Preventive Medicine,School of Medicine,University of California at San Diego,San Diego,CA;5Professor and Webb Endowed Chair of Nutrition Sciences,University of Alabama at Birmingham,Birmingham,AL;6Assistant Professor,The Cancer Institute of New Jersey,New Brunswick,NJ;7Vice President,Epidemiology Research Program,American Cancer Society,Atlanta,GA;8Strategic Director,Cancer Prevention Study-3, American Cancer Society,Atlanta,GA;9Research Associate,American Cancer Society,Atlanta,GA;10Director of Medical Content,American Cancer Society,Atlanta,GA.Corresponding author:Colleen Doyle,MS,RD,Director of Nutrition and Physical Activity,Cancer Control Science,American Cancer Society,250Williams St, NW,Suite600,Atlanta,GA30303;colleen.doyle@DISCLOSURES:The authors report no conflicts of interest.This report was approved by the American Cancer Society National Board of Directors on August5,2011.V C2012American Cancer Society,Inc.doi:10.3322/caac.20140.Available online at 30CA:A Cancer Journal for Cliniciansmaintaining a healthy weight,staying physically active throughout life,and consuming a healthy diet can substantially reduce one’s lifetime risk of developing,5,6 or dying from,5,7cancer.2,8-11These same behaviors are also associated with a decreased risk of developing cardiovascular disease and diabetes.12Indeed,a recent study demonstrated that nonsmoking(former and never smokers)adult men and women whose lifestyles were most consistent with the2006American Cancer Society(ACS)cancer prevention guidelines for weight control,diet,physical activity,and alcohol had a significantly lower risk of dying from cancer,cardio-vascular disease,or all causes combined.7 Although these healthy choices are made by indi-viduals,they may be facilitated or impeded by the social,physical,economic,and regulatory environ-ment in which people munity efforts are therefore essential to create an environment that facilitates healthy food choices and physical activity. Overview of the GuidelinesThe ACS publishes Nutrition and Physical Activity Guidelines to advise health care professionals,policy-makers,and the general public about dietary and other lifestyle practices that reduce cancer risk.13 These Guidelines,updated in2012by the ACS Nutrition and Physical Activity Guidelines Advisory Committee,are based on synthesis of the current scientific evidence on diet and physical activity in relation to cancer risk.The Committee reviewed evi-dence from human population studies and laboratory experiments published since the last release of the Guidelines in2006.13The Committee also consid-ered other comprehensive reviews of diet,obesity, and physical inactivity in relation to cancer.For many aspects of nutrition and physical activity,the most thorough reviews were the2007World Cancer Research Fund/American Institute for Cancer Research(WCRF/AICR)report and the subsequent Continuous Update reports on breast cancer14and colorectal cancer15;other comprehensive reviews or meta-analyses that were published in recent years were also considered.16In weighing the evidence from randomized controlled trials(RCTs),the Committee considered thefindings in relation to the design of the trial,the specific question being addressed,and the importance of the trial results in the context of other evidence from human populations.Prospective cohort studies were weighted more heav-ily than case-control studies,especially when results were available from several cohorts.Population-based case-control studies with at least200cases of cancer were considered more informative than smaller or hospital-based case-control studies.Studies that adjusted for total energy intake,considered other dietary factors,and controlled for other known risk factors were considered more credible than those that failed to meet these criteria.For many issues concerning nutrition and cancer,the evidence is not definitive because the published results are inconsistent or because the methods of studying nutrition and chronic disease in human populations continue to evolve.Part of the uncer-tainty has resulted from studies that focus on specific nutrients or foods in isolation,thereby oversimplify-ing the complexity of foods and dietary patterns;the importance of the dose,timing,and duration of exposure;and the large variations in nutritional sta-tus among human populations.Nutrition and physi-cal activity research is equally challenging in RCTs, generally considered the gold standard for scientific inference.Studies may fail tofind an effect if the intervention begins too late in life,is too small,or ifthe follow-up is too short for a benefit to appear.In addition,RCTs of lifestyle interventions cannot be blinded,and disease endpoints such as cancer require many years of follow-up.No single trial can resolve allof the questions that are relevant to the potential effects of nutrition throughout the lifespan.Moreover, many important questions about how diet,physical activity,and obesity relate to cancer cannot presentlybe addressed in RCTs.For example,while there is substantial interest in the effects of early-life body size and dietary patterns on the risk of adult cancer,it is practically not feasible to conduct RCTs to determinethe long-term consequences of interventions that begin in infancy and extend for many years.Inferences about the many complex interrelation-ships between body weight,physical activity,diet, and cancer risk are therefore based,for the most part,on a combination of shorter-term clinical trials and observational studies coupled with advancing understanding of the biology of cancer.These Guidelines are based on the totality of evidence from these sources,taking into account both the potential health benefits and possible risks from adopting them.No diet or lifestyle pattern can guarantee fullVOLUME62_NUMBER1_JANUARY/FEBRUARY201231protection against any disease;the potential health benefit represents a decreased likelihood that the disease will occur,not a guarantee of total protec-tion.These Guidelines provide a summary of the existing scientific information about weight control, physical activity,and nutrition in relation to cancer and are intended to be followed as a whole.The ACS Guidelines are consistent with guidelines established for cancer prevention by other governmental and non-governmental organizations2,10;those from the American Heart Association17and the American Diabetes Association18for the prevention of coro-nary heart disease and diabetes;and those for general health promotion,as defined by the2010Dietary Guidelines for Americans19and the2008Physical Activity Guidelines for Americans.20In addition to recommendations regarding indi-vidual choices,the ACS Guidelines underscore what communities can and should do to facilitate healthy eating and physical activity behaviors(Table1).The recommendations for community action recognize that a supportive social and physical environment is indispensable if individuals at all levels of society are to have genuine opportunities to choose and main-tain healthy behaviors.ACS Guidelines for Nutrition and Physical ActivityRecommendations for Community Action Social,economic,and cultural factors strongly influ-ence individual choices about diet and physical activ-ity.21-24Although many Americans would like to adopt a healthy lifestyle,many encounter substantial barriers that make it difficult to follow diet and activity guidelines.21,22,24Indeed,according to the Institute of Medicine,‘‘It is unreasonable to expectTABLE1.American Cancer Society Guidelines on Nutrition and Physical Activity for Cancer PreventionACS RECOMMENDATIONS FOR INDIVIDUAL CHOICESAchieve and maintain a healthy weight throughout life.l Be as lean as possible throughout life without being underweight.l Avoid excess weight gain at all ages.For those who are currently overweight or obese,losing even a small amount of weight has health benefits andis a good place to start.l Engage in regular physical activity and limit consumption of high-calorie foods and beverages as key strategies for maintaining a healthy weight.Adopt a physically active lifestyle.l Adults should engage in at least150minutes of moderate intensity or75minutes of vigorous intensity activity each week,or an equivalent combination, preferably spread throughout the week.l Children and adolescents should engage in at least1hour of moderate or vigorous intensity activity each day,with vigorous intensity activity occurring at least3days each week.l Limit sedentary behavior such as sitting,lying down,watching television,or other forms of screen-based entertainment.l Doing some physical activity above usual activities,no matter what one’s level of activity,can have many health benefits.Consume a healthy diet,with an emphasis on plant foods.l Choose foods and beverages in amounts that help achieve and maintain a healthy weight.l Limit consumption of processed meat and red meat.l Eat at least2.5cups of vegetables and fruits each day.l Choose whole grains instead of refined grain products.If you drink alcoholic beverages,limit consumption.l Drink no more than1drink per day for women or2per day for men.ACS RECOMMENDATIONS FOR COMMUNITY ACTIONPublic,private,and community organizations should work collaboratively at national,state,and local levels to implement policy and environmentalchanges that:l Increase access to affordable,healthy foods in communities,worksites,and schools,and decrease access to and marketing of foods and beveragesof low nutritional value,particularly to youth.l Provide safe,enjoyable,and accessible environments for physical activity in schools and worksites,and for transportation and recreation in communities.ACS indicates American Cancer Society.32CA:A Cancer Journal for Cliniciansthat people will change their behavior easily when so many forces in the social,cultural,and physical envi-ronment conspire against such change.’’25Access to and affordability of healthy foods,the availability and extensive marketing of high-calorie foods and beverages of low nutritional value,and barriers to the ability of individuals to be physi-cally active for recreation and transportation in communities have all been implicated as contribu-tors to obesity trends in the United States.24,26 Avoiding unhealthy weight gain,therefore,goes beyond‘‘personal responsibility’’and an individual’s ability to achieve healthy diet and physical activity habits.Reversing obesity trends will require a broad range of multilevel strategies that include policy and environmental changes.These Guidelines therefore emphasize the impor-tance of public,private,and community organiza-tions working collaboratively at national,state,and local levels to implement policy and environmental changes that:Increase access to affordable,healthy foods in com-munities,worksites,and schools,and decrease access to and marketing of foods and beverages of low nutritional value,particularly to youth.Provide safe,enjoyable,and accessible environments for physical activity in schools and worksites,and for transportation and recreation in communities. Current trends toward increasing portion sizes27-29; the consumption of high-calorie convenience foods, sugar-sweetened beverages,and restaurant meals;and declining levels of physical activity are contributing to an obesity epidemic among Americans of all ages and across all population segments.30-32Longer workdays and more households with multiple wage earners reduce the amount of time available for the prepara-tion of meals,with a resulting shift toward the increased consumption of high-calorie foods outside the home,which are frequently less nutritious than foods prepared at home.33Large portion sizes, calorie-dense foods,and sugar-sweetened beverages are extensively marketed by restaurants,supermarkets, and food and beverage companies.29,32,34,35Reduced leisure time,increased amounts of time spent sitting, increased reliance on automobiles for transportation, and increased availability of electronic entertainment and communications media all contribute to reduced levels of physical activity.36-38There is increasing evi-dence of associations between the built environment and obesity and physical activity levels.36,39,40Poor access to sidewalks,parks,and recreation facilities is associated with greater obesity risk,41whereas neigh-borhoods that facilitate walking and safe physical recreation have lower obesity prevalence.21-24The increase in overweight and obesity noted among Americans is of particular concern for a num-ber of population groups,including children,whoare establishing lifelong behavioral patterns that affect health,and people who live in lower income neighborhoods,which are often characterized by nearby stores that lack affordable,high-quality healthy foods,and increased safety concerns that may limit opportunities for physical activity.Evidence suggests that obese children are more likely than normal-weight children to become obese adults,and that their obesity in adulthood is likely tobe more severe.42-44Promoting the establishment of healthy behaviors among youth is more effective, and often easier,than efforts to change unhealthy behaviors already established in adult populations. Therefore,creating environments that make it easierfor children to establish positive eating and physical activity habits early in life are critical.45Improvingthe school environment through policies that require daily,quality physical education and healthier food and beverage choices,and that limit the availabilityof and access to foods and beverages of low nutri-tional value;limiting advertising and marketing of less healthy foods and beverages;and ensuring com-munities have safe places to play,as well as routes that facilitate bicycling and walking to school,are important strategies to consider in addressing youth obesity trends.24,46While all Americans face obstacles to making healthy choices,the challenges are compounded for lower income and racial/ethnic minority groups,who frequently face additional barriers to making healthy food and physical activity choices.Access to super-markets has been associated with more healthful diets, greater consumption of vegetables and fruits,and lower rates of obesity,47,48and numerous studies have shown that communities with a greater proportion of ethnic minority and low-socioeconomic status resi-dents can be characterized as‘‘food deserts’’(ie,they tend to have fewer supermarkets that carry healthy, affordable,high-quality foods).49-51Limited access to supermarkets frequently results in residents shoppingfor food at local convenience stores,where healthyVOLUME62_NUMBER1_JANUARY/FEBRUARY201233food options tend to be fewer,of lesser quality,and more expensive.52Even in neighborhoods where supermarkets are available,low-income residents may more frequently purchase a diet of less expensive, higher-calorie foods;studies have suggested that lower cost foods comprise a greater proportion of the diet of lower income individuals.53Studies also sug-gest that these neighborhoods,as compared with more affluent areas,have greater access to fast food restaurants and other restaurants that are less likely to offer healthier options.50,54,55Research also points to disparities in the built environment,which likely contribute to differences in physical activity.Access to parks,gyms,and other opportunities for physical activity,such as the avail-ability of sidewalks and the close proximity of resi-dential areas to stores,jobs,schools,and recreation centers,have been shown to contribute to more physi-cally active lifestyles.56,57However,studies have found significantly fewer sports areas,parks,greenways, and bike paths in high-poverty areas when compared with areas with lower poverty rates.Even when these facilities are available,cost factors,distance from physical activity facilities,and transportation avail-ability may still affect access among low-income populations.58,59Heavy traffic,lack of street light-ing,unleashed dogs,high crime rates,and a lack of sidewalks and traffic calming measures are other factors that may present barriers to physical activity, particularly in low-income areas.Ensuring that all Americans have access to afford-able,healthy food choices and opportunities for safe physical activity will require multiple strategies and bold action,ranging from the implementation of community,worksite,school,and other health pro-motion programs to policies that affect community planning,transportation,school-based physical edu-cation,food advertising and marketing,and food services.Public,private,and community organiza-tions at local,state,and national levels will need to implement new policies and reallocate or expand resources to facilitate necessary changes.Health care professionals;school,business,faith group,and other community leaders;and policy makers all have opportunities to provide leadership and to promote purposeful changes in public policy and in commu-nity environments that are necessary to help individ-uals maintain a healthy body weight and remain physically active throughout life.Recommendations for Individual Choices Although the previously rapid increases in obesity prevalence appear to be leveling off in women and possibly in men,approximately two-thirds of Ameri-cans are overweight or obese.60The percentage of children,adolescents,and adult men who are over-weight or obese has continued to increase through 2004,although the trend has now stabilized in adult women and youth.60-62In addition,many Americans are less physically active than is optimal for health. Obesity increases the risk of many cancers,and also has adverse effects on coronary heart disease,stroke, type2diabetes,and other health outcomes,including premature mortality.Thus,while there continues to be scientific uncertainty about how specific aspects of excess adiposity,excessive energy intake,and physical inactivity relate to cancer,there is no debate that these contribute to an increased risk of many types of cancer and that they constitute a serious and growing health problem.These Guidelines therefore emphasize the importance of achieving or maintain-ing a healthy body weight;adopting a physically active lifestyle;consuming a healthy diet that emphasizes plant foods,particularly within the con-text of weight management;and limiting consump-tion of alcoholic beverages.1.Achieve and Maintain a Healthy Weight Throughout Life•Be as lean as possible throughout life without being underweight.•Avoid excess weight gain at all ages.For those who are currently overweight or obese,losing even a small amount of weight has health ben-efits and is a good place to start.•Engage in regular physical activity and limit consumption of high-calorie foods and beverages as key strategies for maintaining a healthy weight. Body Weight and Cancer RiskIn the United States,it has been estimated that over-weight and obesity contribute to14%to20%of all cancer-related mortality.63Overweight and obesity are clearly associated with an increased risk of devel-oping many cancers,including cancers of the breast in postmenopausal women,14colon and rectum,15 endometrium,kidney and adenocarcinoma of the esophagus,and pancreas2,64;are probably associated with an increased risk of cancer of the gallbladder2; and may also be associated with an increased risk34CA:A Cancer Journal for Cliniciansof cancer of the liver,non-Hodgkin lymphoma, multiple myeloma,cancer of the cervix,cancer of the ovary,and aggressive prostate cancer.63,65-70In addition,abdominal fatness is convincingly associ-ated with colorectal cancer,and probably related to a higher risk of pancreatic,endometrial,and post-menopausal breast cancer.2Overweight and obesity are thought to affect the risk of these cancers through a variety of mecha-nisms,some of which are specific to particular cancer types.These mechanisms include effects on immune function and inflammation;levels and metabolism of several hormones,including insulin and estradiol; factors that regulate cell proliferation and growth, such as insulin-like growth factor(IGF)-1;and pro-teins that make hormones more or less available to tissues,such as sex hormone-binding globulin and IGF-binding proteins.71-73Overweight and obesity may increase the risk of adenocarcinoma of the esophagus by increasing the risk of gastroesophageal reflux disease and Barrett esophagus.74,75Most research on energy imbalance and cancer focuses on increased risks associated with overweight and obesity.Some studies exploring intentional weight loss suggest that losing weight may reduce the risk of postmenopausal breast cancer76-78and possibly other cancers.79Results from large studies of lifestyle and behavioral weight loss interventions have shown that modest weight loss improves insulin sensitivity and biochemical measures of hormone metabolism, which have been postulated to contribute to the rela-tionship between obesity and certain cancers.79,80 Examples include the Diabetes Prevention Program Study81and the Action for Health in Diabetes (Look AHEAD)study,82,83both of which used life-style interventions to promote weight loss.Even though our knowledge about the relationship between weight loss and cancer risk is incomplete,individuals who are overweight or obese should be encouraged and supported in their efforts to reduce their weight. Achieving and Maintaining a Healthy WeightA healthy weight depends on a person’s height,so rec-ommendations for a healthy weight are often expressed in terms of a body mass index(BMI)(Table2). Although BMI is not a direct measure of adiposity, it is simple to measure and widely used clinically and in research studies.BMI is calculated as body weight in kilograms(kg)divided by height in meters,squared(m2).84Exact cutoffs for a healthy BMI are somewhat arbitrary,but for most adults,experts con-sider a BMI within the range of18.5to25.0kg/m2to be healthy,a BMI between25.0and29.9kg/m2tobe overweight,and a BMI of30.0kg/m2and overto be obese.The World Health Organization has modified this range,based on differential body com-position across various racial/ethnic groups.85For example,individuals with Asian ancestry are con-sidered to be overweight with a BMI greater than 23.0kg/m2.86Individuals should strive to maintain healthy weights as illustrated in Table2.The way to achieve a healthy body weight is to balance energy intake(food and beverage intake) with energy expenditure(physical activity).19,20 Excess body fat can be reduced by decreasing caloric intake and increasing physical activity.For most adults,a reduction of50to100calories per day may prevent gradual weight gain,whereas a reduction of 500calories or more per day is a common initial goalin weight loss programs.Similarly,300minutes or more of moderate to vigorous intensity physical activity per week may be needed to prevent weight gain or to sustain weight loss for previously over-weight people.19,20,30Caloric intake can be reducedby decreasing the size of food portions;limiting between-meal snacks;and limiting the intake of foods and beverages that are high in calories,fat, and/or added sugars,and that provide few nutrients (eg,many fried foods,cookies,cakes,candy,ice cream, and sugar-sweetened beverages).Such foods and bev-erages should be replaced with choices such as vegeta-bles and fruits,beans,whole grains,and lower calorie beverages.87Meals served in many fast food establish-ments and restaurants typically exceed the serving sizes needed to meet daily caloric needs and are often highin hidden fats and sugars.87They also are often low in vegetables,fruits,beans,and whole grains.33Keeping track of food intake and physical activity has been shown to be effective in weight management.87,88The health of young people,and the adults theywill become,is critically linked to the establishmentof healthy behaviors in childhood.50,89,90Risk factors such as excess weight gain,unhealthy dietary pat-terns,and physical inactivity during childhood and adolescence can result in an increased risk of developing cancer,cardiovascular disease and stroke, diabetes,hypertension,and osteoporosis later in life.91 Children who adopt healthy lifestyle habits at an earlyVOLUME62_NUMBER1_JANUARY/FEBRUARY201235age are more likely to continue these behaviors throughout life.Research suggests that the majority of children and adolescents who are overweight will remain overweight in adulthood.92,93For these rea-sons,efforts to establish healthy weight and patterns of weight gain should begin in childhood,but are no less important in adulthood and throughout life.2.Adopt a Physically Active Lifestyle •Adults should engage in at least150minutes of moderate intensity or75minutes of vigorous intensity activity each week,or an equivalent com-bination,preferably spread throughout the week.•Children and adolescents should engage in at least1hour of moderate or vigorous intensity activity each day,with vigorous intensity activ-ity occurring at least3days each week.•Limit sedentary behavior such as sitting,lying down,watching television,or other forms of screen-based entertainment.•Doing some physical activity above usual activ-ities,no matter what one’s level of activity,can have many health benefits.Benefits of Physical ActivityPhysical activity may reduce the risk of several types of cancer,including cancers of the breast,colon,and endo-metrium,as well as advanced prostate cancer,and possi-bly,pancreatic cancer.2,69,94,95Although evidence for many other cancers is limited,associations may exist. Physical activity acts in a variety of ways to affect cancer risk.96Regular physical activity helps maintain a healthy body weight by balancing caloric intake with energy expenditure,and may help to prevent certain cancers via both direct and indirect effects,including regulating sex hormones,insulin,and prostaglandins,and having various beneficial effects on the immune system.97,98 A physically active lifestyle is also associated with a reduced risk of other chronic diseases,such as heart disease,diabetes,osteoporosis,and hypertension.20TABLE2.Adult BMI ChartBMI1920212223242526272829303132333435 HEIGHT WEIGHT IN POUNDS4010009196100105110115119124129134138143148153158162167 4011009499104109114119124128133138143148153158163168173 5097102107112118123128133138143148153158163168174179 50100100106111116122127132137143148153158164169174180185 50200104109115120126131136142147153158164169175180186191 50300107113118124130135141146152158163169175180186191197 50400110116122128134140145151157163169174180186192197204 50500114120126132138144150156162168174180186192198204210 50600118124130136142148155161167173179186192198204210216 50700121127134140146153159166172178185191198204211217223 50800125131138144151158164171177184190197203210216223230 50900128135142149155162169176182189196203209216223230236 501000132139146153160167174181188195202209216222229236243 501100136143150157165172179186193200208215222229236243250 60140147154162169177184191199206213221228235242250258 60100144151159166174182189197204212219227235242250257265 600200148155163171179186194202210218225233241249256284272 60300152160168176184192200208216224232240248256264272279 HEALTHY WEIGHT OVERWEIGHT OBESE BMI indicates body mass index.Source:US Department of Health and Human Services,National Institutes of Health,National Health,Lung,and Blood Institute.The Clinical Guidelines on the Identification,Evaluation and Treatment of Overweight and Obesity in Adults:Evidence Report.N1H Pub.No.98-4083.Bethesda,MD:US Department of Health and Human Services,National Institutes of Health,National Health,Lung,and Blood Institute;1998.36CA:A Cancer Journal for Clinicians。
史上最全癌症预防指南
史上最全癌症预防指南来源:健康指南/果壳网/凤凰健康综合编撰美国癌症协会(ACS)每5年要发布一期关于饮食、营养和体育运动与癌症预防之间关系的报告,作为对大众的科学知识普及、各卫生健康机构和社区团体之间的交流和有关政策方针制定的指南。
1.乳腺癌:美国妇女最多见的肿瘤,为妇女第二大死亡原因的癌症,仅次于肺癌。
绝经后妇女体重超重,则患乳腺癌的风险显著增加。
这与过多脂肪导致血内雌激素水平过高有关。
过多饮酒并叶酸摄入不足也会增加乳腺癌发生的风险。
体育锻炼可降低这一风险。
2.结、直肠癌:在美国因癌症死亡总人数中居于第2位。
肥胖与其有直接关系,男性尤其显著。
大量摄入蔬菜水果和含粗纤维谷物,减少红肉及加工肉类食品的摄入,适当摄入维生素D和钙,同时加强日常的体育锻炼可以降低其发生的风险。
另外,定期筛检、及时发现和切除肠道腺瘤(癌前病变)也至关重要。
3.肺癌:美国因癌症死亡的第一大因素。
超过85%的患者发病与烟草有关。
戒烟和大量摄入蔬菜水果有助于降低其发生。
但要注意:过量食用含胡萝卜素和维生素A的保健食品反而会使吸烟者的肺癌发生危险系数升高。
4.子宫内膜癌:美国妇女癌症发病率中居第4位。
子宫内膜癌与雌激素水平有关。
通过大量运动,增加蔬菜、水果、粗纤维食品及豆类的摄入,保持健康体重均可降低其发生的可能性。
5.肾癌:占男性癌症发病及死亡的3%、女性的2%。
直接相关因素有肥胖和吸烟。
因此,戒烟及保持健康体重尤为重要。
6.胰腺癌:美国癌症死亡原因的第4位。
吸烟、2型糖尿病、过多食用红肉及体育运动不足与其极为相关。
7.上呼吸道和消化道癌症:酗酒、吸烟显著增加口腔癌、咽喉癌和食管癌的可能。
饮食过热导致食道灼伤,可引发食管的慢性炎症最终恶化为食管癌。
改变不良饮食习惯,戒烟酒,减轻体重和多食新鲜蔬菜及水果有利于降低其发生的风险。
8.前列腺癌:美国男性中最常见的癌症。
多食用西红柿、菜花、豆类及鱼肉有助于降低其发生风险。
维生素E和硒及相应辅助保健食品的保护作用目前尚无确定结论。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
2012 年ACS《癌症预防的营养与运动指南》解读
发布日期:
2012-04-23
作者:
浙江大学医学院附属邵逸夫医院肿瘤内科陈薇潘宏铭
出处:
对应指南:
2012 ACS 癌症预防的营养与运动指南
美国癌症学会(ACS,American Cancer Society)
内容介绍:
最近,美国癌症协会(ACS)下属的营养与运动指导委员会发布了2012 年版《癌症预防的营养与运动指南》。
这是继2006 年版后,美国肿瘤学、预防与流行病学及公共卫生学专家通过再次系统回顾相关循证学证据,面向美国社区及广大民众推出的最新癌症防控建议。
证据显示,在美国每年57 万余癌症死亡病例中,有近1/3 病例与饮食及运动习惯相关,另1/3 则死于烟草制品暴露。
由于人口、环境、饮食习惯及地域文化背景等诸多差异,指南中部分内容并不完全适用于我国。
但研究已证实,不论是在欧美等发达地区,还是在亚非等欠发达地区,恶性肿瘤高发均与某一种或一些不良的生活方式相关。
因此,ACS 2012 年版《癌症预防的营养与运动指南》在我国亦有重要现实意义,本文将结合我国实际情况,对该指南重点部分进行解读,希望能对我国肿瘤学临床医生有所裨益。
饮食、运动:多种恶性肿瘤的明确危险因素
乳腺癌乳腺癌的发病率在我国正逐年攀升。
已知的非饮食相关危险因素:绝经后激素替代疗法、青年时期接受电离辐射、月经初潮早于12岁、绝经时间推迟、30 岁以后生育第一胎以及明确的家族史等。
目前认为,绝经后体重增加及饮酒也与乳腺癌发病率升高有关,如以蔬菜、水果、禽肉及鱼为主的食谱或可降低罹患乳腺癌风险。
专家建议,最佳预防方法是坚持日常运动、终生控制体重在合理水平及不饮酒或限制饮酒。
肺癌肺癌是全世界致死率最高的恶性肿瘤,超过85% 的肺癌由吸烟引起。
不仅如此,吸烟还与许多不良生活习惯相关联,如缺少运动、不健康的饮食模式等,这些肺癌风险相关因素很难分开。
在美国,得益于近20 年来的禁烟措施,肺癌发生率已有所下降;但在我国,烟民比率仍旧居高不下。
因此,戒烟是预防肺癌的重中之重。
此外,研究还发现多摄入水果有助于降低肺癌发生率。
胃癌虽然在美国胃癌发病率较低,但其仍是仅次于肺癌的全世界第二高致死率的恶性肿瘤。
幽门螺杆菌(Hp)感染是主要病因之一。
关于体重与胃癌的关系研究较少,最近一项荟萃分析表明,高体重指数与胃癌发病率增加相关。
在饮食种类方面,新鲜的蔬菜及水果类摄入可降低胃癌发病率,而进食腌制或高盐食物会增加患胃癌风险。
我国国民由于饮食方式以团餐为主,Hp 感染率高,也是导致胃癌发病率高的因素之一。
结直肠癌众所周知,结直肠癌(CRC)发病呈家族聚居性,有着比较明确的基因易感性。
研究还发现,长期使用烟草或酒精会增加患病几率;无论男女,体重超标都是CRC 的危险因素,尤其是男性人群。
进一步对CRC 患者体脂分布比较的研究发现,腹部脂肪蓄积与CRC 发病风险高度相关。
另外,增加日常运动也可降低CRC发病风险。
许多研究显示,中等强度的日常规律锻炼可明显地降低结肠癌的发病率。
自1970 年起,红肉(猪牛肉类)的摄入与CRC 的关系屡见报道。
而最近的一项荟萃分析显示,每摄入100 g红肉或50 g 加工过的肉类,罹患CRC风险增加15%~20%。
烤肉中所含的异环胺类及多环芳香类碳水化合物的致癌作用被认为是作用机制之一。
另外,红肉中所含的铁也被认为是产生亚硝胺类致癌物的催化剂。
在降低CRC 发病率方面,高纤维饮食备受关注,但始终缺乏循证学依据。
直至最近,有一项大样本前瞻性队列研究证实了全谷物类纤维素的预防CRC 作用。
补充维生素D 及钙在一些研究中被认为有降低CRC 风险的作用,但由于高钙会增加前列腺癌的风险,所以目前仍不推荐。
前列腺癌目前,已明确的前列腺癌危险因素为年龄、家族史及雄激素水平等,而营养因素对它的影响在最近几年才渐渐明确。
NIH-AARP饮食与健康研究表明,体重超标与前列腺癌的不良预后相关。
另外,高钙被认为与前列腺癌的风险增加相关,而硒或维生素E 等的补充与发病率关系不大。
澄清日常饮食习惯与恶性肿瘤利弊关系
酒精在我国居民生活中,含酒精饮料摄入非常普遍。
数据明确显示,酒精能升高罹患口腔、咽喉、食道、结直肠及乳腺癌的风险。
指南建议常规饮酒人群降低饮用量,至少降低至男性每天10 盎司(约280 g)白酒或24 盎司(约680 g)啤酒,女性每天5 盎司(约140 g)白酒或12 盎司(约340 g)啤酒。
此外,酒精与烟草还有协同致癌作用。
咖啡随着经济的不断发展,我国的咖啡消费量也不断攀升。
虽然曾有研究认为咖啡与胰腺癌存在联系,但未得到最近研究的支持,甚至有研究表明,摄入咖啡是致死性前列腺癌的保护因素。
目前为止,尚无确凿证据显示咖啡增加癌症风险。
钙剂不仅在美国,近年我国也有越来越多的居民加入日常补钙的行列。
研究认为高量钙剂补充能预防结肠癌;但是也有数据显示,补钙会增加前列腺癌风险。
因此,指南认为补钙应适量,推荐19~50 岁人群的钙摄入量为1000mg/d,50 岁以上人群的钙摄入量为1200 mg/d,而且以食物摄入为主,如多进食绿叶类蔬菜等.
抗氧化剂研究显示,摄入蔬菜和水果较多的人群,可从这些富含抗氧化剂食品获益,降低一些癌症风险。
但数项抗氧化补充剂的随机对照试验显示,这些补充剂未降低癌症风险。
因此,指南认为,目前获取抗氧化剂的最佳方法是通过多食用蔬菜水果来达到,服用抗氧化剂药物并非首选。
脂肪流行病学研究很早就注意到,来自高脂肪饮食习惯国家的人群发生乳腺癌、结肠癌及前列腺癌的比例较高。
但是,后续许多更严格的前瞻性研究未进一步证实,高脂饮食与上述各恶性肿瘤间存在因果联系。
因此指南认为,目前没有充足的数据能够证实高脂与癌症间存在联系。
转基因食物在美国,超过90% 的大豆种子及超过70% 的玉米种子接受了以抗杀虫剂及除草剂为目标的基因修饰,随之而来的问题是,这样的转基因食物是否安全?
目前为止,尚无研究显示转基因食物与癌症发生率之间存在关联,也未发现其对人体造成损害的证据;但必须指出的是,无关联并不意味着绝对的安全。
转基因食物大量进入市场不过近十余年时间,一些远期风险还无法评估。
目前,美国食品药品监督管理局及欧洲环境保护局都对市售转基因食物正在进行长期的跟踪研究。
合理饮食、运动四建议
在美国,约2/3 居民存在超重或肥胖的问题;而在我国,得益于饮食结构中蔬菜类比例较高,这一问题尚未如此严重。
已明确证实,肥胖可增加多种癌症的发病率,并且是冠心病、卒中、糖尿病、早产儿死亡的危险因素。
因此,即使肥胖引起上述疾病的机制尚不明确,控制体重也已刻不容缓。
指南就这一目标提出了四大建议:
★终生保持合理体重,在所有的年龄段都不要超重。
保持体重要从坚持日常锻炼及限制高能量食物和饮料入手。
目前已出现超重或肥胖的个体,只要能减轻体重,即使是很少重量,对健康也是有益的;
★坚持日常锻炼。
成人每周至少要参加150 min 中等强度锻炼或75 min 高强度锻炼;减少坐卧不动的时间,如看电视、电脑等;
★坚持健康膳食,多摄入植物性食物。
选择低热量食物,限制红肉类食物,多吃粗加工的谷物如全谷物面包、燕麦片等;
★限制饮酒。
建议常规饮酒者降低饮用量,至少降低至男性每天10 盎司(约280 g)白酒或24 盎司(约680 g)啤酒,女性每天5 盎司(约140 g)白酒或12 盎司(约340 g)啤酒。
笔者认为,虽然我国人民的肥胖问题尚没有欧美国家严重,但是上述四条建议于我国民众同样适用。
过去的30 年,通过各种新技术和新药物的使用,恶性肿瘤的治疗水平明显提高。
但不可否认的是,恶性肿瘤已成为影响我国人民健康的第一致死原因。
而作为受益面最广的措施,癌症的一级预防在欧美发达国家已经得到了长足的发展,但在我国依然任重而道远。
我国经济发展迅速,人民生活水平明显提高,但防癌意识亟需提高,防癌知识须进一步普及。
目前,我国防癌的重点应该是群体和个体防癌意识同时推进,要控制或减少高能耗、高污染企业,规范农药、化肥的使用和管理,加强食品及添加剂的科学管理,个人要戒烟、饮酒要适量、重视体育锻炼,形成良好的生活习惯。