Clinical Evaluation of an Aerolysin-Based
替罗非班在急性进展性脑梗死中应用
现代医学Modern Medical Journal2020,Aug ;48(8):966-970[收稿日期]2020-03-23[修回日期]2020-08-11[作者简介]尹其舵(1982-),男,安徽巢湖人,主治医师。
E -mail :Yqd19820815@163.com[通信作者]吴清阳E -mail :qingyangwumd@163.com[引文格式]尹其舵,李正侠,耿万杰,等.替罗非班在急性进展性脑梗死中应用[J ].现代医学,2020,48(8):966-970.·论著·替罗非班在急性进展性脑梗死中应用尹其舵1,李正侠1,耿万杰1,吴清阳2(1.安徽省阜阳市太和县人民医院神经内科,安徽阜阳236600;2.南京医科大学附属无锡市人民医院影像科,江苏无锡214023)[摘要]目的:探讨替罗非班联合阿司匹林、氯吡格雷对急性进展性脑梗死患者的临床疗效、生活质量ADL 评分、神经功能缺损NIHSS 评分的影响。
方法:前瞻性分析90例急性进展性脑梗死患者,随机分为观察组和对照组,各45例。
对照组给予服用阿司匹林、氯吡格雷治疗,观察组在经替罗非班联合治疗(24 72)h 后贯续服用阿司匹林及氯吡格雷。
比较2组患者治疗后临床疗效、NIHSS 评分(24h 、72h 、7d 及14d )、ADL 评分及不良反应发生率。
结果:观察组总有效率为88.99%,高于对照组的71.11%(P <0.05);观察组治疗后NIHSS 评分低于对照组,且观察组治疗后与治疗前ADL 评分差值高于对照组(P <0.05);不良反应发生率:观察组为13.85%,对照组为7.69%(P >0.05)。
结论:替罗非班联合阿司匹林、氯吡格雷能有效地改善急性进展性脑梗死患者脑组织血流,提高患者生活质量,改善神经功能,安全性较好。
[关键词]急性进展性脑梗死;替罗非班;NIHSS 评分;生活质量[中图分类号]R743.3[文献标识码]A[文章编号]1671-7562(2020)08-0966-05doi :10.3969/j.issn.1671-7562.2020.08.006Effect of tirofiban in patients with acute cerebral infarctionYIN Qiduo 1,LI Zhengxia 1,GENG Wanjie 1,WU Qingyang 2(1.Department of Neurology ,Taihe County People 's Hospital ,Fuyang 236600,China ;2.Department of Radiology ,the Affiliated Wuxi People 's Hospital of Nanjing Medical University ,Wuxi 214023,China )[Abstract ]Objective :To study the clinical efficacy of tirofiban combined with aspirin and clopidogrel on scores ofDaily Living Ability Scale (ADL )and National Institute of Health Stroke Scale (NIHSS )in patients with acute pro-gressive cerebral infarction.Methods :90patients with acute progressive cerebral infarction admitted to our hospi-tal from July 2018to July 2019were randomly divided into observation group and control group (45cases ).The control group was treated with aspirin and clopidogrel ,on top of which the observation group was given tirofiban.The clinical efficacy ,ADL ,NIHSS and adverse reactions between the two groups were statistically analyzed.Results :The total effective rate was 88.89%in the observation group ,71.11%in the control group (P <0.05).In the observation group ,the NIHSS were lower than those during the time of 24h ,72h ,7d and 14d ,respectively (P <0.05)and meanwhile ,the differentials of ADL between post treatment and prior treatment were high than those in the control group (P <0.05).The incidence of adverse reactions was 13.85%in the observation group ,7.69%in the control group (P >0.05).Conclusion :Tirofiban combined with aspirin and clopidogrel has a cura-tive effect in acute progressive cerebral infarction ,improving the brain microcirculation blood flow and nerve func-tion ,enhancing life quality of patients ,and ensuring the safety of the therapy.[Key words ]acute progressive stroke ;tirofiban ;score of NIHSS ;quality of life·669·急性脑梗死是临床常见的一种脑血管疾病,病理生理学基础为脑血供突然中断,可导致脑组织坏死,神经元细胞、星形胶质细胞、胶质细胞不同程度损伤,是出现致残、致死的严重脑血管疾病之一。
玻璃酸钠注射液+塞来昔布对膝骨关节炎患者的临床效果影响分析

药物与临床DOI:10.16662/ki.1674-0742.2024.01.118玻璃酸钠注射液+塞来昔布对膝骨关节炎患者的临床效果影响分析王艳,曹华,丁妍镇江三五九医院,江苏镇江212004[摘要]目的探讨玻璃酸钠注射液+塞来昔布对膝骨关节炎患者的临床疗效的影响。
方法随机选取2022年1月—2023年8月镇江三五九医院收治的90例膝骨关节炎患者为研究对象,依照随机数表法分成对照组和研究组,各45例。
对照组应用玻璃酸钠注射液治疗,研究组联合应用玻璃酸钠注射液+塞来昔布治疗,均持续治疗10周。
两组的总有效率、治疗前后的血清炎性因子指标、疼痛评分、膝关节功能评分、生活质量评分。
结果研究组总有效率为97.78%高于对照组的82.22%,差异有统计学意义(χ2=6.049,P<0.05)。
治疗后,研究组血清C反应蛋白、白细胞介素-6水平均较对照组更低,差异有统计学意义(P均<0.05),研究组的疼痛评分比对照组低,差异有统计学意义(P<0.05),研究组的膝关节功能评分、生活质量4个维度评分均比对照组高,差异有统计学意义(P均<0.05)。
结论将玻璃酸钠注射液与塞来昔布联合用于治疗膝骨关节炎可增强对患者关节炎症反应、疼痛的缓解作用,病情控制效果良好,有利于改善患者膝关节功能,提升其生活质量水平。
[关键词]膝骨关节炎;玻璃酸钠注射液;塞来昔布[中图分类号]R5 [文献标识码]A [文章编号]1674-0742(2024)01(a)-0118-04Analysis of the Clinical Effect of Sodium Hyaluronate Injection + Cele⁃coxib on Patients with Knee Osteoarthritis and the Influence of VAS Score WANG Yan, CAO Hua, DING YanZhenjiang 359 Hospital, Zhenjiang, Jiangsu Province, 212004 China[Abstract] Objective To explore the clinical effect of sodium hyaluronate injection + celecoxib on patients with knee osteoarthritis. Methods 90 patients with knee osteoarthritis admitted to Zhenjiang 359 Hospital from January 2022 to August 2023 were randomly selected as research subjects and divided into control group and study group according to the random number table method, with 45 cases each. The control group was treated with sodium hyaluronate injec⁃tion, and the study group was treated with sodium hyaluronate injection + celecoxib, both group continued for 10 weeks. The total effective rate and the serum inflammatory factor indexes, pain scores, knee function scores, and qual⁃ity of life scores were compared between the two groups before and after treatment. Results Regarding the total effec⁃tive rate was 97.78% in the study group, which was higher than 82.22% in the control group, the difference was statis⁃tically significant (χ2=6.049, P<0.05). After treatment, serum C-reactive protein and interleukin-6 levels in the study group were lower than in the control group, the differences were statistically significant (both P<0.05). Pain scores in the study group were lower than in the control group, the difference was statistically significant (P<0.05). Knee func⁃tion scores and four dimensions of quality of life scores in the study group were higher than in the control group, the differences were statistically significant (all P<0.05). Conclusion The combination of sodium hyaluronate injection and celecoxib for the treatment of knee osteoarthritis can enhance the alleviation of patients' joint inflammatory re⁃sponse and pain, and the condition control effect is good, which is conducive to the improvement of patients' knee joint function and the enhancement of their quality of life level.[Key words] Knee osteoarthritis; Sodium hyaluronate injection; Celecoxib[作者简介] 王艳(1982-),女,本科,主管药师,研究方向为膝骨关节炎。
冰刺激联合康复疗法治疗脑梗死合并假性球麻痹致吞咽困难患者的临床效果
资料与方法2016年1月-2017年5月收治脑梗死并假性球麻痹致吞咽障碍患者129例,根据第5次全国脑血管疾病诊断标准,通过CT/MRI检测所有患者确诊。
使用随机数字法对将129例患者分为观察组65例与对照组64例。
对照组男34例,女30例;年龄52.6~80岁,平均(68.4±6.0)岁。
观察组男36例,女29例;年龄51~78岁,平均(65.8±5.9)岁。
两组一般资料对比,差异无统计学意义(P>0.05),有可比性。
方法:对照组接受常规护理+康复疗法,常规护理包括对症治疗、营养状况改善、保持口腔卫生、消除脑水肿等。
康复训练方法为护理人员指导患者进行面部相关肌群训练,如面颊、空吞咽等,通过对面部肌群训练,带动颈部肌肉、舌的运动,并指导患者如何正确咳嗽、呼吸等。
以上训练方法根据患者接受能力、病情变化等进行加强调整,使患者每日坚持反复训练。
对患者饮食进行控制,早期给予其稀流质食物,同时护理人员需协助患者小口缓慢进食,待患者病情得到改善后,给予其半流质食物,根据患者病情改善程度,过渡至正常食物。
观察组患者在对照组基础上联合冰刺激疗法,具体方法为对患者、上下牙齿咬合面、软腭、腭弓、后腭弓及面颊等部位使用经-4℃生理盐水浸泡后的棉棒进行刺激,每处刺激1min,交替刺激,持续治疗15min,2次/d。
冰刺激治疗完成后,护理人员需指导患者重复做龇牙、鼓腮、空口咽等动作。
观察指标及疗效评定:疗效评定根据患者吞咽功能改善情况进行评估。
①显效:经康复训练治疗后,患者吞咽功能基本恢复或完全恢复,无并发症,且相比于治疗前饮水试验提高1~2级,患者营养状况良好;②有效:患者吞咽功能改善显著,且营养状况较佳,与治疗前对比饮水试验上升1级;③无效:与治疗前比较,治疗后患者吞咽功能基本无较大改善。
观察指标:详细记录两组患者治疗后,吞咽功能障碍病程时间,并对比两组治疗后<10d、10d、20d、30d等时间段占比。
剪切波弹性成像评估慢性心力衰竭患者骨骼肌异常应用现状的研究进展

•前沿进展•剪切波弹性成像评估慢性心力衰竭患者骨骼肌异常应用现状的研究进展张曈,杨华睿,逯雪峰,童明辉【摘要】 晚期慢性心力衰竭(CHF )患者常伴有肌肉质量及力量丧失,肌肉活检结果证实CHF 患者存在外周骨骼肌异常,如肌肉萎缩及肌纤维尺寸减小等,但肌肉活检创伤较大,因此需寻找侵入性较小的检查方法以评估CHF 患者骨骼肌异常。
剪切波弹性成像(SWE )可对肌肉组织进行实时、定量评价,且重复性良好,可为临床诊断和指导CHF 伴骨骼肌异常患者的治疗等提供客观、可靠的依据。
本文主要综述了SWE 评估CHF 患者骨骼肌异常的应用现状。
【关键词】 心力衰竭;弹性成像技术;剪切波弹性成像;肌肉骨骼系统;肌,骨骼;综述【中图分类号】 R 541.6 R 445.1 【文献标识码】 A DOI :10.3969/j.issn.1008-5971.2019.07.y03张曈,杨华睿,逯雪峰,等.剪切波弹性成像评估慢性心力衰竭患者骨骼肌异常应用现状的研究进展[J ].实用心脑肺血管病杂志,2019,27(7):5-8.[ ]ZHANG T ,YANG H R ,LU X F ,et al.Research progress on applications of shear-wave elastography in evaluatingskeletal muscle abnormalities in patients with chronic heart failure [J ].Practical Journal of Cardiac Cerebral Pneumal and Vascular Disease ,2019,27(7):5-8.Research Progress on Applications of Shear-wave Elastography in Evaluating Skeletal Muscle Abnormalities in Patients with Chronic Heart Failure ZHANG Tong ,YANG Huarui ,LU Xuefeng ,TONG Minghui The Second Hospital of Lanzhou University ,Lanzhou 730030,China Corresponding author :TONG Minghui ,E-mail :tongmh1962@【Abstract 】 Chronic heart failure (CHF )patients often accompanied with Loss of muscle mass and strength ,meanwhile muscle biopsy results had confirmed that ,CHF patients may occur peripheral skeletal muscle abnormalities (such as amyotrophia and decrease of muscle fiber size ),but muscle biopsy is relatively traumatogenic ,so less invasive examination method is needed to evaluate the skeletal muscle abnormalities in patients with CHF. Shear-wave elastography (SWE ),a real-time and quantitative evaluation method with Good repeatability for muscular tissue ,may provide objective and reliable basisfor the diagnosis and treatment of CHF patients accompanied with skeletal muscle abnormalities. This paper mainly reviewed theapplications of SWE in evaluating skeletal muscle abnormalities in patients with CHF. 【Key words 】 Heart failure ;Elasticity imaging techniques ;Shear-wave elastography ;Musculoskeletal system ;Muscle ,skeletal ;Review730030甘肃省兰州市,兰州大学第二医院通信作者 :童明辉,E-mail :tongmh1962@慢性心力衰竭(CHF )是多种心血管疾病的终末期表现及导致心血管疾病患者死亡的主要原因,由于其发病率、住院率及病死率均较高,因此CHF 已成为21世纪心血管领域面临的两大挑战之一。
分析高压氧对重症脑外伤患者康复治疗的临床应用效果

分析高压氧对重症脑外伤患者康复治疗的临床应用效果戚永花,赵波,胡欣欣[摘要]目的分析高压氧疗法应用于重症脑外伤患者康复治疗期间的疗效。
方法方便选取2020年6月—2023年6月青岛市城阳区人民医院收治的98例重症脑外伤患者,根据治疗方案的不同分为两组,每组49例,对照组接受常规康复治疗,研究组在对照组基础上加用高压氧治疗,比较两组患者康复治疗效果。
结果研究组治疗有效率(97.96%)显著高于对照组(81.63%),差异有统计学意义(χ2=7.127,P<0.05)。
治疗前,两组患者神经功能缺损评分比较,差异无统计学意义(P>0.05);治疗后,研究组神经功能缺损评分低于对照组,差异有统计学意义(P<0.05)。
治疗前,两组患者格拉斯哥昏迷量表(Glasgow Coma Scale, GCS)评分比较,差异无统计学意义(P>0.05);治疗后,研究组GCS评分高于对照组,差异有统计学意义(P<0.05)。
研究组并发症发生率低于对照组,差异有统计学意义(P<0.05)。
结论重症脑外伤患者在常规康复治疗的基础上予以高压氧治疗,可提升患者的康复速度,改善患者的神经功能,预防并发症的出现,疗效确切。
[关键词]高压氧;重症脑外伤患者;康复治疗;临床效果[中图分类号]R493[文献标识码]A[文章编号]2095-994X(2024)01-0102-04DOI:10.11966/j.issn.2095-994X.2024.10.01.28Analyzing the Clinical Application Effect of Hyperbaric Oxygen on the Rehabilitation of Patients with Critical Traumatic Brain InjuryQI Yonghua, ZHAO Bo, HU XinxinDepartment of Hyperbaric Oxygen, Qingdao Chengyang District People's Hospital, Qingdao, ShandongProvince, 266109 China[Abstract] Objective To analyze the therapeutic effect of hyperbaric oxygen therapy used in the rehabili⁃tation of patients with critical traumatic brain injury. Methods 98 patients with critical traumatic brain injury admitted to Qingdao Chengyang District People's Hospital from June 2020 to June 2023 were conveniently se⁃lected divided into two groups according to different treatment plans, with 49 cases in each group. The control group received routine rehabilitation treatment, and the study group added hyperbaric oxygen therapy on the basis of the control group to compare the rehabilitation treatment effects of the two groups. Results The effec⁃tive rate of the study group was 97.96%, which was significantly higher than that of the control group (81.63%), the difference was statistically significant (χ2=7.127, P<0.05). Before treatment, there was no significant differ⁃ence in neurological function deficit scores between the two groups (P>0.05). After treatment, the neurological impairment score of the study group was lower than that of the control group, and the difference was statisti⁃cally significant (P<0.05). Before treatment, there was no significant difference in the scores of Glasgow Coma Scale (GCS) between the two groups (P>0.05). After treatment, the GCS score of the study group was higher than that of the control group, and the difference was statistically significant (P<0.05). The complication rate of the study group was lower than that of the control group, and the difference was statistically significant (P<0.05). Conclusion Hyperbaric oxygen therapy in patients with critical traumatic brain injury on the basis ofconventional rehabilitation therapy will enhance the recovery speed of patients, improve their neurological function, prevent complications, and achieve precise efficacy.[Key words]Hyperbaric oxygen; Critical traumatic brain injury patients; Rehabilitation; Clinical effect【作者单位】青岛市城阳区人民医院高压氧科,山东青岛 266109【作者简介】戚永花(1986-),女,本科,主治医师,研究方向为急性有毒性气体中毒的高压氧治疗、脑外伤脑卒中后康复联合高压氧治疗102世界复合医学脑外伤指的是发生在人头部的外伤,主要是撞伤、跌坠伤,外力击打也是导致脑外伤发生的主要原因之一。
布地格福吸入气雾剂治疗COPD稳定期的临床疗效及安全性研究

DOI:10.16662/ki.1674-0742.2023.28.072布地格福吸入气雾剂治疗COPD稳定期的临床疗效及安全性研究程易,黄锦宏,由振华,周秀芬,陈虹常熟市第二人民医院呼吸与危重症医学科,江苏常熟215501[摘要]目的探究布地格福吸入气雾剂治疗慢性阻塞性肺疾病(chronic obstructive pulmonary disease, COPD)稳定期的临床疗效及安全性。
方法随机选择2021年9月—2022年9月常熟市第二人民医院就诊的80例COPD稳定期患者,随机数表法将其分为40例对照组和40例研究组。
对照组接受布地奈德福莫特罗治疗,研究组接受布地格福吸入气雾剂治疗。
比较两组疗效及不良反应,并对两组肺功能、6 min步行距离、生活质量[圣乔治呼吸问卷(St.George's Respiratory Questionnaire, SGRQ)评分]、健康情况[COPD患者自我评估测试问卷(COPD Assessment Test, CAT)评分]、血清基质金属蛋白酶-9(matrix metalloproteinse-9, MMP-9)水平及辅助性T细胞(T helper cells, Th)1与Th2比值(Th1/Th2)进行治疗前后对比。
结果研究组治疗总有效率为95.00%,高于对照组的80.00%,差异有统计学意义(χ2=4.114,P<0.05)。
研究组治疗后用力肺活量、第1秒用力呼气量、第1秒用力呼气量/用力肺活量占预计值比治疗前及对照组高,差异有统计学意义(P<0.05)。
研究组治疗后CAT评分、SGRQ评分比治疗前及对照组低,6 min步行距离比治疗前及对照组远,差异有统计学意义(P<0.05)。
研究组治疗后MMP-9、Th1/Th2比治疗前及对照组低,差异有统计学意义(P<0.05)。
结论布地格福吸入气雾剂治疗COPD稳定期的临床疗效确切,可显著改善患者肺功能及运动耐力,且安全性较高。
小剂量多巴酚丁胺早期干预治疗肺炎合并脓毒症的临床效果分析

DOI:10.16662/ki.1674-0742.2020.03.124小剂量多巴酚丁胺早期干预治疗肺炎合并脓毒症的临床效果分析母群华云南省曲靖市第一人民医院呼吸科,云南曲靖655000[摘要]目的观察分析小剂量多巴酚丁胺早期干预治疗肺炎合并脓毒症的临床效果。
方法方便选择在该院进行治疗的肺炎合并脓毒症患者42例,具体的选择时间为2018年4月—2019年4月,将患者随机分为普通组和观察组,每组各21例,普通组行常规治疗,观察组行小剂量多巴酚丁胺早期干预治疗,比较分析两组患者的临床治疗效果、治疗指标、器官衰竭其死亡发生情况。
结果观察组患者的治疗总有效率为95.24%(20例);普通组患者的治疗总有效率为71.43%(15例);观察组患者的治疗有效率明显高于普通组,差异有统计学意义(χ2=4.286,P<0.05)。
观察组患者呼吸困难消失时间为(3.4±0.5)d,血压恢复时间为(4.1±0.7)d,住院天数为(13.5±2.6)d;普通组患者呼吸困难消失时间为(7.9±1.6)d,血压恢复时间为(9.2±1.4)d,住院天数为(19.7±4.8)d,观察组患者的呼吸困难消失时间、血压恢复时间及住院天数明显低于普通组,差异有统计学意义(t=12.302、14.931、5.205,P<0.05)。
观察组患者器官衰竭的发生率为4.76%(1例),未出现死亡患者;普通组患者器官衰竭的发生率为28.57%(6例),死亡发生率为23.81%(4例),观察组患者器官衰竭、死亡发生率明显低于普通组,差异有统计学意义(χ2=4.286、4.421,P<0.05)。
结论通过多巴酚丁胺对肺炎合并脓毒症患者进行早期干预治疗,能够提高患者的治疗效果,缩短症状消失时间,降低患者的器官衰竭及死亡发生率,从而有效挽回患者的生命,值得临床推广使用。
[关键词]多巴酚丁胺;肺炎合并脓毒症;早期干预;小剂量[中图分类号]R720[文献标识码]A[文章编号]1674-0742(2020)01(c)-0124-03Clinical Effect Analysis of Early Intervention of Low-dose Dobutamine in the Treatment of Pneumonia Complicated with SepsisMU Qun-huaDepartment of Respiratory Medicine,the First People's Hospital of Qujing City,Qujing Yunnan Province,655000China[Abstract]Objective To observe and analyze the clinical effect of early intervention with low-dose dobutamine in the treatment of pneumonia complicated with sepsis.Methods42patients with pneumonia and sepsis who were treated in the hospital from April2018to April2019were convenient selected.The patients were randomly divided into two groups,21 cases in each group,21cases in the ordinary group and21cases in the observation group.The occurrence of death.Results The total effective rate of the observation group was95.24%(20cases);the total effective rate of the general group was 71.43%(15cases);the effective rate of the observation group was significantly higher than that of the normal group,the difference was statistically significant(χ2=4.286,P<0.05).The disappearance time of dyspnea in the observation group was (3.4±0.5)d,the recovery time of blood pressure was(4.1±0.7)d,and the number of hospitalization days was(13.5±2.6)d.The time of disappearance of dyspnea in the general group was(7.9±1.6)d,blood pressure recovery time.(9.2±1.4)d,the length of hospital stay was(19.7±4.8)d.The time of disappearance of dyspnea,blood pressure recovery time and hospitalization days were significantly lower in the observation group than in the normal group(t=12.302,14.931,5.205,P<0.05).The inci⁃dence of organ failure in the observation group was4.76%(1case),and no death occurred.The incidence of organ failure in the general group was28.57%(6cases),and the incidence of death was23.81%(4cases).The incidence of organ failure and death was significantly lower in the patients than in the normal group,and the difference was statistically significant(χ2= 4.286,4.421,P<0.05).Conclusion Early intervention with dobutamine in pneumonia patients with sepsis can improve the treatment effect,shorten the disappearance time of symptoms,reduce the incidence of organ failure and death,thus effec⁃tively save the lives of patients,which is worthy of clinical application.[Key words]Dobutamine;Pneumonia with sepsis;Early intervention;Low dose[作者简介]母群华(1971-),女,云南曲靖人,本科,副主任医师,主要从事呼吸系统疾病的诊治工作。
布地奈德雾化吸入联合甲泼尼龙治疗慢阻肺急性期的临床评价

《中外医学研究》第19卷 第11期(总第487期)2021年4月 经验体会 Jingyantihui- 159 -①阳江江华医院 广东 阳江 529500布地奈德雾化吸入联合甲泼尼龙治疗慢阻肺急性期的临床评价叶发展① 彭旭① 刘国文①【摘要】 目的:探究布地奈德雾化吸入联合甲泼尼龙治疗慢性阻塞性肺疾病(COPD)急性期的临床效果。
方法:选择笔者所在医院2019年9月-2020年9月收治的200例COPD 急性期患者为研究对象,根据随机信封法分为对照组100例与观察组100例,两组均给予抗感染、吸氧等对症治疗,对照组给予甲泼尼龙片治疗,观察组在对照组基础上联合布地奈德雾化吸入治疗。
观察比较两组临床治疗效果、治疗前后血气指标、呼吸困难评分及不良反应发生情况。
结果:观察组临床治疗总有效率(97.00%)高于对照组(84.00%),差异有统计学意义(P <0.05);治疗后观察组PaO 2水平高于对照组,PaCO 2水平低于对照组,呼吸困难评分低于对照组,差异均有统计学意义(P <0.05)。
观察组不良反应发生率低于对照组,差异有统计学意义(P <0.05)。
结论:布地奈德雾化吸入联合甲泼尼龙治疗COPD 急性期效果显著,可有效改善患者血气指标,减轻呼吸困难程度,不良反应少。
【关键词】 布地奈德 甲泼尼龙 慢性阻塞性肺疾病 急性期 血气指标 呼吸困难 doi:10.14033/ki.cfmr.2021.11.059文献标识码 B文章编号 1674-6805(2021)11-0159-03 Clinical Evaluation of Budesonide Aerosol Inhalation Combined with Methylprednisolone in Treatment of Acute Chronic Obstructive Pulmonary Disease/YE Fazhan, PENG Xu, LIU Guowen. //Chinese and Foreign Medical Research, 2021, 19(11): 159-161 [Abstract] Objective: To investigate the clinical effect of Budesonide aerosol inhalation combined with Methylprednisolone in treatment of chronic obstructive pulmonary disease (COPD) in the acute phase. Method: A total of 200 COPD patients in the acute stage admitted to our hospital from September 2019 to September 2020 were selected as the research objects, and were divided into the control group (100 cases) and the observation group (100 cases) according to random envelope method, both groups were given symptomatic treatment such as anti-infection and oxygen inhalation, the control group was given Methylprednisolone Tablet treatment, and the observation group was combined with Budesonide aerosol inhalation treatment on the basis of the control group. The clinical treatment effect, blood gas index, dyspnea score and adverse reactions were observed and compared between the two groups before and after treatment. Result: The total effective rate in the observation group (97.00%) was higher than that in the control group (84.00%), the difference was statistically significant (P <0.05). After treatment, the level of PaO 2 in the observation group was higher than that in the control group, the level of PaCO 2 was lower than that in the control group, and the dyspnea score was lower than that in the control group, the differences were statistically significant (P <0.05). The incidence of adverse reactions in the observation group was lower than that in the control group, the difference was statistically significant (P <0.05). Conclusion: Budesonide aerosol inhalation combined with Methylprednisolone in treatment of acute COPD has significant effects, which can effectively improve the blood gas index of patients, reduce the degree of dyspnea, and have fewer adverse reactions. [Key words] Budesonide Methylprednisolone Chronic obstructive pulmonary disease Acute phase Blood gas index Dyspnea First-author ’s address: Yangjiang Jianghua Hospital, Yangjiang 529500, China 慢性阻塞性肺疾病(chronic obstructive pulmonary disease,COPD)是呼吸科常见疾病,以老年人群较为多发,随着我国老龄化社会日益深入,我国COPD 患病人数日益增加[1]。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
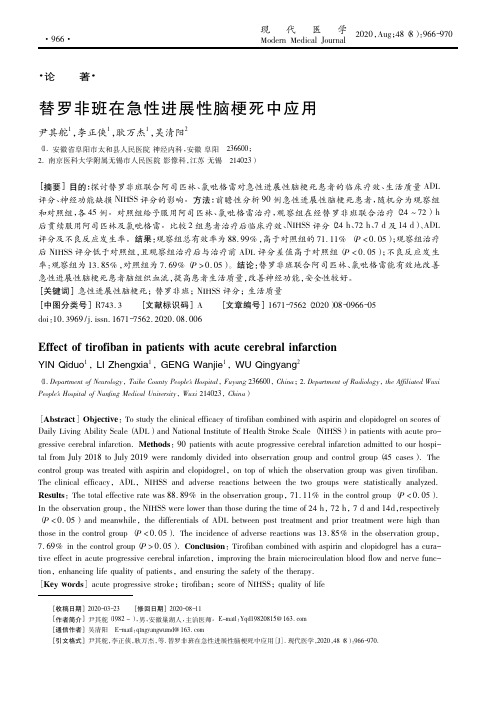
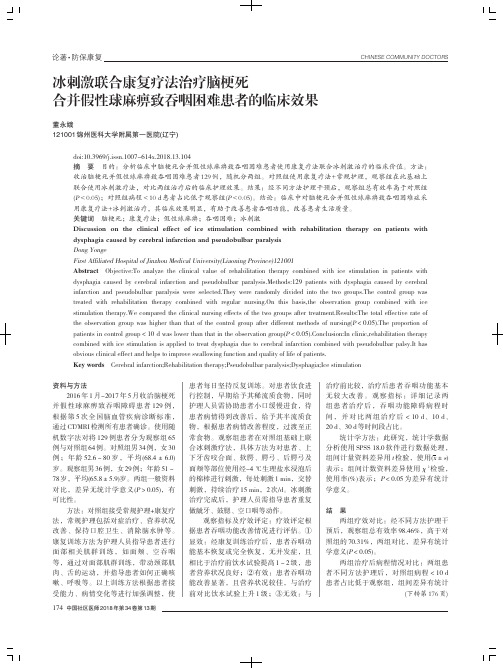
Clinical Evaluation of an Aerolysin-BasedScreening Test for Paroxysmal NocturnalHaemoglobinuriaPietro Edmondo Peghini*and Jo¨rg FehrDivision of Haematology,Department of Internal Medicine,University Hospital Zurich,Zurich,SwitzerlandBackground:Recently,a toxin produced by Aeromonas hydrophila was demonstrated to bind directly to the glycosyl-phosphatidyl-inositol(GPI)anchor.After coupling it to afluorescent dye and applying it in fluorescence-activated cell scanning(FACS),this property was exploited to detect GPI-negative cells in the diagnosis of paroxysmal nocturnal haemoglobinuria(PNH).Methods:We used this reagent according to a very simple staining protocol followed by single-colour FACS and compared the results in patients with PNH and normal controls with those obtained with anti-body-mediated detection of cells lacking GPI-anchored proteins.Results:We observed very good concordance between the two methods,with correlation coefficients (R2)of quantified GPI-deficient cell populations ranging from0.952to0.969.The lower limit of detection was determined at0.50%GPI-negative cells,which was in the range obtained with double-colour stain-ing with antibodies(0.20–1.00%,depending on the antibody).A significant correlation was observed between the fraction of GPI-negative granulocytes and laboratory parameters of haemolysis,with the erythrocyte creatine having the best correlation(R2¼0.671,P<0.0001).Conclusions:Using this protocol,we were able to reliably diagnose PNH with a high sensitivity.The test allows the identification of GPI-negative granulocyte populations as small as0.5%.q2005Wiley-Liss,Inc. Key terms:paroxysmal nocturnal haemoglobinuria;FLAER;haemolysis;immunophenotypingFor many years the diagnosis of paroxysmal nocturnalhaemoglobinuria(PNH)was made by demonstrating thesusceptibility to complement-mediated lysis(1,2).Subse-quently,demonstration of the absence of glycosyl-phospha-tidyl-inositol(GPI)–anchored proteins from the cell surfaceusing antibodies andfluorescence-activated cell scanning(FACS)largely served to replace this approach(3–5).Typi-cally,only a fraction of the cells shows the PNH immuno-phenotype,and it is the demonstration of two cell popula-tions,one positive and one negative in GPI-anchored pro-teins,that is diagnostic for the disease.In different cellpopulations,various antigens are investigated.Aerolysin,the toxin of the bacterium Aeromonashydrophila,binds directly to the GPI anchor.It is secreted as an inactive protoxin,proaerolysin,that isconverted to the active form,by various mammalian pro-teases,through proteolytic removal of a C-terminal pep-tide(6,7).Aerolysin has been used in diagnostic proce-dures to demonstrate the resistance of PNH erythrocytesto aerolysin and to enrich for GPI-negative PNH cells(8,9).Also,two point mutations were introduced toobtain a protein that still binds GPI upon activation butlacks lytic activity.By coupling this mutant proaerolysin to afluorescent marker(Alexa Fluor488),a reagent (FLAER)was produced that stains cells containing GPI proteins but not PNH cells lacking GPI(10).Because this reagent detects the GPI anchor itself,it can be used to investigate all cell types,irrespective of the proteins normally expressed,except erythrocytes,which do not express the necessary activating proteases.In contrast to immunophenotyping,where several antibodies must be employed to investigate different cell populations,FLAER can provide the same information in a single reaction. We used FLAER in whole blood according to a very simple and fast staining protocol as a screening test for the diagnosis of PNH.We determined the lower limit of detection with this simple procedure and compared the results with those from conventional immunophenotyp-ing performed in parallel.In addition,results obtained *Correspondence to:Pietro E.Peghini,Division of Haematology,Uni-versity Hospital Zurich,Ra¨mistr.100,CH-8091Zurich,Switzerland.E-mail:pietro.peghini@usz.chReceived23August2004;Accepted5April2005Published online10June2005Wiley InterScience(www. ).DOI:10.1002/cyto.b.20059Cytometry Part B(Clinical Cytometry)67B:13–18(2005)q2005International Society for Analytical CytologyF IG .1.Demonstration of GPI-negative cells by antibodies and FLAER.A representative example is shown with FACS results for a patient and for a normal control.Parameters measured are as indicated.Gating was performed in a forward versus side scatter plot (Gc,granulocytes;M,monocytes).Antibodies were coupled with fluorescein isothiocyanate (FITC)or phycoerythrin (PE).Antibodies used are indicated on the axes.14PEGHINI AND FEHRwith FLAER were correlated with known parameters of haemolysis.MATERIALS AND METHODSDetection of GPI Anchor by FLAER AssayFLAER was obtained from Protox Biotech (Victoria,Canada).It was stored at 10À6M in phosphate buffered saline (PBS)at À208C.To 25m l of whole blood,anticoa-gulated with ethylenediaminetetraacetic acid or heparin,5m l of the FLAER solution was added,mixed gently,and incubated for 10to 15min in the dark at room tempera-ture.After addition of 500m l of erythrocyte lysing reagent (0.829%NH 4Cl,0.1%K 2HCO 3,and 0.0037%ethyl-enediaminetetraacetic acid in distilled water),samples were measured in parallel with a normal control by sin-gle-colour FACS analysis in channel 1,corresponding to green fluorescence,on a FACScalibur (Becton Dickinson,Basel,Switzerland).Leukocyte subpopulations were gated on a forward versus side scatter plot.A normal control was always stained in parallel.The threshold fluorescence for negative versus positive cells was set where the main peak of this normal control intersected the x-axis.ImmunophenotypingTo 100m l of whole blood,antibodies (Becton Dickin-son)were added at the dilution suggested by the manu-facturer and incubated for 15to 30min at room temper-ature in the dark.Erythrocytes were lysed with 2ml of lysing reagent and leukocytes washed once with 3ml of standard PBS and resuspended with 500m l of PBS.Leu-kocyte subpopulations were identified on a forward ver-sus side scatter plot,which allowed gating for granulo-cytes and monocytes.CD55-negative cells were investi-gated in granulocytes and monocytes in this manner.This test therefore was a single-colour fluorescence experi-ment.For dual-colour fluorescence analysis of CD16,CD24,and CD66b,a monoclonal antibody with a differ-ent fluorescent label (CD13/phycoerythrin)was added to the assay to improve the identification of myelomono-cytic cells.Thus,the investigated cell populations,granu-locytes and monocytes,were identified by virtue of their positivity for CD13and their light scatter properties.CD59staining was performed with CD3/phycoerythrin,which allowed elimination of T cells that could have con-taminated the gates for granulocytes and monocytes based on forward versus side scatter characteristics.CD14was investigated with dual-colour fluorescence analysis on monocytes.A CD64/phycoerythrin-labelled monoclonal antibody served to discern monocytes from lymphocytes contaminating the monocyte gate in for-ward versus side scatters.Lymphocytes were not ana-lysed.We investigated CD16,CD66b,CD24,CD59,and CD55on granulocytes and CD14,CD59,and CD55on monocytes.A normal control was always stained in parallel.The threshold fluorescence for negative versus positive cells was set between the two,readily visible populations in samples with an obvious PNH component.In cases with-out two clear populations,the threshold was set below the dot cloud in the normal control in such a manner that only events clearly separated from this dot cloud were counted as nonfluorescent.Statistical AnalysisLinear correlation and calculation of the correlation coefficient (R 2)were performed with StatView software.RESULTSDemonstration of GPI-Negative CellsGPI-deficient cells were sought by using antibodies as indicated in Materials and Methods and FLAER in sevenTable 1Percentage of GPI-Negative Cells in Granulocytes and Monocytes With FLAER and Various Antibodies*Patient no.Diagnosis %Negative granulocytes %Negative monocytesPNH clone FLAER CD16CD24CD55CD59CD66b FLAER CD14CD55CD591PNH 40292522242643373231Yes 2PNH 981001009910099961009996Yes 3AA/PNH 101199991091234Yes 4MDS0.3 1.50.1 1.90.10.10.30.3 1.2 1.5No 5MDS/PNH516753616741633759Yes 516869535465415047Yes 27372827222621321830Yes*Values were rounded to the nearest integer.The two values missing are due to technical errors.Patient 5was measured three times on different occasions during treatment with antilymphocyte globulin and ciclosporin.AA,aplastic anemia;MDS,myelodys-plastic syndrome.Table 2Correlation Coefficients Between FACS Mediated byFluorescent Antibodies or FLAER in Granulocytes or Monocytes*R 2FLAER GcFLAER MonoGc CD160.959Gc CD240.950Gc CD550.9680.956Gc CD590.9690.901Gc CD66b 0.957CD140.918*Excellent correlation was observed,demonstrating compa-rable accuracy of the two methods in quantifying PNH cells.Gc,granulocytes;Mono,monocytes.15AEROLYSIN-BASED TEST FOR PNHmeasurements in five patients and seven normal con-trols.Figure 1shows the FACS results of patient 5and the respective normal control.Diagnoses were PNH in two,myelodysplastic syndrome (MDS)with a PNH clone in one,MDS without a PNH clone in one,and aplastic anaemia with a PNH clone in 1patient (Table 1).Rele-vant GPI-negative cell populations were observed in four of five patients and in none of seven controls (controls not shown).These results,expressed as dichotomousvalues of PNH clone present or PNH clone absent,were completely concordant between the two methods (Table 1,last column).Correlation Between FACS Mediated by AntibodyVersus FLAER Fourteen measurements of antibody-mediated FACS were performed in parallel with FLAER analysis.The nonfluorescent fraction was determined for each investi-gation and the correlation was determined bylinearF IG .2.Regression plots of nonfluorescent fractions from FACS medi-ated by FLAER versus fluorescent monoclonal antibodies.Representa-tive examples of regression plots are shown.Values on the axes repre-sent percentages of nonfluorescent cells.FLAER is always on the verti-cal axis,and monoclonal antibodies are as indicated on the horizontal axis.Correlation coefficients (R 2)are given in the plots.Gc,granulo-cytes;Mono,monocytes.Table 3Fluorescence-Negative Events in Normal Controls by FLAERAnalysis and Antibody-Mediated FACS*FLAERCD16CD66b CD24CD59CD55n 5077777Mean 0.049 2.4510.1130.2470.143 1.053Minimum 0.000.850.040.000.000.07Maximum 0.488.310.260.990.573.62*Values are percentages of nonfluorescent granulocytes gated by forward versus sidescatter.F IG .3.Percentile plot of fluorescence-negative events in FLAER ver-sus fluorescent monoclonal antibody-mediated FACS in normal con-trols.Values on the vertical axis are percentages of fluorescence-nega-tive events.Percentiles are indicated on the horizontal axis.Only the granulocyte (Gc)gate was investigated.A:FLAER versus antibodies used in a dual-colour FACS experiment.B:FLAER versus CD55stain-ing that was performed as a single-colour FACS experiment.16PEGHINI AND FEHRregression analysis.Correlation coefficients (R 2)and regression plots are presented in Table 2and Figure 2,respectively.Excellent correlations between PNH popu-lations detected by the two methods were observed,demonstrating a comparable accuracy of the two meth-ods for the quantification of PNH cells.Lower Limit of DetectionFor analysis of the lower limit of detection,only granu-locytes were investigated because they represent the largest fraction and were more easily gated in the for-ward versus side scatter plot.Fifty normal control sam-ples were assayed by FLAER and seven by immunophe-notyping.Values between 0%and 0.48%FLAER-negative events were counted in the granulocyte gate.The values observed with fluorescent antibodies were in the same range in double-colour FACS results,as presented in Table 3and by a percentile plot in Figure 3A.However,we performed the CD55staining as a single-colour fluo-rescence assay,and a higher background was observed (0.07–3.62%;Fig.3B).In addition,in CD16staining,higher values were measured in normal controls,but this was due to the absence of CD16from normal eosi-nophil granulocytes.In 50normal controls,the highest value of fluorescence-negative events with FLAER was 0.48%.Therefore,a lower limit of detection can be set at 0.5%.FLAER Correlates With Haemolytic ActivityThe fraction of FLAER-negative cells as a percentage correlated only very weakly with the parameters of hae-molysis LDH,reticulocyte count,and bilirubin.A weak but definitely better correlation was found with the hae-molysis parameter of erythrocyte creatine (R 2¼0.671,P <0.0001;Fig.4)(11).DISCUSSIONPNH enters the differential diagnosis in every case of Coombs-negative haemolysis.In addition,it has recently been shown that patients with myelodysplastic syndrome carrying a PNH clone,even if it is very small,respond more readily to immunosuppressive treatment (12).Therefore,although PNH is a rare disease,it is quite fre-quently investigated,and a simple,reliable screening test with sufficient sensitivity for small PNH clones would be of benefit.Haemolysis in PNH arises from a lack of complement inhibitors from the surface of erythrocytes.This is due to the inability of these cells to synthesize the GPI anchor.Until a few years ago,diagnosis had to rely on indirect methods that demonstrated increased suscepti-bility to complement-mediated lysis (1,2)or the lack of GPI-anchored proteins by immunological methods (3–5).With aerolysin,the toxin of A.hydrophila ,which specif-ically binds to the GPI anchor,a more straightforward diagnostic approach has become possible (10).We have shown that the diagnosis of PNH can be made reliably using this reagent with a very simple and rapid staining protocol and single-colour fluorescence detection.Nonfluorescent events in the FACS analysis of normal controls were always less than 0.5%of peripheral granulocytes.Therefore,the test has a lower limit of detection for PNH clones as small as 0.5%.A comparable performance was obtained with monoclonal antibodies only with dual-colourstaining.F IG . 4.Correlation between the number of FLAER-negative cells and parameters for haemolysis.Linear correlation plots compare percentages of FLAER-nega-tive cells with known parameters of haemolysis.The best correlation was observed with erythrocyte creatine (ec crea;P <0.0001)(11),although all correlations were rather weak.Gc,granulocytes;LDH,lactate de-hydrogenase.17AEROLYSIN-BASED TEST FOR PNHProbably by counterstaining the cell population of interest with an antibody labelled with a secondfluores-cent dye in a FLAER experiment,the lower limit of detection for GPI-negative cells could be decreased. However,this was not the goal of the present method, which was deliberately designed as a rapid and simple screening test for routine analysis.Lymphocytes could not be investigated with the present method because the gating strategy did not per-mit separating them reliably from remaining non-lysed erythrocytes and probably erythrocyte ghosts.Staining with an antibody carrying a secondfluorescent label would likely solve this problem in a setting where the investigation of lymphocytes was important.Moreover, erythrocytes are not amenable to analysis by FLAER because they lack the proteases necessary for proteolytic activation of proaerolysin(10).Because the percentage of FLAER-negative cells corre-lated to a certain degree with haemolytic activity,it can be used as a follow-up parameter to estimate disease severity and response to treatment.In conclusion,by using this very rapid FLAER-based protocol for FACS,we were able to reliably detect GPI-negative cell populations in patients carrying a PNH clone.PNH clones as small as0.5%were readily detected.Because of its simplicity and correlation to hae-molytic activity,this test also lends itself to serial follow-up of the course of PNH.ACKNOWLEDGMENTSWe thank Mrs.Ruth Kalberer,Mrs.Evelyne Giabbani, Mrs.Michelle Handschin,Mrs.Francesca Bianda,and Mrs.Leta Fuchs for excellent technical assistance in FACS.LITERATURE CITED1.Hartmann RC,Jenkins DE.Sugar-water test for paroxysmal noctur-nal hemoglobinuria.N Engl J Med1966;275:155–157.2.Hartmann RC,Jenkins DE,Arnold AB.Diagnostic specificity ofsucrose hemolysis test for paroxysmal nocturnal hemoglobinuria.Blood1970;35:462–475.3.van der Schoot CE,Huizinga TW,ET vtV-K,Wijmans R,Pinkster J,dem Borne AE.Deficiency of glycosyl-phosphatidylinositol-linked membrane glycoproteins of leukocytes in paroxysmal nocturnal hemoglobinuria,description of a new diagnostic cytofluorometric assay.Blood1990;76:1853–1859.4.Hall SE,Rosse WF.The use of monoclonal antibodies andflowcytometry in the diagnosis of paroxysmal nocturnal hemoglobinuria.Blood1996;87:5332–5340.5.Schubert J,Alvarado M,Uciechowski P,et al.Diagnosis of paroxys-mal nocturnal haemoglobinuria using immunophenotyping of peripheral blood cells.Br J Haematol1991;79:487–492.6.Howard SP,Buckley JT.Activation of the hole-forming toxin aeroly-sin by extracellular processing.J Bacteriol1985;163:336–340.7.Garland WJ,Buckley JT.The cytolytic toxin aerolysin must aggre-gate to disrupt erythrocytes,and aggregation is stimulated by human glycophorin.Infect Immun1988;56:1249–1253.8.Mukhina G,Buckley T,Brodsky RA.A rapid spectrophotometricscreening assay for paroxysmal nocturnal hemoglobinuria.Acta Hae-matol2002;107:182–184.9.Brodsky RA,Mukhina GL,Nelson KL,Lawrence TS,Jones RJ,Buck-ley JT.Diagnosis of paroxysmal nocturnal hemoglobinuria(PNH) and selection of small PNH populations using a novel GPI-anchor binding toxin,aerolysin.Blood1998;92:472A.10.Brodsky RA,Mukhina GL,Li S,et al.Improved detection and char-acterization of paroxysmal nocturnal hemoglobinuria usingfluores-cent aerolysin.Am J Clin Pathol2000;114:459–466.11.Fehr J,Knob parison of red-cell creatine level and reticulo-cyte count in appraising the severity of hemolytic processes.Blood 1979;53:966–976.12.Dunn DE,Tanawattanacharoen P,Boccuni P,et al.Paroxysmal noc-turnal hemoglobinuria cells in patients with bone marrow failure syndromes.Ann Intern Med1999;131:401–408.18PEGHINI AND FEHR。