IPCEA Shoulder Pain Lindley 2017
左室压力-应变环定量评估肥厚型心肌病患者心肺运动试验前后左室功能变化
·临床研究·左室压力-应变环定量评估肥厚型心肌病患者心肺运动试验前后左室功能变化侯淑红林瑜芬吴波孙林林李章静张力陈东平摘要目的应用左室压力-应变环(LVPSL)定量评估肥厚型心肌病(HCM)患者心肺运动试验(CPET)前后左室心肌做功变化。
方法选取我院经超声心动图或心脏MRI确诊的非梗阻性HCM患者55例(HCM组)和同期健康志愿者55例(对照组),应用常规超声心动图测量左室舒张末期内径(LVEDd)、左室收缩末期内径(LVEDs)、左房收缩末期内径(LAD)、舒张末期室壁厚度(MWT)、左室射血分数(LVEF)及二尖瓣口舒张早期血流峰值速度与二尖瓣环舒张早期运动峰值速度比值(E/e’),二维斑点追踪及LVPSL技术获取CPET前后整体纵向应变(GLS)、纵向应变达峰时间离散度(PSD)及左室心肌整体做功指数(GWI)、整体有用功(GCW)、整体无用功(GWW),比较两组上述参数的差异。
结果HCM组MWT、LAD、E/e’均较对照组增加,差异均有统计学意义(均P<0.05);两组LVEDd、LVEDs、LVEF比较差异均无统计学意义。
CPET前,HCM组GLS、GCW、GWI均较对照组减低,GWW、PSD均较对照组增加,差异均有统计学意义(均P<0.05);CPET后,HCM组GLS、GCW、GWI均较对照组减低,GWW、PSD均较对照组增加,差异均有统计学意义(均P<0.05)。
HCM组CPET后GLS较CPET前减低,PSD较CPET前增加,差异均有统计学意义(均P<0.05);HCM组CPET前后GCW、GWW、GWI比较差异均无统计学意义。
对照组CPET后GCW、GWW、GWI均较CPET前增加,差异均有统计学意义(均P<0.05);CPET前后GLS、PSD比较差异均无统计学意义。
结论LVPSL可定量评估HCM患者CPET前后左室心肌做功变化,为临床早期干预、优化治疗策略、指导个体化运动提供参考依据,具有一定的临床参考价值。
冻结肩的研究进展

Advances in Clinical Medicine 临床医学进展, 2023, 13(5), 7761-7764 Published Online May 2023 in Hans. https:///journal/acm https:///10.12677/acm.2023.1351084冻结肩的研究进展董 悦,滕俊超*,杨国帅,孟凡刚,张泽南青岛大学附属医院胸外科,山东 青岛收稿日期:2023年4月16日;录用日期:2023年5月9日;发布日期:2023年5月16日摘要冻结肩也称肩周炎,为一种常见的肩关节疾病,主要表现为肩关节疼痛和活动受限。
其病因不明确,对冻结肩的定义和诊断也存在一定误区。
综述旨在回顾冻结肩的定义、流行病学、分类、诊断、鉴别诊断和治疗方法,为冻结肩的诊断提供理论基础。
关键词肩周炎,冻结肩,肩关节疼痛,活动受限Research Progress of Frozen ShoulderYue Dong, Junchao Teng *, Guoshuai Yang, Fangang Meng, Zenan ZhangDepartment of Thoracic Surgery, Affiliated Hospital of Qingdao University, Qingdao Shandong Received: Apr. 16th , 2023; accepted: May 9th , 2023; published: May 16th , 2023AbstractFrozen shoulder, also known as periarthritis of shoulder, is a common shoulder joint disease, mainly manifested by shoulder joint pain and limited activity. Its etiology is not clear, some mi-sunderstandings also exist in the definition and diagnosis of frozen shoulder. The purpose of this review is to review the definition, epidemiology, classification, diagnosis, differential diagnosis and treatment of frozen shoulder, and to provide a theoretical basis for the diagnosis of frozen shoulder. KeywordsPeriarthritis of Shoulder, Frozen Shoulder, Shoulder Joint Pain, Limited Movement*通讯作者董悦等Copyright © 2023 by author(s) and Hans Publishers Inc.This work is licensed under the Creative Commons Attribution International License (CC BY 4.0)./licenses/by/4.0/1. 冻结肩的定义随着生活方式的改变,肩部疼痛的患者越来越多,其中冻结肩的比重最大。
癌痛的阿片类药物治疗【30页】

†例:60mg口服吗啡相当于25ug/h芬太尼透皮贴剂(相当于0.6mg/24h)
19
8.其它给药途径
• 不能口服或无法应用透皮贴剂者,可首选皮 下给药途径;
• 合并皮下给药的禁忌症时,应考虑静脉给药。 • 需要迅速控制疼痛时,宜用吗啡静脉滴定。
20
9.爆发痛的阿片类药物治疗
• 因未控基础性疼痛所致的疼痛加重,给予即释型口服阿片药 物治疗,但要首先对每日按时服用的阿片类镇痛药物剂量进 行调整,而不是一味增加解救治疗的剂量。
• 阿片相关性呕吐的治疗 • 阿片相关性便秘的治疗 • 阿片所致CNS症状的治疗 • 肾衰患者的阿片药物应用 • 对乙酰氨基酚和NSAID与
第三阶梯药物的联合应用 • 神经病理性疼痛的辅助镇
痛药物 • 阿片类药物的脊髓给药
10
1. 第二阶梯药物
• 轻至中度疼痛及规律口服Aceta或NSAID仍 不能满意控制者,二阶梯药物可增效。
• Meta分析(Meta-analysis)作为系统综述中使
用的一种统计方法,过去20年间在医学研究领域
也得到了广泛的应用。
一般性综述 系统综述
Meta-分析
9
癌痛的阿片类药物治疗 -- EAPC基于EBM的推荐(16项)
• 二阶梯药物 • 首选的三阶梯药物 • 阿片滴定 • 阿片转换 • 镇痛效能比 • 美沙酮的作用 • 透皮吸收的剂型 • 其它给药途径 • 爆发痛的治疗
期刊 BMJ 1996; 312: 823-826. British Journal of Cancer 2001; 84:
587–593. Lancet Oncology 2012; 13:e58-68.
6
关于GRADE系统
Philips HeartStart Intrepid监护 除颤器TBI建议说明书
Application notePhilips HeartStart Intrepidmonitor/defibrillator TBI advisory OverviewThe TBI advisory feature on the HeartStart Intrepidassists in the monitoring of patients who are determinedat high risk of having suffered a traumatic brain injury.The TBI advisory provides visual guidance to helpprevent the following conditions:• Hypoxia – low blood oxygen saturation(as measured by SpO 2)• Hypotension – low systolic blood pressure• Hyperventilation-induced hypocapnia – decreasedcarbon dioxide in the blood (as measured by EtCO 2).The TBI advisory is available for both adult and infant/child patients on devices in Monitor Mode configured with SpO 2, NBP, and EtCO 2. The TBI advisory display reflects the appropriate target limits for each TBI Care parameter.IntroductionEvery year, 2.2 million people in the UnitedStates suffer a traumatic brain injury (TBI), with approximately 52,000 deaths and 280,000 hospitalizations.1 The economic burden of TBI is more than USD 60 billion per year.1 TBI occurs when an external mechanical force inflicts sudden trauma to the head disrupting the normal function of the brain.2However, subsequent preventable (secondary) injury to the brain can add dramatically to the primary injury, and the extent of damage during this time is significantly influenced by the early care the patient receives.3 The emphasis on early recognition and early treatment of TBI should be similar to that of other pathologies where survivability and recovery are time-dependent, i.e., sudden cardiac arrest.4TBI PathophysiologyThe brain accounts for the consumption of 20% of bodily oxygen and 25% of the blood glucose. Because of this, cerebral blood flow (CBF) is critical for ensuring adequate brain metabolism and preventing cerebral ischemia. CBF is a function of cerebral perfusion pressure (CPP) and cerebral vascular resistance (CVR), CPP is calculated by subtracting intracranial pressure (ICP) from mean arterial blood pressure (MAP) (CPP= MAP-ICP). Normal ICP ranges from 10-15 mmHg, and normal MAP ranges from 70-95 mmHg; therefore, the average CPP is approximately 60-80 mmHg. CBF is regulated through several mechanisms in the healthy patient; however, disruption of those mechanisms can have catastrophic consequences on the brain and its control of body systems.ICP and TBIThe cerebrum, cerebellum, and brainstem use approximately 80% of the intracranial space (1,200 cc), with blood vessels and cerebral spinal fluid utilizing the remaining volume at 12% (150 cc) and 8% (90 cc), respectively. Cerebral swelling and hemorrhage secondary to TBI increase the cerebral volume and require the body to compensate for the increased volume by reducing the volume of other brain structures and cerebrospinal fluid within the cranium. If the amount of room available to compensate forthe increasing volume is less than the expanding volume, then an increase in ICP will occur. Initially,the brain compensates for an increase in cerebral mass by compressing the cerebral venous blood vessels and, as cerebral volume continues to increase, cerebrospinal fluid is pushed from the skull into the spinal space. The initial compensatory mechanisms can maintain ICP close to normal; however, once those mechanisms are exhausted, ICP quickly rises. The continued increase in ICP impedes arterial flow into the cranial space and constricts cerebral blood vessels. These mechanisms decrease CBF and, subsequently, the cardiocerebrovascular system attempts to compensate for the decreased CBF by increasing SBP. This further increases ICP.The decreased CBF also causes cerebral ischemiaand neuronal hypoxia. If spontaneous ventilationis compromised, pCO2increases, and this results in cerebral vasodilation and additional increases in ICP. Cerebral edema secondary to neuronal injury and cerebral ischemia leads to a further exacerbation of ICP. Ultimately, the continued increase of ICP will lead to profoundly compromised CBF, resulting in death. Figure 1.552Three critical factors of TBI (the 3 H-Bombs)The National EMS TBI Guidelines published by theBrain Trauma Foundation emphasize the importanceof maintaining adequate cerebral oxygenation andperfusion by avoiding three critical factors.7• Hypoxia• Hypotension• Hyperventilation (that leads to hypocapnea andcerebral vasoconstriction)A single incidence of any one of these factorsdramatically increases patient mortality.3 However,maintaining End-Tidal Carbon Dioxide (EtCO2), arterialblood oxygenation (SpO2), and a systolic bloodpressure (SBP) within guidelines established by theTraumatic Brain Injury Foundation have demonstratedimproved outcomes in patients with severe TBI.3HypocapniaPreventing hyperventilation induced hypocapnia(EtCO2<32 mmHg) is critical because of its directcorrelation to CBF.3,7 For example, a patient who hasa pCO2 of 40 mmHg has a CBF of 50 ml per 100g ofbrain tissue per minute.8 However, if pCO2drops to30 mmHg, then CBF will drop to 40ml per 100g ofbrain tissue per minute, a 20% decrease in CBF.8 Therelationship between CBF and pCO2is so delicate thata 1 mmHg change in pCO2can alter CBF up to 5% anddecreasing pCO2by relatively little (i.e., <32 mmHg) isassociated with significant mortality.3,8-10Unfortunately, unrecognized inadvertenthyperventilation in TBI patients is still a majorproblem, at least in the prehospital environment. Inthe San Diego RSI Trial, 59% of patients intubatedbefore arriving at the hospital experienced at leastone incident of hyperventilation resulting in anEtCO2value of less than 25 mmHg.9 The importanceof monitoring EtCO2cannot be overstated. Onestudy observed that prehospital intubation in asetting where capnography was not used reporteda mortality rate of 33%; conversely, the ability tomonitor patients’ EtCO2level and use a ventilator wasassociated with a statistically significant, 18% lowerrelative rate of death.11Figure 1: Relationship between increased intracranial pressure and decreased cerebral perfusion.34Hypotension and hypoxiaMultiple studies have demonstrated a strong correlationbetween a single episode of hypotension (SBP <90mmHg) or hypoxia (SpO 2<90%) and decreased patientsurvival.7,12-14 Independently, hypotension or hypoxiahave a dramatic deleterious effect on patient mortality.However, when a patient experiences both hypotensionand hypoxia, the adjusted probability of death doublesagain (beyond that of either alone).15The Excellence in Prehospital Injury Care (EPIC)TBI study examined the outcome of 13,151 patientswho had suffered major (moderate/severe/critical)TBI over a seven-year period. The researcherscompared the mortality rate of patients whoexperienced neither hypoxia nor hypotension(n=11,545), hypotension only (n=604), hypoxia only(n=790), or hypotension and hypoxia (n=212) in theprehospital environment.15 The study concludedthat having at least one episode of hypotension orhypoxia (alone) resulted in a 20.7% (n=125) and 28.1%(n=222) mortality rate, respectively. The combinationof both hypoxia and hypotension was associated witha 43.9% (n=93) mortality rate.15 Comparatively, patients who did not experience hypoxia or hypotension had a 5.6% (n=644) rate of death.15 The adjusted analysis found that a patient that experiences both hypotension and hypoxia in the prehospital environment has a 600% (aOR = 6.1) higher likelihood of dying than someone who experiences neither.15Another important finding of the EPIC TBI study was the absence of any identifiable SBP threshold in relation to patient mortality. The study identified that over the range of 40 mmHg to 120 mmHg SBP there was a consistent decrease in survival for every 10 mmHg drop and a progressive association between decreasing SBP and both unadjusted and adjusted risk of death.1 In other words, a patient with a SPB of 60 mmHg is 4 times as likely to die than a patient with a SBP of 135 mmHg.1 The implications are obvious: the injured brain is highly sensitive to a lack of perfusion, and the levels of systemic blood pressure associated with increased mortality may be far above the “classic” threshold for “hypotension” (SBP<90 mmHg).1Importance of treating and preventing hypotension, hypoxia, and hypocapnia Researchers from the EPIC TBI study worked with ArizonaEMS agencies to implement prehospital TBI guidelinesfocusing on three areas of prevention and treatment (thethree “H-Bombs”):• Preventing and treating hypoxia by use of high-flowO 2 and emphasis on basic airway maneuvers• Preventing and treating hypotension by rapidlyinfusing isotonic fluids• Preventing hyperventilation by using appropriateventilation rates, adjuncts, and EtCO 2In the EPIC Study, adjusted survival to hospital dischargedoubled (aOR 2.03) for patients with severe TBI (headregion severity score = 3-4) and tripled (aOR 3.28) forpatients with severe TBI that also received positivepressure ventilation (PPV) via bag-valve mask orendotracheal intubation (ETI). The increased survival ofpatients with severe TBI receiving PPV was attributedto the emphasis on maintaining EtCO 2 between 35 and 45 mmHg, rate-timers that gave visual cues for proper manual ventilation and using flow-controlled ventilation bags to help prevent hyperventilation and overventilation.One of the most important findings of the EPIC Study was that the initial improvement of patient survival faded over time, and this was most likely because of the diminished emphasis on following the prehospital TBI guidelines. The researchers could not require retraining of the study participants. Therefore, a method of ensuring that hypoxia, hypotension, and hypocapnea are recognized early should be available to all prehospital providers. The authors concluded that their findings make it likely that the use of monitoring technology that can give cues and real-time feedback to providers during the resuscitation of brain injured patients will improve outcomes by helping to prevent secondary brain injury from hypoxia, hypotension, and hyperventilation.10HeartStart Intrepid Traumatic Brain Injury advisory OverviewThe TBI advisory feature on the HeartStart Intrepidassists in the monitoring of patients who are determinedat high risk of having suffered a traumatic brain injury.The TBI advisory provides visual guidance to helpprevent the following conditions:• Hypoxia – low blood oxygen saturation (asmeasured by SpO2)• Hypotension – low systolic blood pressure• Hyperventilation-induced hypocapnea – decreasedcarbon dioxide in the blood (as measured by EtCO2).The TBI Advisory is available for both adult and infant/child patients on devices in Monitor Mode configuredwith SpO2, NBP, and EtCO2. The TBI Advisory displayreflects the appropriate target limits for each TBI Care parameter.Notes:• These limits must be pre-established andpre-configured prior to using this feature (see “Configuration – TBI Advisory” in the HeartStart Intrepid Instructions for Use).• If a physiological alarm condition occurs, it will have a higher priority than the TBI advisory and will obscure the TBI Indicators.56Enabling the TBI advisory1. TBI: Ensure an SpO 2 sensor, NBP cuff, and EtCO 2 tubing are connected to the patient2. Press the [Enable TBI] soft key.If no patient age has been entered, the Patient Age number selector appears.3. If prompted, enter the patient age.The patient age is displayed in the status area next to patient name/ID.When age is entered, mode text changes from Monitor to Monitor TBI.Notes:• The TBI Advisory is only available in Monitor Mode and is not available during the acquisition of a 12-lead ECG.• Devices must be configured with SpO 2, NBP, andEtCO 2 measurement parameters, and all threeparameters must be in use.• TBI Advisory can only be enabled when TBI limits are pre-configured on the device.• The neonatal patient category is not supported.Displaying the TBI advisoryThe TBI advisory display appears in the numeric parameter area. A TBI limit bar is displayed at the top of the corresponding measure box for NBP , EtCO 2, and SpO 2.TBI for systolic blood pressure (SBP)Systolic blood pressure that falls outside theestablished TBI limits is indicated by a yellow bar, and TBI SBP > High Limit or TBI SBP < Low Limit is displayed, as shown in Figure 2.Systolic blood pressure within limits the setting for the TBI configuration is indicated by TBI SBP on a green bar, as shown in Figure 3.TBI for EtCO 2 If the EtCO 2 value falls outside the established TBI limits, TBI EtCO 2 > High Limit or TBI EtCO 2 < Low Limit is displayed in a yellow TBI bar as shown in Figure 4.If the EtCO 2 value is within the limits setting for the TBI configuration, TBI EtCO 2 is displayed in a green bar as shown in as shown in Figure 5.WARNING: To ensure correct functioning of the CO 2 measurement, use only approved CO 2 accessories as listed in the HeartStart Intrepid Instructions for Use, Chapter 18:Supplies and Accessories.Figure 5: TBI within limits.Figure 2: TBI outside limits.Figure 3: TBI within limits.Figure 4: TBI outside limits.7TBI for SpO 2For SpO 2, there is no upper limit, only a lower limitthreshold for SpO 2 is set. If the SpO 2 value falls belowthe established TBI limit, TBI SpO 2 < Low Limit isdisplayed on a yellow TBI bar as shown in Figure 6.If the SpO 2 value is above the limit set for the TBIconfiguration, the TBI bar is green, and the text TBI SpO 2is displayed on a green bar as shown in Figure 7.Figure 6: SPO 2below TBI limit.Figure 7: SPO 2 above TBI limit.References1. Spaite, D. W., Hu, C., Bobrow, B. J., Chikani, V., Sherrill,D., Barnhart, B., . . . Adelson, P. D. (2017). Mortality andprehospital blood pressure in patients with majortraumatic brain injury: Implications for the hypotension threshold. JAMA Surgery, 152(4), 360-368.2. Rosenfeld, J. V., Maas, A. I., Bragge, P., Morganti-Kossmann, M. C., Manley, G. T., & Gruen, R. L. (2012).Early management of severe traumatic brain injury.The Lancet, 380(9847), 1088-1098.3. Spaite, D. W., Bobrow, B. J., Stolz, U., Sherrill, D., Chikani,V., Barnhart, B., . . . Denninghoff, K. R. (2014). Evaluation of the impact of implementing the emergency medical services traumatic brain injury guidelines in arizona:The excellence in prehospital injury care (epic) study methodology. Academic Emergency Medicine, 21(7), 818-830. doi:doi:10.1111/acem.12411.4. Gaither, J. B., Spaite, D. W., Bobrow, B. J., Denninghoff,K. R., Stolz, U., Beskind, D. L., & Meislin, H. W. (2012).Balancing the potential risks and benefits of out-of-hospital intubation in traumatic brain injury:The intubation/hyperventilation effect. Annals ofEmergency Medicine, 60(6), 732-736.5. Bledsoe, B. E., Porter, R. S., & Cherry, R. A. (2001). Head,facial, and neck trauma. In Paramedic care: Principles & practices trauma emergencies (1 ed., Vol. 4, pp. 285-286). Upper Saddle River, NJ: Prentice Hall.6. Sanders, M. J. (2012). General principles ofpathophysiology. In K. McKenna, L. M. Lewis, & G.Quick (Eds.), Mosby’s paramedic textbook (4th ed., pp.211-256). Burlington, MA: Jones & Bartlett Learning.7. Carney, N., Totten, A. M., O’Reilly, C., Ullman, J. S.,Hawryluk, G. W., Bell, M. J., . . . Ghajar, J. (2017).Guidelines for the management of severe traumaticbrain injury, fourth edition. Neurosurgery, 80(1), 6-15.doi:10.1227/NEU.0000000000001432.8. Giardino, N. D., Friedman, S. D., & Dager, S. R.(2007). Anxiety, respiration and cerebral bloodflow: Implications for functional brain imaging.Comprehensive Psychiatry, 48(2), 103-112.9. Davis, D. P., Heister, R., Poste, J. C., Hoyt, D. B., Ochs, M.,& Dunford, J. V. (2005). Ventilation patterns in patients with severe traumatic brain injury following paramedic rapid sequence intubation. Neurocritical Care, 2(2),165-171. 10. Spaite, D. W., Bobrow, B. J., Keim, S. M., Barnhart, B.,Chikani, V., Gaither, J. B., . . . Hu, C. (2019). Association of statewide implementation of the prehospital traumatic brain injury treatment guidelines with patient survival following traumatic brain injury: The excellence inprehospital injury care (epic) study. JAMA Surgery,e191152-e191152. doi:10.1001/jamasurg.2019.1152.11. Poste, J. C., Davis, D. P., Ochs, M., Vilke, G. M.,Castillo, E. M., Stern, J., & Hoyt, D. B. (2004). Airmedical transport of severely head-injured patientsundergoing paramedic rapid sequence intubation.Air Medical Journal, 23(4), 36-40. doi:https://doi.org/10.1016/j.amj.2004.04.006.12. Shutter, L. A., & Narayan, R. K. (2008). Blood pressuremanagement in traumatic brain injury. Annals ofEmergency Medicine, 51(3, Supplement), S37-S38.doi:https:///10.1016/j.annemergmed.2007.11.013.13. Cormio, M., Robertson, C. S., & Narayan, R. K. (1997).Secondary insults to the injured brain. Journal ofClinical Neuroscience, 4(2), 132-148. doi:https://doi.org/10.1016/S0967-5868(97)90062-X.14. Manley, G. (2001). Hypotension, hypoxia, and headinjury: Frequency, duration, and consequences.Archives of Surgery, 136(10), 1118-1123.15. Spaite, D. W., Hu, C., Bobrow, B. J., Chikani, V., Barnhart,B., Gaither, J. B., . . . Sherrill, D. (2017). The effect ofcombined out-of-hospital hypotension and hypoxia on mortality in major traumatic brain injury. Annalsof Emergency Medicine, 69(1), 62-72. doi:10.1016/j.annemergmed.2016.08.007.8。
明星IP营销 小鬼王琳凯代言德国ISANA安瓶系列

明星IP营销小鬼王琳凯代言德国ISANA安瓶系列2018年,Nine Percent正式出道,团内成员一跃成为现下热门流量小生。
与此同时,流行节目带来的粉丝经济让众多品牌都开始摩拳擦掌,利用明星IP提高品牌知名度和美誉度成为了品牌方司空见惯的操作。
如何充分利用明星IP,通过社交媒体来提高消费者对品牌的辨识度,使得曝光量和转化率最大化,成为了品牌方新的思考契机。
今年10月,德国日化用品专家ROSSMANN在经过对市场和消费者的全方位洞悉后,选择了Nine Percent成员,新晋实力派偶像—小鬼王琳凯作为ROSSMANN子品牌ISANA安瓶系列代言人,并拍摄了“安瓶加你,余生不换”主题系列宣传片造势,从传统的电商模式转型,稳扎稳打地开始了新一轮的营销部署,在定位的消费者和粉丝群体中掀起了一阵安瓶护肤的时尚热潮,收获了大批精致女性群体的喜爱。
营造悬念 ISANA安瓶相关话题“突出重围”通过对安瓶消费群体的预判,ROSSMANN将此次活动的“主力战场”放置在微博这一面向年轻化、女性化,白领化的社交平台。
在10月24日,ROSSMANN官方微博放出一张倒计时照片,除了带有代言人特色的文案外,不含任何关联性的话题,营造了一种别样的悬念,引发众多粉丝进行猜想和讨论。
其后,正式官宣代言人的微博更是高达20.7w的转发量,取得了爆炸式的传播效应。
因为德国日化用品专家ROSSMANN本身严谨求实、值得信赖的品牌调性,粉丝纷纷开始自愿购买产品并进行“晒单”,相关话题的阅读量也随之水涨船高,活动热门话题#小鬼王琳凯ISANA安瓶代言人#阅读量直线上升至3000万+,在同类型产品中“突出重围”,使得小鬼本身自带的热度开始逐步向品牌本身转移。
ISANA安瓶相关话题“突出重围”(图片转自网络,版权归原作者所有)“男友向”广告视频为“琳”心动任务解锁小鬼拍摄ISANA安瓶清新概念视频(图片转自网络,版权归原作者所有)全渠道同步持续热度携手共赢在官方微博活动如火如荼的同时,ROSSMANN官方微信平台和天猫国际官方旗舰店也在配合代言活动助力热度提升。
medipro174;cataloguesupplementStumpSocks…

Stickonto Page 140 of the medipro® General CatalogueU P T O D A T E me d i p r o ®C a talo g u e s u p pl em en tThe optimum supplement to the medipro®Liner RELAX and RELAX TF/ TFCPROPERTIESR elieves or eliminates phantom pain, phantomsensations and idiopathic residual limb pain due to isolation from electromagnetic effects thanks to the metallurgical knit (Umbrellan®) D ouble-knit: protects the residual limb against cold, light bumps, friction, other external influencesKnit with temperature-regulating thread (Clima-Comfort®): • w arming and cooling function, depending on environmental tem-perature • highly elastic knit with SOFT topbands for comfortable, reliable fit – without slipping or constriction• p leasant wearing comfort due to the soft, skin-friendlyUmbrellan® and Clima-Comfort® material • n o heat build-up, as stocking is breathable and moisture- regulating thanks to the well-known Clima-Comfort® technology • particularly suitable for wearing at night and any time no prosthesis is being wornTECHNICAL DATA Material Umbrellan® with Clima-Comfort® Sizes / Length see product tableAmputation levelBelow-knee,knee disarticulation/above-knee CleaningHand wash at max. 30°C using medipro® care neutral soap M. 870.902SuppliedUmbrellan® User Set (medipro® pain diary,medipro® pain scale)Umbrellan® is a unique, patented knitted fabric that combines maximum elasticity with an excellent electromagnetic screen.The materials used on the metallurgical base are hypoallergenic, climate-regulating and have antibacterial properties.Its functionality, therapeutic benefit and quality have been statistically significantly demonstrated.Prospective randomi-sed study available as Art. No. 70.914.d i f f emedi. i feel better.140b140aHead-Office medi · Prosthetics • Medicusstr. 1 • D-95448 Bayreuth • GermanyTelephone +49 921 912 740 • Fax +49 921 912 755 • www.medi.de · medipro®New product InformationThe optimum supplement to the medipro®Liner RELAX and RELAX TF/ TFCPRODUCT TABLEArt. No. M.870.902medipro®care neutralsoap, 200 ml For thorough cleansing of the residual limb and the stocking.Best if ordered together with the stocking.99.802/09.07/3,5‘DesignationCircumference A(level of topband)Size Art. No.Length 30 cmArt. No.Length 40 cmUnit MaterialRELAX Night Care 20 – 26 cm S –1.880.322Piece Umbrellan®RELAX Night Care 26 – 33 cm M 1.880.328 1.880.323Piece Umbrellan®RELAX Night Care 33 – 42 cm L 1.880.329 1.880.324Piece Umbrellan®RELAX Night Care 42 – 52 cm XL 1.880.325 1.880.327Piece Umbrellan®RELAX Night Care52 – 62 cmXXL1.880.326–PieceUmbrellan®SIZE SE LECTION(Below-knee/knee exarticulation/above-knee)1. C hoose the suitable stocking length depending on the length of the resi-dual limb L (30 or 40 cm)*2. M easure the circumference A (at top band)3. T he residual limb length and circum-ference give the correct medipro® RELAX Night Care sizeLength of the residual limb LCircumference A at the level of the topband* Important note: m edipro®RELAX Night Care is available in two standard lengths (30 or 40 cm). Please choose the nearest size in relation to the length of the residual limb.The stocking can be carefully sewn up for residual limbs < 30 cm.N o w e v en q u i c k e ra n d e a s i e rt ome a s u r ef o r s i z e !NE W ! N E W !N E W !N E W !Maximum useful life 3 months.。
韩士生科秘特线

δ 效果立竿见影 维持时间长
δ 连续做2-3次后,维持时间可以到2年以上 δ 联合治疗 效果更佳 δ 100%生物相容性:只使用100%PDO线,确保使用安全性
适应症
泪沟 鼻唇沟 木偶问 下颌 火鸡脖Turkey neck deformity
线雕提升基本概念--方向 & 如何植入
垂直于皱纹方向
150mm
35mm
8mm
47mm
35mm
Mint lift® Fine 规格说明
▣ Mint lift Fine (15cm)
Mint lift 原材料 (Material Type) PDO长度(PDO Length) USP尺寸(USP Size) 包装规格(Package) 钝针尺寸 (Cannula Gauge) 倒钩设计 (Cog Design) 适应症(Indication) 单侧线的数量 (No. thread per side)
倒钩维持时间 Durable Barb
2 months
Mint lift® 家族
II. Mint lift® Portfolio
1. Mint 43cm Mint
2. Mint Mini 17cm
® ® ®
3. Mint Easy 43cm
®
4. Mint Fine 15cm
5. Mint lift Mono Family 6. Mint lift Co [Nose lifting]
® ®
针尺寸 (Needle Gauge) 倒钩设计 (Cog Design)
适应症(Indication)
单侧线的数量 (No. thread per side)
Mint lift® Fine 规格说明
Crafter’s Choice Lavender Chamomile 香料油商品说明书
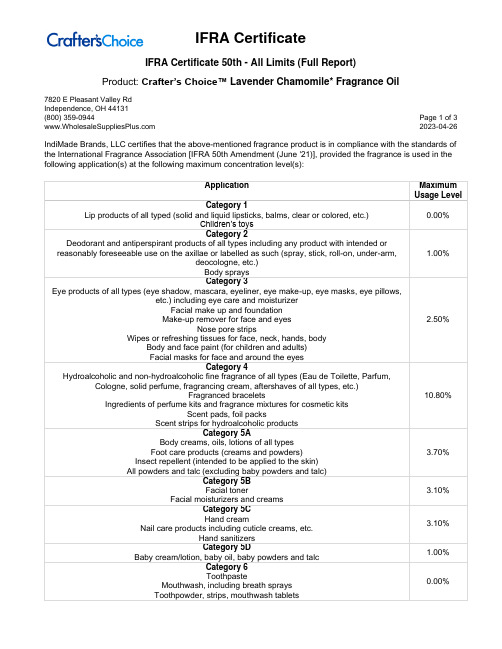
Product: Crafter’s Choice™ Lavender Chamomile* Fragrance Oil7820 E Pleasant Valley RdIndependence, OH 44131(800) 359-0944 Page 1 of 3 2023-04-26 IndiMade Brands, LLC certifies that the above-mentioned fragrance product is in compliance with the standards of the International Fragrance Association [IFRA 50th Amendment (June '21)], provided the fragrance is used in the following application(s) at the following maximum concentration level(s):Product: Crafter’s Choice™ Lavender Chamomile* Fragrance Oil7820 E Pleasant Valley RdIndependence, OH 44131(800) 359-0944 Page 2 of 3 2023-04-26Product: Crafter’s Choice™ Lavender Chamomile* Fragrance Oil7820 E Pleasant Valley RdIndependence, OH 44131(800) 359-0944 Page 3 of 3 2023-04-26For all other applications, or use at higher concentration levels, a new evaluation will be required.The IFRA standards regarding use restrictions are based on safety assessments by the Research Institute for Fragrance Materials (RIFM) Expert Panel (REXPAN) and are enforced by the IFRA Scientific Committee. Evaluation of individual fragrance materials is made according to the safety standards contained in the relevant section of the IFRA Code of Practice.It is the ultimate responsibility of the customer to ensure the safety of the final product containing this fragrance, by further testing, if necessary.The above-mentioned fragrance product contains ingredients which are NOT considered GRAS, Generally Regarded as Safe as a Flavor Ingredient.。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Drop-arm Spurling
Yergason Hawkins
Shoulder disorders
• Clavicular fracture
– Most commonly in the middle 1/3 of the clavicle – Usually happen during fall onto outstretched hand – Xray to verify location and possible dislocation – Conservative treatment with sling for 2-4 weeks
Introduction
• Shoulder is one of the most mobile joints in the human body • Shoulder pain is a very common complaint in primary care • Shoulder injuries are frequently caused by excessive, repetitive motions and overuse • The shoulder allows the upper extremity to rotate up to 180 degrees in 3 different planes • It is important to understand the anatomy of the shoulder, mechanism of injury, physical findings, approach to treatment and indications for a referral to specialist
Shoulder disorders cont
• AC joint Sprain and Separation
– Common injury in athletes – Six grades of separation – On exam swelling and tenderness over AC joint – Xray AP view and axillary for more severe dislocations – Treatment for grades 1 and 2 splinting, 3 and higher orthopedic referral
Physical Exam
• Inspection and palpation • Assessment of range of motion and strength • Provocative testing for instability or impingement • Examine neck and elbow to exclude referred pain
Anatomy
History
• Patient’s age, dominant hand, work or sports activity • Shoulder pain scale, quality, location, radiation, aggravating/alleviating factors • Instability of the joint, stiffness, locking, edema • Acute vs chronic • Important to exclude referred pain such as pneumonia, cardiac ischemia, peptic ulcer disease, malignancy
Shoulder disorders
• Scapular fracture
– Uncommon; result from direct blow – Treatment is a sling for comfort with range of motion exercises as soon as pain is manageable to avoid loss of ROM
•
Shoulder disorders
• Proximal humerus fracture
– Most commonly caused by direct blow or fall on outstretched hand – Physical exam revels crepitus at site of fracture – Xrays AP and lateral, with Y view if needed to see greater tuberosity – Treatment is shoulder immobilization to prevent external rotation and abduction; surgery for more complicated displaced fractures
Shoulder disorders cont
• Biceps tendonitis
– Results from inflammation of the sheath around the long head of the biceps – Pain and tenderness in the area of bicipital grove – Treatment is rest, icing, NSAIDS and corticosteroid injections – When conservative treatment fails surgery is an option
Shoulder disorders cont
• Rotator cuff tear
– Most common in person older than 40 – When rotator cuff ruptures due to chronic impingement syndrome result is muscular atrophy which limits the needed diagnostic testing – Xrays may show calcific tendonitis of the cuff and superior migration of the humeral head
Shoulder disorders cont
• Dislocated shoulder
– Anterior-most common, patient holds the arm in external rotation and abduction, humeral head palpated anteriorly, diagnosis by dimplቤተ መጻሕፍቲ ባይዱ in the skin beneath the acromion – Posterior-uncommon, patient holds the arm close to the body in abduction and internal rotation, limited external rotation and forward elevation on exam – Treatment is relocation of the humerus and immobilization to permit capsular healing
Shoulder Pain
Katarina Lindley DO, FACOFP Medical Director Palo Pinto General Hospital Rural Health Clinics Mineral Wells, Texas
Learning Objectives
• Understand the role of the Primary Care Physician in the management of shoulder pain • Understand the anatomy and potential causes of the pain • Perform shoulder pain history and physical exam • Recognize the differential diagnosis of the pain • Understand treatment options for shoulder pain
Some Tests for Shoulder evaluation
Test Appley scratch Maneuver Patient touches superior and inferior aspect of opposite scapula Arm lowered slowly to waist Spine extended with head rotated to affected shoulder while axially loaded Elbow flexed to 90 degrees with forearm pronated Forward flexion of the shoulder at 90 degrees and internal rotation Positive results Loss of range of motion-rotator cuff problem Rotator cuff tear Cervical nerve root disorder Bicep tendon problem Supraspinatus tendon impingement
Shoulder disorders cont
• Frozen shoulder
– Results from thickening and contraction of the capsule around glenohumeral joint and causes loss of motion and pain – Slow onset with normal Xrays – Most commonly caused by immobility following a shoulder injury – Diagnosis is clinical – Treatment is physical therapy, NSAIDs and occasionally intra-articular steroid injection