9Sustained response to tocilizumab in a patient with relapsing
RECSIT1.1中英文对照全文
New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1)新版实体瘤疗效评价标准:修订的RECIST指南(1.1版本)Abstract摘要Background背景介绍Assessment of the change in tumour burden is an important feature of the clinical evaluation of cancer therapeutics: both tumour shrinkage (objective response) and disease progression are useful endpoints in clinical trials. Since RECIST was published in 2000, many investigators, cooperative groups, industry and government authorities have adopted these criteria in the assessment of treatment outcomes. However, a number of questions and issues have arisen which have led to the development of a revised RECIST guideline (version 1.1). Evidence for changes, summarised in separate papers in this special issue, has come from assessment of a large data warehouse (>6500 patients), simulation studies and literature reviews.临床上评价肿瘤治疗效果最重要的一点就是对肿瘤负荷变化的评估:瘤体皱缩(目标疗效)和病情恶化在临床试验中都是有意义的判断终点。
2016年04月急性冠脉综合征治疗新药临床研究指导原则.(英文版)

30 Churchill Place ● Canary Wharf ● London E14 5EU ● United Kingdom1 April 2016 1 EMA/CHMP/207892/20152 Committee for medicinal products for human use (CHMP)3 Guideline on clinical investigation of new medicinal 4products for the treatment of acute coronary syndrome 5(CPMP/EWP/570/98) 6Draft7 Draft agreed by Cardiovascular Working PartyFebruary 2016 Adopted by CHMP for release for consultation1 April 2016 Start of public consultation 27 April 2016 End of consultation (deadline for comments)31 October 2016 8 This guideline replaces 'Points to consider on the clinical investigation of new medicinal products for the 9 treatment of acute coronary syndrome (ACS) without persistent ST segment elevation' 10 (CPMP/EWP/570/98). 1112 Comments should be provided using this template . The completed comments form should be sent to CVSWPSecretariat@ema.europa.eu .13Keywords Acute coronary syndrome, STE-ACS, NSTE-ACS, guideline, CHMP1415Table of contents16Executive summary (4)171. Introduction (background) (4)182. Scope (5)193. Legal basis and relevant guidelines (5)204. Choice of efficacy criteria (endpoints) (6)214.1. All-cause mortality and CV mortality (6)224.2. New myocardial infarction (6)234.3. Revascularisation (6)244.4. Unstable angina pectoris necessitating hospitalisation (6)254.5. Stent thrombosis (6)264.6. Stroke (7)274.7. Left ventricular function and heart failure (7)284.8. Composite endpoints (7)294.9. Endpoints in fibrinolysis studies (7)305. Methods to assess efficacy (how to measure the endpoints) (8)315.1. Mortality (8)325.2. New myocardial infarction (8)335.3. Revascularisation (8)345.4. Unstable angina pectoris necessitating hospitalisation (8)355.5. Stent thrombosis (8)365.6. Ventricular function and heart failure (9)375.7. Angiographic endpoints (9)386. Selection of patients (9)396.1. Study population (9)406.1.1. STE-ACS (ST elevation acute coronary syndrome) (9)416.1.2. NSTE-ACS (Non-ST elevation acute coronary syndrome) (9)426.1.3. Unstable angina (9)436.2. Inclusion criteria for the therapeutic studies (10)446.3. Exclusion criteria for the therapeutic studies (10)456.4. Risk Stratification (10)466.5. Special populations (11)476.5.1. Older patients (11)487. Strategy and design of clinical trials (11)497.1. Clinical pharmacology (11)507.2. Therapeutic exploratory studies (12)517.2.1. Objectives (12)527.2.2. Design (12)537.3. Confirmatory Therapeutic Studies (12)547.3.1. Objectives (12)557.3.2. Background therapy (12)567.3.3. Choice of comparator (13)577.3.4. Duration of clinical studies (13)587.3.5. Analyses and subgroup analysis (13)598. Safety aspects (14)608.1. Bleedings (14)618.2. All-cause mortality (15)628.3. Thrombocytopenia (15)638.4. Rebound effect (15)648.5. Effects on laboratory variables (15)658.6. Effects on concomitant diseases (15)66References (16)6768Executive summary6970Two CHMP Guidelines have been previously developed to address clinical investigations of new71medicinal products for the treatment of acute coronary syndrome (ACS): (I) the CHMP points toconsider (PtC) on the clinical investigation of new medicinal products for the treatment of acute7273coronary syndrome without persistent ST-segment elevation (CPMP/EWP/570/98), published in 2000 74[1], and (II) the CHMP PtC on the clinical development of fibrinolytic products in the treatment of75patients with ST segment elevation myocardial infarction (CPMP/EWP/967/01), published in 2003 [2].76Since their finalisation, major developments have taken place in the definitions, diagnosis,77interventions and management of ACS, as reflected in the relevant European Society of Cardiology78(ESC) clinical practice guidelines (3, 4). Currently, an update of the above mentioned CHMP Guidelines 79is considered necessary to take these new developments into consideration based on literature review 80and experience gained with medicinal products intended for treatment during the acute phase and81beyond. The present update includes the following changes: 1) guidance addressing both ST-segment 82elevation myocardial infarction (STEMI) and non-ST-segment elevation myocardial infarction83(NSTEMI), as well as unstable angina (UA), 2) update in their definitions, 3) risk stratification using84different scoring systems, 4) investigated endpoints, and 5) clinical developments of new medicinal85products beyond the acute stage, including agents other than antiplatelets and anticoagulants.1. Introduction (background)8687Cardiovascular diseases are currently the leading cause of death in industrialized countries and also 88expected to become so in emerging countries by 2020 [3, 4]. Among these, coronary artery disease 89(CAD) is the most prevalent manifestation and is associated with high mortality and morbidity. ACS 90has evolved as a useful operational term to refer to any constellation of clinical symptoms that are91compatible with acute myocardial ischemia. It encompasses (STEMI), NSTEMI, and UA.92ACS represents a life-threatening manifestation of atherosclerosis. It is usually precipitated by acute 93thrombosis induced by a ruptured or eroded atherosclerotic coronary plaque, with or without94concomitant vasoconstriction, causing a sudden and critical reduction in blood flow. In the complex95process of plaque disruption, inflammation was revealed as a key pathophysiological element. Non-96atherosclerotic aetiologies are rare e.g. such as arteritis and dissection.97The leading symptom of ACS is typically chest pain. Patients with acute chest pain and persistent (>20 min) ST-segment elevation have ST-elevation ACS (STE-ACS) that generally reflect an acute total9899coronary occlusion. Patients with acute chest pain but without persistent ST-segment elevation have 100rather persistent or transient ST-segment depression or T-wave inversion, flat T waves, pseudo-101normalization of T waves, or no ECG changes. At presentation, based on the measurement of102troponins, it is possible to further discriminate between the working diagnosis of non-ST-elevation ACS 103(NSTE-ACS) and unstable angina.104NSTE-ACS is more frequent than STE-ACS [5] with an annual incidence around 3 per 1000 inhabitants, 105but varying between countries [6]. Hospital mortality is higher in patients with STEMI than among 106those with NSTEMI (7% vs. 3–5%, respectively), but at 6 months the mortality rates are very similar 107in both conditions (12% and 13%, respectively) [5,7,8]. Long term follow-up shows that death rates 108were higher among patients with NSTE-ACS than with STE-ACS, with a two-fold difference at 4 years[8]. This difference in mid- and long-term evolution may be due to different patient profiles, since 109110NSTE-ACS patients tend to be older with more co-morbidities, especially diabetes and renal failure.2. Scope111112The aim of this guideline is to provide guidance when performing trials to develop medicinal products 113in the management of ACS. The primary goals of therapy for patients with ACS are to:1. Treat acute, life-threatening complications of ACS, such as serious arrhythmias, pulmonary 114115oedema, cardiogenic shock and mechanical complications of acute myocardial infarction (AMI). [9] 1162. Reduce the amount of myocardial necrosis that occurs in patients with AMI, thus preserving 117left ventricular (LV) function, preventing heart failure (HF), and limiting other cardiovascular118complications.1193. Prevent major adverse cardiac events like death, non-fatal myocardial infarction (MI), andneed for urgent revascularization.120121The focus in this Guideline concerns mainly the medical treatment of ACS (treatment goals 2 and 3). 122The choice of interventional procedures [percutaneous coronary intervention (PCI) or coronary artery 123bypass graft CABG)] falls outside the scope of this guideline.3. Legal basis and relevant guidelines124125This guideline has to be read in conjunction with the introduction and general principles and parts I 126and II of the Annex I to Directive 2001/83 as amended.127Pertinent elements outlined in current and future EU and ICH guidelines, should also be taken into 128account, especially those listed below:129•Dose-Response Information to Support Drug Registration (ICH E4; CPMP/ICH/378/95).130•Statistical Principles for Clinical Trials (ICH E9; CPMP/ICH/363/96).131•Choice of Control Group and Related Issues in Clinical Trials (ICH E10; CPMP/ICH/364/96).132•Points to consider on an Application with 1) Meta-analyses 2) One pivotal study133(CPMP/EWP/2330/99).134•Points to consider on multiplicity issues in clinical trials (CPMP/EWP/908/99).135•Investigation of subgroups in confirmatory clinical trials (EMA/CHMP/539146/2013).136•The Extent of Population Exposure to Assess Clinical Safety for Drugs (ICH E1A;137CPMP/ICH/375/95).138•Pharmacokinetic Studies in Man (3CC3A).139•Studies in Support of Special Populations: Geriatrics (ICH E7 CHMP/ICH/379/95) and related Q&A 140document (EMA/CHMP/ICH/604661/2009).141•Note for Guidance on the Investigation of Drug Interactions (CPMP/EWP/560/95).142•Reporting the Results of Population Pharmacokinetic Analyses (CHMP/EWP/185990/06).143•Reflection paper on the extrapolation of results from clinical studies conducted outside the EU to 144the EU-population (EMEA/CHMP/EWP/692702/2008).145•Draft Guideline on clinical investigation of medicinal products for the treatment of chronic heart 146failure (EMA/392958/2015 )•Guideline on clinical investigation of medicinal products for the treatment of acute heart failure147148(CPMP/EWP/2986/03 Rev. 1)4. Choice of efficacy criteria (endpoints)149150Definitions of clinical endpoints in confirmatory trials should be in line with the relevant clinical151guidelines to facilitate interpretation of the results, to allow comparisons across clinical studies and to 152extrapolate to clinical practice. Endpoints should be centrally adjudicated by a blinded committee. The 153following endpoints are relevant to the investigation of efficacy in patients with ACS.4.1. All-cause mortality and CV mortality154155As one of the goals of treatment of ACS is reduction of mortality, this is an important endpoint to156measure. There is an ongoing debate around the use of all-cause versus cardiovascular mortality in 157cardiovascular (CV) trials. All cause mortality is the most important endpoint in clinical trials for the 158estimation of the benefit-risk balance of a drug, in particular when investigating newer medicinal159products with possible safety issues. On the other hand, CV mortality is more specifically linked to the 160mode of action of CV medicinal products/intervention and is especially relevant when the earliest part 161of the follow up is assessed. The choice is also dependent on the objective of the study i.e. in non-162inferiority trials, CVmortality may be preferred while in superiority trials all cause mortality is usually 163used. In fibrinolysis studies, all cause mortality is preferred (see section 4.9).164As such, one of the two mortality endpoints should be included as a component of the primary165endpoint, with the other investigated as a key secondary endpoint.4.2. New myocardial infarction166167New onset MIis a relevant endpoint in studies of ACS and should always be investigated. The definition 168of MI has evolved through the years; at the time of drafting of this Guideline, the third universal169definition of MI is applicable [10]. Criteria of MI are the same as those used to define the index event 170(see below).4.3. Revascularisation171172Some clinical trials have included revascularization endpoints (PCI or CABG) as part of the primary 173composite with conflicting results [11, 12]. Such endpoints are considered more relevant tointerventional studies, and in the scope of this Guideline, their inclusion as a primary endpoint should 174175be clearly justified and their assessment pre-defined and systematically assessed.4.4. Unstable angina pectoris necessitating hospitalisation176177Unstable angina has been investigated in ACS clinical trials. Due to the varying definitions used, the 178associated subjectivity and the influence of local clinical practice, this endpoint is not encouraged to be 179included in the composite primary endpoint.4.5. Stent thrombosis180181Stent thrombosis (ST) is a rare event that can have fatal consequences. ST has been captured in some 182registration studies, but not consistently in the primary endpoint (PEP). The investigation of ST as part 183of the primary endpoint is not encouraged due to the uncertainty of the clinical relevance of all184captured events, except for the "definite" subcategory. Another category identified by the timing isintra-procedural stent thrombosis (IPST), which is a rare event indicating the development of occlusive 185186or non-occlusive new thrombus in or adjacent to a recently implanted stent before the PCI procedure is187completed. Some recent studies [13,14] show that these events may be of prognostic value. As such they should also be collected and presented as secondary endpoint but not included in the analysis of 188189ST.4.6. Stroke190191Stroke should be defined by a generally accepted definition [15]. Clinical studies in ACS have used192non-fatal stroke in the primary endpoint , including any types of strokes. However it is preferred to193include only ischemic strokes in the primary endpoint, as this is the true measure of efficacy;194haemorrhagic stroke should be included as a safety endpoint. An ischaemic stroke with haemorrhagic195conversion should be considered as “primary ischaemic”. The subgroup of “undefined strokes” should196be as small as possible in order to be able to properly assess the effect of the study treatment. In case 197all types of strokes are included in the primary endpoint, a sensitivity analysis including only ischemic198stroke should be submitted.4.7. Left ventricular function and heart failure199Some medicinal products such as modulators of reperfusion injury or inflammation, or gene/cell200201therapy are developed to improve myocardial function and reduce the occurrence of HF. In these202cases, measurement of myocardial function could be a relevant endpoint to investigate the mechanismof action. In phase III studies, these endpoints can be investigated as secondary endpoints to support 203204the clinical endpoints. Occurrence of HF should be considered as a clinical endpoint in phase III studies205aimed at showing benefit in long-term cardiovascular outcome. All-cause mortality and long term206follow-up are mandatory in studies with novel interventions.4.8. Composite endpoints207Due to the rather low incidence of cardiovascular events during the follow-up period after the acute 208209phase of the ACS, composite endpoints consisting of relevant components are acceptable, both as210primary and secondary endpoints. The composite of CV death, non-fatal MI and non-fatal stroke (Major211Adverse Cardiovascular Events, [MACE]) has commonly been used in registration studies, with non-212fatal strokes showing limited contribution to the results. As such, it is preferred to investigate the213composite of death and non-fatal MI in confirmatory studies; non-fatal ischaemic stroke could beincluded in the composite if justified. Sometimes different definitions of MACE are being used with214215novel therapies [16], that should be justified when used in place of MACE. The inclusion of less216objective and clinically derived outcomes in the same composite is generally not encouraged, as they217may either drive the efficacy or dilute the results. In case these endpoints are included they have to be218stringently defined, and adjudicated. Each component of the primary composite endpoint should be219analysed as secondary endpoint.220The net clinical benefit that includes both benefit and safety issues of the studied drug may be used as221a secondary endpoint to be evaluated if it contributes to the discussion on the benefit-risk balance of222the studied drug.4.9. Endpoints in fibrinolysis studies223224In fibrinolysis studies, angiographic studies using the TIMI (Thrombolysisi in Myocardial Infarction)perfusion grades as evaluation criteria are often used. However, complete recanalization cannot be 225226considered as a surrogate for survival when assessing fibrinolytic drugs, as some medicinal productsproviding higher complete recanalization rates than alteplase, failed to demonstrate additional survival 227228benefit. For this reason, all cause mortality is the most relevant endpoint or a combined endpoint as 229previously discussed (see 4.1). Secondary endpoints such as heart failure hospitalisations, left230ventricular function, ventricular arrhythmias, the need for rescue recanalization (emergent and/or231planned) should also be considered and justified.5. Methods to assess efficacy (how to measure the232endpoints)2335.1. Mortality234235Definition of CV death should be clearly defined, in line with acceptable standards [17]. It is mandatory 236to report and centrally adjudicate all mortality data where survival is an endpoint of the study.237Assessment of cardiovascular mortality will require censoring of other “types” of mortality, which may 238complicate its interpretation, in particular when non-CV deaths are in high proportion.5.2. New myocardial infarction239240The diagnostic of MI is based on the detection of a rise and/or fall of cardiac biomarker values241[preferably cardiac troponin (cTn)] with at least one value above the 99th percentile upper reference 242limit (URL). All MIs should be collected and also classified by their different sub types (i.e,243spontaneous, secondary to an ischemic imbalance, related to PCI, related to ST or CABG) [10]. This is 244particularly important considering the different prognostic values of each type of MI. For the same 245reason and to support the clinical relevance of post procedural MIs, these events should be presented 246with higher cut-off values (≥ 5 and ≥10x upper level of normal ULN, in case of CK-MB or ≥70x ULN of 247cTn) [18]. These higher cut-off values can also help in diagnosing MIs in the setting of elevated248baseline biomarkers, which is a problematic situation. In such cases, serial measurements of the249biomarkers are necessary, in addition to new ECG changes or signs of worsening of cardiac function, 250e.g. HFor hypotension [18].5.3. Revascularisation251252The underlying cause of revascularization should be identified: restenosis, ST or disease progression. 253In the latter case target vessel revascularization (TVR) could be included. Early target lesion eventsafter revascularization (before 30 days) are more likely to be caused by an angiographic complication 254255and should preferably be included as safety endpoint (see ST).5.4. Unstable angina pectoris necessitating hospitalisation256257When investigated, robust definitions should be employed. In order to support the seriousness of the 258event it should also be shown that it has led to a revascularisation procedure. Since a medicinalproduct that prevents death and/or new MI might result in more patients suffering from UA, the259260analysis of this endpoint should take into account censoring issues as well.5.5. Stent thrombosis261262ST should be collected and classified as definite, probable and possible in line with acceptable263definitions [19]. In addition, the timing of ST should be documented (acute, sub-acute, late and very 264late), as risk factors and clinical sequels differ with timing.5.6. Ventricular function and heart failure265266Investigation of cardiac function should follow state of the art methods. This can include among others 267measurement of ventricular function by isotopic method and/or by cardiac magnetic resonance imaging 268and/or echocardiography. Investigation of HFshould follow the relevant CHMP guidelines.5.7. Angiographic endpoints269270Angiograms should undergo central blinded reading. In principle, the rate of TIMI 3 flow (complete 271revascularization) of the infarct related artery at 90 minutes is considered the most relevant272angiographic endpoint, as it has been shown to correlate with an improved outcome in terms of273mortality and left ventricular function. An earlier evaluation of the patency pattern (i.e. 30 and 60274minutes) may provide important information on the speed of recanalization. Whatever is the time-point 275selected as primary outcome, it must be properly justified and pre-specified in the clinical trial.6. Selection of patients2766.1. Study population277The definition of the different ACS subtypes should be based on current guidelines/universal definition 278279of MI including STEMI and NSTEMI as well as UA [3, 4, 10].6.1.1. STE-ACS (ST elevation acute coronary syndrome)280281In patients with acute chest pain and persistent (>20 min) ST-segment elevation on ECG the282diagnostic of STE-ACS is made [3]. This condition generally reflects an acute total coronary occlusion.Most patients will ultimately develop an ST-elevation myocardial infarction (STEMI) with the criteria of 283284acute myocardial infarction described before [see 5.2].6.1.2. NSTE-ACS (Non-ST elevation acute coronary syndrome)285286In patients with acute chest pain but no persistent ST-segment elevation the diagnostic of NSTE-ACS is 287made [4]. ECG changes may include transient ST-segment elevation, persistent or transient ST-288segment depression, T-wave inversion, flat T waves or pseudo-normalization of T waves or the ECG 289may be normal. The clinical spectrum of non-ST-elevation ACS (NSTE-ACS) may range from patients 290free of symptoms at presentation to individuals with ongoing ischaemia, electrical or haemodynamic 291instability or cardiac arrest. The pathological correlate at the myocardial level is cardiomyocyte292necrosis (NSTEMI) or, less frequently, myocardial ischaemia without cell loss (UA). Currently, cardiac 293troponins play a central role in establishing a diagnosis and stratifying risk, and make it possible to 294distinguish between NSTEMI and UA[4].6.1.3. Unstable angina295296Unstable angina (UA) is defined as myocardial ischemia at rest or minimal exertion in the absence of 297cardiomyocytes necrosis, i.e. without troponin elevation. Among NSTE-ACS population, the higher298sensitivity of troponin has resulted in an increase in the detection of MI [4]; the diagnosis of UAis less 299frequently made.6.2. Inclusion criteria for the therapeutic studies300301Inclusion of both STEMI and NSTEMI and/or NSTE-ACS patients in the same clinical trial (or not)302should be justified based on the mechanism of action of the investigated product and the proposed 303time of intervention. If both subgroups are investigated in the same trial, both subgroups should be 304well represented. For interventions aimed at post-acute and longer term phases (secondary305prevention or plaque stabilisation) it may be justified to address both conditions in the same clinical 306trial. Time of inclusion of the patients in relation to the index event should be set and adequately307discussed a priori.308Patients with unstable angina represent a different risk category and prognosis that necessitates309different interventions than NSTEMI patients. However, during the acute presentation of NSTE-ACS it may be difficult to discriminate NSTEMI from UA so both groups have been included in some clinical 310311studies. In general, the investigation of interventions in these patients is encouraged, but preferably in 312separate clinical trials.If fibrinolysis is considered, inclusion criteria should be in line with the current treatment guidelines 313314concerning the inclusion for fibrinolysis [3].6.3. Exclusion criteria for the therapeutic studies315316If the patients do not fulfil the above criteria for ACS they should be excluded from the ACS studies. 317Other life-threatening conditions presenting with chest pain, such as dissecting aneurysm,318myopericarditis or pulmonary embolism may also result in elevated troponins and should always be 319considered as differential diagnoses [4].320If drugs interfering with the haemostatic system are tested, patients with a significant risk of bleeding 321(e.g. recent stroke, recent bleeding, major trauma or surgical intervention) and/or a propensity to 322bleed (e.g. thrombocytopenia, clotting disturbances, intracranial vascular diseases, peptic ulcers,323haemophilia) should be excluded from participation in the clinical studies.324Attention should be paid to the time elapsed between a previous application of antiplatelet or325anticoagulant acting agent beforehand and the administration of study drug (e.g. the pharmacokinetic 326[PK] and even more importantly, the pharmacodynamic [PD] half-life of these previously administered 327drugs).328For reasons of generalisability of the study results to the future target population it is strongly advised 329not to define the exclusion criteria too narrow, i.e. polymorbid patients (e.g. renal and/or hepatic330impairment, heart failure), should not automatically be excluded from the main therapeutic clinical 331trials.332When fibrinolysis is considered, exclusion criteria for fibrinolysis should be strictly respected [3].6.4. Risk Stratification333334In clinical trials, the ability of the therapy to demonstrate a treatment effect may depend on the335underlying risk and expected event rates. Enrichment strategies are sometimes used in trials to obtain 336the required number of events with a reasonable time in specific subgroups who are likely to exhibit a 337higher event rate than the overall target population and potentially larger treatment effect. In thatcase, it has to be shown that the results of this enriched study population can be extrapolated to the 338339general population.。
非感染性葡萄膜炎药物治疗进展

国际眼科纵览 2021 年4月第45 卷第2 期IntRevOphthalmol, Apr. 2021,V〇1.45, No.2• 89 •••非感染性葡萄膜炎药物治疗进展张传宏薛黎萍昆明医科大学第四附属医院眼科650021通信作者:薛黎萍,Email:xueliping001@ 163. com【摘要】糖皮质激素及其他免疫抑制剂是非感染性葡萄膜炎的主要治疗方案,新型生物可降解缓释玻璃体植人剂临床应用前景广阔,生物制剂显示出独特疗效。
目前应用的局部糖皮质激素包括氟西奈德植人剂、地塞米松玻璃体植入剂等。
免疫抑制剂包括抗代谢药甲氨蝶呤、硫唑嘌呤、霉酚酸酯等;T细胞抑制剂环孢霉素、他克莫司、雷帕霉素等;烷化剂环磷酰胺、苯丁酸氮芥等。
生物制剂包括抗肿瘤坏死因子制剂英夫利昔单抗、阿达木单抗、依那西普、戈利木单抗、赛妥珠单抗等;白细胞介素受体拮抗剂阿那白滞素、康纳单抗、托珠单抗等;选择性B淋巴细胞抑制剂利妥昔单抗;选择性T淋巴细胞抑制剂阿巴西普等。
不同药物各有其适用范围和不良反应,根据不同患者病情选择合适治疗方案、控制疾病进展、减少并发症的发生尤为重要。
(国际眼科纵览,202人4539-9S)【关键词】非感染性葡萄膜炎;激素植人剂;免疫抑制剂;生物制剂基金项目:云南省科技厅-昆明医科大学联合专项重点项目(2019FE001-169)D0I :10.3760/ cma. j. issn. 1673-5803. 2021.02.002Drug treatment of non-infectious uveitisZhang Chuanhong,Xue LipingDepartment of Ophthalmology, the Fourth Affiliated Hospital of Kunming Medical University, the Second People * 5Hospital of Yunnan Province, Kunming 650021, ChinaCorresponding author:Xue Liping, Email:********************【Abstract】Glucocorticoids and other immunosuppressants are the primary therapeutic options fornon-infectious uveitis. Novel biodegradable sustained-release vitreous implants are promising for extensiveclinical applications, and biological agents have shown unique efficacy. The currently applied topical glucocorticoid implants include fluocinolone acetonide implant, dexamethasone vitreous implant, etc. The immunosuppressants include antimetabolites methotrexate, azathioprine,and mycophenolate mofetil, etc. ; Tcell inhibitors cyclosporine, tacrolimus, and rapamycin, etc. ;and alkylating agents cyclophosphamide andchlorambucil, etc. The biological agents include anti-tumor necrosis factor agents infliximab, adalimumab,etanercept, golimumab, and certolizumab, etc. ; interleukin receptor antagonists anakinra, canalizumab,and tocilizumab, etc. ;selective B lymphocyte inhibitor rituximab;and selective T lymphocyte inhibitor abat-acept, etc. Different agents have their respective scopes of application and adverse reactions. It is particularly important to select a treatment regimen appropriate for the patient * s condition, to control disease progression, and to reduce complications. (Int Rev Ophthalmol, 2021 ^45:89-98)【Key words 】non-infectious uveitis; corticosteroid implant; immunosuppressor; biologic agentFund program:Applied Basic Research Foundation of Yunnan Province, China (2019FE001-169)DOI:10.3760/ cma. j. issn. 1673-5803.2021.02.002非感染性葡萄膜炎(non-infectious uveitis,NIU)为葡萄膜炎最常见类型。
罗氏新药Ocrelizumab两项临床三期研究圆满完成

罗氏新药Ocrelizumab两项临床三期研究圆满完成
佚名
【期刊名称】《临床合理用药杂志》
【年(卷),期】2015(8)29
【摘要】近日,罗氏公司开发的治疗多发性硬化症新药Ocrelizumab圆满完成了两项临床三期研究,公司信心满满希望借此挑战多发性硬化症市场“霸权”。
此前,罗氏的研究人员希望该药成为一种成功的关节炎药物。
然而,随着在关节炎研究领域的失败,罗氏转而寻求这种药物在多发性硬化症治疗领域有所作为。
数据显示这种药物能够有效降低患者发病次数以及延缓患者身体机能的下降。
罗氏公司预计将于明年的第一季度将Ocrelizumab提交美国FDA和欧洲医药管理部门进行审核。
【总页数】1页(P107-107)
【正文语种】中文
【中图分类】R979.5
【相关文献】
1.罗氏调经种子丸治疗肾虚肝郁型月经不调临床效果研究
2.B细胞淋巴瘤治疗新药美罗华临床研究进展
3.罗氏风痰咳嗽方治疗风痰阻肺型感染后咳嗽临床研究
4.罗氏非小细胞肺癌新药Tarceva研究进展
5.惠氏公司公布用于更年期综合征的新药Desvenlafaxine的Ⅲ期临床研究数据
因版权原因,仅展示原文概要,查看原文内容请购买。
新型冠状病毒肺炎疫情下的医院药事管理与药学服务实践

2021年5月第9期卫生管理与医学教育新型冠状病毒肺炎疫情下的医院药事管理与药学服务实践蒋建梅,李文*淮安市洪泽区人民医院,江苏 淮安 221000【摘要】目的:探讨新型冠状病毒肺炎疫情下的药事管理和药学服务方面的特点,总结经验和不足,为以后遇到突发公共卫生事件提供参考。
方法:回顾分析2020年1月以来的药事管理和药学服务工作,从制度、人员、药品和服务实践等方面进行分析。
结果:通过药学人员的共同努力,很好的完成了药品供应、药学信息传递、处方审核和用药咨询工作。
结论:新型冠状病毒虽然来势凶猛,但面对疫情,药学人员沉着应对,在实践中通过不断尝试,保证了医院药事和药学服务的顺利进行,取得了令人满意的效果。
【关键词】新型冠状病毒肺炎;药事管理;药学服务[中图分类号]R95 [文献标识码]A [文章编号]2096-5249(2021)09-0174-02 Novel coronavirus pneumonia in hospital pharmacy management and pharmaceutical care practiceJIANG jian-mei, LI Wen* (People’s Hospital of Hongze District, Huai’an Jiangsu 221000, China)[Abstract] Objective: discuss to explore the novel coronavirus pneumonia epidemic situation under the situation of pharmaceutical administration and pharmaceutical care, summarize experience and insufficiency, and provide reference for future public health emergencies. Methods: The pharmaceutical administration and pharmaceutical care since January 2020 were reviewed and analyzed from the aspects of system, personnel, drug and service practice. Results: Through the joint efforts of pharmaceutical personnel, we have completed the drug supply, pharmaceutical information transmission, prescription audit and medication consultation. Conclusion: Although the novel coronavirus is fierce, it is a calm response for pharmaceutical practitioners to face the epidemic. In practice, through continuous trial, the hospital pharmacy and pharmaceutical services have been successfully carried out and satisfactory results have been achieved.[Key words] Novel coronavirus pneumonia; Pharmaceutical Administration; Pharmaceutical care自2019年12月新型冠状病毒肺炎疫情在武汉爆发,引起了全世界的关注。
胆囊癌临床诊疗的新进展
胆囊癌临床诊疗的新进展中华外科杂志普外空间 2022-08-10 10:00 发表于北京作者:杨自逸,刘诗蕾,蔡晨,吴自友,熊逸晨,李茂岚,吴向嵩,全志伟,龚伟文章来源:中华外科杂志, 2022, 60(8)摘要胆囊癌的恶性程度极高,尚缺乏早期诊断方法和有效治疗手段,亟需高质量研究突破诊疗瓶颈。
本文回顾了2021年国内外发表的胆囊癌研究相关文献,对临床诊疗领域的重要进展进行综述,详细介绍了胆囊癌最新流行病学数据及危险因素、新兴的外周血实验室检查和影像学诊断方法、病理学类型新分类、外科治疗的热点与争议及系统性综合治疗动态。
这些研究结果有助于探索更有效的胆囊癌诊治方法,为改善胆囊癌患者的预后带来希望。
胆囊癌是胆道系统常见的恶性肿瘤,具有症状隐匿、发展迅速、早期转移、预后极差的特点。
我国是胆囊癌的高发地区之一,近年来发病率和病死率呈缓慢上升趋势。
目前仍缺乏特异度和灵敏度均较好的胆囊癌早期诊断手段,临床发现的胆囊癌多为中晚期。
尽管医学科技不断发展,早期诊断和根治性手术切除仍是可能治愈胆囊癌的手段,行之有效的系统性治疗方法依然在不断探索中。
本文展示了2021年胆囊癌临床诊疗领域的研究进展,以探索更好的胆囊癌诊疗方法。
一、流行病学特征(一)发病率与死亡率2020年全球癌症统计数据显示,全球胆囊癌新发115 949例(男性41 062例,女性74 887例),死亡84 695例(男性30 265例,女性54 430例)[1],均居消化系统肿瘤第6位。
胆囊癌全球发病率存在明显的地域差异,全球年龄标准化发病率平均为2.3/10万人,以东亚、南美最高,西欧、北美则发病率较低[2];且近年来男性和年轻群体的胆囊癌发病率呈升高趋势。
我国国家癌症中心数据显示,国内胆囊癌发病率为3.95/10万人(男性3.70/10万人,女性4.21/10万人),死亡率为2.95/10万人(男性1.9/10万人,女性2.1/10万人)[3]。
国际骨髓瘤工作组骨髓瘤缓解标准

国际骨髓瘤工作组骨髓瘤缓解标准国际骨髓瘤工作组骨髓瘤缓解标准1. 国际骨髓瘤工作组骨髓瘤缓解标准是指哪些标准?国际骨髓瘤工作组骨髓瘤缓解标准(International Myeloma Working Group, IMWG)是一个由全球专业医生组成的组织,致力于制定和更新骨髓瘤治疗的指南和标准。
骨髓瘤是一种恶性肿瘤,对标准化的治疗和缓解标准是非常重要的。
IMWG提出的骨髓瘤缓解标准包括完全缓解(CR)、非完全缓解(nCR)、部分缓解(PR)、疾病稳定(SD)以及疾病进展(PD)等不同级别的缓解状态,这些标准对于评估患者的疗效和预后都具有重要的参考价值。
2. 骨髓瘤缓解标准对患者的治疗和预后有何重要性?对于骨髓瘤患者来说,缓解标准是评估治疗效果和预测疾病进展的重要依据。
通过对患者进行缓解状态的评估,医生可以更好地选择合适的治疗方案,并在治疗过程中进行动态监测和调整。
缓解标准也可以帮助患者和家属更清晰地了解疾病的发展和预后,有助于患者对治疗和康复过程的心理调适。
3. IMWG骨髓瘤缓解标准的发展历程和意义IMWG骨髓瘤缓解标准的发展历程经历了多次的修订和升级,旨在更准确地反映患者疾病状态的变化。
这些缓解标准是通过对全球范围内大量骨髓瘤临床数据的分析和总结得出的,具有较为科学和权威的医学依据。
这些标准的制定和应用,不仅在临床诊疗中起到了重要的指导作用,也推动了世界范围内对骨髓瘤治疗和研究的进步。
4. 个人观点和理解在我看来,国际骨髓瘤工作组骨髓瘤缓解标准是一项非常重要的医学成果。
它不仅对于骨髓瘤患者的治疗和预后具有重要意义,也为临床医生提供了标准化的治疗指导。
在今后的临床实践中,我相信这些标准会继续发挥着重要的作用,为更多的患者带来福音。
总结回顾:通过对国际骨髓瘤工作组骨髓瘤缓解标准的全面探讨,我们深入了解了这一标准的制定意义、内容要点以及对患者治疗和预后的重要性。
这些标准不仅是医学研究的成果,也是临床实践的指导。
阿替利珠单抗 Atezolizumab说明书

阿替利珠单抗Atezolizumab说明书Tecentriq(atezolizumab)注射液使用说明2016年第一版批准治疗:2016年5月18日;公司:Genentech,Inc.FDA为批准对膀胱癌新靶向治疗。
Tecentriq是FDA批准的第一个PD-L1抑制剂。
FDA的药品评价和研究中心血液学和肿瘤产品室主任Richard Pazdur,M.D.说:“Tecentriq提供这些患者一个新治疗靶向PD-L1通路,”“产品阻断PD-1/PD-L1的机制部分地与机体的免疫系统和它的与癌细胞间相互作用相互关系有关。
”突破性治疗指定,优先审批状态和加速批准处方资料重点这些重点不包括安全和有效使用TECENTRIQ所需所有资料。
请参阅TECENTRIQ完整处方资料。
TECENTRIQTM(atezolizumab)注射液,为静脉使用美国初次批准:2016适应证和用途TECENTRIQ是一种程序死亡配体1(PD-L1)阻断抗体适用为有局部晚期或转移尿路上皮癌患者的治疗患者:⑵含铂化疗期间或后有疾病进展(1)⑵用含铂化疗新辅助或辅助治疗12个月内有疾病进展(1)这个适应证在加快批准下被根据肿瘤反应率和反应时间批准的。
继续批准这个适应证可能取决于在验证性试验临床获益的确证和描述。
(1,14)剂量和给药方法每3周给予1200 mg作为一次静脉输注历时60分。
(2.1)静脉输注前稀释。
(2.3)剂型和规格注射液:1200 mg/20 mL(60 mg/mL)溶液在一单剂量小瓶中(3)禁忌证无。
(4)警告和注意事项●免疫相关肺炎:对中度不给和对严重或危及生命肺炎永久地终止。
(5.1)●免疫相关肝炎:监视肝功能变化。
对中度不给和对严重或危及生命转氨酶或总胆红素升高永久地终止。
(5.2) ●免疫相关结肠炎:对中度不给或严重,和对危及生命结肠炎永久地终止。
(5.3)●免疫相关内分泌病(5.4):o 垂体炎:对中度不给或严重和对危及生命垂体炎永久地终止。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
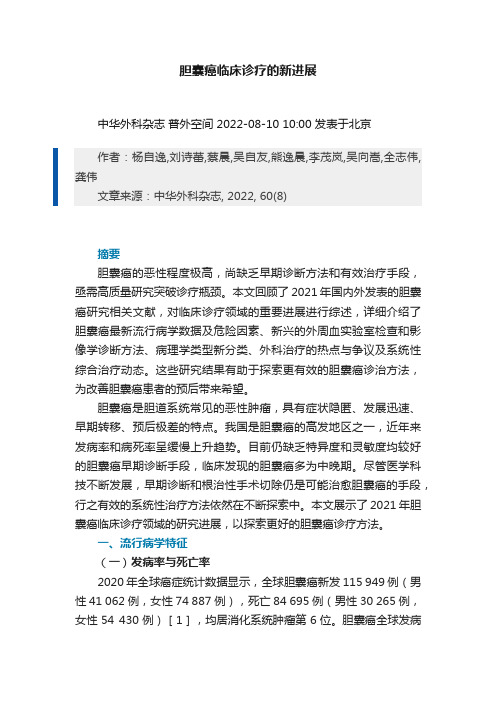
CASE BASED REVIEWSustained response to tocilizumab in a patient with relapsing polychondritis with aortic involvement:a case based reviewRebecca Stael &Vanessa Smith &Ruth Wittoek &David Creytens &Herman MielantsReceived:30April 2014/Accepted:5May 2014/Published online:16May 2014#Clinical Rheumatology 2014Abstract This paper presents a case with refractory relapsing polychondritis (RPC),complicated with severe aortic involve-ment,which is successfully treated with tocilizumab.Previous treatments consisted of methotrexate,corticosteroids,cyclo-sporine,cyclophosphamide,infliximab,and etanercept.With these treatments,the patient had recurrent episodes of fever,polyarthritis,tenosynovitis,subcutaneous nodules,and pro-gressive cardiac disease.One year after the start of treatment with tocilizumab,there is resolution of all symptoms,normal-ization of C-reactive protein (CRP)and erythrocyte sedimen-tation rate (ESR),and the dose of prednisolone is tapered down to 2mg/day.We have reviewed the English literature for reports of patients with refractory RPC,successfully treat-ed with tocilizumab.We found five additional case reports.In one case report,a patient with refractory RPC complicated with aortitis was successfully treated with tocilizumab.In three case reports,patients with refractory RPC complicated with laryngotracheal involvement were successfully treated with tocilizumab.All cases had,like our patient,failed con-ventional treatment.We also reviewed the literature for reports of the effect of biologicals on cardiac involvement in RPC.Current literature is presented and discussed.Keywords Aortic wall biopsy .Aortitis .Auriculair chondritis .Relapsing polychondritis .TocilizumabIntroductionRelapsing polychondritis (RPC)is a rare immune-mediated disease which is associated with inflammation in the cartilag-inous tissue throughout the body.Especially the cartilaginous structures of the ear,nose,joints,and respiratory tract are affected.The incidence is estimated to be three per million population with an onset around 40–60years [1–3].Established diagnostic criteria are the original McAdam ’s criteria that require the presence of three or more of the following clinical features:bilateral auricular chondritis,nonerosive,seronegatieve inflammatory polyarthritis,nasal chondritis,ocular inflammation,respiratory tract chondritis,and chochlear and/or vestibular dysfunction [1–5].In addition to corticosteroids,several immunomodulatory and anti-inflammatory drug regimes have been used to treat the dis-ease.Some reports are made on the successful treatment of RPC with biological agents including anti-tumor necrosis factor alpha and anti-interleukine 1receptor antagonists [1,2,5].In this case,we report a man with refractory RPC compli-cated with aortitis,successfully treated with tocilizumab,anti-interleukine 6receptor antagonist,along with a literature review of similar published cases.CaseA 25-year old male was referred to our rheumatology clinic in 2003because of a new onset of inflammatory joint complaints of the knees and the ankles.He was diagnosed with peripheral spondyloarthritis based on HLA-B27positivity,an asymmet-rical oligoarthritis,and a tendinitis of the achilles tendon.Treatment was initiated with sulfasalazine 3g daily and non-steroidal anti-inflammatory drug piroxicam 20mg daily.Due to poor response to this conventional treatment,etanerceptR.Stael (*):V .Smith :R.Wittoek :H.MielantsDepartment of Rheumatology,University Hospital of Ghent,De Pintelaan 185,9000Ghent,Belgium e-mail:rebecca_stael@D.CreytensDepartment of Pathology,University Hospital of Ghent,De Pintelaan 185,9000Ghent,BelgiumClin Rheumatol (2015)34:189–193DOI 10.1007/s10067-014-2670-750mg,once a week subcutaneously,was initiated in May 2003.Despite this therapy,biochemical inflammation persisted and he had recurrent flares.Three years later,he developed auricular inflammation and nodules at the elbows and the fingers (Fig.1).Histologic examination of a biopsied lesion of the thumb showed a palisaded neutrophilic granulomatous dermatitis.This is a rare skin disease possibly related to underlying autoimmune pathology.In the same year,he developed a scleritis of the left eye.Etiology was considered of autoimmune origin and it was treated with methylprednisolone 16mg daily and methotrex-ate 10mg weekly.In 2007,he was admitted because of a pneumonia with severe sepsis.During the admission,he de-veloped a cardiogenic shock caused by acute severe aortic regurgitation.Emergency aortic valve replacement was per-formed and the patient recovered.Tissue samples were taken during surgery and showed signs of chronic focal active endocarditis.A few histopathologic changes being present could be related to RPC including increase of vasa vasorum,endothelial swelling,and cuffing of lymphocytes (Fig.2a,b ).Based on these new findings,the diagnosis of peripheral spondyloarthritis was rejected and RPC was retained based on the presence of bilateral auricular chondritis,ocular inflam-mation (scleritis),peripheral joint disease (oligoarthritis and tendinitis of the Achilles tendon),aortic valve disease,and skin involvement (subcutaneous nodules).Besides this,the presence of HLA-B27positivity was considered not signifi-cant.The ocular inflammation was not due to an uveitis,a known nonspinal feature associated with spondyloarthritis,but due to a scleritis.At the time of diagnosis of RPC,therapy with corticoste-roids (prednisolone 10mg/day)and cyclosporine (2×100mg /day)was initiated.Whenever the patient developed an arthritis,this was managed with local corticosteroid in-jection or treatment with a nonsteroidal anti-inflammatory drug.In May 2008,he developed a partial dehiscence of his mechanical aortic valve due to presence of fragile aortic tissue.This caused a paravalvular leakage which was treated surgically.Unfortunately,in 2010,the paravalvular leakage relapsed and could only be treated conservatively (pharmacologically)since the operative risk had become too high.The secondary aortic regurgitation caused adilata-Fig.1Subcutaneous nodules at thefingersFig.2Biopsy from the aortic wall taken during surgery in 2007showed a chronic focal active endocarditis and b mild increase of vasa vasorum,endothelial swelling,and cuffing oflymphocytes.Biopsy from the aortic wall taken during operation in 2012showed c more active mesaortitis and d more prominent increase of vasa vasorum,endothelial swelling,and cuffing of lymphocytestion of the left ventricle and cardiac arrhythmias.Eventually, a pacemaker needed to be implanted because of a complete atrioventricular block.In2011,despite therapy,the patient developed polyarthritis and had recurrent episodes of fever.A treatment with cyclo-phosphamide500mg intravenously,every3weeks,was commenced in combination with prednisolone20mg/day. He received three pulses of cyclophosphamide,but in spite of this therapy,he experienced recurrent polyarthritis.In May2011,an anti-TNF-alpha antibody,infliximab (5mg/kg)eight times weekly,was commenced in combination with prednisolone20mg/day.Under this therapy,symptoms improved;the patient developed less fever and arthritis.There was a good biochemical response(decrease of C-reactive protein(CRP)and erythrocyte sedimentation rate(ESR))and the dose of prednisolone was tapered to10mg/day.After initial resolution of the symptoms for a few months,they reappeared and CRP and ESR values increased again to pretreatment levels.By the end of2011,the dose frequency of infliximab was increased to four times weekly and methotrexate15mg was initiated.The dose of prednisolone was again increased to 20mg/day.In February2012,the patient developed an episode of scleritis.Despite of the therapy changes,he failed to show clinical remission.Therefore,in June2012,treatment was switched to toci-lizumab(intravenously,8mg/kg)administered monthly in combination with corticosteroids(prednisolone10mg/day)and methotrexate15mg weekly.Again,there was a good clinical and biochemical response and the dose of predniso-lone could be lowered.In August2012,the patient was admitted to the hospital because of sustained ventricular tachycardia.He suffered from severe aortic regurgitation with dilatation of the left ventricle.Again,surgical treatment was needed and a total aortic root replacement with a composite valve graft and implantation of the coronary arteries was performed (Bentall procedure).The pacemaker was replaced by a defibrillator.The biopsy from the aortic wall taken during surgery showed more active mesaortitis.The aortic wall was infiltrated with collections of neutrophilic granulocytes and fibrinoid necrosis of the aortic wall was seen.Also,an infiltrate of lymphocytes and macrophages was present.A more prominent increase of vasa vasorum was seen togeth-er with endothelial swelling and perivascular cuffing of lymphocytes(Fig.2c,d).In November2012,the patient had a recurrent episode of ventricular tachycardia which was treated with amiodarone. Subsequently,the cardiac situation stabilized.One year after initiating treatment with tocilizumab,symp-toms have markedly improved.Treatment using this anti-IL-6 receptor antagonist resulted in normalization of CRP and ESR and resolution of all symptoms(no fever,no arthritis,disap-pearance of the subcutaneous noduli at the fingers).The dose of methotrexate could be tapered down to7.5mg a dayandFig.3Evolution of the inflammation parameters(CRP and ESR)and the changes of doses of prednisolone and methothrexate in function of the administration of infliximab(5mg/kg eight times weekly),infliximab (5mg/kg four times weekly),and tocilizumab(8mg/kg monthly).The administration of tocilizumab was started at day0the dose of prednisolone was tapered down to 2mg a day (Fig.3).DiscussionA standardized therapeutic protocol for RPC has not yet been established.Current medical therapy is largely empiric and based on case reports [1–5].Pharmacological options should be made according to the clinical presentation and consist of steroids,nonsteroidal anti-inflammatory drugs,colchicine,and immunomodulatory agents such as methotrexate,cyclo-phosphamide,azathioprine,dapsone,cyclosporine,mycophe-nolate mofetil,and intravenous immunoglobulin [1,6].A number of case reports have suggested that blockade of the pro-inflammatory cytokines such as TNF-alpha and IL-1can be used to successfully treat RPC.Moreover,serum cytokine profiles of patients with active RPC have shown elevated levels of IL-8,monocyte chemotactic protein-1,and macrophage inflammatory protein-1-beta,but no statistically significant elevation of serum TNF-alpha,IL-1,or IL-6levels [7].However,several case reports indicate efficacy of bio-logics in RPC for a variety of disease-related manifestations.Especially,anti-TNF-alpha agents (infliximab first and fore-most,but also etanercept and adalimumab)have been used in RPC.Some case reports also mention effectiveness of anakinra and abatacept in the treatment of RPC.The main limitation of this therapeutic strategy is the lack of supporting evidence from any randomized controlled trial.Five case reports of patients with refractory RPC treated with tocilizumab have been published earlier (Table 1).In one case report,two patients with RPC complicated with laryngotracheal involvement were successfully treated with tocilizumab.One of these patients was first treated with infliximab with partial response.Nine months after initiating tocilizumab,the clinical symptoms improved,there was a normalization of the CRP-level,and the dose of corticosteroids could be tapered.The other patient was directly treated with tocilizumab.Five months later,he showed a good clinical and biochemical response [9].In the other case report,a patient with RPC complicated by aortitis was successfully treated with tocilizumab.Previously,the patient had been treated with infliximab and adalimumab,which initially resulted in a com-plete resolution of symptoms,but was stopped afterwards because of recurrence of symptoms.In contrast to infliximab,adalimumab resulted in a sustained remission for 6years.Treatment with tocilizumab resulted in immediate normaliza-tion of the CRP and complete resolution of all symptoms.A sustained response to tocilizumab was reported for at least 18months [10].In the third case report,a patient with RPC complicated with Sweet ’s syndrome was successfully treated with tocilizumab.Before that,the patient had been treated with adalimumab and etanercept,which initially resulted in aT a b l e 1S u m m a r y o f r e p o r t e d c a s e s o f r e f r a c t o r y R P C s u c c e s s f u l l y t r e a t e d w i t h t o c i l i z u m a b (8m g /k g m o n t h l y )[8–12]R e f e r e n c eA g e (s e x )D i s e a s e d u r a t i o n O r g a n i n v o l v e m e n t F o r m e r b i o l o g i c a l t r e a t m e n t O u t c o m e c r i t e r i a O n s e t o f e f f i c a c y D u r a t i o n o f f o l l o w -u p A d v e r s e e v e n t s K a w a i e t a l [9]29y e a r s (F )N A L a r y n g o t r a c h e a l i n v o l v e m e n t I n f l i x i m a b C l i n i c ,C R P ,C T s c a n ,s t e r o i d r e g i m e n N A 12m o n t h s N o K a w a i e t a l [9]52y e a r s (M )N A A o r t i t i s N o f o r m e r b i o l o g i c a l t r e a t m e n t C l i n i c ,C R P ,s t e r o i d r e g i m e n N A N A N o N a r s h i e t a l [10]43y e a r s (F )20y e a r s L a r y n g o t r a c h e a l i n v o l v e m e n t I n f l i x i m a b ,a d a l i m u m a b C l i n i c ,C R P ,s t e r o i d r e g i m e n R a p i d 18m o n t h s N o C h a n a e t a l [11]68(M )N A N o o r g a n i n v o l v e m e n t A d a l i m u m a b ,e t a n e r c e p t C l i n i c ,C R P ,s t e r o i d r e g i m e n R a p i d N A N o W a l l a c e e t a l [12]65(F )9m o n t h s L a r y n g o t r a c h e a l i n v o l v e m e n t I n f l i x i m a b C l i n i c ,C R P ,s t e r o i d r e g i m e n R a p i d N A N o W e b e r e t a l [12]40(M )3y e a r s L a r y n g o t r a c h e a l i n v o l v e m e n t I n f l i x i m a b C l i n i c ,C R P ,s t e r o i d r e g i m e n ,m e t h o t r e x a t e r e g i m e n 2n d m o n t h N A N oN A n o t a v a i l a b l eresponse,but failed to suppress the disease activity.After administration of adalimumab,the patient developed an ery-thematous pustular rash,consistent on biopsy with Sweet’s syndrome[11].In the fourth and the fifth case report,patients with refractory RPC complicated with laryngotracheal in-volvement were successfully treated with tocilizumab[12, 13].Our case supports the potential use of IL-6receptor blockade in at least a subset of patients with refractory RPC.Cardiovascular complications affect approximately one quarter of patients with RPC.Cardiac involvement is more prominent in the male population and requires more invasive procedures and complex surgery[14].After cardiac surgery, second-line immunosuppressive therapy should be initiated promptly in order to taper the corticosteroids.This approach may prevent or reduce the severity of some of the serious sequelae of RPC[14].The effect of biologicals on cardiac involvement is not very clear.We found three case reports where a beneficial effect on the aortic tissue was described.In one case report,a reduction of aortic aneurysm size was seen in a patient with RPC treated with infliximab[15].In another case report,a reduction of aortic aneurysm size was observed in a patient with MAGIC (mouth hand genital ulcers with inflamed cartilage)syndrome, treated with infliximab[16].In another case of RPC,a treat-ment with adalimumab seemed to be effective for aortitis[17]. In our case report,the cardiac situation had stabilized after initiating tocilizumab.We hypothesize a possible beneficial effect of tocilizumab on the cardiac involvement in RPC. More detailed studies with respect to cardiac tissue complica-tions are needed[14].In conclusion,we report a sustained response to toci-lizumab in a patient with refractory RPC with aortic involve-ment.Tocilizumab can be considered a therapeutic option in RPC patients who have failed anti-TNF therapy.However,to date,no clinical trial data on how to use biologics in RPC are available.More research is needed to assess the efficacy and adverse reactions of these agents in RPC since their use is currently restricted to patients not responding to conventional medical therapy[1,8].Disclosures None.Referenceshmer T,Treiber M,V on Werder A,Foerger F,Knopf A,HeemannU,Thuermel K(2010)Relapsing polychondritis:an autoimmunedisease with many faces.Autoimmun Rev9:540–546.doi:10.1016/ j.autrev.2010.02.0162.Rapini RP,Warner NB(2006)Relapsing polychondritis.J ClinDermatol24:482–4853.Zeuner M,Straub RH,Rauh G,Albert ED,Schölmerich J,Lang B(1997)Relapsing polychondritis:clinical and immunogenetic analy-sis of62patients.J Rheumatol24:96–1014.McAdam LP,O’Hanlan MA,Bluestone R,Pearson CM(1976)Relapsing polychondritis:prospective study of23patients and a review of the literature.Med(Baltimore)55(3):193–2155.Kent PD,Michet CJ Jr,Luthra HS(2004)Relapsing polychondritis.Curr Opin Rheumatol16(1):56–616.Kemta Lekpa F,Kraus VB,Chevalier X(2012)Biologics in relaps-ing polychondritis:a literature review.Semin Arthritis Rheum41: 712–719.doi:10.1016/j.semarthrit.2011.08.0067.Stabler T,Piette JC,Chevalier X,Marini-Portugal A,Kraus VB(2004)Serum cytokine profiles in relapsing polychondritis suggest monocyte/macrophage activation.Arthritis Rheum50:3663–3667 8.Sharma A,Gnanapandithan K,Sharma K,Sharma S(2013)Relapsing polychondritis:a review.Clin Rheumatol32:1575–1583.doi:10.1007/s10067-013-2328-x9.Kawai M,Hagihara K,Hirano T,Shima Y,Kuwahara Y,Arimitsu J,Narazaki M,Ogata A,Kawase I,Kishimoto T,Tanaka T(2009) Sustained response to tocilizumab,anti-interleukin-6receptor anti-body,in two patients with refractory relapsing polychondritis.Rheumatology(Oxford)48:318–331.doi:10.1093/rheumatology/ ken46810.Narshi CB,Allard SA(2012)Sustained response to tocilizumab,anti-IL-6antibody,following anti-TNF-alpha failure in a patient with relapsing polychondritis complicated by aortitis.Rheumatology51: 952–953.doi:10.1093/rheumatology/ker45111.Chana JK,Ahmed AA,Edmonds S(2012)Successful use oftocilizumab in a Caucasian patient with relapsing polychondritis complicated by Sweet’s syndrome.Rheumatology51(suppl3): iii153–iii15412.Wallace ZS,Stone JH(2013)Refractory relapsing polychondritistreated with serial success with interleukin6receptor blockade.J Rheumatol40(1):100–101.doi:10.3899/jrheum.12038113.Weber E,Gaultier JB,Paul S,Guichard I,Monard E,Cathébras P(2013)Sustained response with tocilizumab in a case of refractory relapsing polychondritis.Rev Med Interne.doi:10.1016/j.revmed.2013.02.01914.Dib C,Moustafa SE,Mookadam M,Zehr KJ,Michet CJ Jr,Mookadam F(2006)Surgical treatment of the cardiac manifestations of relapsing polychondritis:overview of33patients identified through literature review and the mayo clinic records.Mayo Clin Proc81(6):772–77615.Marie I,Lahaxe L,Josse S,Levesque H(2009)Sustained response toinfliximab in a patient with relapsing polychondritis with aortic involvement.Rheumatology(Oxford)48:1328–1329.doi:10.1093/ rheumatology/kep22416.Mekinian A,Lambert M,Beregi JP,Morell-Dubois S,Launay D,Queyrel V,Midulla M,Hachulla E,Hatron PY(2009)Aortic aneu-rysm in MAGIC syndrome successfully managed with combined anti-TNF-alpha and stent grafting.Rheumatology(Oxford)48: 1169–1170.doi:10.1093/rheumatology/kep17217.Seymour MW,Home DM,Williams RO,Allard SA(2007)Prolonged response to anti-tumour necrosis factor treatment with adalimumab(Humira)in relapsing polychondritis complicated by aortitis.Rheumatology(Oxford)46:1738–1739。