边缘叶脑炎最新综述
新型边缘叶脑炎一例3年随访观察

( 收稿 日期 : 2 O 1 4 — 1 0 — 1 0 ) ( 本 文 编辑 : 邹晨 双)
i n d u c e d l y mp h o p e n i a i n r a t s [ J ] .P L o S On e ,2 0 1 3 ,8( 3 ) :
( n 一1 0 , ± s )
目前 , 脑 缺 血 后 脑 损 伤 程 度 与 外 周 血 T 淋 巴 细 胞 亚 群 的 关 系 尚不 明确 , 本 研 究 旨 在 通 过 分 析 脑 缺 血 大 鼠 神 经 功 能评分 、 脑梗 死 面 积 百 分 比 与 外 周 血 C D 3 、 C D 4 。 。 、 C D 8 水平 、 C D 4 / C D8 比值 的 相关 性 来 探 索 脑缺 血 后 脑 损 伤 程 度 与 外 周 血 T 淋 巴细 胞 亚 群 的关 系 。结 果 显 示 , 模 型 组 大 鼠神 经 功 能 评 分 与 C D 8 水 平 及 脑 梗 死 面积 百 分 比 均 呈 正 相关 , 脑 梗死 面积百分 比与 C D 8 水 平 呈 正 相 关 , 与 C D4 水平及 C D 4 / C D 8 比值 呈 负 相 关 ; 这 与 Hu g等 [ 6 的 研 究
a r t e r y o c c l u s i o n:e v a l u a t i o n o f t h e mo d e l a n d d e v e l o p me n t o f a
n e u r o l o g i c e x a mi n a t i o n [ J ] . S t r o k e ,1 9 8 6 ,1 7 ( 3 ) : 4 7 2 — 4 7 6 .
边缘叶脑炎患者的临床及影像学特征及免疫治疗

边缘叶脑炎患者的临床及影像学特征及免疫治疗李桂霞【期刊名称】《中国继续医学教育》【年(卷),期】2016(8)12【摘要】目的:探析边缘叶脑炎患者影像学特征以及免疫治疗对策,为临床治疗提供依据。
方法回顾性分析我院2015年3月收治的边缘叶脑炎患者的个案资料,并分析免疫治疗的效果。
结果该患者以脑电图异常、行为及精神症状、明显近记忆力损害等表现为主,通过免疫治疗后,获得的效果较为明显。
结论边缘叶脑炎可能合并其他免疫性疾病,通过脑电图检查、脑MRI、脑脊液等检查对早期诊断边缘叶脑炎产生一定的帮助,采用免疫治疗干预获得的治疗效果较为明显。
%Objective To explore imaging characteristics and the edge of leaf encephalitis patients immune treatment measures, provide the basis for clinical treatment. Methods A retrospective analysis in March 2015 the edge of the leaf encephalitis patients in our hospital case information, and analyzes the effect of immunotherapy. Results The patients with abnormal electroencephalogram, behavior and mental symptoms, such as obvious in recent memory damage performance is given priority to, through the immune therapy, the effect is more obvious. Conclusion The edge of the leaf encephalitis may merge other autoimmune disease, through the eeg examination, MRI, cerebrospinal lfuid examination for early diagnosis of edge encephalitis produce certain help, by immune therapy intervention for treatment effect is more obvious.【总页数】2页(P56-57)【作者】李桂霞【作者单位】内蒙古赤峰学院附属医院中西医结合脑病科,内蒙古赤峰024000【正文语种】中文【中图分类】R742【相关文献】1.4例副肿瘤性边缘叶脑炎的临床和影像学特征报道 [J], 翟秀珍;王松柏2.副肿瘤性边缘叶脑炎临床特征分析 [J], 李波;闫佳兰;朱艳霞;冯连元;王雪笠3.副肿瘤性边缘叶脑炎的临床及影像学特征 [J], 汪东;王伟光;宁铁英;吕少萍4.边缘叶脑炎患者的临床及影像学特征1例 [J], 刘洋5.副肿瘤性边缘叶脑炎的临床和影像学特征 [J], 徐全刚;吴卫平;尹岭因版权原因,仅展示原文概要,查看原文内容请购买。
一例边缘叶脑炎的病例分析

一例抗NMDA-Ab抗体脑炎合并症状性癫痫的病例分析1 病例摘要1.1病史资料患者男,44岁,50天前足底按摩时自觉左脚抽筋感,随后感左下肢抽筋,意识尚清楚,随后双眼上翻、牙关紧闭、口吐白沫,伴肢体强直阵挛抽搐,伴意识丧失,无舌咬伤、二便失禁,持续2-3分钟缓解,共发作4次,最后一次发作后伴恶心,伴左下肢酸沉感,左脚底发热。
自发病以来,神志清,精神差,饮食可,睡眠差,二便正常,体重减轻3kg 智力发育正常;体格发育正常;性格、行为、心理发育正常。
饮酒8年,每周一次,一次半斤到一斤,已戒3年;吸烟20年,20支/天1.2治疗过程患者入院后,完善常规检查化验,头核磁双侧额叶皮层下洒在缺血性白质病变,PET-CT提示右顶叶代谢略减低,视频脑电监测期间未发作,为边缘脑电图,O,脑脊液蛋白升高,鞘内IgG合成率异常升高,脑脊腰穿脑脊液压力为290mmH2液抗NMDA-Ab(+):1:10,诊断为抗NMDA-Ab抗体脑炎合并症状性癫痫,给予注射用甲泼尼龙琥珀酸钠500mg,QD冲击治疗5天,并逐渐减量,由注射改为口服,激素治疗过程中,给予保护胃黏膜预防性治疗。
同时给予丙戊酸钠缓释片,500mg,BID,抗癫痫治疗。
自患者入院治疗,未出现癫痫发作,患者病情平稳,于2016-03-09出院。
2 分析及讨论2.1 抗NMDA-Ab抗体脑炎抗NMDA-Ab抗体脑炎是边缘叶脑炎的一种。
边缘叶脑炎是发生于大脑边缘系统的临床症候群。
特别是自身免疫介导性LE,临床上常呈亚急性起病,常常表现为近事遗忘、定向力障碍,也可出现精神行为异常,并常有癫痫发作等症状;有时难与病毒性脑炎、桥本脑病等相鉴别。
脑炎根据病因可以分为感染性脑炎和自身免疫性脑炎。
自身免疫性脑炎又可以分为抗NMDA受体脑炎、VGKC抗体脑炎、LGI1抗体脑炎《Lancet Neurol》2016年2月发布了《A clinical approach to diagnosis of autoimmune encephalitis》其中提出了抗NMDA受体脑炎诊断标准:单纯疱疹病毒性脑炎患者发病后数周可存在复发性免疫介导的神经系统症状(单纯疱疹后脑炎)同时满足以下三项标准可诊断:1.急性起病(少于3个月)或至少包括以下6个标准中的4项①异常(精神)行为或认知障碍②语言功能障碍(多语,少语,缄默症)③癫痫发作④运动失调,运动障碍,或强直/异常姿势⑤自主神经功能失调或中枢性低通气2.至少以下两项实验室研究结果:①异常EEG(局部或弥漫性慢波,或不规则电活动、癫痫活动、或极端δ波)②脑脊液细胞数增多或有寡克隆带3.合理排除其他疾病患者基本符合上述诊断标准,NMDA-Ab抗体脑炎的诊断成立。
两个不典型病例—边缘叶性脑炎 周盛年

• 左心房粘液瘤致颅内广泛多发性病变
•病例2
病例介绍
患者为22岁未婚女性,山东省菏泽市成武县人,因“发热伴 意识障碍,抽搐20天”入院。患者于2009年2月初无明显 诱因出现类似“感冒”症状:发热,乏力,头痛等。在当 地诊所按“感冒”治疗,无好转。2天后就诊于成武县人 民医院,仍持续发热,体温最高达38.2℃。住院2天后出 现注意力涣散,感情淡漠,胡言乱语,且有间歇性全身强 直性抽搐发作。当地医院未明确诊断,按“脑炎”治疗, 给予氯丙嗪、阿昔洛韦等药物,患者病情持续加重。发热 10天后患者陷入浅昏迷状态,转入我院急诊科治疗。
• 手术切除肿瘤。术后病理检查结果:右卵巢未成 熟畸胎瘤Ⅱ级,肿瘤体积11*8.5*5.3cm • 术后10天左右患者开始出现明显好转,意识逐渐 恢复,不自主运动消失,肌张力改善。
病例特点
患者主要表现为精神症状,自主神经功能障碍以及肌张力 障碍,癫痫发作。神经功能损伤定位于边缘系统,手术切 除卵巢肿瘤,经病理证实为卵巢未成熟畸胎瘤,肿瘤未侵 及神经系统。手术治疗后患者病情明显缓解,症状减轻。 诊断:畸胎瘤相关性边缘叶性脑炎
• 患者在发病前1周有过感冒病史,发病前5天有一过性右上 肢疼痛病史。否认高血压、糖尿病及冠心病病史,否认肝 炎、结核及此类传染病接触史。无手术外伤史、输血史及 药物过敏史。生于原籍,无外地久居史及毒物接触史,饮 酒20余年,约半斤/天,已戒除1年余。适龄结婚,育有1 子,妻子及儿子均体健。否认家族遗传病史。
患者早期可无症状或仅有轻微腹痛,大部分患者直到出现 神经系统症状就诊于神经科时才会发现单侧或双侧盆腔包 块。据报道,近60%患者在发现肿瘤之前先出现神经精神 症状。本例患者即是在发现原发肿瘤前先出现神经系统症 状。
诊断标准
感染性边缘叶脑炎的治疗及护理

治疗原则及目标
01
抗病毒治疗:使用抗病毒药物, 02
抗炎治疗:使用抗炎药物,如糖
如阿昔洛韦、更昔洛韦等
皮质激素、非甾体抗炎药等
03
降低颅内压:使用降颅内压药物, 04
预防并发症:预防和治疗脑水肿、
如甘露醇、呋塞米等
脑疝等并发症
05
维持生命体征:保持呼吸、循环、 06
康复治疗:进行康复治疗,如物
水电解质平衡等生命体征稳定
边缘叶脑炎的发生
免疫反应:自身免 疫反应或免疫缺陷
导致
临床表现及诊断
临床表现:发热、头 痛、恶心、呕吐、意 识障碍、肢体瘫痪等
鉴别诊断:与其他脑 炎、脑膜炎等疾病进 行鉴别
护理措施:保持呼吸 道通畅、预防感染、 维持水电解质平衡等
诊断方法:脑脊液检 查、影像学检查、病 原学检查等
治疗原则:抗病毒、 抗炎、支持治疗等
手术治疗
01
手术目的:清除病灶,减 轻症状
02
手术方式:开颅手术或立 体定向手术
03
手术时机:根据病情和患 者身体状况决定
04
术后护理:密切观察病情, 预防并发症,促进康复
康复治疗
03
04
心理治疗:针对患者的心理 问题进行心理疏导和治疗, 帮助患者恢复心理健康
认知治疗:通过认知训练和 康复帮助患者恢复认知功能
理治疗、言语治疗、认知训练等,
以改善患者预后和生活质量。
2
感染性边缘叶脑炎的治疗 方法
药物治疗
01
02
03
抗病毒药物:如阿昔洛 韦、更昔洛韦等
抗炎药物:如糖皮质激 素、非甾体抗炎药等
抗癫痫药物:如苯妥英 钠、卡马西平等
04
边缘性脑炎的研究进展

边缘性脑炎的研究进展
张玉波;田洪;刘磊
【期刊名称】《脑与神经疾病杂志》
【年(卷),期】2012(20)3
【摘要】边缘性脑炎(1imbicencephalitis,LE)是一种自身免疫性疾病,以行为改变以及记忆缺损等为主要临床特征的少见神经系统病变,有研究者把它分为副肿瘤性边缘性脑炎(paraneoplasticlimbicencephalitics,PLE)和非副肿瘤性边缘性脑炎(non-paraneoplasticlimbicencephalitics,NPLE),但笔者认为LE 首先应是自身抗原抗体反应导致的脑炎,从1960年LE的发现至今,人们对LE患者的病因、发病机制、临床表现、实验室检查、治疗与预后等方面都有了一定的认识。
现就LE的上述各方面的最新研究进展作一综述。
【总页数】3页(P239-241)
【作者】张玉波;田洪;刘磊
【作者单位】400020,重庆,解放军第324医院神经内科;400020,重庆,解放军第324医院神经内科;400020,重庆,解放军第324医院神经内科
【正文语种】中文
【中图分类】R741.02
【相关文献】
1.边缘性脑炎的临床研究进展 [J], 张玉波;周虎传;宋川;田洪;刘磊
2.电压门控钾通道自身抗体相关性边缘性脑炎的研究进展 [J], 周玲;翁泽安;李明;
张晓佳;查运红
3.边缘性脑炎的研究进展 [J], 吴倩;姜亚平
4.边缘性脑炎研究进展 [J], 王佳伟
5.病毒性脑炎与边缘性脑炎脑脊液病理学特征的对比分析 [J], 张萍淑; 陶莉; 刘妍; 吴小英; 张健; 乔思佳; 李佳慧; 郑慧; 元小冬
因版权原因,仅展示原文概要,查看原文内容请购买。
抗NMDAR脑炎:一种新型边缘叶脑炎

・综 述 ・
抗 NMDA R脑 炎: 一种新型边缘 叶脑 炎
周 晨 光 王建 平‘
郑 州 大学 第五 附属 医 院神经 内五科 . 河南 郑 州
4 5 0 0 5 2
【 摘要】 抗N 一 甲基一 M一 天冬氨酸受体 ( N — m e t h y l — D — a s p a r t a t e r e c e p t o r )脑炎是一种 自2 0 0 7 年确认 的由抗 N M D A
【 中图分 类号】R 5 1 2 . 3
【 文献标 识 码】 A
[ 文章 编号】1 6 7 3 — 9 7 0 1 ( 2 0 1 4 ) 1 2 t h y l - D- a s p a r t a t e r e c e p t o r e n c e p h a l i t i s : A n E W l i mb i c e n c e p h a l i t i s
受体 抗 体介 导 的可 治性 新 型边 缘 叶脑 炎 , 好 发 于年轻 女 性 , 临床 上 主要 表 现 为发 展 迅速 的神经 和 精神 障 碍综 合
征, 包 括 突 出 的精 神行 为 异 常 、 癫 痫发 作 、 异 常运 动 、 自主 神经 功 能 紊 乱 等 , 其 中 口面颌 肌 张 力 障碍 和 中 枢性 通 气 不 足是 该病 的相对 特 征性 表现 。MR I 检查 无 特异 性 改变 , 脑 电 图常 提 示 弥漫 性 的异 常 , 常规 脑脊 液 检查 无 特 异性 , 血和 脑脊 液 中 的 N MD A R亚 单位 N R1 抗 体 阳性 可 以明确 诊 断 。 对糖 皮 质激 素 、 免 疫球 蛋 白、 血浆 置 换等 免 疫 治疗 及 肿瘤 切 除反 应 良好 。 为更好 地 认识 该 疾病 , 本文 对其 临 床特 点 及发 病机 制 等做 一综 述 。 【 关 键词 】 新 型边 缘 叶脑 炎 ; 抗 N一甲基一 M一天冬 氨 酸受体 抗 体 ; 中枢性 通 气 不足
自身免疫性脑炎、自边缘叶脑炎、AR脑炎、皮质脑炎、小脑脑干脑炎等疾病分类、影像学特征和疾病要点
自身免疫性脑炎、自边缘叶脑炎、AR脑炎、皮质脑炎、小脑脑干脑炎等疾病分类、影像学特征和疾病要点自身免疫性脑炎及分类概念回顾自身免疫性脑炎是由脑实质的弥漫性或者多发性炎性病变导致的神经功能障碍,病理改变以灰质和神经元受累为主,也可累及白质和血管。
脑炎分为感染性和分感染性,感染性脑炎就是病原微生物导致的,如COVID-19感染导致脑炎。
非感染性脑炎,如免疫介导性的,妊娠引起的和药物引起的。
而免疫介导这组疾病就以自身免疫性脑炎多见,重要特点为:①非感染性;②经过临床治疗后大多数可以缓解。
AE分类:按抗原部位分类,按离子通道分类,按解剖部位来分类。
①重点关注抗细胞表面抗原抗体介导的自身免疫性脑炎,其中的抗NMDAR脑炎是最常见但又最不典型的,它的临床表现各异,各种情况都会出现,包括肢体无力、记忆下降、精神异常等,同样也可能没有任何特殊的症状。
特别是当病人早期以反应迟钝、活动缓慢到急诊室就诊时,需要特别警惕,容易漏诊和误诊。
②抗LGI1抗体相关脑炎、抗GABABR抗体相关脑炎、抗CASPR2抗体相关脑炎和抗AMPAR抗体相关脑炎较易识别,这四种脑炎的病变部位主要累及边缘系统,以精神、行为、记忆下降为突出表现,部分病人可能会出现癫痫发作。
但值得注意的是抗NMDAR脑炎同样也可以累及边缘系统,从而出现相关症状。
③自身免疫性脑炎还包括抗GAD65抗体相关脑炎,抗细胞内抗原抗体介导的以副肿瘤综合征为代表的疾病。
自边缘叶脑炎影像学特征概念回顾边缘系统是包含海绵体及杏仁体在内,负责多种功能如情绪、嗅觉、行为及长期记忆的大脑结构。
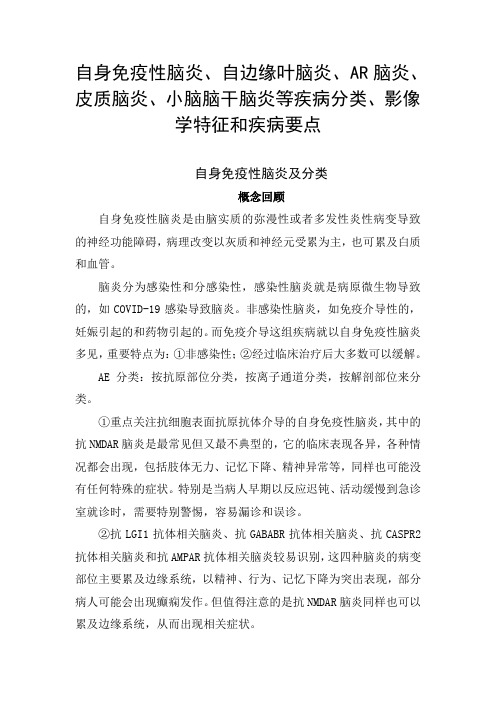
抗LGI1抗体相关脑炎为最常见的自身免疫性边缘叶脑炎,主要表现为海马和/或杏仁核肿胀、信号增高。
发病初期,MRI可表现为正常,随着疾病进展出现颞叶内侧高信号,长期随访发现41%-95%的患者发展为海马萎缩。
图1 抗LGI1抗体相关脑炎影像学表现①为电压门控性钾离子通道的脑炎,主要是以边缘系统损害为主,影像学上大多数以颞叶对称性损害,亦可为非对称性。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
ReviewLimbic encephalitis –a reviewN.E.Anderson *,P.A.BarberNeurology Department,Auckland City Hospital,Private Bag 92024,Auckland,New ZealandReceived 1October 2007;accepted 31December 2007AbstractThe clinical features of limbic encephalitis are diverse and early diagnosis of the disorder is frequently difficult.Four patients with limbic encephalitis are described.An antineuronal antibody was identified in three of these patients.Antibodies directed against volt-age-gated potassium channels,the N -methyl-D-aspartate receptor and an unidentified neuropil antigen were each found in one patient.The fourth patient had multifocal paraneoplastic encephalitis associated with small cell lung cancer.The clinical and imaging findings associated with these antibodies and the other antineuronal antibodies described in patients with limbic encephalitis are reviewed.An approach to the diagnosis and management of limbic encephalitis is presented.Ó2008Elsevier Ltd.All rights reserved.Keywords:Autoantibodies;Limbic encephalitis;Paraneoplastic syndromes1.IntroductionThe cardinal sign of limbic encephalitis is a severe impairment of short-term memory.1–4Anterograde amne-sia is often associated with behavioural and psychiatric symptoms such as anxiety,depression,irritability,person-ality change,acute confusional state,hallucinations and complex partial and secondary generalised seizures.The symptoms typically develop over a few weeks or months,but they may evolve over a few days.The neuropathologi-cal findings include mononuclear inflammatory cell infil-trates,loss of neurons,and proliferation of astrocytes and microglia in the hippocampus and amygdala.5,6In many patients limbic encephalitis is a paraneoplastic syn-drome,which is most commonly associated with small cell lung cancer (SCLC),breast cancer,testicular tumours,ter-atomas,Hodgkin’s lymphoma and thymomas.2Neurolog-ical symptoms precede diagnosis of the malignancy in 60%–75%of these patients.2,4Limbic encephalitis can also occur in the absence of malignancy.7,8The clinical manifestations of limbic encephalitis are di-verse and patients often present with a puzzling clinical pic-ture.Delayed diagnosis is common,but improvements in neuroimaging and identification of antineuronal antibodies in patients with limbic encephalitis have facilitated recogni-tion of the disorder.Early diagnosis is important,because limbic encephalitis may improve after immunotherapy or removal of a tumour,if one is present.We describe four patients with limbic encephalitis.We review the antineuronal antibodies associated with limbic encephalitis and describe a clinical approach to patients with suspected limbic encephalitis.2.Patients 2.1.Patient 1A 41-year-old woman presented following a generalised tonic-clonic seizure.During the previous six months there had been a change in her behaviour and loss of interest in normal activities.In the two weeks prior to admission,she experienced recurrent stereotyped episodes with flash-ing lights in the right visual field and a left hemicranial headache.One week later she developed focal motor status epilepticus in the right arm.She had a history of smoking0967-5868/$-see front matter Ó2008Elsevier Ltd.All rights reserved.doi:10.1016/j.jocn.2007.12.003*Corresponding author.Tel.:+6493797440;fax:+6493754309.E-mail address:neila@ (N.E.Anderson)./locate/jocnAvailable online at Journal of Clinical Neuroscience 15(2008)961–971for30years.Neurological examination showed impairment of short-term memory,dysphasia and right inferior quadrantanopia.Antinuclear antibody was positive(titre1:320),but dou-ble-stranded DNA,extractable nuclear antigen,antineutr-ophil cytoplasmic and thyroid microsomal antibodies were absent.Chest radiography was normal.MRI with T2-weighted andfluid attenuation inversion recovery (FLAIR)sequences showed multiple hyperintense cortical and subcortical lesions in both cerebral hemispheres including the medial temporal lobes(Fig.1).Contrast-en-hanced scans were not obtained.Cerebral angiography was normal.Electroencephalography(EEG)showed epi-leptiform activity arising independently from both hemi-spheres and electrographic seizures originating in the right fronto-temporal and left posterior temporal regions. The cerebrospinalfluid(CSF)had9Â106/L lymphocytes, but was otherwise normal.A right frontal lobe brain biopsy was normal except for a focal collection of lympho-cytes in the overlying dura.Dural and brain cultures were sterile.Prednisone60mg/day and azathioprine200mg/day were started,but there was no improvement in the dyspha-sia or cognitive impairment.Focal motor status,complex partial seizures and occasional generalised seizures contin-ued despite treatment with multiple anti-epileptic drugs. MRI six months later did not show any change.Fifteen months after her original presentation she was readmitted with generalised status epilepticus.A chest radiograph showed opacification of the left upper lobe.She died four days later.Post-mortem examination revealed a SCLC arising in the left main bronchus and disseminated systemic metasta-ses with one small metastasis in the right frontal lobe of the brain.There were patchy perivascular lymphocytic infil-trates,astrocytic proliferation and loss of neurons in the cerebral cortex including the amygdala and parahippocam-pal gyri.Serum and CSF were not available to search for antineuronal antibodies.2.2.Patient2A67-year-old woman with Type II diabetes mellitus and treated hypothyroidism presented with a three-month his-tory of progressive anterograde amnesia,fluctuating confu-sion,anxiety,delusions,hallucinations,and complex partial and tonic-clonic seizures.She had had persistent hyponatraemia for nine months prior to presentation. She was afebrile,drowsy,restless and disorientated. Short-term memory was impaired,verbal and motor re-sponses were slow and her mini-mental state examination (MMSE)score was16/30.The rest of the neurological examination was normal.Thyroid function tests,thyroid antibodies,MRI,CSF and CT of the chest,abdomen and pelvis were normal.The EEG showed widespread irregular slow wave activity.Voltage-gated potassium channel(VGKC)antibodies(courtesy of Dr Angela Vin-cent)were present at a level of5441pM(normal<100 pM).She was treated with methylprednisolone1g/day over5days,but no other immunosuppressive treatment was used.Three months after treatment her mental state had improved(MMSE26/30),the EEG had normalised and the VGKC antibody level had dropped to311pM. Twelve months later the MMSE was28/30.2.3.Patient3A58-year-old woman developed a prodromal illness with arthralgias,rash and headache.Two weeks later there was a rapid change in her behaviour with elevatedmood, Fig.1.Patient1:Fluid attenuation inversion recovery(FLAIR)MRI showing increased signal in both medial temporal lobes and the left occipital lobe(a) and the left lateral temporal lobe(b).962N.E.Anderson,P.A.Barber/Journal of Clinical Neuroscience15(2008)961–971poor concentration,hallucinations,insomnia,disinhibited social and sexual behaviour,and coprophagia.At times she was restless and agitated,but for long periods she was catatonic,mute and akinetic with severe rigidity and dystonia in the limbs.These periods were accompanied by apnoeic episodes causing respiratory acidosis.There were no focal neurological signs.Psychotropic medications and electroconvulsive therapy did not produce any improvement.She developed recurrent seizures and hypo-ventilation requiring admission to the intensive care unit. Thyroid function tests,thyroid microsomal antibodies, MRI and CSF were normal.The EEG showed a severe generalised abnormality of the background activity.Anti-bodies to the N-methyl-D-aspartate receptor(NMDAR) were identified,but antineuronal nuclear antibody,type I (anti-Hu)and anti-Ma2antibodies were not present.CT of the chest,abdomen and pelvis,and intravaginal ultra-sound were normal.She had a bilateral oophorectomy, but no ovarian abnormality was found.She was treated with high dose steroids,two courses of intravenous immu-noglobulin and pulsed intravenous cyclophosphamide. There was a gradual improvement in her behavioural symptoms over the next six months,but there was a persis-tent deficit of immediate and delayed recall on memory tests.2.4.Patient4A58-year-old woman presented with a six-month his-tory of severe anxiety,panic attacks,depression,dysphasia and partial motor seizures involving the right face.The neurological examination showed anterogradeamnesia, Fig.2.Patient4:Fluid attenuation inversion recovery(FLAIR)MRI at presentation showing areas of increased signal in the(a)right anterior temporal and medial temporal lobes;(b)both medial temporal lobes;(c)insular cortex bilaterally,right medial frontal lobe and left occipital lobe and(d)left parietal lobe.N.E.Anderson,P.A.Barber/Journal of Clinical Neuroscience15(2008)961–971963non-fluent dysphasia and minor upper motor neuron signs in the right arm.The serum sodium was128mmol/L.MRI revealed multiple non-enhancing cortical lesions including abnormalities in both medial temporal lobes(Fig.2).The CSF protein was0.79g/L,but the leukocyte count and glu-cose concentration were normal and there were no oligocl-onal bands.There was generalised slowing of the background EEG activity,but there was no focal or epilep-tiform abnormality.Anterior mediastinal and pleural masses were identified on CT.Biopsy of the pleural mass showed metastatic thymoma.She was treated with cyclo-phosphamide,adriamycin,cisplatin and prednisone followed by surgical debulking of the tumour.Her symp-toms resolved and the neurological examination returned to normal during chemotherapy.After six months MRI showed complete resolution of the cortical lesions.An antibody that recognised an antigen expressed on neuronal cell membranes and dendrites in the hippocampus and the molecular layer of the cerebellum was found in the patient’s serum(courtesy of Dr Josep Dalmau).Anti-Hu, collapsin response-mediator protein(CRMP-5)and VGKC antibodies were absent.3.DiscussionThese four patients illustrate several points about auto-immune limbic encephalitis:the clinical manifestations are diverse,paraneoplastic and non-paraneoplastic forms of the disease exist,and improvement may occur with treat-ment.An antineuronal antibody was identified in three of our patients:VGKC antibody in patient2,NMDAR anti-body in patient3and an antineuropil antibody in patient4. Serum and CSF from patient1were not available to search for an antineuronal antibody,but we suspect this patient had the anti-Hu antibody.A SCLC was discovered at au-topsy and the post-mortem abnormalities were typical of paraneoplastic encephalomyelitis.Anti-Hu is a marker of paraneoplastic encephalomyelitis associated with SCLC and epilepsia partialis continua can be the presenting man-ifestation of anti-Hu-associated encephalomyelitis.9,10 The clinical manifestations of limbic encephalitis are protean,but investigations can assist in the diagnosis.A lymphocytic pleocytosis,an increased protein concentra-tion and oligoclonal bands in the CSF provide support for a diagnosis of limbic encephalitis.However,similar CSF abnormalities can occur with other inflammatory dis-orders or infections,and the CSF may be normal in limbic encephalitis.The EEG typically shows focal or generalised slow wave abnormalities,and epileptiform activity,electro-graphic seizures or periodic lateralised epileptiform dis-charges in the temporal regions.4T2-weighted and FLAIR MRI sequences often show hyperintense signal and mild swelling of the medial temporal lobes.11,12These changes may eventually be replaced by medial temporal lobe atrophy.Fluorodeoxyglucose positron emission tomography(PET)may reveal hypermetabolism in the medial temporal lobes,even when MRI is normal.13Several antineuronal antibodies have been described in patients with limbic encephalitis.These antibodies are help-ful diagnostic markers in a patient presenting with an unu-sual constellation of clinical and imaging abnormalities (Table1).3.1.Anti-neuronal nuclear antibody,type IAnti-neuronal nuclear antibody,type I(anti-Hu)recog-nises a family of RNA-binding proteins expressed in neuro-nal nuclei.One of these proteins,HuD,is expressed in SCLC cells and has a major role in triggering the immune response.14The most common clinical presentation of anti-Hu-associated paraneoplastic disease is sensory neuronop-athy.Limbic encephalitis is the main presenting manifesta-tion in10%of patients.15Other manifestations may include brainstem encephalitis,cerebellar ataxia,motor neuronop-athy,autonomic neuropathy,and symptoms of multifocal cortical disease including epilepsia partialis continua,apha-sia and visualfield abnormalities.15,16Three-quarters of the Table1Anti-neuronal antibodies associated with limbic encephalitisAntibody MaintumoursAdditional clinicalfeaturesResponse totreatment aAnti-Hu SCLC Sensory neuronopathy PoorBrain stem,cerebellarsignsMotor neuronopathyAutonomicneuropathyMultifocalencephalomyelitisAnti-Ma2Testis Hypothalamicdysfunction30%improveRostral brain stemdysfunctionAtypical ParkinsonismCRMP-5SCLC,thymomaCerebellar ataxia PoorEncephalomyelitisChorea,parkinsonismUveitis,retinopathyNeuropathyAmphiphysin Breast,SCLCStiffperson syndrome PoorMultifocal diseaseVGKC Nil REM sleep behaviourdisorderGoodHyponatraemiaNMDAR OvarianteratomaPsychiatric symptoms GoodDystoniaDepressedconsciousnessHypoventilationNeuropil SCLC,thymomaMultiple GoodCRMP-5=collapsin response-mediator protein-5;NMDAR=N-methyl-D-aspartate receptor;SCLC=small cell lung carcinoma;VGKC=volt-age-gated potassium channel;REM=rapid eye movement.a Treatment of tumour,immunotherapy,or both.964N.E.Anderson,P.A.Barber/Journal of Clinical Neuroscience15(2008)961–971patients with anti-Hu have SCLC,15,16but only50%of pa-tients with limbic encephalitis and SCLC have anti-Hu.17 Anti-Hu-negative patients with limbic encephalitis and SCLC do not usually develop symptoms beyond the limbic system and are more likely to improve after treatment of the cancer than anti-Hu-positive patients.17Anti-Hu-associated paraneoplastic encephalomyelitis typically has a poor prognosis.Treatment of the tumour may be associated with stabilisation of the neurological symptoms,but a dramatic improvement is rare.15Limbic encephalitis is more likely to respond to treatment than the other neurological manifestations of anti-Hu.23.2.Anti-Ma2Ma proteins have a role in the biogenesis of mRNA.18 They are expressed in neurons,tumours of patients with anti-Ma-associated paraneoplastic disease and testicular germ cells.18–20Ma2is the major autoantigen,but addi-tional antibodies to Ma1or Ma3occur in40%of patients.18Anti-Ma2is mainly found in young men with a testicu-lar germ cell tumour,but it can occur with non-small cell lung cancer,breast cancer and other tumours.18,21A classi-cal syndrome of limbic encephalitis is seen in20%of anti-Ma2patients,but more commonly limbic encephalitis is associated with hypothalamic and brain stem dysfunction. Symptoms of hypothalamic disease may include hypersom-nia,cataplexy,rapid eye movement(REM)sleep behaviour disorder,hypnagogic hallucinations,gelastic seizures, weight gain,hyperthermia and diabetes insipidus.21,22Ver-tical gaze paresis and mild cerebellar ataxia are the most common signs of brain stem disease.Atypical Parkinson-ism is an uncommon manifestation.Most Ma2-positive patients have MRI abnormalities in the hypothalamus,thalamus,midbrain and medial tempo-ral lobes.Some lesions show contrast enhancement and mi-mic a tumour.18,21CSF hypocretin levels are low or undetectable.23Neuropathological examination demon-strates perivascular and interstitial infiltrates of T and B lymphocytes,and plasma cells.18,24The neurological symptoms of Ma2-encephalitis im-prove following immunotherapy or treatment of the tu-mour in one-third of patients.21Men below the age of50 with Ma2-encephalitis usually have a microscopic intratu-bular germ cell tumour,even when tumour markers and imaging show no evidence of cancer.25Orchidectomy is recommended if there is no other type of tumour and there is new testicular enlargement,a history of cryptorchidism or ultrasound evidence of testicular microcalcification. The neurological disorder often improves after an orchidectomy.3.3.Collapsin response-mediator protein antibodyThe CRMP-5antibody is associated with a wide variety of clinical syndromes including cerebellar ataxia,encepha-lomyelitis,parkinsonism,uveitis,retinopathy,optic neu-ropathy,polyradiculopathy,and sensory,sensorimotor, autonomic,or cranial neuropathy.26,27An association be-tween limbic encephalitis and chorea is a clue to the pres-ence of the CRMP-5antibody.28Some patients with the CRMP-5antibody have clinical,MRI and neuropatho-logicalfindings that are indistinguishable from other forms of paraneoplastic limbic encephalitis.29,30Limbic encephalitis may be associated with multifocal cortical disease.30,31The CRMP-5antibody has been found in patients with SCLC,malignant thymoma and other neoplasms,but10% of patients do not have an identifiable neoplasm.26This antibody has been identified in a few patients with SCLC or thymoma without paraneoplastic disease.26Neurologi-cal improvement may follow treatment of an underlying thymoma.29The CRMP-5antibody is probably identical to the anti-CV2antibody.29,32,333.4.Amphiphysin antibodiesAmphiphysin antibodies werefirst discovered in women with breast cancer and stiffperson syndrome,but these antibodies are associated with a broad spectrum of neuro-logical disorders including encephalopathy,cerebellar atax-ia,myelopathy and neuropathy.34Three-quarters of patients with amphiphysin antibodies have coexisting auto-antibodies,which may account for the diverse clinical man-ifestations.Rarely,amphiphysin antibodies have been found in patients with limbic encephalitis and SCLC.34,35 Some of these patients have coexisting anti-Hu and VGKC antibodies,which may be independently associated with limbic encephalitis.3.5.Voltage-gated potassium channel antibodiesMost patients with VGKC-associated limbic encephali-tis present with a subacute amnesic syndrome,as seen for patient2.Simple motor and complex partial seizures,and REM sleep behaviour disorder are common,but headache, drowsiness and loss of consciousness are not usually pres-ent.36–39Hyponatraemia is common.The CSF leukocyte count is often normal,but there may be a mild lymphocytic pleocytosis.38MRI abnormalities are usually confined to the hippocampus and amygdala37,38but occasionally there also is signal change in the basal ganglia.40Most patients with VGKC antibodies do not have an underlying malig-nancy,but patients with SCLC,malignant thymoma and prostate adenocarcinoma have been found.36,37,41,42A coexisting antiglial nuclear antibody may indicate an underlying SCLC.43VGKC-associated limbic encephalitis should be treated with high-dose intravenous methylprednisolone.37Patients also may respond to intravenous immunoglobulins or plas-mapheresis followed by high dose prednisone.41Although patients often improve following treatment,residual medial temporal lobe atrophy and memory deficits areN.E.Anderson,P.A.Barber/Journal of Clinical Neuroscience15(2008)961–971965common.37,38Improvement is more likely with early treat-ment.Clinical improvement is associated with a reduction in the antibody level.VGKC antibodies also are found in patients with iso-lated neuromyotonia and Morvan’s syndrome.44–47Mor-van’s syndrome resembles limbic encephalitis with hallucinations,delirium,memory impairment,insomnia, REM sleep behaviour disorder and autonomic hyperactiv-ity accompanied by myokymia.45,46The CSF and MRI are often normal.There usually is no underlying malignancy, but Morvan’s syndrome may occur in patients with thy-moma and other malignancies.Autonomic hyperactivity and neuromyotonia occasionally occur with VGKC-associ-ated limbic encephalitis.36–39VGKC antibodies are detected with a radioimmunopre-cipitation assay using a-dendrotoxin,which binds to Kv1.1,Kv1.2and Kv1.6ion channel subunits.48Hippo-campal Kv1.1potassium channels have a role in neuronal excitability and memory.Sera from patients with limbic encephalitis bind preferentially to Kv1.1channels,whereas sera from patients with neuromyotonia or Morvan’s syn-drome bind relatively more strongly to Kv1.2and Kv1.6 channels.48This may explain why some patients develop central nervous system symptoms without peripheral nerve involvement.VGKC antibody titres are lower in patients with neuromyotonia and Morvan’s syndrome than in pa-tients with limbic encephalitis.3.6.N-methyl-D-aspartate receptor antibodiesAntibodies directed against the NMDAR have been identified in young women with an ovarian teratoma and a severe but treatment-responsive encephalitis.49–55Most of these patients have a prodromalflu-like illness,which is followed by acute,severe psychiatric symptoms including personality change,paranoia and delusional thought pro-cesses.Agitation and confusion alternate with periods of staring,dystonia and catatonic posturing.These symptoms are often wrongly attributed to acute schizophrenia,neuro-leptic malignant syndrome or lethal catatonia and the pa-tients are initially referred to a psychiatrist.54Severe anterograde amnesia is often present,but it may be masked by the psychiatric manifestations.Other clinical features may include generalised and complex partial seizures,cho-reoathetosis,myoclonus,dyskinesias,decreased level of consciousness,central hypoventilation and signs of auto-nomic instability.49,52Hyponatraemia does not usually occur.55Most patients with an NMDAR antibody have an ovar-ian teratoma,of which70%are benign.In some patients a teratoma has been found in the mediastinum and other pa-tients have no underlying tumour.52The ovarian tumour may be detected with CT or intravaginal ultrasound. PET may be negative if the tumour is benign.A CSF lymphocytic pleocytosis and oligoclonal bands are found in most of these patients.52MRI of the brain is often normal,but may show T2and FLAIR abnormalities in the medial temporal lobes,other areas of the cerebral cortex,cerebellum and brain stem.Neuropathological abnormalities include microglial proliferation and neuro-nal degeneration in the hippocampus,but the changes may be more widespread.52,56Unlike the other forms of autoimmune limbic encephalitis,perivascular and intersti-tial T cell infiltrates are uncommon.Serum and CSF contain antibodies directed against an antigen expressed on the cell membranes of hippocampal neurons.The antibody may be barely detectable in the ser-um.52These antibodies react with glutamate-binding NR1/ NR2B-containing heteromers of the NMDAR.The tu-mours in these patients contain nervous tissue that express NR1/NR2subunits and react with the patient’s antibody. Ectopic expression of NR1/NR2subunits by nervous tissue in a teratoma may cause failure of immune tolerance and trigger the immune response.The prodromal viral-like ill-ness may facilitate the abnormal immune response.52 There often is a dramatic clinical improvement following tumour resection,plasmapheresis,intravenous immunoglobulin or immunosuppressive therapy.52Immu-notherapy alone may produce a transient improvement, but resection of the tumour appears to be essential for maintenance of the response.The encephalitis may recur if the tumour recurs.52An NMDAR antibody was found in patient3.Her clin-ical presentation was typical of the clinical syndrome associ-ated with this antibody,but our patient was unusual in thata tumour was not found and there was no CSF pleocytosis.3.7.Antibodies against novel cell membrane antigenAn antibody to an unknown antigen expressed in the cell membrane of hippocampal neurons has been found in patients with limbic or multifocal encephalitis,as seen with patient4.55,57The clinical and imaging features are similar to NMDAR antibody-associated encephalitis. These patients have either a teratoma or thymoma.55Pa-tient4illustrates the dramatic improvement that follows treatment of the tumour.553.8.Other paraneoplastic antineuronal antibodiesAn antibody to adenylate kinase5was found in two men with non-paraneoplastic limbic encephalitis that was refractory to immunotherapy,while an antibody to BR ser-ine/threonine kinase2was detected in a patient with limbic encephalitis and SCLC.58,59Anti-neuronal nuclear anti-body types II(anti-Ri)and III may be associated with an encephalopathy or dementia,but the clinical features and neuropathology suggest disease extending beyond the lim-bic system.60,613.9.Pathogenic significance of antineuronal antibodiesEctopic expression of a neuronal protein within a tu-mour appears to trigger an anti-tumour immune response.966N.E.Anderson,P.A.Barber/Journal of Clinical Neuroscience15(2008)961–971If there is a breakdown of immune tolerance in the brain, antibodies and cytotoxic T cells generated by this immune response may react with neurons expressing these onconeu-ral antigens.62However,it is not known if these anti-neu-ronal antibodies are involved in the pathogenesis of neurological disease.Antibodies directed against ion chan-nels and receptors in cell membranes,dendrites and syn-apses(VGKC and NMDAR antibodies)may interfere with neural transmission.Limbic encephalitis associated with antibodies against cell membrane antigens often improves after removal of the antibody,or treatment of the tumour.57Except for pa-tients with anti-Ma2and a testicular tumour,patients who have antibodies against intracellular antigens do not re-spond as well to immunotherapy or treatment of the cancer.15,573.10.Diagnostic approachBased on recent studies,an approach to the investiga-tion and acute management of patients with limbic enceph-alitis has been proposed.63Thefirst step is to obtain MRI of the brain and CSF examination.MRI abnormalities in the medial temporal lobes are helpful in confirming a diag-nosis of limbic encephalitis11,12but normal imaging does not exclude the diagnosis.Medial temporal lobe abnormal-ities also occur with herpes simplex encephalitis and other disorders.Once an infectious cause has been excluded,the second step is to search for a tumour and an antineuronal antibody.There are no clinical,imaging or CSF abnormal-ities that are specific to any particular immune phenotype, but there may be clues to which tumour and antibody is present(Fig.3).Many of the appropriate antibody tests are not available in commercial laboratories and,depend-ing on the clinical situation,CSF and serum may need to be sent to a research laboratory(Table2).57Patients with autoimmune limbic encephalitis can deteriorate rapidly and treatment with intravenous immunoglobulin or high-dose intravenous methylprednisolone should be com-menced while awaiting the results of the antibody tests.57,63 3.11.Differential diagnosisOne of the difficulties in the diagnosis of limbic enceph-alitis is that other neurological disorders can have a similar clinical presentation(Table3).It may be difficult distin-guishing between limbic encephalitis and an acute confusional state secondary to a metabolic or toxic enceph-alopathy.Impairment of attention and global cognitive impairment are typical of an acute confusional state,but these features may be present in limbic encephalitis.Anter-ograde amnesia is the dominant early manifestation of Alz-heimer’s disease,but degenerative neurological disorders have a more insidious onset of symptoms than limbicN.E.Anderson,P.A.Barber/Journal of Clinical Neuroscience15(2008)961–971967。