三环类抗抑郁药(专业知识值得参考借鉴).docx
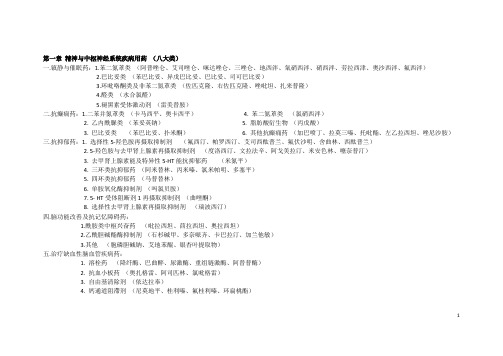
三环类抗抑郁药&部分抗精神病药的药代动力学参数及参考治疗浓度范围

三环类抗抑郁药&部分抗精神病药的药代动力学参数及参考治疗浓度范围药物血浆半衰期(h)达峰时间(h)达稳态血药浓度时间(Day)常用剂量(mg/day)成人老人有效血药浓度(ng/ml)阿米替林17~40 2~8 4~10 150~300 20~100 80~250*去甲替林15~93 2~8 4~19 50~150 10~75 50~150丙咪嗪6~24 1~6 2~5 75~300 20~100 150~250*去甲丙咪嗪12~76 2~8 2~11 50~200 10~75 125~300*多虑平8~36 2~6 2~8 200~400 30~200 150~250*氯丙咪嗪17~28 2~8 4~10 75~300 100~350 部分抗精神病药的药代动力学参数及参考治疗浓度范围药物达峰时间(h)半衰期(h)生物利用度(%)表观分布容积(L/Kg)血浆清除率(L/min)参考治疗浓度范围(ng/ml)氯丙嗪2~4 30 30 20 0.6 50~500氟哌啶1~6 20 60 25 1 4~15 醇氯氮平 1.1~3.6 9.1~17.4 1.6~7.3 8.7~53.3 100~800氟奋乃2~5 16 0.2~2.5 静奋乃静2~5 10 low 20 1.6 0.2~4甲硫达2~4 24 250~1250 嗪三氟拉1~5 16 1~3嗪丁酰拉1~3 12 50~300 嗪美索达2~4 20 150~1000 嗪氨砜噻1~3 34 2~14 吨碳碳生物利用度 100%动力学参数达峰浓度时间2~4h表观分布容积 0.79±0.34L/kg消除半衰期 22±8 h(12~30h)血浆清除率 0.35±0.11ml/min/kg经尿排出 95±15%有效血清锂浓度 0.3~1.3mmol/L中毒血清锂浓度 >1.5mmol/L卡马西平的浓效关系抗癫痫的有效浓度范围为8~12mg/L (34~51mmol/L)用于治疗燥狂发作和情感障碍维持治疗的有效浓度范围为4~12mg/L(17~ 51mmol/L)我院吴艳梅、姜佐宁等1994年的研究结果是,卡马西平浓度在5.1~9.8mg/L的范围内63.7%的病人对维持治疗有效。
药学专业知识(二)各系统药物大汇总

第一章精神与中枢神经系统疾病用药第一节镇静与催眠药巴比妥类:苯巴比妥苯二氮卓类:地西泮其他类:唑吡坦、佐匹克隆第二节抗癫痫药巴比妥类:苯巴比妥、异戊巴比妥、扑米酮苯二氮卓类:地西泮、氯硝西泮、硝西泮乙酰脲类:苯妥英钠二苯并氮卓类:卡马西平、奥卡西平γ-氨基丁酸类似物:加巴喷丁、氨己烯酸脂肪酸类:丙戊酸钠第三节抗抑郁药三环类:阿米替林、丙咪嗪、多塞平5-羟色胺与去甲肾上腺素再摄取抑制剂〔SNRI〕:文拉法辛、度洛西汀四环类:马普替林选择性去甲肾上腺素再摄取抑制剂:瑞波西汀选择性5-羟色胺再摄取制剂〔SSRI〕:帕罗西汀、舍曲林、西酞普兰、氟西汀单胺氧化酶抑制剂:吗氯贝胺其他:去甲肾上腺素能及特异性5-HT再摄取抑制剂〔NaSSA〕:米氮平5-HT手提阻断剂/再摄取抑制剂〔SARI〕:曲唑酮第四节脑功能改善及抗记忆障碍药酰胺类中枢兴奋药:吡拉西坦、茴拉西坦、奥拉西坦乙酰胆碱酯酶抑制剂:多奈哌齐、利斯的明、石杉碱甲其他类:胞磷胆碱钠、艾地苯醌、银杏叶提取物第五节镇痛药1.麻醉性镇痛药阿片生物碱:吗啡、可待因、罂粟碱半合成吗啡:双氢可待因、丁丙诺啡、氢吗啡酮合成阿片类:1〕苯哌啶类:芬太尼、舒芬太尼、阿芬太尼2〕二苯甲烷类:美沙酮、右丙氧酚3〕吗啡烷类:佐啡诺、布托啡诺4〕苯并吗啡烷类:喷他佐辛、非那佐辛2.非麻醉性镇痛药非甾体抗炎药:吲哚美辛、布洛芬中枢性镇痛药:曲马多第二章解热、镇痛抗炎药及抗通风药第一节解热、镇痛抗炎药水酸类:阿司匹林、贝诺酯乙酰苯胺类:对乙酰氨基酚芳基乙酸类:吲哚美辛、双氯芬酸、萘美丁酮芳基丙酸类:布洛芬、萘普生1,2-苯并噻嗪类:吡罗昔康、美洛昔康选择性COX-2抑制剂:塞来昔布、依托考昔、尼美舒利第二节抗痛风药选择性抗通风性关节炎药:秋水仙碱抑制尿酸生成药:别嘌醇促进尿酸排泄药:丙磺舒、苯溴马隆促进尿酸分解药:拉布立酶、聚乙二醇尿酸酶第三章呼吸系统疾病用药第一节镇咳药中枢性镇咳药:右美沙芬、喷托维林、地美索脂、二氧丙嗪、替培啶、福米诺本、普罗吗酯、福尔可定、可待因外周性镇咳药:苯丙哌林、普诺地嗪第二节祛痰药多糖纤维素分解剂:溴己新、氨溴索、乙酰半胱氨酸粘痰溶解剂:氯化铵含有分解脱氧核糖核酸的酶类:糜蛋白酶、脱氧核糖核酸酶黏液调节剂:羧甲司坦、厄多司坦第三节平喘药1.β2受体冲动剂:1〕长效:福莫特罗、沙美特罗、丙卡特罗2〕短效:沙丁胺醇、特布他林2.白三烯受体阻断剂:孟鲁司特、扎鲁司特3.磷酸二酯酶抑制剂:茶碱、氨茶碱、多索茶碱、二羟丙茶碱4.M胆碱受体阻断剂:异丙托溴铵、噻托溴铵5.吸入性糖皮质激素:丙酸倍氯米松、丙酸氟替卡松、布地奈德第四章消化系统疾病用药第一节抗酸剂与抑酸剂1.抗酸剂:1〕吸收性抗酸剂:碳酸氢钠2〕非吸收性抗酸剂:铝、镁制剂〔铝碳酸镁、氢氧化铝、三硅酸镁〕2.抑酸剂:1〕组胺H2受体阻断剂:西咪替丁、雷尼替丁、法莫替丁、尼扎替丁2〕质子泵抑制剂:奥美拉唑、兰索拉唑、泮托拉唑、雷贝拉唑、埃索美拉唑第二节胃黏膜保护剂1.铝剂:硫糖铝2.铋剂:胶体果胶秘、枸橼酸铋钾3.萜烯类化合物:提普瑞酮第三节助消化药1.乳酸菌制剂:乳酶生、乳酸菌素2.消化酶制剂:胰酶、胃蛋白酶第四节解痉药与促胃肠动力药1.解痉药:颠茄、阿托品、东莨菪碱、山莨菪碱2.促胃肠动力药:1〕多巴胺D2受体阻断剂〔中枢和外周〕:甲氧氯普胺2〕外周性多巴胺D2受体阻断剂:多立酮3〕5-羟色胺受体冲动剂:西沙必利、莫沙必利第五节泻药与止泻药1.泻药:1〕容积性泻药:硫酸镁、硫酸钠2〕渗透性泻药:乳果糖3〕刺激性泻药:酚酞、比沙可啶、番泻叶、蓖麻油4〕润滑性泻药:甘油栓剂〔开塞露〕5〕膨胀性泻药:聚乙二醇40002.止泻药:1〕吸附药和收敛药:双八面体蒙脱石2〕抗动力药:洛哌丁胺、地酚诺酯3.微生态制剂:1〕乳酸菌类:乳酸杆菌、双歧杆菌、粪肠球菌、枯草杆菌2〕芽孢杆菌类:蜡状芽孢杆菌、地衣芽孢杆菌3〕非常驻菌类:丁酸梭菌、诺酸梭菌4〕复方制剂:双歧杆菌-嗜酸杆菌-肠球菌三联活菌、枯草杆菌-肠球菌二联活菌第六节肝胆疾病辅助用药1.促代类药及维生素:门冬氨酸钾镁、各种氨基酸制剂、各种水溶性维生素2.必需磷脂类:多烯磷脂酰胆碱3.解毒类:复原性谷胱甘肽、硫普罗宁、葡醛酯4.抗炎药:复方甘草甜素、甘草酸二铵、异甘草酸镁5.降酶药:联苯双酯、双环醇6.利胆药:腺苷蛋氨酸、熊去氧胆酸第五章循环系统疾病用药第一节抗心力衰竭药1.强心苷类正性肌力药:地高辛、甲地高辛、毛花苷丙〔兰〕、去乙酰毛花苷〔兰D〕2.非强心苷类正性肌力药:1〕β受体冲动剂:多巴胺、多巴酚丁胺2〕磷酸二酯酶〔PDE〕III抑制剂:米力农、氨力农第二节抗心律失常药1.I类:1〕Ia类-Na+通道适度阻滞:奎尼丁、普鲁卡因胺2〕Ib类-Na+通道轻度阻滞:利多卡因、美西律、苯妥英钠3〕Ic类-Na+通道重度阻滞:普罗帕酮、氟卡尼2.II类:1〕β受体阻滞剂-非选择性β受体阻滞剂:普萘洛尔2〕β受体阻滞剂-选择性β受体阻滞剂:比索洛尔、美托洛尔、阿替洛尔3〕β受体阻滞剂-兼有α1受体阻滞剂:卡维地洛、拉贝洛尔3.III类-延长动作电位时程:胺碘酮、索他洛尔4.IV类-Ca2+通道阻滞:维拉帕米、地尔硫卓第三节抗心绞痛药1.硝酸酯类药:硝酸甘油、戊四醇酯、硝酸异山梨酯、5-单硝酸异山梨酯2.钙通道阻滞剂:1〕选择性钙通道阻滞:①二氢吡啶类:硝苯地平、尼莫地平、非洛地平、拉平、尼卡地平、左氨氯地平、氨氯地平②非二氢吡啶类:地尔硫卓、维拉帕米2〕非选择性钙通道阻滞:氟桂利嗪、桂利嗪第四节抗高血压药1.血管紧素转换酶抑制剂〔ACEI〕:卡托普利、依那普利、贝那普利、雷米普利、福辛普利2.血管紧素II受体阻断剂:缬沙坦、厄贝沙坦、替米沙坦、坎地沙坦3.肾素抑制剂:阿利克仑4.其他抗高血压药1〕交感神经抑制药:利血平〔交感神经末梢抑制剂〕、可乐定、甲基多巴〔作用于中枢神经系统〕2〕血管平滑肌扩剂:硝普钠、肼屈嗪3〕α1受体阻断剂:哌唑嗪第五节调节血脂药1.羟甲基戊二酰辅酶A复原酶抑制剂:辛伐他汀、氟伐他汀、阿托伐他汀、瑞舒伐他汀2.贝丁酸类药:非诺贝特、苯扎贝特3.烟酸类:1〕烟酸类:烟酸2〕盐酸衍生物:阿斯莫司第六章血液系统疾病用药第一节促凝血药1.促凝血因子合成药:维生素K12.促凝血因子活性药:酚磺乙胺3.抗纤维蛋白溶解药:氨甲环酸、氨基乙酸、氨甲苯酸4.作用于血管通透性药物:卡巴克络5.蛇毒血凝酶:蛇毒血凝酶6.鱼精蛋白:鱼精蛋白第二节抗凝血药1.微生素K拮抗剂:华法林、双香豆素、双香豆素乙酯、新抗凝、2.肝素和低分子肝素:依诺肝素、那屈肝素、替他肝素、达肝素3.直接凝血酶抑制剂:水蛭素、重组水蛭素、达比加群酯4.凝血因子X抑制剂:磺达肝葵纳、依达肝素、阿哌沙班、利伐沙班第三节溶栓药1.非特异性纤溶酶原激活剂:链激酶、尿激酶2.特异性纤溶酶原激活剂:阿替普酶、瑞替普酶第四节抗血小板药1.环氧酶抑制剂:阿司匹林2.二磷酸腺苷P2Y12受体阻断剂:喹氯匹啶、氯吡格雷、阿那格雷、普拉格雷、依诺格雷、替格雷洛、坎格雷洛3.整合素受体阻断剂〔血小板膜糖蛋白受体阻断剂〕:阿昔单抗、替罗非班、拉米非班、依替非巴肽4.磷酸二酯酶抑制剂:双嘧达莫、西洛他唑5.血小板腺苷环化酶刺激剂:肌苷、前列环素、伊洛前列素、西卡前列素6.血栓烷合成酶抑制剂:奥扎格雷钠第五节抗贫血药1.抗缺铁性贫血药物:硫酸亚铁、右旋糖酐铁、枸橼酸铁铵2.抗巨幼细胞性贫血药物:叶酸、维生素B123.促红细胞生成药物:重组人促红素第六节升白细胞药1.兴奋骨髓造血功能药:腺嘌呤、小檗胺2.粒细胞集落刺激因子和粒细胞-巨噬细胞集落刺激因子:非格司亭、沙格司亭第七章利尿剂与泌尿系统疾病用药第一节利尿剂1.袢利尿剂:呋塞米、布美他尼、依他尼酸、托拉塞米2.噻嗪类利尿剂:1〕噻嗪类利尿剂:氢氯噻嗪、氯噻嗪、苄噻嗪、氢氟噻嗪、环戊噻嗪2〕噻嗪样作用利尿剂:吲达帕胺、氯噻酮〔氯酞酮〕、美托拉宗3.留钾利尿剂:1〕醛固酮受体阻断剂:螺酯、依普利酮、坎利酮、坎利酸钾2〕肾小管上皮细胞Na+通道抑制剂:氨苯蝶啶、阿米洛利第二节抗前列腺增生症药1.α1受体阻断剂:1〕第一代非选择性:酚卡明2〕第二代选择性:哌唑嗪、特拉唑嗪、多沙唑嗪、阿夫唑嗪3〕第三代高选择性:坦洛新、西洛多辛第三节治疗男性勃起功能障碍药物1.第一亚类5型磷酸二酯酶抑制剂磷酸二酯酶-5型抑制剂:那非、伐地那非、他达拉非2.第二亚类雄激素雄激素:十一酸睾酮、丙酸睾酮第八章分泌系统疾病用药第一节肾上腺糖皮质激素1.长效:地塞米松、倍他米松2.中效:泼尼松、泼尼松龙、甲泼尼松、曲安西龙3.短效:氢化可的松、可的松第二节雌激素1.天然雌激素:雌二醇、雌三醇2.人工合成雌激素:戊酸雌二醇、炔雌醇、孕马雌酮、尼尔雌醇、炔雌醇、普罗雌烯第三节孕激素1.天然孕激素黄体酮及其合成衍生物:黄体酮、醋酸甲羟孕酮、地屈孕酮、屈螺酮2.合成的孕激素:1〕19-去甲基睾酮类:炔诺酮、去氧炔诺酮、左炔诺酮2〕17α-羟孕酮类:环丙孕酮19-去甲基孕酮类:炔诺孕酮、甲地孕酮、已酸羟孕酮第四节避孕药1.短效口服避孕药:复方炔诺酮片、复方甲地孕酮片、复方左炔诺孕酮片、去氧孕烯炔雌醇、复方孕二烯酮、复方环丙孕酮片、左炔诺孕酮炔雌醇片2.紧急避孕药:左炔诺孕酮、米非司酮3.长效避孕药:复方甲地孕酮注射液、复方庚酸炔诺酮注射液4.外用避孕药:壬苯醇醚栓5.皮下埋植避孕药:左炔诺孕酮的硅胶棒、甲硅环、庚炔诺酮微球针、复方甲地孕酮微囊第五节蛋白同化激素蛋白同化激素:苯丙酸诺龙、司坦挫醇第六节甲状腺激素及抗甲状腺药第一亚类甲状腺激素1.四碘甲状腺原氨酸:左甲状腺素2.三碘甲状腺原氨酸:碘塞罗宁3.动物甲状腺体加工药:甲状腺片第二亚类抗甲状腺药1.硫脲类:丙硫氧嘧啶、甲巯咪唑2.碘制剂:碘、碘化物、放射性碘3.β受体阻断剂:普萘洛尔第七节胰岛素及胰岛素类似物1.超短效胰岛素:门冬胰岛素、赖脯胰岛素2.短效胰岛素:速效胰岛素、普通胰岛素、可溶性胰岛素、中性胰岛素3.中效胰岛素:低精蛋白锌胰岛素4.长效胰岛素:精蛋白锌胰岛素5.超长效胰岛素:甘精胰岛素、地特胰岛素6.预混胰岛素:精蛋白锌重组人胰岛素混合注射液、精蛋白锌重组赖脯胰岛素混合注射液第八节口服降糖药1.磺酰脲类促胰岛素分泌药:格列本脲、格列美脲、格列齐特、格列吡嗪、格列喹酮2.非磺酰脲类促胰岛素分泌药:瑞格列奈、那格列奈、米格列奈3.双胍类药:苯乙双胍、二甲双胍4.α葡萄糖苷酶抑制剂:阿卡波糖、伏格列波糖、米格列醇5.胰岛素增敏剂〔噻唑烷二酮类〕:罗格列酮、吡格列酮6.胰高糖素样多肽-1受体冲动剂:艾塞那肽、利拉鲁肽7.二肽基肽酶-4抑制剂:西格列汀、维格列汀、沙格列汀、利格列汀第九节调节骨代与形成药1.钙剂和维生素D及其活性代物1〕钙剂:碳酸钙、葡萄糖酸钙2〕维生素D活性代物:骨化三醇、阿法骨化醇2.双膦酸盐类1〕第一代:依替膦酸二钠、氯屈膦酸二钠2〕帕米膦酸二钠3〕阿仑膦酸钠3.降钙素:降钙素、依降钙素4.雌激素受体调节剂:雷洛昔芬、依普黄酮第九章调节水、电解质、酸碱平衡药与营养药第一节调节水电解质平衡药1.钠盐:氯化钠2.钾盐:氯化钾、枸橼酸钾、门冬氨酸钾镁3.钙盐:氯化钙4.镁盐:硫酸镁、门冬氨酸钾镁第二节调节酸碱平衡药1.调节酸平衡药:碳酸氢钠、乳酸钠、氨丁三醇、复方乳酸钠山梨醇2.调节碱平衡药:氯化铵、氯化钠、盐酸精氨酸第三节葡萄糖与果糖:葡萄糖与二磷酸果糖钠第四节维生素1.水溶性维生素:维生素B1、维生素B2、维生素维生素B6、维生素C、烟酸、烟酸2.脂溶性维生素:维生素A、维生素D、维生素E、维生素K第五节氨基酸1.肝病用氨基酸:支链氨基酸、复方氨基酸〔3AA〕、复方氨基酸〔6AA〕2.肾病用氨基酸:复方氨基酸〔9AA〕、复方氨基酸〔18AA-N〕3.儿童用氨基酸:儿童复方氨基酸4.其他用氨基酸:复方氨基酸〔15AA〕、复方氨基酸〔20AA〕第十章抗菌药物第一节青霉素类抗菌药物1.天然青霉素:青霉素G2.半合成青霉素:1〕口服耐酸青霉素:青霉素V2〕耐青霉素酶青霉素:甲氧西林、苯唑西林、氧唑西林、双氯西林3〕广谱青霉素:羧苄西林、哌拉西林4〕抗革兰阴性杆菌青霉素:美西林、替莫西林第二节头孢菌素类抗菌药物1.第一代头孢菌素:注射剂:头孢唑林、头孢拉定口服制剂:头孢拉定、头孢氨苄、头孢羟氨苄2.第二代头孢菌素:注射剂:头孢呋辛、头孢替安口服制剂:头孢克洛、头孢呋辛酯、头孢丙烯3.第三代头孢菌素:注射剂:头孢他啶、头孢哌酮、头孢噻肟、头孢曲松口服制剂:头孢克肟、头孢泊污酯4.第四代头孢菌素:头孢吡肟5.第五代头孢菌素:头孢洛林酯、头孢托罗、头孢吡普第三节其他β-酰胺类抗菌药物1.头霉素类:头孢西丁、头孢美唑2.单酰胺类:氨曲南3.氧头孢烯类:拉氧头孢、氟氧头孢4.碳青霉烯类:亚胺培南、美罗培南、帕尼培南、厄他培南5.β-酰胺酶抑制剂:克拉维酸、舒巴坦、他唑巴坦第四节氨基糖苷类抗菌药物:链霉素、庆大霉素、阿米卡星、依替米星、大观霉素第五节大环酯类抗菌药物1.第一代:红霉素、琥乙红霉素2.第二代:罗红霉素、克拉霉素、阿奇霉素3.第三代:泰利霉素第六节四环素类抗菌药物:四环素、米诺环素、多西环素、金霉素、土霉素、美他环素第七节林可霉素类抗菌药物:林可霉素、克林霉素第八节多肽类抗菌药物:万古霉素、去甲万古霉素、替考拉宁、多粘菌素E、多粘菌素B、杆菌肽、短杆菌肽第九节酰胺醇类抗菌药物:氯霉素、甲砜霉素第十节氟喹诺酮类抗菌药物:左氧氟沙星、环丙沙星、莫西沙星、加替沙星、诺氟沙星、氧氟沙星、培氟沙星第十一节硝基呋喃类抗菌药物:呋喃唑酮、呋喃它酮、呋喃妥因、呋喃西林第十二节硝基咪唑类抗菌药物:甲硝唑、替硝唑、奥硝唑、塞克硝唑、地美硝唑、洛硝唑第十三节磺胺类抗菌药物及甲氧苄啶1.全身应用磺胺药:1〕短效类:磺胺异恶唑、磺胺二甲嘧啶2〕中效类:磺胺嘧啶、磺胺甲恶唑3〕长效类:磺胺多辛2.局部应用磺胺药:柳氮磺吡啶、磺胺米隆、磺胺嘧啶银、磺胺醋酰第十四节其他抗菌药物:磷霉素、利奈唑胺、夫酸、小檗碱第十五节抗结核分枝杆菌药1.一线抗结核药物:异烟肼、利福平、比嗪酰胺、乙胺丁醇、链霉素2.二线抗结核药物:对氨基水酸、氨硫脲、卷曲霉素、乙硫异烟胺第十六节抗真菌药1.多烯类:两性霉素B、制霉菌素2.唑类:酮康唑、伊曲康唑3.丙烯胺类:特比萘芬4.棘白菌素类:卡泊芬净、米卡芬净5.其他类:灰黄霉素、阿莫罗芬、利拉萘酯、环吡酮胺第十一章抗病毒药1.广谱抗病毒药:利巴韦林、干扰素2.抗流感病毒药:金刚烷胺、金刚乙胺、奥司他韦3.抗疱疹病毒药:阿昔洛韦、喷昔洛韦、更昔洛韦、泛昔洛韦、阿糖腺苷、膦甲酸钠4.抗肝炎病毒药:拉米夫定、阿德福韦、恩替卡韦第十二章抗寄生虫药第一节抗疟药1.控制病症的药物:青蒿素、氯喹、奎宁2.阻止复发和传播的药物:伯氨喹3.病因性预防的药物:乙胺嘧啶第二节抗肠蠕虫药1.哌嗪类驱虫药:哌嗪2.咪唑类驱虫药:阿苯达唑、左旋咪唑、甲苯达唑3.嘧啶类驱虫药:噻嘧啶第十三章抗肿瘤药第一节直接影响DNA构造和功能的药物1.破坏DNA的烷化剂:环磷酰胺、白消安、塞替派、司莫司汀2.破坏DNA的铂类化合物:顺铂、卡铂、奥沙利铂3.破坏DNA的抗生素类药物:丝裂霉素、博来霉素4.拓扑异构酶抑制剂:伊立替康、依托泊苷、羟喜树碱第二节干扰核算生物合成的药物〔抗代药〕1.二氢叶酸复原酶抑制剂:甲氨蝶呤、培美曲塞2.胸腺核苷合成酶抑制剂:氟尿嘧啶、卡培他滨3.嘌呤核苷合成酶抑制剂:巯嘌呤、硫鸟嘌呤4.核苷酸复原酶抑制剂:羟基脲5.DNA多聚酶抑制剂:阿糖胞苷、吉西他滨第三节干扰转录过程和阻滞RNA合成的药物〔作用于核算转录药物〕:多柔比星、柔红霉素第四节抑制蛋白质合成与功能的药物〔干扰有丝分裂药〕1.碱类:新碱、碱、地辛、瑞滨2.紫杉烷类:紫杉醇、多西他赛3.高三尖杉酯碱:高三尖杉酯碱4.门冬酰胺酶:门冬酰胺酶第五节调节体激素平衡的药物1.雌激素类:己烯雌酚2.抗雌激素类:他莫昔芬、托瑞米芬、来曲唑、阿那曲唑3.孕激素类:甲羟孕酮、甲地孕酮4.雄激素类:丙酸睾丸酮5.抗雄激素类:氟他胺第六节靶向抗肿瘤药1.络氨酸酶抑制剂:吉非替尼、厄洛替尼2.大分子单克隆抗体:曲妥珠单抗、利妥昔单抗、西妥昔单抗第七节放疗与化疗止吐药1.多巴胺受体阻断剂:甲氧氯普胺2.5-HT3受体阻断剂:昂丹司琼、格雷司琼、托烷司琼3.神经激肽-1〔NK-1〕受体阻断剂:阿瑞吡坦第十四章眼科疾病用药第一节抗眼部细菌感染药:氯霉素、红霉素、左氧氟沙星、诺氟沙星、环丙沙星、氧氟沙星、妥布霉素、庆大霉素、利福平、四环素可的松、多黏菌素B第二节降低眼压药1.拟M胆碱药:毛果芸香碱2.β受体阻断剂:卡替洛尔、美替洛尔、噻吗洛尔、倍他洛尔3.前列腺素类似物:拉坦前列素、曲伏前列素、比马前列素4.肾上腺素受体冲动剂:地匹福林、溴莫尼定第三节抗眼部病毒感染药:阿昔洛韦、更昔洛韦、利巴韦林、羟苄唑第四节眼用局部麻醉药:丁卡因、奥布卡因、丙美卡因、利多卡因第五节散瞳药1.M胆碱阻断剂类药物:硫酸阿托品、氢溴酸后马托品、复方托吡卡胺2.α肾上腺素受体冲动剂:去氧肾上腺素第五节调节体激素平衡的药物1.雌激素类:己烯雌酚2.抗雌激素类:他莫昔芬、托瑞米芬、来曲唑、阿那曲唑3.孕激素类:甲羟孕酮、甲地孕酮4.雄激素类:丙酸睾丸酮5.抗雄激素类:氟他胺第六节靶向抗肿瘤药1.络氨酸酶抑制剂:吉非替尼、厄洛替尼2.大分子单克隆抗体:曲妥珠单抗、利妥昔单抗、西妥昔单抗第七节放疗与化疗止吐药1.多巴胺受体阻断剂:甲氧氯普胺2.5-HT3受体阻断剂:昂丹司琼、格雷司琼、托烷司琼3.神经激肽-1〔NK-1〕受体阻断剂:阿瑞吡坦第十四章眼科疾病用药第一节抗眼部细菌感染药:氯霉素、红霉素、左氧氟沙星、诺氟沙星、环丙沙星、氧氟沙星、妥布霉素、庆大霉素、利福平、四环素可的松、多黏菌素B第二节降低眼压药1.拟M胆碱药:毛果芸香碱2.β受体阻断剂:卡替洛尔、美替洛尔、噻吗洛尔、倍他洛尔3.前列腺素类似物:拉坦前列素、曲伏前列素、比马前列素4.肾上腺素受体冲动剂:地匹福林、溴莫尼定第三节抗眼部病毒感染药:阿昔洛韦、更昔洛韦、利巴韦林、羟苄唑第四节眼用局部麻醉药:丁卡因、奥布卡因、丙美卡因、利多卡因第五节散瞳药1. M胆碱阻断剂类药物:硫酸阿托品、氢溴酸后马托品、复方托吡卡胺2.α肾上腺素受体冲动剂:去氧肾上腺素第十五章耳鼻喉科疾病用药第一节消毒防腐药:硼酸滴耳剂、酚甘油滴耳剂、3%过氧化氢溶液第二节减鼻充血药〔α受体冲动剂〕:盐酸麻黄碱滴鼻液、盐酸羟甲唑啉滴鼻液、盐酸赛洛唑啉滴鼻液第十六章皮肤科疾病用药第一节皮肤寄生虫感染治疗:5%-10%硫磺软膏、林丹霜、γ-六氯化苯乳膏、10%克罗米通乳膏第二节:痤疮治疗药1.非抗生素类抗菌药:过氧苯甲酰、壬二酸2.抗角化药:维A酸、阿达帕林、异维A酸第三节皮肤真菌感染治疗药1.抗生素类抗真菌药:1〕多烯类抗生素:两性霉素B、制霉菌素2〕非多烯类抗生素:灰黄霉素2.唑类抗真菌药1〕咪唑类:酮康唑、咪康唑、益康唑、克霉唑、联苯苄唑2〕三唑类:伊曲康唑、氟康唑、伏立康唑3.丙烯胺类抗真菌药:萘替芬、特比萘芬4.吗啉类抗真菌药:阿莫罗芬5.吡啶酮类抗真菌药:环吡酮胺第四节外用糖皮质激素1.弱效:醋酸氢化可的松2.中效:醋酸地塞米松、丁酸氢化可的松、醋酸曲安奈德3.强效:糠酸莫米松、二丙酸倍氯米松、氟轻松、哈西奈德〔0.025%〕4.超强效:卤米松、哈西奈德〔0.1%〕、丙酸氯倍他索。
药学专业知识:抗抑郁药考点

第三节抗抑郁药
抗抑郁药分类
1.典型不良反应
(1)三环类抗抑郁药和四环类抗抑郁药常见抗胆碱能效应(如口干、出汗、便秘、尿潴留、排尿困难、视物模糊、眼内压升高)。
(2)文拉法辛常见嗜睡、失眠、焦虑、性功能障碍等;严重不良反应有粒细胞缺乏、紫癜。
(3)度洛西汀嗜睡、眩晕、疲劳、性功能障碍。
(4)米氮平体重增加、困倦;严重则急性骨髓功能抑制。
2.用药监护
(1)用药宜个体化,从小剂量开始,逐增剂量。
(2)切忌频繁换药:抗抑郁药起效缓慢,大多数药物起效时间需要一定的时间,需要足够长的疗程,一般4~6周方显效(起效快的米氮平和文拉法辛,也需1周左右)。
(3)换用抗抑郁药时要谨慎。
氟西汀
适用证:用于抑郁症、强迫症以及神经性贪食症。
帕罗西汀
适应证:用于抑郁症、强迫症、惊恐障碍及社交恐惧症等。
舍曲林适应证
1.用于治疗抑郁症的相关症状,包括伴随焦虑、有或无躁狂史的抑郁症。
疗效满意后,继续服用可有效防止抑郁症的发生。
2.治疗强迫症。
治疗满意后,继续服用可有效防止强迫症初始症状的复发。
(氯丙咪嗪等)三环类抗抑郁药-2013-clinical pharmacology and therapeutics

CPIC GuIdelInesnature publishing groupPolymorphisms in CYP2D6 and CYP2C19 affect the efficacy and safety of tricyclics, with some drugs being affected by CYP2D6 only, and others by both polymorphic enzymes. Amitriptyline, c lomipramine, doxepin, imipramine, and trimipramine are demethylated by CYP2C19 to pharmacologically active metabolites. These drugs and their metabolites, along with desipramine and nortriptyline, undergo hydroxylation by CYP2D6 to less active metabolites. Evidence from published literature is presented for CYP2D6 and CYP2C19 genotype–direc ted dosing of tric yc lic antidepressants.The use of tricyclics to treat psychological disorders has declined in part because of the occurrence of undesirable side effects. Although tricyclics are still used to treat depression,1 their main therapeutic use is often for pain management.2,3 Interindividual differences in side effects and treatment response have been associated with variability of tricyclic plasma concentrations.4,5 Because both enzymes influence plasma concentrations, the effectiveness and tolerability of tricyclics are affected by CYP2D6 metabolism and partially by CYP2C19 metabolism.4 The purpose of this guideline is to provide information regarding how to use existing CYP2D6 and/or CYP2C19 genotyping test results to guide dosing of tricyclics for psychological disorders and pain manage-ment, focusing particularly on amitriptyline and nortriptyline.Optimal therapeutic plasma concentrations for the tricyclics have been defined.6 Poor or ultrarapid metabolizers of CYP2D6and CYP2C19 may have tricyclic plasma concentrations outside the recommended therapeutic range, thereby increasing the risk of treatment failure or side effects.7–10 Therefore, this guideline takes into consideration both clinical outcomes and observed tricyclic plasma concentrations based on genotype/phenotype characteristics. Detailed guidelines for use of other laboratory tests including therapeutic drug monitoring of tricyclics are beyond the scope of this article. The Clinical Pharmacogenetics Implementation Consortium (CPIC) of the National Institutes of Health’s Pharmacogenomics Research Network develops peer-reviewed gene–drug guidelines that are published and updated periodically at based on new developments in the field.FOCUSED LITERATURE REVIEWA systematic literature review focused on CYP2D6 and CYP2C19 genotyping and its relevance to gene-based dosing of tricyclics was conducted (see Supplementary Data online). This guideline was developed based on interpretation of the literature by the authors and experts in the field.GENES: CYP2D6 AND CYP2C19CYP2D6 backgroundThe CYP2D6 gene is highly polymorphic.11 More than 100 known allelic variants and subvariants have been identified, and there are substantial ethnic differences in observed allele frequencies (Supplementary Data online). The most commonly reportedReceived 1 October 2012; accepted 27 December 2012; advance online publication 13 March 2013. doi:10.1038/clpt.2013.2Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2D6 andCYP2C19 Genotypes and Dosing of Tricyclic AntidepressantsJK Hicks 1, JJ Swen 2, CF Thorn 3, K Sangkuhl 3, ED Kharasch 4, VL Ellingrod 5,6, TC Skaar 7, DJ Müller 8, A Gaedigk 9 and JC Stingl 101Department of Pharmaceutical Sciences, St. Jude Children’s Research Hospital, Memphis, Tennessee, USA; 2Department of Clinical Pharmacy and Toxicology, LeidenUniversity Medical Center, Leiden, The Netherlands; 3Department of Genetics, Stanford University, Stanford, California, USA; 4Division of Clinical and Translational Research, Department of Anesthesiology, Washington University in St. Louis, St. Louis, Missouri, USA; 5Department of Clinical, Social and Administrative Sciences,College of Pharmacy, Ann Arbor, Michigan, USA; 6Department of Psychiatry, School of Medicine, University of Michigan, Ann Arbor, Michigan, USA; 7Division of Clinical Pharmacology, Department of Medicine, Indiana University School of Medicine, Indianapolis, Indiana, USA; 8Neurogenetics Section, Centre for Addiction and Mental Health, and Department of Psychiatry, University of Toronto, Toronto, Ontario, Canada; 9Division of Pediatric Pharmacology and Medical Toxicology, Children’s Mercy Hospital & Clinics, Kansas City, Missouri, USA; 10Division of Research, Federal Institute for Drugs and Medical Devices, University Bonn Medical Faculty, Bonn, Germany. Correspondence: JC Stingl (cpic@ )CPIC GuIdelInesalleles are categorized into functional groups as follows: functional (e.g., CYP2D6*1 and *2), reduced function (e.g., CYP2D6*9, *10, and *41), and nonfunctional (e.g., CYP2D6*3–*6).11,12 Because CYP2D6 is subject to deletions or duplications, most clinical labo-ratories also report copy number. Deletions are indicated by the CYP2D6*5 allele, and gene duplications are denoted by an “xN” following the allele (e.g., CYP2D6*1xN, where xN represents the number of CYPD6 gene copies).CYP2C19 backgroundSimilar to CYP2D6, the CYP2C19 gene is highly polymorphic; more than 30 known allelic variants and subvariants have been identified.13 Although there are ethnic differences in allele fre-quencies (Supplementary Data online), the majority of patients carry a CYP2C19*1, *2, or *17 allele.13CYP2C19*1 is the wild-type allele encoding a fully functional enzyme, and CYP2C19*2 is the most common loss-of-function allele. Multiple CYP2C19 loss-of-function alleles have been identified (e.g., CYP2C19*3–*8), but their allele frequencies are <1%, with the exception of CYP2C19*3, which has a frequency of 2–15% in Asians.13The CYP2C19*17 allele results in enhanced gene transcription purportedly leading to increased metabolic activity.14 However, the clinical importance of the CYP2C19*17 allele is a matter of debate. Some studies indicate that CYP2C19*17 enhances clopidogrel response and increases the probability of therapeu-tic failure for proton pump inhibitors or antidepressants due to altered drug plasma concentrations, but there are conflicting clinical data.13–19Genetic test interpretationClinical laboratories usually test for the more frequently observed CYP2D6 and CYP2C19 genetic variants and translate the results into star-allele (*) nomenclature. Each star-allele, or haplotype, is defined by a specific combination of single-nucleotide polymor-phisms and/or other genetic variants within the gene locus of either CYP2D6 or CYP2C19.11,13 Genetic test results are reported as the summary of inherited maternal and paternal star-alleles referred to as a diplotype (e.g., CYP2D6*1/*2 and CYP2C19*1/*1). See Supplementary Data online for the more frequently observed alleles and their functional status.Scoring systems have been developed in an attempt to provide a uniform approach to quantitate the predicted functional status of CYP2D6 alleles as follows: 1 for functional, 0.5 for reduced function, and 0 for nonfunctional alleles (Supplementary Data online).11,12 The activity value for each allele of the diplotype is totaled to provide a CYP2D6 activity score. If CYP2D6 gene duplications are detected, the activity value of the duplicated allele is multiplied by the number of duplications present before calculating the activity score. The CYP2D6 activity score is used to assign phenotype in this guideline as follows: patients with an activity score of 0 are classified as poor metabolizers, those with a score of 0.5 are intermediate metabolizers, those with a score from 1.0 to 2.0 are extensive metabolizers, and those with a score >2.0 are classified as ultrarapid metabolizers (Table 1, Supplementary Data online). Extensive metabolizers are con-sidered to have normal CYP2D6 enzyme activity.There is a lack of consensus with regard to whether patients with a CYP2D6 activity score of 1.0 should be assigned an exten-sive or intermediate phenotype.11 Pharmacokinetic data suggest that patients with an activity score of 1.0 have a higher CYP2D6 metabolic capacity as compared with patients with an activity score of 0.5 but less CYP2D6 enzyme activity as compared with patients with an activity score of 2.0.12 Patients with one functional and one nonfunctional CYP2D6 allele do not haveTable 1 Assignment of likely phenotypes based on diplotypesLikely phenotype Activity score a Genotypes Examples of diplotypes Assignment of CyP2D6 phenotypeUltrarapid metabolizer (~1–2% of patients)b>2.0An individual carrying duplications of functionalalleles (*1/*1)xN, (*1/*2)xN, (*2/*2)xN cExtensive metabolizer (~77–92% of patients) 1.0–2.0d An individual carrying two functional alleles ortwo reduced function alleles or one functional andnonfunctional allele or one functional and reducedfunction allele *1/*1, *1/*2, *2/*2, *1/*9, *1/*41, *41/*41, *1/*5,*1/*4Intermediate metabolizer (~2–11% of patients)0.5An individual carrying one reduced function andone nonfunctional allele*4/*41, *5/*9, *4/*10 Poor metabolizers (~5–10% of patients)0An individual carrying only nonfunctional alleles*4/*4, *3/*4, *5/*5, *5/*6 Assignment of CyP2C19 phenotypeUltrarapid metabolizer (~5–30% of patients)e An individual carrying two gain-of-function allelesor one functional allele and one gain-of-functionallele*17/*17, *1/*17Extensive metabolizer (~35–50% of patients)An individual carrying two functional alleles*1/*1 Intermediate metabolizer (~18–45% of patients)An individual carrying one functional allele and oneloss-of-function allele*1/*2, *1/*3Poor metabolizers (~2–15% of patients)An individual carrying two loss-of-function alleles*2/*2, *2/*3, *3/*3a See Supplementary Data for additional information about CyP2D6 activity score and its limitations.b CyP2D6 metabolizer status frequencies are based on data from Caucasians and may differ from other ethnicities.c xN represents the number of CYP2D6 gene copies.d Patients with an activity score of 1.0 may be classified as intermediate metabolizers by some reference laboratories. e CyP2C19 metabolizer status frequencies are based on average multiethnic frequency.CPIC GuIdelInessignificantly different nortriptyline plasma concentrations as compared with patients with two functional CYP2D6 alleles,20 although another study reported conflicting data.7 Herein, we classified patients with a CYP2D6 activity score of 1.0 as exten-sive metabolizers, which is analogous to the CPIC guideline for codeine.11The predicted CYP2C19 phenotype based on the diplotype (Table 1 and Supplementary Data online) is consistent with the CPIC guideline for clopidogrel.13 Patients with two func-tional alleles are categorized as extensive metabolizers, which is considered normal CYP2C19 enzyme activity. Individuals carrying one or two loss-of-function alleles are considered intermediate and poor metabolizers, respectively. Patients with two gain-of-function alleles are classified as ultrarapid metabolizers. The predicted phenotype for a patient carrying the CYP2C19*17 gain-of-function allele in combination with a loss-of-function allele is a matter of debate. Limited data sug-gest that CYP2C19*17 may not compensate for the CYP2C19*2 allele.15,21Reference laboratories use varying methods to assign pheno-types. Before pharmacotherapy modifications are made based on this guideline, it is advisable to determine a patient’s pheno-type as described above.Available genetic test optionsCYP2D6 and CYP2C19 genotyping is available from several ref-erence laboratories (see Supplementary Data online and http:// ).Incidental findingsIndependent of drug metabolism and response, there are cur-rently no diseases or conditions that have been convincingly linked to variants in the CYP2D6 or CYP2C19 genes.11,13 Reports describing an association between CYP2D6 ultrarapid metabolizers and suicidality, and CYP2C19 polymorphisms and depressive symptoms are available.22–24 These associations are poorly understood and may be explained by alterations in either drug or endogenous substrate metabolism.DRUGS: AMITRIPTYLINE AND NORTRIPTYLINE BackgroundTricyclics are mixed serotonin and norepinephrine reuptake inhibitors used to treat several disease states including depres-sion, obsessive–compulsive disorder, and neuropathic pain in addition to migraine prophylaxis. The tricyclics have simi-lar but distinct chemical structures referred to as tertiary and secondary amines. The pharmacological properties of the ter-tiary and secondary amines differ, with tertiary amines having a more pronounced serotonergic effect and secondary amines having a greater noradrenergic effect (Supplementary Data online).25,26 The tertiary amines (e.g., amitriptyline) are mainly metabolized by CYP2C19 to desmethyl metabolites (Figure 1), also referred to as secondary amines (e.g., nortriptyline). It should be noted that the desmethyl metabolites, nortriptyline as well as desipramine, are antidepressant drugs themselves with distinct clinical features that differ from the parent drugs amitriptyline and imipramine. Both the tertiary and second-ary amines are metabolized by CYP2D6 to less active hydroxy metabolites (Figure 1, Supplementary Data online). CYP2C19 impacts the ratio of tertiary to secondary amine plasma concen-trations but may have less influence on overall drug clearance than CYP2D6.27 However, CYP2C19 metabolism may modu-late antidepressant activity and side effects through the phar-macological actions of the tertiary amines. Serotonin reuptake inhibition is expected be more pronounced in CYP2C19 poor metabolizers due to the decreased conversion of tertiary to sec-ondary amines.26Patients may be predisposed to treatment failure or adverse effects due to polymorphisms in CYP2D6 and CYP2C19 alter-ing drug clearance or the ratio of parent drug to metabolites, respectively. Tricyclics are associated with multiple adverse effects, which can cause patients to fail therapy. Common adverse effects include anticholinergic, central nervous system, and cardiac effects. Tertiary and secondary amines along with their metabolites have unique side-effect profiles as detailed in Supplementary Data online.Both amitriptyline and nortriptyline are used as model drugs for this guideline because the majority of pharmacogenomic studies have focused on these two drugs. However, the results of these studies may apply to other tricyclics because these drugs have comparable pharmacokinetic properties.4,8 Tricyclics are well absorbed from the gastrointestinal tract, and the average extent of first-pass metabolism is ~50%, although the average first-pass metabolism of doxepin may be closer to 70%.4 The clearance of tricyclics is mostly a linear process, but satura-tion of the hydroxylation pathway may occur at higher plasma concentrations for certain tricyclics, including imipramine and desipramine.4,28 In addition, extrapolated dose adjustments based on metabolizer status are similar across the tricyclic class.8 Because some studies investigating the influence of CYP2D6 and/or CYP2C19 genotype/phenotype on the pharmacokinetics of tricyclics used a single dose, it should be noted that tricyclic metabolism is thought to be similar after single and multiple dosing.5Linking genetic variability to variability in drug-relatedp henotypesPsychiatric disorders such as depression have a 30–50% failure rate with initial treatment, which may, in part, be attributed to adverse effects or altered plasma concentrations.9,29 There is substantial evidence linking CYP2D6 and CYP2C19 genotypes to phenotypic variability in tricyclic side-effect and pharma-cokinetic profiles. Modifying pharmacotherapy for patientsFigure 1 Major metabolic pathway of amitriptyline and nortriptyline.demethylationNortriptylineAmitriptylineCYP2C19CPIC GuIdelIneswho have CYP2D6 or CYP2C19 genomic variants that affect drug efficacy and safety could potentially improve clinical outcomes and reduce the failure rate of initial treatment. The application of a grading system to the evidence linking CYP2D6 and CYP2C19 genotypic variations to phenotypic variability in response to amitriptyline or nortriptyline indicates a high qual-ity of evidence in the majority of cases (Supplementary Data online). This body of evidence, rather than randomized clinical trials, provides the basis for amitriptyline and nortriptyline dos-ing recommendations in Tables 2 and 3. Because the tricyclics have comparable pharmacokinetic properties, it may be reason-able to apply this guideline to other tricyclics, including clomi-pramine, desipramine, doxepin, imipramine, and trimipramine (Supplementary Data online), with the acknowledgment that there are fewer data supporting dose adjustments for these drugs than for amitriptyline or nortriptyline.Table 2 Dosing recommendations for amitriptyline and nortriptyline based on CYP2D6 phenotypephenotype implication Therapeutic recommendation Classification of recommendation aCyP2D6 ultrarapid metabolizer Increased metabolism of tricyclics to lessactive compounds as compared with extensivemetabolizersAvoid tricyclic use due to potential lack of efficacy.Consider alternative drug not metabolized byCyP2D6StrongLower plasma concentrations will increaseprobability of pharmacotherapy failureIf a tricyclic is warranted, consider increasing thestarting dose.b Use therapeutic drug monitoring toguide dose adjustmentsCyP2D6 extensivemetabolizerNormal metabolism of tricyclics Initiate therapy with recommended starting dose b StrongCyP2D6 intermediate metabolizer Reduced metabolism of tricyclics to less activecompounds as compared with extensive metabolizersConsider 25% reduction of recommended startingdose.b Use therapeutic drug monitoring to guidedose adjustmentsModerateHigher plasma concentrations will increase theprobability of side effectsCyP2D6 poor metabolizer Greatly reduced metabolism of tricyclics to less activecompounds as compared with extensive metabolizersAvoid tricyclic use due to potential for side effects.Consider alternative drug not metabolized byCyP2D6StrongHigher plasma concentrations will increase theprobability of side effectsIf a tricyclic is warranted, consider a 50% reductionof recommended starting dose.b Use therapeuticdrug monitoring to guide dose adjustmentsIf CYP2C19 genotyping results are also available, see Table 3 for CYP2C19-based dosing recommendations along with Supplementary Data online. Dosing recommendations apply only to higher initial doses of amitriptyline or nortriptyline for treatment of conditions such as depression. See “Other Considerations” for dosing recommendations for conditions in which lower initial doses are used, such as neuropathic pain. For the dosing guidelines for clomipramine, desipramine, doxepin, imipramine, and trimipramine, see Supplementary Data online.a The rating scheme for the recommendation classification is described in the Supplementary Data online.b Patients may receive an initial low dose of tricyclics, which is then increased over several days to the recommended steady-state dose. The starting dose in this guideline refers to the recommended steady-state dose.Table 3 Dosing recommendations of amitriptyline based on CYP2C19 phenotypephenotype implication Therapeutic recommendation Classification of recommendation aCyP2C19 ultrarapid metabolizer Increased metabolism of amitriptyline as comparedwith extensive metabolizersConsider alternative drug not metabolized byCyP2C19OptionalIf a tricyclic is warranted, use therapeutic drugmonitoring to guide dose adjustmentsCyP2C19 extensive metabolizer Normal metabolism of amitriptyline Initiate therapy with recommended startingdose bStrongCyP2C19 intermediate metabolizer Reduced metabolism of amitriptyline as comparedwith extensive metabolizersInitiate therapy with recommended startingdose bStrongCyP2C19 poor metabolizer Greatly reduced metabolism of amitriptyline ascompared with extensive metabolizersConsider a 50% reduction of recommendedstarting dose.b Use therapeutic drug monitoringto guide dose adjustmentsModerateHigher plasma concentrations of amitriptyline willincrease the probability of side effectsIf CYP2D6 genotyping results are also available, see Table 2 for CYP2D6-based dosing recommendations along with Supplementary Data online. Dosing recommendations apply only to higher initial doses of amitriptyline for treatment of conditions such as depression. See “Other Considerations” for dosing recommendations for conditions at which lower initial doses are used, such as neuropathic pain. For dosing guidelines for clomipramine, doxepin, imipramine, and trimipramine, see Supplementary Data online.a The rating scheme for the recommendation classification is described in the Supplementary Data online.b Patients may receive an initial low dose of tricyclics, which is then increased over several days to the recommended steady-state dose. The starting dose in this guideline refers to the recommended steady-state dose.CPIC GuIdelInesTherapeutic recommendationsCYP2D6 dosing recommendations. For neuropathic pain treat-ment, in which lower initial doses of tricyclics are used, gene-based dosing recommendations are found in the “Other Considerations” section. Table 2 summarizes the gene-based dosing recommendations for amitriptyline and nortriptyline based on CYP2D6 phenotype for situations requiring a higher initial dose, such as depression treatment. The recommended starting dose of amitriptyline or nortriptyline does not need adjustment based on genotype for CYP2D6 extensive metabo-lizers. A 25% reduction of the recommended dose may be considered for CYP2D6 intermediate metabolizers.30 Because patients with a CYP2D6 activity score of 1.0 are inconsistently categorized as intermediate or extensive metabolizers in the literature, these are difficult to evaluate, resulting in a moder-ate recommendation classification.CYP2D6 ultrarapid metabolizers have a higher probability of failing amitriptyline or nortriptyline pharmacotherapy due to subtherapeutic plasma concentrations, and therefore alternative agents are preferred. There are documented cases of CYP2D6 ultrarapid metabolizers receiving large doses of nortriptyline to achieve therapeutic concentrations.10 However, very high plasma concentrations of the nortriptyline hydroxy metabolite were present, which may increase the risk for cardiotoxicity. If a tricyclic is warranted, there are insufficient data in the literature to calculate a starting dose for a patient with CYP2D6 ultrarapid metabolizer status, and therapeutic drug monitoring is strongly recommended. Adverse effects are more likely in CYP2D6 poor metabolizers due to elevated tricyclic plasma concentrations,31 therefore, alternative agents are preferred. If a tricyclic is war-ranted, consider a 50% reduction of the usual dose; therapeutic drug monitoring is strongly recommended.CYP2C19 dosing recommendations. Dosing recommendations for neuropathic pain treatment with amitriptyline are discussed in the “Other Considerations” section. Table 3 summarizes the gene-based dosing recommendations for CYP2C19 and ami-triptyline when higher initial starting doses are warranted. The usual starting dose of amitriptyline may be used in CYP2C19 extensive and intermediate metabolizers. Although CYP2C19 intermediate metabolizers would be expected to have a modest increase in the ratio of amitriptyline to nortriptyline plasma concentrations, the evidence does not indicate that CYP2C19 intermediate metabolizers should receive an alternative dose. Patients taking amitriptyline who are CYP2C19 ultrarapid metabolizers may be at risk of having altered plasma concen-trations or adverse events. Although the CYP2C19*17 allele did not alter the sum of amitriptyline plus nortriptyline plasma con-centrations, it was associated with higher nortriptyline plasma concentrations, possibly increasing the risk of adverse events.15 For patients taking amitriptyline, extrapolated pharmacokinetic data suggest that CYP2C19 ultrarapid metabolizers may need a dose increase.8 Due to the need for further studies investi-gating the clinical importance of the CYP2C19*17 allele and the possibility of altered tricyclic concentrations, we recom-mend consideration of an alternative tricyclic or other drug not affected by CYP2C19. Because the clinical importance of CYP2C19*17 is currently poorly understood, this recommenda-tion is classified as optional. If amitriptyline is administered to a CYP2C19 ultrarapid metabolizer, therapeutic drug monitoring is recommended.CYP2C19 poor metabolizers are expected to have a greater ratio of amitriptyline to nortriptyline plasma concentrations.32 The elevated amitriptyline plasma concentrations may increase the chance of a patient experiencing side effects. Consider a 50% reduction of the usual amitriptyline starting dose along with therapeutic drug monitoring.8CYP2D6 and CYP2C19 combined dosing recommendations. Although specific combinations of CYP2D6 and CYP2C19 alleles are likely to result in additive effects on the pharmacokinetic properties of tricyclics, little information is available on how to adjust initial doses based on combined genotype information. Patients carrying at least one CYP2D6 nonfunctional allele and two CYP2C19 functional alleles had an increased risk of expe-riencing side effects when administered amitriptyline, whereas patients with at least one CYP2C19 loss-of-function allele and two CYP2D6 functional alleles had a low risk of experienc-ing side effects.10,33 Because there is only sparse clinical evi-dence for an additive effect of CYP2D6 and CYP2C19 on tri-cyclic dosing, the recommendations are classified as optional (Supplementary Data online).Other considerationsGene-based dosing recommendations for neuropathic pain treatment. Amitriptyline is often used at lower dosages (e.g., 0.1 mg/kg/ day in pediatric patients) for treatment of neuropathic pain than when used for depressive disorders.2,3 Because of the lower dosage, it is less likely that CYP2D6 or CYP2C19 poor or intermediate metabolizers will experience adverse effects due to supratherapeutic plasma concentrations of amitriptyline.34 Therefore, we recommend no dose modifications for poor or intermediate metabolizers when prescribed amitriptyline at a lower dose for treatment of neuropathic pain, but these patients should be monitored closely for side effects. If larger doses of amitriptyline are warranted, we recommend following the gene-based dosing guidelines presented in Tables 2 and 3. Providing dose recommendations for CYP2C19 ultrarapid metabolizers when amitriptyline is prescribed at lower doses for neuropathic pain treatment is difficult. On the basis of predicted and observed pharmacokinetic data, CYP2D6 ultrarapid metab-olizers are at risk of failing amitriptyline therapy for neuropathic pain, and thus alternative agents such as gabapentin should be considered.35 Although little information is available on how to adjust initial amitriptyline doses based on combined CYP2D6 and CYP2C19 genetic results when treating neuropathic pain, caution should be used when patients have a combination of poor or ultrarapid phenotypes (e.g., a CYP2D6 poor metabolizer also having CYP2C19 ultrarapid or poor metabolism).Consideration of drug interactions and patient characteristics. Patients treated for psychiatric disorders often require m ultipleCPIC GuIdelInesm edications, which can influence tricyclic plasma concen-trations, side effects, and therapeutic failure.4 For example, patients taking amitriptyline in combination with a potent CYP2D6 inhibitor, such as fluoxetine, may have dramatic increases in plasma concentrations.36 It has been suggested that patients taking strong CYP2D6 inhibitors should be treated similarly to CYP2D6 poor metabolizers.11 In addition, patients with increased age, liver disease, and reduced renal function may require reduced doses of tricyclics.4,37,38 Drug–drug interactions along with patient characteristics should be considered in addition to the gene-based dosing recommenda-tions presented herein.Minor metabolic pathw ays of tricyclics. Other cytochrome P450 enzymes, including CYP3A4 and CYP1A2, metabolize tri-cyclics to a lesser extent.4,34,39,40 There is currently no strong evidence supporting gene-based dosing recommendations for other cytochrome P450 enzymes that metabolize tricyclics.Potential benefits and risks for the patientFor patients who have existing CYP2D6 and/or CYP2C19 gen-otyping test results, the potential benefit is identifying those patients who are at an elevated risk of experiencing side effects or therapeutic failure. For those patients, dose adjustments can be made or an alternative agent selected. A limitation inherent to most commercially available genotyping tests is that rare or de novo variants are not detected. In addition, some alleles are not well characterized, resulting in uncertainty when predict-ing the phenotype for some genetic test results. Genotyping is reliable when performed in qualified reference laboratories, but, as with any laboratory test, an error can occur. Any errors in genotyping or phenotype prediction, along with the presence of a rare genomic variant not tested for, could potentially affect the patient lifelong.Caveats: appropriate use and/or potential misuse ofg enetic testsThe application of genotype-based dosing is most appropriate when initiating therapy with a tricyclic. Obtaining a pharma-cogenetic test after months of drug therapy may be less helpful in some instances, given that the drug dose may have already been adjusted based on plasma concentrations, response, or side effects. Similar to all diagnostic tests, genetic tests are one of several pieces of clinical information that should be considered before initiating drug therapy.SUPPLEMENTARY MATERIAL is linked to the online version of the paper at /cptDISCLAIMERCPIC guidelines reflect expert consensus based on clinical evidenceand peer-reviewed literature available at the time they are written; theyare intended only to assist clinicians in decision making and to identify questions for further research. New evidence may have emerged since the time a guideline was submitted for publication. Guidelines are limited in scope and are not applicable to interventions or diseases not specifically identified. Guidelines do not account for all individual variations among patients and cannot be considered inclusive of all proper methods of care or exclusive of other treatments. It remains the responsibility of the health-care provider to determine the best course of treatment for a patient. Adherence to any guideline is voluntary, with the ultimate determination regarding its application to be made solely by the clinician and the patient. CPIC assumes no responsibility for any injury to persons or damage to persons or property arising out of or related to any use of CPIC’s guidelines, or for any errors or omissions.ACKNOWLEDGMENTSWe acknowledge the critical input of M. Relling, T. Klein, K. Crews, and members of the Clinical Pharmacogenetics Implementation Consortiumof the Pharmacogenomics Research Network and funding by the National Institutes of Health (NIH). J.K.H. is supported by NIH/National Instituteof General Medical Sciences (NIGMS) Pharmacogenomics Research Network (U01 GM92666 and U01 HL105198) and by ALSAC. C.F.T. and K.S. are supported by NIH/NIGMS (R24 GM61374). E.D.K. is supported by R01 GM63674 and R01 DA14211. T.C.S. is supported by R01 GM088076 andthe Agency for Healthcare Research and Quality (R01 HS19818-01). V.L.E.is supported by the NIMH (R01 MH082784). D.J.M. is supported by a New Investigator Salary Award from the Canadian Institutes of Health Research, a New Investigator Fellowship Award from the Ontario Mental Health Foundation, and an Early Researcher Award by the Ministry of Research and Innovation of Ontario. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality.AUTHOR CONTRIBUTIONSAll the authors contributed to the development of the gene-based dosing guidelines and writing of the manuscript and supplementary material. CONFLICT OF INTERESTThe authors declared no conflict of interest.© 2013 American Society for Clinical Pharmacology and Therapeutics1. American Psychiatric Association, A.P. Practice Guideline for the Treatmentof Patients With Major Depressive Disorder 3rd edn. (American PsychiatricPublishing, Arlington, VA, 2010).2. Watson, C.P. The treatment of neuropathic pain: antidepressants and opioids.Clin. J. Pain16, S49–S55 (2000).3. Laird, B., Colvin, L. & Fallon, M. Management of cancer pain: basic principlesand neuropathic cancer pain. Eur. J. Cancer44, 1078–1082 (2008).4. Rudorfer, M.V. & Potter, W.Z. Metabolism of tricyclic antidepressants. Cell. Mol.Neurobiol.19, 373–409 (1999).5. Potter, W.Z., Zavadil, A.P. 3rd, Kopin, I.J. & Goodwin, F.K. Single-dose kineticspredict steady-state concentrations on imipramine and desipramine. Arch.Gen. Psychiatry37, 314–320 (1980).6. Hiemke, C. et al. AGNP consensus guidelines for therapeutic drug monitoringin psychiatry: update 2011. Pharmacopsychiatry44, 195–235 (2011).7. Dalén, P., Dahl, M.L., Bernal Ruiz, M.L., Nordin, J. & Bertilsson, L.10-Hydroxylation of nortriptyline in white persons with 0, 1, 2, 3, and 13functional CyP2D6 genes. Clin. Pharmacol. Ther.63, 444–452 (1998).8. Stingl, J.C., Brockmöller, J. & Viviani, R. Genetic variability of drug-metabolizingenzymes: the dual impact on psychiatric therapy and regulation of brainfunction. Mol. Psychiatry (2012); e-pub ahead of print 8 May 2012.9. Kirchheiner, J. & Seeringer, A. Clinical implications of pharmacogenetics ofcytochrome P450 drug metabolizing enzymes. Biochim. Biophys. Acta1770, 489–494 (2007).10. Bertilsson, L., Aberg-Wistedt, A., Gustafsson, L.L. & Nordin, C. Extremely rapidhydroxylation of debrisoquine: a case report with implication for treatment with nortriptyline and other tricyclic antidepressants. Ther. Drug Monit.7,478–480 (1985).11. Crews, K.R. et al. Clinical Pharmacogenetics Implementation Consortium(CPIC) guidelines for codeine therapy in the context of cytochrome P450 2D6 (CyP2D6) genotype. Clin. Pharmacol. Ther.91, 321–326 (2012).12. Gaedigk, A., Simon, S.D., Pearce, R.E., Bradford, L.D., Kennedy, M.J. & Leeder, J.S.The CyP2D6 activity score: translating genotype information into a qualitative measure of phenotype. Clin. Pharmacol. Ther.83, 234–242 (2008).13. Scott, S.A. et al. Clinical Pharmacogenetics Implementation Consortiumguidelines for cytochrome P450-2C19 (CyP2C19) genotype and clopidogrel therapy. Clin. Pharmacol. Ther.90, 328–332 (2011).。
三环类抗抑郁药(专业知识值得参考借鉴)

三环类抗抑郁药(专业知识值得参考借鉴)一概述三环类抗抑郁药(TcAs)是临床上治疗抑郁症最常用的药物之一,其核心结构是中间一个七元杂环两边连接一个苯环构成。
其中,丙米嗪是最早发现的具有抗抑郁作用的化合物,目前常用药物还有氯米帕明、阿米替林、多赛平等。
TCAs主要在肝脏代谢,参与的代谢酶有CYP1A2、CYP2D6、CYP3A4等。
主要代谢为三环核氧化,如2位或10位碳原子羟化(CYP2D6催化)、脂肪侧链氧化、氮原子的去甲基化(CYP3A4催化)。
由于CYP的活性受多种因素的影响,血浆中活性代谢产物的浓度与原药浓度的比率有明显的个体差异。
二药理作用TCAs阻断了去甲肾上腺素(NA)能和5羟色胺(5-HT)能神经末梢对NA和5-HT的再摄取,增加了突触间隙单胺类递质的浓度,临床上表现为抑郁症状的改善。
目前研究发现,抗抑郁药对递质再摄取的抑制作用是立即发生的,而长期用药后则可以降低受体的敏感性(下调作用),这与抗抑郁药的临床效应滞后(用药2~3周后起效)密切相关。
NA再摄取的阻断使神经突触间隙内源性NA浓度增加,进而可以降低突触前膜α2受体的敏感性,长期使用还可能减少中枢α2受体的数目。
5-HT再摄取的抑制首先也是增加胞体部位突触间隙内源性5-HT浓度,通过下调突触前胞体膜的5-HT1A受体,增加末梢释放5-HT,最终达到抗抑郁作用。
TCAs还有很强的阻断5-HT2A 受体作用。
三适用范围适用于治疗各类以抑郁症状为主的精神障碍,如内因性抑郁、恶劣心境障碍、反应性抑郁及器质性抑郁等。
还可用于治疗广泛性焦虑症、惊恐发作和恐怖症。
小剂量丙米嗪可米嗪可用于治疗儿童遗尿症,氯米帕明则常用于治疗强迫症。
对精神分裂症患者伴有的抑郁症状,治疗宜谨慎,TCAs可能使精神病性症状加重或明显化。
三环类抗抑郁药曾经是首选的抗抑郁药,但是由于该类药物抗胆碱能和心血管不良反应较大,禁忌证和药物相互作用较多,安全范围较窄,使其临床应用受限。
执业西药师-药学专业知识二-目录
第一章精神与中枢神经系统疾病用药(八大类)一.镇静与催眠药:1.苯二氮䓬类(阿普唑仑、艾司唑仑、咪达唑仑、三唑仑、地西泮、氣硝西泮、硝西泮、劳拉西津、奥沙西泮、氟西泮)2.巴比妥类(苯巴比妥、异戊巴比妥、巴比妥、司可巴比妥)3.环吡咯酮类及非苯二氮䓬类(佐匹克隆、右佐匹克隆、唑吡坦、扎来普隆)4.醛类(水合氯醛)5.褪黑素受体激动剂(雷美替胺)二.抗癫痫药:1.二苯并氮䓬类(卡马西平、奥卡西平) 4. 苯二氮䓬类(氯硝西泮)2. 乙内酰脲类(苯妥英钠) 5. 脂肪酸衍生物(丙戊酸)3. 巴比妥类(苯巴比妥、扑米酮) 6. 其他抗癫痛药(加巴喷丁、拉莫三嗪、托吡酯、左乙拉西坦、唑尼沙胺)三.抗抑郁药:1. 选择性5-羟色胺再摄取抑制剂(氟西汀、帕罗西汀、艾司西酞普兰、氟伏沙明、舍曲林、西酞普兰)2. 5-羟色胺与去甲肾上腺素再摄取抑制剂(度洛西汀、文拉法辛、阿戈美拉汀、米安色林、噻奈普汀)3. 去甲肾上腺素能及特异性5-HT能抗抑郁药(米氮平)4. 三环类抗抑郁药(阿米替林、丙米嗪、氯米帕明、多塞平)5. 四环类抗抑郁药(马普替林)6. 单胺氧化酶抑制剂(吗氯贝胺)7. 5- HT受体阻断剂1再摄取抑制剂(曲唑酮)8. 选择性去甲肾上腺素再摄取抑制剂(瑞波西汀)四.脑功能改善及抗记忆障碍药:1.酰胺类中枢兴奋药(吡拉西坦、茴拉西坦、奥拉西坦)2.乙酰胆碱酯酶抑制剂(石杉碱甲、多奈哌齐、卡巴拉汀、加兰他敏)3.其他(胞磷胆碱钠、艾地苯醌、银杏叶提取物)五.治疗缺血性脑血管疾病药:1. 溶栓药(降纤酶、巴曲醉、尿激酶、重组链激酶、阿替普酶)2. 抗血小板药(奥扎格雷、阿司匹林、氯吡格雷)3. 自由基清除剂(依达拉奉)4. 钙通道阻滯剂(尼莫地平、桂利嗪、氟桂利嗪、环扁桃酯)15. 直接作用于血管平滑肌的血管扩张剂(尼麦角林、罂粟碱)6. 改善微循环、降低血黏度药(己酮可可碱、烟酸占替诸诺、维生素E烟酸酯)7. 脑代谢改善药(胞磷胆碱、神经节苷脂)8. 其他(倍他司汀、丁苯酞、曲克芦丁、灯盏花素、长春胺、长春西汀、川芎嗪)六.镇痛药:A.麻醉性镇痛药 1.阿片生物碱(吗啡、可待因)2. 半合成吗啡样镇痛药(双氢可待因、丁丙诺啡、氢吗啡酮和羟吗啡酮)3. 合成阿片类镇痛药(a.苯哌啶类: 芬太尼、舒芬太尼、阿芬太尼等 b.二苯甲烷: 美沙酮、右丙氧芬c.吗啡烷类: 左啡诺、布托啡诺d.苯并吗啡烷类: 喷他佐辛、非那佐辛)B.非麻醉性镇痛药(非阿片类) (曲马多非甾体抗炎药)七.抗帕金森病药:A.拟多巴胺药1.拟多巴胺药多巴胺前体(左旋多巴)2. 外周脱羧酶抑制剂(卡比多巴、苄丝肼等)3.儿茶酚胺氧位甲基转移酶抑制剂(恩他卡朋)4.中枢多巴胺受体激动剂(溴隐亭、培高利特、普拉克索)B.抗胆碱类(苯海索)C.单胺氧化酶-B抑制剂(司来吉兰、雷沙吉兰)D.其他(金刚烷胺、美金刚)八. 抗精神病药A. 第一代抗精神病药 1.吩噻嗪类(氯丙嗪、硫利达嗪、奋乃静、氟奋乃静、三氟拉嗪)2.硫杂蒽类(三氟噻吨、氯氯哌噻吨、氯普噻吨)3.丁酰苯类(氟哌啶醇、五氟利多)4.苯甲酰胺类(舒必利)B.第二代抗精神病药物(氯氮平、利培酮、奥氮平、喹硫平、齐拉西酮、阿立哌唑)2第二章解热、镇痛、抗炎、抗风湿药及抗痛风药一.解热、镇痛、抗炎药(非甾体抗炎药)A.非选择性COX抑制剂1. 水杨酸类(阿司匹林、贝诺酯、赖氨匹林)2.乙酰苯胺类(对乙酰氨基酚)3.芳基乙酸类(吲哚美辛、双氯芬酸)4.芳基丙酸类(布洛芬、蔡普生)5. 1. 2-苯并噻嗪类(吡罗昔康)6.吡唑酮类(保泰松)7.非酸性类(萘丁美酮)B.COX -2抑制剂(塞来昔布、依托考昔、尼美舒利、美洛昔康)二.抗风湿药1.非甾体抗炎药(布洛芬、双氯芬酸、萘普生)2.糖皮质激素(泼尼松、泼尼松龙、地塞米松等)3.慢作用抗风湿药(甲氨蝶呤、柳氮磺吡啶、来氟米特、羟氯喹和氯喹、金制剂、双醋瑞因、青霉胺、雷公藤总苷、硫唑嘌呤、环孢素)4. 生物制剂 a.融合蛋白类(依那西普) b.单克隆抗体(阿达木单抗、英夫利昔单抗)三. 抗痛风药1.抑制粒细胞浸润炎症反应药(秋水仙碱)2.促进尿酸排泄药(苯溴马隆、丙磺舒)3.抑制尿酸生成药(别嘌醇、非布司他)4.碱化尿液药(碳酸氢钠)3第三章呼吸系统疾病用药一.镇咳药1.中枢性镇咳药(可待园、双氢可待因、福尔可定、喷托维林、右美沙芬、苯丙哌林、依普拉酮、二氧丙嗪)2.外周性镇咳药(那可丁、左羟丙哌嗪)二.祛痰药1.恶心性祛痰药(氯化铵、愈创甘油醚、桔梗流浸膏)2.刺激性祛痰药(碘化钾、愈创木酚磺酸钾)3.黏痰溶解剂(溴已新、氨溴索、乙酰半胱氨酸、按柠蒎、厄多司坦、福多司担、美司坦、糜蛋白酶)4.黏痰稀释剂(羧甲司坦)三.平喘药1. β肾上腺素受体激动剂(麻黄碱、异丙肾上腺素、?沙丁胺醇、特布他林、氯丙那林、海索那林、福莫特罗、沙美特罗、丙卡特罗、克仑特罗、班布特罗、甲氧那明)2.M胆碱受体阻断剂(异丙托溴铵、噻托溴铵)3.黃嘌呤类药物(茶碱、氨茶碱、多索茶碱、二羟丙茶碱、胆茶碱、甘氨酸茶碱钠、赖氨酸茶碱)4.过敏介质阻释剂(色甘酸钠、酮替芬、曲尼司特、西替利嗪、氣雷他定)5.肾上腺皮质激素(布地奈德、氟替卡松、倍氯米松、曲安奈德、糠酸莫米松)6.白三烯受体拮抗剂(孟鲁司特、普仑司特、吡嘧司特、异丁司特)7.具有平喘作用的复方制剂(沙美特罗替卡松、布地奈德福莫特罗、复方异丙托溴铵)4第四章消化系统疾病用药一. 抗酸药和胃黏膜保护药抗酸药(铝碳酸镁、碳酸氢钠)胃黏膜保护药(枸橼酸铋钾、胶体果胶铋钾、复方铝酸鉍、硫糖铝、吉法酯、瑞巴派特、替普瑞酮)二.抑酸药1.H2受体阻断剂(法莫替丁、雷尼替丁)2.质子泵抑制剂(奥美拉唑、埃索美拉唑(艾斯奥美拉唑)、艾普拉唑、兰索拉唑、雷贝拉唑、泮托拉唑)3.钾离子竞争性酸抑制剂(沃诺拉赞)4.前列腺素类((米索前列醇)三. 解痉药、胃肠动力药和治疗功能性胃肠病药1.解痉药(颠茄、阿托品、山莨菪碱、丁溴东莨菪碱、东莨菪碱)2.胃肠动力药(甲氧氯普胺、莫沙必利、多潘立酮、溴米那普鲁卡因)3.治疗功能性胃肠病药(匹维溴铵、二甲硅油、间第三酚、曲美布汀、罌栗碱)四.止吐药昂丹司琼、多拉司琼、格拉司琼、帕洛诺司琼、托烷司琼、阿瑞匹坦五. 肝胆疾病用药1.肝脏疾病用药(联苯双酯、促肝细胞生长素、多烯磷脂酰胆碱、复方甘草甜素(复方甘草酸等)、甘草酸二铵、谷胱甘肽、还原型谷胱甘肽、硫普罗宁、门冬氨酸鸟氨酸、葡醛内酯、双环醇、水飞蓟宾、水飞蓟宾葡甲胺、水飞蓟素、异甘草酸镁、腺苷蛋氨酸)2.胆疾病用药(熊去氧胆酸、去氢胆酸)六.泻药和便秘治疗药(聚乙二醇、开塞露、硫酸镁、多库酯钠、复方聚乙二醇电解质1、II、H、IV、甘油、聚卡波非钙、普芦卡必利、乳果糖、利那洛肽)七.止泻药、肠道抗感染药、肠道消炎药A.止泻药1.肠道吸附剂(蒙脱石)2.含碳水化合物的电解质(补液盐I、II、III)3.抗动力药(洛哌丁胺)4.抗分泌药(消旋卡多曲)5. 微生态制剂地衣芽孢杆菌活菌、枯草杆菌、肠球菌二联活菌、枯草杆菌二联活菌、双歧杆菌活菌、双歧杆菌乳杆菌、三联活菌、双歧杆菌三联活菌、双歧杆菌四联活菌5B.肠道抗感染药(小檗碱、利福昔明、新霉素)C.肠道消炎药(柳氮磺砒啶、美沙拉嗪)八.助消化药(乳酶生、复发阿嗪米特、干酵母、米曲菌胰酶、易霉)6第五章心血管系统疾病用药一.抗心律失常药1.β受体阻断剂(普蔡洛尔、美托洛尔、阿替洛尔、阿罗洛尔)2.作用于心血管系统离子通道的药物a.钠通道阻滞剂( I类抗心律失常药) (普罗帕酮、奎尼丁、利多卡因、美西律、氟卡尼、伊布利特)b.延长动作电位时程药(III类抗心律失常药)(胺碘酮、索他洛尔)c.钙通道阻滞剂(IV类抗心律失常药) ( 维拉帕米、地尔硫䓬)二.抗高血压药1.肾素-血管紧张素系统抑制药a.血管紧张素转化酶抑制剂( ACEI) (卡托普利、福辛普利、贝那普利、依那普利、雷米普利、赖诺普利、培哚普利)b.血管紧张素II受体阻断剂(ARB ) ( 缬沙坦、厄贝沙坦、奥美沙坦、氯沙坦、替米沙坦、坎地沙坦)c.肾素抑制药(阿利吉仑)2. 钙通道阻滞剂a.二氢吡啶类钙通道阻滞剂(硝苯地平、氨氯地平、非洛地平、拉西地平、尼卡地平、尼群地平、西尼地平、马尼地平、贝尼地平)b.非二氢吡啶类钙通道阻滞剂(地尔硫䓬、维拉帕米)3.β受体阻断剂a.非选择性β受体阻断剂(普萘洛尔)b.选择性β1受体阻断剂(美托洛尔、比索洛尔、阿替洛尔)c.a1和β受体阻断剂(卡维地洛、拉贝洛尔、阿罗洛尔)4. 利尿剂a.噻嗪类利尿剂(氢氯噻嗪、吲达帕胺)b.袢利尿剂(呋塞米、托拉塞米)c.留钾利尿剂(阿米洛利、螺内酯)5.其他抗高血压药特拉唑嗪、肼屈嗪、甲基多巴、利血平、硝普钠三.调节血脂药71.主要降胆固醇的药物a.羟甲基戊二酰辅酶A还原酶抑制剂(洛伐他汀、普伐他汀、辛伐他汀、氟伐他汀、阿托伐他汀、瑞舒伐他汀、匹伐他汀)b.胆固醇吸收抑制剂(依折麦布)c.抗氧化剂(普罗布考)d.胆汁酸结合树脂(考来烯胺)2.主要降三酰甘油的药物a.贝丁酸类药(非诺贝特)b.烟酸类药(阿昔莫司)c.高纯度鱼油(多烯不饱和脂肪酸类)四.抗心绞痛药1.抗血小板药(阿司匹林、氯吡格雷、替格瑞洛)2.他汀类药物(洛伐他汀、普伐他汀、辛伐他汀、氟伐他汀、阿托伐他汀、瑞舒伐他汀、匹伐他汀)3. β受体阻断剂(美托洛尔、比索洛尔、卡维地洛、阿罗洛尔)4.ACEI类或ARB类药物(雷米普利、赖诺普利、培哚普利)5.钙通道阻滞剂(氨氯地平、非洛地平、地尔硫䓬、维拉帕米)6.硝酸酯类药物(硝酸甘油、硝酸异山梨酯、单硝酸异山梨酯)7.抗凝药(肝素、低分子量肝素、华法林、达比加群酯)8.其他(尼可地尔)五.抗心力衰竭药物1. 利尿剂(呋塞米、托拉塞米、氢氯噻嗪、螺内酯)2.血管紧张素转化酶抑制剂(卡托普利、福辛普利、贝那普利、雷米普利、赖诺普利、培哚普利)3. 血管紧张素II受体阻断剂(缬沙坦、氯沙坦、坎地沙坦)4. β受体阻断剂(美托洛尔、比索洛尔、卡维地洛)5. 强心苷类(地高辛、米力农)6.其他(沙库巴曲缬沙坦、伊伐布雷定、达格到净)8第六章血液系统疾病用药一.抗血栓药1.维生素K拮抗剂华法林、双香豆素、醋硝香豆素2.肝素和低分子肝素肝素钠、肝素钙、达肝素钠、那屈肝素钙、依诺肝素钠3.直接口服抗凝药达比加群酯、利伐沙班、阿哌沙班4. 抗血小板药a.血栓素素TXA2抑制剂(阿司匹林)b.二磷酸腺苷(ADP) P2Y12受体阻断剂(噻氯匹定、氯吡格雷、替格瑞洛)c.血小板糖蛋白(GP ) IIb/ lIa受体阻断剂(替罗非班、依替巴肽)d.其他抗血小板药(双嘧达莫、西洛他唑)f.溶栓药(溶栓酶) (尿激酶、重组链激酶、阿替普酶、瑞替普酶、重组人尿激酶原)二.抗出血药1.维生素K类(维生素K、维生素K、甲蔡氢醌、亚硫酸氢钠甲萘醌)2.凝血因子(人凝血酶原复合物、人纤维蛋白原、人凝血因子VIII、重组人凝血因子VIII、重组人凝血因子IX)3.蛇毒血凝酶(白眉蛇毒血凝酶、尖吻蝮蛇血凝酶、矛头蝮蛇血凝酶)4.抗纤维蛋白溶解药(氨基已酸、氨甲环酸)5.促血小板生成药(重组人血小板生成素、艾曲泊帕乙醇胺)6.毛细血管止血药(卡络磺钠、酚磺乙胺)6.血管硬化剂聚桂醇三.抗贫血药1. 铁剂(硫酸亚铁、右旋糖酐铁、葡萄糖酸亚铁、富马酸亚铁、蛋白琥珀酸铁、多糖铁复合物等。
三环类抗抑郁药致急性肺栓塞一例并文献复习

HE C h u n — l a i , HA N X u e( D e p a r t m e n t o f E m e r g e n c y ,G e n e r a l H o s p i t a l o f J i n g me i G r o u p , B e i j i n g 1 0 2 3 0 0 ,C h i n a )
[ 2 O ] 江 腊 梅 , 齐 向荣 . 1 6 0例 克林 霉 素 注 射 剂 致 肾毒 性 病 例
・6 5・
[ 2 4 ]梁 雁 , 张本静. 北京市 2 1 2 1例 克 林 霉 素 致 不 良反 应 分
分析 [ J ] . 中 国药 物 警 戒 , 2 0 1 2 , 9 ( 9 ) : 5 5 0 — 5 5 2 .
( 2): 8 7 — 8 9 .
[ 2 2 ] 路 长 飞 , 田春 华 , 田月沽 , 等. 药 品 不 良 反 应 信 号 的 验
证 和统 计 分 析 研 究 方 法 的 探 索 — — 基 于 克 林 霉 素 注 射 剂 致 肾毒 性 的 不 良反 应 监 测 数 据 [ J ] . 中 国 药 物 警
( 收稿时间 : 2 0 1 5 — 0 7 — 0 6 修 回时间 : 2 0 1 5 ・ 0 8 — 2 0 )
三环 类抗抑郁药致急 性肺 栓塞一例并文献复 习
何春来, 韩 雪
探讨 三环类抗抑郁药致急性肺 栓塞 ( p u l m o n a y r e mb o l i s m,P E) 的临床特 点 、 诊 断及治 疗方法 , 以 [ 摘要 ] 目的
减少漏误诊 。方法
对三环类抗抑郁药 致急性 P E 1 例 的 临 床 资 料 进 行 回顾 性 分 析 , 并 复 习 相 关 文 献 。 结 果 本 例
常用的抗抑郁药包括SSRI类三环类和MAOI类等

常用的抗抑郁药包括SSRI类三环类和MAOI类等抑郁症是一种常见的心理障碍,常常造成患者情绪低落、失眠等症状。
抗抑郁药是治疗抑郁症的主要方法之一,其中常用的抗抑郁药包括SSRI类、三环类和MAOI类等。
在使用这些药物时,需特别注意其副作用和禁忌症,以避免不必要的健康风险。
一、SSRI类抗抑郁药SSRI即选择性5-羟色胺再摄取抑制剂(Selective serotonin reuptake inhibitors),它是目前治疗抑郁症的主流药物之一。
SSRI 类抗抑郁药物通过抑制5-羟色胺再吸收,增加5-羟色胺在脑内的含量,从而改善患者的情绪障碍症状。
常见的SSRI类抗抑郁药物有帕罗西汀、舍曲林、氟西汀、西酞普兰等。
但是,使用SSRI类药物也存在副作用,例如口干、头痛、恶心、失眠、性功能障碍等。
在部分患者中,还可能引发自杀性心理和自杀倾向。
因此,在使用SSRI类药物时,需严格遵医嘱,避免自行增减药量或停药。
同时,需要密切观察患者的病情反应,如出现副作用、过敏等异常情况,应及时就医治疗。
二、三环类抗抑郁药三环类抗抑郁药是指结构上含有三种环式结构的药物,它具有强烈的抗抑郁作用,因此受到医生和患者的青睐。
三环类抗抑郁药物通过抑制去甲肝上腺素和5-羟色胺的再吸收,从而缓解患者的情绪障碍症状。
常用的三环类抗抑郁药物有阿米替林、多塞平、丙米嗪等。
然而,三环类抗抑郁药也存在很多副作用,如口干、头晕、便秘、心动过速等,同时还有心脏传导阻滞、抑制和谐性等严重副作用。
此外,三环类抗抑郁药物与多种药物有相互作用,如与某些高血压药、抗精神病药等联用会增加不良反应的风险。
因此,在选用三环类抗抑郁药物时,需要根据患者的实际情况进行调整,并密切观察患者的不良反应和副作用。
三、MAOI类抗抑郁药MAOI类抗抑郁药(monoamine oxidase inhibitors)是一类利用药物抑制单胺氧化酶(MAO)来达到抗抑郁效果的药物。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
三环类抗抑郁药 ( 专业知识值得参考借鉴 )
一概述三环类抗抑郁药 (TcAs) 是临床上治疗抑郁症最常用的药物之一,其核心结构是中间一个七
元杂环两边连接一个苯环构成。
其中,丙米嗪是最早发现的具有抗抑郁作用的化合物,目前常用药物还有氯米帕明、阿米替林、多赛平等。
TCAs主要在肝脏代谢,参与的代谢酶有CYP1A2、CYP2D6、CYP3A4等。
主要代谢为三环核氧化,如2 位或10 位碳原子羟化(CYP2D6催化)、脂肪侧链氧化、氮原子的去甲基化( CYP3A4催化)。
由于 CYP的活性受多种因素的影响,血浆中活性代谢产物的浓
度与原药浓度的比率有明显的个体差异。
二药理作用 TCAs阻断了去甲肾上腺素( NA)能和 5 羟色胺( 5-HT)能神经末梢对 NA和 5-HT 的再
摄取,增加了突触间隙单胺类递质的浓度,临床上表现为抑郁症状的改善。
目前研究发现,抗抑郁药对递质再摄取的抑制作用是立即发生的,而长期用药后则可以降低受体的敏感性(下调作用),这与抗抑郁药的临床效应滞后(用药 2~3 周后起效)密切相关。
NA再摄取的阻断使神经突触间隙
内源性 NA浓度增加,进而可以降低突触前膜α2 受体的敏感性,长期使用还可能减少中枢α 2 受体的数目。
5-HT 再摄取的抑制首先也是增加胞体部位突触间隙内源性5-HT 浓度,通过下调突触前胞体膜的 5-HT1A受体,增加末梢释放 5-HT,最终达到抗抑郁作用。
TCAs还有很强的阻断 5-HT2A 受体作用。
三适用范围适用于治疗各类以抑郁症状为主的精神障碍,如内因性抑郁、恶劣心境障碍、反应性
抑郁及器质性抑郁等。
还可用于治疗广泛性焦虑症、惊恐发作和恐怖症。
小剂量丙米嗪可米嗪可用
于治疗儿童遗尿症,氯米帕明则常用于治疗强迫症。
对精神分裂症患者伴有的抑郁症状,治疗宜谨慎, TCAs可能使精神病性症状加重或明显化。
三环类抗抑郁药曾经是首选的抗抑郁药,但是由于该类药物抗胆碱能和心血管不良反应较大,禁忌证和药物相互作用较多,安全范围较窄,使其临床应用受限。
TCAs服用超过一天剂量的10 倍时就有致命性危险,心律失常是最常见的致死原因。
四不良反应 1. 抗胆碱能不良反应
三环类抗抑郁药常见药物不良反应有口干、便秘、视物模糊、尿潴留、嗜睡、体重增加等,是其抗
胆碱能作用和抗组织胺作用的结果,与血药浓度相关,在治疗浓度范围内即可出现,存在着较大的
个体差异,并不是中毒的表现。
轻度的抗胆碱能药物不良反应一般不需做特殊处理,必要时可加用
少量胆碱。
2.中枢神系毒性
TCAs引起的中枢神系毒性反有情降低、注意力不集中、社会行异常、震、运失、
作、思障碍、幻妄想、定向力障碍、焦不安、妄、意模糊、昏迷等。
3.心血管系毒性
TCAs引起的心血管毒性反包括体位性低血、心速、阻滞、心律失常及心跳停等。
TCAs所致的体位性低血,主要与受体的敏感性有关,在低血度就可生,更多于老
年人和患有充血性心力衰竭的病人。
五注意事重心、肝、疾病患者,以及粒胞减少、青光眼、前列腺肥大患者禁用,妊娠
3个月禁用。
患者和老年人慎用。
(明:上述内容作介,物使用必正医院在医生指下行。
)
寄:“身体是革命的本”。
身体健康是人最基本的,也是很达到的目。
今天,你能开口,能用眼睛、耳、鼻子去感知身的一切事物,能正常地用双腿行走,无病无痛⋯⋯些看起
来是很而易的,但是你是否想些却是极度重要且来之不易的,如果某一天你失去了,怎么?看到街上那些失明失、断手少腿的残疾人,你是否在想:幸好我没有像他那,你了,
生命充意外,能保你明天不会成他中的一呢?那你又是否因此更加懂得珍惜健康呢 ?
那就不要透支自己的身体健康,赶快行起来,身体,身心健康吧! 要清楚意到自己目前的健康状况是稍即逝的,明确健康是我做任何事情的本,要懂得珍惜健康!。