2009年糖尿病用药市场研究报告
2009年中国糖尿病药物市场分析

2009年中国糖尿病药物市场分析发表时间:2009年11月 9日糖尿病已成为人类第四大死因,全球每年有超过380万人死于糖尿病及其并发症。
目前全世界已有2.46亿糖尿病患者。
我国近20年来糖尿病发病率增长了5倍多,是全球增长最快的国家之一。
如此高的糖尿病发病率催生出潜力巨大的糖尿病用药市场。
糖尿病用药领域也已成为各大药企征战的重点。
2008年,全球糖尿病市场总销售额高达240亿美元,而在全球糖尿病药物中,口服药市场份额略高于胰岛素制剂。
外资产品称霸市场据华源医药电子商务数据推算,在国内4900家综合医院及近万家政府办中医院,口服糖尿病用药的购药金额均在逐年增加,且近几年在整体市场中所占份额相对稳定。
在口服糖尿病用药市场上,外企所占金额份额远远大于国内企业。
其中,拜耳医药保健有限公司最为突出,其拳头产品阿卡波糖(拜糖平)独占了30%的市场份额;在销售业绩排在前10名的企业中,三资企业占到90%,内资企业仅有北京万辉双鹤药业一家跻身前10。
造成这种市场格局很重要的原因是,口服降糖药中的明星产品基本为国外企业的专利药,虽然仿制药也层出不穷,但并未对专利药产生太大的影响;同时,专利药的推广也非常成功,牢牢控制着市场。
口服降糖药品种浅析口服糖尿病用药城市主要集中在北京和上海,两地用药金额份额超过50%。
两地用药金额最大的都是阿卡波糖。
目前国内批准使用的口服降糖药有促胰岛素分泌剂(磺酰脲类、格列奈类)和非促胰岛素分泌剂(α-糖苷酶抑制剂、双胍类、噻唑烷二酮胰岛素增敏剂)。
华源医药电子商务抽样数据涉及常用的20多个口服降糖药品种,按照用药金额份额依次降低排序为α-糖苷酶抑制剂、磺酰脲类促胰岛素分泌剂、非磺酰脲类胰岛素分泌剂、双胍类、噻唑烷二酮胰岛素增敏剂和中药降糖药,其中α-糖苷酶抑制剂在金额份额上一直领先。
近年来,非磺脲类促泌剂的销售增势最为明显,并在2008年将双胍类挤出前三。
双胍类代表药物盐酸二甲双胍作为2型糖尿病的一线用药备受市场青睐,所以从口服降糖药销售数量来看,双胍类药物仍遥遥领先。
2009年度我院降糖药物用药分析

2009年度我院降糖药物用药分析【摘要】目的总结河南省人民医院2009年降糖药的应用现状和发展趋势。
方法利用计算机网络管理系统对本院2009年各种降糖药的用药频度(DDDs)、用药金额、日治疗费用(DDC)及其排序等统计数据进行分析。
结果2009年应用的降糖药共有30个品种,其中注射剂19种,占用药金额的79.87%;口服剂型11个品种,占用药金额的20.13%;结论本院胰岛素制剂的应用占主导地位,该类药物使用合理。
【关键词】降糖药; 用药分析糖尿病是一组以慢性血糖水平增高为特征的代谢疾病群,是常见病、多发病,已成为继心血管病和肿瘤之后的第三大非传染性病症[1]。
良好的血糖控制可以减少糖尿病患者慢性并发症的发生,而降血糖药物是控制血糖的有效方法。
为了探讨临床用药的经济性、方便性和合理性,现对本院2009年降糖药物的应用情况进行统计、分析,报告如下。
1 资料与方法1.1 资料来源原始数据取自我院药库微机管理系统数据库,以2009年降糖药品出库数量和金额为基本素材,利用计算机进行数据合并、统计、排序等处理。
1.2 分析方法采用DDD分析法和金额排序法,综合分析该类药物使用情况:①限定日剂量(DDD)的确定:具体计算参照WHO药物统计中心制定的方法结合药品说明书和临床使用情况设定;②用药频度(DDDs)=总用药量/相应药品DDD 值, DDDs排序在前表示用药频率高;③药物限定日费用(DDC)=药品的销售总金额/该药品DDDs,DDC代表着该药的价格水平,表示患者应用该种药物平均的日费用;对用药总金额和DDDs 值排序,并求其比值,评价药物费用的合理程度;比值接近1.00时,表示购药与用药频度同步性良好;④采用金额排序法,统计注射用胰岛素和口服降糖药的用药金额及百分比;各类口服降糖药的构成比;各种胰岛素制剂的详细用药情况。
2 结果2009年应用的降糖药共有30个品种,其中注射剂19种,占用药金额的79.87%;口服剂型11个品种,占用药金额的20.13%。
我院2009年至2010年门诊口服降糖药使用分析
Ke rs Oa hp g cm eae t; e i t nf qe c DD s ; s gaa s ywod r yol e i gns M dc i eun y( D ) U i n yi l y ao r n l s
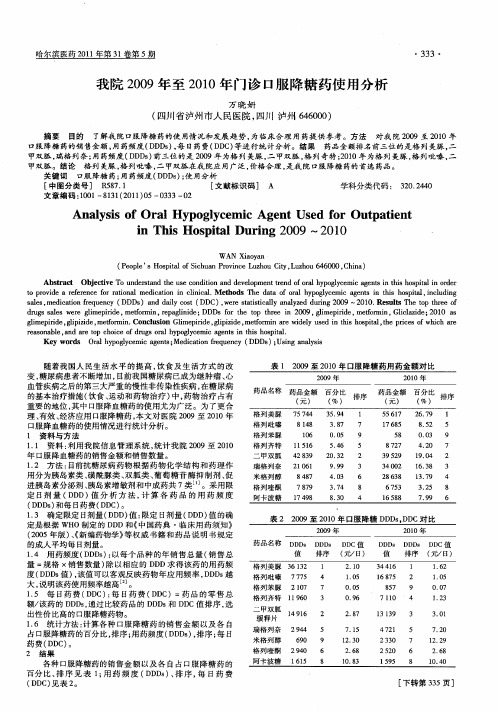
随着我 国人 民生 活水 平 的提 高 , 饮食 及生 活 方式 的改 变, 糖尿病 患者不断增加 , 目前 我国糖尿病 已成 为继肿瘤 、 心 血 管疾病之后 的第 三大严重 的慢性非传染性 疾病 , 在糖 尿病 的基本治疗措施 ( 饮食 、 运动 和药物治 疗 ) , 中 药物 治疗 占有 重 要的地位 , 其中 口服降血糖药 的使 用尤 为广泛 。为 了更合 理、 有效 、 经济应用 1服 降糖 药 , : 3 本文 对 医院 20 0 9至 2 1 00年 口服降血糖药 的使用情况进 行统计分析 。 1 资 料 与 方 法 1 1 资料 : . 利用我 院信 息管理 系统 , 统计我 院 20 0 9至 2 1 00 年 口服降血糖药 的销售金额 和销售数量 。 12 方法 : . 目前抗糖尿病 药物 根据 药物化 学结 构 和药理 作 用 分为胰 岛素类 、 磺酰脲类 、 双胍类 、 葡萄糖 苷 酶抑制 剂 、 促 进 胰岛素分泌剂 、 胰岛素增敏剂和 中成 药共 7类 J 。采用限 定 日剂 量 ( D 值 分 析 方 法 , 算 各 药 品 的用 药 频 度 D D) 计 ( D s 和每 日药费 ( D ) D D) D C 。 13 确定 限定 日剂 量( D 值 : . D D) 限定 日剂 量 ( D 值 的确 D D) 定是 根据 WHO制定的 D D和《 D 中国药典 ・ 临床用 药须知 》 ( 0 5年版 ) 《 20 、 新编药物学 》 等权 威书 籍和 药 品说 明书规 定 的成 人 平 均 每 日剂 量 。 14 用药频度 ( D s : . D D ) 以每个 品种 的年 销售 总量 ( 销售 总 量 =规格 ×销售数量 ) 除以相应 的 D D求得该药 的用 药频 D 度 ( D s ) 该值 可以客观反映药物 年应 用频率 , D s D D值 , D D 越 大 , 明该 药使 用频率越 高 J 说 。 1 5 每 日药 费 ( D : 日药 费 ( D . D C) 每 D C)=药 品 的零 售 总 额/ 该药 的 D D , D s通过 比较药 品 的 D D D s和 D C值排 序 , D 选 出性价 比高 的口服降糖药物 。 I 6 统计方法 : 算各种 口服 降糖药 的销 售金 额 以及 各 自 . 计 占 口服降糖药的百分 比, 排序 ; 用药频度 ( D s , 序 ; 日 D D )排 每 药 费( D ) D C。
2009—2011年我院糖尿病治疗药物应用情况研究

y e a r s o f hi t s h o s p i ml w e r e c a l c u l a t e d a n d a n a l y z e d . Re s u l t s Du i r n g he t p a s t t h r e e y e a r s ,t he n u mb e r o f p a t i e n t s wi t h d i be a t e s
p l e S H o s p i t a l ,H e j i a n g 6 4 6 2 0 0 ,C h i n a
【 A b s t r a c t 】 O b j e c i t v e T o e x p l o r e t h e s t a t u s q u o o f a : p p l i c a t i o n a n d d e v e l o p m e n t t r e n d o f a n t i — d i a b e t i c d r u g s .Me t h -
雷 芳 ,任 莉 莉
【 摘要】 目的 探讨糖尿病治疗药物的应用现状和发展趋势。方法
主要品种、金额 、用 药频度 、联合用药等情况进行统计和分析。结果
对近 3年来我院糖尿病治疗药物的处方、
3年 中糖尿病 患者人 数增 长 了5 8 . 1 % ,处方数
从2 0 0 9年的 3 8 7 1张增加到 2 0 1 1 年的5 8 8 9张 ,增长率为 5 2 . 1 3 %。糖尿病 药物销售额所 占总额的比例从 1 . 0 5 %上升到
・l 0・ Fra bibliotekC l i n i c a l Ra t i o n a l Dr u g Us e ,F e b ua r r y 2 01 3, Vo 1 . 6 N o . 2 C
2009年至2011年我院口服降糖药应用分析

关键词 : 口服 降糖药; 用药分析 ; 用药频度 ; 限定 日费用
中图 分 类 号 : F 4 0 7 . 7 ; R 9 6 9 . 3 ; R9 7 7 . 1 5 文献标识码 : A 文 章编 号 : 1 0 0 6— 4 9 3 1 ( 2 0 1 3 ) 1 6—0 0 6 1— 0 2
2 0 0 9年 至 2 0 1 1 年1 3 ' 服 降糖 药进 行 分 类 统 计 、 综合 分析 。 结 果 各 年 度 口服 降 糖 药 的 用 药 金 额 和 D D D s 均 呈现 增 长 趋 势 , 胰 岛 素 增 敏 药用量 呈下降趋 势。 销 售 金 额 排 序 前 2位 的 始 终 是 瑞 格 列奈 和 阿 卡 波 糖 , D D D s 排 序 前 2位 的 始 终 是 二 甲双 胍 、 瑞格 列奈 。 结 论 该
App l i c a t i o n o f Or a l Hy po g l y c e mi c Dr u g s i n Our Ho s p i t a l b e t we e n 2 0 0 9 a nd 2 01 1
Xi e Me i , Hu Zh e n gb o, Xu Ch un h o n g, Xu L i
d ug r s . Me t h o d s T h e s a l e s a mo u n t , DDD s a n d D DC we r e a d o p t e d t o c o n d u c t t h e c l a s s i i f e d s t a t i s t i c a n d t h e c o mp r e h e n s i v e a n a l y s i s o n t h e u t i l i z a t i o n o f o r a l h y p o g l y c e mi c d r u g s b e t we e n 2 0 0 9 a n d 2 0 1 1 . Re s u l t s T h e s a l e s a mo u n t a n d DDD s o f o r a l h y p o g l y c e mi c d r u g s i n
2009年在研的183种糖尿病药Diabetes_图文(精)

2009DiabetesME D I C I N E SI NDE V E L O P M E N TF O RReportP R E S E N T E DB YA M E R I C A’S P H A R M A C E U T I C A L R E S E A R C H C O M P A N I E SBiopharmaceutical Companies Developing Record183 Medicines to Treat Diabetes and Related Conditions* For more information about a specific medicine in this report, please call the telephone number listed.GLP-1Emisphere Technologies type 2 diabetes Phase I (oralCedar Knolls, NJ(973 532-8000GLP-1 FC Eli Lilly type 2 diabetes Phase IIIndianapolis, IN(800 545-5979GLP-1 PEG Eli Lilly type 2 diabetes Phase IIndianapolis, IN(800 545-5979HDV-insulin Diasome Pharmaceuticals type 2 diabetes Phase II Conshohocken, PA(609 923-9443HE3286Hollis-Eden type 2 diabetes Phase II Pharmaceuticals(858 587-9333San Diego, CAHSD016Wyeth Pharmaceuticals diabetes Phase ICollegeville, PA(800 934-5556IL-1 antibody Eli Lilly type 2 diabetes Phase IIndianapolis, IN(800 545-5979INCB-13739Incyte type 2 diabetes Phase IIWilmington, DE(302 498-6700INCB-19602Incyte type 2 diabetes Phase IIWilmington, DE(302 498-6700INCB-20817Incyte type 2 diabetes Phase IIWilmington, DE(302 498-6700INGAP peptide Kinexum Metabolics type 1 diabetes, type 2 diabetes Phase II completed Harper’s Ferry, WV(304 535-3037insulin inhalation Baxter Healthcare diabetes Phase IDeerfield, IL(800 422-9837insulin inhalation MicroDose Technologies diabetes Phase I completed Monmouth Junction, NJ(732 355-2100insulin nasal spray MDRNA type 2 diabetes Phase IIBothell, WA(425 908-3601insulin oral Emisphere Technologies type 2 diabetes Phase I/IICedar Knolls, NJ(973 532-8000insulin oral Generex Biotechnology type 1 diabetes Phase III Toronto, Canada(416 364-2551insulin transdermal Dermisonics type 1 diabetes, type 2 diabetes Phase I Irvine, CA(888 401-3376INT-131InteKrin Therapeutics type 2 diabetes Phase IILos Altos, CA(650 941-5501Intesulin™Coremed diabetes Phase Iinsulin oral Lake Bluff, IL(847 772-6868ISIS 113715Isis Pharmaceuticals type 2 diabetes Phase II Carlsbad, CA(combination therapy(800 679-4747ISIS-SGLT2rx Isis Pharmaceuticals type 2 diabetes Phase I Carlsbad, CA(800 679-4747JTT-654Akros Pharma type 2 diabetes Phase IPrinceton, NJ(609 919-9570application submitted—An applica-tion for marketing has been submit-ted by the company to the Food and Drug Administration (FDA.diabetes—A chronic disease in which the body does not produce or properly use insulin, a hormone that is needed to convert sugar, starches and other food into energy needed for daily life. Symptoms may include excessive thirst, hunger, urination and weight loss. The cause of dia-betes continues to be a mystery, although both genetics and environ-mental factors such as obesity and lack of exercise appear to play roles. Type 1 diabetes, th e more severe form, results from the body’s failure to produce insulin, which “unlocks”the cells of the body, allowing glu-cose to enter and fuel them. It is estimated that 5 percent to 10 per-cent of Americans who are diag-nosed with diabetes have type 1, which requires insulin treatment. Type 2 diabetes results from insulin resistance (a condition in which the body fails to properly use insulin, combined with relative insulin defi-ciency. Most Americans who are diagnosed with diabetes have type 2, which in most cases can be con-trolled by a combination of dietary measures, weight loss, and oral medication.diabetic peripheral neuropathy—Nerve damage in the arms, hands, legs, and feet caused by diabetes. The condition develops slowly and worsens over time. Depending on the types of nerves involved, one or more signs and symptoms may be present in diabetic peripheral neu-ropathy. Sensory neuropathy results in numbness or tingling in the feetor pain or discomfort in the feet or legs, including prickly, sharp pain or burning feet. Motor neuropathyinvolves muscle weakness and lossof muscle tone in the feet and lowerlegs, loss of balance, or changes infoot shape that can lead to areas ofincreased pressure. Autonomic neu- ropathy results in dry feet and cracked skin. The loss of sensation and other problems associated with nerve damage make a patient prone to developing skin ulcers (open sores that can become infected and may not heal. This serious complica- tion of diabetes can lead to the loss of a foot, a leg, or even a life. diabetic retinopathy—The most common diabetic eye disease anda leading cause of blindness in American adults. It is caused by changes in the blood vessels of the retina, the light-sensitive tissue at the back of the eye that is necessary for good vision. In some people with diabetic retinopathy, blood vesselsmay swell and leak fluid. In others, abnormal new blood vessels grow on the surface of the retina. Over time, diabetic retinopathy, which usually affects both eyes, can worsen and cause vision loss. The condition has four stages: 1 mild nonprolifera- tive retinopathy, the earliest stage during which microaneurysms occur in the retina’s tiny blood vessels; 2 moderate nonproliferative retinopa- thy, during which some blood ves- sels that nourish the retina are blocked; 3 severe nonproliferative retinopathy, when many more blood vessels are blocked and deprive several areas of the retina with their blood supply; and 4 proliferative retinopathy, the advanced stagewhen signals sent by the retina for nourishment trigger the growth of new blood vessels, which grow along the retina and the surface of the clear, vitreous gel that fills the inside of the eye. If those thin, frag- ile blood vessels leak blood, severe vision loss and even blindness can result. Up to 45 percent of Americans diagnosed with diabetes have some stage of diabetic retinopathy. macular edema—A condition in which fluid can leak into the center of the macula, the part of the eye where sharp, straight-ahead vision occurs. The fluid makes the macula swell, thus blurring vision. It can occur at any stage of diabetic retinopathy, although it is morelikely to occur as the disease pro- gresses. About half of the people with proliferative retinopathy also have macular edema.Phase I—Safety testing and pharma- cological profiling of new drugs in small numbers of humans.Phase II—Effectiveness testing and identification of side effects of new drugs in humans.Phase III—Extensive clinical trials in humans to verify effectiveness and monitor adverse reactions of new drugs.polyneuropathy—A diffuse periph- eral nerve disorder that is bilaterally symmetrical and thus not confined to the distribution of a single nerve or a single limb. Electrodiagnostictests are done to classify the nerve structures involved, their distribu- tion, and the severity of the disorder in order to help identify the cause. Some polyneuropathies, such as those caused by lead toxicity or tick bite, affect primarily motor fibers. Others, such as those caused by diabetes or AIDS, affect primarily sensory fibers. Diabetic neuropathiescan also affect cranial nerves.T he U.S. system of new drug approvals is perhaps the most rigorous in the world.It takes 10-15 years, on average, for an experimental drug to travel from lab to U.S. patients, according to the Tufts Center for the Study of Drug Development, based on drugs approved from 1994 through 1998. Only five in 5,000 compounds that enter preclinical testing make it to human testing. And only one of those five is approved for sale.On average, it costs a company $1.3 billion to get one new medicine from the laboratory to U.S. patients, according to a 2007 study by the Tufts Center for the Study of Drug Development.Once a new compound has been identified in the laboratory, medicines are developed as follows: Preclinical Testing. A pharmaceutical company con -ducts laboratory and animal studies to show biological activity of the compound against the targeted disease, and the compound is evaluated for safety.Investigational New Drug Application (IND.After completing preclinical testing, a company files an IND with the U.S. Food and Drug Administration (FDA to begin to test the drug in people. The IND becomes effective if FDA does not disapprove it within 30 days. The IND shows results of previous experiments; how, where and by whom the new studies will be conducted; the chemical structure of the compound; how it is thought to work in the body; any toxic effects found in the animal studies; and how the compound is man -ufactured. All clinical trials must be reviewed and approved by the Institutional Review Board (IRB where the trials will be conducted. Progress reports on clinical trials must be submitted at least annually to FDA and the IRB.Clinical Trials, Phase I.These tests involve about 20 to 100 normal, healthy volunteers. The tests study a drug’s safety profile, including the safe dosage range. The studies also determine how a drug is absorbed, distributed, metabolized, and excreted as well as the duration of its action.Clinical Trials, Phase II.In this phase, controlled trials of approximately 100 to 500 volunteer patients (people with the disease assess a drug’s effectiveness.Clinical Trials, Phase III.This phase usually involves 1,000 to 5,000 patients inc linics and hospitals. Physicians monitor patients closely to confirm efficacy and identify adverse events.New Drug Application (NDA/Biologic License Application (BLA.Following the completion of all three phases of clinical trials, a company analyzes all of the data and files an NDA or BLA with FDA if the data successfully demonstrate both safety and effec -tiveness. The applications contain all of the scientific information that the company has gathered. Applications typically run 100,000 pages or more. The average review time for the 24 new therapeutics approved by the FDA in 2008 was 17.8 months.Approval.Once FDA approves an NDA or BLA, the new medicine becomes available for physicians to prescribe. A company must continue to submit periodic reports to FDA, including any cases of adverse reactions and appropriate quality-control records. For some medicines, FDA requires additional trials (Phase IV to evaluate long-term effects.Discovering and developing safe and effective new medicines is a long, difficult, and expensive process. Pharmaceutical companies invested an estimated $65.2 billion in research and development in 2008.‘Sharing Miracles’ Television Program Features Inspirational Stories of Real Diabetes Patients S haring Miracles—a 30-minute public affairs television program—tells the compelling and inspirational stories of real patients. Two recent episodes focused on patients who suffer from diabetes— Leave It to Beaver star Jerry Mathers and professional basketball star Dominique Wilkins. Mathers is an American icon, best known for his portrayal of the mischievous Theodore “Beaver” Cleaver. Currently shown on TV Land and in countries throughout the world, Leave It to Beaver has made JerryMathers one of the best-known actors in television history. D espite Beaver’s seemingly perpetual youth, life caught up with Mathers when he was diagnosed with diabetes. Originally faced with a life expectancy of three to five years, he has kept his disease at bay over the last 10 years. Speaking of his experience on Sharing Miracles, Mathers says, “You have to take control of your diabetes; you can’t let it take control of you.” Now, Mathers works tirelessly as a patient advocate, using his celebrity to help spread the word to others. Hall-of-Famer Dominique Wilkins is one of the greatest players in the history of the National Basketball Association (NBA. Wilkins is a nine-time NBA all-star, league scoring champion, and the winner of the NBA’s slam dunk contest. But today, in addition to fame, he also lives with diabetes, a disease that took the life of his father and grandfather, and has afflicted other members of his family. “Once I found out what my problem was, I changed my diet, and I started to exercise and take my medication…I didn’t want what happened to my father to happen to me, and I wasn’t going to let diabetes beat me,” Wilkins says. “For me, going through what I’ve been through with diabetes made me realize that I have to be a champion in helping try to eradicate this disease.” Previous episodes of Sharing Miracles have featured Academy Award-winning actress Marcia Gay Harden, a breast cancer advocate; Grammy Award-winning country music superstar Naomi Judd, who overcame hepatitis C; Emmy Award-winning actor Joey Pantoliano, who suffers from clinical depression; Super Bowl Champion and former Pittsburgh Steelers running back Jerome Bettis, who has asthma; two-time NCAA tournament-winning University of Connecticut basketball coach Jim Calhoun, who has overcome cancer three times; Emmy-nominated former star of Family Ties Meredith Baxter, who survived breast cancer; Olympic Gold Medal winners Mark Spitz (high cholesterol, Bruce Jenner (attention deficit disorder, and Greg Louganis (HIV; syndicated television talk show host Montel Williams, who suffers from multiple sclerosis; pop icon and Broadway star Deborah Gibson, who has suffered from devastating anxiety attacks; and Pro Football Hall-of-Famer and Super Bowl Champion Len Dawson, who survived prostate cancer. Sharing Miracles is produced by PhRMA’s Communica tions & PublicAffairs Department and airs on Sunday mornings on more than 300 television stations across the United States, reaching more than 50 million households. The show’s corresponding Web site, , is an interactive forum for people to relate their own personal stories of hope and survival. Every patient’s battle is unique, but the collective power of shared experiences can offer great help and courage to others who are fighting for their lives. You can find out where Sharing Miracles is showing in your area and order free DVDs of the show on the web site or by calling 202-835-3460. You can also view the show in it’s entirety at anytime on our web site,. New Medicines. New Hope.® Pharmaceutical Research and Manufacturers of America 950 F Street, NW Washington, DC 20004 | | | | 5/09。
2009~2012年我院抗糖尿病药物用药分析

2009~2012年我院抗糖尿病药物用药分析
李磊
【期刊名称】《齐齐哈尔医学院学报》
【年(卷),期】2013(034)015
【摘要】目的了解我院降糖药临床使用情况和变化趋势,探讨降糖药的合理使用.方法采用金额排序、DDDs排序的分析方法对我院2009~2012年抗糖尿病药物进行统计、分析.结果 4年来我院降糖药使用金额逐年上升,用药金额与用药频度基本呈正相关性.双胍类、磺脲类及胰岛素类药连续4年为临床主要使用的降糖药.二甲双胍、格列吡嗪、普通胰岛素、诺和灵30R等为一线用药.结论我院降糖药使用是合理的.
【总页数】3页(P2276-2278)
【作者】李磊
【作者单位】221002 徐州市第一人民医院药剂科
【正文语种】中文
【相关文献】
1.我院2012~2014年抗糖尿病药物用药分析 [J], 董洪明
2.我院2009-2012年门诊抗精神病药用药分析 [J], 李焕芬;王来海;蒋立新
3.我院抗糖尿病药物用药分析 [J], 张桂芳;张金凤;田绍丽;滑翔
4.2010年我院口服抗糖尿病药物用药分析 [J], 吴杏梅
5.我院药房抗糖尿病药物的用药分析 [J], 周娟
因版权原因,仅展示原文概要,查看原文内容请购买。
2009~2012年住院患者口服抗糖尿病的药物分析

2009~2012年住院患者口服抗糖尿病的药物分析目的了解我院抗糖尿病药物的使用情况,为临床合理用药提供一定的参考。
方法采用金额排序法和频度分析法(DDDS)抽取我院于2009年~2012年收治的住院患者口服抗糖尿病药物的应用情况,并进行统计分析。
结果经过统计结果分析显示,口服抗糖尿病用药金额呈现逐年增长的趋势。
住院患者口服抗糖尿病药物的用药频度(DDDs)中,二甲双胍的用药频度(DDDS)最高,说明深受患者所欢迎。
同时,在4年内的用药频度(DDDS)连续上升的药物分别是二甲双胍、阿卡波糖、吡格列酮、瑞格列奈以及格列吡嗪。
4年内用药频度(DDDS)出现连续下降的药物分别是格列本脲和格列硅酮两种药物。
结论本院口服抗糖尿病药物的使用基本合理,安全性高、依从性好、价格适中,深受临床医师和住院患者的欢迎。
标签:住院患者;糖尿病;口服;药物糖尿病(Diabetes)是一种临床较为常见的疾病,多由胰岛素分泌缺陷或者胰岛素作用障碍所致[1]。
作为一种以高血糖为特征的代谢性疾病,如果患者没有得到及时有效的治疗,则易出现多种较为严重的并发症,如肾脏病变、血管病变等,甚至会危及患者的生命[2]。
临床治疗方法大多数是对症治疗,将患者的高血糖恢复至正常水平,以减少相关并发症的发生[3]。
目前,糖尿病的基本治疗多以药物为主,其中口服抗糖尿病药物占据多数。
本文采用金额排序法和频度分析法(DDDS)抽取我院于2009年~2012年收治的住院患者口服抗糖尿病药物的应用情况,并进行统计分析,为临床合理用药提供一定的指导。
1资料与方法1.1一般资料所有数据均来源于我院计算机系统,收集2009年~2012年住院患者口服抗糖尿病药用药数据,包括药品的种类、药品的名称、药品的规格以及药品的用药金额等。
1.2方法本次研究中主要采用金额排序法和用药频度(DDDs)分析法。
其中,金额排序法主要用于统计并比较2009年~2010年我院住院患者口服抗糖尿病药物用药的金额。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
糖尿病用药市场研究报告(2009 年)
第一部份 糖尿病用药市场概述
© Copyright of 广州标点医药信息有限公司 3
糖尿病用药市场研究报告(2009 年)
第一节:糖尿病流行病学分析
第十二届中华医学会糖尿病分会于 2008 年 11 月 7 日在厦门开幕,大会主 席杨文英教授报告了中华医学会糖尿病分会的流行病学研究发现,中国大、中城 市和乡镇 20 岁以上的人群糖尿病患病率已经超过 10%,标志着中国糖尿病流行 已跨入 10.0 时代。而且糖尿病前期高达 15%,糖尿病的防治雪上加霜,今后 10 年糖尿病防治的任务更加艰难。
标点行业信息服务
糖尿病用药市场研究报告(2009 年)
TIME:2008 年全年
糖尿病用药市场研究报告
广州标点医药信息有限公司
2009 年
Tel:020-37886776
© Copyright of 广州标点医药信息有限公司 0
Байду номын сангаас
糖尿病用药市场研究报告(2009 年)
第四部份 糖尿病用药市场品种分析……………………………………………………… 22 第一节:胰岛素制剂…………………………………………………………………………23 第二节:阿卡波糖……………………………………………………………………………24 第三节:二甲双胍……………………………………………………………………………25 第四节:瑞格列奈……………………………………………………………………………26 第五节:罗格列酮……………………………………………………………………………27 第六节:格列吡嗪……………………………………………………………………………28 第七节:格列喹酮……………………………………………………………………………29 第八节:格列齐特……………………………………………………………………………30 第九节:那格列奈……………………………………………………………………………31 第十节:消渴丸………………………………………………………………………………32
糖尿病用药市场研究报告(2009 年)
化率为 10.299%) 随着年龄的增加,糖尿病的患病率明显增加,男性的患病率明 显高于女性。
★ 未诊断率近六成 1994 年,有糖尿病但未诊断出来的患者为 70.3%,而这次调查未诊断出来的 患者约为 57%,这说明“不查不知道”的糖尿病患者占 57%,城市的未诊断率为 52.5%,农村则高达 67.64%,凸现了农村医疗状况落后的局面。 ★ 糖尿病前期患病率达 15% 糖尿病前期的患病率已经超过了糖尿病患病率, 高达 15.19% (人口标化率 为 14.77%)。今后我们的防治任务更加艰巨。在单纯空腹血糖受损(IFG)方面, 中年男性明显高于女性。而单纯糖耐量异常(IGT)则是中年女性高于男性。 ★ 中年男性患病率增加明显 与 1994 年的糖尿病患病率相比,2007~2008 年度调查的中青年人的糖尿病 患病率明显升高,而且糖尿病前期的增长幅度更为明显。20~60 岁年龄段的男 性糖尿病患病率显著高于女性。与以前的数据相比,25~64 岁的年龄段在 15 年 中糖尿病患病率增加了 4 倍。中国目前的糖尿病患病率已经接近台湾和香港等以 城市为主的地区。 经分析,遗传不能解释男性糖尿病患病率显著高于女性。在相同的年龄段中, 男性诊断为糖尿病的年龄比女性提前了 2 年,体重指数和腰围都高于女性,男性 的甘油三酯也高于女性。男性有 34.29%为中心性肥胖(腰围>90cm),女性则有 26.53%为中心性肥胖(腰围>85cm)。 我国代谢综合征的总患病率已达 14%。男性代谢综合征的患病率明显高于同 年龄组的女性。 ★ 确立糖尿病高危人群 年龄是糖尿病的主要危险因素,中青年人群,尤其是男性糖尿病患病率变化 明显,可能与肥胖、高甘油三酯有关,城市和农村的糖尿病均明显升高。根据目 前的结论,在中国仅城市糖尿病患者就高达 4100 万人。 研究表明,有糖尿病家族史者患糖尿病的危险增加 3 倍。研究还发现,文化 程度越低,患糖尿病的风险越高;年龄每增加 10 岁,糖尿病的风险增加 60%; 收缩压每升高 10 mmHg,糖尿病的风险增加 20%;中心型肥胖或以前肥胖者糖尿 病风险增加 1 倍;甘油三酯每升高 50mg,糖尿病的风险增加 5%;而高收入者和 女性糖尿病风险降低。
目录
第一部份 糖尿病用药市场概述………………………………………………………………3 第一节:糖尿病流行病学分析………………………………………………………………4 第二节:糖尿病用药简介及分类……………………………………………………………7
第二部份 国外糖尿病用药市场状况……………………………………………………… 9 第一节:2007-2008 年全球糖尿病治疗新药上市情况……………………………………10 第二节:全球糖尿病用药市场概况…………………………………………………………12
表 表 1:2007 年全球批准的抗糖尿病 NME……………………………………………………10 表 2:2008 年全球处方药市场 15 大畅销治疗类别………………………………………12 表 3:2007 年全球畅销药物 50 强抗糖尿病药物…………………………………………13 表 4:2007 年我国糖尿病用药各类别市场规模分布………………………………………17 表 5:2007 年我国糖尿病口服用药前 10 位品牌…………………………………………17 表 6:2005-2008 年全国糖尿病用药医院市场份额排名前 20 位的厂家…………………19 表 7:2005-2008 年全国糖尿病用药医院市场集中度表…………………………………20 表 8:2005-2008 年市场份额前 10 位糖尿病治疗药物医院市场份额及增长率…………21 表 9:2008 年胰岛素制剂医院市场份额排名前五位的厂家情况…………………………23 表 10:2008 年阿卡波糖市场份额排名前三位的厂家情况………………………………24 表 11:2008 年二甲双胍市场份额排名前五位的厂家情况………………………………25 表 12:2008 年瑞格列奈市场份额排名前二位的厂家情况………………………………26 表 13:2008 年罗格列酮市场份额排名前五位的厂家情况………………………………27 表 14:2008 年格列吡嗪市场份额排名前五位的厂家情况………………………………28 表 15:2008 年格列喹酮市场份额排名前四位的厂家情况………………………………29 表 16:2008 年格列齐特市场份额排名前五位的厂家情况………………………………30 表 17:2008 年那格列奈市场份额排名前六位的厂家情况………………………………31 表 18:在研的Ⅱ/Ⅲ期临床糖尿病药物……………………………………………………41
2、最新糖尿病流行病学调查结果公布
★ 成人糖尿病患病率逾一成 我国 20 岁以上的成人糖尿病患病率已经超过 10%,达到 11.66% (人口标化 率为 11.28%),其中男性 13.31%(人口标化率为 12.91%),女性 10.59%(人口标
© Copyright of 广州标点医药信息有限公司 4
第五部份 中国糖尿病用药生产厂家、商品名、价格及进入医保目录情况………………33 第一节:糖尿病用药主要品种生产企业、商品名及市场价格……………………………34 第二节:《2004 年国家基本医疗保险和工伤保险药品目录》情况………………………38
第六部份 糖尿病用药研发状况…………………………………………………………… 39 第一节:Ⅱ型糖尿病的非胰岛素治疗………………………………………………………40
3、为何亚洲人易患糖尿病? 为什么包括中国、日本在内的亚洲人容易患糖尿病?国际糖尿病联盟亚太区 后任主席 Yutaka Seino 在本次会议上指出,欧美人长期以狩猎为生体形偏胖, 胰岛分泌功能较好,即使体重增加,达到肥胖的程度,也可能是糖耐量异常(IGT); 而长期以农耕为生的亚洲人,胰岛分泌功能较差,在体重正常时就为 IGT,偏胖 一点就可能成为糖尿病,因此,对于亚洲人而言控制体重尤为重要。 在 2008 年 10 月出版的《柳叶刀中国特刊》上,中国卫生部统计信息中心主 任饶克勤和美国哈佛大学公共卫生学院刘远立博士等人发表论文指出,过去 20 年,中国居民平均每天动物性食品的摄入量由 66g 增加到 160g,其中城市居民 为 110g~215g。1982 年,城市居民每人每天的脂肪摄入量为 68g,2002 年则超 过 90g。动物性脂肪增加非常快。过去 10 年,中国人口的超重率上升 40%,肥胖 症上升 100%。
第三部份 中国糖尿病用药总体市场状况………………………………………………… 15 第一节:历年我国糖尿病用药市场规模及增长率…………………………………………16 第二节:糖尿病用药市场厂家医院市场份额分析…………………………………………19 第三节:糖尿病用药医院市场主要品种市场份额及增长率分析…………………………21
1、全国糖尿病流行病学调查背景 杨文英报告了 2007 年 6 月~2008 年 5 月由中华医学会糖尿病分会发起的全 国糖尿病的流行病学调查,目的是调查我国糖尿病的流行病学情况和特点,并据 此研究如何防治糖尿病。 我国曾在 1980 年、1994 年、1996 年和 2002 年进行过糖尿病的流行病学调 查。按照当时的研究标准,1980 年全国 14 省市 30 万人的流行病学调查结果显 示,糖尿病患病率为 0.67%。1994 年全国 19 省市 21 万人的调查,25~64 岁年 龄段糖尿病的患病率为 2.5%(人口标化率为 2.28%),糖耐量减低 (IGT)为 3.2% (人口标化率为 2.12%)。这一数字与同等发展水平国家的数据相近,比 1980 年 增加了近 3 倍。2002 年全国营养调查同时调查了糖尿病的流行情况。该调查主 要根据空腹血糖诊断 IFG 和糖尿病,空腹血糖较高的部分患者做了口服葡萄糖 耐量(OGTT)试验。在 18 岁以上的人口中,糖尿病患病率为 2.6%,其中城市患 病率为 4.5%,农村为 1.8%(见图 1)。而最近十几年来,由于生活水平的提高,