对乙酰氨基酚的肝毒性:NAC的作用机制EastvoldJS-Paper-3-Acetaminophen
提高对乙酰氨基酚肝毒性的认识

・小专论・提高对乙酰氨基酚肝毒性的认识钱燕 陈成伟作者单位:200235 上海南京军区临床肝病研究中心 对乙酰氨基酚(acetaminophen )又称扑热息痛(paracetam ol ),是广泛用于临床的解热镇痛药。
目前该药是导致美国和欧洲急性肝功能衰竭(A LF )的首要原因。
在正常情况下,绝大多数的对乙酰氨基酚与葡萄糖醛酸和硫酸结合,少部分在细胞色素P4502E1、3A4、1A2和2A6作用下,转化为毒性产物N 2乙酰2对2苯醌胺(NAPQI )。
在服用治疗剂量时所产生的NAPQI 在肝细胞内由谷胱甘肽结合解毒;如服用过量,谷胱甘肽耗竭,NAPQI 便与肝细胞的高分子共价结合导致肝细胞坏死。
由于对乙酰氨基酚是经细胞色素P450酶代谢产生活性代谢物而致肝损害,因而这种非直接作用就显得更加隐蔽,应引起医生和患者的高度重视。
对乙酰氨基酚肝毒性与剂量有关。
其常用剂量小于2g Πd ,成人最大推荐剂量为4g Πd ,若超过该剂量可致肝损害,大于10g Πd 可致A LF 甚至死亡。
在英国,过量服用对乙酰氨基酚的病例常见于蓄意自杀,仅8%与治疗目的有关。
而美国的资料显示,更多的患者是由于未按规定剂量服用,或不了解许多制剂品种都含有对乙酰氨基酚成分,结果造成服用过量。
对乙酰氨基酚的中毒剂量并非固定不变,在很大程度上取决于患者有无饮酒史、营养状况、合并用药情况及有无并发症等诸多因素。
乙醇可诱导产生肝细胞色素P450酶并耗竭谷胱甘肽,使酗酒者对药物的敏感性增高;饥饿、营养不良和体内硒、维生素E 缺乏者对该药的敏感性也增高。
因此,当患者有酗酒史、营养不良、合用肝细胞色素P450诱导药(如乙醇、异烟肼、奥美拉唑和苯巴比妥等)以及具有能增加谷胱甘肽消耗和NAPQI 形成的因素时,即使对乙酰氨基酚水平在安全范围内,也要考虑中毒的可能性。
美国食品药品管理局(FDA )告诫人们尤应警惕的是乙醇,从2003年开始FDA 要求药品生产厂家在药瓶上均标明“酒精警告”。
对乙酰氨基酚与肝损害
对乙酰氨基酚与肝损害2014年1月20日有媒体报道,如果超量服用含有对乙酰氨基酚的感冒药,存在肝损害、肝功能衰竭的风险。
媒体引用美国食品与药物管理局(FDA)近日发出的公告,限制医生对含有对乙酰氨基酚成分感冒药的临床应用。
FDA认为过量服用对乙酰氨基酚将有可能导致严重肝脏损害,甚至导致肝功能衰竭乃至死亡。
对乙酰氨基酚也称之为扑热息痛,是目前临床常用的解热镇痛药。
因其能够有效缓解疼痛和退热,对胃肠道刺激性小,而被广泛应用于感冒的辅助治疗,是治疗感冒及镇痛类药物中最常用的成分,有报道约80%的抗感冒药都含有对乙酰氨基酚。
早在1899年,研究人员就发现对乙酰氨基酚是退热冰(乙酰苯胺)的代谢产物。
乙酰苯胺是磺胺类药物的原料,可用作止痛剂和退热剂,但是大剂量摄入可引起高铁血红蛋白血症等毒副作用。
1948年国外研究人员发现退热冰的止痛、退热治疗作用要归功于其代谢产物对乙酰氨基酚,而对乙酰氨基酚通常没有类似退热冰的毒副作用,研究者提出使用对乙酰氨基酚来替代退热冰。
1955年对乙酰氨基酚在美国上市销售,商品名为泰诺;1956年。
500毫克一片的对乙酰氨基酚在英国上市销售,商品名为必理通。
近年来,涉及对乙酰氨基酚不良反应的报道越来越多,引起人们的广泛关注。
有研究者报道,对乙酰氨基酚所引起的原发性肝细胞毒性,主要是因为在药物的生物转化过程中产生了毒性较大的自由基代谢产物N-乙酰一对一苯醌亚胺(NAPQI)。
在体内还原型谷胱甘肽等保护因子含量充足的情况下,NAPQI与还原型谷胱甘肽结合而起到解毒作用,但是在还原型谷胱甘肽被耗竭时NAPQI会与细胞内其他生物大分子结合,进而导致肝损害发生。
因此,对乙酰氨基酚的肝损害发生与否,与患者服用剂量有关。
有文献报道,一名67岁男性患者,因感冒服用对乙酰氨基酚片(0.5g,3次/日)和复方氨酚烷胺胶囊(含对乙酰氨基酚0.25g,2次/日),共计2天,患者出现恶心、呕吐、上腹疼痛、全身乏力现象;检查患者血清谷丙转氨酶(ALT)217U/L,血清谷草转氨酶(AST)243 U/L;患者经乙酰半胱氨酸注射治疗3天后,复查ALT34U/L、AST29U/L,患者治愈出院。
科学认识感冒药中“对乙酰氨基酚”的肝毒性

一、对乙酰氨基酚相关事件带外,还多与其他药物制成复方制和肌肉痛等。
自我用药不宜长期或来的疑惑剂,常用于治疗感冒咳嗽,如泰大量使用,用于止痛不得超过52011年起,美国食品药品管诺、新康泰克、百服宁、白加黑天,用于退热不得超过3天,理局(FDA)发布信息,由于对乙等,是老百姓日常生活中的“老朋FDA推荐的剂量是每天合计不要超酰氨基酚超剂量使用可能导致严重友”。
而FDA发布的关于对乙酰氨过4 g。
的肝损伤,甚至肝衰竭、肝移植和基酚的相关信息,以及生活中偶有要知道对乙酰氨基酚为何会引死亡,因此建议停止处方和销售含因服用感冒药而引起肝损伤的新起肝毒性,就需要了解它是如何在对乙酰氨基酚超过325 mg的处方闻,使得不少公众担心,我们日常我们体内代谢的。
进入人体的对乙药(不包括非处方药),同时服用的感冒药真的会引起肝损伤酰氨基酚90%~95%通过肝脏代FDA要求所有含对乙酰氨基酚的处吗?感冒药中单剂量含对乙酰氨基谢,其中4%~5%的药物经肝脏细方药说明书中增加黑框警告,提示酚超过325 mg还能否继续使用?胞色素P450氧化酶系统代谢为N-严重肝损伤风险。
2014年美国食使用过程中到底应该注意什么?这乙酰苯亚胺醌(NAPQI),它能品药品管理局(FDA)再次发布信个公众使用最广泛的药物似乎成了迅速与体内谷胱甘肽结合成水溶性无息,当对乙酰氨基酚单位剂量超过“最熟悉的陌生人”!毒化合物由尿排出。
如果大量服用对325 mg时,没有数据显示其额外二、 最熟悉的药物你知多少乙酰氨基酚,则代谢产生的NAPQI不效益大于增加的肝损伤风险,对乙酰氨基酚是使用最广泛的能被有限的谷胱甘肽结合,转而与肝FDA将撤销市场上对乙酰氨基酚单乙酰苯胺类解热镇痛药,解热作用细胞内蛋白的巯基结合,产物可致位含量超过325 mg的复方药物的与镇痛作用与阿司匹林相似,几乎肝细胞损害、坏死,严重者可致肝许可。
不具有抗炎抗风湿作用,对血小板肾衰竭、肝性脑病、脑水肿、低血对乙酰氨基酚作为一种被使用和凝血时间无明显影响。
对乙酰氨基酚及其前体中毒致肝损伤的解救
通 信 作 者 :刘 莹 ,Email:duyanhongzhang@163.com
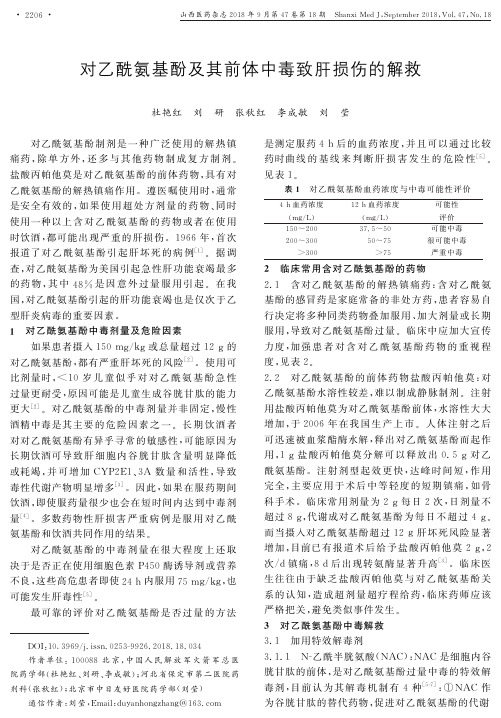
是测定服药4h后的血 药 浓 度,并 且 可 以 通 过 比 较 药时曲 线 的 基 线 来 判 断 肝 损 害 发 生 的 危 险 性 . [5]
完全,主 要 应 用 于 术 后 中 等 轻 度 的 短 期 镇 痛,如 骨
科手术.临床常用剂量为 2g每日 2 次,日剂量不 超过8g,代谢成对 乙 酰 氨 基 酚 为 每 日 不 超 过 4g. 而当摄入对乙酰氨基 酚 超 过 12g肝 坏 死 风 险 显 著 增加,目前已有 报 道 术 后 给 予 盐 酸 丙 帕 他 莫 2g,2 次/d镇痛,8d后 出 现 转 氨 酶 显 著 升 高[3]. 临 床 医
乙酰氨基酚水溶性较差,难以制成静脉制 剂.注 射
用盐酸丙帕他莫为对乙酰氨基酚前体,水溶性 大 大
增加,于2006 年 在 我 国 生 产 上 市. 人 体 注 射 之 后
可迅速被血浆酯酶水解,释出对乙酰氨基酚而 起 作
用,1g 盐 酸 丙 帕 他 莫 分 解 可 以 释 放 出 0.5g 对 乙 酰氨基酚.注 射 剂 型 起 效 更 快,达 峰 时 间 短,作 用
如果患者摄入150mg/kg或总量超过 12g的 对乙酰氨基酚,都有严重 肝 坏 死 的 风 险 . [2] 使 用 可 比剂量时,<10 岁 儿 童 似 乎 对 对 乙 酰 氨 基 酚 急 性 过量更耐受,原因可能是儿童生成谷胱甘肽的能 力 更大[2].对乙酰氨基酚的中 毒 剂 量 并 非 固 定,慢 性 酒精中毒是其主要的危险因素之一.长期饮酒者 对对乙酰氨基酚有异乎寻常的敏感性,可能原因 为 长期饮酒可导致肝细胞内谷胱甘肽含量明显降低 或耗竭,并 可 增 加 CYP2E1、3A 数 量 和 活 性,导 致 毒性代谢产物明显增多 . [3] 因 此,如 果 在 服 药 期 间 饮酒,即使服药量很少也会在短时间内达到中毒 剂 量 . [4] 多数药 物 性 肝 损 害 严 重 病 例 是 服 用 对 乙 酰 氨基酚和饮酒共同作用的结果.
对乙酰氨基酚作用机理是什么

对乙酰氨基酚作用机理是什么
对乙酰氨基酚,通常称为阿司匹林,是一种广泛应用于医疗保健领域的药物。
它有着杀菌、消炎、退热、镇痛等多种作用,被广泛用于治疗发热、头痛、关节炎等疾病。
那么,对乙酰氨基酚产生这些功效的机理是什么呢?
对乙酰氨基酚的生物学作用
对乙酰氨基酚的主要生物学作用是通过抑制体内一种名为“环氧化酶”的酶类。
环氧化酶是一种参与脂质代谢的酶,其中的COX-1和COX-2是最为人熟知的两种亚型。
COX-1主要参与维持体内生理平衡,例如保护胃黏膜、促进胃粘液分泌等;而COX-2则主要参与炎症过程中的前列腺素合成。
退热镇痛的作用机理
对乙酰氨基酚通过抑制环氧化酶,干扰前列腺素的合成,从而减少了炎症过程中相关炎症介质(如PGE2)的生成,降低了炎症刺激所导致的发热和疼痛反应。
抗炎作用的机理
在炎症反应中,受刺激的组织会释放炎症介质,引发局部炎症反应。
对乙酰氨基酚抑制环氧化酶的作用,减少了前列腺素等炎症介质的合成,从而减轻了炎症过程的细胞活性,减轻了组织的炎症反应,达到抗炎效果。
镇痛作用的机理
对乙酰氨基酚的镇痛作用机理也是通过抑制环氧化酶,减少炎症反应时产生的前列腺素等炎症介质。
这些炎症介质会刺激神经末梢,使得疼痛感知增强。
通过减少这些刺激物质的合成和释放,对乙酰氨基酚能够减轻疼痛感知,产生镇痛效果。
结语
综上所述,对乙酰氨基酚的作用机理主要是通过抑制环氧化酶,减少前列腺素等炎症介质的合成和释放,达到退热、镇痛、抗炎等作用。
当人体遇到炎症、疼痛等情况时,对乙酰氨基酚可以帮助减轻症状,提高患者的舒适度。
在使用药物时,应当谨慎遵医嘱使用,避免不当使用带来不良影响。
对乙酰氨基酚的药理作用
对乙酰氨基酚的药理作用发表时间:2012-11-22T09:54:39.733Z 来源:《医药前沿》2012年第23期供稿作者:曲明[导读] 急性呼吸道病毒感染发热38.5℃以下,对于正常背景小儿来说,这一适应性防御反应有利于疾病的康复,不需要用解热药.曲明 (吉林省公主岭市怀德镇中心卫生院吉林公主岭 136121)【摘要】急性呼吸道病毒感染发热38.5℃以下,对于正常背景小儿来说,这一适应性防御反应有利于疾病的康复,不需要用解热药.世界卫生组织仅推荐扑热息痛在儿科临床应用。
对乙酰氨基酚(扑热息痛)以毒性最低、安全、高效快速降热和维持降热时间长为特点.对乙酰氨基酚(扑热息痛)的主要作用是抑制在发热机制中起重要作用的前列腺素的合成。
【关键词】发热药理适应证不良反应【中图分类号】R96 【文献标识码】A 【文章编号】2095-1752(2012)23-0056-02 扑热息痛,中文名:对乙酰氨基酚一.药理作用本品为乙酰苯胺类解热镇痛药。
通过抑制环氧化酶,选择性抑制下丘脑体温调节中枢前列腺素的合成,导致外周血管扩张、出汗而达到解热的作用,其解热作用强度与阿司匹林相似;通过抑制前列腺素等的合成和释放,提高痛阈而起到镇痛作用,属于外周性镇痛药,作用较阿司匹林弱,仅对轻、中度疼痛有效。
本品无明显抗炎作用。
1.药效学本品镇痛作用的机制尚未十分明了,可能是通过抑制中枢神经系统中前列腺素的合成(包括抑制前列腺素合成酶)以及阻断痛觉神经末梢的冲动而产生镇痛,后者可能与抑制前列腺素或其他能使痛觉受体敏感的物质(如5-羟色胺、缓激肽等)的合成有关。
解热作用则可能是通过下视丘体温调节中枢而起作用,可能与下视丘的前列腺素合成受到抑制有关。
2.药动学口服后自胃肠道吸收迅速、完全(在高碳水化合物饮食后服药可能降低吸收),吸收后在体液中分布均匀,约有 25%与血浆蛋白结合。
小量时(血药浓度<60μg/ml)与蛋白结合不明显, 大量或中毒量则结合率较高, 可达43%。
对乙酰氨基酚的药代动力学及其肝毒性的生理节律调控

对乙酰氨基酚过量应用可导致药物性肝病

对乙酰氨基酚过量应用可导致药物性肝病1 讨论药物性肝病发生机制为:通过改变肝细胞膜的物理特性(如粘滞度)和化学特性(如胆固醇/磷脂比),抑制细胞膜上的Na+-K+-ATP酶,干扰肝细胞的摄取过程,破坏细胞骨架功能,在胆汁中形成不可溶性的复合物等途径直接导致损伤,也可选择性破坏细胞成分,与关键分子共价结合,间接的引起肝损伤。
在病理上,药物性肝病主要表现为肝细胞损害。
考虑有两个主要途径:一是药酶的化学反应激活了结构稳定的药物,形成了亲电子的中间代谢产物,这些强大的烷基化、芳基化和酰基化物质与肝细胞内与生命有关的大分子(DNA、RNA)共价结合引起肝细胞坏死;二是由P450氧化产生的自由基,与细胞膜上的蛋白质或非饱和脂肪酸共价结合,产生脂质过氧化物引起细胞膜损伤。
两种途径最终引起该离子Ca++自稳机制的破坏,膜泵衰竭,线粒体功能抑制,细胞骨架破坏,最终导致细胞死亡。
由于肝小叶第3区(Zone3)药酶浓度最高,所以,坏死绝大部分发生在这里[1]。
对乙酰氨基酚(扑热西痛)过量或长期应用,就是通过以上发病机制,主要引起第三区(即小叶)中心性坏死,伴有散在的脂肪变性,但炎症反应少见。
临床表现酷似急性病毒性肝炎,常有发热、乏力、纳差、黄疸和血清转氨酶超过正常2~30倍的升高,ALP和白蛋白受影响较少,高胆红素血症和凝血酶原时间延长与肝损严重程度相关。
2治疗最主要的是停用对乙酰氨基酚(扑热西痛)及其他一切有可能引起药物性肝病的药物,适当休息,加强营养,支持疗法,给予高蛋白高糖富维生素低脂饮食,补充维生素C、B、E。
应用还原型谷胱甘肽,补充体内SH基团,有利于药物的生物转化,增加肝细胞解毒作用和对线粒体保护作用,用法:1.8~2.4g/d静滴4~8周,到症状及生物指标改善。
也可应用N-乙酰半胱氨酸(N-AC),这是半胱氨酸前体,用于补充1.4内谷胱氨肽。
用法:70mg/kg,q4h,po ,共72小时。
熊去氧胆酸(UDCA)有稳定细胞膜,免疫抑制及对线粒体保护作用,用法:150~450mg,tid/qidpo。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
77:222 Spring 2005 Free Radicals in Biology and Medicine Page 0 This student paper was written as an assignment in the graduate courseFree Radicals in Biology and Medicine(77:222, Spring 2005)offered by theFree Radical and Radiation Biology ProgramB-180 Med LabsThe University of IowaIowa City, IA 52242-1181Spring 2005 TermInstructors:GARRY R. BUETTNER, Ph.D.LARRY W. OBERLEY, Ph.D.with guest lectures from:Drs. Freya Q . Schafer, Douglas R. Spitz, and Frederick E. Domann The Fine Print:Because this is a paper written by a beginning student as an assignment, there are no guarantees that everything is absolutely correct and accurate.In view of the possibility of human error or changes in our knowledge due to continued research, neither the author nor The University of Iowa nor any other party who has been involved in the preparation or publication of this work warrants that the information contained herein is in every respect accurate or complete, and they are not responsible for any errors or omissions or for the results obtained from the use of such information. Readers are encouraged to confirm the information contained herein with other sources.All material contained in this paper is copyright of the author, or the owner of the source that the material was taken from. This work is not intended as a threat to the ownership of said copyrights.Acetaminophen Hepatotoxicity:Underlying Mechanisms of Toxicity and the Protective Role of N-acetylcysteineByJoshua S. EastvoldUniversity of Iowa Roy J. and Lucille A. Carver College of MedicineAnatomy and Cell BiologyFor 77:222, Spring 2005March 14, 2005AbbreviationsAPAP N-acetyl-para-aminophenol, acetaminophen, paracetamolAscH−ascorbateGSH glutathioneGSSG glutathione disulfideGST glutathione S-transferaseHRP horseradish peroxidaseMPT mitochondrial permeability transitionNAC N-acetylcysteineN-acetyl-p-benzoquinone imineNAPQINAPSQI N-acetyl-p-benzosemiquinone imine radicalROS reactive oxygen speciesRNS reactive nitrogen speciesTable of Contents ……………………………………………………………….. Page1. Abstract (2)2. Introduction (3)3. Structure and Properties (4)4. Redox Chemistry…………………………...……………………………...……..4-55. Biochemistry…… …..…………………………………………………...…….....5-86. N-acetylcysteine ………...……………………………………………..…………8-97. Summary (9)7. References (10)AbstractAcetaminophen is a widely used analgesic-antipyretic. While it is considerably safe at low doses, it can cause centrilobular hepatic necrosis if taken in high doses. This toxicity is in part mediated by the metabolic activation of acetaminophen to yield reactive metabolites and subsequent depletion of glutathione stores. With the cell’s major antioxidant defense system hindered, covalent modification of vital proteins and oxidative damage ensue. This review will discuss the metabolic pathways of acetaminophen, and the intermediates believed to be involved in its toxicity. Further, the role of N-acetylcysteine (NAC) in the treatment of acetaminophen-induced hepatotoxicity will be discussed.IntroductionSince its clinical introduction in 1950, acetaminophen (N-acetyl-para-aminophenol; APAP; paracetamol) has become a widely used analgesic-antipyretic. Although remarkably safe at therapeutic doses, excessive amounts of APAP cause centrilobular hepatic necrosis and acute renal tubular necrosis [1], which is the leading cause of acute liver failure in the United States [2].Toxicity is thought to occur via two stages: (i) metabolic phase, and (ii) and oxidative phase [11]. The metabolic phase consists of cytochrome P450-mediated oxidation of APAP forming reactive intermediates, such as N-acetyl-p-benzoquinone imine (NAPQI) [6]. Since NAPQI is detoxified by the glutathione (GSH)-glutathione transferase (GST) system, cellular stores of GSH become depleted resulting in impaired detoxification of peroxides and peroxynitrite, and covalent modification of vital thiol-containing proteins [11].The susceptibility to oxidative damage (oxidative phase) is thought to cause mitochondrial permeability transition (MPT), which is an increase in permeability of the inner membrane. This membrane perturbation leads to uncoupling of oxidative phosphorylation, ion dysregulation, and superoxide production, which culminate in cell death [11].Due to the prevalence of APAP-induced acute liver failure, understanding the mechanisms of hepatotoxicity are of utmost clinical importance. This review addresses the metabolic pathways involved in both the normal detoxification, and when these pathways have gone awry resulting in toxicity. Further, the role of N-acetylcysteine (NAC) in the treatment of APAP-induced hepatotoxicity will be discussed.Structure and PropertiesAcetaminophen is white, odorless crystalline powder with a bitter taste.† Its structure and physical properties are depicted in Figure 1. APAP is derived from the interaction of p-aminophenol and an aqueous solution of acetic anhydride. It is soluble in organicsolvents such as methanol and ethanol, but insoluble in water and ether. Maximal UVabsorbance is at 245 nm. Fig. 1 Structure and physical properties ofacetaminophen.Redox ChemistryAcetaminophen can participate in many redox reactions, but only those deemed biologically relevant will be discussed here. Acetaminophen can undergo a one-electron oxidation to yield the APAP phenoxyl radical (N -acetyl-p -benzosemiquinone imine; NAPSQI) and a direct two-electron oxidation to produce N -acetyl-p -benzoquinone imine (NAPQI) Figure 2 [6]. The two-electron oxidation pathway is thought to be the major pathway in vivo , generating the highly reactive intermediate NAPQI.Fig. 2 Oxidation of APAP occurs either through a one-electron or two-electron process. † /pwmirror/pwy/paracetamol/pharmwebpicm.html. Visited 2-25-05.The biological importance of NAPSQI formation is much debated, but several groups have shown that it is formed as an intermediate in the one-electron peroxidase-dependent oxidation of APAP [7, 8]. In the absence of reactive compounds, NAPSQI dismutes rapidly by second-order kinetics with a rate constant of 2.2 x 109 M -1 s -1 [8]. In the presence of glutathione (GSH) or ascorbate (AscH −), NAPSQI is reduced to form the glutathionyl radical or ascorbate radical,respectively, and regenerate APAP (Figure 3) [6]. In the absence of reducing agents (e.g., GSH), two molecules of NAPSQI can polymerize to form APAP dimers (Figure 4) [7].R +Asc •−AscH −Fig. 3 Scheme for the reactions of ascorbate and glutathione with NAPSQ1. AscH −(ascorbate), Asc •− (ascorbate radical), GS • (glutathionyl radical), GSH (glutathione), GSSG(glutathione disulfide), HRP (horseradish peroxidase), R (APAP), R • (NAPSQ1). Adaptedfrom [6]. Fig. 4 The polymerization of NAPSQ1 to form APAP dimers. Adapted from [7].BiochemistryAcetaminophen exhibits its antipyretic-analgesic activity via inhibiting the cyclooxygenase activity of prostaglandin-endoperoxide synthase, which prevents the formation of prostaglandins responsible for inducing fever and pain sensation [13].At therapeutic doses, 90 percent of APAP is metabolized in the liver via the phase IIbiotransformation enzymes (e.g., sulfotransferase and UDP-glucuronosyl transferase) to yield non-toxic water-soluble compounds that are excreted in the urine (Figure 5) [3]. Of the remaining APAP, half is e hepaticcytochrome P450(2E1, 1A2, 3A4and 2A6subfamilie system to yieldthe highl reactive,electrophilicintermediateNAPQI [4]. Under normal conditions, NAPQI is rapidly conjugated with glutathione (GSH) to form no cysteine and mercaptate compounds that are renally excreted [5].With toxic amounts of APAP, the detoxificatio xcreted unchanged in the urine and bile. The remaining APAP is oxidized via the ,s)yntoxic n pathways become saturated and cellularins Fig. 5 Metabolic pathways involved in detoxification and hepatotoxicity. Adapted from [11].stores of GSH become depleted [5]. This leads to the accumulation of NAPQI, which can react with cellular constituents and induce cell damage. Of importance, NAPQI covalently binds prote as an APAP-cysteine adduct, presumably rendering them inactive [9]. NAPQI can also oxidize protein thiol groups to disulfides, forming intra- and interprotein crosslinks and GSH-protein mixed disulfides. These APAP adducts correlate to hepatotoxicity and localize to the centrilobularTable 1 The APAP-adducts formed during hepatotoxicity. a Proteins identified by isolation b etry. Adapted from [11]. necrotic areas. A multitude of host protein adducts have been identified and are summarized Table 1 [10]. This has been characterized as the metabolic phase (or phase 1) of APAP-induced hepatotoxicity. It has been shown that repletion of GSH prevents toxicity [9], and this is the basis of N-acetylcysteine (NAC) treatment (refer to later section).and sequence analysis. Proteins idenitified by mass spectrom inThe depletion of GSH that occurs during the metabolic phase is a critical event for the progression to the oxidative phase, whereby mitochondrial permeability transition (MPT) and cell death ensue. This second stage is less well characterized, and thus will not be discussed in greatFig. 6 The proposed two-staged mechanism of APAP hepatotoxicity. MPT (mitochondrial transition permeability), ROS (reactive oxygenspecies), RNS (reactive nitrogen species).detail. Briefly, the data support the hypothesis proposed by James and Hinson (Figure 6) [11].They propose depleted GSH stores predispose the cell to oxidative stress, since GSH is important in the detoxification of peroxides and peroxynitrite. Increased levels of hydrogen peroxide may initiate oxidative damage via Fenton chemistry. One such damagingevent is the oxidation of critical vicinal thiol groups at the MPT pore, which leads to an increase the inner mitochondrialmembrane permeability. This leads to uncoupling of oxidative phosphorylation and the release of superoxide, which is a lethal event for the cell.N-acetylcysteineN-acetylcysteine is the treatment of choice for patients suffering from APAP toxicity. It functions ains an antidote via providing cysteine substrate for the replenishment of intracellular GSH stores, thus increasing the ability of the cell to detoxify NAPQI [14]. The administration of GSH is ) the d , which relates the time of ingestion to the serum APAP level (ii) not feasible because it is not taken up by cells, whereas nearly 70% of NAC is metabolized by hepatocytes [15]. NAC also exhibits antioxidant properties, which may limit secondary APAP-induced tissue damage [17].The administration of NAC is indicated if any of the following conditions is satisfied: (i serum APAP concentration is above the “possible hepatic toxicity” line according to the modifie Rumack-Matthew nomogram presence of liver tenderness, (iii) elevation of aminotransferases, (iv) serum APAP concentrationsgreater than 20 mg/ml, and (v) susceptible to hepatoxocity (i.e., chronic alcohol use, fasting, or of P450-inducing drugs) [16].If toxicity is suspected, NAC (Mucomyst ®) is given PO (by mouth) or by gastric tube as a 140 mg/kg loading dose followe use d by 17 doses of 70 mg/kg every 4 hours. The initial dose can be rs f the initial serum APAP level. Thus, mortality usually results from a taminophen is a widely used analgesic-antipyretic that can cause centrilobular hepatic necrosis if taken in high doses. This toxicity o phases: (i) the metabolic activation of cetam togiven with activated charcoal with no impairment of its efficacy. If the patient cannot tolerate oral NAC (e.g., intractable vomiting) or if the patient has fulminant hepatic failure, NAC can be given intravenously (IV). The initial dose is 140 mg/kg IV over 1 hour, followed by 70 mg/kg every 4 hours for 48 hours [16].The outcome of APAP is extremely good (no deaths reported) if NAC is given within 10 h of overdose, regardless o delay in seeking medical attention, in recognizing the overdose, or in administering NAC (i.e., > 10 hrs) [16].SummaryAce occurs in tw a inophen to yield reactive metabolites (e.g., NAPQI) and subsequent depletion of glutathione stores (known as the metabolic phase), which progresses to (ii) the oxidative phase, wherebyoxidative damage culminates in cell death. The progression into the potentially lethal “oxidative” phase can be prevented if N-acetylcysteine is promptly administered, largely due to its ability increase intracellular stores of glutathione.JS Eastvold ________________ Acetaminophen_____ 10References1. Davidson, DG, Eastham, WN. (1966) Acute liver necrosis following overdosage of paracetamol. Br Med J . 5512:497.2. Lee WM. (2004) Acetaminophen and the U.S. ilure Study Group: lowering the risks of hepatic . Forre ents JA, Prescott LF. (1982) Clinical pharmacokinetics of paracetamol. Clin Pharmacokinet . 4) N-acetyl-p-benzoquinone imine: A cytochrome P-450-. Mitch DJ, Potter WZ. (1973) Acetaminophen-induced hepatic necrosis: Protective role of . Rama f the acetaminophen -p-benzoquinone imine with reduced glutathione, . Bisby ne-electron oxidation of acetaminophen-- Biochem Pharmacol 37(14):. Jollow B. (1973) Acetaminophen-induced hepatic 0. Hins phen-induced hepatotoxicity: Role of tentiation in the intact rat of the hepatotoxicity of acetaminophen byArch Biochem Biophys 267: ynska-Cedro K, Vane JR. (1972) Effects of anti-inflammatory drugs on u Rev Pharmacol Toxicol . ne and ambroxol in6. Goo 01) Medical emergencies. In Ahya SN, Flood K, Paranjothi S, ed. The Washington th ms & Wilkins; pp 548-7. Jones AL. (1998) Mechanism of action and value of N-acetylcysteine in the treatment of early and late acetaminophen poisoning: a critical review. J Toxicol Clin Toxicol 36(4): 277-85. Acute Liver Fa failure. Hepatology. 40(1): 6-9.st JA, Clem 3 7(2):93-107. Dahlin DC, Miwa GT, Lu AY, Nelson SD. (1984 mediated oxidation product of acetaminophen. Proc Nati Acad Sci. 81: 1327-1331.ell JR, Jollow 5 glutathione. J Pharmacol Exp Ther . 187: 211.krishna Rao DN, Fischer V, Mason RP. (1990) Glutathione and ascorbate reduction o 6 radical formed by peroxidase. J Biol Chem . 265(2): 844-847.. Potter DW, Hinson JA. (1986) Reactions of N-acetyl 7 acetaminophen, and NADPH. Mol Pharmacol. 30(1): 33-41.RH, Tabassum N. (1988) Properties of the radicals formed by o 8 a pulse radiolysis study.. 2731-8.DJ, Mitchell JR, Potter WZ, Davis DC, Gillette JR, Brodie B 9 necrosis: Role of covalent binding in vivo. J Pharmacol Exp Ther . 187: 195–202.on JA, Reid AB, McCullough SS, James LP. (2004) Acetamino 1 metabolic activation, reactive oxygen/nitrogen species, and mitochondrial permbeability transition. Drug Metabolism Reviews . 36: 805-822.11. James LP, Mayeux PR, Hinson JA. (2003) Acetaminophen-induced hepatotxicity. Drug Metabolism and Disposition . 31: 1499-1506.2. Nakae D, Oakes JW, Farber JL. (1988) Po 1 1,3-bis(2-chloroethyl)-1-nitrosourea.. 651-659.3. Flower R, Gryglewski R, Herbacz 1 prostaglandin biosynthesis. Nat New Biol . 238(82): 104-6.4. Prescott LF, Critchley JA (1983) The treatment of acetaminophen poisoning. Ann 1 23: 87-101.5. Gillissen A, Nowak D. (1998) Characterization of N-acetylcystei 1 antioxidant therapy. Resp Med. 92: 609-623.denberger D. (201 manual of medical therapeutics, 30 edition . Philadelphia, PA: Lippincott Willia 552.1。