LOCS III 白内障分级 权威
白内障分级标准locs

白内障分级标准locs
白内障分级标准通常使用的是Lens Opacities Classification System III (LOCS III)。
这个分类系统是根据白内障患者的晶状体浑浊程度来进行分级的。
根据LOCS III,白内障分为浑浊度分级(NUC)和颜色分级(CO)两个部分。
浑浊度分级(NUC)包括以下五个等级:
1. N0:无浑浊
2. N1:非致命性轻度浑浊
3. N2:轻度浑浊
4. N3:重度浑浊
5. NC:中央区域完全浑浊
颜色分级(CO)包括以下五个等级:
1. C1:无颜色
2. C2:非致命性轻度颜色
3. C3:轻度颜色
4. C4:重度颜色
5. CO:中央区域完全有颜色
通过将浑浊度分级和颜色分级相结合,可以对白内障进行更详细的分级。
比如,N1C2表示非致命性轻度浑浊和轻度颜色。
这些分级标准可以帮助医生评估白内障的程度以及选择适当的治疗方案。
白内障cnp分级标准

白内障cnp分级标准白内障CNP分级标准。
白内障是一种常见的眼部疾病,通常会导致患者视力模糊甚至失明。
白内障的分级标准对于临床诊断和治疗非常重要。
CNP(中国白内障研究中心)制定了一套白内障分级标准,以帮助医生准确评估患者的病情并制定相应的治疗方案。
本文将详细介绍白内障CNP分级标准的内容,以便广大医生和患者了解和应用。
一、分级标准概述。
CNP的白内障分级标准主要包括了白内障的类型、分级以及治疗建议。
其中,白内障的类型包括了成熟白内障、不成熟白内障、白内障性青光眼等。
分级则根据白内障的密度、大小、位置等因素进行评估,分为轻、中、重三个级别。
治疗建议则根据分级结果提供了相应的手术和药物治疗建议。
二、分级标准详解。
1. 轻度白内障。
轻度白内障通常表现为晶状体轻微混浊,对患者视力影响不大。
在CNP分级标准中,轻度白内障主要是指晶状体轻微混浊,但未影响患者正常生活和工作。
治疗建议可以采用药物治疗,如使用抗氧化剂和营养素来延缓白内障的进展。
2. 中度白内障。
中度白内障的晶状体混浊程度较重,患者视力已经受到一定影响,但仍能够完成日常生活和工作。
在CNP分级标准中,中度白内障需要考虑手术治疗的可能性,尤其是对于那些视力受到较大影响的患者。
3. 重度白内障。
重度白内障是指晶状体混浊程度严重,患者视力已经严重受损,甚至出现失明的危险。
在CNP分级标准中,重度白内障需要紧急进行手术治疗,以恢复患者的视力并避免进一步的并发症发生。
三、分级标准的意义。
白内障CNP分级标准的制定对于临床诊断和治疗具有重要意义。
首先,它可以帮助医生准确评估患者的病情,为患者制定个性化的治疗方案提供了重要依据。
其次,分级标准还可以帮助患者了解自己的病情,及时就医并接受相应的治疗,避免病情恶化。
最后,分级标准还可以为科研提供重要数据支持,促进白内障治疗技术的进步和创新。
四、结语。
白内障CNP分级标准的制定和应用对于白内障患者的治疗具有重要意义。
白内障cnp分级标准图

白内障cnp分级标准图白内障(Cataract)是一种常见的眼部疾病,是指眼睛的晶状体透明度下降,导致视力模糊。
白内障是一种老年性眼病,也可以发生在儿童或年轻人身上。
在临床上,为了更好地评估白内障的严重程度,医生们通常会采用CNP分级标准图进行评估。
CNP分级标准图是一种用于评估白内障严重程度的图表,通过观察患者眼睛的晶状体混浊程度,可以将白内障分为不同的级别。
这种分级标准图通常包括了一系列不同程度的晶状体混浊图片,医生们可以根据患者眼睛的实际情况,将其与标准图进行比对,从而确定白内障的分级。
在CNP分级标准图中,通常会包括5个不同级别的白内障图片,分别是轻度、中度、重度、严重和极重度。
通过观察这些图片,医生们可以更准确地判断患者的白内障病情,为患者制定更合理的治疗方案提供参考。
轻度白内障的图片通常表现为晶状体轻微混浊,患者视力可能略有下降,但日常生活不受太大影响。
中度白内障的图片显示晶状体混浊程度加重,患者视力明显下降,可能出现眩晕、视物模糊等症状。
重度、严重和极重度白内障的图片则呈现出晶状体混浊程度不同程度的加重,患者视力急剧下降,严重影响日常生活和工作。
通过CNP分级标准图,医生们可以更准确地了解患者的白内障病情,为患者制定个性化的治疗方案提供重要参考。
对于轻度白内障患者,可以通过药物治疗、营养调理等方法延缓病情发展;对于中度和重度白内障患者,通常需要进行手术治疗,通过人工晶状体植入等方式恢复视力;对于严重和极重度白内障患者,需要及时进行手术治疗,以避免病情进一步加重。
总之,CNP分级标准图在评估白内障严重程度方面起着至关重要的作用,可以帮助医生们更准确地判断患者的病情,为患者制定个性化的治疗方案提供重要参考。
希望广大患者能够及时关注自身眼部健康,定期进行眼部检查,及时发现并治疗白内障,保障自己的视力健康。
晶状体功能失调指数与视力、晶状体混浊程度相关性分析
-328-中国中医眼科杂志2020年5月第30卷第5期•论著:临床研究•晶状体功能失调指数与视力、晶状体混浊程度相关性分析路露,杨立东,王颜[摘要]目的探究晶状体功能失调指数(DLI)与年龄相关性白内障患者LogMAR视力、晶状体混浊程度分级系统皿(LOCS!)分级评分的相关性。
方法纳入年龄相关性白内障患者48例(96只眼)组成白内障组&另随机选取同期就诊于沧州眼科医院的同年龄段健康体检者40例(80只眼)组成健康组。
观察指标有LogMAR视力,晶状体混浊程度(LOCS!分级体系判断并评分),晶状体功能失调指数DLI值(采用iTrace视功能分析仪测量)。
结果(1)白内障组患者LogMAR视力(仁23.326,"=0.000)、LOC!分级晶状体核的混浊程度(NO)评分(t=32.427,"=0.000)、LOC!分级晶状体核的颜色(NC)评分(t=27.987,"=0.000)均高于健康组,均有统计学意义;白内障组DLI值低于健康组(t=32.453,"=0.000),差异有统计学意义;(2)年龄相关性白内障患者DLI与LogMAR视力(#=-0.626,"=0.000)、L0CS!-N0评分($=-0.516,%=0.000)、L0CS!-NC评分($=-0.495,"=0.000)均呈负相关;LogMAR视力(t=6.834,"=0.005)、LOCS皿-NO评分(t=7.002,"=0.004)、L0CS!-NC评分(t=6.491,"=0.006)是年龄相关性白内障患者DLI值的密切相关因素;DLI对年龄相关性白内障患者诊断的曲线下面积(AUC)为0.857。
结论年龄相关性白内障患者DLI与LogMAR视力、LOCS!分级评分呈负相关,DLI对年龄相关性白内障有诊断价值,值得临床筛选鉴。
[关键词]年龄相关性白内障;晶状体功能失调指数;LogMAR视力:晶状体混浊程度分级系统!中图分类号:R776.1文献标识码:A7章编号:1002-4379(2020)05-0328-05Analysis of correlations between lens dysfunction index and LogMAR Visual Acuityand LOCS III grading criteria in age-related cataract patients LU Lu,YANG Lidong,WANGYan.Cangzhou Ophthalmological Hospital,Cangzhou061000,China[Abstract]OBJECTIVE To explore the correlation between the lens dysfunction index(DLI)with the LogMAR vision and lens opacities classification system(LOCS III)in age-related cataractpatients.METHODS96eyes of48age-related cataract patients who met the inclusion criteriawere selected as the study group.In addition,40age-matched healthy people(80eyes)who wereadmitted to Cangzhou Ophthalmological Hospital were randomly selected as the control group.TheLogMAR vision was examined in both groups,according to LOCS III classification system,the degree of lens opacity was judged and scored.The DLI value was measured by iTrace visual functionanalyzer.RESULTS(1)LogMAR visual acuity(t=23.326,%=0.000),LOCS H-NO scores(t=32.427,P=0.000)and LOCS!-NC scores(t=27.987,%=0.000)in the research group were significantlyhigher than those in the control group;the DLI scores of the research group were significantly lowerthan that of the control group(t=32.453,P=0.000);(2)The DLI in age-related cataract patients wasnegatively correlated with LogMAR visual acuity(厂=-0.626,P=0.000),LOCS III-NO scores($=-0516,DOI:10.13444/ki.zgzyykzz.2020.05.006作者单位:河北省沧州眼科医院,沧州061000通讯作者:路露,E-mail: ****************P=0.000)and LOCS III-NC scores(r=-0.495,P=0.000) in age-related cataract patients;(3)LogMAR visual acuity(t=6.834,P=0.005),LOCS III-NO scores(t= 7.002,P=0.004)and LOCS III-NC scores(t=6.491,P =中国中医眼科杂志2020年5月第30卷第5期・329・0.006)were closely related factors of DLI in age-related cataract patients.(4)The diagnostic AUCof DLI for age-related cataract patients was0.857.CONCLUSION The DLI is negatively correlated with LogMAR visual acuity and LOCS III grading scores in age-related cataract patients,DLIhas diagnostic value for senile cataract and is worthy promoting in clinical screening.[Keywords]age related cataract;lens dysfunction index;LogMAR vision;LOCS III gradingscores白内障是以晶状体透明度下降为特征的眼科常见疾病,也是世界范围内首位致盲性眼病叫2010年研究报道全球有9400万人视力受损,白内障患者占1/3,2000万人因白内障而失明,占比过半叫在我国,白内障患者约为1100万例,且以每年80万例的速度迅速增加[3]o随着我国人口老龄化的加剧,年龄相关性白内障导致的社会负担日益加重,为当前我国的叫年龄相关性白内障晶状体混浊程度评价方法主要为主观分。
白内障cnp分级标准
白内障cnp分级标准白内障(Cataract)是一种常见的眼部疾病,随着人口老龄化趋势的加剧,白内障患病率也逐渐上升。
为了更科学地评估和分级白内障的严重程度,临床上制定了一套白内障CNP分级标准,以指导医生进行治疗和管理。
本文将对白内障CNP 分级标准进行详细介绍,帮助医生和患者更好地了解这一标准。
白内障CNP分级标准是根据白内障的临床特征和病变程度,将白内障分为不同的级别,以便于医生进行诊断和治疗。
根据国内外多项研究和实践经验,白内障CNP分级标准主要包括以下几个方面:1. 白内障类型,根据白内障的类型,可以将其分为老年性白内障、儿童性白内障、创伤性白内障等。
不同类型的白内障在临床表现和治疗方面有所差异,因此对于不同类型的白内障,医生需要采取相应的治疗措施。
2. 白内障密度,白内障的密度是评估白内障严重程度的重要指标之一。
根据白内障的密度,可以将其分为轻度、中度和重度白内障。
轻度白内障一般不会对患者的视力产生明显影响,而重度白内障则会导致患者严重的视力损失。
3. 白内障核分级,白内障核分级是根据白内障核的混浊程度进行评估的,主要分为1~5级。
其中1级表示白内障核较为清晰,5级表示白内障核非常混浊。
通过核分级,医生可以更准确地判断白内障的严重程度,为手术治疗提供参考依据。
4. 白内障晶状体混浊程度,晶状体混浊程度是评估白内障严重程度的重要指标之一,通常分为轻度、中度和重度。
晶状体混浊程度的增加会导致患者视力逐渐下降,严重影响日常生活和工作。
5. 白内障对比敏感度(CST),CST是一种评估白内障严重程度的客观指标,通过对比敏感度检测,可以更准确地了解白内障患者的视觉功能状态,为手术治疗提供重要参考。
总的来说,白内障CNP分级标准是一套科学严谨的评估体系,可以帮助医生更准确地评估和分级白内障的严重程度,为患者提供个性化的治疗方案。
同时,患者在了解自身白内障情况时,也可以更清晰地了解自己的病情,积极配合医生的治疗和管理。
1990年眼科学
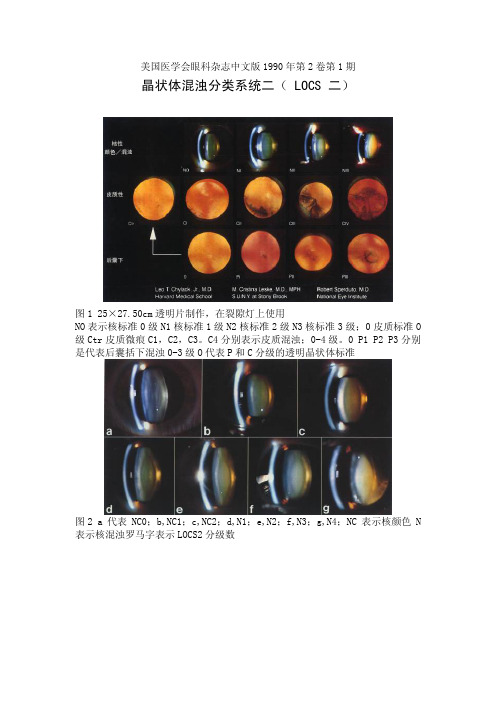
美国医学会眼科杂志中文版1990年第2卷第1期晶状体混浊分类系统二( LOCS 二)图1 25×27.50cm透明片制作,在裂隙灯上使用NO表示核标准0级N1核标准1级N2核标准2级N3核标准3级;0皮质标准O 级Ctr皮质微痕C1,C2,C3。
C4分别表示皮质混浊;0-4级。
0 P1 P2 P3分别是代表后囊括下混浊0-3级O代表P和C分级的透明晶状体标准图2 a代表NC0;b,NC1;c,NC2;d,N1;e,N2;f,N3;g,N4;NC表示核颜色N 表示核混浊罗马字表示LOCS2分级数图3 a表示Ctr;b,C1;c,C2;d,C3;e,C4;f,C5;g,Pi;h,P2;I,P3;j,P4;C代表皮质P代表囊膜下Arch Ophthalmol 1989;107∶991~997美国医学会眼科杂志中文版1990年第2卷第1期:3~10白血病的眼部表现图1 白血病性浸潤,一团白细胞遮挡下血管弓图2 更大的团块显著地遮挡下血管弓图3 伴有严重贫血及血小板减少的急性髓性白血病患者发生双侧下睑血肿提示可能同时有眶内出血图4 患者昏迷视力一定有减退,可能为视盘旁视网膜下出血,有小片视网膜内出血及黄斑部视网膜前出血 图 5伴有明显高粘血症患者的右眼底轻度视网膜中央静脉阻塞,左眼底也是有同样表现Arch Ophthalmol 1989;107∶697~700美国医学会眼科杂志中文版1990年第2卷第1期:22~25眶内容剜出术并发脑脊液漏图1 眶内容剜出术中脑脊液漏(箭头)图2 左,干头颅,注意静脉板障(箭头)右,干头颅,双侧眼眶衰老性缺损(箭头)国3 实验模型 右侧眼底大量荧光倾倒于颅前窝。
T示碟骨鞍结节,f示大脑镰图4 实验模型 右眼眶b示暗斑点,最大烧灼区末显示渗漏,荧光素仅出现在医源性缺损区(箭头)示眶尖Arch Ophthalmol 1989;107∶827~830美国医学会眼科杂志中文版1990年第2卷第1期:26~29视网膜巨大破孔图1 用 PFO 液将巨大裂孔复位。
晶状体核硬度分级标准

晶状体核硬度分级标准
晶状体核硬度分级标准是基于晶状体核的硬度程度来划分的,一般分为四级,具体如下:
1. 一级硬度:晶状体核很软,可以被轻易切割和吸出。
2. 二级硬度:晶状体核柔软,但需要适当的力量才能切割和吸出。
3. 三级硬度:晶状体核相对坚硬,需要比较强的力量才能切割和吸出。
4. 四级硬度:晶状体核非常坚硬,需要非常大的力量才能切割和吸出,有时需要使用额外的工具。
硬度分级标准通常由医生根据患者的情况进行评估和确定。
在晶体诱发性白内障手术中,硬度分级对手术的难易程度和治疗效果具有重要影响。
白内障(2)
〖病因〗 病因〗
白内障囊外摘除术后或晶状 体外伤后,残留皮质及脱落在晶 体外伤后, 状体后囊上的上皮细胞增生形成 膜状混浊 。
〖临床表现〗 临床表现〗
⑴ 手术或外伤史 ⑵ 后囊膜混浊机化。 后囊膜混浊机化。
〖治疗〗 治疗〗
薄者:YAG激光 ⑴ 薄者:YAG激光 ⑵ 厚者:手术 厚者:
视网膜母细胞瘤
思考题
1.白内障的定义和分类? 2.年龄相关性白内障的病因与分类? 3.皮质性白内障的分期和处理原则? 4.先天性白内障的病因、常见类型和治疗原则? 5.常见的代谢性白内障有哪几种? 6.白内障人工晶体植入术的手术适应症、术前 检查? 7.晶状体异位和脱位的病因与治疗原则?
再 见
〖临床表现〗 临床表现〗 有原发病改变。 ⑴ 有原发病改变。 晶状体后囊膜、 ⑵ 晶状体后囊膜、后囊下 皮质混浊,发展至全混浊。 皮质混浊,发展至全混浊。
〖治疗〗 治疗〗
⑴ 治疗原发病 ⑵ 手术治疗
五、代谢性白内障
糖尿病性白内障
〖病因〗 病因〗 由于糖代谢障碍引起。
〖临床表现〗 临床表现〗
1.发生于老年者: 发生于老年者: 与老年性白内障相似,发展快。 与老年性白内障相似,发展快。
——囊膜 ——溶解的皮质 ——晶体核
③可引起晶状体过敏性葡萄膜炎 或晶状体溶解性青光眼。 或晶状体溶解性青光眼。 视力:可略有增进。 ④视力:可略有增进。
晶状体溶解性青光眼
(二)核性白内障
①核混浊,呈深黄或棕黑色。 核混浊,呈深黄或棕黑色。 早期晶状体周边部较透明。 ②早期晶状体周边部较透明。 老视减轻,近视增加。 ③老视减轻,近视增加。 发展缓慢。 ④发展缓慢。
〖鉴别诊断〗 鉴别诊断〗
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Clinical application of the Lens Opacities Classification System III in the performance of phacoemulsificationJames A.Davison,MD,Leo T.Chylack Jr.,MDPurpose:To report the correlation of features of cataracts graded by the Lens Opacities Classification System,version III (LOCS III),with phacoemulsification energy expenditure and the balanced salt solution (BSS ®)volume used during cataract surgery.Setting:Wolfe Clinic,Marshalltown,Iowa,USA.Methods:This was a retrospective review of 2364cases operated on by a single surgeon from January 1998to July 2000in which the cataract had been graded at the slitlamp using the 4grading scales of the LOCS III:nuclear opalescence (NO),nuclear color (NC),cortical cataract (C),and posterior subcapsular cataract (P).Polynomial best-fit lines were derived using regression analysis correlating the 4preoperative LOCS III characteristics with 3intraoperative observations:ma-chine-measured phacoemulsification time,mean power expenditure,and BSS volume.Results:As determined by best-fit lines and their coefficient of determination (R 2),there were exponential relationships between machine-measured phaco-emulsification time and the degree of NC (R 2ϭ0.48)and NO (R 2ϭ0.40).Trends existed between NC and NO and the amount of BSS used (R 2ϭ0.08and R 2ϭ0.07,respectively).No relationships were observed between the LOCS III classes of cataract,C and P,at any intraoperative observation.Conclusions:Exponentially,greater phacoemulsification energy was required as NC and NO increased.The LOCS III cataract grading system enhanced the ability to estimate ultrasonic energy expenditure and BSS volume use during phaco-emulsification.Preoperative LOCS III cataract classification can help to create a more formally organized,integrated,customized operative plan.J Cataract Refract Surg 2003;29:138–145©2003ASCRS and ESCRSThe LensOpacitiesClassification System,versionIII (LOCSIII),isa widelyused,scientificallyvalid,standardizedphotographic comparisonsystemfor grad-ingthe featuresof thehuman age-relatedcataract.1–5It hasbeen used to grade the type and severity of cataract incross-sectional studies and the progression of cataract in longitudinal studies.It also has been used to grade cata-racts at the slitlamp.3Grading using LOCS III involves the assessment of 4features shown on 3sets of photographs on an 8.5-inch ϫ11-inch color transparency (Figure 1).The features of nuclear opacification and brunescence are graded according to 1set of 6photographs.The bright-ness of scatter from the nuclear region has been desig-nated nuclear opalescence (NO)and the intensity of brunescence,nuclear color (NC).The amount of corti-cal cataract (C)is determined by comparing the esti-mated aggregate of cortical spoking to that seen inAccepted for publication September 12,2002.From the Wolfe Clinic,Marshalltown,Iowa,USA.Presented at the Symposium on Cataract,IOL and Refractive Surgery,San Diego,California,USA,April 2001Reprint requests to James A.Davison,MD Wolfe Clinic,309East Church Street,Marshalltown,Iowa,USA.©2003ASCRS and ESCRS0886-3350/03/$–see front matter Published by Elsevier Science Inc.doi:10.1016/S0886-3350(02)01839-45separate photographs.Similarly,the estimated amountof posterior subcapsular cataract(P)is determined by comparing it to another5photographs depicting in-creasing amounts of posterior subcapsular cataract.The grade for each feature is derived by locating the image of the patient’s lens on the scale of severity for each feature represented in the color transparency.The NC and NO are graded on a decimal scale of0.1to6.9. The severity of C and P are graded on a decimal scale of 0.1to5.9.The final LOCS III grade comprises4deci-mal values,1each for NO,NC,C,and P.In the original publication describing the LOCS III system,1an assessment of within-grader and between-grader reproducibility was done and expressed as a“95% confidence interval”for each scale.On average,these 95%confidence intervals were approximately0.7units. The intervals were used to define a significant change in the severity of the cataract.For example,if the NO grade was2.3at baseline and1year later it was3.5,the increase in severity(3.5–2.3ϭ1.2)was greater than the95% confidence interval(0.7)and it was therefore reasonable to conclude that one was95%confident that the change was statistically significant.If the increase had been only 0.5units,the increase could more likely be the result of the intrinsic methodologic noise of the LOCS III system and not a true increase in the severity of the cataract.Since1998,LOCS III has been used systematically in the clinical practice of one author(J.A.D.).Preoper-ative LOCS III grading of all surgical patients was done at the slitlamp to improve clinical documentation in the clinical record.Parenthetical descriptions were rarely added but usually included the critical nature of the centrality within the visual axis of subtle localized inter-faced zones of NO and NC,cortical spokes,or subcap-sular opacities.There was consistency in grading over time,and patients could be told with greater confidence whether their cataracts were stable or progressing.It was also helpful to have accurate measures of cataract severity when discussing cases with third-party payer representa-tives;surgical interventional decisions to offer surgery to some patients could be better defended.Over time,LOCS III slitlamp grading was empiri-cally incorporated into the decision-making process and planning of upcoming surgeries.Ultimately,this re-sulted in a more organized,integrated,customized op-erative plan for each patient.Patients and MethodsIn this retrospective study,2364consecutive cases of phacoemulsification were analyzed with respect to the 4LOCS III characteristics and machine-measured phaco-emulsification time,average machine measured power(%), and the balanced salt solution(BSS)volume used.All data points had been recorded in2186cases.Surgery was per-formed from January1998to July2000by a single surgeon (J.A.D),who also performed LOCS III grading of all cataracts at the slitlamp.A standardized nuclear-fracture quadrant-aspiration phacoemulsification technique was used with a straight 45-degree0.9mm ABS MicroTip with the Alcon Legacy 20,000machine.6After topical anesthesia was administered,a temporal clear corneal incision was made.Grooving was ac-complished with the machine in memory I(phacoemulsifica-Figure1.(Davison)The LOCS III standard images in an8.5-inchϫ11-inch color transparency as used in the office at the slitlamp.The top row contains the standards for NO and NC.The second row contains the standards for grading C and the bottom row,for grading P.J CATARACT REFRACT SURG—VOL29,JANUARY2003139tion power maximum,90%;vacuum maximum,50mm Hg;aspiration flow rate,14cc/minute)(Figure 2).Wider,deeper grooves were made as nuclear hardness increased.The pos-terior nuclear plate was torn from the periphery toward the center by cross action with the phacoemulsification tip and a custom,modified,0.37mm cyclodialysis spatula (Figure 3).Quadrant aspiration was accomplished in memory III (phaco-emulsification power maximum,70%;vacuum maximum,500ϩmm Hg;aspiration flow rate,35cc/minute).The aspiration process was kept posterior to the iris plane within the capsular bag as much as possible to protect thecorneal endothelium from damage from fragment impact and abrasion (Figures 4to 6).Sodium hyaluronate 3.0%–chon-droitin sulfate 4.0%(Viscoat )was usually injected into the anterior chamber before quadrant aspiration when the NC was greater than 4.5.In some cases,Viscoat was reinjected before aspiration of the fourth quadrant because of the ten-dency of the capsular bag to flatten after the third quadrant had been removed,which forces the remaining process ante-rior to the iris plane.In some eyes,soft quadrants or the last fragment of the fourth firm quadrant were removed using reduced vacuum (maximum 300mm Hg),maximumpowerFigure 2.(Davison)After initial grooving is completed,a secondrotation of the nucleus allows for improved visualization while deeper grooving progresses in hardnuclei.Figure 3.(Davison)Nuclear cracking is created from the peripherytoward the center with a cross action of the phacoemulsi fication tip and the cyclodialysisspatula.Figure 4.(Davison)The 45-degree phacoemulsi fication tip isturned sideways with its aperture facing the interior wall of the first nuclear quadrant.Low levels of emulsi fication energy are used to engage and impale the central portion of thequadrant.Figure 5.(Davison)A low level of ultrasonic energy and a higherlevel of vacuum allow the tip to adhere to the softer edge of the quadrant and drag it centrally.J CATARACT REFRACT SURG —VOL 29,JANUARY 2003140(50%),and a reduced aspiration flow rate (25cc/minute)(Figures 7and 8).Polynomial best-fit lines were derived by regression anal-ysis among the 4LOCS III characteristics and the 3phaco-emulsification observations.ResultsThe mean machine-measured phacoemulsification time increased as the NO and NC grades increased (Table 1).As determined by the best-fit lines and their coefficients of determination (R 2),there was an expo-nential relationship between NO and machine-mea-sured phacoemulsification time (R 2ϭ0.40).A trend existed between NO and the mean power (R 2ϭ0.15)and the amount of BSS used (R 2ϭ0.07)(Figure 9).A slightly stronger exponential relationship existed between NC and machine-measured phacoemulsifica-tion time (R 2ϭ0.48).A trend also existed between NC and mean power (R 2ϭ0.18)and the amount of BSS used (R 2ϭ0.08)(Figure 10).No relationships were observed between the LOCS III classes of cataract,C and P,and any intraoperative observation (Figures 11and 12).DiscussionIn the original LOCS III publication,the NO and NC scales were highly correlated with each other and the relationships between objective measures of NO,NC,and the LOCS III grade of the standard imageswereFigure 6.(Davison)The bulk of the quadrant is central while mod-erate ultrasonic energy,vacuum,and aspiration flow are used to remove the firm portions of thequadrant.Figure 7.(Davison)Aspiration can begin after an edge of the lastquadrant is lifted free of the posteriorcapsule.Figure 8.(Davison)The cyclodialysis spatula protects the poste-rior capsule as phacoemulsi fication power is applied during removal of the last quadrant.Lower levels of vacuum and aspiration flow rate help protect the posterior capsule from inadvertent aspiration.Table 1.Mean machine-measured ultrasound time(minutes).J CATARACT REFRACT SURG —VOL 29,JANUARY 2003141Figure9.(Davison)A significant relationship is seen betweenLOCS III NO and ultrasound time but not mean ultrasound power andBSS volume used.Figure10.(Davison)A significant relationship is seen betweenLOCS III NC and ultrasound time but not mean ultrasound power andBSS volume used.142J CATARACT REFRACT SURG—VOL29,JANUARY2003Figure11.(Davison)No relationship is seen between LOCS III Cand ultrasound time,mean ultrasound power,and BSS volume used.Figure12.(Davison)No relationship is seen between LOCS III Pand ultrasound time,mean ultrasound power,and BSS volume used. J CATARACT REFRACT SURG—VOL29,JANUARY2003143nearly linear.The NO was assessed independently with image analysis of optical density,and NC was assessed independently with fast spectral scanning colorimetry of each LOCS III standardized image.Highly different grades of NO and NC in the same cataract were un-likely.Similarly,the relationship between the expendi-ture of phacoemulsification energy and the LOCS III grades of NO and NC appears to be linear for LOCS III grades below approximately3.7.Above that,the rela-tionship between LOCS III grade and phacoemulsifica-tion energy expenditure seems to become exponential. Although in LOCS III NO and NC are graded sepa-rately,most clinicians are accustomed to describing nu-clear change by a single term,nuclear sclerosis.Both color change and increased light scattering are part of the pro-cess of nuclear sclerosis,and it is therefore not surprising to have found that both NO and NC are similarly pos-itively correlated with ultrasonic energy exposure.When viewing a cataractous lens with LOCS III NO and NC grades of4.0to5.0,most surgeons intu-itively anticipate increased phacoemulsification times. The nucleus is simply harder,so it will take more energy to emulsify.The LOCS III NC grade has been corre-lated with hardness of the central nucleus as measured by the resistance to a fine conical probe measured by a dynamometer.7Phacoemulsification energy recorded by cumulative delivered energy as well as by postopera-tive anterior chamber flare has been shown to be corre-lated with LOCS III NC and NO.8The surgeon in this study finds it useful to be able to accurately grade opalescence and brunescence(and the severity of C and P)to better estimate when prolonged ultrasonic time or increased ultrasonic energy is likely.It has proved advantageous to integrate LOCS III grading into routine operative planning.By doing so,the sur-geon will be better prepared to manage the more scle-rotic nucleus and his or her preoperative planning can be more patient specific.The surgeon in this study empirically formulated several recommendations for customizing a surgical plan using preoperative LOCS III grading as a part of a com-plete preoperative ophthalmic examination.These are listed below.1.A retentive viscoelastic material is recommended in cases in which the LOCS III NO or NC grade is4.0 or greater.2.If the LOCS III NO or NC grade is5.0,the capsulorhexis will be more easily visualized if indocya-nine green dye is used to stain the anterior capsule.3.If the pupil is smaller than4.5mm and the LOCS III NO or NC grade is greater than4.5,use of a pupil expansion/maintenance device should be considered.4.If zonular integrity is compromised and the LOCS III NO or NC grade is4.5or greater,a backup ciliary-sulcus-supported intraocular lens(IOL)or ante-rior chamber IOL should be available.5.Surgeons in training should learn and use LOCS III grading to enable them to select“normal”cases with nuclei of enough substance to easily manipulate yet readily emulsify.Very soft or very hard nuclei may present unnecessary challenges.6.The LOCS III is helpful and should be used in the trials of new technologies for cataract removal.For ex-ample,in one author’s experience(J.A.D.)with early AquaLase technology(Alcon Surgical),efficient removal of a nucleus with an NC grade greater than3.7was not possible.Of course,the relationships between LOCS III characteristics and phacoemulsification energy expendi-ture vary with the individual technique and equipment used.Despite this individual-specific variation,it is likely that the trends observed will be seen with other surgeons as long as a mechanical removal technique is used.Incorporating LOCS III grading into a preopera-tive regimen should not only improve surgical planning, it should also improve clinical documentation,commu-nication among providers and with third-party payers, and the accuracy of longitudinal follow-up.Most im-portant,preoperative LOCS III classification should contribute to more predictable and effective cataract surgery.References1.Chylack LT Jr,Wolfe JK,Singer DM,et al.The LensOpacities Classification System III;the Longitudinal Study of Cataract Study Group.Arch Ophthalmol1993;111:831–8362.Maraini G,Pasquini P,Tomba MC,et al.An independentevaluation of the Lens Opacities Classification System II (LOCS II);the Italian-American Cataract Study Group Ophthalmology1989;96:611–6153.Karbassi M,Khu PM,Singer DM,Chylack LT Jr.Evalu-J CATARACT REFRACT SURG—VOL29,JANUARY2003 144ation of Lens Opacities Classification System III applied at the slitlamp.Optom Vis Sci1993;70:923–928ton RD,Chylack LT Jr,Ko¨pcke W.Letters to theeditor.Ophthalmic Epidemiol1996;3:59–605.van den Berg TJTP,Coppens JC.Conversion of lens slitlamp photographs into physical light-scattering units.In-vest Ophthalmol Vis Sci1999;40:2151–21576.Davison JA.Performance comparison of the Alcon Legacy200001.1mm TurboSonics and0.9mm Aspiration By-pass System tips.J Cataract Refract Surg1999;25:1386–13917.Hu C,Zhang X,Hui Y,Chung H.[The nuclear hardnessand associated factors of age-related cataract].[Chinese] Yen Ko Tsa Chih2000;36:337–3408.Ursell PG,Spalton DJ,Tilling K.Relation between post-operative blood-aqueous barrier damage and LOCS III cataract gradings following routine phacoemulsification surgery.Br J Ophthalmol1997;81:544–547J CATARACT REFRACT SURG—VOL29,JANUARY2003145。