67 Paclitaxel poliglumex药理药效研究 动物模型
药理学研究中的动物模型

药理学研究中的动物模型药理学是研究药物对生物系统的作用、药物相互作用及其在人体内的代谢和排泄等方面的科学。
而动物模型则是药理学研究的重要手段之一,是在药理学研究中广泛应用的实验方法。
本文将探讨动物模型在药理学研究中的运用以及存在的问题。
一、动物模型在药理学研究中的运用1.药效学研究药物剂量-反应关系是药一个药物治疗效果的关键参数。
通过对动物模型进行药效学研究,可以帮助研究者确定药物的剂量和给药方法,及其对特定疾病产生的治疗作用。
2.药代动力学研究药代动力学研究涉及药物在生物体内的吸收、分布、代谢及排泄等过程。
通过使用动物模型,研究者可以更好地理解人体内药物相互作用的机制,以及药物在体内的代谢及排泄吸收规律。
3.毒理学研究另外,动物模型也广泛应用于毒理学研究方面。
通过使用动物模型,研究者可以评估药物的毒性,并为药物的临床使用提供指导。
二、动物模型存在的问题1.模型转化性能的问题研究者对动物模型的应用需要深刻认识到动物模型本身具有的局限性。
动物模型无法完全反映人体内部各种细微变化的复杂性,因此,能否将动物的结果转化为人体的治疗方案存疑。
2.道德问题另外,动物模型研究也存在一定的道德问题。
因为动物在实验中往往会受到一定程度的折磨,所以必须确保实验的道德可接受,避免动物受到过度转化。
3.统计学意义上的问题最后,动物模型的应用还可能存在统计学意义上的问题,研究者必须严格控制实验中的各种环境因素,以确保研究结果的可靠性。
三、结语总体来说,动物模型在药理学研究中扮演着重要的角色。
尽管存在一些问题,但研究者仍需要认真对待这种研究方法,尽力避免它的局限性,改善其缺陷,并为临床应用提供可靠的依据。
同时,必须通过科学的伦理道德评估来确保研究过程的公正公平。
只有慎重对待,才能更好地补充人类已知的药理学知识,为发现从动物实验中发现的新药物奠定基础。
博来霉素诱导的肺纤维化动物模型
博来霉素诱导的肺纤维化动物模型
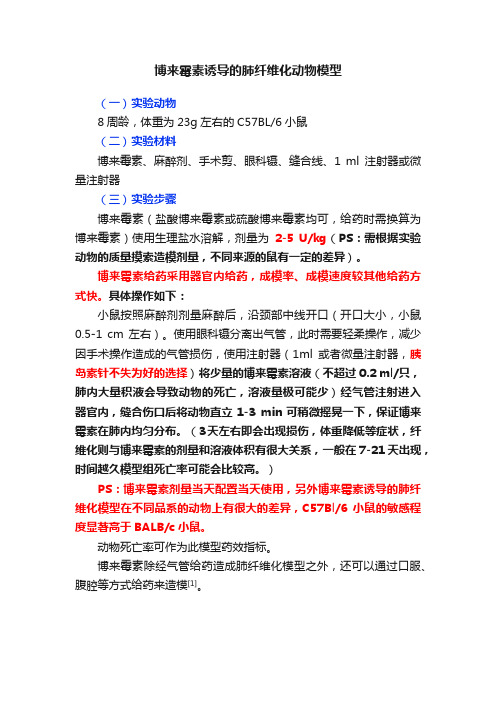
(一)实验动物
8周龄,体重为23g左右的C57BL/6小鼠
(二)实验材料
博来霉素、麻醉剂、手术剪、眼科镊、缝合线、1 ml注射器或微量注射器
(三)实验步骤
博来霉素(盐酸博来霉素或硫酸博来霉素均可,给药时需换算为博来霉素)使用生理盐水溶解,剂量为2-5 U/kg(PS:需根据实验动物的质量摸索造模剂量,不同来源的鼠有一定的差异)。
博来霉素给药采用器官内给药,成模率、成模速度较其他给药方式快。
具体操作如下:
小鼠按照麻醉剂剂量麻醉后,沿颈部中线开口(开口大小,小鼠0.5-1 cm左右)。
使用眼科镊分离出气管,此时需要轻柔操作,减少因手术操作造成的气管损伤,使用注射器(1ml或者微量注射器,胰岛素针不失为好的选择)将少量的博来霉素溶液(不超过0.2 ml/只,肺内大量积液会导致动物的死亡,溶液量极可能少)经气管注射进入器官内,缝合伤口后将动物直立1-3 min可稍微摇晃一下,保证博来霉素在肺内均匀分布。
(3天左右即会出现损伤,体重降低等症状,纤维化则与博来霉素的剂量和溶液体积有很大关系,一般在7-21天出现,时间越久模型组死亡率可能会比较高。
)
PS:博来霉素剂量当天配置当天使用,另外博来霉素诱导的肺纤维化模型在不同品系的动物上有很大的差异,C57Bl/6小鼠的敏感程度显著高于BALB/c小鼠。
动物死亡率可作为此模型药效指标。
博来霉素除经气管给药造成肺纤维化模型之外,还可以通过口服、腹腔等方式给药来造模[1]。
紫杉醇(PTX)在食管癌同期放化疗中的研究进展

紫杉醇(PTX)在食管癌同期放化疗中的研究进展邓家营【摘要】紫杉醇(paclitaxel,PTX)是食管癌化疗中最有活性的药物之一,因其独特的作用机制和良好的耐受性,被广泛与顺铂(cisplatin,DDP)、5氟尿嘧啶(fluorouracil,5 Fu)等联合应用.PTX还有一定的放射增敏作用,作为放射增敏剂之一常被用于同期放化疗.在临床上,PTX类药物有不同的制剂类型和用药方案,本文就其在食管癌放化疗中的研究进展,在不同方案中的作用以及应用中存在的问题作一综述.【期刊名称】《复旦学报(医学版)》【年(卷),期】2014(041)005【总页数】5页(P697-700,705)【关键词】食管肿瘤;同期放化疗;紫杉醇(PTX)【作者】邓家营【作者单位】复旦大学附属肿瘤医院放疗科上海200032;复旦大学上海医学院肿瘤学系上海200032【正文语种】中文【中图分类】R735.1食管癌是我国常见的恶性肿瘤之一,也是世界范围内常见的癌症死亡原因。
因其早期症状不明显,30%~40%的食管癌确诊时已属无法手术切除的局部晚期。
食管癌单纯放疗效果不佳,5年生存率约为20%,局部未控和复发可达60%~80%。
单纯的化疗又很少获得病理完全缓解,且缓解期较短。
所以临床上更多地应用同期放化疗来治疗局部区域性食管癌非手术的患者。
顺铂(cisplatin,DDP)联合5-氟尿嘧啶(5-fluorouracil,5-Fu)是经典化疗方案,但是该方案患者耐受性差且疗效不理想。
探索更加高效、低毒并有放射增敏作用的新化疗药物是进一步提高食管癌同期放化疗疗效的重要途径之一。
紫杉醇(paclitaxel,PTX)是一种二萜类生物碱,主要从红豆杉树皮中分离提取。
作为抗肿瘤药,PTX具有独特的作用机制,一方面它可与β-微管蛋白结合并促进其聚合,诱导有丝分裂阻滞于G2/M期,从而使细胞出现分裂性死亡;另一方面,它还可以影响信号通路诱发细胞凋亡。
动物模型在药物研究中的应用及其限制
动物模型在药物研究中的应用及其限制药物研究是一个复杂的过程,其中动物模型在药物研究的发展中起到了极为重要的作用。
动物模型可以模拟人体内的生理和病理过程,尤其是可以模拟人体内药物的代谢和副作用。
然而,动物模型也有其局限性。
本文将讨论动物模型在药物研究中的应用及其限制。
一、动物模型在药物研究中的应用1. 建立疾病模型疾病模型可以为药物研究提供一个可靠的模拟环境,疾病模型可以通过动物模型来建立。
例如,研究肿瘤药物可以使用小鼠肿瘤模型,研究糖尿病药物可以使用小鼠和大鼠糖尿病模型。
这些模型可以用于检测药物的疗效和副作用。
2. 药代动力学药代动力学是研究药物在人体内的吸收、分布、代谢和排泄的过程。
动物模型可以用于检测药物的药代动力学。
这些动物模型可以为研究人类体内的药物动力学提供一定的参考。
3. 安全性评估药物在人体内可以引起各种不良反应,例如中毒、过敏反应和疾病进展。
在药物研究的早期阶段,动物模型可以检测药物的安全性。
这些动物模型可以检测药物的副作用、毒性和耐受性等数据。
二、动物模型在药物研究中的限制尽管动物模型在药物研究中起着至关重要的作用,但是它们也有其局限性。
以下是动物模型在药物研究中的限制。
1. 种属差异不同的动物有不同的生理和代谢过程,因此药物在不同动物体内的代谢方式也有所不同。
例如,大鼠和小鼠在药物代谢方面存在明显差异。
因此,使用不同种类的动物进行药物研究可能会导致误判和误导。
2. 疾病模型不准确虽然动物模型可以模拟人类疾病的一些特征,但是它们仍然不能完全模拟人类内部环境。
例如,化学药物在动物体内的代谢方式和在人体内的代谢方式是不同的。
因此,在进行药物研究时需要谨慎评估动物模型的准确性和适用性。
3. 数据解释困难药物在动物体内和人体内的代谢方式和生理反应不尽相同。
因此,在动物模型中获得的数据需要进行解释和转化,以便用于预测人体内的药物代谢和生理反应。
这一转化过程可能会导致推理和缺乏可重复性的困难。
小细胞肺癌可视化PDOX肿瘤动物模型免疫表型Ki-67表达的研究进展

小细胞肺癌可视化PDOX肿瘤动物模型免疫表型Ki-67表达的研究进展作者:吴柳盛李小强来源:《中国医学创新》2021年第25期【摘要】小细胞肺癌(SCLC)是肺癌所有病理类型中预后最差的一种,患者生存周期极短,死亡率极高。
虽然SCLC对化疗药物敏感,临床上抗肿瘤药物治疗成为主流,但有循证医学研究发现在临床中不同的患癌个体之间对抗肿瘤药物的敏感性和耐受性存在着差异,这给临床治疗带来了困难和挑战。
因此,人们急需要一种能高度模拟体内肿瘤细胞生长微环境,能与患者进行同步化动态观察抗肿瘤药物应答的理想动物模型。
可视化PDOX肿瘤动物模型满足了这些需求,这也是目前国际上最前沿的肿瘤动物模型构建技术,避免了个体差异,为临床治疗提供了个性化思路,同时Ki-67免疫表型表达的监测为早期SCLC的诊断提供了有效帮助。
现对最近国内外SCLC可视化PDOX肿瘤动物模型构建技术和免疫表型Ki-67表达监测的研究进展以及该模型对临床上不同个体之间抗肿瘤药物应答差异做全面综述。
【关键词】小细胞肺癌可视化PDOX肿瘤动物模型 Ki-67[Abstract] Small cell lung cancer (SCLC) has the worst prognosis among all pathological types of lung cancer. The survival cycle of patients is very short and the mortality rate is very high. Although SCLC is sensitive to chemotherapy drugs and anti-tumor drug therapy has become the mainstream in clinical practice, evidence-based medicine studies have found that there are differences in the sensitivity and tolerance of anti-tumor drugs among different cancer patients in clinical practice, which brings difficulties and challenges to clinical treatment. Therefore, there is an urgent need for an ideal animal model that can highly simulate the microenvironment of tumor cell growth in vivo and can dynamically observe the response to antitumor drugs in synchronization with patients. Visualized PDOX tumor animal model meets these needs, which is also the most advanced tumor animal model construction technology in the world at present. It avoids individual differences and provides personalized ideas for clinical treatment. Meanwhile, the monitoring of Ki-67 immunophenotype expression provides effective help for the diagnosis of early SCLC. In this paper,the research progress of visualized PDOX tumor animal model construction technology and immunophenotype Ki-67 expression monitoring of SCLC at home and abroad, as well as the clinical differences of anti-tumor drug response among different individuals in this model are comprehensively reviewed.[Key words] SCLC Visualized PDOX tumor animal model Ki-67First-author’s address: Peking University Shenzhen Hospital, Shenzhen 518036, Chinadoi:10.3969/j.issn.1674-4985.2021.25.042小細胞肺癌(small cell lung cancer,SCLC)占全部肺癌的15%~17%[1],病情恶化快,可迅速出现远处内脏肿瘤转移,生存寿命短,死亡率极高,同时在临床上不同肿瘤患者个体之间存在着抗肿瘤药物的耐受差异,给临床治疗与疗效评估带来了困难。
动物模型在药物研究中的应用

动物模型在药物研究中的应用药物研究是一个综合性强、需要借助各种手段和方法才能完成的科学研究。
其中,动物模型是一个重要的研究手段,在药物研究中应用广泛。
动物模型可以帮助研究人员更好地了解药物的药理作用、剂量、毒性等方面的信息,提高药物研究的效率和成功率。
本文将探讨动物模型在药物研究中的应用,并分析其优缺点。
一、1. 药物的药理作用研究动物模型可以帮助研究人员更好地了解药物的药理作用。
例如,针对肿瘤的化疗药物,研究人员可以通过动物模型来评估药物的抗肿瘤作用、毒性和耐受性。
动物模型可以模拟人体中的肿瘤环境,通过观察动物体内的肿瘤变化,了解药物的药理作用和剂量范围,为药物的临床应用提供依据。
2. 药效学研究动物模型可以帮助研究人员进行药效学研究。
例如,对于心血管疾病的药物,研究人员可以通过动物模型来评估药物的心血管效应、有效剂量、安全剂量等信息。
通过动物实验,研究人员可以获取药物在动物体内的体内药效学参数,了解药物的药效学特性,为药物的临床应用提供依据。
3. 毒理学研究动物模型可以帮助研究人员进行毒理学研究。
例如,在新药研究过程中,需要对药物的毒性进行评估。
通过动物模型,研究人员可以获取药物的毒性数据,包括剂量效应关系、生化毒性、组织学和病理学损伤等信息。
这些数据可以为药物的临床应用提供依据,帮助研究人员了解药物的毒性水平,以及如何使用药物时避免毒性损害。
4. 药物代谢动力学研究动物模型可以帮助研究人员进行药物代谢动力学研究。
例如,在新药研究过程中,需要了解药物的代谢途径、代谢产物和半衰期等信息。
通过动物实验,研究人员可以获得药物代谢动力学参数,如药物清除率、药物代谢酶的活性等,为药物的临床应用提供依据。
二、动物模型在药物研究中的优缺点1. 优点(1)相对真实:动物模型的研究结果相对比较真实,因为它可以模拟人体生理环境,给人类疾病的研究提供一定的可靠性。
(2)有利于筛选药效:动物模型有助于筛选药物的药效,检索药物的安全性、有效性等,从而为药物的研发和临床应用提供依据。
预测肿瘤药物临床试验效果的动物模型新进展

预测肿瘤药物临床试验效果的动物模型新进展余飞;丁慧【期刊名称】《中国比较医学杂志》【年(卷),期】2015(000)006【摘要】基于人体试验的实际应用及伦理方面的考虑,合适的动物模型对于肿瘤药物研发至关重要。
制药公司和研究机构在肿瘤治疗新药的开发过程中消耗大量资源,最佳动物体内模型的选择可以改进或缩短研发进程。
在技术复杂性方面,肿瘤遗传工程小鼠模型( GEMM)已逐步完善,并且GEMM能够准确重建人类肿瘤的同源发生,为加快肿瘤药物的开发提供机遇。
本文主要综合比较预测肿瘤药物临床试验效果的不同类型动物模型,探讨其优劣,并对体内模型的评估方法及与临床转化等进行简述,为肿瘤药物临床前试验提供参考。
%Due to practical and ethical concerns associated with human experiments, animal models have been essential in cancer research.Vast resources are expended during the development of new cancer therapeutics, and selection of optimal in vivo models should improve this process.Genetically engineered mouse models ( GEMM) of cancer have progressively improved in technical sophistication and, accurately recapitulating the human cognate condition, have provided opportunities to accelerate the development of cancer drugs.In this article we consider the different types of animal models used for predicting the results of clinical trials of cancer drugs, and discuss the strengths and weaknesses of each in this regard.In addition, the methods of predicting in vivo models and clinical translation are discussed.【总页数】6页(P65-69,70)【作者】余飞;丁慧【作者单位】南京大学医学院附属鼓楼医院,南京 210008;南京大学医学院附属鼓楼医院,南京 210008【正文语种】中文【中图分类】R-33【相关文献】1.新冠肺炎疫情下抗肿瘤药物临床试验现状与紧急应对策略 [J], 刘小保; 高素彬; 衡建福; 刘洋; 杨农; 李坤艳; 王静; 肖亚洲2.新冠肺炎疫情下抗肿瘤药物临床试验中受试者访视管理的紧急应对 [J], 蒋云; 刘小保; 汤清涛; 杨农; 黄钢; 王静; 李坤艳3.某院抗肿瘤药物临床试验方案偏离的回顾性研究 [J], 叶丽君;蔡淑帆;林能明;王飞4.通过基于风险评估统计模型的中心化监查优化抗肿瘤药物临床试验质量管理 [J], 胡劲;徐炎;周高超;殷悦;金迪蒂5.影像组学在抗肿瘤药物临床试验疗效评估中的应用和挑战 [J], 李佳铮;唐磊因版权原因,仅展示原文概要,查看原文内容请购买。
淋巴瘤药理药效研究动物模型
弥漫大B细胞淋巴瘤(DLBCL)
DLBCL是一种大B淋巴细胞弥漫性增生 所组成的肿瘤,瘤细胞核至少2倍于正 常小淋巴细胞核或大于巨噬细胞核
DLBCL临床特点
☞ 最常见的恶性淋巴瘤 ☞ 任何年龄均可发生,高峰年龄60~69岁,
男性稍多 ☞ 淋巴结无痛性增大,40%可原发于结外 ☞ 可原发或继发于其它小B细胞淋巴瘤 ☞ 50%患者临床分期Ⅲ或Ⅳ期 ☞ 总的5年生存率46%
► 11、滤泡性淋巴瘤 -胃肠道滤泡性淋巴瘤 -儿童滤泡性淋巴瘤 -“原位”滤泡性淋巴瘤 12、结内边缘带B细胞淋巴瘤 13、套细胞淋巴瘤 14、弥漫大B细胞淋巴瘤 -弥漫大B细胞淋巴瘤,非特殊类型 T细胞/组织细胞丰富的大B细胞淋巴瘤 老年人EBV阳性的弥漫大B细胞淋巴瘤 慢性炎症相关的弥漫大B细胞淋巴瘤 -脓胸相关淋巴瘤 -慢性骨髓炎相关淋巴瘤 -植入物相关淋巴瘤
CLL/SLL临床特点
☞ 老年人,中位年龄65岁,男∶女=2∶1 ☞ 无症状或表现无力,自体免疫性贫血,易
感染,骨髓和周围血大多累及,可伴脾脏 肿大
☞ 5%患者进展为DLBCL(Richter综合征) ☞ 5年生存率51%
CLL/SLL形态学
肿瘤细胞
小圆形淋巴细胞,幼淋巴细胞和副免疫 母细胞
组织结构
(占GI的85%)。以下依次为肺、头颈 部、眼眶、皮肤、甲状腺和乳腺等
☞ 临床分期大多为Ⅰ或Ⅱ期 ☞ 幽门螺杆菌胃炎史或自体免疫性疾病史 ☞ 5年生存率74%
MALTL形态学
肿瘤细胞
边缘区(中心细胞样)细胞,单核 细胞样B细胞,小淋巴细胞,IB样和 CB样细胞
组织结构
滤泡的边缘区和/或滤泡间区分布 滤泡植入 淋巴上皮病变
ki-67阳性细胞>30% 者预后 较差
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
O RIGINAL A RTICLEPaclitaxel Poliglumex(PPX-Xyotax)and Concurrent Radiation for Esophageal and Gastric CancerA Phase I StudyTom Dipetrillo,MD,*Luka Milas,MD,†Devon Evans,MD,*Paul Akerman,MD,*Thomas Ng,MD,* Tom Miner,MD,*Dennis Cruff,MD,*Bharti Chauhan,MD,*David Iannitti,MD,*David Harrington,MD,*and Howard Safran,MD*Objectives:To determine the maximal tolerated dose(MTD)and dose limiting toxicities of poly(L-glutamic acid)-paclitaxel(PPX)and con-current radiation(PPX/RT)for patients with esophageal and gastric cancer.Methods:Patients with esophageal or gastric cancer receiving chemo-radiation for loco-regional,adjuvant,or palliative intent were eligible. The initial dose of PPX was40mg/m2/wk,for6weeks with50.4Gy radiation.Dose levels were increased in increments of10mg/m2/wk of PPX.Results:Twenty-one patients were enrolled over5dose levels.Sixteen patients had esophageal cancer and5had gastric cancer.Twelve patients received PPX/RT as definitive loco-regional therapy,4patients had undergone resection and received adjuvant PPX/RT,and5patients had metastatic disease and received PPX/RT for palliation of dyspha-gia.Dose limiting toxicities of gastritis,esophagitis,neutropenia,and dehydration developed in3of4patients treated at the80mg/m2dose level.Four of12patients(33%)with loco-regional disease had a complete clinical response.Conclusions:The maximally tolerated dose of PPX with concurrent radiotherapy is70mg/m2/wk for patients with esophageal and gastric cancer.Key Words:paclitaxel polyglumex,concurrent chemoradiation, esophageal cancer,gastric cancer,macromolecule drug conjugate (Am J Clin Oncol2006;29:376–379)P PX is a drug conjugate that links paclitaxel to a biodegrad-able polymer,poly-L-glutamic acid.1Preclinically,poly(L-glutamic acid)-paclitaxel(PPX)has demonstrated tumor tissue radiation enhancement factors from4.0to8.0compared with1.5 to 2.0for paclitaxel.2PPXs macromolecular structure may underlie its improved radiation enhancement.PPX has a molec-ular weight of40,000compared with854for paclitaxel.3Solid tumors are more permeable to macromolecules thannormal tissue because of altered capillary endothelium.4Further-more,macromolecules persist longer in tumor tissue because ofthe relative decrease in lymphatics compared with non-neoplas-tic tissue.5Radiation increases the vascular permeability of solidtumors.6,7Local tumor irradiation in tumor cell lines increasesvascular permeability and increases PPX uptake.2Tumor se-creted vascular endothelial growth factor also increases vascularpermeability.8The combination of PPX and radiation in theovarian Oca-1carcinoma implanted in C3Hf/Kam mice pro-duced a significantly greater tumor growth delay than treatmentwith radiation and paclitaxel when both drugs were given at anequivalent paclitaxel dose(enhancement factors of4.44versus1.50).2These preclinicalfindings support the hypothesis that thesupra-additive effect of combined PPX/RT is because of themodulation of the enhanced permeability and retention effect ofmacromolecules by radiation.Paclitaxel is an important radiation sensitizer in uppergastrointestinal malignancies.9–14We initiated a phase I trial ofPPX/RT for patients with esophageal and gastric cancer.This isthefirst report of a clinical study utilizing a poly L-glutamic acidmacromolecule as a radiation sensitizer in human malignancies.MATERIALS AND METHODS EligibiltyPatients with a histologically confirmed diagnosis of esoph-ageal adenocarcinoma or squamous cell carcinoma,or gastric ade-nocarcinoma were enrolled between January2004and May2005.PPX/RT could be administered as definitive loco-regional oradjuvant therapy.Patients with metastatic disease with dyspha-gia were also eligible.Required laboratory parameters includedabsolute neutrophil countϾ1,500L hemoglobinϾ10g/dL, plateletsϾ100,000L,creatinineϽ1.5mg/dL,bilirubinϽ1.5 mg/dL,alanine aminotransferase,and alkaline phosphatase Ͻ2.5ϫupper limit of normal,and calciumϽ12mg/dL.Patients with previous irradiation,Eastern Cooperative Oncology Group(ECOG)performance statusϾ1,life expectancyϽ12weeks,tracheobronchial invasion,tracheoesophagealfistula,unstableFrom The*Brown University Oncology Group,Providence,RI;and the †Department of Experimental Radiation Oncology,The University of Texas M.D.Anderson Cancer Center,Houston TX.Reprints:Devon Evans,MD,Brown University,Department of Hematology/ Oncology,164Summit Avenue,Providence,RI02906.E-mail:devans@ .Copyright©2006by Lippincott Williams&WilkinsISSN:0277-3732/06/2904-0376DOI:10.1097/01.coc.0000224494.07907.4ecardiac disease within6months,active infection,brain metas-tasis,laryngeal or phrenic nerve paralysis,unstable neurologic symptoms,sensory or motor neuropathy greater than grade1,or other concurrent malignancy,were excluded.A complete his-tory and physical examination were performed on all patients before treatment.Height,weight,performance status,and tumor stage were recorded.Required staging studies included a com-puted tomography(CT)scan of the chest,abdomen,and pelvis. Pre-and post-treatment endoscopies were required only in pa-tients with loco-regional disease.The study was approved by the institutional review boards of all participating hospitals and Brown University.All patients gave written informed consent according to federal and institutional guidelines. ChemotherapyPPX was administered as a10-minute infusion before radiotherapy on days1,8,15,22,29,36on an outpatient basis. Patients were treated with PPX according to a dose escalation scheme,with patients enrolled in cohorts of3at each dose level. The initial dose level was40mg/m2/wk in3patients,and was increased in increments of10mg/m2/wk in the next patient cohort if no patients had a dose limiting toxicity(DLT).All toxicities were graded according to the NCI Common Toxicity Criteria,Version3.Dose limiting toxicities were defined as grade3esophagitis,enteritis or gastritis,grade3nausea(despite maximal antinausea treatment)or dehydration,any other grade3 or4nonhematologic toxicity,and grade4neutropenia or throm-bocytopenia lasting more than1week.Toxicities were consid-ered dose limiting only if they resulted from toxicity of chemo-radiation,and not from disease progression.If one or2patients experienced a DLT,then3additional patients were enrolled at the same dose level.If no more than2patients total experienced a DLT at that dose level,than the dose was escalated for the next patient cohort.IfϾ2patients had a DLT,then the dose was de-escalated to the next dose level,and3additional patients enrolled.The MTD was defined as the dose at which no more than2of6patients have a DLT.RadiotherapyPatients received radiation concurrently with chemother-apy to a total dose of50.4Gy,administered at1.8Gy/d,for a total of28days(5days/wk)using aՆ10-MV linear accelerator. Three-dimensional conformal radiation was used to treat all patients.For esophageal and gastric cancers extending to the esophagus,the treatmentfields extended5cm beyond the superior and inferior borders,and2cm beyond the lateral margins.For gastric tumors confined to the stomach,the radia-tionfields encompassed the primary tumor and draining lymph nodes with a2to3cm margin in all directions.The right lateral margins included the portal,hepatic,and common bile duct as well as the head of the pancreas.Postsurgical patients receiveda radiation dose of45Gy delivered in25fractions(1.8Gy/d)for5.5weeks followed by a cone down after45Gy to encompass gross or microscopic disease with a margin of1to1.5cm,for a total dose of50.4Gy.ResponseResponse to treatment was assessed by pre-and posttreat-ment upper endoscopy.Only patients with loco-regional disease had disease assessable for response.A clinical complete re-sponse was defined as no tumor visible on follow-up endoscopy and no tumor on posttreatment biopsy.RESULTSPatient CharacteristicsTwenty-one patients(all Caucasian)were enrolled in this study.Patient characteristics are listed in Table1.Sixteen pa-tients had esophageal cancers,and5patients had gastric cancers extending to the gastroesophageal junction.Twenty patients had adenocarcinomas,and1patient had squamous cell carcinoma. Twelve patients received PPX/RT to treat loco-regional disease. Four patients received PPX/RT for adjuvant therapy after resec-tion,and5patients with metastatic disease at study entry were treated with PPX/RT for local control and symptom palliation. Seven patients had been treated previously with chemotherapy. ToxicityPatients received PPX/RT over5dose levels(see Table2). At the80mg/m2dose level,3of4patients had dose limiting toxicities including grade3esophagitis/gastritis(nϭ2),grade3 dehydration(nϭ1),and grade4neutropenia(nϭ1).One of6 patients at the70mg/m2dose level had grade3esophagitis. There were no grade3or4toxicities at dose levels below PPX 70mg/m2/wk.Dose limiting toxicities did not correlate with either disease site(gastric versus esophageal)or previous che-motherapy treatment.Except for the4patients who experienced a dose limiting toxicity,all patients completed the full6weeks of concurrent chemoradiation.Acute toxicities during chemoradiation are listed in Table3. Multiple toxicities in a single patient are scored as separate events.Esophagitis and dehydration were the most common grade3/4toxicities.One grade2hypersensitivity reaction(urti-caria)was noted among the21patients treated.The patient was TABLE1.Patient CharacteristicsNo.patients enrolled21 SexMale18 Female3 Tumor typeEsophageal16 Gastric5 PathologyAdenocarcinoma20 Squamous cell1 Treatment indicationLoco-regional12 Adjuvant4 Palliation(metastatic)5 Prior chemotherapy7 Median age in years(range)63(41–91)American Journal of Clinical Oncology•Volume29,Number4,August2006PPX-Xyotax and Radiation for Esophagogastric Cancersuccessfully retreated without further hypersensitivity reaction following dexamethasone and diphenhydramine premedication. No alopecia was observed in this study.ResponseTwelve patients had loco-regional disease and were as-sessable for response on posttreatment endoscopy.Four of12 patients(33%)had complete clinical response.An additional7 patients hadϾ50%tumor reduction as assessed by posttreat-ment endoscopy.Loco-regional activity was seen in patients who developed systemic metastases during treatment.DISCUSSIONPaclitaxel is a commonly used radiation sensitizer in multiple tumor types.9–18Paclitaxel synchronizes cells in G2/M, the most radiosensitive phase of the cell cycle,by enhancing microtubule assembly and preventing microtubule depolymer-ization.19–21Paclitaxel has the exceptional property of killing tumor cells in the absence of wild-type p53function in vitro.22 We demonstrated that p53gene mutations are not predictors of unfavorable response to paclitaxel/RT.23Paclitaxel radiosensi-tizes small bowel progenitor cells less than tumor cells poten-tially increasing the therapeutic index of paclitaxel radiosensi-tization in upper gastrointestinal cancers.24PPX is a drug conjugate that links paclitaxel to a biode-gradable polymer,poly-L-glutamic acid.The resulting macro-molecule has several beneficial properties.It is water-soluble, eliminating the need for Cremophor EL and thus reducing the risk of hypersensitivity reactions,and can be given as a10-minute infusion.The hyperpermeable angiogenic vasculature and suppressed lymphatic clearance of tumors facilitate PPX retention within the tumor space,resulting in higher intratumor drug concentrations over prolonged periods.This effect has been described as the enhanced permeability and retention effect(EPR).PPX is absorbed by tumor cells by endocytosis,bypassing the MDR pathway that commonly causes chemotherapy drug resistance.25,26PPX has been evaluated in a phase III trial in patients with performance status2advanced nonsmall cell lung cancer.This study demonstrated a similar response and sur-vival of PPX and carboplatin as compared with paclitaxel and carboplatin.27Radiation increases the vascular permeability of solid tumors.6,7The modulation of the EPR of macromolecules by radiation may underlie the striking preclinical enhancement of radiation and PPX.2This is thefirst clinical trial of PPX and concurrent RT.The maximum tolerated dose of PPX is70 mg/m2/wk with50.4Gy radiation for patients with esophageal and gastric cancer.The toxicities observed in this study of esophagitis,gastritis,and nausea were attributable to PPX in-duced RT enhancement.Substantial preliminary activity was demonstrated in this phase I study with one-third of patients undergoing a complete clinical response to PPX/RT alone.Loco-regional activity was demonstrated in some patients developing systemic progression illustrating that PPXs most important effect was as a radiation sensitizer.We have initiated a phase I study evaluating PPX, cisplatin,and concurrent radiation for patients with esophageal and gastric cancer.Based on the strong preclinical data and the promising preliminary results with PPX/RT,further evaluation of PPX radiosensitization in other human tumors is warranted.REFERENCES1.Singer JW,Baker B,de Vries P,et al.Poly-(L)-glutamic acid–paclitaxel(CT-2103)͓XYOTAXt͔,a biodegradable polymeric drug conjugate.Adv Exp Med Biol.2003;519:81–99.2.Chun Li,Shi Ke,Qing-Ping Wu,et al.Tumor irradiation enhances thetumor-specific distribution of poly(l-glutamic acid)-conjugated pacli-taxel and its antitumor efficacy.Clin Cancer Res.2000;6:2829–2834.3.Li C,Yu DF,Newman RA,et plete regression of well-estab-lished tumors using a novel water-soluble poly(l-glutamic acid)-pacli-taxel conjugate.Cancer Res.1988;58:2404–2409.4.Gerlowski LE,Jain RK.Microvascular permeability of normal andneoplastic tissue.Microvasc Res.1986;31:288–305.5.Maeda H,Matsumura Y.Tumoritropic and lymphotropic principles ofmacromolecular drugs.Crit Rev Ther Drug Carrier Syst.1989;6:193–210.6.Baker DG,Krochak RJ.The response of the microvascular system toradiation:a review.Cancer Invest.1989;7:287–294.7.Chohen FM,Kuwatsuru R,Shames DM,et al.Contrast-enhancedmagnetic resonance imaging estimation of altered capillary permeability in experimental mammary carcinomas after X-irradiation.Invest Radiol.1994;29:970–977.8.Dvorak HF,Brown LF,Detmar M,et al.Vascular permeability factor/vascular endothelial growth factor,microvascular hyperpermeability and angiogenesis.Am J Pathol.1995;146:1029–1039.9.Safran H,King T,Choy H,et al.Paclitaxel and concurrent radiation forlocally advanced pancreatic and gastric cancer:a phase I study.J Clin Oncol.1997;15:901–907.10.Safran H,Wanebo HJ,Hesketh PK,et al.Paclitaxel and concurrentradiation for gastric cancer.Int J Radiat Oncol Biol Phys.2000;46:889–894.TABLE2.Dose Limiting Toxicities(DLTs)PPX Dose (mg/m2/wk)No.PatientsToxicities(grade3–4)DehydrationGastritis/Esophagitis Weakness ANC40300005040000604000070601008042211TABLE3.ToxicityՆGrade2No.Patients(n؍21)Grade2Grade3Grade4NonhematologicalEsophagitis/gastritis530Nausea/vomiting310Anorexia400Dehydration720Fatigue/weakness610Infection200Hypersensitivity100HematologicalNeutropenia001Thrombocytopenia110Dipetrillo et al American Journal of Clinical Oncology•Volume29,Number4,August200611.Safran H,Gaissert H,Akerman P,et al.Paclitaxel,cisplatin andconcurrent radiation for esophageal cancer.Cancer Invest.2001;1:1–7.12.Safran H,Moore T,Iannitti D,et al.Paclitaxel and concurrent radiationfor locally advanced pancreatic cancer.Int J Radiat Oncol Biol Phys.2001;49:1275–1279.13.Ajani JA,Mansfield PF,Crane CH,et al.Paclitaxel-based chemoradio-therapy in localized gastric carcinoma:degree of pathologic response and not clinical parameters dictated patient outcome.J Clin Oncol.2005;23:1237–1244.14.Brenner B,Ilson DH,Minsky BD,et al.Phase I trial of combined-modality therapy for localized esophageal cancer:escalating doses of continuous-infusion paclitaxel with cisplatin and concurrent radiation therapy.J Clin Oncol.2004;22:45–52.15.Choy H,Akerley W,Safran H,et al.A phase I trial of concurrent weeklytaxol administered as a3hour infusion and radiation therapy for advanced non-small cell lung cancer.J Clin Oncol.1994;12:2682–2686.16.Choy H,Akerley W,Glantz M,et al.Concurrent paclitaxel and radiationtherapy for solid tumors.Cancer Control.1996;3:310–318.17.Choy H,Safran H,Akerley W,et al.Phase II trial of weekly paclitaxeland concurrent radiation therapy for locally advanced non-small cell lung cancer.Clin Cancer Res.1998;4:1931–1936.18.Choy H,Akerley W,Safran H,et al.Multi-institutional phase II trial ofpaclitaxel,carboplatin and concurrent radiation therapy for locally ad-vanced non-small cell lung cancer.J Clin Oncol.1998;16:3316–3322.19.Sinclair WK,Morton RA.X-ray sensitivity during the cell generationcycle of cultured Chinese hamster cells.Radiat Res.1996;29:450–474.20.Liebmann J,Cook JA,Fisher J,et al.In vitro studies of taxol as aradiation sensitizer in human tumor cells.J Natl Cancer Inst.1994;86: 441–446.21.Minarik L,Hall EJ.Taxol in combination with acute and low dose rateirradiation.Radiother Oncol.1994;32:124–128.22.Wahl AF,Donaldson KL,Fairchild C,et al.Loss of normal p53functionconfers sensitization to Taxol by increasing G2/M arrest and apoptosis.Nature Med.1996;2:72–79.23.King T,Akerley W,Fan A,et al.p53mutations do not predict responseto paclitaxel in metastatic non-small cell lung cancer.Cancer.2000;89: 769–773.24.Mason KA,Milas L,Peters LJ.Effect of paclitaxel(taxol)alone and incombination with radiation on the gastrointestinal mucosa.Int J Radiat Oncol Biol Phys.1997;38:623–631.25.Duncan R.The dawning era of polymer therapeutics.Nat Rev DrugDiscov.2003;2:347–360.26.McCormick-Thomson LA,Duncan R.Poly(amino acid)copolymers asa potential soluble drug delivery system,I:pinocytic uptake and lyso-somal degradation measured in vitro.J Bioact Compat Polym.1989;4: 242–251.nger CJ,Socinski MA,Ross H,et al.Paclitaxel poliglumex(PPX)/carboplatin vs paclitaxel/carboplatin for the treatment of PS2 patients with chemotherapy-naı¨ve advanced non-small cell lung can-cer(NSCLC):a phase III study.Proc Am Soc Clin Oncol.2005;LBA: 7011.American Journal of Clinical Oncology•Volume29,Number4,August2006PPX-Xyotax and Radiation for Esophagogastric Cancer。