PROCYSBI FDA说明书(英文)
盐酸度洛西汀FDA说明书(英文)
1HIGHLIGHTS OF PRESCRIBING INFORMATIONdays of stopping an MAOI intended to treat psychiatric disorders.These highlights do not include all the information needed to use In addition, do not start Cymbalta in a patient who is being treated CYMBALTA safely and effectively. See full prescribing with linezolid or intravenous methylene blue (4.1) information for CYMBALTA. •Use in patients with uncontrolled narrow-angle glaucoma (4.2)CYMBALTA (duloxetine hydrochloride) Delayed-Release Capsules for Oral Use.Initial U.S. Approval: 2004WARNING: SUICIDAL THOUGHTS AND BEHAVIORS See full prescribing information for complete boxed warning. • Increased risk of suicidal thinking and behavior in children,adolescents, and young adults taking antidepressants (5.1) • Monitor for worsening and emergence of suicidal thoughtsand behaviors (5.1) • Cymbalta is not approved for use in pediatric patients (8.4) ---------------------------RECENT MAJOR CHANGES --------------------------Dosage and Administration:Switching a Patient To or From a Monoamine Oxidase Inhibitor (MAOI) Intended to Treat Psychiatric Disorders (2.5) 10/2012 Use of Cymbalta with Other MAOIs such as Linezolid or Methylene Blue (2.6) 10/2012 Contraindications – Monoamine Oxidase Inhibitors (4.1) 10/2012 Warnings and Precautions: Serotonin Syndrome (5.4) 10/2012 Discontinuation of Treatment with Cymbalta (5.7) 08/2012 ----------------------------INDICATIONS AND USAGE ---------------------------Cymbalta ® is a serotonin and norepinephrine reuptake inhibitor (SNRI) indicated for: • Major Depressive Disorder (MDD) (1.1) • Generalized Anxiety Disorder (GAD) (1.2)• Diabetic Peripheral Neuropathic Pain (DPNP) (1.3)• Fibromyalgia (FM) (1.4)• Chronic Musculoskeletal Pain (1.5)------------------------DOSAGE AND ADMINISTRATION-----------------------• Cymbalta should generally be administered once daily withoutregard to meals. Cymbalta should be swallowed whole andshould not be chewed or crushed, nor should the capsule beopened and its contents be sprinkled on food or mixed with liquids (2) Indication Starting Dose Target DoseMaximumDose MDD (2.1, 2.2)40 mg/day to 60 mg/day Acute Treatment: 40 mg/day (20 mg twice daily) to 60 mg/day (once daily or as 30 mg twice daily); Maintenance Treatment: 60 mg/day 120 mg/day GAD (2.1) 60 mg/day 60 mg/day (once daily) 120mg/day DPNP (2.1) 60 mg/day 60 mg/day (once daily) 60 mg/day FM (2.1)30 mg/day 60 mg/day (once daily) 60 mg/day Chronic Musculoskeletal Pain (2.1)30 mg/day 60 mg/day (once daily) 60 mg/day • Some patients may benefit from starting at 30 mg once daily (2.1) • There is no evidence that doses greater than 60 mg/day confersadditional benefit, while some adverse reactions were observed to be dose-dependent (2.1) • D iscontinuing Cymbalta: A gradual dose reduction isrecommended to avoid discontinuation symptoms (2.4, 5.7) ----------------------DOSAGE FORMS AND STRENGTHS---------------------20 mg, 30 mg, and 60 mg capsules (3)-------------------------------CONTRAINDICATIONS ------------------------------• Serotonin Syndrome and MAOIs: Do not use MAOIs intended totreat psychiatric disorders with Cymbalta or within 5 days ofstopping treatment with Cymbalta. Do not use Cymbalta within 14------------------------WARNINGS AND PRECAUTIONS -----------------------• Suicidality: Monitor for clinical worsening and suicide risk (5.1) • Hepatotoxicity: Hepatic failure, sometimes fatal, has been reported in patients treated with Cymbalta. Cymbalta should be discontinued in patients who develop jaundice or other evidence of clinically significant liver dysfunction and should not be resumed unless another cause can be established. Cymbalta should not be prescribed to patients with substantial alcohol use or evidence of chronic liver disease (5.2)• Orthostatic Hypotension and Syncope: Cases have been reportedwith duloxetine therapy (5.3)• Serotonin Syndrome: Serotonin syndrome has been reported withSSRIs and SNRIs, including with Cymbalta, both when taken alone, but especially when co-administered with other serotonergic agents (including triptans, tricyclic antidepressants, fentanyl, lithium, tramadol, tryptophan, buspirone and St. John’s Wort). If such symptoms occur, discontinue Cymbalta and initiate supportive treatment. If concomitant use of Cymbalta with other serotonergic drugs is clinically warranted, patients should be made aware of a potential increased risk for serotonin syndrome, particularly during treatment initiation and dose increases (5.4) • Abnormal Bleeding: Cymbalta may increase the risk of bleedingevents. Patients should be cautioned about the risk of bleeding associated with the concomitant use of duloxetine and NSAIDs, aspirin, or other drugs that affect coagulation (5.5, 7.4)• Severe Skin Reactions: Severe skin reactions, including erythemamultiforme and Stevens-Johnson Syndrome (SJS), can occur with Cymbalta. Cymbalta should be discontinued at the firstappearance of blisters, peeling rash, mucosal erosions, or any other sign of hypersensitivity if no other etiology can be identified. (5.6)• Discontinuation: May result in symptoms, including dizziness,headache, nausea, diarrhea, paresthesia, irritability, vomiting, insomnia, anxiety, hyperhidrosis, and fatigue (5.7) • Activation of mania or hypomania has occurred (5.8)• Seizures: Prescribe with care in patients with a history of seizuredisorder (5.9)• Blood Pressure: Monitor blood pressure prior to initiatingtreatment and periodically throughout treatment (5.10)• Inhibitors of CYP1A2 or Thioridazine: Should not administer withCymbalta (5.11)• Hyponatremia: Cases of hyponatremia have been reported (5.12) • Hepatic Insufficiency and Severe Renal Impairment: Should ordinarily not be administered to these patients (5.13)• Controlled Narrow-Angle Glaucoma: Use cautiously in thesepatients (5.13)• Glucose Control in Diabetes: In diabetic peripheral neuropathicpain patients, small increases in fasting blood glucose, and HbA 1c have been observed (5.13)• Conditions that Slow Gastric Emptying: Use cautiously in these patients (5.13)• Urinary Hesitation and Retention (5.14)-------------------------------ADVERSE REACTIONS------------------------------• Most common adverse reactions (≥5% and at least twice theincidence of placebo patients): nausea, dry mouth, somnolence, constipation, decreased appetite, and hyperhidrosis (6.3). To report SUSPECTED ADVERSE REACTIONS, contact Eli Lilly and Company at 1-800-LillyRx (1-800-545-5979) or FDA at 1-800-FDA-1088 or /medwatch.-------------------------------DRUG INTERACTIONS ------------------------------• Potent inhibitors of CYP1A2 should be avoided (7.1). • Potent inhibitors of CYP2D6 may increase duloxetineconcentrations (7.2).• Duloxetine is a moderate inhibitor of CYP2D6 (7.9). ------------------------USE IN SPECIFIC POPULATIONS-----------------------• Pregnancy and Nursing Mothers: Use only if the potential benefitjustifies the potential risk to the fetus or child (2.3, 8.1, 8.3).See 17 for PATIENT COUNSELING INFORMATION and MedicationGuide Revised: 10/20122FULL PRESCRIBING INFORMATION: CONTENTS*WARNING: SUICIDAL THOUGHTS AND BEHAVIORS1 INDICATIONSANDUSAGE1.1 Major Depressive Disorder1.2 Generalized Anxiety Disorder1.3 Diabetic Peripheral Neuropathic Pain1.4 F ibromyalgia1.5 Chronic Musculoskeletal Pain2 DOSAGEANDADMINISTRATION2.1 I nitialTreatment2.2 M aintenance/Continuation/ExtendedTreatment2.3 Dosing in Special Populations2.4 D iscontinuingCymbalta2.5 Switching a Patient To or From a Monoamine OxidaseInhibitor (MAOI) Intended to Treat Psychiatric Disorders2.6 Use of Cymbalta with Other MAOIs such as Linezolid orMethylene Blue3 DOSAGE FORMS AND STRENGTHS4 CONTRAINDICATIONS4.1 Monoamine Oxidase Inhibitors (MAOIs)4.2 U ncontrolledNarrow-AngleGlaucoma5 WARNINGSANDPRECAUTIONS5.1 Suicidal Thoughts and Behaviors in Adolescents andYoung Adults5.2 H epatotoxicity5.3 Orthostatic Hypotension and Syncope5.4 S erotoninSyndrome5.5 A bnormalBleeding5.6 Severe Skin Reactions5.7 Discontinuation of Treatment with Cymbalta5.8 Activation of Mania/Hypomania5.9 S eizures5.10 Effect on Blood Pressure5.11 Clinically Important Drug Interactions5.12 H yponatremia5.13 Use in Patients with Concomitant Illness5.14 Urinary Hesitation and Retention5.15 L aboratoryTests6 ADVERSEREACTIONS6.1 Clinical Trial Data Sources6.2 Adverse Reactions Reported as Reasons forDiscontinuation of Treatment in Placebo-Controlled Trials6.3 Most Common Adverse Reactions6.4 Adverse Reactions Occurring at an Incidence of 5% orMore Among Duloxetine-Treated Patients in Placebo-Controlled Trials6.5 Adverse Reactions Occurring at an Incidence of 2% orMore Among Duloxetine-Treated Patients in Placebo-Controlled Trials6.6 Effects on Male and Female Sexual Function6.7 Vital Sign Changes6.8 W eightChanges6.9 L aboratoryChanges6.10 E lectrocardiogramChanges6.11 Other Adverse Reactions Observed During thePremarketing and Postmarketing Clinical Trial Evaluationof Duloxetine6.12 Postmarketing Spontaneous Reports7 DRUGINTERACTIONS7.1 Inhibitors of CYP1A27.2 Inhibitors of CYP2D67.3 Dual Inhibition of CYP1A2 and CYP2D67.4 Drugs that Interfere with Hemostasis (e.g., NSAIDs,Aspirin, and Warfarin)7.5 L orazepam7.6 T emazepam7.7 Drugs that Affect Gastric Acidity7.8 Drugs Metabolized by CYP1A27.9 Drugs Metabolized by CYP2D67.10 Drugs Metabolized by CYP2C97.11 Drugs Metabolized by CYP3A7.12 Drugs Metabolized by CYP2C197.13 Monoamine Oxidase Inhibitors (MAOIs)7.14 S erotonergicDrugs7.15 A lcohol7.16 C NSDrugs7.17 Drugs Highly Bound to Plasma Protein8 USE IN SPECIFIC POPULATIONS8.1 P regnancy8.2 Labor and Delivery8.3 N ursingMothers8.4 P ediatricUse8.5 G eriatricUse8.6 G ender8.7 S mokingStatus8.8 R ace8.9 H epaticInsufficiency8.10 Severe Renal Impairment9 DRUGABUSEANDDEPENDENCE9.2 A buse9.3 D ependence10 OVERDOSAGE10.1 Signs and Symptoms10.2 M anagementofOverdose11 DESCRIPTION12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.2 P harmacodynamics12.3 P harmacokinetics13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility14 CLINICAL STUDIES14.1 Major Depressive Disorder14.2 Generalized Anxiety Disorder14.3 Diabetic Peripheral Neuropathic Pain14.4 F ibromyalgia14.5 Chronic Musculoskeletal Pain16 HOW SUPPLIED/STORAGE AND HANDLING16.1 H owSupplied16.2 S torage17 PATIENT COUNSELING INFORMATION17.1 Information on Medication Guide17.2 Suicidal Thoughts and Behaviors17.3 M edicationAdministration17.4 Continuing the Therapy Prescribed17.5 H epatotoxicity17.6 A lcohol17.7 Orthostatic Hypotension and Syncope17.8 S erotoninSyndrome17.9 A bnormalBleeding17.10 Severe Skin Reaction17.11 Discontinuation of Treatment17.12 Activation of Mania or Hypomania17.13 Seizures17.14 Effects on Blood Pressure17.15 Concomitant Medications17.16 Hyponatremia17.17 Concomitant Illnesses17.18 Urinary Hesitancy and Retention17.19 Pregnancy and Breast Feeding17.20 Interference with Psychomotor Performance* Sections or subsections omitted from the full prescribing information are not listed.FULL PRESCRIBING INFORMATIONWARNING: SUICIDAL THOUGHTS AND BEHAVIORSAntidepressants increased the risk of suicidal thoughts and behavior in children, adolescents, and young adults in short-term studies. These studies did not show an increase in the risk of suicidal thoughts and behavior with antidepressant use in patients over age 24; there was a reduction in risk with antidepressant use in patients aged 65 and older [see Warnings and Precautions (5.1)].In patients of all ages who are started on antidepressant therapy, monitor closely for worsening, and for emergence of suicidal thoughts and behaviors. Advise families and caregivers of the need for close observation and communication with the prescriber [see Warnings and Precautions (5.1)].Cymbalta is not approved for use in pediatric patients [see Use in Specific Populations (8.4)].USAGEAND1 INDICATIONS1.1 Major Depressive DisorderCymbalta is indicated for the treatment of major depressive disorder (MDD). The efficacy of Cymbalta was established in four short-term and one maintenance trial in adults [see Clinical Studies (14.1)].A major depressive episode (DSM-IV) implies a prominent and relatively persistent (nearly every day for at least 2 weeks) depressed or dysphoric mood that usually interferes with daily functioning, and includes at least 5 of the following 9 symptoms: depressed mood, loss of interest in usual activities, significant change in weight and/or appetite, insomnia or hypersomnia, psychomotor agitation or retardation, increased fatigue, feelings of guilt or worthlessness, slowed thinking or impaired concentration, or a suicide attempt or suicidal ideation.AnxietyDisorder1.2 GeneralizedCymbalta is indicated for the treatment of generalized anxiety disorder (GAD). The efficacy of Cymbalta was established in three short-term trials and one maintenance trial in adults [see Clinical Studies (14.2)].Generalized anxiety disorder is defined by the DSM-IV as excessive anxiety and worry, present more days than not, for at least 6 months. The excessive anxiety and worry must be difficult to control and must cause significant distress or impairment in normal functioning. It must be associated with at least 3 of the following 6 symptoms: restlessness or feeling keyed up or on edge, being easily fatigued, difficulty concentrating or mind going blank, irritability, muscle tension, and/or sleep disturbance.1.3 Diabetic Peripheral Neuropathic PainCymbalta is indicated for the management of neuropathic pain (DPNP) associated with diabetic peripheral neuropathy [see Clinical Studies (14.3)].1.4 FibromyalgiaCymbalta is indicated for the management of fibromyalgia (FM) [see Clinical Studies (14.4)].PainMusculoskeletal1.5 ChronicCymbalta is indicated for the management of chronic musculoskeletal pain. This has been established in studies in patients with chronic low back pain (CLBP) and chronic pain due to osteoarthritis [see Clinical Studies (14.5)].2 DOSAGE AND ADMINISTRATIONCymbalta should be swallowed whole and should not be chewed or crushed, nor should the capsule be opened and its contents sprinkled on food or mixed with liquids. All of these might affect the enteric coating. Cymbalta can be given without regard to meals.Treatment2.1 InitialMajor Depressive Disorder — Cymbalta should be administered at a total dose of 40 mg/day (given as 20 mg twice daily) to 60 mg/day (given either once daily or as 30 mg twice daily). For some patients, it may be desirable to start at 30 mg once daily for 1 week, to allow patients to adjust to the medication before increasing to 60 mg once daily. While a 120 mg/day dose was shown to be effective, there is no evidence that doses greater than 60 mg/day confer any additional benefits. The safety of doses above 120 mg/day has not been adequately evaluated [see Clinical Studies (14.1)].Generalized Anxiety Disorder — For most patients, the recommended starting dose for Cymbalta is 60 mg administered once daily. For some patients, it may be desirable to start at 30 mg once daily for 1 week, to allow patients to adjust to the medication before increasing to 60 mg once daily. While a 120 mg once daily dose was shown to be effective, there is no evidence that doses greater than 60 mg/day confer additional benefit. Nevertheless, if a decision is made to increase the dose beyond 60 mg once daily, dose increases should be in increments of 30 mg once daily. The safety of doses above 120 mg once daily has not been adequately evaluated [see Clinical Studies (14.2)].Diabetic Peripheral Neuropathic Pain — The recommended dose for Cymbalta is 60 mg administered once daily. There is no evidence that doses higher than 60 mg confer additional significant benefit and the higher dose is clearly less well tolerated [see Clinical Studies (14.3)]. For patients for whom tolerability is a concern, a lower starting dose may be considered.Since diabetes is frequently complicated by renal disease, a lower starting dose and gradual increase in dose should be considered for patients with renal impairment [see Dosage and Administration (2.3), Use in Specific Populations (8.10), and Clinical Pharmacology (12.3)].Fibromyalgia — The recommended dose for Cymbalta is 60 mg administered once daily. Treatment should begin at 30 mg once daily for 1 week, to allow patients to adjust to the medication before increasing to 60 mg once daily. Some patients may respond to the starting dose. There is no evidence that doses greater than 60 mg/day confer additional benefit, even in patients who do not respond to a 60 mg dose, and higher doses are associated with a higher rate of adverse reactions [see Clinical Studies (14.4)].Chronic Musculoskeletal Pain — The recommended dose for Cymbalta is 60 mg once daily. Dosing may be started at 30 mg for one week, to allow patients to adjust to the medication before increasing to 60 mg once daily. There is no evidence that higher doses confer additional benefit, even in patients who do not respond to a 60 mg dose, and higher doses are associated with a higher rate of adverse reactions [see Clinical Studies (14.5)].Treatment2.2 M aintenance/Continuation/ExtendedMajor Depressive Disorder — It is generally agreed that acute episodes of major depression require several months or longer of sustained pharmacologic therapy. Maintenance of efficacy in MDD was demonstrated with Cymbalta as monotherapy. Cymbalta should be administered at a total dose of 60 mg once daily. Patients should be periodically reassessed to determine the need for maintenance treatment and the appropriate dose for such treatment [see Clinical Studies (14.1)].Generalized Anxiety Disorder — It is generally agreed that episodes of generalized anxiety disorder require several months or longer of sustained pharmacological therapy. Maintenance of efficacy in GAD was demonstrated with Cymbalta as monotherapy. Cymbalta should be administered in a dose range of 60-120 mg once daily. Patients should be periodically reassessed to determine the continued need for maintenance treatment and the appropriate dose for such treatment [see Clinical Studies (14.2)].Diabetic Peripheral Neuropathic Pain — As the progression of diabetic peripheral neuropathy is highly variable and management of pain is empirical, the effectiveness of Cymbalta must be assessed individually. Efficacy beyond 12 weeks has not been systematically studied in placebo-controlled trials.Fibromyalgia — Fibromyalgia is recognized as a chronic condition. The efficacy of Cymbalta in the management of fibromyalgia has been demonstrated in placebo-controlled studies up to 3 months. The efficacy of Cymbalta was not demonstrated in longer studies; however, continued treatment should be based on individual patient response.Chronic Musculoskeletal Pain — The efficacy of Cymbalta has not been established in placebo-controlled studies beyond 13 weeks.2.3 Dosing in Special PopulationsHepatic Insufficiency — It is recommended that Cymbalta should ordinarily not be administered to patients with any hepatic insufficiency [see Warnings and Precautions (5.13) and Use in Specific Populations (8.9)].Severe Renal Impairment — Cymbalta is not recommended for patients with end-stage renal disease or severe renal impairment (estimated creatinine clearance <30 mL/min) [see Warnings and Precautions (5.13) and Use in Specific Populations (8.10)].Elderly Patients — No dose adjustment is recommended for elderly patients on the basis of age. As with any drug, caution should be exercised in treating the elderly. When individualizing the dosage in elderly patients, extra care should be taken when increasing the dose [see Use in Specific Populations (8.5)].Pregnant Women — There are no adequate and well-controlled studies in pregnant women; therefore, Cymbalta should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus [see Use in Specific Populations (8.1)].Lilly maintains a pregnancy registry to monitor the pregnancy outcomes of women exposed to Cymbalta while pregnant. Healthcare providers are encouraged to register any patient who is exposed to Cymbalta during pregnancy by calling the Cymbalta Pregnancy Registry at 1-866-814-6975 or by visiting Nursing Mothers — Because the safety of duloxetine in infants is not known, nursing while on Cymbalta is not recommended [see Use in Specific Populations (8.3)].2.4 D iscontinuingCymbaltaSymptoms associated with discontinuation of Cymbalta and other SSRIs and SNRIs have been reported. A gradual reduction in the dose rather than abrupt cessation is recommended whenever possible [see Warnings and Precautions (5.7)].2.5 Switching a Patient To or From a Monoamine Oxidase Inhibitor (MAOI) Intended to Treat PsychiatricDisordersAt least 14 days should elapse between discontinuation of an MAOI intended to treat psychiatric disorders and initiation of therapy with Cymbalta. Conversely, at least 5 days should be allowed after stopping Cymbalta before starting an MAOI intended to treat psychiatric disorders [see Contraindications (4.1)].2.6 Use of Cymbalta with Other MAOIs such as Linezolid or Methylene BlueDo not start Cymbalta in a patient who is being treated with linezolid or intravenous methylene blue because there is an increased risk of serotonin syndrome. In a patient who requires more urgent treatment of a psychiatric condition, other interventions, including hospitalization, should be considered [see Contraindications (4.1)].In some cases, a patient already receiving Cymbalta therapy may require urgent treatment with linezolid or intravenous methylene blue. If acceptable alternatives to linezolid or intravenous methylene blue treatment are not available and the potential benefits of linezolid or intravenous methylene blue treatment are judged to outweigh the risks of serotonin syndrome in a particular patient, Cymbalta should be stopped promptly, and linezolid or intravenous methylene blue can be administered. The patient should be monitored for symptoms of serotonin syndrome for 5 days or until 24 hours after the last dose of linezolid or intravenous methylene blue, whichever comes first. Therapy with Cymbalta may be resumed 24 hours after the last dose of linezolid or intravenous methylene blue [see Warnings and Precautions (5.4)].The risk of administering methylene blue by non-intravenous routes (such as oral tablets or by local injection) or in intravenous doses much lower than 1 mg/kg with Cymbalta is unclear. The clinician should, nevertheless, be aware of the possibility of emergent symptoms of serotonin syndrome with such use [see Warnings and Precautions (5.4)].3 DOSAGE FORMS AND STRENGTHSCymbalta is available as delayed release capsules:20 mg opaque green capsules imprinted with “Lilly 3235 20mg”30 mg opaque white and blue capsules imprinted with “Lilly 3240 30mg”60 mg opaque green and blue capsules imprinted with “Lilly 3237 60mg”60 mg opaque green and blue capsules imprinted with “Lilly 3270 60mg”4 CONTRAINDICATIONS4.1 Monoamine Oxidase Inhibitors (MAOIs)The use of MAOIs intended to treat psychiatric disorders with Cymbalta or within 5 days of stopping treatment with Cymbalta is contraindicated because of an increased risk of serotonin syndrome. The use of Cymbalta within 14 days of stopping an MAOI intended to treat psychiatric disorders is also contraindicated [see Dosage and Administration (2.5) and Warnings and Precautions (5.4)].Starting Cymbalta in a patient who is being treated with MAOIs such as linezolid or intravenous methylene blue is also contraindicated because of an increased risk of serotonin syndrome [see Dosage and Administration (2.6) and Warnings and Precautions (5.4)].4.2 Uncontrolled Narrow-Angle GlaucomaIn clinical trials, Cymbalta use was associated with an increased risk of mydriasis; therefore, its use should be avoided in patients with uncontrolled narrow-angle glaucoma [see Warnings and Precautions (5.13)].PRECAUTIONS5 WARNINGSAND5.1 Suicidal Thoughts and Behaviors in Adolescents and Young AdultsPatients with major depressive disorder (MDD), both adult and pediatric, may experience worsening of their depression and/or the emergence of suicidal ideation and behavior (suicidality) or unusual changes in behavior, whether or not they are taking antidepressant medications, and this risk may persist until significant remission occurs. Suicide is a known risk of depression and certain other psychiatric disorders, and these disorders themselves are the strongest predictors of suicide. There has been a long-standing concern, however, that antidepressants may have a role in inducing worsening of depression and the emergence of suicidality in certain patients during the early phases of treatment.Pooled analyses of short-term placebo-controlled trials of antidepressant drugs (SSRIs and others) showed that these drugs increase the risk of suicidal thinking and behavior (suicidality) in children, adolescents, and young adults (ages 18-24) with major depressive disorder (MDD) and other psychiatric disorders. Short-term studies did not show an increase in the risk of suicidality with antidepressants compared to placebo in adults beyond age 24; there was a reduction with antidepressants compared to placebo in adults aged 65 and older.The pooled analyses of placebo-controlled trials in children and adolescents with MDD, obsessive compulsive disorder (OCD), or other psychiatric disorders included a total of 24 short-term trials of 9 antidepressant drugs in over 4400 patients. The pooled analyses of placebo-controlled trials in adults with MDD or other psychiatric disorders included a total of 295 short-term trials (median duration of 2 months) of 11 antidepressant drugs in over 77,000 patients. There was considerable variation in risk of suicidality among drugs, but a tendency toward an increase in the younger patients for almost all drugs studied. There were differences in absolute risk of suicidality across the different indications, with the highest incidence in MDD. The risk of differences (drug vs placebo), however, were relatively stable within age strata and across indications. These risk differences (drug-placebo difference in the number of cases of suicidality per 1000 patients treated) are provided in Table 1.Table 1Age Range Drug-Placebo Difference in Number of Cases ofSuicidality per 1000 Patients TreatedIncreases Compared to Placebo<18 14 additional cases18-24 5 additional cases Decreases Compared to Placebo25-64 1 fewer case≥65 6 fewer casesNo suicides occurred in any of the pediatric trials. There were suicides in the adult trials, but the number was notsufficient to reach any conclusion about drug effect on suicide.It is unknown whether the suicidality risk extends to longer-term use, i.e., beyond several months. However, thereis substantial evidence from placebo-controlled maintenance trials in adults with depression that the use ofantidepressants can delay the recurrence of depression.All patients being treated with antidepressants for any indication should be monitored appropriately andobserved closely for clinical worsening, suicidality, and unusual changes in behavior, especially during the initialfew months of a course of drug therapy, or at times of dose changes, either increases or decreases.The following symptoms, anxiety, agitation, panic attacks, insomnia, irritability, hostility, aggressiveness,impulsivity, akathisia (psychomotor restlessness), hypomania, and mania, have been reported in adult and pediatricpatients being treated with antidepressants for major depressive disorder as well as for other indications, both psychiatricand nonpsychiatric. Although a causal link between the emergence of such symptoms and either the worsening ofdepression and/or the emergence of suicidal impulses has not been established, there is concern that such symptomsmay represent precursors to emerging suicidality.Consideration should be given to changing the therapeutic regimen, including possibly discontinuing themedication, in patients whose depression is persistently worse, or who are experiencing emergent suicidality or symptomsthat might be precursors to worsening depression or suicidality, especially if these symptoms are severe, abrupt in onset,or were not part of the patient’s presenting symptoms.If the decision has been made to discontinue treatment, medication should be tapered, as rapidly as is feasible,but with recognition that discontinuation can be associated with certain symptoms [see Dosage and Administration (2.4)and Warnings and Precautions (5.7) for descriptions of the risks of discontinuation of Cymbalta].Families and caregivers of patients being treated with antidepressants for major depressive disorder orother indications, both psychiatric and nonpsychiatric, should be alerted about the need to monitor patients for the emergence of agitation, irritability, unusual changes in behavior, and the other symptoms described above, as well as the emergence of suicidality, and to report such symptoms immediately to health care providers. Such monitoring should include daily observation by families and caregivers. Prescriptions for Cymbalta should bewritten for the smallest quantity of capsules consistent with good patient management, in order to reduce therisk of overdose.Screening Patients for Bipolar Disorder — A major depressive episode may be the initial presentation of bipolardisorder. It is generally believed (though not established in controlled trials) that treating such an episode with anantidepressant alone may increase the likelihood of precipitation of a mixed/manic episode in patients at risk for bipolardisorder. Whether any of the symptoms described above represent such a conversion is unknown. However, prior toinitiating treatment with an antidepressant, patients with depressive symptoms should be adequately screened todetermine if they are at risk for bipolar disorder; such screening should include a detailed psychiatric history, including afamily history of suicide, bipolar disorder, and depression. It should be noted that Cymbalta (duloxetine) is not approvedfor use in treating bipolar depression.5.2 HepatotoxicityThere have been reports of hepatic failure, sometimes fatal, in patients treated with Cymbalta. These cases havepresented as hepatitis with abdominal pain, hepatomegaly, and elevation of transaminase levels to more than twenty times the upper limit of normal with or without jaundice, reflecting a mixed or hepatocellular pattern of liver injury. Cymbalta should be discontinued in patients who develop jaundice or other evidence of clinically significant liver dysfunction and should not be resumed unless another cause can be established.Cases of cholestatic jaundice with minimal elevation of transaminase levels have also been reported. Otherpostmarketing reports indicate that elevated transaminases, bilirubin, and alkaline phosphatase have occurred in patientswith chronic liver disease or cirrhosis.Cymbalta increased the risk of elevation of serum transaminase levels in development program clinical trials. Livertransaminase elevations resulted in the discontinuation of 0.3% (89/29,435) of Cymbalta-treated patients. In mostpatients, the median time to detection of the transaminase elevation was about two months. In placebo-controlled trials in any indication, for patients with normal and abnormal baseline ALT values, elevation of ALT >3 times the upper limit of normal occurred in 1.37% (132/9611) of Cymbalta-treated patients compared to 0.49% (35/7182) of placebo-treated patients. In placebo-controlled studies using a fixed dose design, there was evidence of a dose response relationship for ALT and AST elevation of >3 times the upper limit of normal and >5 times the upper limit of normal, respectively.。
盐酸西那卡塞FDA说明书
__________________________________________________________________________________________________________________________________FDA approved label August 1, 2011HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use Sensipar safely and effectively. See full prescribing information for Sensipar. Sensipar ® (cinacalcet) Tablets Initial US Approval: 2004 ----------------------------RECENT MAJOR CHANGES -------------------------Indications and Usage: Primary Hyperparathyroidism (1.3)02/2011 Dosage and Administration: Parathyroid Carcinoma / PrimaryHyperparathyroidism (2.2) 02/2011 Contraindications: Hypocalcemia (4) 02/2011 ----------------------------INDICATIONS AND USAGE--------------------------- Sensipar is a calcium-sensing receptor agonist indicated for:•Secondary Hyperparathyroidism (HPT) in patients with chronic kidney disease (CKD) on dialysis. (1.1)•Hypercalcemia in patients with Parathyroid Carcinoma (PC). (1.2) •Severe hypercalcemia in patients with primary HPT who are unable to undergo parathyroidectomy. (1.3)----------------------DOSAGE AND ADMINISTRATION-----------------------For all indications, Sensipar should be taken with food or shortly after a mealand should always be taken whole and not divided.•Secondary HPT in patients with CKD on dialysis (2.1): oStarting dose is 30 mg once daily. oTitrate dose no more frequently than every 2 to 4 weeks through sequential doses of 30, 60, 90, 120, and 180 mg once daily as necessary to achieve targeted intact parathyroid hormone (iPTH) levels.oiPTH levels should be measured no earlier than 12 hours after most recent dose.•Hypercalcemia in patients with PC or severe hypercalcemia in patients with primary HPT (2.2):oStarting dose is 30 mg twice daily. oTitrate dose every 2 to 4 weeks through sequential doses of 30 mg twice daily, 60 mg twice daily, 90 mg twice daily, and 90 mg three orfour times daily as necessary to normalize serum calcium levels.---------------------DOSAGE FORMS AND STRENGTHS---------------------- Tablets: 30, 60, and 90 mg tablets (3) -------------------------------CONTRAINDICATIONS ---------------------------- Hypocalcemia: Sensipar treatment should not be initiated if serum calcium isless than the lower limit of the normal range. (4, 5.1)-----------------------WARNINGS AND PRECAUTIONS-----------------------• Hypocalcemia and/or seizures: May occur due to significant reductions inserum calcium. (5.1, 5.2) • Isolated, idiosyncratic occurrences of hypotension, worsening heart failure, and/or arrhythmia: Have been reported in patients with impaired cardiacfunction during Sensipar treatment, which may be mediated by reductionsin serum calcium. (5.3)• Adynamic bone disease: May develop if iPTH levels are suppressed below100 pg/mL. (5.4)• Laboratory tests: Serum calcium, serum phosphorus, and iPTH levelsshould be monitored during the dose initiation, dose titration, and maintenance therapy. (5.6) • Hepatic Impairment: Cinacalcet exposure is increased in patients withmoderate and severe hepatic impairment. Patients should be closelymonitored throughout treatment. (5.5, 8.7)------------------------------ADVERSE REACTIONS------------------------------- The most frequently reported adverse reactions (incidence in patients ≥ 5% inthe Sensipar group) were nausea, vomiting, and diarrhea. (6.1, 6.2)To report SUSPECTED ADVERSE REACTIONS, contact AmgenMedical Information at 1-800-77-AMGEN (1-800-772-6436) or FDA at1-800-FDA-1088 or/medwatch . ------------------------------DRUG INTERACTIONS-------------------------------• Co-administration with a strong CYP3A4 inhibitor may increase serumlevels of cinacalcet. Dose adjustment and monitoring of iPTH serumphosphorous and serum calcium may be required. (7.1)• Cinacalcet is a strong inhibitor of CYP2D6. Dose adjustments may berequired for concomitant medications that are predominantly metabolizedby CYP2D6. (7.2) -----------------------------USE IN SPECIFIC POPULATIONS------------------ • Pregnancy: Sensipar should only be used if the potential benefit justifiesthe potential risk to the fetus. Pregnancy registry available. (8.1)See 17 for PATIENT COUNSELING INFORMATION Revised:08/2011 FULL PRESCRIBING INFORMATION: CONTENTS*1 I NDICATIONS AND USAGE1.1 Secondary Hyperparathyroidism 1.2 P arathyroid Carcinoma 1.3 P rimary Hyperparathyroidism2 D OSAGE AND ADMINISTRATION2.1 S econdary Hyperparathyroidism in Patients with Chronic KidneyDisease on Dialysis 2.2 Parathyroid Carcinoma and Primary Hyperparathyroidism3 DOSAGE FORMS AND STRENGTHS4 CONTRAINDICATIONS5 WARNINGS AND PRECAUTIONS5.1 H ypocalcemia5.2 S eizures5.3 Hypotension and/or Worsening Heart Failure5.4 Adynamic Bone Disease 5.5 H epatic Impairment 5.6 Laboratory Tests6 A DVERSE REACTIONS6.1 Clinical Trials Experience6.2 Postmarketing Experience with Sensipar7 D RUG INTERACTIONS7.1 Strong CYP3A4 Inhibitors 7.2 CYP2D6 Substrates8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy: Category C8.3 N ursing Mothers 8.4 P ediatric Use 8.6 R enal Impairment 8.7 H epatic Impairment 10 OVERDOSAGE 11 DESCRIPTION12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action 12.2 Pharmacodynamics 12.3 Pharmacokinetics 13 N ONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility 14 C LINICAL STUDIES 14.1 Secondary Hyperparathyroidism in Patients with Chronic Kidney Disease on Dialysis 14.2 Parathyroid Carcinoma 14.3 Patients with Severe Hypercalcemia Due to Primary Hyperparathyroidism 16 HOW SUPPLIED/STORAGE AND HANDLING 17PATIENT COUNSELING INFORMATION *Sections or subsections omitted from the full prescribing information are not listed.1 FULL PRESCRIBING INFORMATION INDICATIONS AND USAGE 1.1 Secondary Hyperparathyroidism Sensipar is indicated for the treatment of secondary hyperparathyroidism (HPT) in patients with chronic kidney disease (CKD) on dialysis [see Clinical Studies (14.1)]. 1.2 Parathyroid Carcinoma Sensipar is indicated for the treatment of hypercalcemia in patients with Parathyroid Carcinoma [see Clinical Studies (14.2)]. 1.3 Primary Hyperparathyroidism Sensipar is indicated for the treatment of severe hypercalcemia in patients with primary HPT who are unable to undergo parathyroidectomy [see Clinical Studies (14.3)]. 2 DOSAGE AND ADMINISTRATION Sensipar tablets should be taken whole and should not be divided. Sensipar should be taken with food orshortly after a meal. Dosage must be individualized. 2.1 Secondary Hyperparathyroidism in Patients with Chronic Kidney Disease on DialysisThe recommended starting oral dose of Sensipar is 30 mg once daily. Serum calcium and serum phosphorusshould be measured within 1 week and intact parathyroid hormone (iPTH) should be measured 1 to 4 weeksafter initiation or dose adjustment of Sensipar. Sensipar should be titrated no more frequently than every2 to 4 weeks through sequential doses of 30, 60, 90, 120, and 180 mg once daily to target iPTH levels of150 to 300 pg/mL. Serum iPTH levels should be assessed no earlier than 12 hours after dosing with Sensipar. Sensipar can be used alone or in combination with vitamin D sterols and/or phosphate binders.During dose titration, serum calcium levels should be monitored frequently and if levels decrease below thenormal range, appropriate steps should be taken to increase serum calcium levels, such as by providingsupplemental calcium, initiating or increasing the dose of calcium-based phosphate binder, initiating orincreasing the dose of vitamin D sterols, or temporarily withholding treatment with Sensipar [see Warnings andPrecautions (5.1, 5.6)]. 2.2 Parathyroid Carcinomaand Primary Hyperparathyroidism The recommended starting oral dose of Sensipar is 30 mg twice daily. The dose of Sensipar should be titrated every 2 to 4 weeks through sequential doses of 30 mg twice daily, 60 mg twice daily, and 90 mg twice daily, and 90 mg 3 or 4 times daily as necessary to normalize serum calcium levels [see Warnings and Precautions (5.6)].DOSAGE FORMS AND STRENGTHS Sensipar tablets are formulated as light-green, film-coated, oval-shaped tablets marked with “AMG” on one sideand “30” or “60” or “90” on the opposite side of the 30 mg, 60 mg, or 90 mg strengths, respectively.34 CONTRAINDICATIONSHypocalcemia: Sensipar treatment should not be initiated if serum calcium is less than the lower limit of the normal range [see Warnings and Precautions (5.1)].5 WARNINGS AND PRECAUTIONS5.1 HypocalcemiaSensipar lowers serum calcium and, therefore, patients should be carefully monitored for the occurrence of hypocalcemia. Potential manifestations of hypocalcemia include paresthesias, myalgias, muscle cramping, tetany, and convulsions.Serum calcium should be measured within 1 week after initiation or dose adjustment of Sensipar. Once the maintenance dose has been established, serum calcium should be measured approximately monthly [see Dosage and Administration (2.1)].If serum calcium falls below 8.4 mg/dL but remains above 7.5 mg/dL, or if symptoms of hypocalcemia occur, calcium-containing phosphate binders and/or vitamin D sterols can be used to raise serum calcium. If serum calcium falls below 7.5 mg/dL, or if symptoms of hypocalcemia persist and the dose of vitamin D cannot be increased, withhold administration of Sensipar until serum calcium levels reach 8.0 mg/dL and/or symptoms of hypocalcemia have resolved. Treatment should be reinitiated using the next lowest dose of Sensipar [see Dosage and Administration (2.1)].In 26-week studies of patients with CKD on dialysis, 66% of patients receiving Sensipar compared with 25% of patients receiving placebo developed at least one serum calcium value < 8.4 mg/dL. Less than 1% of patients in each group permanently discontinued study drug due to hypocalcemia.Sensipar is not indicated for patients with CKD not on dialysis. In patients with secondary HPT and CKD not on dialysis, the long term safety and efficacy of Sensipar have not been established. Clinical studies indicate that Sensipar-treated patients with CKD not on dialysis have an increased risk for hypocalcemia compared with Sensipar-treated patients with CKD on dialysis, which may be due to lower baseline calcium levels. In a phase 3 study of 32 weeks duration and including 404 patients with CKD not on dialysis (302 cinacalcet,102 placebo), in which the median dose for cinacalcet was 60 mg per day at the completion of the study, 80% of Sensipar-treated patients experienced at least one serum calcium value < 8.4 mg/dL compared with 5% of patients receiving placebo.5.2 SeizuresIn clinical studies, seizures (primarily generalized or tonic-clonic) were observed in 1.4% (43/3049) of Sensipar-treated patients and 0.7% (5/687) of placebo-treated patients. While the basis for the reported difference in seizure rate is not clear, the threshold for seizures is lowered by significant reductions in serum calcium levels. Therefore, serum calcium levels should be closely monitored in patients receiving Sensipar, particularly in patients with a history of a seizure disorder [see Warnings and Precautions (5.1)].5.3 Hypotension and/or Worsening Heart FailureIn postmarketing safety surveillance, isolated, idiosyncratic cases of hypotension, worsening heart failure,and/or arrhythmia have been reported in patients with impaired cardiac function, in which a causal relationship to Sensipar could not be completely excluded and which may be mediated by reductions in serum calcium levels [see Adverse Reactions (6.2)].5.4 Adynamic Bone DiseaseAdynamic bone disease may develop if iPTH levels are suppressed below 100 pg/mL. One clinical study evaluated bone histomorphometry in patients treated with Sensipar for 1 year. Three patients with mildhyperparathyroid bone disease at the beginning of the study developed adynamic bone disease during treatment with Sensipar. Two of these patients had iPTH levels below 100 pg/mL at multiple time points during the study. In three 6-month, phase 3 studies conducted in patients with CKD on dialysis, 11% of patients treated with Sensipar had mean iPTH values below 100 pg/mL during the efficacy-assessment phase. If iPTH levels decrease below 150 pg/mL in patients treated with Sensipar, the dose of Sensipar and/or vitamin D sterols should be reduced or therapy discontinued.5.5 Hepatic ImpairmentCinacalcet exposure, as defined by the Area Under the Curve (AUC0-inf), is increased by 2.4 and 4.2 fold in patients with moderate and severe hepatic impairment, respectively. These patients should be monitored throughout treatment with Sensipar [see Use in Specific Populations (8.7) and Clinical Pharmacology (12.3)].5.6 Laboratory TestsSecondary Hyperparathyroidism in Patients with Chronic Kidney Disease on DialysisSerum calcium and serum phosphorus should be measured within 1 week and iPTH should be measured 1 to4 weeks after initiation or dose adjustment of Sensipar. Once the maintenance dose has been established, serum calcium and serum phosphorus should be measured approximately monthly, and iPTH every 1 to 3 months [see Dosage and Administration (2.1)]. Measurements of PTH during the Sensipar studies were obtained using the Nichols iPTH immunoradiometric assay (IRMA).In patients with end-stage renal disease, testosterone levels are often below the normal range. In aplacebo-controlled study in patients with CKD on dialysis, there were reductions in total and free testosterone in male patients following 6 months of treatment with Sensipar. Levels of total testosterone decreased by a median of 15.8% in the Sensipar-treated patients and by 0.6% in the placebo-treated patients. Levels of free testosterone decreased by a median of 31.3% in the Sensipar-treated patients and by 16.3% in the placebo-treated patients. The clinical significance of these reductions in serum testosterone is unknown.Patients with Parathyroid Carcinoma or Primary HyperparathyroidismSerum calcium should be measured within 1 week after initiation or dose adjustment of Sensipar. Once maintenance dose levels have been established, serum calcium should be measured every 2 months [see Dosage and Administration (2.2)].REACTIONS6 ADVERSE6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared with rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.Secondary Hyperparathyroidism in Patients with Chronic Kidney Disease on DialysisIn three double-blind, placebo-controlled clinical trials, 1126 patients with CKD on dialysis received study drug (656 Sensipar, 470 placebo) for up to 6 months. The most frequently reported adverse reactions (incidence of at least 5% in the Sensipar group and greater than placebo) are provided in Table 1. The most frequently reported adverse reactions in the Sensipar group were nausea, vomiting, and diarrhea.Seizures were observed in 1.4% (13/910) of cinacalcet-treated patients and 0.7% (5/641) of placebo-treated patients across all completed placebo controlled trials.Table 1. Adverse Reaction Incidence (≥ 5%) in Patients on DialysisEvent*: Placebo(n = 470) (%)Sensipar (n = 656) (%) Nausea Vomiting Diarrhea Myalgia Dizziness Hypertension Asthenia Anorexia Pain Chest, Non-Cardiac Access Infection 19 15 20 14 8 5 4 4 4 431 27 21 15 10 7 7 6 6 5 The incidence of serious adverse reactions was similar in the Sensipar and placebo groups (29% vs. 31%,respectively). 12-Month Experience with Sensipar in Secondary HyperparathyroidismTwo hundred sixty-six patients from two of the phase 3 studies in patients with CKD on dialysis continued toreceive Sensipar or placebo treatment in a 6-month, double-blind extension study (12-month total treatmentduration). The incidence and nature of adverse reactions in this long term extension study were comparable tothose observed in the original phase 3 studies. Parathyroid Carcinoma and Primary HyperparathyroidismThe safety profile of Sensipar in these patient populations is generally consistent with that seen in patients withCKD on dialysis. Forty six patients were treated with cinacalcet in a single arm study, 29 with ParathyroidCarcinoma and 17 with intractable pHPT. Nine (20%) of the patients withdrew from the study due to adverseevents. The most frequent adverse reactions and the most frequent cause of withdrawal in these patient populations were nausea and vomiting. Severe or prolonged cases of nausea and vomiting can lead todehydration and worsening hypercalcemia so careful monitoring of electrolytes is recommended in patientswith these symptoms. Eight patients died while on study, 7 with Parathyroid Carcinoma (24%) and 1 (6%) with intractable pHPT.Causes of death were cardiovascular (5 patients), multi-organ failure (1 patient), gastrointestinal hemorrhage(1 patient) and metastatic carcinoma (1 patient). Adverse events of hypocalcemia were reported in threepatients (7%). Seizures were observed in 0.7% (1/140) of cinacalcet-treated patients and 0.0% (0/46) of placebo-treated patients in all clinical studies.Table 2. Adverse Reactions Occurring in ≥10% of Total SubjectsCinacalcetParathyroid IntractableCarcinoma pHPT Total Preferred Term (N=29) (N=17) (N=46)n (%) n (%) n (%) Number of Subjects Reporting Adverse 28 (97) 17 (100) 45 (98) EventsNausea 19 (66) 10 (59) 29 (63) Vomiting 15 (52) 6 (35) 21 (46) Paresthesia 4 (14) 5 (29) 9 (20) Fatigue 6 (21) 2 (12) 8 (17) Fracture 6 (21) 2 (12) 8 (17) Hypercalcemia 6 (21) 2 (12) 8 (17) Anorexia 6 (21) 1 (6) 7 (15) Asthenia 5 (17) 2 (12) 7 (15) Dehydration 7 (24) 0 (0) 7 (15) Anemia 5 (17) 1 (6) 6 (13) Arthralgia 5 (17) 1 (6) 6 (13) Constipation 3 (10) 3 (18) 6 (13) Depression 3 (10) 3 (18) 6 (13) Headache 6 (21) 0 (0) 6 (13) Infection Upper Respiratory 3 (10) 2 (12) 5 (11) Pain Limb 3 (10) 2 (12) 5 (11)6.2 Postmarketing Experience with SensiparThe following adverse reactions have been identified during postapproval use of Sensipar. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.Rash, hypersensitivity reactions (including angioedema and urticaria), diarrhea, and myalgia have been identified as adverse reactions during postapproval use of Sensipar. Isolated, idiosyncratic cases of hypotension, worsening heart failure, and/or arrhythmia have been reported in Sensipar-treated patients with impaired cardiac function in postmarketing safety surveillance.INTERACTIONSDRUG77.1 Strong CYP3A4 InhibitorsCinacalcet is partially metabolized by CYP3A4. Dose adjustment of Sensipar may be required if a patient initiates or discontinues therapy with a strong CYP3A4 inhibitor (e.g., ketoconazole, itraconazole). The iPTH and serum calcium concentrations should be closely monitored in these patients [see Clinical Pharmacology (12.3)].7.2 CYP2D6 SubstratesCinacalcet is a strong inhibitor of CYP2D6. Dose adjustments may be required for concomitant medications that are predominantly metabolized by CYP2D6 (e.g., desipramine, metoprolol, and carvedilol) and particularly those with a narrow therapeutic index (e.g., flecainide and most tricyclic antidepressants) [see Clinical Pharmacology (12.3)].8 USESPECIFIC POPULATIONSIN8.1 Pregnancy: Category CIn pregnant female rats given oral gavage doses of 2, 25, 50 mg/kg/day cinacalcet during gestation, no teratogenicity was observed at doses up to 50 mg/kg/day (exposure 4 times those resulting with a human oral dose of 180 mg/day based on Area Under the Curve [AUC] comparison). Decreased fetal body weights were observed at all doses (less than 1 to 4 times a human oral dose of 180 mg/day based on AUC comparison) in conjunction with maternal toxicity (decreased food consumption and body weight gain).In pregnant female rabbits given oral gavage doses of 2, 12, 25 mg/kg/day cinacalcet during gestation, no adverse fetal effects were observed (exposures less than with a human oral dose of 180 mg/day based on AUC comparisons). Reductions in maternal food consumption and body weight gain were seen at doses of12 and 25 mg/kg/day. Sensipar has been shown to cross the placental barrier in rabbits.In pregnant rats given oral gavage doses of 5, 15, 25 mg/kg/day cinacalcet during gestation through lactation, no adverse fetal or pup (post-weaning) effects were observed at 5 mg/kg/day (exposures less than with a human therapeutic dose of 180 mg/day based on AUC comparisons). Higher doses of 15 and 25 mg/kg/day cinacalcet (exposures 2 to 3 times a human oral dose of 180 mg/day based on AUC comparisons) were accompanied by maternal signs of hypocalcemia (periparturient mortality and early postnatal pup loss), and reductions in postnatal maternal and pup body-weight gain.There are no adequate and well-controlled studies of Sensipar in pregnant women. Sensipar should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.Women who become pregnant during Sensipar treatment are encouraged to enroll in Amgen’s Pregnancy Surveillance Program. Patients or their physicians should call 1-800-77-AMGEN (1-800-772-6436) to enroll.Mothers8.3 NursingStudies in rats have shown that Sensipar is excreted in the milk with a high milk-to-plasma ratio. It is not known whether this drug is excreted in human milk. Considering these data in rats, and because many drugs are excreted in human milk and there is a potential for clinically significant adverse reactions in infants who ingest Sensipar, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the lactating woman.8.4 Pediatric UseThe safety and efficacy of Sensipar in pediatric patients have not been established.Use8.5 GeriatricOf the 1136 patients enrolled in the Sensipar phase 3 clinical program in patients with CKD on dialysis,26% were ≥ 65 years old, and 9% were ≥ 75 years old. No differences in the safety and efficacy of Sensipar were observed in patients greater or less than 65 years of age. No dosage adjustment is required for geriatric patients [see Clinical Pharmacology (12.3)].8.6 RenalImpairmentNo dosage adjustment is necessary for renal impairment [see Clinical Pharmacology (12.3)].Impairment8.7 HepaticPatients with moderate and severe hepatic impairment should have serum calcium, serum phosphorus, and iPTH levels monitored closely throughout treatment with Sensipar because cinacalcet exposure (AUC0-inf) is increased by 2.4 and 4.2 fold, respectively, in these patients [see Warnings and Precautions (5.5) and Clinical Pharmacology (12.3)].10 OVERDOSAGEDoses titrated up to 300 mg once daily have been safely administered to patients on dialysis. Overdosage of Sensipar may lead to hypocalcemia. In the event of overdosage, patients should be monitored for signs and symptoms of hypocalcemia and appropriate measures taken to correct serum calcium levels [see Warnings and Precautions (5.1)].Since Sensipar is highly protein bound, hemodialysis is not an effective treatment for overdosage of Sensipar.11 DESCRIPTIONSensipar (cinacalcet) is a calcimimetic agent that increases the sensitivity of the calcium-sensing receptor to activation by extracellular calcium. Sensipar tablets contain the hydrochloride salt of cinacalcet. Its empirical formula is C22H22F3N⋅HCl with a molecular weight of 393.9 g/mol (hydrochloride salt) and 357.4 g/mol (free base). It has one chiral center having an R-absolute configuration. The R-enantiomer is the more potent enantiomer and has been shown to be responsible for pharmacodynamic activity.The hydrochloride salt of cinacalcet is a white to off-white, crystalline solid that is soluble in methanol or 95% ethanol and slightly soluble in water.Sensipar tablets are formulated as light-green, film-coated, oval-shaped tablets for oral administration in strengths of 30 mg, 60 mg, and 90 mg of cinacalcet as the free base equivalent (33 mg, 66 mg, and 99 mg as the hydrochloride salt, respectively).The hydrochloride salt of cinacalcet is described chemically as N-[1-(R)-(-)-(1-naphthyl)ethyl]-3-[3(trifluoromethyl)phenyl]-1-aminopropane hydrochloride and has the following structural formula:Inactive IngredientsThe following are the inactive ingredients in Sensipar tablets: pre-gelatinized starch, microcrystalline cellulose, povidone, crospovidone, colloidal silicon dioxide and magnesium stearate. Tablets are coated with color (Opadry® II green), clear film coat (Opadry® clear), and carnauba wax.PHARMACOLOGY12 CLINICAL12.1 Mechanism of ActionSecondary HPT in patients with CKD is a progressive disease, associated with increases in PTH levels and derangements in calcium and phosphorus metabolism. Increased PTH stimulates osteoclastic activity resultingin cortical bone resorption and marrow fibrosis. The goals of treatment of secondary HPT are to lower the levels of PTH, calcium, and phosphorus in the blood in order to prevent progressive bone disease and the systemic consequences of disordered mineral metabolism. Reductions in PTH are associated with a decrease in bone turnover and bone fibrosis in patients with CKD on dialysis and uncontrolled secondary HPT.The calcium-sensing receptor on the surface of the chief cell of the parathyroid gland is the principal regulator of PTH synthesis and secretion. Sensipar directly lowers PTH levels by increasing the sensitivity of the calcium-sensing receptor to extracellular calcium. The reduction in PTH is associated with a concomitant decrease in serum calcium levels. Measurements of PTH during the Sensipar studies were obtained using the Nichols IRMA.12.2 PharmacodynamicsReduction in iPTH levels correlated with the plasma cinacalcet concentrations in patients with CKD. The nadir in iPTH level occurs approximately 2 to 6 hours post dose, corresponding with the maximum plasma concentration (C max) of cinacalcet. After steady-state cinacalcet concentrations are reached (which occurs within 7 days of dose change), serum calcium concentrations remain constant over the dosing interval in patients with CKD.12.3 PharmacokineticsAbsorption and DistributionAfter oral administration of cinacalcet, C max is achieved in approximately 2 to 6 hours. Cinacalcet C max and AUC(0-inf) were increased by 82% and 68%, respectively, following administration with a high-fat meal compared with fasting in healthy volunteers. The C max and AUC(0-inf) of cinacalcet were increased by65% and 50%, respectively, when cinacalcet was administered with a low-fat meal compared with fasting. After absorption, cinacalcet concentrations decline in a biphasic fashion with a terminal half-life of30 to 40 hours. Steady-state drug levels are achieved within 7 days, and the mean accumulation ratio is approximately 2 with once daily oral administration. The median accumulation ratio is approximately 2 to 5 with twice daily oral administration. The AUC and C max of cinacalcet increase proportionally over the dose range of 30 to 180 mg once daily. The pharmacokinetic profile of cinacalcet does not change over time with once daily dosing of 30 to 180 mg. The volume of distribution is approximately 1000 L, indicating extensive distribution. Cinacalcet is approximately 93% to 97% bound to plasma protein(s). The ratio of blood cinacalcet concentration to plasma cinacalcet concentration is 0.80 at a blood cinacalcet concentration of 10 ng/mL. Metabolism and ExcretionCinacalcet is metabolized by multiple enzymes, primarily CYP3A4, CYP2D6, and CYP1A2. After administration of a 75 mg radiolabeled dose to healthy volunteers, cinacalcet was metabolized via: 1) oxidative N-dealkylation to hydrocinnamic acid and hydroxy-hydrocinnamic acid, which are further metabolized viaβ-oxidation and glycine conjugation; the oxidative N-dealkylation process also generates metabolites that contain the naphthalene ring; and 2) oxidation of the naphthalene ring on the parent drug forming dihydrodiols, which are further conjugated with glucuronic acid. The plasma concentrations of the major circulating metabolites, including the cinnamic acid derivatives and glucuronidated dihydrodiols, markedly exceed the parent drug concentrations. The hydrocinnamic acid metabolite and glucuronide conjugates have minimal or no calcimimetic activity. Renal excretion of metabolites was the primary route of elimination of radioactivity. Approximately 80% of the dose was recovered in the urine and 15% in the feces.Drug InteractionsIn vitro studies indicate that cinacalcet is a strong inhibitor of CYP2D6, but not an inhibitor of CYP1A2,CYP2C9, CYP2C19, and CYP3A4. In vitro induction studies indicate that cinacalcet is not an inducer ofCYP450 enzymes. Tables 3 and 4 list the findings from in vivo drug-drug interaction studies.。
帕博西尼(Ibrance,Palbociclib)FDA 官方说明书
帕博西尼(Ibrance,Palbociclib)FDA官方说明书1 适应症和用途IBRANCE是适用与来曲唑联用对有雌激素受体(ER)-阳性,人表皮生长因子受体2(HER2)-阴性晚期乳癌绝经后妇女作为初始基于内分泌治疗对其转移疾病的治疗。
这个适应症是根据无进展生存(PFS)在加速批准下被批准的[见临床研究(14)]。
对此适应症的继续批准可能取决于在验证性试验中临床获益的证明和描述。
2 剂量和给药方法2.1 一般给药信息IBRANCE的推荐剂量是一粒125 mg胶囊口服服用每天一次共21天,接着不用治疗7天组成一个28天完整疗程。
IBRANCE应与食物服用[见临床药理学(12.3)]与来曲唑2.5 mg每天一次联用连续28-天疗程自始至终给予。
应鼓励患者在每天接近相同时间服用他们的剂量。
如患者呕吐或丢失一剂,在那天不应服用另外剂量。
在寻常的时间服用下一次处方剂量。
IBRANCE胶囊应被整吞(在吞咽前不要咀嚼,压碎或打开胶囊)。
如破碎,压碎或不完整时不应摄入胶囊。
2.2 剂量调整建议根据个体安全性和耐受性调整IBRANCE剂量[见警告和注意事项(5)]。
某些不良反应的处理[见警告和注意事项(5)]可能需要暂时中断剂量/延迟和/或减低剂量,或永久终止如同表1,2和3提供每种剂量减低计划[见警告和注意事项(5),不良反应(6)和临床研究(14)]。
见制造商处方资料对共同给药产品,来曲唑,在毒性事件中剂量调整指导原则和其他相关安全性资料或禁忌证。
为与强CYP3A抑制剂使用剂量调整避免强CYP3A抑制剂的同时使用和考虑没有或小CYP3A抑制作用另外同时药物。
如患者必须用强CYP3A抑制剂共同给药,减低IBRANC剂量至75 mg每天一次。
如强抑制剂被终止,增加IBRANCE剂量(抑制剂的3–5个半衰期后)至强CYP3A抑制剂使用前剂量[见药物相互作用(7.1)和临床药理学(12.3)]。
3 剂型和规格125 mg胶囊:不透明硬明胶胶囊,大小0,有焦糖帽和体,帽上用白墨汁印,体上“PBC 125”。
碧云天生物技术 PreScission Protease 产品说明书
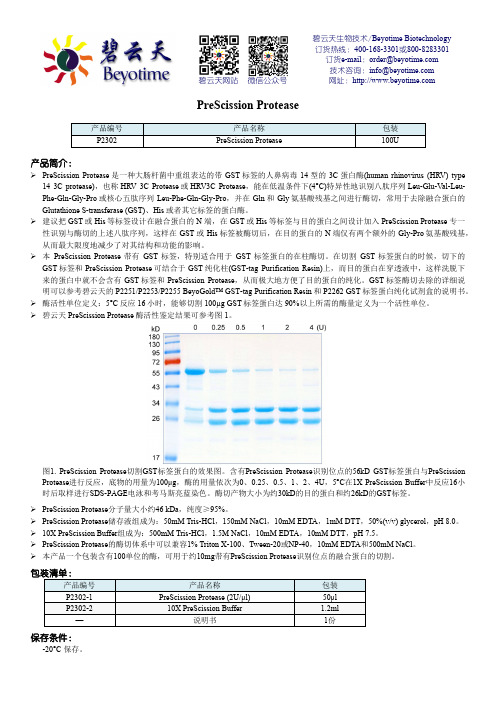
碧云天生物技术/Beyotime Biotechnology订货热线:400-168-3301或800-8283301订货e-mail:******************技术咨询:*****************碧云天网站微信公众号网址:PreScission Protease产品编号产品名称包装P2302 PreScission Protease 100U产品简介:PreScission Protease是一种大肠杆菌中重组表达的带GST标签的人鼻病毒14型的3C蛋白酶(human rhinovirus (HRV) type14 3C protease),也称HRV 3C Protease或HRV3C Protease,能在低温条件下(4°C)特异性地识别八肽序列Leu-Glu-Val-Leu-Phe-Gln-Gly-Pro或核心五肽序列Leu-Phe-Gln-Gly-Pro,并在Gln和Gly氨基酸残基之间进行酶切,常用于去除融合蛋白的Glutathione S-transferase (GST)、His或者其它标签的蛋白酶。
建议把GST或His等标签设计在融合蛋白的N 端,在GST或His等标签与目的蛋白之间设计加入PreScission Protease 专一性识别与酶切的上述八肽序列,这样在GST或His标签被酶切后,在目的蛋白的N端仅有两个额外的Gly-Pro氨基酸残基,从而最大限度地减少了对其结构和功能的影响。
本PreScission Protease带有GST标签,特别适合用于GST标签蛋白的在柱酶切。
在切割GST标签蛋白的时候,切下的GST标签和PreScission Protease可结合于GST纯化柱(GST-tag Purification Resin)上,而目的蛋白在穿透液中,这样洗脱下来的蛋白中就不会含有GST标签和PreScission Protease,从而极大地方便了目的蛋白的纯化。
利塞膦酸钠FDA说明书

____________________________________________________________________________________________________________________________________ HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to useACTONEL safely and effectively. See full prescribing information forACTONEL. ACTONEL ® (risedronate sodium) tabletsInitial U.S. Approval: 1998----------------------------RECENT MAJOR CHANGES--------------------------Warnings and Precautions (5.3) 7/2009 ----------------------------INDICATIONS AND USAGE---------------------------ACTONEL is a bisphosphonate indicated for: •Treatment and prevention of postmenopausal osteoporosis (1.1), •Treatment to increase bone mass in men with osteoporosis (1.2), •Treatment and prevention of glucocorticoid-induced osteoporosis (1.3), •Treatment of Paget’s disease (1.4). ----------------------DOSAGE AND ADMINISTRATION-----------------------Must be taken with plain water (6 to 8 oz) at least 30 minutes before the firstfood or drink of the day; do not lie down for 30 minutes (2) Treatment of Osteoporosis in Postmenopausal Women: 5 mg daily, 35 mg once a week, 75 mg taken on two consecutive days each month, or 150 mg once a month (2.1) Prevention of Osteoporosis in Postmenopausal Women: 5 mg daily, or 35 mg once a week (2.2)Men with Osteoporosis: 35 mg once a week (2.3)Treatment and Prevention of Glucocorticoid-Induced Osteoporosis: 5 mg daily(2.4)Paget’s Disease: 30 mg daily for 2 months (2.5)---------------------DOSAGE FORMS AND STRENGTHS----------------------Tablets: 5, 30, 35, 75, and 150 mg (3) -------------------------------CONTRAINDICATIONS------------------------------• Inability to stand or sit upright for at least 30 minutes (4, 5.1) • Hypocalcemia (4, 5.2)• Known hypersensitivity to any component of this product (4, 6.2) -----------------------WARNINGS AND PRECAUTIONS------------------------• Upper gastrointestinal irritation may occur. Dosing instructions should be followed. Discontinue use if new or worsening symptoms occur (5.1). • Hypocalcemia may worsen and must be corrected prior to use (5.2). • Osteonecrosis of the jaw has been reported rarely (5.3). • Severe bone, joint, or muscle pain may occur. Consider discontinuing use if severe symptoms develop (5.4, 6.2). • Before initiating treatment in patients with glucocorticoid-induced osteoporosis, sex steroid hormonal status of both men and women should be ascertained and appropriate replacement considered (5.6). • Bisphosphonates may interfere with bone-imaging agents (5.7). ------------------------------ADVERSE REACTIONS-------------------------------Most common adverse reactions reported in >10% of patients treated with ACTONEL and with a higher frequency than placebo are: back pain, arthralgia, abdominal pain, and dyspepsia (6.1). Hypersensitivity reactions (angioedema, generalized rash, bullous skin reactions), and eye inflammation (iritis, uveitis) have been reported rarely (6.2). To report SUSPECTED ADVERSE REACTIONS, contact Procter & Gamble Pharmaceuticals, Inc. at 1-800-836-0658 or FDA at 1-800-FDA1088 or /medwatch.------------------------------DRUG INTERACTIONS-------------------------------Calcium, antacids, or oral medications containing divalent cations interfere with the absorption of ACTONEL (7.1). -----------------------USE IN SPECIFIC POPULATIONS------------------------ACTONEL is not recommended for use in patients with severe renal impairment (creatinine clearance <30 mL/min) (5.5, 8.6, 12.3). ACTONEL is not indicated for use in pediatric patients (8.4).See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling. Revised: 07/2009 FULL PRESCRIBING INFORMATION: CONTENTS*1 INDICATIONS AND USAGE 1.1 Postmenopausal Osteoporosis 1.2 Osteoporosis in Men 1.3 Glucocorticoid-Induced Osteoporosis 1.4 Paget’s Disease 2DOSAGE AND ADMINISTRATION 2.1 Treatment of Postmenopausal Osteoporosis [see Indications and Usage (1.1)]2.2 Prevention of Postmenopausal Osteoporosis [see Indications and Usage (1.1)] 2.3Treatment to Increase Bone Mass in Men with Osteoporosis [see Indications and Usage (1.2)] 2.4 Treatment and Prevention of Glucocorticoid-Induced Osteoporosis [see Indications and Usage (1.3)] 2.5 Treatment of Paget’s Disease [see Indications and Usage (1.4)] 3 DOSAGE FORMS AND STRENGTHS 4 CONTRAINDICATIONS 5 WARNINGS AND PRECAUTIONS 5.1 Upper Gastrointestinal Adverse Reactions 5.2 Mineral Metabolism 5.3 Jaw Osteonecrosis 5.4 Musculoskeletal Pain 5.5 Renal Impairment 5.6 Glucocorticoid-Induced Osteoporosis 5.7 Laboratory Test Interactions 6ADVERSE REACTIONS 6.1 Clinical Studies Experience 6.2 Postmarketing Experience 7 DRUG INTERACTIONS 7.1 Calcium Supplements/Antacids 7.2 Hormone Replacement Therapy 7.3 Aspirin/Nonsteroidal Anti-Inflammatory Drugs 7.4 H 2 Blockers and Proton Pump Inhibitors (PPIs) 8 USE IN SPECIFIC POPULATIONS 8.1 Pregnancy 8.3 Nursing Mothers 8.4 Pediatric Use 8.5 Geriatric Use 8.6 Renal Impairment 8.7 Hepatic Impairment 10 OVERDOSAGE 11 DESCRIPTION 12 CLINICAL PHARMACOLOGY 12.1 Mechanism of Action 12.2 Pharmacodynamics 12.3 Pharmacokinetics 13 NONCLINICAL TOXICOLOGY 13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility 13.2 Animal Toxicology and/or Pharmacology 14 CLINICAL STUDIES 14.1 Treatment of Osteoporosis in Postmenopausal Women 14.2 Prevention of Osteoporosis in Postmenopausal Women 14.3 Men with Osteoporosis 14.4 Glucocorticoid-Induced Osteoporosis 14.5 Treatment of Paget’s Disease 16 HOW SUPPLIED/STORAGE AND HANDLING 17 PATIENT COUNSELING INFORMATION 17.1 FDA-Approved Patient Labeling *Sections or subsections omitted from the full prescribing information are not listed.FULL PRESCRIBING INFORMATION1 INDICATIONS AND USAGEOsteoporosis1.1 PostmenopausalACTONEL is indicated for the treatment and prevention of osteoporosis in postmenopausal women. In postmenopausal women with osteoporosis, ACTONEL reduces the incidence of vertebral fractures and a composite endpoint of nonvertebral osteoporosis-related fractures [see Clinical Studies (14.1, 14.2)].1.2 Osteoporosis in MenACTONEL is indicated for treatment to increase bone mass in men with osteoporosis.Osteoporosis1.3 Glucocorticoid-InducedACTONEL is indicated for the treatment and prevention of glucocorticoid-induced osteoporosis in men and women who are either initiating or continuing systemic glucocorticoid treatment (daily dosage of ≥ 7.5 mg prednisone or equivalent) for chronic diseases. Patients treated with glucocorticoids should receive adequate amounts of calcium and vitamin D.Disease1.4 Paget’sACTONEL is indicated for treatment of Paget’s disease of bone in men and women.2 DOSAGE AND ADMINISTRATIONACTONEL should be taken at least 30 minutes before the first food or drink of the day other than water.To facilitate delivery to the stomach, ACTONEL should be swallowed while the patient is in an upright position and with a full glass of plain water (6 to 8 oz). Patients should not lie down for 30 minutes after taking the medication [see Warnings and Precautions (5.1)].Patients should receive supplemental calcium and vitamin D if dietary intake is inadequate [see Warnings and Precautions (5.2)]. Calcium supplements and calcium-, aluminum-, and magnesium-containing medications may interfere with the absorption of ACTONEL and should be taken at a different time of the day. ACTONEL is not recommended for use in patients with severe renal impairment (creatinine clearance <30 mL/min). No dosage adjustment is necessary in patients with a creatinine clearance ≥30 mL/min or in the elderly.2.1 Treatment of Postmenopausal Osteoporosis [see Indications and Usage (1.1)]The recommended regimen is:•one 5 mg tablet orally, taken dailyor•one 35 mg tablet orally, taken once a weekor•one 75 mg tablet orally, taken on two consecutive days for a total of two tablets each monthor•one 150 mg tablet orally, taken once a month2.2 Prevention of Postmenopausal Osteoporosis [see Indications and Usage (1.1)]The recommended regimen is:•one 5 mg tablet orally, taken dailyor•one 35 mg tablet orally, taken once a weekor•alternatively, one 75 mg tablet orally, taken on two consecutive days for a total of two tablets each month may be consideredor•alternatively, one 150 mg tablet orally, taken once a month may be considered2.3 Treatment to Increase Bone Mass in Men with Osteoporosis [see Indications andUsage (1.2)]The recommended regimen is:•one 35 mg tablet orally, taken once a week2.4 Treatment and Prevention of Glucocorticoid-Induced Osteoporosis [see Indicationsand Usage (1.3)]The recommended regimen is:•one 5 mg tablet orally, taken daily2.5 Treatment of Paget’s Disease [see Indications and Usage (1.4)]The recommended treatment regimen is 30 mg orally once daily for 2 months. Retreatment may be considered (following post-treatment observation of at least 2 months) if relapse occurs, or if treatment fails to normalize serum alkaline phosphatase. For retreatment, the dose and duration of therapy are the same as for initial treatment. No data are available on more than 1 course of retreatment.3 DOSAGE FORMS AND STRENGTHS• 5 mg film-coated, oval, yellow tablet with RSN on 1 face and 5 mg on the other.•30 mg film-coated, oval, white tablet with RSN on 1 face and 30 mg on the other.•35 mg film-coated, oval, orange tablet with RSN on 1 face and 35 mg on the other.•75 mg film-coated, oval, pink tablet with RSN on 1 face and 75 mg on the other.•150 mg film-coated, oval, blue tablet with RSN on 1 face and 150 mg on the other.4 CONTRAINDICATIONS•Inability to stand or sit upright for at least 30 minutes [see Dosage andAdministration (2), Warnings and Precautions (5.1)]•Hypocalcemia [see Warnings and Precautions (5.2)]•Known hypersensitivity to any component of this product [see Adverse Reactions(6.2)]5 WARNINGS AND PRECAUTIONS5.1 Upper Gastrointestinal Adverse ReactionsBisphosphonates, including ACTONEL, may cause upper gastrointestinal disorders such as dysphagia, esophagitis, and esophageal or gastric ulcers. ACTONEL should be taken according to the dosing instructions to minimize the risk of these events. Patients should discontinue use if new or worsening symptoms occur. [see Contraindications (4), Adverse Reactions (6.1), Information for Patients (17.1)].Metabolism5.2 MineralHypocalcemia and other disturbances of bone and mineral metabolism should be effectively treated before starting ACTONEL therapy. Adequate intake of calcium and vitamin D is important in all patients, especially in patients with Paget’s disease in whom bone turnover is significantly elevated [see Contraindications (4), Adverse Reactions (6.1), Information for Patients (17.1)].Osteonecrosis5.3 JawOsteonecrosis of the jaw (ONJ), which can occur spontaneously, is generally associated with tooth extraction and/or local infection with delayed healing, and has been reported in patients taking bisphosphonates, including ACTONEL. Known risk factors for osteonecrosis of the jaw include invasive dental procedures (e.g., tooth extraction, dental implants, boney surgery), diagnosis of cancer, concomitant therapies (e.g., chemotherapy, corticosteroids), poor oral hygiene, and co-morbid disorders (e.g., periodontal and/or other pre-existing dental disease, anemia, coagulopathy, infection, ill-fitting dentures).For patients requiring invasive dental procedures, discontinuation of bisphosphonate treatment may reduce the risk for ONJ. Clinical judgment of the treating physician and/or oral surgeon should guide the management plan of each patient based on individual benefit/risk assessment.Patients who develop osteonecrosis of the jaw while on bisphosphonate therapy should receive care by an oral surgeon. In these patients, extensive dental surgery to treat ONJ may exacerbate the condition. Discontinuation of bisphosphonate therapy should be considered based on individual benefit/risk assessment. [see Adverse Reactions (6.2)]5.4 MusculoskeletalPainIn postmarketing experience, there have been reports of severe and occasionally incapacitating bone, joint, and/or muscle pain in patients taking bisphosphonates [see Adverse Reactions (6.2)]. The time to onset of symptoms varied from one day to several months after starting the drug. Most patients had relief of symptoms after stopping medication. A subset had recurrence of symptoms when rechallenged with the same drug or another bisphosphonate. Consider discontinuing use if severe symptoms develop.5.5 Renal ImpairmentACTONEL is not recommended for use in patients with severe renal impairment (creatinine clearance <30 mL/min).Osteoporosis5.6 Glucocorticoid-InducedBefore initiating ACTONEL treatment for the treatment and prevention of glucocorticoid-induced osteoporosis, the sex steroid hormonal status of both men and women should be ascertained and appropriate replacement considered.5.7 Laboratory Test InteractionsBisphosphonates are known to interfere with the use of bone-imaging agents. Specific studies with ACTONEL have not been performed.REACTIONS6 ADVERSE6.1 Clinical Studies ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.Treatment of Postmenopausal OsteoporosisDaily DosingThe safety of ACTONEL 5 mg once daily in the treatment of postmenopausal osteoporosis was assessed in four randomized, double-blind, placebo-controlled multinational trials of 3232 women aged 38 to 85 years with postmenopausal osteoporosis. The duration of the trials was up to three years, with 1619 patients exposed to placebo and 1613 patients exposed to ACTONEL 5 mg. Patients with pre-existing gastrointestinal disease and concomitant use of nonsteroidal anti-inflammatory drugs, proton pump inhibitors, and H2 antagonists were included in these clinical trials. All women received 1000 mg of elemental calcium plus vitamin D supplementation up to 500 IU per day if their 25-hydroxyvitamin D3 level was below normal at baseline.The incidence of all-cause mortality was 2.0% in the placebo group and 1.7% in the ACTONEL 5 mg daily group. The incidence of serious adverse events was 24.6% in the placebo group and 27.2% in the ACTONEL 5 mg group. The percentage of patients who withdrew from the study due to adverse events was 15.6% in the placebo group and 14.8% in the ACTONEL5 mg group. Table 1 lists adverse events from the Phase 3 postmenopausal osteoporosis trials reported in ≥5% of patients. Adverse events are shown without attribution of causality.Table 1Adverse Events Occurring at a Frequency ≥5% in Either Treatment Group Combined Phase 3 Postmenopausal Osteoporosis Treatment TrialsBody System PlaceboN = 16195 mg ACTONELN = 1613% %Body as a WholeInfection 29.931.1 Back Pain 26.1 28.0Accidental Injury 16.8 16.9Pain 14.014.1 Abdominal Pain 9.9 12.2Flu Syndrome 11.6 10.5Headache 10.89.9 Asthenia 4.55.4 Neck Pain 4.7 5.4Chest Pain 5.1 5.0Allergic ReactionCardiovascular System5.9 3.8Hypertension Digestive System 9.810.5Constipation 12.612.9 Diarrhea 10.010.8 Dyspepsia 10.610.8Nausea Metabolic & Nutritional Disorders 11.210.5Peripheral EdemaMusculoskeletal System8.8 7.7Arthralgia 22.123.7 Arthritis 10.19.6 Traumatic Bone Fracture 12.3 9.3Joint Disorder 5.3 7.0Myalgia 6.26.7 Bone PainNervous System4.85.3Dizziness 5.77.1 Depression 6.16.8Insomnia Respiratory System 4.65.0Bronchitis 10.410.0 Sinusitis 9.18.7 Rhinitis 5.16.2 Pharyngitis 5.06.0 Increased CoughSkin and Appendages6.3 5.9Rash Special Senses 7.17.9Cataract Urogenital System 5.76.5Urinary Tract Infection 10.4 11.1Gastrointestinal Adverse Events: The incidence of adverse events in the placebo and ACTONEL 5 mg daily groups were: abdominal pain (9.9% vs. 12.2%), diarrhea (10.0% vs. 10.8%), dyspepsia (10.6% vs. 10.8%), and gastritis (2.3% vs. 2.7%). Duodenitis and glossitis have been reported uncommonly in the ACTONEL 5 mg daily group (0.1% to 1%). In patients with active upper gastrointestinal disease at baseline, the incidence of upper gastrointestinal adverse events was similar between the placebo and ACTONEL 5 mg daily groups.Musculoskeletal Adverse Events: The incidence of adverse events in the placebo and ACTONEL 5 mg daily groups were: back pain (26.1% vs. 28.0%), arthralgia (22.1% vs. 23.7%), myalgia (6.2% vs. 6.7%), and bone pain (4.8% vs. 5.3%).Laboratory Test Findings: Throughout the Phase 3 studies, transient decreases from baseline in serum calcium (<1%) and serum phosphate (<3%) and compensatory increases in serum PTH levels (<30%) were observed within 6 months in patients in osteoporosis clinical trials treated with ACTONEL 5 mg once daily. There were no significant differences in serum calcium, phosphate, or PTH levels between placebo and ACTONEL 5 mg once daily at 3 years. Serum calcium levels below 8 mg/dL were observed in 18 patients, 9 (0.5%) in each treatment arm (placebo and ACTONEL 5 mg once daily). Serum phosphorus levels below 2 mg/dL were observed in 14 patients, 3 (0.2%) treated with placebo and 11 (0.6%) treated with ACTONEL5 mg once daily. There have been rare reports (<0.1%) of abnormal liver function tests.Endoscopic Findings: In the ACTONEL clinical trials, endoscopic evaluation was encouraged in any patient with moderate-to-severe gastrointestinal complaints, while maintaining the blind. Endoscopies were performed on equal numbers of patients between the placebo and treated groups [75 (14.5%) placebo; 75 (11.9%) ACTONEL]. Clinically important findings (perforations, ulcers, or bleeding) among this symptomatic population were similar between groups (51% placebo; 39% ACTONEL).Once-a-Week DosingThe safety of ACTONEL 35 mg once-a-week in the treatment of postmenopausal osteoporosis was assessed in a 1-year, double-blind, multicenter study comparing ACTONEL5 mg daily and ACTONEL 35 mg once-a-week in postmenopausal women aged 50 to 95 years. The duration of the trials was one year, with 480 patients exposed to ACTONEL 5 mg daily and 485 exposed to ACTONEL 35 mg once-a-week. Patients with pre-existing gastrointestinal disease and concomitant use of non-steroidal anti-inflammatory drugs, proton pump inhibitors, and H2 antagonists were included in these clinical trials. All women received 1000 mg of elemental calcium plus vitamin D supplementation up to 500 IU per day if their25-hydroxyvitamin D3 level was below normal at baseline.The incidence of all-cause mortality was 0.4% in the ACTONEL 5 mg daily group and 1.0% in the ACTONEL 35 mg once-a-week group. The incidence of serious adverse events was 7.1% in the ACTONEL 5 mg daily group and 8.2% in the ACTONEL 35 mg once-a-week group. The percentage of patients who withdrew from the study due to adverse events was 11.9% in the ACTONEL 5 mg daily group and 11.5% in the ACTONEL 35 mg once-a-week group. The overall safety and tolerability profiles of the two dosing regimens were similar.Gastrointestinal Adverse Events: The incidence of gastrointestinal adverse events was similar between the ACTONEL 5 mg daily group and the ACTONEL 35 mg once-a-week group: dyspepsia (6.9% vs. 7.6%), diarrhea (6.3% vs. 4.9%), and abdominal pain (7.3% vs. 7.6%).Musculoskeletal Adverse Events: Arthralgia was reported in 11.5% of patients in the ACTONEL 5 mg daily group and 14.2% of patients in the ACTONEL 35 mg once-a-week group. Myalgia was reported by 4.6% of patients in the ACTONEL 5 mg daily group and 6.2% of patients in the ACTONEL 35 mg once-a-week group.Laboratory Test Findings: The mean percent changes from baseline at 12 months were similar between the ACTONEL 5 mg daily and ACTONEL 35 mg once-a-week groups, respectively, for serum calcium (0.4% vs. 0.7%), phosphate (-3.8% vs. -2.6%) and PTH (6.4% vs. 4.2%).Monthly DosingTwo Consecutive Days per MonthThe safety of ACTONEL 75 mg administered on two consecutive days per month for the treatment of postmenopausal osteoporosis was assessed in a double-blind, multicenter study in postmenopausal women aged 50 to 86 years. The duration of the trial was two years; 613 patients were exposed to ACTONEL 5 mg daily and 616 were exposed to ACTONEL 75 mg two consecutive days per month. Patients with pre-existing gastrointestinal disease and concomitant use of non-steroidal anti-inflammatory drugs, proton pump inhibitors, and H2 antagonists were included in this clinical trial. All women received 1000 mg of elemental calcium plus 400 to 800 IU of vitamin D supplementation per day.The incidence of all-cause mortality was 1.0% for the ACTONEL 5 mg daily group and 0.5% for the ACTONEL 75 mg two consecutive days per month group. The incidence of serious adverse events was 10.8% in the ACTONEL 5 mg daily group and 14.4% in the ACTONEL75 mg two consecutive days per month group. The percentage of patients who withdrew from treatment due to adverse events was 14.2% in the ACTONEL 5 mg daily group and 13.0% in the ACTONEL 75 mg two consecutive days per month group. The overall safety and tolerability profiles of the two dosing regimens were similar.Acute Phase Reactions: Symptoms consistent with acute phase reaction have been reported with bisphosphonate use. The overall incidence of acute phase reaction was 3.6% of patients on ACTONEL 5 mg daily and 7.6% of patients on ACTONEL 75 mg two consecutive days per month. These incidence rates are based on reporting of any of 33 acute phase reaction-like symptoms within 5 days of the first dose. Fever or influenza-like illness with onset within the same period were reported by 0.0% of patients on ACTONEL 5 mg daily and 0.6% of patients on ACTONEL 75 mg two consecutive days per month.Gastrointestinal Adverse Events: The ACTONEL 75 mg two consecutive days per month group resulted in a higher incidence of discontinuation due to vomiting (1.0% vs. 0.2%) and diarrhea (1.0% vs. 0.3%) compared to the ACTONEL 5 mg daily group. Most of these events occurred within a few days of dosing.Ocular Adverse Events: None of the patients treated with ACTONEL 75 mg two consecutive days per month reported ocular inflammation such as uveitis, scleritis, or iritis;1 patient treated with ACTONEL 5 mg daily reported uveitis.Laboratory Test Findings: When ACTONEL 5 mg daily and ACTONEL 75 mg two consecutive days per month were compared in postmenopausal women with osteoporosis, the mean percent changes from baseline at 24 months were 0.2% and 0.8% for serum calcium, -1.9% and -1.3% for phosphate, and -10.4% and -17.2% for PTH, respectively. Compared to the ACTONEL 5 mg daily group, ACTONEL 75 mg two consecutive days per month resulted in a slightly higher incidence of hypocalcemia at the end of the first month of treatment (4.5% vs. 3.0%). Thereafter, the incidence of hypocalcemia with these regimens was similar at approximately 2%.Once-a-MonthThe safety of ACTONEL 150 mg administered once a month for the treatment of postmenopausal osteoporosis was assessed in a double-blind, multicenter study in postmenopausal women aged 50 to 88 years. The duration of the trial was one year, with642 patients exposed to ACTONEL 5 mg daily and 650 exposed to ACTONEL 150 mg once-amonth. Patients with pre-existing gastrointestinal disease and concomitant use of non-steroidal anti-inflammatory drugs, proton pump inhibitors, and H2 antagonists were included in this clinical trial. All women received 1000 mg of elemental calcium plus up to 1000 IU of vitamin D supplementation per day.The incidence of all-cause mortality was 0.5% for the ACTONEL 5 mg daily group and 0.0% for the ACTONEL 150 mg once-a-month group. The incidence of serious adverse events was 4.2% in the ACTONEL 5 mg daily group and 6.2% in the ACTONEL 150 mg once-a-month group. The percentage of patients who withdrew from treatment due to adverse events was 9.5% in the ACTONEL 5 mg daily group and 8.6% in the ACTONEL 150 mg once-a-month group. The overall safety and tolerability profiles of the two dosing regimens were similar.Acute Phase Reactions: Symptoms consistent with acute phase reaction have been reported with bisphosphonate use. The overall incidence of acute phase reaction was 1.1% in the ACTONEL 5 mg daily group and 5.2% in the ACTONEL 150 mg once-a-month group. These incidence rates are based on reporting of any of 33 acute phase reaction-like symptoms within3 days of the first dose and for a duration of 7 days or less. Fever or influenza-like illness with onset within the same period were reported by 0.2% of patients on ACTONEL 5 mg daily and 1.4% of patients on ACTONEL 150 mg once-a-month.Gastrointestinal Adverse Events: A greater percentage of patients experienced diarrhea with ACTONEL 150 mg once-a-month compared to 5 mg daily (8.2% vs. 4.7%, respectively). The ACTONEL 150 mg once-a-month group resulted in a higher incidence of discontinuation due to abdominal pain upper (2.5% vs. 1.4%) and diarrhea (0.8% vs. 0.0%) compared to the ACTONEL 5 mg daily regimen. All of these events occurred within a few days of the first dose. The incidence of vomiting that led to discontinuation was the same in both groups (0.3% vs.0.3%).Ocular Adverse Events: None of the patients treated with ACTONEL 150 mg once-amonth reported ocular inflammation such as uveitis, scleritis, or iritis; 2 patients treated with ACTONEL 5 mg daily reported iritis.Laboratory Test Findings: When ACTONEL 5 mg daily and ACTONEL 150 mg once-a-month were compared in postmenopausal women with osteoporosis, the mean percent changes from baseline at 12 months were 0.1% and 0.3% for serum calcium, -2.3% and -2.3% for phosphate, and 8.3% and 4.8% for PTH, respectively. Compared to the ACTONEL 5 mg daily regimen, ACTONEL 150 mg once-a-month resulted in a slightly higher incidence of hypocalcemia at the end of the first month of treatment (0.2% vs. 2.2%). Thereafter, the incidence of hypocalcemia with these regimens was similar at approximately 2%.Prevention of Postmenopausal OsteoporosisDaily DosingThe safety of ACTONEL 5 mg daily in the prevention of postmenopausal osteoporosis was assessed in two randomized, double-blind, placebo-controlled trials. In one study of postmenopausal women aged 37 to 82 years without osteoporosis, the use of estrogen replacement therapy in both placebo- and ACTONEL-treated patients was included. The duration of the trial was one year, with 259 exposed to placebo and 261 patients exposed to ACTONEL 5 mg. The second study included postmenopausal women aged 44 to 63 years without osteoporosis. The duration of the trial was one year, with 125 exposed to placebo and 129 patients exposed to ACTONEL 5 mg. All women received 1000 mg of elemental calcium per day.In the trial with estrogen replacement therapy, the incidence of all-cause mortality was 1.5% for the placebo group and 0.4% for the ACTONEL 5 mg group. The incidence of serious adverse events was 8.9% in the placebo group and 5.4% in the ACTONEL 5 mg group. The percentage of patients who withdrew from treatment due to adverse events was 18.9% in the placebo group and 10.3% in the ACTONEL 5 mg group. Constipation was reported by 1.9% of the placebo group and 6.5% of ACTONEL 5 mg group.In the second trial, the incidence of all-cause mortality was 0.0% for both groups. The incidence of serious adverse events was 17.6% in the placebo group and 9.3% in the ACTONEL5 mg group. The percentage of patients who withdrew from treatment due to adverse events was6.4% in the placebo group and 5.4% in the ACTONEL 5 mg group. Nausea was reported by 6.4% of patients in the placebo group and 13.2% of patients in the ACTONEL 5 mg group. Once-a-Week DosingThere were no deaths in a 1-year, double-blind, placebo-controlled study of ACTONEL 35 mg once a week for prevention of bone loss in 278 postmenopausal women without osteoporosis. More treated subjects on ACTONEL reported arthralgia (placebo 7.8%; ACTONEL 13.9%), myalgia (placebo 2.1%; ACTONEL 5.1%), and nausea (placebo 4.3%; ACTONEL 7.3%) than subjects on placebo.。
palbociclib英文说明书
6 7 7
FULL PRESCRIBING INFORMATION 1 INDICATIONS AND USAGE
IBRANCE is indicated in combination with letrozole for the treatment of postmenopausal women with estrogen receptor (ER)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced breast cancer as initial endocrine-based therapy for their metastatic disease. This indication is approved under accelerated approval based on progression-free survival (PFS) [see Clinical Studies (14)] . Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial. 2 2.1 DOSAGE AND ADMINISTRATION General Dosing Information
----------------------- WARNINGS AND PRECAUTIONS ---------------------- • Hematologic: Neutropenia may occur. Monitor complete blood count prior to start of IBRANCE therapy and at the beginning of each cycle, as well as on Day 14 of the first two cycles, and as clinically indicated. (5.1) • Infections: Monitor for signs and symptoms and withhold dosing as appropriate. (5.2) • Embryo-Fetal Toxicity: Can cause fetal harm. Advise patients of potential risk to a fetus and to use effective contraception. (5.4, 8.1, 8.3) ------------------------------ ADVERSE REACTIONS ----------------------------- Most common adverse reactions (incidence ≥10%) were neutropenia, leukopenia, fatigue, anemia, upper respiratory infection, nausea, stomatitis, alopecia, diarrhea, thrombocytopenia, decreased appetite, vomiting, asthenia, peripheral neuropathy, and epistaxis. (6) To report SUSPECTED ADVERSE REACTIONS, contact Pfizer, Inc. at 1-800-438-1985 or FDA at 1-800-FDA-1088 or /medwatch. ------------------------------ DRUG INTERACTIONS------------------------------ • CYP3A Inhibitors: Avoid concurrent use of IBRANCE with strong CYP3A inhibitors. If the strong inhibitor cannot be avoided, reduce the IBRANCE dose. (2.2, 7.1) • CYP3A Inducers: Avoid concurrent use of IBRANCE with strong and moderate CYP3A inducers. (7.2) • CYP3A Substrates: The dose of sensitive CYP3A4 substrates with narrow therapeutic indices may need to be reduced when given concurrently with IBRANCE. (7.3) See 17 for PATIENT COUNSELING INFORMATION and FDAapproved patient labeling. Revised: [02/2015]
硫酸吗啡FDA说明书(英文)
• AVINZA is not for use:
•
As an as-needed (prn) analgesic (1) For pain that is mild or not expected to persist for an extended period of time (1) For acute pain (1) For postoperative pain, unless the patient is already receiving chronic opioid therapy prior to surgery, or if the postoperative pain is expected to be moderate to severe and persist for an extended period of time (1) AVINZA 90 mg and 120 mg capsules are only for patients in whom tolerance to an opioid of comparable potency is established. (1)
-----------------------WARNINGS AND PRECAUTIONS----------------------- Elderly, cachectic, and debilitated patients, and patients with chronic pulmonary disease: Monitor closely because of increased risk of respiratory depression. (5.5, 5.6) Interaction with CNS depressants: Consider dose reduction of one or both drugs because of additive effects. (5.7, 7.2) Hypotensive effect: Monitor during dose initiation and titration (5.8) Patients with head injury or increased intracranial pressure: Monitor for sedation and respiratory depression. Avoid use of AVINZA in patients with impaired consciousness or coma susceptible to intracranial effects of CO 2 retention. (5.9) ------------------------------ADVERSE REACTIONS------------------------------Most common adverse reactions (≥10%) are constipation, nausea, somnolence, vomiting and headache. (6.1) To report SUSPECTED ADVERSE REACTIONS, contact Pfizer Inc. at 1-800-438-1985 or FDA at 1-800-FDA-1088 or /medwatch ------------------------------DRUG INTERACTIONS------------------------------ Mixed agonist/antagonist opioid analgesics: Avoid use with AVINZA because they may reduce analgesic effect of AVINZA or precipitate withdrawal symptoms. (5.12, 7.3) Muscle relaxants: Avoid use with AVINZA because of increased risk of respiratory depression. (7.4) Monoamine oxidase inhibitors (MAOIs): Avoid AVINZA in patients taking MAOIs or within 14 days of stopping such treatment. (7.5) -----------------------USE IN SPECIFIC POPULATIONS----------------------- Pregnancy: Based on animal data, may cause fetal harm. (8.1) Nursing mothers: Morphine has been detected in human milk. Closely monitor infants of nursing women receiving AVINZA. (8.3)
Probios产品指南说明书

9 Better Off With Probios®Page 1...the world leader in probioticsProbios® and Probiocin® are registered trademarks of Chr. Hansen, Inc.Intelli ora® is a registered trademark of Vets Plus, Inc.®Why use Probios® brand? Probios is the world’s most widely used, researched, and recognized brand of direct-fed microbials (DFMs).Science-Based Research: More than 95 individual studies have been performed at universities and under practical field conditions. These trials, involving 30,000 microbial products in dairy, beef, swine, and sheep. Additional studies have shown positive results for Probios in horses and in starter, grower, and finisher pigs, chickens, and turkeys.Backed by Quality: Probios is safe and effective when fed to animals. Probios contains guaranteed levels of Enterococcus faecium, Lactobacillus acidophilus, Lactobacillus casei, and Lactobacillus plantarum.Stability and Viability: Probios contains bacteria of proven efficacy in numbers capable of remaining viable during manufacturing and storage. Additionally, every guaranteed bacterium (expressed in CFUs or Colony Forming Units) will be available to the animal upon use.Manufactured in the U.S.A. Vets Plus, Inc. is the exclusive manufacturer of Probios microbial products in the U.S. These products are manufactured in an SQF Level 3 Edition 7.2 certified facility.For questions about Probios, call 715.231.1234.The ABCs of DFMs(Direct-fed microbials)Direct-fed microbials are also known as probiotics. The word “probiotic” literally means “for life” and is the opposite of the word antibiotic. Probiotics are good bacteria that can help boost the levels of beneficial bacteria in the gut, whereas antibiotics attack and kill infections and unwanted bacteria. For animals, probiotics are more commonly referred to as direct-fed microbials, or DFMs.DFMs help maintain intestinal balance, overall health and performance by:Helping maintain natural immunitiesHelping maintain pH in the gutHelping maintain nutrient absorptionHelping maintain gut microflora balanceEvery animal with a digestive system, including humans, has bacteria in their digestive system. Without bacteria an animal could not digest food. Animals have an extremely complex collection of about 100 trillion micro-organisms in their entire digestive tract. The intestine of animals contains billions of bacteria, some of which are beneficial (good bacteria) and some of which are pathogenic (bad bacteria).Under certain conditions, such as stress, the natural balance of beneficial bacteria in the digestive system is disrupted. The number of pathogens increases while the number of beneficial organisms decreases, causing digestive upsets including diarrhea, constipation, and discomfort. In animals, DFMs may help restore the normal microbial balance in the gut and overall health of the animal.Newborn animals do not have bacteria in their intestine. The intestine rapidly becomes colonized by natural means from the mother and the environment. Studies have shown providing DFMs to an animal at birth plays an important role in the growth and health of animals.CHR-980: 120 g jar, 6 per caseCHR-985: 240 g jar, 6 per case Suggested Use:Probios Soft Chews feature a highly palatable chicken liver flavor that makes administering them to your dog a breeze. Each soft chew provides two strains of live (viable) bacteria that help support proper digestion. These provide the ideal supplement for your pet’s stomach caused by situations like travel or visits to the vet.Feeding Recommendations:120 g jar: 2 chews per 10 lbs of body weight240 g jar: 1-3 chews per 50 lbs of body weightPage 3Probios® Digestive TabletsAvailable Sizes:CHR-910: 45 ct jar, 6 per caseCHR-911: 180 ct jar, 6 per caseSuggested Use:Probios Digestive Dog Tablets are a chewable, probiotic supplement that contain a source of live, naturally occurring micro-organisms to help support proper digestion during diet changes, kenneling and travel.Feeding Recommendations:Puppies: 1 tablet per dayDogs: 1 tablet per 20 lbs body weight per dayPage 4Probios® Chewables for DogsDigestion SupportAvailable Sizes:CHR-950/6: 1 lb pouch, 6 per case Suggested Use:Probios Digestion Support Treats for Dogs are suggested for daily use to maintain a healthy digestive system. Also suggested for use during traveling, kenneling, or training to help support proper digestion.Feeding Recommendations:Give 3-6 treats daily. Repeat as needed.Page 5Probios ® Chewables for Dogs Joint Support Page 6Available Sizes: CHR-951/6: 1 lb pouch, 6 per caseSuggested Use: Probios Joint Support Treats are suggested to deliver probiotic benefits and help support healthy joint function. For use in all breeds of dogs.Feeding Recommendations:Give 3-6 treats daily. Repeat as needed.Probios® Dispersible PowderAvailable Sizes:CHR-404: 240 g jar, 12 per caseCHR-403: 5 lb jar, 6 per caseCHR-402: 25 lb pail, 1 per case Suggested Use:This unique product helps support proper digestion. The supplement provides more than 10 million colony forming units of four different strains of lactic acid bacteria that work to naturally facilitate digestion.Feeding Recommendations:Dogs: (under 1 lb): 1/4 tsp / pet / dayDogs: (1 to 10 lbs): 1/2 tsp / pet / dayDogs: (>10 lbs): 1 tsp / pet / dayPage 7Probios® Pro-Pill Pods™Page 8 Available Sizes:CHR-991: (3.7 oz) 30 ct jar, 12 per case (Chicken)CHR-992: (7.4 oz) 30 ct jar, 12 per case (Chicken)CHR-996: (3.7 oz) 30 ct jar, 12 per case (Peanut Butter)CHR-997: (7.4 oz) 30 ct jar, 12 per case (Peanut Butter) Suggested Use:Highly palatable Pro-Pill Pods take the hassle out of medicating your dogs by concealing medicinal odors and taste. Ideal size that fits most tablets and capsules. May be cut in half for smaller pills.Directions for Use:Hold the pod with thumb and forefinger. Insert pill. Squeeze ends shut. Pro-Pill Pod is now ready to offer to your pet. Provide fresh water at all times.Probios® Intelliflora® for DogsAvailable Sizes:CHR-800: 1 g packets (30 ct), 6 per case, 24 per master case Suggested Use:Probios Intelliflora is designed to be used as a daily supplement to help support normal digestion. Feeding Recommendations:Sprinkle one packet daily on top of your pet’s food.Page 9Probiocin® Pet GelAvailable Sizes:CHR-900: 15 cc tube, 72 per case Suggested Use:Probiocin is a probiotic supplement that helps maintain a healthy digestive system by supporting the proper bacterial balance in the lower intestine.Feeding Recommendations:Newborns: 1 g at birthPage 10Made with realyogurtHelps freshenbreathCarefully crafted with natural ingredientsProbiotics, prebiotics, and soluble fiber help maintain proper digestionSpecifically designed for maximum tooth abrasionfor cleaner teethDental SticksAvailable Sizes:CHR-970: 8.11 oz pouch, 12 per caseSuggested Use:Helps reduce plaque and tartar as your dog chews.Prebiotics and probiotics help support proper digestion.Feeding Recommendations:Small Dogs (5-25 lbs): 1/2 chew, twice dailyMedium and Large Dogs (20-60+ lbs): 1 chew, twice dailyPage 11Page 12Probios® Dispersible PowderAvailable Sizes:CHR-404: 240 g jar, 12 per caseCHR-403: 5 lb jar, 6 per caseCHR-402: 25 lb pail, 1 per case Suggested Use:This unique product helps support proper digestion. The supplement provides more than 10 million colony forming units of four different strains of lactic acid bacteria that work to naturally facilitate digestion.Feeding Recommendations:Cats: (under 1 lb): 1/4 tsp / pet / dayCats: (1 to 10 lbs): 1/2 tsp / pet / dayCats: (>10 lbs): 1 tsp / pet / dayPage 13Probiocin® Pet GelAvailable Sizes:CHR-900: 15 cc tube, 72 per case Suggested Use:Probiocin is a probiotic supplement that helps maintain a healthy digestive system by supporting the proper bacterial balance in the lower intestine.Feeding Recommendations: Newborns: 1 g at birthPage 14Probios® Intelliflora® for CatsAvailable Sizes:CHR-805: 1 g packets (30 ct), 6 per case, 24 per master case Suggested Use:Probios Intelliflora is designed to be used as a daily supplement to help support normal digestion. Feeding Recommendations:Sprinkle one packet daily on top of your pet’s food.Page15Page 15Probios ® Cat Product ChartPage16Probios® Chewables for HorsesJoint SupportAvailable Sizes:CHR-752/6: 1 lb pouch, 6 per case Suggested Use:Probios Chewables for Horses Joint Support are recommended to support healthy joints, joint flexibility and mobility in addition to supplying probiotic benefits. Feeding Recommendations:3 to 6 treats daily.Page 17Available Sizes:CHR-750/6 - 1 lb pouch, 6 per caseSuggested Use:Probios Equine Digestion Support treats are recommended to support healthy digestion. The beneficial bacteria helps maintain appetite and gut function during situations like travel or showing.Feeding Recommendations:Provide 1-2 treats daily. Repeat as needed.Probios ® Chewables for HorsesDigestion SupportPage18Available Sizes:CHR-795 - 1.32 lbs pouch, 6 per caseSuggested Use:Probios Equine Digestion Support soft chews arerecommended to support healthy digestion. The beneficial bacteria helps maintain appetite and gut function during situations like travel or showing.Feeding Recommendations:Provide 1-2 treats daily. Repeat as needed.Probios ® Soft Chews for HorsesDigestion SupportPage 19Probios® Equine One Oral GelAvailable Sizes:CHR-700: 30 cc tube, 72 per case Suggested Use:Probios Equine One Oral Gel helps support microbial balance in your horse’s gastrointestinal tract. This probiotic formula utilizes four different strains of lactic acid bacteria and includes more than 10 million colony forming units per gram.Feeding Recommendations: Newborns: 10 g at birth and day 4Adults: 15 g / head / dayPage 20Probios® Dispersible PowderAvailable Sizes:CHR-404: 240 g jar, 12 per caseCHR-403: 5 lb jar, 6 per caseCHR-402: 25 lb pail, 1 per case Suggested Use:This unique product helps support proper digestion. The supplement provides more than 10 million colony forming units of four different strains of lactic acid bacteria that work to naturally facilitate digestion.Feeding Recommendations:Equine-Foals: 5 g / head / dayAdults: 10 g-15 g / head / dayPage 21 Page 21Probios® Horse Product ChartPage 22Probios ® Bovine One Oral GelAvailable Sizes:CHR-100: 300 cc tube, 24 per case CHR-101: 60 cc tube, 72 per caseSuggested Use:This unique product helps support proper digestion. The supplement provides more than 10 million colony forming units per gram of four different strains of lactic acid bacteria that work to naturally facilitate digestion.Feeding Recommendations:Beef:Newborns:5 g at birthCalves: <400 lbs, 10 g >400 lbs, 15 g Incoming Feedlot/ <400 lb, 10 g Stockers: >400 lb, 15 g Hospital: 15 g on first and lastday of therapyGoats/Sheep:Newborns: 5 g at birthPage 23Dairy: Calves: 5 g at birth Heifers <400 lb, 10 g >400 lb, 15 g Cows: 30 g at freshening Hospital: 15 g on first and last day of therapyProbios ® Bovine One Oral GelMAXAvailable Sizes:CHR-110: 300 cc tube, 24 per case CHR-111: 60 cc tube, 72 per caseSuggested Use:This unique product helps support proper digestion. The supplement provides more than 15 million colony forming units per 10 grams of four different strains of lactic acid bacteria that work to naturally facilitate digestion.Feeding Recommendations:Beef:Newborns:5 g at birthCalves: <400 lbs, 10 g >400 lbs, 15 g Incoming Feedlot/ <400 lb, 10 g Stockers: >400 lb, 15 gHospital: 15 g on first and lastday of therapyGoats/Sheep:Newborns: 5 g at birthPage 24Dairy: Calves: 5 g at birth Heifers <400 lb, 10 g >400 lb, 15 g Cows: 30 g at fresheningHospital: 15 g on first and last day of therapyProbios ® Bovine One Oral Gelwith Natural EAvailable Sizes:CHR-120: 300 cc tube, 24 per case CHR-121: 60 cc tube, 72 per caseSuggested Use:This unique product helps support proper digestion. The supplement provides more than 10 million colony forming units per gram of four different strains of lactic acid bacteria that work to naturally facilitate digestion with natural Vitamin E.Feeding Recommendations:Beef:Newborns:5 g at birthCalves: <400 lbs, 10 g >400 lbs, 15 g Incoming Feedlot/ <400 lb, 10 g Stockers: >400 lb, 15 gHospital: 15 g on first and lastday of therapyPage 25Dairy: Calves: 5 g at birth Heifers: <400 lb, 10 g >400 lb, 15 g Cows: 30 g at fresheningHospital: 15 g on first and last day of therapyProbios ® Dispersible PowderAvailable Sizes:CHR-404: 240 g jar, 12 per case CHR-403: 5 lb jar, 6 per case CHR-402: 25 lb pail, 1 per caseSuggested Use:This unique product helps support proper digestion. The supplement provides more than 10 million colony forming units of four different strains of lactic acid bacteria that work to naturally facilitate digestion.Feeding Recommendations:Dairy/Beef: Calves: 5 g / head / day Adult: 15 g / head / day Swine: Nursery: 2 g / head / day Adult:5 g / head / dayPage 26Equine:Foals: 5 g / head / day Adult: 10-15 g / head / day Sheep/Goat:All: 5 g / head / dayProbios® Oral Bolus1/4 ozAvailable Sizes:CHR-501: 50 ct, 12 per caseSuggested Use:This unique product helps support proper digestion. The supplement provides more than 49 million colony forming units per bolus of four different strains of lactic acid bacteria that work to naturally facilitate digestion. Feeding Recommendations:Dairy/Beef:Newborns: 1 bolus at birthCalves: < 400 lbs, 1 bolus / head / day> 400 lbs, 2 boluses / head / day Cows: 4 boluses at fresheningSheep/Goats: 1 bolusPage 27Probios® Oral Bolus1/2 ozAvailable Sizes:CHR-500: 50 ct, 12 per caseSuggested Use:This unique product helps support proper digestion. The supplement provides more than 98 million colony forming units per bolus of four different strains of lactic acid bacteria that work to naturally facilitate digestion. Feeding Recommendations:Dairy/Beef:Newborns: 1 bolus at birthCalves: < 400 lbs, 1/2 bolus / head / day> 400 lbs, 1 boluses / head / day Cows: 2 boluses at fresheningSheep/Goats: 1/2 bolusPage 28Page 29Probios® Feed GranulesAvailable Sizes:CHR-406: 5 lb, 6 per caseCHR-405: 50 lb, 1 per caseSuggested Use:This unique product helps support proper digestion. The supplement provides more than 10 million colony forming units per bolus of four different strains of lactic acid bacteria that work to naturally facilitate digestion. Feeding Recommendations:Calves: 5 g / head / dayIncomingFeedlot/ 10-15 g / head / dayStocker:Heifers: 10 g / head / dayCows: 10 g / head / dayPage 29Probios® Livestock Product ChartPage 30Questions? Check out our websitefor more information: Learn more about our products!We’re a Social Bunch!Better Off With Probios®。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
5.3 Gastrointestinal Ulcers and Bleeding
5.4 Central Nervous System Symptoms
5.5 Leukopenia and Elevated Alkaline Phosphatase Levels
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use PROCSYBI safely and effectively. See full prescribing information for PROCSYBI. PROCYSBI (cysteamine bitartrate) delayed-release capsules, for oral use Initial U.S. Approval: 1994 ---------------------------INDICATIONS AND USAGE (1)-----------------------PROCYSBI is a cystine depleting agent indicated for the management of nephropathic cystinosis in adults and children ages 6 years and older. (1.1) ----------------------DOSAGE AND ADMINISTRATION (2)-------------------PROCYSBI should be prescribed by a physician experienced in management of nephropathic cystinosis. (2.1) Swallow capsules whole or after sprinkling on food or in recommended liquids. Administer via gastrostomy tube (12 F or larger) after mixing with food. ( 2.3 ) Total daily dose is 1.3 gram/m2/day in two divided doses, every 12 hours. (2.2 ) Take PROCYSBI at least 2 hours after and at least 30 minutes before eating. ( 2 ) Goal of therapy is to maintain a white blood cell (WBC) cystine level < 1 nmol ½ cystine/mg protein or a plasma cysteamine concentration > 0.1 mg/L. (2.6) Switching from Immediate-Release Cysteamine to PROCYSBI Total daily dose of PROCYSBI equal to their previous total daily dose of immediate-release cysteamine bitartrate. (2.7) Initial Dosage in Cysteamine-naïve patients Starting Dose1/6 to 1/4 of the maintenance dose of PROCYSBI (2.1) Maintenance Dose: 1.3 gram/m2/day, in two divided doses every 12 hours (2.2) See Full Prescribing Information for details on administration. ( 2.3) ---------------------DOSAGE FORMS AND STRENGTHS (3)-----------------Delayed-release capsules: 25 mg and 75 mg (3) -----------------------------CONTRAINDICATIONS (4)--------------------------Hypersensitivity to penicillamine (4.1)
12.2 Pharmacodynamics
12.3 Pharmacokinetics
NONCLINICAL TOXICOLOGY 13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
CLINICAL STUDIES 14.1 Clinical Trials with Immediate-release Cysteamine
17.3 Use by Pregnant Women
---------------------WARNINGS AND PRECAUTIONS (5)------------------- Ehler-Danlos like Syndrome: Reduce dosage if skin and bone lesions occur. (5.1) Skin Rash: Discontinue PROCYSBI if severe skin rash such as erythema multiforme bullosa or toxic epidermal necrolysis occurs. (5.2) Gastrointestinal: Monitor for symptoms of gastrointestinal ulceration and bleeding. (5.3) Central Nervous System: Monitor for seizures, lethargy, somnolence, depression, and encephalopathy. (5.4) Leukopenia and Elevated Alkaline Phosphatase Levels: Monitor white blood count and elevated alkaline phosphatase levels. (5.6) Benign Intracranial Hypertension: Monitor for signs and symptoms of benign intracranial hypertension. (5.7) ----------------------------ADVERSE REACTIONS (6)----------------------------Most commonly reported adverse reactions (>5%) are vomiting, abdominal pain/discomfort, headaches, nausea, diarrhea, anorexia/decreased appetite, breath odor, fatigue, dizziness, skin odor, and rash. (6.1) To report SUSPECTED ADVERSE REACTIONS, contact Raptor Pharmaceuticals Inc. at 1-855-888-4004 or FDA at 1-800-FDA-1088 or /medwatch. ---------------------------DRUG INTERACTIONS (7)-----------------------------PROCYSBI (cysteamine bitartrate) delayed-release capsules can be administered with electrolyte (except bicarbonate) and mineral replacements necessary for management of Fanconi Syndrome as well as vitamin D and thyroid hormone (7). ---------------------USE IN SPECIFIC POPULATIONS (8)---------------------Nursing Mothers: Breastfeeding is not recommended while taking PROCYSBI. (8.3) See 17 for PATIENT COUNSELING INFORMATION and FDAapproved patient labeling. Revised: April 2013
2.7 Transferring Patients from Immediate-release Cysteamine
Bitartrate Capsules
DOSAGE FORMS AND STRENGTHS CONTRAINDICATIONS WARNINGS AND PRECAUTIONS 5.1 Ehler-Danlos like Syndrome
14.2 Clinical Trials with PROCYSBI
HOW SUPPLIED/STORAGE AND HANDLING PATIENT COUNSELING INFORMATION 17.1 Laboratory Monitoring
17.2 Dosing and Administration
8.3 Nursing Mothers
8.4 Pediatric Use
9 10 11 12 DRUG ABUSE AND DEPENDENCE OVERDOSAGE DESCRIPTION CLINICAL PHARMACOLOGY 12.1 Mechanism of Action