奥利司他全合成
Cetilistat(西替利司他,ATL962)

赛利司他(ATL-962)、利莫那班和赛尼可的研发与市场趋势阎家麒高荣谢建平(泰州市今朝伟业精细化工有限公司,江苏泰州225327)摘要:本文阐述了赛利司他、利莫那班和赛尼可三种新减肥药物的研发和市场趋势,同时对这三种减肥药物作了疗效比较,并对各种药物的优缺点进行了分析。
赛利司他和利莫那班蕴藏着巨大商机,尤其是脂肪酶抑制剂赛利司他。
关键词:赛利司他;利莫那班;赛尼可;减肥药物Research and Development and Market Trends of Anti-obesity Drugs such as Cetilistat (ATL-962), Rimonabant and XenicalYAN Jia-qi , Gao Rong , XIE Jian-ping(Taizhou Jinzhaoweiye Fine Chemicals Co., Ltd., Jiangsu Taizhou 225327)Abstract: This paper presents the research and development of three new anti-obesity drugs such as Cetilitat(ATL-962), Rimonabant and Xenical and their current market trends. Meanwhile, the three drugs effects in administration and the advantages and disadvantages of each was analyzed. Cetilitat(ATL-962), Rimonabant have the potential to greatly enhance the market opportunity for lipase inhibitors and thus the potential for Cetilistat.Key words: Cetilitat(ATL-962); Rimonabant; Xenical; anti-obesity drugs赛利司他(Cetilistat, ATL-962,西替利司他,新利司他) 是英国Alizyme公司研发的一种新的胃肠道脂肪酶抑制剂,用于治疗肥胖和II型糖尿病的特效药物。
Thorpe-Ingold效应及其在有机成环反应中的应用
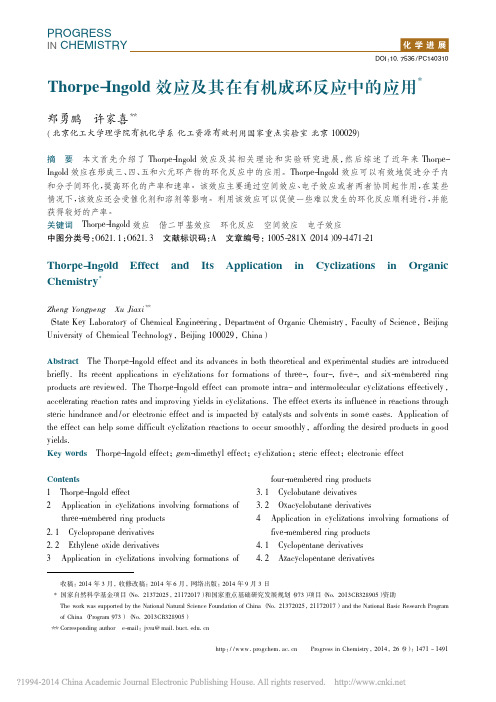
图式 1 加成
[6 ]
2Alder 环 富 马 酸 糠甲 醇 酯 的 分 子 内 DielsIntramolecular DA reaction of 2furyl methyl
Scheme 1 fumarates
[6 ]
结果, 无取代底物 1a 环化速率最慢, 单甲基取 代 1b 和单叔丁基取代 1c 的环化速率略有增加, 但
14711491thorpeingold效应及其在有机成环反应中的应用北京化工大学理学院有机化学系化工资源有效利用国家重点实验室北京100029本文首先介绍了thorpeingold效应及其相关理论和实验研究进展然后综述了近年来thorpeingold效应在形成三四五和六元环产物的环化反应中的应用
PROGRESS IN CHEMIreaction
rates
generally
increase
from
unsubstituted to monosubstituted to disubstituted substrates various cyclizations, annulations, cycloadditions, intramolecular insertions,etc.
1
ThorpeIngold 效应
ThorpeIngold 效 应, 又被称为偕二甲基效应 ( gemdimethyl effect ) 或角压缩 ( angle compression ) 效应, 是指通过分子链上的偕二取代促进环化 。 [2 ] 该效应最早由 Thorpe 和 Ingold 等提出 , 即当 分子链中亚甲基上的氢被大体积烷基取代后 , 该处 内角( 键角) 被压缩, 分子链末端两个反应基团相互 靠近, 有利于分子内环化( 图 1 ) 。
奥利司他胶囊说明书 奥利司他胶囊主治功能

奥利司他胶囊说明书奥利司他胶囊主治功能奥利司他胶囊(植恩)用于肥胖或体重超重患者(体重指数≥24)的治疗。
下面是学习啦小编整理的奥利司他胶囊说明书,欢迎阅读。
奥利司他胶囊商品介绍通用名:奥利司他胶囊生产厂家: 重庆植恩药业有限公司批准文号:国药准字H20123131药品规格:0.12g*18粒药品价格:¥253元奥利司他胶囊说明书【商品名】雅塑奥利司他胶囊【通用名】奥利司他胶囊【英文名】Orlistat Capsules【汉语拼音】Ao’LiSiTaJiaoNang【性状】本品为胶囊剂,内容物为白色或类白色颗粒或粉末。
【成份】本品每粒含奥利司他0.12g,辅料为:预胶化淀粉、微粉硅胶和硬脂酸镁。
【适应症】用于肥胖或体重超重患者(体重指数≥24)的治疗。
【用法用量】成人:餐时或餐后1小时内口服1粒。
如果有一餐未进或食物中不含脂肪,则可省略一次服药。
【药理作用】奥利司他胶囊是长效和强效的特异性胃肠道脂肪酶抑制剂,它通过与胃中的胃脂肪酶和小肠腔内的胰脂肪酶的活性丝氨酸部位形成共价键,使酶失活,而发挥治疗作用。
失活的酶不能将食物中的脂肪(主要是甘油三酯)水解为可吸收的游离脂肪酸和单酰基甘油。
未消化的甘油三酯不能被身体吸收,从而减少热量摄入,控制体重。
该药并不通过全身吸收发挥药效。
【不良反应】1、常见不良反应为:油性斑点,胃肠排气增多,大便紧急感,脂肪(油)性大便,脂肪泻,大便次数增多和大便失禁。
随膳食中脂肪成分增加,发生率也相应增高。
大部分病人用药一段时间后可改善。
、较多出现的胃肠道急性反应有:腹痛/腹部不适、胃肠胀气、水样便、软便、直肠痛/直肠部不适、牙齿不适、牙龈不适。
、观察到的其他少见不良事件有:上呼吸道感染、下呼吸道感染、流行性感冒、头痛、月经失调、焦虑、疲劳、泌尿道感染。
、使用奥利司他已有罕见的转氨酶升高、碱性磷酸酶升高和重度肝炎的报告,并出现肝衰竭病例,其中部分患者需要进行肝移植或可直接导致死亡。
IT医疗信息化

方 案 专题 大 会 ,本 届展 会 上 来 自微 软 、戴 尔 、
GE、I M 、 飞 利 浦 、S B AP和 锐 捷 网 络 等 近 5 O
多家 国 内 外 I 企 业 展 出 了 他 们 最 新 的 产 品 与 解 T
决方案 。 HI S M S总 裁 兼 首 席 执 行 官 S e h n ib r tp e L e e 表 示 , 中 国 已 经 成 为 医 疗 _ 生 信 息 技 术 的 供 应 l J 商以及 国际医疗服 务机构进 入亚太市 场的 门户 , 希 望 HI S M S大 会 能 够 成 为 中 国 医 疗 领 域 与 国 际 同 行 知 识 和 专 业技 能 共 享 交流 的 平 台 。
产 上 市 。 奥 利 司 他 为 目前 国 际 公 认 f
降 脂 药 , 占 据 全 球 8% 的 减 肥 市 场 O
其 具 备 较 高 的 安 全 性 , 20 0 7年 被 姜
中外医 疗I 专家 齐聚H M S 2 1亚太 博览 会 T I S 00
2l O o年 5 月 2 目 ,HI S As P c 0 0 8 MS l a 2 1 a
Hale Waihona Puke 结核 病药物 研发 取得 新进展
近 期 ,由全球 结 核病 药物 研发 l
员组 织 HI S主 办 , 中 华 人 民 共 和 国 卫 生 部 副 MS 部 长 尹 力 出 席 大 会 并 发 言 ,他 指 出 , “ 强 信 息 加
标准 化和 公 共服 务信息 平台 建设 将是 下一 阶段 中 国 卫 生 信 息 化 建 设 的 重 点 。 ” HI S博 览 会 的 一 个 主 要 特 色 是 行 业 解 决 MS
准成 为 O TC产 品 。 重 庆 植 恩 药 业 致 他 全 合 成 工 艺 研 究 ,实 现 了 奥 利 司 1 产 工 艺 的 技 术 突 破 ,并 率 先 在 国 内 ; 产 业 化 规 模 的 全 合 成 工 艺 路 线 ,年
奥利司他(舒尔佳)-选择性抑制脂肪吸收可用于长期减肥(英文)

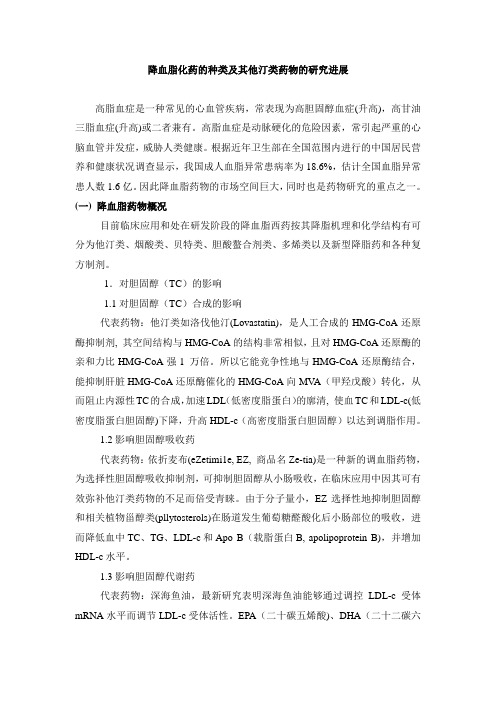
Received June 14, 2000; Accepted June 14, 2000.Author to whom all correspondence and reprint requests should be addressed:Dr. Jonathan Hauptman, Hoffmann-La Roche Inc., 340 Kingsland Street,Nutley, NJ 07110-1199. E-mail: jonathan.hauptman@201Orlistat is a novel, noncentrally acting antiobesity agent that selectively inhibits gastrointestinal lipase activity, thereby reducing the absorption of dietary fat by approximately one-third. In a series of 1- and 2-yr randomized, placebo-controlled trials of obese sub-jects, treatment with orlistat in combination with a mildly calorie-restricted diet consistently produced significantly greater mean weight loss than diet alone.More orlistat-treated subjects than placebo recipients achieved clinically meaning ful weig ht reduction (*5%or *10% of initial body weig ht) after 1 and 2 yr. Orlistat was also associated with a significant reduction in the regain of lost weight during long-term treatment. In addition, orlistat therapy resulted in sig nificant improvements in several cardiovascular risk factors including serum total and low-density lipoprotein–cholesterol, serum insulin levels, systolic and diastolic blood pressure, and waist circumference. Further-more, obese subjects with type 2 diabetes achieved a sig nificantly g reater decrease in body weig ht with orlistat compared with placebo, as well as significant improvements in HbA 1c and fasting g lucose levels.Among subjects with impaired g lucose tolerance,orlistat compared with placebo reduced the propor-tion who developed type 2 diabetes. Conversely,orlistat increased the proportion of subjects who achieved a normalization of g lucose tolerance. Orlistat acts locally in the g astrointestinal tract and is only minimally absorbed. In long -term clinical trials,orlistat was well tolerated by both diabetic and non-diabetic subjects.Key Words:Orlistat; antiobesity agents; fat-restricted diet; weight loss; coronary risk.IntroductionThe etiology of obesity is complex and involves the interplay of numerous environmental and genetic factors.However, obesity is essentially the consequence of a long-term positive energy balance in which energy intake exceeds energy expenditure.Dietary intake and composition, together with physical activity, are the primary modifiable factors that influence energy balance. In particular, the excessive consumption of dietary fat may have a major contributory role in the devel-opment of obesity (1–3). Dietary fat has a higher energy density than other macronutrients, providing 9 kcal/g (37kJ/g) compared with just 4 kcal/g (17 kJ/g) with either pro-tein or carbohydrate. Moreover, fat has only a weak effect on postprandial satiety. In studies of obese subjects, high-carbohydrate meals suppressed subsequent food intake to a greater extent than high-fat meals that were matched for energy density, volume, and sensory properties (4). In another study, obese patients who ate from a range of either high-fat or high-carbohydrate foods voluntarily consumed twice as much energy from the high-fat items (5). Several factors may play a role in the low satiating effect of fat,including stomach distension, nutrient absorption, hor-monal release, and oxidation of nutrients.Fat also tends to be very palatable, and studies have shown that both male and female obese individuals tend to report definite preferences for high-fat foods (6). This,together with the high energy density and low satiating effect of fat, can result in the overeating or passive overcon-sumption of high-fat foods.In addition, whereas the oxidation of both carbohydrate and protein is tightly correlated with intake, fat balance is less well controlled (7). Fat oxidation, unlike the oxidation of either carbohydrate or protein, is correlated with energy intake rather than fat intake (8,9). As a result, energy from fat leads to greater weight gain than calories from other macronutrients because they are less likely to be oxidized,and instead are readily stored as body fat. There is evidence to suggest that obese subjects have a reduced ability to oxidize fat in comparison with lean individuals. In one study, a 7-d high-carbohydrate diet resulted in a signifi-cant increase in carbohydrate oxidation in both obese and lean subjects. However, on a high-fat diet, fat oxidation increased among lean subjects but not obese subjects (10).In another study, previously obese women with a genetic predisposition toward obesity were less able to increase fat oxidation in response to increased dietary fat content com-pared with never-obese control subjects (11).OrlistatSelective Inhibition of Caloric Absorption Can Affect Long-Term Body Weight Jonathan HauptmanHoffmann-La Roche Inc., Nutley, NJOrlistat: Inhibition of Fat Absorption/Hauptman202EndocrineThe treatment of obesity involves the creation of a nega-tive energy balance in order to reduce body fat stores. Sev-eral studies have shown that low-fat diets can promoteweight loss in both lean and obese subjects, and ametaanalysis of 33 controlled studies of ad libitum low-fatdietary interventions reported that a 1% reduction in di-etary fat produced a 0.22-kg weight loss (3,12).H owever, long-term weight reduction is difficult tomaintain by dietary intervention alone, and most obesepatients eventually regain much of their lost weight (13,14).This may be partially attributed to compensatory physi-ologic processes that act to oppose weight loss and themaintenance of lower body weight. However, much of thefailure associated with conventional dietary and behavioralmodification is a direct result of the inability of many obeseindividuals to maintain long-term compliance with signifi-cant dietary and lifestyle changes.The limited success of dietary and behavioral interven-tions in long-term weight control has meant that adjunctivepharmacotherapy that is both well tolerated and effectivewill become increasingly important in the management ofobesity. One approach is the induction of weight loss bydrug-mediated inhibition of fat absorption. Orlistat(Xenical®, Hoffmann-La Roche Inc.), a novel, noncentrallyacting antiobesity agent, is a highly potent inhibitor of gas-trointestinal (GI) lipases, enzymes that play a crucial rolein the digestion of long-chain triglycerides. Orlistat pro-duces a partial inhibition of triglyceride hydrolysis and areduction in the subsequent absorption of free fatty acidsand monoglycerides (Fig.1) (15).The inhibitory effect of orlistat on dietary fat absorption has been evaluated using fecal fat excretion as a represen-tative pharmacodynamic parameter. The inhibition of dietary fat absorption with orlistat is dose dependent, with the optimal therapeutic dosage being 120 mg administered three times daily with main meals (16). This dosage consis-tently and reliably reduces the absorption of dietary fat by approximately one-third, resulting in a decrease in avail-able calories after ingestion (15).Orlistat is highly selective and has no significant inhibi-tory effect on the hydrolysis and absorption of carbohydrates, proteins, and phospholipids. In addition, the absorption of orlistat from the GI tract is minimal, and therefore orlistat has virtually no potential for an inhibitory effect on systemic lipase activity (17). Consequently, in contrast to some cen-trally acting appetite suppressants, adverse events owing to systemic drug absorption should be fewer with orlistat. Weight Loss and Prevention of Weight RegainIn clinical trials, treatment with orlistat in combination with a mildly calorie-restricted diet has consistently pro-duced significantly greater weight loss than diet alone in obese subjects. Unless otherwise stated, the results pre-sented subsequently come from the intent-to-treat popula-tion, which includes data from all patients who received at least one dose of study medication and had at least one follow-up efficacy assessment. In a multicenter, 2-yr, ran-domized, placebo-controlled trial conducted in the United States by Davidson et al. (18), 1187 obese men and women (body mass index (BMI) of 30–43 kg/m2) were enrolled in a 1-mo single-blind, placebo lead-in period during which they were encouraged to follow a mildly hypocaloric diet. This diet was designed to provide a 600 kcal/d energy defi-cit with 30% of calories as fat. Subjects (n= 892) who completed this dietary lead-in period were randomly assigned (in a 3:1 ratio) to treatment with 120 mg of orlistat (n= 668) or placebo (n= 224) three times daily for 1 yr. Subjects continued to follow the hypocaloric diet during the first year of double-blind treatment. After 1 yr, subjects treated with orlistat had achieved significantly greater mean weight loss than placebo recipients (8.8 vs 5.8% of initial body weight; p<0.001). Moreover, a significantly higher proportion of orlistat-treated subjects achieved a clinically meaningful weight loss of *5% (65.7 vs 43.6%; p<0.01) or *10% (38.9 vs 24.8%; p <0.05). In the second year of the study, orlistat subjects who completed the first year were rerandomized to three times daily treatment with orlistat (n= 153), half-dose orlistat (60 mg) (n= 152), or placebo (n= 138), while subjects who received placebo during yr 1 Fig. 1. Mode of action of orlistat. TG, triglyceride; MG, monoglyceride; FA, fatty acids.Orlistat: Inhibition of Fat Absorption/HauptmanVol. 13, No. 2203 continued to do so for a second year. In addition, all sub-jects were advised to follow a weight maintenance dietdesigned to promote stable body weight rather than con-tinue with their hypocaloric weight loss diet. Of subjectswho were treated with orlistat during the first year, thosewho were rerandomized to 120 mg of orlistat regained sig-nificantly less of their body weight during the second yearcompared with subjects rerandomized to placebo (35.2 vs63.4% weight regain; p<0.001). Treatment with 120 mg oforlistat for 2 yr resulted in mean weight loss of 7.6%, sig-nificantly greater than with 2 yr of placebo (4.5%; p<0.001). In addition, twice as many orlistat-treated sub-jects maintained a weight reduction of *10% after 2 yr(34.1 vs 17.5%; p <0.05).The weight loss efficacy of orlistat has also been demon-strated in European trials that shared a design and method-ology similar to that of the US study (19,20). In a 2-yr studyof 743 obese subjects (BMI of 28–47 kg/m2), significantly greater mean weight loss was achieved with orlistat plus diet compared to diet alone after 1 yr (10.2 vs 6.1%; p <0.001) (Fig.2) (19). More orlistat-treated subjects than placebo recipients achieved a weight loss of *5% (68.5 vs 49.2%), and twice as many subjects in the orlistat group as in the placebo group achieved a weight reduction of *10% (38.8 vs 17.7%). After 2 yr of treatment, subjects in the orlistat group achieved mean weight loss of 7.8%, com-pared with 4.6% in the placebo group. Twice as many orlistat-treated subjects as placebo recipients maintained a weight loss of *10% (33.8 vs 14.6%; p<0.05). In another 2-yr European study, a significantly greater weight reduc-tion was achieved with orlistat in conjunction with diet compared to diet alone after 1 yr (9.7 vs 6.6%; p<0.001). This significantly greater weight loss with orlistat was sus-tained after 2 yr (7.6 vs 4.5%; p <0.001) (20).As with the study by Davidson et al. (18), participants in both of these European studies switched from a weight loss diet to a weight maintenance diet for the second year. As expected, some regain of lost weight occurred during yr2. However, in both studies, weight regain was reduced by treatment with orlistat compared to placebo.In each of these three 2-yr randomized, controlled trials of orlistat, obese subjects were generally recruited at spe-cialist obesity clinics. However, in a further study, the ef-fect of orlistat was investigated among subjects in a primary care setting (21). A total of 796 obese subjects (BMI of 30–43 kg/m2) entered a 1-mo dietary lead-in period before being randomized to 120 mg of orlistat, 60 mg of orlistat, or placebo three times daily. Subjects were prescribed a hypocaloric diet during the first year of treatment and were switched to a weight maintenance diet for the second year. Unlike previous studies of orlistat, subjects were counseled by health care staff who had no specialist training in diet or obesity management.After 1 yr, subjects treated with 120 mg of orlistat had achieved significantly greater weight loss than placebo recipients (7.9 vs 4.2%; p<0.0001). Significantly greater weight loss with orlistat compared to placebo was sustained after 2 yr of treatment (5.0 vs 1.7%; p<0.0001). In addition, almost three times as many subjects in the orlistat group as in the placebo group maintained a weight loss of *10% after 2 yr (18.6 vs 6.6%; p<0.001). Mean weight reduction in this study, in both the orlistat and placebo groups, was slightly less than that achieved in other trials of orlistat (18,19). H owever, the additional weight loss effect of orlistat compared with diet alone in this study was similar, if not greater, than reported in other studies and suggests that orlistat may be an important adjunct in the manage-ment of obesity in primary care.The maintenance of lower body weight and the preven-tion of weight regain are essential components of success-ful long-term obesity management. In addition to the reduction in weight regain reported in 2-yr studies of orlistat, the effect of orlistat on weight regain has been specifically investigated in a large US multicenter study (22). Obese subjects (BMI of 28–43 kg/m2) were recruited at 17 clinical research centers and prescribed a hypocaloric diet (1000kcal/d deficit) designed to produce a weight loss of 0.5–1.0 kg/wk for a 6-mo period. On completion, sub-jects who had lost *8% of their body weight were random-ized to double-blind treatment with either placebo or 30, 60, or 120 mg of orlistat three times daily in combination with a weight maintenance diet for 1 yr. Of the 1313 sub-jects who entered the weight loss period, 729 achieved a weight reduction of *8% (mean weight loss of 10 kg) and entered the double-blind treatment period. After 1 yr, there was significantly less weight regain with 120 mg of orlistat compared to placebo (32.8 vs 58.7%; p <0.001).The effect of orlistat on body weight has also been dem-onstrated in a multicenter, US-based study of obese sub-jects with type 2 diabetes (23). Weight loss is an important goal of therapy for obese type 2 diabetes patients. However, diabetic patients often have greater difficulty than nondia-betic subjects in achieving clinically meaningful weight Fig. 2. Mean weight loss after 1 yr in obese patients randomized to double-blind treatment with 120 mg of orlistat (n= 343) or placebo (n= 340) plus a mildly hypocaloric diet. (Adapted from Sjöström et al. ref. 19.)Orlistat: Inhibition of Fat Absorption /Hauptman 204Endocrinereduction and maintaining lower body weight through di-etary restriction or behavioral modification (24–26).Weight loss may be especially difficult if patients are re-ceiving treatment with diabetic medications that promote weight gain, such as insulin or sulfonylureas (27,28).A total of 391 subjects with type 2 diabetes controlled with oral sulfonylureas entered a 5-wk lead-in period dur-ing which they received placebo and a nutritionally bal-anced mildly hypocaloric diet (500 kcal/d deficit) (23). On completion, subjects were randomized to either 120 mg of orlistat or placebo three times daily plus dietary interven-tion for 1 yr. Subjects treated with orlistat achieved signifi-cantly greater weight loss than placebo recipients (6.2 vs 4.3%;p <0.001). Furthermore, twice as many patients re-ceiving orlistat lost *5% of their initial body weight (49 vs 23%;p <0.001). Similarly, more orlistat-treated patients than placebo recipients achieved a weight reduction of *10% (17.9 vs 8.8%; p = 0.017).In addition to significantly greater weight loss, patients treated with orlistat also had a greater mean decrease in waist circumference in this study (–4.8 vs –2.0 cm; p <0.01).Waist circumference is a marker of visceral abdominal obesity (29). Excess visceral abdominal adipose tissue is associated with the insulin resistance syndrome, also known as the metabolic syndrome, and is an independent predictor of type 2 diabetes and coronary heart disease (30–32). Sig-nificant reductions in waist circumference after treatment with orlistat were also reported in studies of obese nondia-betic subjects (18,20).Effects of Orlistat on Cardiovascular Risk FactorsModerate weight loss of 5–10% is associated with improvements in several cardiovascular risk factors,includ-ing dyslipidemia, hypertension, hyperinsulinemia, glucose intolerance, and type 2 diabetes (33,34). The effects of weight management with adjunctive orlistat therapy on these coronary risk factors have been assessed in several clinical trials.DyslipidemiaIn the 2-yr study by Davidson et al. (18), patients treated with orlistat achieved significantly greater reductions in serum total and low-density lipoprotein (LDL)-cholesterol than placebo recipients. During the 4-wk dietary lead-in period, total and LDL-cholesterol declined by approx 8%.However, after randomization, total and LDL-cholesterol concentrations increased in the placebo group despite further weight loss, but continued to decline in the orlistat group.After 1 yr, reductions in total and LDL-cholesterol were sig-nificantly greater with orlistat vs placebo (p <0.001) (Fig.3).The improvements in total and LDL-cholesterol achieved with orlistat were independent of the greater weight loss with orlistat compared to placebo. This additional lipid-lowering effect of orlistat is probably related to the partial inhibition of fat absorption from the GI tract. A similar independent lipid-lowering effect was reported in the European trials of orlistat (19,20)as well as in the study of overweight subjects with type 2 diabetes (23).Blood PressureTreatment with orlistat is also associated with improve-ments in systolic and diastolic blood pressure (BP). Numerous studies have reported that clinically significant reductions in BP are achieved with moderate weight loss and that a weight reduction of just 5 kg can significantly reduce BP in obese patients with or without hypertension (35–37). In the David-son et al. (18)study, systolic BP was reduced to a signifi-cantly greater extent with orlistat than placebo after 1 yr (p = 0.002). Diastolic BP also decreased more in the orlistat group than in the placebo group (p = 0.009). Sjöström et al.(19), also reported significantly greater reductions in both systolic and diastolic BP after 1 yr of orlistat compared to placebo. The greater reductions in BP associated with orlistat treatment are consistent with the greater degree of weight loss experienced by the subjects.The effect of orlistat on BP has been further assessed ina metaanalysis of five phase III clinical trials of orlistatFig. 3. Mean (±SEM) changes in serum total and LDL-cholesterol in obese patients randomized to double-blind treatment with 120 mg of orlistat or placebo plus a mildly hypocaloric diet. (Reproduced with permission from ref. 18.)Orlistat: Inhibition of Fat Absorption /HauptmanVol. 13, No. 2205(38). Obese subjects were randomized to orlistat (n = 1559)or placebo (n = 1116) in combination with diet for 1 yr.Among patients who achieved 5% weight loss (59% of orlistat-treated subjects vs 41% of placebo-treated sub-jects), mean systolic and diastolic BPs were reduced by 7.1and 5.4mmHg, respectively, with orlistat (vs 6.7 and 4.5 mmHg, respectively, with placebo). By comparison,reductions in systolic and diastolic BP were substantially smaller in subjects losing <5% of their body weight.Insulin and Glucose MetabolismThere is considerable evidence to suggest that both hyper-insulinemia and hyperglycemia are independent risk factors for cardiovascular disease (39–41). Treatment with orlistat is associated with improvements in insulin and glucose metabolism. In studies of nondiabetic obese subjects, orlistat in combination with diet resulted in significantly greater improvements in levels of fasting serum insulin and glucose after 1 and 2 yr than treatment by dietary intervention alone (18,19). In addition, a metaanalysis of three randomized,placebo-controlled trials has shown that treatment with orlistat may have potential use in preventing or delaying the progression from impaired glucose tolerance to type 2 diabe-tes (42). A total of 650 obese subjects were randomized to double-blind treatment with orlistat or placebo in combina-tion with a mildly hypocaloric diet for 1 or 2 yr. Oral glucose tolerance tests were performed before and after treatment (average duration of follow-up of 587 d). Orlistat-treated subjects lost more weight than placebo-treated subjects (6.7vs 3.8 kg; p <0.001). Among subjects with impaired glucose tolerance at baseline, fewer progressed to diabetic status in the orlistat group than in the placebo group (3.0 vs 7.5%).Conversely, more subjects with impaired glucose tolerance at baseline achieved normal glucose tolerance after orlistat treatment (71.6%) compared with placebo (49.1%) (Fig.4).Treatment with orlistat was also associated with significantly greater reductions in the integrated glucose and insulin areas after oral glucose challenge.Type 2 DiabetesIn a 1-yr study of obese patients with type 2 diabetes by H ollander et al. (23), greater weight loss with orlistat compared to placebo was accompanied by a more marked improvement in glycemic control. H emoglobin A 1c decreased by 0.28% after randomization to orlistat treat-ment whereas the placebo group increased by 0.18%(p <0.001). Fasting glucose decreased by 0.02 mmol/L fol-lowing the use of orlistat whereas it increased by 0.54 mmol/L in the placebo group (p <0.001). In addition, patients treated with orlistat were able to reduce their average dose of sulfonylurea medication to a greater extent than placebo recipients (–23 vs –9%; p <0.05) and fewer orlistat-treated patients withdrew from the study as a result of poor glyce-mic control (2.5 vs 8.8% of patients).Treatment with orlistat also produced greater improve-ments in several serum lipid parameters than placebo in patients with type 2 diabetes. Total cholesterol, LDL-cho-lesterol, LDL:high-density lipoprotein–cholesterol ratio,apolipoprotein-B (all p <0.001), and triglycerides (p <0.05)were all reduced to a significantly greater degree in the orlistat group vs the placebo group after 1 yr.Safety of OrlistatBecause orlistat acts locally in the GI tract and is only minimally absorbed, it has not been shown to be associated with serious systemic adverse events such as those that have been reported with some centrally acting appetite suppressant drugs. Indeed, in clinical trials, orlistat has been shown to be well tolerated by both diabetic and nondia-betic obese subjects (18,19,23). Orlistat was, however,associated with a higher incidence of certain GI events that relate to its partial inhibition of fat absorption, such as fatty/oily stools and fecal urgency. These GI conse-quences of orlistat tended to be of mild to moderate inten-sity, transient, and limited to one to two episodes perpatient. Moreover, these effects mostly occurred withinFig. 4. Percentage of subjects with (A)improvement or (B)deterioration in oral glucose tolerance from randomization to end of treatment. The distribution of categorical status at the end point differed across treatments within the normal at baseline and impaired at baseline cohorts (p <0.05). IGT, impaired glucose tolerance. (Adapted from ref. 42.)Orlistat: Inhibition of Fat Absorption/Hauptman206Endocrinethe first 12 weeks of therapy, with half occurring within the first month. These findings, together with supportive anec-dotal evidence, suggest that the pharmacologic effect of orlistat on fat absorption may encourage long-term compli-ance with a reduced-fat diet (43).The inhibition of dietary fat absorption by one-third with orlistat could, theoretically, have a potential impact on lev-els of fat-soluble vitamins and `–carotene. However, in 2-yr clinical trials, mean levels of vitamins A, D, and E and `-carotene remained within clinical reference ranges (18,19). In the study by Davidson et al. (18), treatment with orlistat compared to placebo was associated with a slightly higher incidence of two or more consecutive low values of vita-mins A (2.5 vs 1.0% of subjects), D (5.8 vs 1.4%), and E (4.2 vs 0.5%) and `-carotene (4.5 vs 0.0%). Supplementa-tion with once-daily multivitamins restored vitamins to within normal ranges in those individuals who experienced low levels.ConclusionPartial inhibition of dietary fat absorption with orlistat has been shown to be a well-tolerated and effective option as an adjunct to mild dietary modification in the long-term management of obesity. In clinical trials, orlistat in con-junction with dietary intervention has consistently and reli-ably been associated with significantly greater weight loss than achieved with diet alone in obese subjects with and without type 2 diabetes. Moreover, significant improve-ments in several obesity-related coronary risk factors, including hypercholesterolemia, hypertension, glucose intolerance, and insulin resistance, have all been reported with orlistat treatment.References1.Lissner, L. and Heitmann, B. L. (1995). Eur. J. Clin. Nutr.49,79–90.2.Golay, A. and Bobbioni, E. (1997). Int. J. Obes.21(Suppl.),S2–S11.3.Bray, G. A. and Popkin, B. M. (1998). Am. J. Clin. Nutr.68,1157–1173.4.Rolls, B. J. (1995). Am. J. Clin. Nutr.61(Suppl. 4),960S–967S.5.Blundell, J. E., Burley, V. J., Cotton, J. R., and Lawton, C. L.(1993).Am. J. Clin. Nutr.57(5 Suppl.), 772S–777S.6.Drewnowski, A., Kurth, C., Holden-Wiltse, J., and Saari, J.(1992).Appetite18, 207–221.7.Abbott, W., Howard, B., Christin, L., et al. (1988). Am. J.Physiol.255, E332–E337.8.Schutz, Y., Flatt, J. P., and Jequier, E. (1989). Am. J. Clin.Nutr.50, 307–314.9.Tremblay, A., Plourde, G., Despres, J.-P., and Bouchard, C.(1989).Am. J. Clin. Nutr.49, 799–805.10.Thomas, C., Peters, J., Reed, G., Abumrad, N. N., Sun, M., andHill, J. O. (1992). Am. J. Clin. Nutr.55, 934–942.11.Astrup, A., Buemann, B., Christenson, N., and Toubro, S.(1994).Am. J. Physiol.266, E592–E599.12.Astrup, A., Ryan, L., Storgaard, M., Saris W. H. M., Hill J. O.(1999).Int. J. Obes.23(Suppl. 5), A304.13.Hyman, F. N., Sempos, E., Saltsman, J., and Glinsmann, W.H. (1993). Arch. Intern. Med.119, 681–687.14.Wadden, T. A. (1993). Arch. Intern. Med.119, 688–693.15.Guerciolini, R. (1997). Int. J. Obes.21(Suppl.), S12–S23.16.Zhi, J., Melia, A. T., Guerciolini, R., et al. (1994). Clin.Pharmacol. Ther.56, 82–85.17.Shepherd, T. Y., Jensen, D. R., Blotner, S., Zhi, J., GuercioliniR., Pace, D., and Eckel R. H. (2000). Int. J. Obes., in press.18.Davidson, M. H., Hauptman, J., DiGirolamo, M., et al. (1999).JAMA281, 235–242.19.Sjostrom, L., Rissanen, A., Andersen, T., et al. (1998). Lancet352, 167–172.20.Rössner, S., Sjöström, L., Noack, R., Meinders, A. E., andNoseda, G. (2000). Obes. Res., in press.21.Hauptman, J., Lucas, C., Boldrin, M., and Collins, H. (2000).Arch. Fam. Med., in press.22.Hill, J. O., Hauptman, J., Anderson, J. W., et al. (1999). Am.J. Clin. Nutr.69, 1108–1116.23.Hollander, P. A., Elbein, S. C., Hirsch, I. B., et al. (1998).Diabetes Care21, 1288–1294.24.Henry, R. R., Wiest-Kent, T. A., Schaeffer, O. G., Kolterman,O. G., and Olefsky, J. M. (1986). Diabetes35, 155–164. 25.Wing, R. R., Marcus, M. D., Epstein, L. H., and Salata, R.(1987).Diabetes Care10, 563–566.26.Guare, J. C., Wing, R. R., and Grant, A. (1995). Obes. Res.3,329–335.27.United Kingdom Prospective Diabetes Study (UKPDS).(1995).BMJ310, 83–88.28.Hanefield, M., Fischer, S., Schmechel, H., et al. (1991). Dia-betes Care14, 308–317.29.Lemieux, S., Prud’homme, D., Bouchard, C., Tremblay, A.,and Despres, J. P. (1996). Am. J. Clin. Nutr.64, 685–693.30.Chan, J. M., Rimm, E. B., Colditz, G. A., Stampfer, M. J., andWillett, W. C. (1994). Diabetes Care17, 961–969.31.Rimm, E. B., Stampfer, M. J., Giovanucci, E., et al. (1995).Am. J. Epidemiol.141, 1117–1127.32.Rexrode, K. M., Carey, V. J., Hennekans, C. H., et al. (1998).JAMA280, 1843–1848.33.Goldstein, D. J. (1992). Int. J. Obes.16, 397–415.34.Pi-Sunyer, F. X. (1996). Clin. Ther.18, 1006–1035.ngford, H. G., Davis, B. R., Blaufox, D., et al. (1991). Hy-pertension17, 210–217.36.Whelton, P. K., Appel, L. J., Espeland, M. A., et al. (1998).JAMA79, 839–846.37.National Institutes of H ealth. National H eart, Lung andBlood Institute. (1997). The sixth report of the Joint National Committee on Prevention, Detection, Evaluation and Treat-ment of High Blood Pressure. National Institutes of Health: Bethesda, MD.38.Patakay, Z. and Golay, A. (1999). Int. J. Obes.23(Suppl. 5),S175.39.Després, J., Lamarche, B., Mauriege, P., et al. (1996). N. Engl.J. Med.334, 952–957.40.Niskanen, L., Turpeinen, A., Penttila, I., and Uusitupa, M. I.(1998).Diabetes Care21, 1861–1869.41.Balkau, B., Shipley, M., Jarrett, R. J., et al. (1998). DiabetesCare21, 360–367.42.Heymsfield, S. B., Segal, K. R., Hauptman, J., Lucas, C.P.,Boldrin, M.N., Rissanen, A. Wilding, J. P. H., and Sjöström, L. (2000). Arch. Intern. Med., in press.43.Aronne, L. J. (1998). J. Am. Diet. Assoc.98(Suppl. 2),S23–S26.。
降血脂的化药种类及他汀类药物研究情况
降血脂化药的种类及其他汀类药物的研究进展高脂血症是一种常见的心血管疾病,常表现为高胆固醇血症(升高),高甘油三脂血症(升高)或二者兼有。
高脂血症是动脉硬化的危险因素,常引起严重的心脑血管并发症,威胁人类健康。
根据近年卫生部在全国范围内进行的中国居民营养和健康状况调查显示,我国成人血脂异常患病率为18.6%,估计全国血脂异常患人数1.6亿。
因此降血脂药物的市场空间巨大,同时也是药物研究的重点之一。
(一) 降血脂药物概况目前临床应用和处在研发阶段的降血脂西药按其降脂机理和化学结构有可分为他汀类、烟酸类、贝特类、胆酸螯合剂类、多烯类以及新型降脂药和各种复方制剂。
1.对胆固醇(TC)的影响1.1对胆固醇(TC)合成的影响代表药物:他汀类如洛伐他汀(Lovastatin),是人工合成的HMG-CoA还原酶抑制剂, 其空间结构与HMG-CoA的结构非常相似,且对HMG-CoA还原酶的亲和力比HMG-CoA强1 万倍。
所以它能竞争性地与HMG-CoA还原酶结合,能抑制肝脏HMG-CoA还原酶催化的HMG-CoA向MV A(甲羟戊酸)转化,从而阻止内源性TC的合成,加速LDL(低密度脂蛋白)的廓清, 使血TC和LDL-c(低密度脂蛋白胆固醇)下降,升高HDL-c(高密度脂蛋白胆固醇)以达到调脂作用。
1.2影响胆固醇吸收药代表药物:依折麦布(eZetimi1e, EZ, 商品名Ze-tia)是一种新的调血脂药物,为选择性胆固醇吸收抑制剂,可抑制胆固醇从小肠吸收,在临床应用中因其可有效弥补他汀类药物的不足而倍受青睐。
由于分子量小,EZ选择性地抑制胆固醇和相关植物甾醇类(pllytosterols)在肠道发生葡萄糖醛酸化后小肠部位的吸收,进而降低血中TC、TG、LDL-c和Apo B(载脂蛋白B, apolipoprotein B),并增加HDL-c水平。
1.3影响胆固醇代谢药代表药物:深海鱼油,最新研究表明深海鱼油能够通过调控LDL-c受体mRNA水平而调节LDL-c受体活性。
Thorpe_Ingold效应及其在有机成环反应中的应用

Ingold 效应及其在有机成环反应中的应用 郑勇鹏等: Thorpe-
综述与评论
的非键相互作用和转动熵下降, 提高了分子内环化 速率。 2009 年 Karaman 通过计算研究了偕二取代溴 丁胺动力学和热力学特性, 表明速率常数仅由基态 和过渡态的自由能决定( 图式 2 )
[8 ]
。
图式 3 图式 2
[8 ] 4溴丁胺的环化
分子内环丙烷化
[10 ]
Scheme 3
Intramolecular cyclopropanation[10]
Scheme 2
Cyclization of 4bromobutylamines[8]
2010 年 Kostal 和 Jorgensen 使用量子和统计力 12学计算分别研究了气相和液相中 2氯乙醇、 氯212丙醇、 甲基氯丙醇在碱催化下反应生成相应 [9 ] CC 键角确实随 环氧化物 。结果表明, 主链中 CQ 着取代甲基数目增加而减小。 气相 MP2 和 CBS计算表明, 三个氯乙醇衍生物反应过程的能量变化 差别非常小; 考虑连续的水合作用或者用 MC / FEP 计算均能准确复现在水存在下的反应情况 , 由此推 测键角压缩效应在氯乙醇环化中主要是溶剂作用 。 Ingold 效 应 可 能 会 受 到 溶 综上 可 知,Thorpe助剂和取代基团等多方面因素的影响 。因此, 在 剂、 Ingold 效应的作用时, 考虑反应中 Thorpe要充分考 虑这些因素。 Ingold 效应的实质还没有完善的理 虽然 ThorpeIngold 效应有效地促使 论来解释, 但是应用 Thorpe确实是一个很好的方法。 本文侧重讨 分子内环化, Ingold 效应用于分子内和分子间环化形成 论 Thorpe三至六元环产物的研究。
奥利司他胶囊说明书---文本资料

奥利司他胶囊说明书请认真阅读说明书并按说明使用或在药师指导下购置和使用。
[ 药品名称 ]通用名称:奥利司他胶囊商品名称:英文名称:汉语拼音:[成份 ][性状 ][ 作用类型 ] 本品为抗肥胖症药类非处方药药品。
[ 适应症 ]用于肥胖或体重超重患者(体重指数≥ 24)的治疗。
[ 规格 ]0.12 克[ 用法用量 ] 成人:餐时或餐后 1 小时内口服 1 粒。
假若有一餐未进或食品中不含脂肪,则可省略一次服药。
[ 不良反响 ]1.常有不良反响为:油性斑点,胃肠排气增加,大便紧迫感,脂肪(油)性大便,脂肪泻,大便次数增加和大便失禁。
随饮食中脂肪成分增添,发生率也相应增高。
大多数病人用药一段时间后可改良。
2.许多出现的胃肠道急性反响有:腹痛/ 腹部不适、胃肠胀气、水样便、软便、直肠痛/直肠部不适、牙齿不适、牙龈不适。
3.察看到的其余少见不良事件有:上呼吸道感染、下呼吸道感染、流行性感冒、头痛、月经失调、忧虑、疲惫、泌尿道感染。
4.使用奥利司他已有稀有的转氨酶高升、碱性磷酸酶高升和重度肝炎的报告,并出现肝衰竭病例,此中部分患者需要进行肝移植或可直接致使死亡。
奥利司他还有发生稀有过敏反响的报导,主要临床表现为瘙痒、皮疹、荨麻疹、血管神经性水肿、支气管痉挛和过敏性反响,出现大疱疹十分稀有。
上市后监测还发现有胰腺炎的报导。
[禁忌 ]1.孕妇禁用。
2.对奥利司他或药物制剂中任何一种成份过敏的患者禁用。
3.慢性汲取不良综合征、胆汁郁积症患者禁用。
4.器质性肥胖患者(如甲状腺机能减退)禁用。
[ 注意事项 ]1.第一次使用本品前应咨询医师,治疗时期应按期到医院检查。
特别是伴发高血脂、高血压、糖尿病和中度以上脂肪肝的病人,应在医师指导下联合其余药物进行治疗。
2.不介绍体重指数低于24 的人群使用本品。
体重指数近似值的计算方法为体重/身高 2(体重以千克为单位计算,身高以米为单位计算)。
3.服用本品时应尽量减少摄取脂肪含量高的食品。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
奥利司他的全合成摘要介绍了减肥药物奥司利他的12种不同的全合成方法.关键词奥利司他;全合成;减肥药物;不对称合成Total Synthesis of OrlistatAbstract Introduction of twelve different methods in total synthesis of orlistat.Key words Orlistat;total synthesis;anti-obesity drug;Mitsunobu reaction;asymmetric synthesis奥利司他[1]是由瑞士霍夫曼罗氏公司(Hoffmann-La Roche Inc)研制生产的一类新药,于1999年4月23日由FDA批准作为处方药上市用于肥胖治疗。
本品是链霉菌属toxytricini的天然产物lipstain的化学合成衍生物。
别名伊宁曼、雅塑、舒尔佳、赛乐西、赛尼可、赛乐西、奥列司他、xenical、tetrahydrolipstatin,产品名称为伊宁曼或伊宁曼奥利司他片。
2011年3月正式在国内上市,非处方药,是国内唯一通过临床验证过的同类药物,有中国版的Alli之称。
奥利司他是目前全球唯一的OTC减肥药,全球超过40000000人服用并成功减重,是目前最畅销的减肥产品。
奥利司他是一种强效和长效的特异性胃肠道脂肪酶抑制剂,它可抑制胃肠道消化脂肪所需的酵素,包括胰酯及胃酯,而减少胃肠道酯对脂肪的吸收,以辅助减肥通过直接阻断人体对食物中脂肪的吸收,摄入的热能和脂肪一旦小于消耗,体内脂肪自然减少,从而达到减重的目的。
它是安全减肥药,有效成分不进入血液循环,不作用于中枢神经,副作用较少,不会出现头晕、心慌、失眠、口干等情况,但仍需配合运动及饮食,方有减肥之功效。
目前中国市场上存在的奥利司他分为奥利司他片及奥利司他胶囊。
伊宁曼奥利司他片是浙江海正药业汇集博士学位者50多人,硕士学者位200多人,外籍专家20多人的团队历时6年研究仿制的产品。
奥利司他胶囊为重庆植恩药业生产。
一.奥利司他的基本信息奥利司他(Orlistat),商品名称为伊宁曼或伊宁曼奥利司他片,分子式C29H53NO5,分子量495.7。
化学别名为:(3s,4s)-3-己基-4-[(2s)-2-羟基十三烷基]-2-氧杂环丁酮N-甲酰基-L-亮氨酸酯。
白色结晶性粉末,几乎不溶于水,易溶于氯仿,极易溶于甲醇和乙醇。
其分子是含四个手性中心的非对应异构体,在波长529nm 处,其乙醇溶液具负旋光性[1]。
化学结构式如下:H2)5CH 3二.奥司利他的全合成2.1 徐勤耀等[2]人以月桂醛和1,3-二(三甲基硅氧基)-1-甲氧基-1,3-丁二烯(Chan ’s Diene)在(s)-(-)-1,1’联-2-萘酚以及催化剂作用下发生向山羟醛不对称反应(Mukaiyama-aldol)反应得到手性羟基十六酮酸酯,用甲氧基苄基(PMB)保护羟基,再进行Noyori 催化氢化,经过β-羟基酸酯不对称烷基化(Frater-Seebach)反应,酯的水解得酸,然后通过对甲苯磺酰氯环化,对甲氧基苄基在钯碳作用下脱除,最后与L-亮氨酸通过Mitsunobu 反应接上氨基酸侧链后即得到目标分子奥利司他。
C 11H 23CHO +OTMS TMSO4C 11H PMBOC(=NH)CCl 3PPTSC 11H(S)-BINAP-RuCl 2,H 2,MeOHC 11H613C 11H613KOHC 11HC 11H2)5CH 3Pd/C,H 2,EtOHC 11H 2)5CH 32)5CH 32.2 Barbier, P.等[2-3]以月桂醛为原料,首先亲核加成,烯丙位碳负离子进攻月桂醛,手性试剂作用下构建了手性化合物,三乙胺作用下脱氯化氢,后成环反应,过氧化氢成环,开环得手性羟基,羟基保护,开环,羰基α位引入手性基团,分子内成环,Mitsunobu 反应和催化加氢反应,最后发生亲核反应得到奥利司他。
OC 11H 23H 2CBrCH 2HOC 11H 23H 2C OClTEA,DMAPH 2C OOCH 2C 11H 23Grubbs catalystOOC 11H 232211H 23411H 23Tbdms-Cl11H 23tbdmsTEA C 11H 23OHOtbms OCH 3OC 11H 23OOtbms OCH 3O phtC 11H 23O OHOCH 3O thp C 11H O 3thp 6136132C 11H C 11H 6H 136H 13OHOPhDCC, DMAP6H 1326H 13H 2)5CH 32.3 以3-羟基-6-庚烯酸乙酯为起始原料,在烯烃氧化和Wittig 反应延长碳链后, 还原酯基得到醛中间体,与辛酸进行Aldol 缩合构建了消旋的奥利司他分子的碳链骨架。
柱层析得到反式构型的β-羟基羧酸中间体,在苯磺酰氯和吡啶的条件下环合,脱去THP 保护基后得到反式β内酯环。
最后Mitsunobu 反应接上氨基酸侧链和催化加氢得到消旋的目标分子奥利司他[2-5]。
2Et①②③CH 3(CH 2)7PPh 3Br,BuLi,r.t DIBHLC 7H 15CO 2H,-50℃,LDA2H2)5CH 322)5CH 3PPTS, 50℃,charomatography2)5CH 3N-formylleucine, PPh 3, DEAD2H2)5CH 32.4 以β-酮酯为起始原料,同样以Aldol 反应构建了碳链骨架。
在β内酯环形成之后,柱层析分离得到两组消旋的反式β内酯环中间体。
在Mitsunobu 反应后得到4个非对映异构体产物,其中的一个产物与目标分子完全一致。
在将消旋的反式内酯环中间体转化成六元环化合物后,核磁共振分析得以确定相对构型,再结合目标分子中的构型的手性源进行分析,可以确认所需的奥利司他分子构型[3-5]。
O(CH 2)5CH 3COOMe ①③NaBH 4,THF,MeOHH 3C(H 2C)10OHOTHP CO 2Me (CH 2)5CH 3①②C 6H 6SO 2Cl,Py,0~5℃H 3C(H 2C)10THPOOO(CH 2)5CH 3H 3C(H 2C)2)5CH 3H 2)5CH 32.5 以苄基保护的R-β-羟基醛为原料,以消旋的Aldol 反应缩合形成主碳链的骨架。
消旋的中间体环合得六元环的β-羟基-δ-内酯后,氧化得到β-酮基-δ-内酯。
氯仿溶液中,化合物主要以烯醇式存在。
在催化加氢的条件下,得到单一构型的β-羟基-δ-内酯,之后开环,成环内酯,最后脱苄基,Mitsunobu 反应接上氨基酸侧链后即得到目标分子奥利司他[4,6]。
H 3C(H 2C)①②LDA,octanoic acid 10% Pd/C,H 2H 3C(H 2C)253①②Jone's oxidation2)5CH 3H 3C(H 2C)2)5CH 3H 3C(H 2C)22)5CH 3H 3C(H 2C)①②③1mol ·L -1 KOH BnBr,THF,HMPAH 3C(H 2C)2Bn 2)5CH 3①②10% Pd/C,H 2③C 6H 5SO 2ClH 3C(H 2C)2)5CH 3①②PPTSPPh 3,DEAD,N-formyl-leucineH2)5CH 32.6 首先进行酯化和氧化反应,缩合可以一步得到反式的β-内酯环中间体,非对映异构体的比率为4∶1。
柱层析得到所需中间体后,Mitsunobu 反应接上氨基酸侧链后即得到目标分子奥利司他[5,7]。
H 3C(H 2C)10OOH O①PPTS, 2-methoxy-propene H 3C(H 2C)10H OO OCH 3(CH 2)5OLiBtH 3C(H 2C)2)5CH 3H 3C(H 2C)2)5CH 3+N-formylleucine, PPh 3,DEADH 2)5CH 32.7以(-)-N-甲基麻黄碱为手性辅助试剂,在TiCl4的催化下,手性烯醇硅醚与苄基保护的R-β-羟基醛缩合,以较高的立体选择性得到目标分子中的手性中心(dr=3:1)。
再水解脱去手性辅助试剂、成环、脱去苄基以及Mitsunobu反应接上氨基酸侧链后即得到目标分子奥利司他[3,5]。
N(CH2)5CH3+H3C(H2C)4H3C(H2C)252mol·L-1 KOHH3C(H2C)253C6H5SO2Cl,Py,0℃H3C(H2C)2)5CH3②2PPh3,DEAD,N-formylleucineH2)5CH32.8以(R)-α-苯甲酰氧基酮和苄基保护的R-β-羟基醛为原料,在硼试剂的参与下,高立体选择性地得到反式Aldol缩合物。
再将Aldol产物中的手性辅基部分转化成二醇,并氧化断链后,成环、脱去苄基以及Mitsunobu反应接上氨基酸侧链后即得到目标分子奥利司他[5,8-10]。
H3C(H2C)10OBzOCH3c-HexBCl,Me2NEt-78℃,H2O2,NaOH,MeOHH3C(H2C)LiAlH4,-78~20℃H3C(H2C)2324H3C(H2C)613C6H5SO2Cl,Py,0~4℃H3C(H2C)2)5CH310% Pd/C,H23H2)5CH32.9以月桂醛为原料得到的(R)-β-烷硅氧基十四醛,在CH2Cl2/H2O的两相体系中及相转移催化剂(n-Bu4N+I-)的存在下,与(2E)-壬烯基三氟化硼钾盐反应,得到1,2-anti-2,4-anti加成物和1,2-anti-2,4-syn加成物,比例为3:1。
苄基保护的R-β-羟基醛在催化下得到反式加成物和顺式加成物,臭氧氧化化合物中的双键得酸中间体,在PhSO 2Cl 和Pyridine 的条件下环化成反式和顺式β内酯。
顺式可在动力学条件下50%转化成反式。
成环、脱去苄基以及Mitsunobu 反应接上氨基酸侧链后即得到目标分子奥利司他[5,11]。
C 11H③①①(2E)-n-C H =CHCH BF -K +, n-BuN +I-222C 11H 613①②224t-BuOH,CH 3CH=C(CH 3)2C 11H 61323N-formylleucine,PPh 3,DEADH 2)5CH 32.10 以(E,E)-2,4-十六二烯酸甲酯为原料,与羧酸反应成酯后,Shar-pless 不对称二羟基化反应得到二醇。
二醇中间体在SOCl 2的作用下得到环亚硫酸酯,烷基化反应立体选择性得到中间体。
锌粉/醋酸脱酯后,在CH 2Cl 2/NaHCO 3水溶液的两相体系中,反式内酯产物和顺式内酯产物的比例为1∶2。