大前庭水管综合征家系SLC26A4基因突变分析
GJB2、SLC26A4基因相关耳聋儿童的听力损失特点分析

GJB2、SLC26A4基因相关耳聋儿童的听力损失特点分析崔庆佳;孙喜斌;戴朴;黄丽辉;王国建;张媛;杨影;康东洋;杜延顺;赵丽萍;黄莎莎;张伟【摘要】Objective To determine the audiological characteristics in 832deaf children with biallelic causative mutations in GJB2 ,SLC26A4gene .Methods The 832 patients received deafness gene screening ,553 were GJB2 gene biallelic causative mutations ,279 were SLC26A4 gene biallelic causative mutations .Patients were divided into four groups according to ages of hearing loss onset :<1 ,1~3 ,3~6 ,6~12 years old ,and the audiological character-istics and prevalence of GJB2 ,SLC26A4 gene mutations at different ages of onset .Results The prevalence of GJB2 gene mutations at four groups was 37 .97% (210/553) ,38 .34% (212/553) ,16 .27% (90/553) ,7 .41% (41/553) ,re-spectively ;the prevalence of SLC26A4 gene mutations at four groups was 25 .45% (71/279) ,44 .80% (125/279) , 20 .07% (56/279) ,9 .67% (27/279) ,respectively .The difference between GJB2 and SLC26A4 gene was significant(P=0 .001) .The prevalence of profound hearing loss with GJB2 gene mutations at four groups were 66 .67%(140/210) ,61 .32% (130/212) ,47 .78% (43/90) ,41 .46%(17/41) ,respectively .The difference was significant (P=0 .004) ,while the difference in 279 patients with SLC26A4 gene mutations was not statistically significant (P= 0 . 083) .Conclusion The age of hearing loss onset in patients with biallelic causative mutations in GJB 2 or SLC26A4 gene refers to 0~3 years -old ,hearing loss in patients with GJB2 ,SLC26A4 gene mutations gives priority to pro-found .The age of hearing loss onsetis smaller ,the ratio of profound hearing loss is higher .Patients with severe and profound hearing impairment should be performed the genetic testing when the age of onset under 12 .%目的:探讨明确为GJB2、SLC26A4基因相关耳聋儿童的听力损失特点。
【国家自然科学基金】_大前庭水管综合征_基金支持热词逐年推荐_【万方软件创新助手】_20140801
2013年 序号
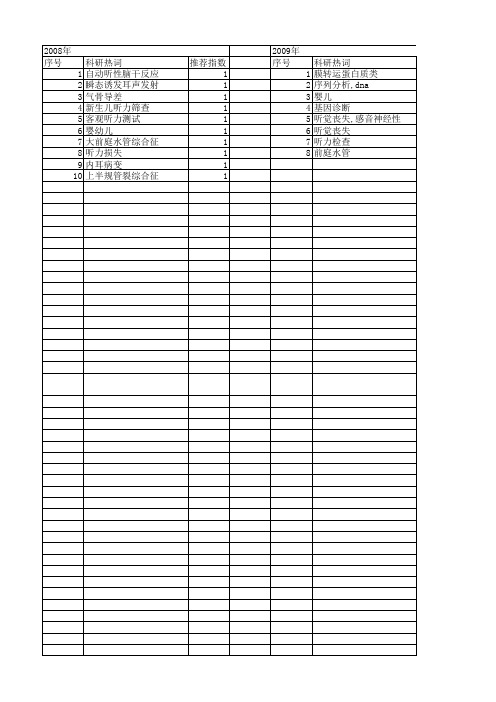
科研热词 1 疗效 2 大前庭水管综合征 3 住院患者
推荐指数 1 1 1
2014年 序号 1 2 3 4 5 6 7 8 9 10
2014年 科研热词 推荐指数 耳聋 2 致病性 1 突变 1 大前庭水管综合征(单侧) 1 大前庭水管综合征 1 基因诊断 1 基因芯片 1 slc26a4基因 1 slc26a4 1 ivs16+10 c>t 1
2008年 序号 1 2 3 4 5 6 7 8 9 10
科研热词 自动听性脑干反应 瞬态诱发耳声发射 气骨导差 新生儿听力筛查 客观听力测试 婴幼儿 大前庭水管综合征 听力损失 内耳病变 上半规管裂综合征
推荐指数 1 1 1 1 1 1 1 1 1 1
2009年 序号 1 2 3 4 5 6 7 8
推荐指数 2 2 1 1 1 1 1 1 1 1 1
2011年 序号 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33
2011年 科研热词 推荐指数 错义突变 1 遗传咨询 1 转运功能 1 致病性 1 耳聋综合征 1 耳聋 1 细胞膜 1 突变谱 1 突变体蛋白 1 突变 1 离子转运 1 甲状腺激素 1 甲状腺功能低下 1 热点突变 1 感音神经性聋 1 序列分析 1 寡核苷酸序列分析 1 家族性甲状腺肿 1 大前庭水管综合征 1 大前庭水管 1 基因芯片 1 基因突变 1 基因异常 1 基因(gene) 1 基因 1 听力障碍 1 听力受损者 1 前庭疾病(vestibular diseases) 1 前庭水管 1 内耳畸形 1 内淋巴管 1 内淋巴囊 1 slc26a4基因 1
Goldengate高通量耳聋基因芯片在大前庭水管综合征中的有效性验证及应用分析
•138 •屮华耳鼻咽喉头颈外科杂志202丨年 2 月第56 #第2 期(:丨丨in J ()t»>rhim>lar>ng»l Head Neck Surg, M>mar> 2021. V»l. 56, V>. 2•新技术新材料-Goldengate尚通量耳聋基因芯片在大如庭水管综合征中的有效性验证及应用分析吴宏蒋璐刘畅刘亚兰龙梦琦梅凌云贺楚峰蔡鑫章陈红胜冯永中南大学湘雅医院耳鼻咽喉头颈外科耳鼻咽喉科重大疾病研究湖南省重点实验室,长沙 410008冯永现在南华大学附属长沙中心医院耳鼻咽喉科410004通信作者:冯永,Email:***********************oni【摘要】目的将Goldengale高通量耳聋基因芯片应用于大前庭水管综合征患者,验证芯片的准确性及有效性,为制定更加详细的大前庭水管综合征遗传检测策略提供参考方法2016年8月至2018年2月利用本研究团队研发的Goldmgate高通迓耳聋检测芯片,检测丨5例确诊为大前庭水管综合征耳浮患者及60例健康人对照样本,并•利用S anyr测序法验证芯片检测结果所有大前庭水管综合征患者均进行57X26,44基因测序,并与芯片结果进行对比分析结果12/15患者通过芯片检测出.S’LC26,44椹W突变,通过芯片检测和SAC26.料基因直接测序共检出9种突变,其中7种突变被两种方法均检出,该芯片可检测出基W1*£接测序法所提供的等位基因信息的93.33%( 28/30)除•S/X26.44基因以外,丨5例大前庭水管综合征患者通过芯片还同时检测出、PC’/)///5、m C7、M V Y沁以及线粒体基丨大丨的突变,并均经过S anyr测序法得到验证结论Goldengate*高通量耳聋基W芯片具有检测潰盖广、准确性高等特点,可作为大前庭水管综合征患者的初步检测手段【关键词】大前庭水管综合征;基因芯片基金项目:湖南f t「丨然科学基•金(20丨7JJ3476)Validation and analysis of Goldengate high-throughput deafness gene chip in detecting thepatients with enlarged vestibular aq u e d u ct syndrom eWu Hong, Jiang Lu, Liu Chang, Liu Yalan, Long Mengqi, Mei Lingyun, He Chufeng, Cai Xinzhang,Chen Hongsheng, Feng YongDepartment of Otorhinolaryngology Head and Neck Surgery, Xiangya Hospital, Central SouthUniversity, Key Laboratory of Otorhinolaryngology, Hunan Province, Changsha 410008, ChinaFeng Yong is now in the Department o f Otorhinolaryngology, Changsha Central Hospital, University ofSouth China, Changsha 410004, ChinaCorresponding author: Feng Yong, Email: ***********************【A bstract 】Objective To verify the accuracy and effectiveness of Goldengatehigh-throughput deafness gene chip in detecting the patients with enlarged vestibular aqueductsyndrome(EVAS), and to provide a reference for genetic detection strategy of EVAS. Methods FromAugust 2016 to February 2018, 15 patients with EVAS and 60 normal controls were detected byGoldengate high-throughput deafness detection chip developed by our team, and the results wereverified by Sanger sequencing. SLC26A4gene sequencing was carried out in all the patients withEVAS. Results 12/15 of patients with EVAS were detected mutations of SLC26A4gene. Ninem utations were detected by chip detection and SLC26A4gene direct sequencing, seven of whichD O I: 10.3760/l 15330-20200302-00150收稿日期2020-03-02 本文编辑金昕引用本文:吴宏,蒋璐.刘畅,等.Goldengate高通量耳聋基W芯片在大前庭水管综合征中的有效性验证及应用分析I J1.中华耳鼻咽喉头颈外科杂志,2021. 56(2): 138-143.丨)()丨:10.3760/(ma. j.cn115330-20200302-00150.中 $丨〔鼻咽喉头颈外f’l H、202 I<丨'2 ).j 第 56 卷第2 期(Ihin .1()t«>rhi!i〇Unyng()l Head N<-ck Smg. I rhruary 2021, \Ol. 56. No. 2•139 •were detected by both methods. The chip could detect 93.33%(28/30) of the allele informationprovided by SLC26A4gene direct sequencing. In addition to SLC26A4gene, m utations of G]B2,PCDH15, TMC1, MY06and mitochondrial genes were detected in 15 patients with EVAS. Theseresults were verified by Sanger sequencing. Conclusion Goldengate high-throughput deafnessgene chip possesses the traits of wide coverage and high accuracy, which can be used as apreliminary detection method for patients with EVA S.【K e y w o r d s】Vestibular aqueduct enlargement syndrome; Gene chipFund program:Hunan Natural Science Foundation Project(2017)J3476)耳聋是最常见的感觉神经性疾病:|,据报道,全球有2.5亿人患有中度以上听力损失2 :中国每 年约有3万先天性听力损失患儿出生:3]。
感音神经性耳聋患者大前庭导水管综合征相关SLC26A4基因IVS7-2A>G的全序列分析

感音神经性耳聋患者大前庭导水管综合征相关SLC26A4基因IVS7-2A>G的全序列分析李琦;黄德亮;朱庆文;袁永一;方如平;戴朴【期刊名称】《中华医学遗传学杂志》【年(卷),期】2010(027)006【摘要】目的对携带SLC26A4基因IVS7-2A>G单杂合突变感音神经性耳聋患者进行 SLC26A4基因的全序列检测,以期发现除IVS7-2A>G以外的其他突变.方法应用直接测序法对80例携带IVS7-2A>G单杂合突变的感音神经性耳聋患者进行SLC26A4基因进行全序列测序.结果 80例患者中47例发现另1个突变位点,其余33例未发现复合杂合突变,IVS7-2A>G单杂合突变找到另外1个突变的比例为58.8%(47/80).发现了 3个新的突变,分别是5+2T>A、14-2A>G和1825del G,最为常见的5种突变为H723R(20%)、T410M(5%)、15+5G>A(5%)、L676Q(5%)、N392Y(3.75%).第17外显子是突变发生种类最多的外显子.结论SLC26A4基因IVS7-2A>G单杂合突变者应该进行其他突变的筛查,SLC26A4基因复合突变可以解释部分的耳聋原因.%Objective To investigate the whole sequence of the SLC26A4 gene in moderate to profound sensorineural hearing loss (SNHL) patients with IVS7-2A>G mutation of the gene in China.Methods Whole SLC26A4 gene sequence was analyzed by direct sequencing in 80 SLC26A4 gene IVS7-2A>G mutation carriers for the occurrence of a second mutation in the gene. Results Forty-seven out of the 80 patients were found to have a second heterozygous mutation, whereas a single IVS7- 2A> G mutation could be responsible for SNHL inthe remaining 33 patients. Three novel mutations, 5+ 2T>A,14-2A>G and 1825del G, were identified. The five most common mutations includeH723R (20%),T410M (5%), C. 1705+5G>A (15+5G>A) (5%), L676Q(5%), and N392Y (3. 75%). Exon 17 harbored the most types of compound heterozygosity with the IVS7 - 2A>G mutation. Conclusion A Chinese specific SLC26A4 diversity was found, and comparable SLC26A4 contributing to deafness. This study suggested that if a heterozygous SLC26A4 mutation is found in a patient with deafness, other exons of the SLC26A4 gene should be analyzed. Furthermore, double heterozygosity of theSLC26A4 gene may also account for some of the disease phenotype.【总页数】6页(P610-615)【作者】李琦;黄德亮;朱庆文;袁永一;方如平;戴朴【作者单位】210008,南京医科大学附属南京儿童医院耳鼻咽喉-头颈外科;210008,南京医科大学附属南京儿童医院儿童听力中心;中国人民解放军总医院耳鼻咽喉-头颈外科;中国人民解放军总医院耳鼻咽喉-头颈外科;中国人民解放军总医院耳鼻咽喉-头颈外科;210008,南京医科大学附属南京儿童医院耳鼻咽喉-头颈外科;中国人民解放军总医院耳鼻咽喉-头颈外科【正文语种】中文【相关文献】1.30例大前庭水管综合征患者 SLC26A4基因诊断与听性脑干电位特性分析2.大前庭水管综合征患者的SLC26A4基因诊断3.大前庭水管综合征家系特征与SLC26A4基因分析4.27个省市聋校学生基于SLC26A4基因IVS7-2A>G突变的全序列分析5.河南两地区聋儿教育机构患者大前庭水管相关SLC26A4基因热点突变筛查分析因版权原因,仅展示原文概要,查看原文内容请购买。
大前庭水管相关SLC26A4基因热点突变区域筛查方案探讨

2 2・ 9
C ieeJ un l fO oo yVo. , o3 2 1 hn s o ra tlg 18 N ., 0 0 o
●
Hale Waihona Puke 临床研究・ 大前庭水管相关 S C 6 基 因热点突变 区域 L 2A 4 筛查方案探讨
袁 永一 王 国建 黄 德 亮 康 东 洋 戴 朴
突变 区域 的筛 查 策 略 。 方 法
患 者 外周 血 并 提 取 D A, 行 S C 6 4基 因 编码 区 2 N 进 L 2A 0个 外 显 子测 序 ,总 结 筛 查 到 的 各种 S C 6 4基 因 突变 类 型 L 2A 在 不 同外 显子 的分 布 及 各 外 显 子 上 S C 6 4基 因突 变 数 占全 部 突 变 的 比例 。 结 果 L 2A 9 .% ( 5 / 6 ) 5 4 2 1 2 3 的大 前 庭 水
中 国人 民解 放 军 总 医 院耳 鼻 咽 喉头 颈 外科 耳 鼻 咽 喉研 究 所 聋 病 分子 诊 断 中心 ( 京 1 0 5 ) 北 0 83
【 摘要 】目的
明确中国人群大前庭 水管相关 S C 6 4基 因热点突变区域 , L 2A 制定耳聋人群 乩 C 6 4基 因热点 2A
确 诊 大 前庭 水 管 患 者 2 3例 ,所 有 患 者 都 接 受 了 高 分 辨 率 颞 骨 C 6 T检 查 , 集 受 检 采
的明 确为 研 制 S C 6 L 2 A4基 因专 病 诊 断 芯片 提 供 了依 据 。
【 键词 】 大前 庭 水 管综 合 征 ; s C 6 关 L 2A4基 因 ; 热点 突变 区域 ; 筛查 策 略 【 中图分 类号 】 R 6 .3 R 9 .1 747 , 3 41 2 【 文献 标 识 码 】 A 【 章 编 号 】 1 7 — 9 2 2 1 )3 22 0 文 6 2 2 2 (0 0 0 — 9 - 4
大前庭导水管综合征

04 治疗与康复
药物治疗
药物治疗
对于大前庭导水管综合征引发的眩晕和听力下降等症状,医 生可能会开具药物治疗,如抗眩晕药、改善微循环药物等, 以缓解症状。
药物治疗注意事项
药物治疗需在医生指导下进行,患者需严格遵守医嘱,注意 药物副作用和相互作用,如有不适及时就医。
助听器与人工耳蜗植入
助听器
对于听力下降的患者,医生可能会建 议使用助听器来提高听力水平。选择 合适的助听器并进行专业调试,有助 于改善患者的听力状况。
新型治疗方法
开发出针对大前庭导水管综合征的药物治疗和听力康复方法,有效 改善患者生活质量。
临床诊断标准
建立了一套准确、可靠的诊断标准,有助于早期识别和干预大前庭导 水管综合征。
未来发展方向
跨学科合作
加强医学、生物学、物理学等多学科的合作,共同推进大前庭导 水管综合征的研究。
临床试验与转化研究
开展更多的临床试验,将研究成果转化为实际的治疗手段,惠及更 多患者。
定期复查
患者应遵医嘱定期到医院复查,以便及时了解病 情变化。
听力训练
对于听力下降的患者,可以进行听力训练,以改 善听力状况。
注意事项
避免过度使用药物
01
患者应避免过度使用药物,尤其是耳毒性药物,以免加重听力
损伤。
注意情绪调节
02
患者应注意情绪调节,保持乐观的心态,以利于病情的恢复。
及时就医
03
如出现听力下降、眩晕等症状加重或持续不缓解的情况,应及
人工耳蜗植入
对于严重听力丧失的患者,人工耳蜗 植入是一种有效的治疗方法。通过手 术将人工耳蜗植入体内,患者可以重 新获得听觉功能。
康复训练
平衡与协调训练
单侧大前庭水管综合征SLC26A4基因的突变分析
HU ANG S h a s h a ,HU A NG Ba n g q i n g  ̄ ,DONG Mi n ,ME NG Xi a o x i a o ,DA I Pu ’
t i b u l a r a q u e d u c t s y n d r o me ,a n d e x p l o r e t h e r i s k f a c t o r s o f t h e u n i l a t e r a l e n l a r g e d v e s t i b u l a r a q u e d u c t s y n d r o me . Me t h o d s Al l p a t i e n t s wi t h h e a i r n g t e s t a n d t e mp o r a l b o n e C T s c a n r e c e i v e d t h e g e n e t i c t e s t s i n c o d i n g r e g i o n o f S L C 2 6 A4 , a n d t h e p a - t i e n t s we r e d i v i d e d i n t o t w o g r o u p s a c c o r d i n g t o t h e t e mp o r l a b o n e C T: u n i l a t e r a l a n d b i l a t e r a l e n l a r g e d v e s t i b u l a r a q u e d u c t .
C o r r e s p o n d i n g a u h o r D AI Pu , Ema i l d a i p u 3 O l @ v i p . s i n a . c o n r
大前庭水管综合征及其相关的基因_SLC26A4

大前庭水管综合征及其相关的基因—SLC26A4赵亚丽翟所强王秋菊中国人民解放军总医院耳鼻咽喉研究所(北京100853)临床和流行病学研究表明,每1000名新生儿中就有1名先天性耳聋的患儿。
大前庭水管综合征(largevestibularaqueductsyndrome,LVAS)是先天性耳聋的一种。
1978年,Valvassori和Clemis[1]在对3700例颞骨连续分层摄片中发现,有50例前庭水管扩大,并将其命名为大前庭水管(dilatedvestibularaqueduct,DVA),又将临床上伴感音神经性听力损失等症状者称“大前庭水管综合征”。
近年,随着CT、MRI以及分子遗传学的发展,对此病的认识已经从影像学诊断、临床表现、发展到了分子诊断的水平。
1大前庭水管综合征的临床表现、发病机理及诊断大前庭水管是儿童感音神经性聋最常见的内耳畸形,由其导致的大前庭水管综合征是一种独立性疾病,除了前庭水管扩大外,不合并其它畸形,属于非综合征型耳聋。
其临床表现为波动性感音神经性听力损失,多呈进行性下降。
可从出生后至青春期这一年龄段内任何时期开始起病,但多数为出生后几年内发病。
发病突然或隐匿,通常之前有感冒、轻微颅外伤或其他使颅内压增高的病史。
约81%-94%的患者为双侧发病,单侧发病者少见[2]。
听力受损以高频为主,听力图多为下降型,少数为平坦型,无一例为上升型[3]。
听力下降的程度与前庭水管的大小无关,可表现为从接近正常到极重度聋。
并且,双耳听力可不对称。
大多数患者仅表现为听力损失,只有少数患者伴有前庭症状,约占29%,但有人认为前庭症状少见可能与发病人群多为幼儿有关[4]。
目前,关于前庭水管扩大导致感音神经性聋的致病机理还不是很清楚,通常有三种假说:(1)内淋巴液返流学说,前庭水管扩大时,往往同时伴有内淋巴管和内淋巴囊的异常扩大,突然的脑压变化,迫使两层脑膜间内淋巴囊内容返流入耳蜗,囊内高渗内淋巴进入耳蜗基底周,损伤神经感觉上皮,产生感音神经性耳聋。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
syndrome in 6 nuclear families were recruited.A family unit consisted of a mother and father and their children.Genome DNA was extracted from the peripheral blood.All the 21 exons were amplified by intronic polymerase chain reaction fPCRl.Then the PCR products were purified and directly sequenced.The sequences were analysed with DNAStar and BioEdit.Results All the 1 2 patients in the 6 families had two mutant alleles.A total of 6 SLC26A 4 mutations were
【Key words】Large vestibular aqueduct syndrome;SLC26A 4 gene;Gene mutation;Genotype
大前庭水管综合征(Large vestibular aqueduct syndrome)是一种常见的先天性内耳畸形,自从1978 年Valvassori和Clemis等…在颞骨连续摄片中发现 并将其命名以来,对于大前庭水管综合征的研究已 广泛开展。目前,对于大前庭水管综合征临床表现 的了解已较为清楚:表现为感音神经性听力损失, 部分患者存在低频骨气导差,具有混合性听力损失 成分:听力下降常常发生在学龄前,呈波动性或进 行性下降:听力损失程度从轻度到极重度不等,多 数达重度或极重度。
1746delG and’H723R/E303Q,respectively.Genotypes of two patients in each familie were the same.However,the
genotypes of two patients in family 673 or 701 were different,because the proband inherited two mutant alleles from both
所有参加者均接受了详细的病史和家族史调 查,并进行了系统的体格检查,以便排除环境因素 及综合征因素造成的听力损失患者。甲状腺的评估 由专科医生进行。耳镜检查。听力学检测:声导 抗,根据检测年龄及配合程度选择纯音测听、行为 测听、听性脑干诱发电位或多频稳态诱发电位评估 听力损失情况。有眩晕症状者进行前庭功能的评估。 全部听力损失患者均行颞骨轴位高分辨率扫描。对 大前庭水管综合征患者进行随诊.反复检查其听力。 1.1.2大前庭水管综合征的诊断标准
2 Department ofOtorhinolaryngology Head and Neck Surgery,Second Hospital ofLanzhou University, Lanzhou 730030,China
【Abstract】Objective To analysis the SLC26A4 mutations and their origins of patients associated with large vestibu— lar aqueduct syndrome in 6 nuclear families.Methods A total of 1 2 patients associated with large vestibular aqueduct
detected in the present study,including 3 novel mutations(G209E、E303Q and 1746delG)and 3 reposed mutations.
Genotypes of patients in family 389,1332,1440 and 1748 were G209E/G209E,IVS7—2>G/IVS7-2>G,IVS7—2>G/
颞骨高分辨率轴位CT示:从半规管总脚到前 庭水管外口的1/2处直径大于1.5 mm,即诊断为
LVAS[1I。
1.1.3 听力损失程度的分级标准 本研究中听力损失程度的分级是根据2003年
Van camp等㈣欧洲工作组倡导的遗传性耳聋的分 级标准来诊断的:轻度(20—40 dB HL)、中度 (41—70 dB HL)、重度(71—95 dB HL)及极重度(> 95 dB HL)。 1.2 实验方法 1.2.1基因组DNA提取
万方数据
பைடு நூலகம்
中华耳科学杂志2006年第4卷第4期
·323·
his parents.In family 673,the proband’s genotype were IVS7-2>G/H723R and the genotype of her father associated with large vestibular aqueduct syndrome was IVS7—2>G/IVS7—2>G.Her mother with a normal inner ear was the earrier of H723R.In the family 70 1.the genotypes of the proband and his mother with LVAS were IVS7—2>G/N392Y and IVS7—2> G/IVS7—2>G.respectively.His father was a carrier of N392Y.Conclusion In this study,6 SLC26A 4 mutations were detected.A1l patients in each family have two mutant alleles.We have identified the SLc26A 4 mutation types in these families and the characteristics of inheritance.These results may help to decrease the biah rate of patients associated with large vestibular aqueduct syndrome.
·322·
Chinese Journal of Otology V01.4,No.4,2006
·大前庭水管综合征·
大前庭水管综合征家系SLC26A4基因突变分析
赵亚丽, 王秋菊, 兰兰1 袁虎1 关静。徐百成2纵亮1 1 解放军总医院耳鼻咽喉一头颈外科,解放军耳鼻咽喉科研究所(北京 2兰州大学第二医院耳鼻咽喉一头颈外科(兰州 730030)
基金项目:本研究由国家自然科学基金面上项目(No.30370782&30470956),北京市重大科技项目课题(No.H020220020610),全国优 秀博士学位论文作者专项资金资助项目(No.200463),军队”十一五”杰出人才项目(No.06J018)联合资助。
作者简介:赵亚丽(1980一),女,河北人,医学硕士。专业方向:遗传性聋的分子流行病学和分子遗传机制研究。 通讯作者:王秋菊。Email:wqcr@263.net
1材料与方法
1.1 临床资料 1.1.1 临床资料的收集
所有家系资料均来自中国人民解放军耳鼻咽喉
研究所聋病资源库,对于该项目的伦理论证由解放 军总医院伦理委员会认可。本研究共收集6个大前 庭水管综合征核心家系(仅包括父母和其子女的家 系),分别命名为家系389、701、673、1332、1440 和1748,每个家系包括两名大前庭水管综合征患 者。12名大前庭水管综合征患者包括男性7名,女 性5名,年龄从0.3岁到32岁。选取84名听力正 常且无听力障碍家族史者作为正常对照。
Investigation of SLC26.44 mutations in families associated with large vestibular aqueduct syndrome
ZHA 0 Ya—lii,WANG Qiu-jul,LAN Lanl,YUAN HuI,GUAN靠n营,XU Bai-chen季,ZONG Lianf,ZHAI Suo—qianf 1 Department of Otorhinolaryngology—Heod and Neck Surgery,Chinese PLA General Hospital; Chinese咒A Institute of Otolaryngology,Bering 100853.China
翟所强 100853)
【摘要】目的通过对6个大前庭水管综合征(1arge vestibular aqueduct syndrome,LVAS)家系SLC26A4基因突 变的分析.明确家系中大前庭水管综合征患者5Lc26A4的突变类型和突变形式,探讨其突变来源和传递规律。方