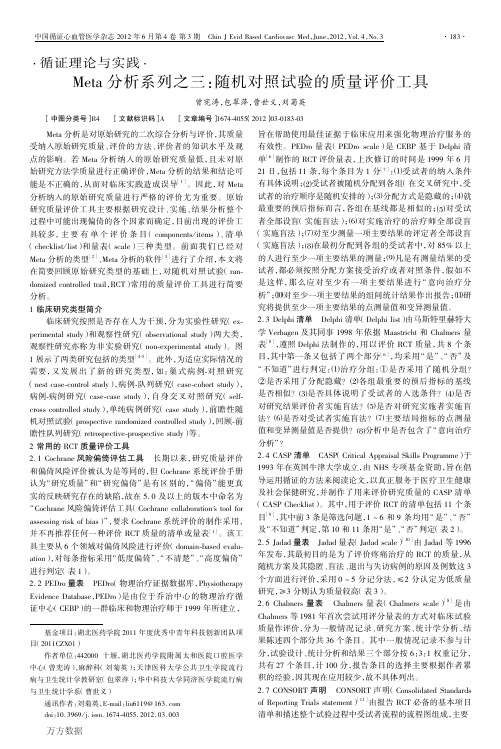
The Cochrane Collaboration’s tool for assessing risk
cochrane评分表

Risk of biasItem Authors'judgementDescriptionAdequate sequence generation? Yes Prinicipal authorstated thatcomputergeneratedallocation wasusedAllocation concealment? Yes Prinicipal authorstated thatallocation wasconcealedBlinding? Unclear No mention ofstudy personnel orparticipantsbeing blind totreatment groupIncompleteoutcome dataaddressed? Yes All participants accounted for, one 'drop out'recorded butincluded by us in analysisFree of other bias? Unclear Possible unevendistribution ofcomplete andincompleteparalysis at startof study betweenthe two treatmentgroupsQuality assessmentThe quality of the trials was assessed and graded independently by two authors according to the criteria described in The Cochrane Handbook 4.2.6 (Higgins 2006). Gradings were compared and any inconsistencies between the authors in the interpretation of inclusion criteria and their significance to the selected study were discussed and resolved.The selected study was assessed for the following characteristics:1. The adequacy of the randomisation process (possible selection bias). Adequate randomisation includes any one of the following methods: computer generated or table of random numbers, drawing of lots, coin-toss, shuffling cards or throw of a dice. Inadequate methods of randomisation include the following: case record number, date of birth or alternate numbers.2. The adequacy of the allocation concealment (possible selection bias). Adequate methods of allocation concealment include either central randomisation (i.e. separate to other aspects of trial administration) or sequentially numbered sealed opaque envelopes. Inadequate concealment means an open allocation sequence in which either participants or trialists were able to foresee the upcoming assignment.3. The blinding of outcome assessors (i.e. whether the persons assessing the outcome of care were aware of which treatment the participant had received - possible performance bias).4. The extent and handling of losses to follow up (possible attrition bias). Adequate handling of losses to follow up involves a clear description and explanation being given of any significant difference between the losses of the intervention groups. An unacceptable loss in any one intervention group was considered to be loss greater than 20%.Study gradings A, B or C were employed for overall quality as follows.A: Minimisation of bias in all four categories above: i.e. adequate randomisation, few losses to follow up and intention-to-treat analysis, blinding of outcome assessors, high quality outcome assessment;B: Each of the criteria in A partially met;C: One or more of the criteria in A not met.Risk of bias in included studiesWe classified this study as grade C because of the uncertainty about blinding. The possibility of anuneven distribution of complete and incomplete palsies between the two groups is another potential source of bias and we conclude overall that this is a low quality study.Table 8.5.a: The Cochrane Collaboration’s tool for assessing risk of biasTable 8.5.c: Criteria for judging risk of bias in the ‘Risk of bias’ assessment toolFig ure 8.6.a: Example of a ‘Risk of bias’ table for a single study (fictional)Table 8.7.a: Possible approach for summary assessments of the risk of bias for each important outcome (across domains) within and across studies。
Meta分析系列之三-随机对照试验的质量评价工具
·循证理论与实践·Meta分析系列之三:随机对照试验的质量评价工具曾宪涛,包翠萍,曹世义,刘菊英 [中图分类号]R4 [文献标识码]A [文章编号]1674⁃4055(2012)03⁃0183⁃03 Meta分析是对原始研究的二次综合分析与评价,其质量受纳入原始研究质量、评价的方法、评价者的知识水平及观点的影响。
若Meta分析纳入的原始研究质量低,且未对原始研究方法学质量进行正确评价,Meta分析的结果和结论可能是不正确的,从而对临床实践造成误导[1]。
因此,对Meta 分析纳入的原始研究质量进行严格的评价尤为重要。
原始研究质量评价工具主要根据研究设计、实施、结果分析整个过程中可能出现偏倚的各个因素而确定,目前出现的评价工具较多,主要有单个评价条目(components/items)、清单(checklist/list)和量表(scale)三种类型。
前面我们已经对Meta分析的类型[2]、Meta分析的软件[3]进行了介绍,本文将在简要回顾原始研究类型的基础上,对随机对照试验(ran⁃domized controlled trail,RCT)常用的质量评价工具进行简要分析。
1临床研究类型简介 临床研究按照是否存在人为干预,分为实验性研究(ex⁃perimental study)和观察性研究(observational study)两大类,观察性研究亦称为非实验研究(non⁃experimental study)。
图1展示了两类研究包括的类型[4⁃5]。
此外,为适应实际情况的需要,又发展出了新的研究类型,如:巢式病例⁃对照研究(nest case⁃control study),病例⁃队列研究(case⁃cohort study),病例⁃病例研究(case⁃case study),自身交叉对照研究(self⁃cross controlled study),单纯病例研究(case study),前瞻性随机对照试验(prospective randomized controlled study),回顾⁃前瞻性队列研究(retrospective⁃prospective study)等。
meta分析教程

meta分析教程Step 1: Formulate your research questionBefore conducting a meta-analysis, it is crucial to clearly define your research question or objective. This will help guide your search for relevant studies and determine the criteria for including or excluding studies from your analysis.The next step is to perform an extensive literature search to identify all relevant studies on your research question. This can be done by searching electronic databases, such as PubMed or Google Scholar, using specific keywords and inclusion/exclusion criteria. Additionally, it may be helpful to review the reference lists of selected articles to find additional studies that were missed during the initial search.Step 3: Screen and select studiesStep 4: Extract data from selected studiesStep 5: Assess study quality and risk of biasTo evaluate the quality and risk of bias of the included studies, a critical appraisal should be conducted. This involves assessing factors such as study design, sample size, blinding, randomization, and potential sources of bias. Various tools and checklists, such as the Cochrane Collaboration's Risk of Bias Tool, can be used to systematically assess the quality of individual studies.Step 6: Analyze the dataStep 7: Assess heterogeneityHeterogeneity refers to the variability in effect sizes across studies. It is important to assess and quantify heterogeneity using statistical tests, such as the Q test or I² statistic. If significant heterogeneity is present, subgroup analyses or sensitivity analyses may be conducted to explore potential sources of heterogeneity.Step 8: Publication bias assessmentPublication bias occurs when studies with statistically significant results are more likely to be published, while studies with nonsignificant or negative findings remain unpublished. To assess publication bias, funnel plots can be used to visually examine the symmetry of the distribution of effect sizes. Statistical tests, such as Egger's regression or Begg's rank correlation, can also be applied to quantify the degree of asymmetry.Step 9: Interpret and report the findingsFinally, the results of the meta-analysis should be interpreted and reported in a clear and concise manner. The findings should be discussed in light of the research question, the characteristics of the included studies, and the limitationsof the analysis. Conclusions should be drawn based on the strength of evidence provided by the meta-analysis.。
20世纪口腔医学文献 英文

20世纪口腔医学文献英文Oral healthcare has witnessed remarkable advancements in the20th century. The rapid progress in the field of dentistry is evident from the multitude of scholarly literature that emerged during this era. These publications not only helped to disseminate knowledge but also played a pivotal role in shaping the modern landscape of oral medicine. This article aims to provide a brief overview of some influential and seminal works from the 20th-century dental literature.One of the most significant contributions to the field of oral medicine in the 20th century was the discovery of fluoride's role in dental caries prevention. The groundbreaking research by Dr. H. Trendley Dean and his colleagues in the 1930s established the efficacy of water fluoridation in reducing tooth decay. Their studies demonstrated the importance of fluoride in the remineralization process, which helped revolutionize oral healthcare practices worldwide.Another notable advancement in oral medicine during the 20th century was the development of dental implants. Dr. Per-IngvarBrånemark's research and clinical work on osseointegration led to the introduction of modern implantology. His studies demonstrated the successful integration of titanium implants with surrounding bone, providing a breakthrough in the treatment of edentulism and significantly impacting the field of prosthodontics.The introduction of adhesive dentistry, also known as bonding, was another pivotal moment in dental history. The work of Dr. Michael Buonocore in the 1950s laid the foundation for theapplication of adhesive materials to enamel and dentin surfaces. This technique enabled the preservation of tooth structure, avoiding the need for invasive restorative procedures, and revolutionized the field of conservative dentistry.Oral and maxillofacial surgery witnessed significant advancements during the 20th century. Prof. William H. Bell's comprehensive textbook, "Oral and Maxillofacial Surgery" published in the 1970s, became a staple for both undergraduate and postgraduate dentistry education. This manuscript covered a wide range of topics, including diagnosis, surgical techniques, and management of various oral and facial conditions. It provided a solid foundation for oral surgeons and contributed to the progress of this specialized branch of dentistry.The introduction of cone beam computed tomography (CBCT) imaging was another significant milestone in oral medicine. This three-dimensional imaging technique allowed for precise diagnosis and treatment planning in the fields of oral and maxillofacial radiology, orthodontics, and implantology. Dr. Dale A. Miles' publication, "Cone Beam Imaging: The State of the Art," published in the early 2000s, provided a comprehensive overview of CBCT technology and its various applications in dentistry.Last but not least, the emergence of evidence-based dentistry greatly impacted clinical decision-making in the 20th century. The Cochrane Collaboration, a global network of researchers, contributed immensely to the field by conducting systematic reviews and meta-analyses of dental interventions. Their publications, such as "The Cochrane Database of SystematicReviews," provided robust evidence to guide dental professionals in delivering effective and evidence-based care to their patients. In conclusion, the 20th-century dental literature witnessed significant advancements in oral healthcare. The discovery of fluoride's role in dental caries prevention, the development of dental implants, the advent of adhesive dentistry, the standardization of oral and maxillofacial surgery, the introduction of cone beam computed tomography imaging, and the influence of evidence-based dentistry were some of the key contributions that shaped modern oral medicine. These seminal works continue to serve as a foundation for dental professionals, helping them achieve better patient outcomes and pave the way for future advancements in the field.。
低强度他汀加其他降脂药在降低LDL-C效果上可以与高强度他汀相媲美,但长期获益仍不确定
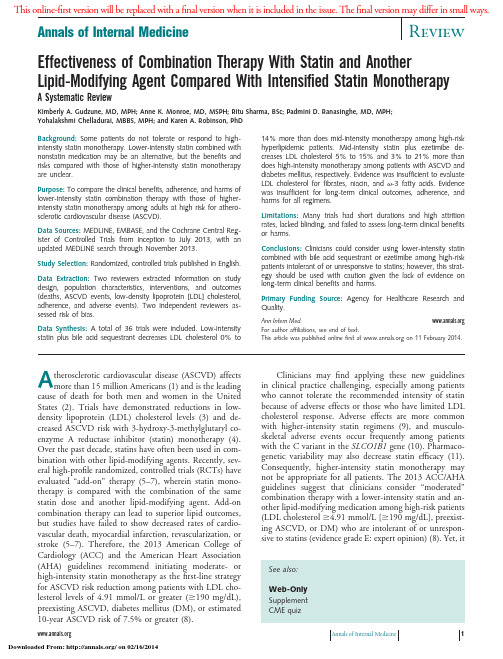
Effectiveness of Combination Therapy With Statin and Another Lipid-Modifying Agent Compared With Intensified Statin Monotherapy A Systematic ReviewKimberly A.Gudzune,MD,MPH;Anne K.Monroe,MD,MSPH;Ritu Sharma,BSc;Padmini D.Ranasinghe,MD,MPH;Yohalakshmi Chelladurai,MBBS,MPH;and Karen A.Robinson,PhDBackground:Some patients do not tolerate or respond to high-intensity statin monotherapy.Lower-intensity statin combined with nonstatin medication may be an alternative,but the benefits and risks compared with those of higher-intensity statin monotherapy are unclear.Purpose:To compare the clinical benefits,adherence,and harms of lower-intensity statin combination therapy with those of higher-intensity statin monotherapy among adults at high risk for athero-sclerotic cardiovascular disease(ASCVD).Data Sources:MEDLINE,EMBASE,and the Cochrane Central Reg-ister of Controlled Trials from inception to July2013,with an updated MEDLINE search through November2013.Study Selection:Randomized,controlled trials published in English.Data Extraction:Two reviewers extracted information on study design,population characteristics,interventions,and outcomes (deaths,ASCVD events,low-density lipoprotein[LDL]cholesterol, adherence,and adverse events).Two independent reviewers as-sessed risk of bias.Data Synthesis:A total of36trials were included.Low-intensity statin plus bile acid sequestrant decreases LDL cholesterol0%to 14%more than does mid-intensity monotherapy among high-risk hyperlipidemic patients.Mid-intensity statin plus ezetimibe de-creases LDL cholesterol5%to15%and3%to21%more than does high-intensity monotherapy among patients with ASCVD and diabetes mellitus,respectively.Evidence was insufficient to evaluate LDL cholesterol for fibrates,niacin,and-3fatty acids.Evidence was insufficient for long-term clinical outcomes,adherence,and harms for all regimens.Limitations:Many trials had short durations and high attrition rates,lacked blinding,and failed to assess long-term clinical benefits or harms.Conclusions:Clinicians could consider using lower-intensity statin combined with bile acid sequestrant or ezetimibe among high-risk patients intolerant of or unresponsive to statins;however,this strat-egy should be used with caution given the lack of evidence on long-term clinical benefits and harms.Primary Funding Source:Agency for Healthcare Research and Quality.Ann Intern For author affiliations,see end of text.This article was published online first at on11February2014.A therosclerotic cardiovascular disease(ASCVD)affectsmore than15million Americans(1)and is the leading cause of death for both men and women in the United States(2).Trials have demonstrated reductions in low-density lipoprotein(LDL)cholesterol levels(3)and de-creased ASCVD risk with3-hydroxy-3-methylglutaryl co-enzyme A reductase inhibitor(statin)monotherapy(4). Over the past decade,statins have often been used in com-bination with other lipid-modifying agents.Recently,sev-eral high-profile randomized,controlled trials(RCTs)have evaluated“add-on”therapy(5–7),wherein statin mono-therapy is compared with the combination of the same statin dose and another lipid-modifying agent.Add-on combination therapy can lead to superior lipid outcomes, but studies have failed to show decreased rates of cardio-vascular death,myocardial infarction,revascularization,or stroke(5–7).Therefore,the2013American College of Cardiology(ACC)and the American Heart Association (AHA)guidelines recommend initiating moderate-or high-intensity statin monotherapy as thefirst-line strategy for ASCVD risk reduction among patients with LDL cho-lesterol levels of4.91mmol/L or greater(Ն190mg/dL), preexisting ASCVD,diabetes mellitus(DM),or estimated 10-year ASCVD risk of7.5%or greater(8).Clinicians mayfind applying these new guidelines in clinical practice challenging,especially among patients who cannot tolerate the recommended intensity of statin because of adverse effects or those who have limited LDL cholesterol response.Adverse effects are more common with higher-intensity statin regimens(9),and musculo-skeletal adverse events occur frequently among patients with the C variant in the SLCO1B1gene(10).Pharmaco-genetic variability may also decrease statin efficacy(11). Consequently,higher-intensity statin monotherapy may not be appropriate for all patients.The2013ACC/AHA guidelines suggest that clinicians consider“moderated”combination therapy with a lower-intensity statin and an-other lipid-modifying medication among high-risk patients (LDL cholesterolՆ4.91mmol/L[Ն190mg/dL],preexist-ing ASCVD,or DM)who are intolerant of or unrespon-sive to statins(evidence grade E:expert opinion)(8).Yet,it See also:Web-OnlySupplementCME quizAnnals of Internal Medicine Review Annals of Internal Medicine1is unclear whether this strategy results in similar ASCVD risk reductions and fewer adverse effects compared with higher-intensity statin monotherapy.A2009systematic re-view that examined these questions found insufficient evi-dence to weigh benefits and risks of moderated combina-tion therapy(12).We aimed to compare the effectiveness,safety,and tolerability of moderated combination therapy of statin with another lipid-modifying medication(bile acid seques-trant,ezetimibe,fibrate,niacin,or-3fatty acid)with those of higher-intensity statin monotherapy among high-risk patients.We sought to compare the long-term clinical benefits and short-term lipid effects of moderated combi-nation therapy with those of higher-intensity statin mono-therapy,as well as to determine whether these regimens differ in rates of adherence and harms.M ETHODSWe developed and publicly posted a protocol to con-duct this review(/index .cfm/search-for-guides-reviews-and-reports/?pageaction ϭdisplayproduct&productidϭ1496and the search strate-gies and detailed evidence tables are available online(13). Given the recent release of the2013ACC/AHA guidelines (8),we narrowed the scope of this manuscript to focus on evidence most relevant to high-risk populations for whom combination therapy might be considered.Data Sources and SearchesWe searched the following databases for primary studies published from May2008through July2013: MEDLINE,EMBASE,and the Cochrane Central Register of Controlled Trials.To update our review,we searched MEDLINE through November2013.We screened all ar-ticles included in the prior review(12).We also reviewed the reference lists of each included article,relevant review articles,relevant studies identified on , and scientific information packets provided by pharmaceu-tical manufacturers.Study SelectionTwo study team members independently screened each identified article against prespecified eligibility criteria (Table1of the Supplement,available at ). We included RCTs in adults with high ASCVD risk(LDL cholesterol levelՆ4.91mmol/L[Ն190mg/dL],preexist-ing ASCVD,or DM)(8)that compared a moderated com-bination regimen with higher-intensity statin mono-therapy.We excluded studies not reported in English.We also considered nonrandomized extensions of clinical trials more than24weeks’duration and U.S.Food and Drug Administration reports for evaluation of long-term bene-fits,serious adverse events,and harms.We anticipated that few trials of only statin-intolerant or statin-unresponsive patients would exist and therefore included studies of statin-tolerant and statin-responsive patients.Data Extraction and Quality AssessmentTwo team members extracted data on study design, setting,population characteristics,and intervention charac-teristics.Our long-term clinical outcomes included mortal-ity,acute coronary events,cerebrovascular events,and re-vascularization procedures.Our lipid outcome was LDL cholesterol.Investigator-defined outcomes included adher-ence,serious adverse events,withdrawals due to adverse events,and occurrence of any adverse event.Secondary harms outcomes included elevations in liver aminotrans-ferase levels,elevated measures of muscle-related harm(for example,elevated creatinine phosphokinase or myalgia), acute kidney injury,or incident DM.We rated the strength of evidence(SOE)by evaluating the risk of bias,consistency of results,directness,and pre-cision.We assessed risk of bias using the Cochrane Collab-oration’s tool(14)for studies identified in the new search and the Jadad score(15)for studies identified during the prior review.Two reviewers independently assessed the risk of bias for each included study.We labeled results as con-sistent if most of the interventions’point estimates favored statin monotherapy or combination therapy.Most out-comes were directly measured,except for LDL cholesterol. We considered the outcome of calculated LDL cholesterol to be indirect because the Friedewald equation may under-estimate LDL cholesterol among high-risk patients(16). We assessed precision on the basis of the studies’variance estimates and sufficiency of the sample size by comparing them to the optimal information size.To be rated as high SOE,the body of evidence would need to be rated as having low risk of bias and as being consistent,direct,and precise.We rated the SOE as moderate if1of these ele-ments was downgraded.We rated the SOE as low if2or more of these elements were downgraded.Data Synthesis and AnalysisThe evidence base contained different statins and dif-ferent statin doses both within and across studies,which limited our ability to make statin-specific comparisons. Prior studies have suggested schemes to group statins on the basis of their reported LDL cholesterol reduction(17, 18),which are similar to the strategy used by the ACC/ AHA committee(8).We used the strategy proposed by Weng and colleagues(18)to group statins when synthesiz-ing data(Table2of the Supplement).We compared mod-erated combination therapy with higher-intensity statin monotherapy among high-risk patients with LDL choles-terol levels of4.91mmol/L or greater(Ն190mg/dL),pre-existing ASCVD,or DM.For all comparisons,we report the qualitative synthesis of data by calculating and displaying the individual mean differences with95%CIs(if calculable)for individual studies grouped by combination therapy agent,statin in-tensity,and high-risk population.For studies with2 monotherapy arms of the same intensity,we used only1 arm as the comparator to the combination arms accordingReview Effectiveness of Combination Therapy With Statin2Annals of Internal Medicine to a priori criteria:1)If the arms involved the same statin,we used the arm with the higher dose,and 2)if the arms involved different statins,we selected the arm according to prioritized statin agent (rosuvastatin,atorvastatin,simva-statin,lovastatin,pravastatin,and fluvastatin;no studies used pitavastatin).We performed no meta-analyses given the small number of heterogeneous trials.Role of the Funding SourceFunding was provided by the Agency for Healthcare Research and Quality.The funding source had no role in study selection,quality assessment,or data synthesis or in the decision to submit the manuscript for publication.R ESULTSThe Appendix Figure summarizes the search results,and Table 3of the Supplement lists all included studies.The literature search identified 4369unique citations.We included 36studies,reported in 43articles.The Table summarizes the study and population characteristics of in-cluded studies by combination agent and by population.All trials were RCTs.No nonrandomized extensions ofclinical trials greater than 24weeks’duration and Food and Drug Administration reports met our inclusion criteria.Most study populations included men in their 50s to 60s.Long-term Clinical OutcomesWe found insufficient evidence to compare long-term clinical outcomes (mortality,acute coronary events,cere-brovascular events,and revascularization procedures)for all combination therapy and statin intensity comparisons.Fig-ure 1presents an evidence map of studies that evaluated these outcomes (19–27).Most studies that reported events lasted less than 20weeks;event rates were very low or no events occurred.LDL Cholesterol,Treatment Adherence,and Harms OutcomesCombination Therapy With Bile Acid Sequestrants by Intensity ComparisonFigure 2shows the differences in change in LDL cho-lesterol among high-risk groups by nonstatin agent (28–61).Five RCTs compared statin monotherapy to combi-nation therapy with bile acid sequestrant (371participants)Statin Monotherapy PotencyCombination Therapy PotencyRCTs by Population,n (N eligible)Range of StudyDuration,wk Overall Baseline Population Characteristics Risk of BiasRCTs That ReceivedPharmaceutical Company Support,%Mean Age Range,yRange of Women,%Range of White Patients,%Mean LDL Cholesterol Range,mg/dL *Bile acid sequestrants High-intensity Low-intensity 0High-intensity Mid-intensity 1HLD (83)1251–5314–38NR 218–224Low100Mid-intensity Low-intensity 4HLD (288)6–2452–6129–42†95–98†180–236Moderate 100EzetimibeHigh-intensityLow-intensity1HLD (23)4NR NR NR 200–206Moderate 01CVD (112)65643–46NR 126–128Low 1001DM (21)856–6555–60NR 145–147Low 100High-intensity Mid-intensity1HLD (145)857–5947–4884–87198–202Low 10012CVD (2590)4–1259–72†17–51†73–93†84–151†Low 5011DM (Ͼ3448)6–2458–66†38–56†0–96†91–147†Low100Mid-intensity Low-intensity1DM (24)1064–6550–58NR 154–164Moderate NRFibratesHigh-intensity Low-intensity 1HLD (396)5250–5227–33NR 203–208Low NR High-intensity Mid-intensity 1HLD (389)5250–5226–30NR 196–203Low NR 1CVD (102)1356–584–20NR 92–102High NR Mid-intensity Low-intensity 1DM (291)1256–5749–55NR 127–128Low 100NiacinHigh-intensity Low-intensity 0High-intensity Mid-intensity 1HLD (315)1652–5425–3184–89189–196Low100Mid-intensityLow-intensity 2HLD (219)20–2858–6136–5074–88186–200Moderate 100-3fatty acids High-intensity Low-intensity 0CVD ϭsubgroup with preexisting atherosclerotic cardiovascular disease;DM ϭsubgroup with diabetes mellitus;HLD ϭsubgroup with low-density lipoprotein cholesterol level Ն190mg/dL (Ն4.91mmol/L);LDL ϭlow-density lipoprotein;NR ϭnot reported;RCT ϭrandomized,controlled trial.*Wide range of LDL cholesterol values may be reported because some studies evaluated baseline LDL cholesterol while participants were receiving lipid-modifying therapy.LDL cholesterol values can be converted from traditional units to SI units by multiplying the value in mg/dL by 0.026to calculate the value in mmol/L.†Only a subset of trials reported this characteristic,so range reflects that of those studies reporting.ReviewEffectiveness of Combination Therapy With StatinAnnals of Internal Medicine3among hyperlipidemic patients (28–33).We identified no studies that reported results within the ASCVD and DM groups.Four trials compared low-intensity statin in combina-tion with bile acid sequestrants to mid-intensity statin monotherapy (288participants)(29–33).Low-intensity statin in combination with bile acid sequestrant decreases LDL cholesterol 0%to 14%more than did mid-intensity statin monotherapy (SOE:moderate).One study reported adherence,which was 97%among monotherapy recipients and 93%to 95%among combination therapy recipients (33).One study reported on withdrawals due to adverse events at 6weeks,which did not statistically significantly differ between groups (0participants receiving mono-therapy;3%of participants receiving combination therapy;P ϭ0.28)(29).Evidence was insufficient to evaluate LDL cholesterol outcomes for other intensity comparisons and to compare adherence and harms,regardless of statin intensity.Combination Therapy With Ezetimibe by Intensity ComparisonTwo RCTs compared statin monotherapy and combi-nation therapy with ezetimibe (168participants)among hyperlipidemic patients (34,36).We identified 12RCTs and 1RCT subgroup analysis among patients with preex-isting ASCVD (2702participants).We identified 9RCTsand 4RCT subgroups analyses among patients with DM (Ͼ3493participants).Results of all trials are displayed in Figure 2.There was insufficient evidence to evaluate LDL cholesterol,adherence,and harms for other intensity com-parisons among patient groups other than those reported below.Eleven RCTs and 1RCT subgroup analysis compared mid-intensity statin combined with ezetimibe to high-intensity statin monotherapy (2590participants)among patients with preexisting ASCVD (19–21,38–48).Mid-intensity statin combined with ezetimibe decreases LDL cholesterol 5%to 15%more than does high-intensity sta-tin monotherapy (SOE:moderate).Two trials reported ad-herence,which was greater than 95%in all groups (38,40).Three studies reported serious adverse events,which were similar between groups (0%to 2%of monotherapy recipients;0%to 2%of combination therapy recipients)(19,38,39),and 5reported withdrawals due to adverse events,which occurred among more monotherapy recipi-ents (difference,1%to 18%)(19,20,38,39,43,44).Secondary harms,including elevated liver aminotransferase levels and muscle-related events,when reported,occurred infrequently (Table 4of the Supplement ).Seven RCTs and 4RCT subgroup analyses compared mid-intensity statin combined with ezetimibe to high-intensity statin monotherapy (Ͼ3448participants)among patients with DM (22–25,38,39,47–56).Mid-intensity statin combined with ezetimibe decreases LDL cholesterol 3%to 21%more than does high-intensity statin mono-therapy (SOE:moderate).One trial reported treatment ad-herence as high in both groups (99%and 98%for mono-therapy and combination therapy,respectively)(22).Five studies reported on serious adverse events,which were sim-ilar between groups (0%to 3%of monotherapy recipients;0%to 5%of combination therapy recipients)(22–25,38,54,56).Four reported on withdrawals due to adverse events,which occurred in 1%to 5%of monotherapy re-cipients and 2%to 4%of combination therapy recipients (22–25,38,56).Secondary harms,including elevated liver aminotransferase levels and muscle-related events,when reported,occurred infrequently (Table 4of the Supplement ).Combination Therapy With Fibrate by Intensity ComparisonWe identified 1RCT in each high-risk population (hyperlipidemia,654participants;ASCVD,102partici-pants;DM,291participants)(Figure 2)(26,58,59).We found insufficient evidence to compare LDL cholesterol,adherence,and harms regardless of statin intensity and population.Secondary harms,when reported,occurred in-frequently (Table 4of the Supplement ).Combination Therapy With Niacin by Intensity ComparisonThree RCTs (534participants)were identified among hyperlipidemic patients (Figure 2)(27,60,61).We iden-S t u d y D u r a t i o n , w kt imibe : Dea t hs t es : Dea t hs : Dea t hsEze t imibe : ACS Fibra t es : ACSt imibe : CVA Fibra t es : CVAThe figure includes the clinical outcomes of deaths (green ),ACS (black ),and CVA (white ).No studies reported on revascularization procedures.The different combination therapy agents are represented by the differ-ent symbols (diamond ϭezetimibe [27,34,38,43,51];circle ϭfibrates [58];square ϭniacin [60]).No trials with bile acid sequestrants or -3fatty acids reported on any clinical outcomes.Each marker represents a different trial,where the sample size is represented by the size of the marker and the y -axis reflects the study duration.Differences in popula-tions,potency comparisons,or event rates are not represented.Most event rates were very low or no events occurred,which limited our ability to make any inferences.ACS ϭacute coronary syndrome;CVA ϭcere-brovascular event.ReviewEffectiveness of Combination Therapy With Statin4Annals of Internal MedicineS t u d y, Year (Reference)M ean M ono t herapyBaseline LDL Choles t erol Level,mg/dLM ean Combina t ion Therapy Baseline LDL Choles t erol Level, mg/dLPopula t ionTime Poin t , wkBile aci d seques t ran t sHi g h-in t ensi t y s t a t in mono t herapy vs. mi d -in t ensi t y s t a t in combinaJohansson, 1995 (28)Johansson, 1995 (28)M i d -in t ensi t y s t a t in mono t herapy vs. low-in t ensi t y s t a t in combina t Knapp e t al, 2001 (29)Ismail e t al, 1990* (30, 31)P M SG II e t al, 1993 (32)Schro tt e t al, 1995 (33)Schro tt e t al, 1995 (33)Eze t imibeHi g h-in t ensi t y s t a t in mono t herapy vs. low-in t ensi t y combina t ion t Araujo e t al, 2010 (34)Ru d ofsky e t al, 2012 (35)Hi g h-in t ensi t y s t a t in mono t herapy vs. mi d -in t ensi t y s t a t in combina M cKenney e t al, 2007 (36)Piorkowski e t al, 2007 (37)Averna e t al, 2010 (19)Bar d ini e t al, 2010 (38)Barrios e t al, 2005 (39)Cho e t al, 2011 (40)Pesaro e t al, 2011* (41, 42)Os t a d e t al, 2009 (20)Ham d an e t al, 2011 (43)M a t sue e t al, 2013 (44)Oka d a e t al, 2011 (45)Yamazaki e t al, 2013 (46)Zieve e t al, 2010* (47, 48)Bar d ini e t al, 2010 (38)Barrios e t al, 2005 (39)Bays e t al, 2013 (49)Cons t ance e t al, 2007 (22)Gol d ber g e t al, 2006* (50–52)Rosen e t al, 2013* (23–25)Foo d y e t al, 2010 (53)Lee e t al, 2013 (54)Torimo t o e t al, 2013 (55)Zieve e t al, 2010* (47, 48)Gau d iani e t al, 2005 (56)M i d -in t ensi t y s t a t in mono t herapy vs. low-in t ensi t y s t a t in combina t Kawa g oe e t al, 2011 (57)Fibra t esHi g h-in t ensi t y s t a t in mono t herapy vs. low-in t ensi t y s t a t in combina A t hyros e t al, 2002 (58)A t hyros e t al, 2002 (58)Hi g h-in t ensi t y s t a t in mono t herapy vs. mi d -in t ensi t y s t a t in combina A t hyros e t al, 2002 (58)A t hyros e t al, 2002 (58)Shah e t al, 2007 (59)Shah e t al, 2007 (59)M i d -in t ensi t y s t a t in mono t herapy vs. low-in t ensi t y s t a t in combina t Farnier e t al, 2011 (26)NiacinHi g h-in t ensi t y s t a t in mono t herapy vs. mi d -in t ensi t y s t a t in combina Bays e t al, 2003 (60)Bays e t al, 2003 (60)M i d -in t ensi t y s t a t in mono t herapy vs. low-in t ensi t y s t a t in combina t Insull e t al, 2004 (61)Insull e t al, 2004 (61)Hunnin g hake e t al, 2003 (27)218224196232236191186201154202140126128124134991511249412184NR 128NR NR 8914599NR 139111NR 9416420820319919692921271901892001911922222221802242361951952061511981351281241241321011481319512089NR 124NR NR 9314697NR 134112NR 92154203203203203102102128196196196196186Favors Combina t ion Therapy Favors S t a t in M ono t herapyHLDHLD HLD HLD HLD HLD HLDHLD D M HLD ASCVD ASCVD ASCVD ASCVD ASCVD ASCVD ASCVD ASCVD ASCVD ASCVD ASCVD ASCVD D M D M D M D M D M D M D M D M D M D M D M D MHLD HLD HLD HLD ASCVD ASCVD D MHLD HLD HLD HLD HLDPa t ien t s, n5554NR NR NR NR NR232114551112NR 4228578NR 7524381NR 891NR NR 495423479629NR 12575216210242642632602604647289NR NR NR NR NR1212688121248846666681212121212666666121212122412525252521313121616202028M ean Be t ween-Group Difference in LDL Choles t erol Level Chan g e %t o –5)t o –9)t o 6)t o –12)t o –10)t o 4)t o 9)t o –3)t o –3)t o –13)t o 0)t o 6)t o –12)t o –15)t o 28)t o 15)t o 13)t o 10)t o 5)ASCVD ϭatherosclerotic cardiovascular disease;DM ϭdiabetes mellitus;HLD ϭsubgroup with low-density lipoprotein cholesterol level 4.91mmol/L or greater (Ն190mg/dL);LDL ϭlow-density lipoprotein;NR ϭnot reported;PMSG ϭPravastatin Multicenter Study Group.*These study results were reported in multiple articles,which are listed in Table 3of the Supplement.LDL cholesterol values can be converted from traditional units to SI units by multiplying the LDL cholesterol value in mg/dL by 0.026to calculate the value in mmol/L.ReviewEffectiveness of Combination Therapy With Statin Annals of Internal Medicine 5tified no studies that reported results within the ASCVD and DM groups.Two trials compared low-intensity statin combined with niacin to mid-intensity statin monotherapy(219par-ticipants)(27,61).We found inconsistent effects on low-ering LDL cholesterol for this comparison(SOE:insuffi-cient).One trial reported on adherence,which was96%in each group(61).One trial reported withdrawals due to adverse events,which did not statistically significantly dif-fer between groups(19%of monotherapy recipients;10% of combination therapy recipients;Pϭ0.06)(27).Sec-ondary harms occurred infrequently(Table4of the Supplement).Combination Therapy With Omega-3Fatty Acidby Intensity ComparisonWe identified no relevant studies with-3fatty acids.D ISCUSSIONPrior National Cholesterol Education Program Adult Treatment Panel III guidelines emphasized achieving cer-tain LDL cholesterol targets(62,63);however,the new ACC/AHA guidelines have departed from this strategy given the lack of evidence supporting this approach(8). These new guidelines recommend prescribing at least a moderate-intensity statin to all patients with moderate or greater ASCVD risk regardless of LDL cholesterol value. Statins may reduce ASCVD by reducing LDL cholesterol and inflammation(64).Although this strategy offers evidence-based risk reduction for many patients,it creates a clinical conundrum for high-risk patients who cannot tolerate higher-intensity statins because of adverse effects or who have limited LDL cholesterol response to statins.Higher-intensity statin regimens have been linked to a statistically significant increased risk for adverse events and discontinuation of therapy due to adverse events(65).Sta-tin users have a50%greater adjusted odds of reporting musculoskeletal pain than nonusers(66),and such symp-toms may lead to medication nonadherence.Individual LDL cholesterol responses to statins vary widely.One study found that4%of patients do not respond,and an-other10%have inadequate LDL cholesterol reduction (67).The ACC/AHA guidelines suggest the addition of a nonstatin lipid-modifying agent to maximally tolerated statin among high-risk statin-intolerant or statin-unresponsive patients(8).This recommendation was based on expert opinion,and the authors did not offer recom-mendations with respect to which nonstatin agent or agents should be used,other than recommending that cli-nicians weigh potential ASCVD risk-reduction benefits against risk for adverse events.Given that statin intolerance and unresponsiveness are relatively common,many clini-cians will probably care for these patients at some point; our review may address,in part,this evidence gap.Our results suggest that moderated statin combination therapy with bile acid sequestrants decreases LDL choles-terol to a similar or greater extent compared with higher-intensity statin monotherapy among patients at high risk for ASCVD.Unfortunately,we could not determine whether the LDL cholesterol benefits of these regimens translate into decreased risk for death,ASCVD events,or revascularization procedures.We suspect that the short du-ration of most trials included in this review contributed to their failure to capture changes in these clinical outcomes, which typically require follow-up over several years.A 7-year RCT of hypercholesterolemic men found that bile acid sequestrant monotherapy conferred a24%reduction in risk for coronary heart disease deaths and a19%reduc-tion in risk for nonfatal MI compared with placebo(68). Few trials included in this review reported on harms or adherence.Prior reviews have found that adverse effects of bile acid sequestrant monotherapy include constipation and bloating;increased plasma triglyceride levels;and de-creased absorption of anionic medications,including stat-ins(68,69).Reported rates of gastrointestinal adverse effects and drug interactions differ by agent,with co-lesevelam typically producing fewer effects(69,70).When considering combination therapy with a lower-intensity statin and bile acid sequestrant,patients may benefit from counseling on separating drug administration to ensure maximal effect of each medication.We also found that the combination of ezetimibe and lower-intensity statin would offer LDL cholesterol–lower-ing benefits similar to or better than those of higher-intensity statin monotherapy among patients at high ASCVD risk,while producing similar rates of short-term adverse events.Previous reviews link ezetimibe use with diarrhea,and the incidence of elevated liver aminotransfer-ase levels may increase with coadministration of ezetimibe and statin(69,70).No trials in this review had statistically significant between-group differences in liver aminotrans-ferase elevations,although event rates were low and all trials lasted24weeks or less.We again could not determine whether the LDL cholesterol benefits of lower-intensity statin and ezetimibe translate into decreased risk for death, ASCVD events,or revascularization procedures,which we suspect is related to the short duration of included trials. Although clinicians could consider combination of lower-intensity statin and ezetimibe to decrease LDL cholesterol among high-risk patients who are statin intolerant or unresponsive,clinicians should counsel patients that this regimen may or may not result in reduced ASCVD risk.We found insufficient evidence regarding LDL choles-terol reduction when comparing moderated combination therapy withfibrates,niacin,or-3fatty acids to higher-intensity statin monotherapy.The role of niacin or-3fatty acids combined with a statin as alternative strategies remains unclear;the niacin trials demonstrated inconsis-tent results for LDL cholesterol,only1reported on long-Review Effectiveness of Combination Therapy With Statin6Annals of Internal Medicine 。
cochrane纳入的RCT文献质量评价(风险偏倚评估工具)中英文对照版
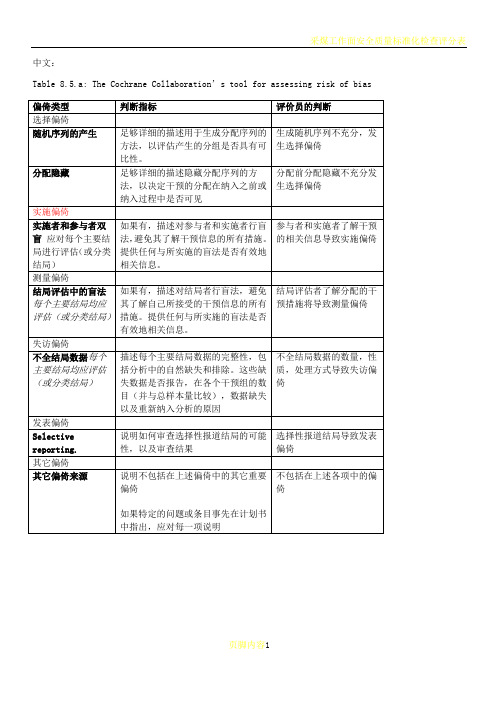
中文:Table 8.5.a: The Cochrane Collaboration’s tool for assessing risk of biasTable 8.5.d: Criteria for judging risk of bias in the ‘Risk of bias’ assessment tool研究者描述随机序列产生过程譬如:参考随机数字表使用计算机随机数字生成器扔硬币洗牌的卡片和信封掷骰子抽签最小化*最小化,可实现无随机元素,被认为相当于是随机的。
研究者描述序列的产生使用的是非随机的方法。
通常是系统的非随机方法,例如:通过奇偶或出生日期产生序列通过入院日期产生序列通过类似住院号或门诊号产生序列相对于上面提到的系统方法,其它非随机的方法少见的多,也更明显。
通常包括对参与者进行判断或非随机的方法,例如:临床医生判断如何分配参与者判断如何分配基于实验室检查或系列测试的结果分配基于干预的可获取性进行分配中心分配(包括电话,网络,药房控制随机)相同外形的顺序编号的药物容器;顺序编号、不透明、密封的信封参与者以及纳入参与者的研究者可能事先知道分配,因而引入选择偏倚,譬如基于如下方法的分配:使用摊开的随机分配表(如随机序列清单)分发信封但没有合适的安全保障(如透明、非密封、非顺序编号)交替或循环出生日期病历号其它明确的非隐藏过程任何如下标准:无盲法或盲法不充分,但系统评价员判断结局不太可能受到缺乏盲法的影响参与者和主要实施者均实施可靠的盲法,且盲法不太可能被打破任何如下标准:无盲法或盲法不充分,但系统评价员判断结局很可能受到缺乏盲法的影响尝试对关键的参与者和实施者行盲法,但盲法很可能被打破,结局很可能受到缺乏盲法的影响任何如下标准:没有足够信息判断为低风险或高风险研究未描述此情况任何如下标准:无盲法或盲法不充分,但系统评价员判断结局不太可能受到缺乏盲法的影响参与者和主要实施者均实施可靠的盲法,且盲法不太可能被打破任何如下标准:无盲法或盲法不充分,但系统评价员判断结局很可能受到缺乏盲法的影响尝试对关键的参与者和实施者行盲法,但盲法很可能被打破,结局很可能受到缺乏盲法的影响任何如下标准:没有足够信息判断为低风险或高风险研究未描述此情况任何如下标准:无缺失数据缺失数据的产生不大可能与真实结局相关(对于生存数据,删失不大可能引入偏倚)缺失数据的数目在各干预组相当,且各组缺失原因类似对二分类变量,与观察事件的发生风险相比,缺失比例不足以影响预估的干预效应对连续性结局数据,缺失数据的合理效应规模(均数差或标准均数差)不会大到影响观察的效应规模;缺失的数据用合适的方法进行估算任何如下标准:缺失数据的产生很大可能与真实结局相关, 缺失数据的数目及缺失原因在各干预组相差较大对二分类变量,与观察事件的发生风险相比,缺失比例足以影响预估的干预效应对连续性结局数据,缺失数据的合理效应规模(均数差或标准均数差)足以影响观察的效应规模;意向治疗分析中存在实际干预措施与随机分配的干预相违背的情况对缺失数据进行简单的不合适的估算任何如下标准:没有报道缺失或排除的情况,无法判断高风险或低风险(如未说明随机的数量,未提供数据缺失的原因)研究未描述此情况任何如下标准:实验的计划书可获取,系统评价感兴趣的所有首要或次要结局均按计划书预先说明的方式报道实验计划书不可得,但很明显发表的报告包括所有的结局,包括预先说明的结局(这种性质的有说服力的文字可能少见)任何如下标准:不是所有的预先说明的首要结局均被报道一个或多个首要结局为采用预先说明的测量方法、分析方法或数据子集来报道系统评价感兴趣的一个或多个首要结局报道不全,以至于不能纳入meta分析研究未报道此研究应当包含的主要关键结局具有与特殊试验设计相关的潜在偏倚来源或被指欺诈或其它问题可能存在偏倚风险,但存在以下两种中的一种没有足够信息评估是否存在其它重要的偏倚风险没有足够的证据认为发现的问题会引入偏倚Table 8.7.a: Possible approach for summary assessments of the risk of bias for each important outcome (across domains) within and across studies英文:Table 8.5.a: The Cochrane Collaboration’s tool for assessing risk of biasTable 8.5.d: Criteria for judging risk of bias in the ‘Risk of bias’ assessment toolprocess such as:Referring to a random number table;Using a computer random number generator;Coin tossing;Shuffling cards or envelopes;Throwing dice;Drawing of lots;Minimization*.*Minimization may be implemented without a random element, and this isconsidered to be equivalent to being random.judgement The investigators describe a non-random component in the sequence generation process. Usually, the description would involve somesystematic, non-random approach, for example:Sequence generated by odd or even date of birth;Sequence generated by some rule based on date (or day) of admission;Sequence generated by some rule based on hospital or clinic recordnumber.Other non-random approaches happen much less frequently than thesystematic approaches mentioned above and tend to be obvious. Theyusually involve judgement or some method of non-random categorization ofparticipants, for example:Allocation by judgement of the clinician;Allocation by preference of the participant;Allocation based on the results of a laboratory test or a seriesof tests;Allocation by availability of the intervention.Criteria for a judgement Participants and investigators enrolling participants could not foreseeassignment because one of the following, or an equivalent method, was usedto conceal allocation:Central allocation (including telephone, web-based andpharmacy-controlled randomization);Sequentially numbered drug containers of identical appearance;Sequentially numbered, opaque, sealed envelopes.judgement Participants or investigators enrolling participants could possiblyforesee assignments and thus introduce selection bias, such as allocationbased on:Using an open random allocation schedule (e.g. a list of randomnumbers);Assignment envelopes were used without appropriate safeguards(e.g. if envelopes were unsealed or nonopaque or not sequentiallynumbered);Alternation or rotation;Date of birth;Case record number;Any other explicitly unconcealed procedure.Criteria for a judgement Any one of the following:No blinding or incomplete blinding, but the review authors judgethat the outcome is not likely to be influenced by lack of blinding;Blinding of participants and key study personnel ensured, andunlikely that the blinding could have been broken.judgementAny one of the following:No blinding or incomplete blinding, and the outcome is likely tobe influenced by lack of blinding;Blinding of key study participants and personnel attempted, butlikely that the blinding could have been broken, and the outcomeis likely to be influenced by lack of blinding.judgement ‘Unclear risk’ ofAny one of the following:Insufficient information to permit judgement of ‘Low risk’ or ‘High risk’;The study did not address this outcome.Criteria for a judgement Any one of the following:No blinding of outcome assessment, but the review authors judge thatthe outcome measurement is not likely to be influenced by lack ofblinding;Blinding of outcome assessment ensured, and unlikely that theblinding could have been broken.judgementAny one of the following:No blinding of outcome assessment, and the outcome measurement islikely to be influenced by lack of blinding;Blinding of outcome assessment, but likely that the blinding couldhave been broken, and the outcome measurement is likely to beinfluenced by lack of blinding.judgement ‘Unclear risk’ ofAny one of the following:Insufficient information to permit judgement of ‘Low risk’ or‘High risk’;The study did not address this outcome.Criteria for a judgement Any one of the following:No missing outcome data;Reasons for missing outcome data unlikely to be related to trueoutcome (for survival data, censoring unlikely to be introducingbias);Missing outcome data balanced in numbers across interventiongroups, with similar reasons for missing data across groups;For dichotomous outcome data, the proportion of missing outcomescompared with observed event risk not enough to have a clinicallyrelevant impact on the intervention effect estimate;For continuous outcome data, plausible effect size (difference inmeans or standardized difference in means) among missing outcomesnot enough to have a clinically relevant impact on observed effectsize;Missing data have been imputed using appropriate methods.judgement Any one of the following:Reason for missing outcome data likely to be related to trueoutcome, with either imbalance in numbers or reasons for missingdata across intervention groups;For dichotomous outcome data, the proportion of missing outcomescompared with observed event risk enough to induce clinicallyrelevant bias in intervention effect estimate;For continuous outcome data, plausible effect size (difference inmeans or standardized difference in means) among missing outcomesenough to induce clinically relevant bias in observed effect size;‘As-treated’ analysis done with substantial departure of theintervention received from that assigned at randomization;Potentially inappropriate application of simple imputation.judgement ‘Unclear risk’ ofAny one of the following:Insufficient reporting of attrition/exclusions to permit judgement of ‘Low risk’ or ‘High risk’ (e.g. number ran domized not stated,no reasons for missing data provided);The study did not address this outcome.Criteria for a judgement Any of the following:The study p rotocol is available and all of the study’spre-specified (primary and secondary) outcomes that are of interestin the review have been reported in the pre-specified way;The study protocol is not available but it is clear that thepublished reports include all expected outcomes, including thosethat were pre-specified (convincing text of this nature may beuncommon).judgementAny one of the following:Not all of the study’s pre -specified primary outcomes have beenreported;One or more primary outcomes is reported using measurements,analysis methods or subsets of the data (e.g. subscales) that werenot pre-specified;One or more reported primary outcomes were not pre-specified(unless clear justification for their reporting is provided, suchas an unexpected adverse effect);One or more outcomes of interest in the review are reportedincompletely so that they cannot be entered in a meta-analysis;The study report fails to include results for a key outcome thatwould be expected to have been reported for such a study.judgementThere is at least one important risk of bias. For example, the study: Had a potential source of bias related to the specific study designused; orHas been claimed to have been fraudulent; orHad some other problem.judgement ‘Unclear risk’ ofThere may be a risk of bias, but there is either:Insufficient information to assess whether an important risk of bias exists; orInsufficient rationale or evidence that an identified problem willintroduce bias.Table 8.7.a: Possible approach for summary assessments of the risk of bias for each important outcome (across domains) within and across studies。
data extraction form - cochrane collaboration:数据提取表格cochr
Timing/frequency
Duration
Setting
Length of follow-up
Were treatment groups comparable at baseline?
YesNoDon’t know
Include study?
No (give reasons for exclusion)
Intervention 1
Intervention 2
Control
2.2Outcome
Time of measurement
Number improved (n (%))
Total number
Mean improvement
SD
Notes/Additional data/Missing data
The Cochrane Collaboration’s tool for assessing risk of bias
Domain
Description
Review authors’ judgement
Sequence generation.
Was the allocation sequence adequately generated?Age (mean Nhomakorabea sd)
Sex (male n (%))
Number of participants entered in trial
severity (mean, sd)orno. of patients with severe, moderate, mild condition: give definitions in footnote
一区sci文章 英文
一区sci文章英文Sure, here is an example of a scientific article in English:Title: "The Effects of Exercise on Cognitive Function in Older Adults: A Systematic Review"Abstract:The aim of this systematic review was to examine the effects of exercise on cognitive function in older adults.A comprehensive search was conducted in electronic databases, and studies published between 2010 and 2020 were included. The methodological quality of the included studies was assessed using the Cochrane Collaboration'stool for assessing risk of bias. A total of 15 studies met the inclusion criteria and were included in the review. The findings suggest that exercise has a positive effect on cognitive function in older adults, particularly in the domains of executive function and memory. However, theeffects of exercise on other cognitive domains, such as attention and processing speed, were less consistent. Further research is needed to determine the optimal type, duration, and intensity of exercise for improving cognitive function in older adults.Introduction:Cognitive decline is a common age-related phenomenon that can significantly impact the quality of life of older adults. Exercise has been proposed as a potential intervention to mitigate cognitive decline and improve cognitive function in this population. While previous studies have investigated the effects of exercise on cognitive function, the results have been inconsistent. Therefore, this systematic review aims to provide a comprehensive synthesis of the current evidence regarding the effects of exercise on cognitive function in older adults.Methods:A systematic search was conducted in electronic databases, including PubMed, Embase, and PsycINFO, using relevant keywords and MeSH terms. Studies published between 2010 and 2020 were included in the review. The inclusion criteria were as follows: (1) participants aged 60 years and older, (2) intervention involving exercise, (3) cognitive function as an outcome measure, and (4) randomized controlled trials or prospective cohort studies. The methodological quality of the included studies was assessed using the Cochrane Collaboration's tool for assessing risk of bias.Results:A total of 15 studies met the inclusion criteria and were included in the review. The majority of the studies were randomized controlled trials (n=12), while the remaining three were prospective cohort studies. The interventions varied in terms of type, duration, and intensity of exercise. The outcome measures used to assess cognitive function also varied across studies, with executive function, memory, attention, and processing speedbeing the most commonly assessed domains. Overall, the findings suggest that exercise has a positive effect on cognitive function in older adults. Specifically, exercise was found to improve executive function and memory in this population. However, the effects of exercise on attention and processing speed were less consistent.Discussion:The results of this systematic review support the notion that exercise can have a beneficial impact on cognitive function in older adults. The improvements observed in executive function and memory are particularly promising. However, the heterogeneity in study designs, interventions, and outcome measures makes it difficult to determine the optimal type, duration, and intensity of exercise for improving cognitive function. Future research should aim to address these limitations and provide more specific recommendations for exercise interventions in older adults.Conclusion:In conclusion, exercise appears to have a positive effect on cognitive function in older adults, particularly in the domains of executive function and memory. However, further research is needed to establish the optimal exercise parameters for maximizing cognitive benefits. These findings have important implications for the development of interventions aimed at promoting healthy aging and preserving cognitive function in older adults.。
Cochrane风险偏倚评估工具
Cochrane 偏倚风险评估工具水天之间2013年11月11日目录随机对照试验/临床对照试验 偏倚的来源偏倚风险评估工具的解读偏倚风险评价结果的总结 偏倚风险评估工具的软件实现 偏倚风险评估工具的实例Cochrane 手册将RCT (randomized controlled tril )和CCT (controlled clinical trial )进行了区分,判定标准为:1.在1个或多个患者中进行的一种研究;2.比较两种干预措施,试验措施可以为一种药物、外科手术、物理疗法、预防措施,对照措施为另一种药物、安慰剂或不做任何处理的空白对照;3.RCT 为采用随机分配方法如随机数字表法、计算机随机排序、抛硬币法等将受试者分入不同处理组,CCT 则为采用办随机分配法(按入院顺序、住院号、研究对象的生日的奇偶数交替分配)分配到对照或治疗组者;4.提示性术语有:随机(random )、交替(crossover/cross-over )或安慰剂(placebo )等。
符合这4条的文献将在美国国家医学图书馆(the US national library of medicine, NLM )指定其出版类型是RCT 或CCT ,并在取得NLM 的许可后纳入Cochrane 临床对照试验中心注册库(the Cochrane Central Register of Controlled Trials ,CENTRAL)选择性偏倚(selection bias ):发生在选择和分配研究对象时,因随机方法不完善造成的组间基线不可比,可夸大或缩小干预措施的疗效。
采用真正的随机方法并对随机进行分配隐藏可避免这类偏倚的影响。
实施偏倚(performance bias ):发生在干预措施的实施过程中,指除比较的措施外,向试验组和对照组对象提供的其他措施不一样。
标准化治疗方案和对研究对象及实施研究措施者采用盲法可避免实施偏倚。
丹参川芎嗪注射液治疗冠心病心绞痛系统评价
丹参川芎嗪注射液治疗冠心病心绞痛系统评价吴嘉瑞;张晓朦;张冰;赵梦迪;盛晓光【摘要】Objective To systematically evaluate the clinical efficacy and safety of Danshen Chuanxiongqin Injection (DCI) in the treatment of angina pectoris. Methods Randomized controlled trials (RCTs) regarding DCI in the treatment of angina pectoris were searched in CNKI, VIP, Wanfang Database, CBM, PubMed, Embase and Cochrane Library by Feb. 2014. Two researchers independently retrieved the RCTs and extracted the information. The Cochrane risk of bias method was used to assess the quality of the included studies, and a meta-analysis was conducted with Review Manager 5.2 software. Results A total of 12 RCTs with 1145 participants were included. The meta-analysis indicated that the combined use of DCI and conventional treatment with western medicine was more effective in the outcomes of the total clinical effective rate [RR=1.27, 95%CI (1.19,1.35), P<0.000 01], the total effective rate of ECG [RR=1.34, 95%CI (1.23,1.46), P<0.000 01], and decrease of plasma viscosity [MD=-0.15, 95%CI (-0.25,-0.05), P=0.004] and fibrinogen [MD=-0.96, 95%CI (-1.14,-0.78), P<0.000 01]. And there were no adverse drug reaction reports. Conclusion Based on this systematic evaluation, DCI combined with conventional therapy is effective and relatively safe in treating angina pectoris, but it still needs larger samples, multi-center, and high quality RCT to verify.%目的:系统评价丹参川芎嗪注射液用于治疗冠心病心绞痛的有效性及安全性。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
The Cochrane Collaboration’s tool for assessing risk of bias in randomisedtrialsOPEN ACCESSFlaws in the design, conduct, analysis, and reporting of randomised trials can cause the effect of an intervention to be underestimated or overestimated.The Cochrane Collaboration ’s tool for assessing risk of bias aims to make the process clearer and more accurateJulian P T Higgins senior statistician 1,Douglas G Altman director 2,Peter C Gøtzsche director 3,Peter Jüni head of division 4,David Moher senior scientist 56,Andrew D Oxman senior researcher 7,Jelena Savovićpostdoctoral fellow 8,Kenneth F Schulz vice president 9,Laura Weeks researchassociate 5,Jonathan A C Sterne professor of medical statistics and epidemiology 8,Cochrane Bias Methods Group,Cochrane Statistical Methods Group1MRC Biostatistics Unit,Institute of Public Health,Cambridge CB20SR,UK;2Centre for Statistics in Medicine,University of Oxford,Oxford,UK;3The Nordic Cochrane Centre,Rigshospitalet and University of Copenhagen,Denmark;4Institute of Social and Preventive Medicine,University of Bern,Switzerland;5Clinical Epidemiology Program,Ottawa Hospital Research Institute,Ottawa,Ontario,Canada;6Department of Epidemiology and Community Medicine,Faculty of Medicine,University of Ottawa,Canada;7Preventive and International Health Care Unit,Norwegian Knowledge Centre for the Health Services,Oslo,Norway;8Department of Social Medicine,University of Bristol,Bristol,UK;9FHI,Research Triangle Park,North Carolina,USARandomised trials,and systematic reviews of such trials,provide the most reliable evidence about the effects of healthcare interventions.Provided that there are enough participants,randomisation should ensure that participants in the intervention and comparison groups are similar with respect to both known and unknown prognostic factors.Differences in outcomes of interest between the different groups can then in principle be ascribed to the causal effect of the intervention.1Causal inferences from randomised trials can,however,be undermined by flaws in design,conduct,analyses,and reporting,leading to underestimation or overestimation of the trueintervention effect (bias).2However,it is usually impossible to know the extent to which biases have affected the results of a particular trial.Systematic reviews aim to collate and synthesise all studies that meet prespecified eligibility criteria 3using methods that attempt to minimise bias.To obtain reliable conclusions,review authors must carefully consider the potential limitations of the included studies.The notion of study “quality”is not well defined but relates to the extent to which its design,conduct,analysis,and presentation were appropriate to answer its research question.Many tools for assessing the quality of randomised trials are available,including scales (which score the trials)and checklists(which assess trials without producing a score).4-7Until recently,Cochrane reviews used a variety of these tools,mainly checklists.8In 2005the Cochrane Collaboration’s methods groups embarked on a new strategy for assessing the quality of randomised trials.In this paper we describe the collaboration’s new risk of bias assessment tool,and the process by which it was developed and evaluated.Development of risk assessment toolIn May 2005,16statisticians,epidemiologists,and review authors attended a three day meeting to develop the new tool.Before the meeting,JPTH and DGA compiled an extensive list of potential sources of bias in clinical trials.The items on the list were divided into seven areas:generation of the allocation sequence;concealment of the allocation sequence;blinding;attrition and exclusions;other generic sources of bias;biases specific to the trial design (such as crossover or clusterrandomised trials);and biases that might be specific to a clinical specialty.For each of the seven areas,a nominated meeting participant prepared a review of the empirical evidence,a discussion of specific issues and uncertainties,and a proposed set of criteria for assessing protection from bias as adequate,inadequate,or unclear,supported by examples.Correspondence to: J P T Higgins julian.higgins@.Further details on the items included in risk assessment tool (see /content/343/bmj.d5928/suppl/DC1)BMJ 2011;343:d5928doi:10.1136/bmj.d5928Page 1of 9RESEARCH METHODS &REPORTINGDuring the meeting decisions were made by informal consensus regarding items that were truly potential biases rather than sources of heterogeneity or imprecision.Potential biases were then divided into domains,and strategies for their assessment were agreed,again by informal consensus,leading to the creation of a new tool for assessing potential for bias.Meeting participants also discussed how to summarise assessments across domains,how to illustrate assessments,and how to incorporate assessments into analyses and conclusions.Minutes of the meeting were transcribed from an audio recording in conjunction with written notes.After the meeting,pairs of authors developed detailed criteria for each included item in the tool and guidance for assessing the potential for bias.Documents were shared and feedback requested from the whole working group(including six who could not attend the meeting).Several email iterations took place,which also incorporated feedback from presentations of the proposed guidance at various meetings and workshops within the Cochrane Collaboration and from pilot work by selected review teams in collaboration with members of the working group.The materials were integrated by the co-leads into comprehensive guidance on the new risk of bias tool.This was published in February2008and adopted as the recommended method throughout the Cochrane Collaboration.9 Evaluation phaseA three stage project to evaluate the tool was initiated in early 2009.A series of focus groups was held in which review authors who had used the tool were asked to reflect on their experiences. Findings from the focus groups were then fed into the design of questionnaires for use in three online surveys of review authors who had used the tool,review authors who had not used the tool(to explore why not),and editorial teams within the collaboration.We held a meeting to discuss the findings from the focus groups and surveys and to consider revisions to the first version of the risk of bias tool.This was attended by six participants from the2005meeting and17others,including statisticians,epidemiologists,coordinating editors and other staff of Cochrane review groups,and the editor in chief of the Cochrane Library.The risk of bias toolAt the2005workshop the participants agreed the seven principles on which the new risk of bias assessment tool was based(box).The risk of bias tool covers six domains of bias:selection bias, performance bias,detection bias,attrition bias,reporting bias, and other bias.Within each domain,assessments are made for one or more items,which may cover different aspects of the domain,or different outcomes.Table1⇓shows the recommended list of items.These are discussed in more detail in the appendix on .For each item in the tool,the assessment of risk of bias is in two parts.The support for judgment provides a succinct free text description or summary of the relevant trial characteristic on which judgments of risk of bias are based and aims to ensure transparency in how judgments are reached.For example,the item about concealment of the randomised allocation sequence would provide details of what measures were in place,if any, to conceal the rmation for these descriptions will often come from a single published trial report but may be obtained from a mixture of trial reports,protocols,published comments on the trial,and contacts with the investigators.The support for the judgment should provide a summary of known facts,including verbatim quotes where possible.The source of this information should be stated,and when there is no information on which to base a judgment,this should be stated. The second part of the tool involves assigning a judgment of high,low,or unclear risk of material bias for each item.We define material bias as bias of sufficient magnitude to have a notable effect on the results or conclusions of the trial, recognising the subjectivity of any such judgment.Detailed criteria for making judgments about the risk of bias from each of the items in the tool are available in the Cochrane Handbook.13If insufficient detail is reported of what happened in the trial,the judgment will usually be unclear risk of bias.A judgment of unclear risk should also be made if what happened in the trial is known but the associated risk of bias is unknown—for example,if participants take additional drugs of unknown effectiveness as a result of them being aware of their intervention assignment.We recommend that judgments be made independently by at least two people,with any discrepancies resolved by discussion in the first instance. Some of the items in the tool,such as methods for randomisation,require only a single assessment for each trial included in the review.For other items,such as blinding and incomplete outcome data,two or more assessments may be used because they generally need to be made separately for different outcomes(or for the same outcome at different time points). However,we recommend that review authors limit the number of assessments used by grouping outcomes—for example,as subjective or objective for the purposes of assessing blinding of outcome assessment or as“patient reported at6months”or “patient reported at12months”for assessing risk of bias due to incomplete outcome data.Evaluation of initial implementation The first(2008)version of the tool was slightly different from the one we present here.The2008version did not categorise biases by the six domains(selection bias,performance bias, etc);had a single assessment for blinding;and expressed risk of bias in the format‘”yes,”“no,”or“unclear”(referring to lack of a risk)rather than as low,high,or unclear risk.The2010 evaluation of the initial version found wide acceptance of the need for the risk of bias tool,with a consensus that it represents an improvement over methods previously recommended by the Collaboration or widely used in systematic reviews. Participants in the focus groups noted that the tool took longer to complete than previous methods.Of187authors surveyed, 88%took longer than10minutes to complete the new tool,44% longer than20minutes,and7%longer than an hour,but83% considered the time taken acceptable.There was consensus that classifying items in the tool according to categories of bias (selection bias,performance bias,etc)would help users,so we introduced these.There was also consensus that assessment of blinding should be separated into blinding of participants and health professionals(performance bias)and blinding of outcome assessment(detection bias)and that the phrasing of the judgments about risk should be changed to low,high,and unclear risk.The domains reported to be the most difficult to assess were risk of bias due to incomplete outcome data and selective reporting of outcomes.There was agreement that improved training materials and availability of worked examples would increase the quality and reliability of bias assessments.Principles for assessing risk of bias1.Do not use quality scalesQuality scales and resulting scores are not an appropriate way to appraise clinical trials.They tend to combine assessments of aspects of the quality of reporting with aspects of trial conduct,and to assign weights to different items in ways that are difficult to justify.Both theoretical considerations10and empirical evidence11suggest that associations of different scales with intervention effect estimates are inconsistent and unpredictable2.Focus on internal validityThe internal validity of a study is the extent to which it is free from bias.It is important to separate assessment of internal validity from that of external validity(generalisability or applicability)and precision(the extent to which study results are free from random error).Applicability depends on the purpose for which the study is to be used and is less relevant without internal validity.Precision depends on the number of participants and events in a study.A small trial with low risk of bias may provide very imprecise results,with a wide confidence interval. Conversely,the results of a large trial may be precise(narrow confidence interval)but have a high risk of bias if internal validity is poor 3.Assess the risk of bias in trial results,not the quality of reporting or methodological problems that are not directly related to risk of biasThe quality of reporting,such as whether details were described or not,affects the ability of systematic review authors and users of medical research to assess the risk of bias but is not directly related to the risk of bias.Similarly,some aspects of trial conduct,such as obtaining ethical approval or calculating sample size,are not directly related to the risk of bias.Conversely,results of a trial that used the best possible methods may still be at risk of bias.For example,blinding may not be feasible in many non-drug trials,and it would not be reasonable to consider the trial as low quality because of the absence of blinding.Nonetheless,many types of outcome may be influenced by participants’knowledge of the intervention received,and so the trial results for such outcomes may be considered to be at risk of bias because of the absence of blinding,despite this being impossible to achieve4.Assessments of risk of bias require judgmentAssessment of whether a particular aspect of trial conduct renders its results at risk of bias requires both knowledge of the trial methods and a judgment about whether those methods are likely to have led to a risk of bias.We decided that the basis for bias assessments should be made explicit,by recording the aspects of the trial methods on which the judgment was based and then the judgment itself5.Choose domains to be assessed based on a combination of theoretical and empirical considerationsEmpirical studies show that particular aspects of trial conduct are associated with bias.212However,these studies did not include all potential sources of bias.For example,available evidence does not distinguish between different aspects of blinding(of participants,health professionals, and outcome assessment)and is very limited with regard to how authors dealt with incomplete outcome data.There may also be topic specific and design specific issues that are relevant only to some trials and reviews.For example,in a review containing crossover trials it might be appropriate to assess whether results were at risk of bias because there was an insufficient“washout”period between the two treatment periods6.Focus on risk of bias in the data as represented in the review rather than as originally reportedSome papers may report trial results that are considered as at high risk of bias,for which it may be possible to derive a result at low risk of bias.For example,a paper that inappropriately excluded certain patients from analyses might report the intervention groups and outcomes for these patients,so that the omitted participants can be reinstated7.Report outcome specific evaluations of risk of biasSome aspects of trial conduct(for example,whether the randomised allocation was concealed at the time the participant was recruited) apply to the trial as a whole.For other aspects,however,the risk of bias is inherently specific to different outcomes within the trial.For example,all cause mortality might be ascertained through linkages to death registries(low risk of bias),while recurrence of cancer might have been assessed by a doctor with knowledge of the allocated intervention(high risk of bias)Presentation of assessmentsResults of an assessment of risk of bias can be presented in a table,in which judgments for each item in each trial are presented alongside their descriptive justification.Table2⇓presents an example of a risk of bias table for one trial included in a Cochrane review of therapeutic monitoring of antiretrovirals for people with HIV.14Risks of bias due to blinding and incomplete outcome data were assessed across all outcomes within each included study,rather than separately for different outcomes as will be more appropriate in some situations. Presenting risk of bias tables for every study in a review can be cumbersome,and we suggest that illustrations are used to summarise the judgments in the main systematic review document.The figure⇓provides an example.Here the judgments apply to all meta-analyses in the review.An alternative would be to illustrate the risk of bias for a particular meta-analysis(or for a particular outcome if a statistical synthesis is not undertaken),showing the proportion of information that comes from studies at low,unclear,or high risk of bias for each item in the tool,among studies contributing information to that outcome.Summary assessment of risk of biasTo draw conclusions about the overall risk of bias within or across trials it is necessary to summarise assessments across items in the tool for each outcome within each trial.In doing this,review authors must decide which domains are most important in the context of the review,ideally when writing their protocol.For example,for highly subjective outcomes such as pain,blinding of participants is critical.The way that summary judgments of risk of bias are reached should be explicit and should be informed by empirical evidence of bias when it exists,likely direction of bias,and likely magnitude of bias. Table3⇓provides a suggested framework for making summary assessments of the risk of bias for important outcomes within and across trials.Assessments of risk of bias and synthesis of resultsSummary assessments of the risk of bias for an outcome within each trial should inform the meta-analysis.The two preferable analytical strategies are to restrict the primary meta-analysis to studies at low risk of bias or to present meta-analyses stratified according to risk of bias.The choice between these strategies should be based on the context of the particular review and the balance between the potential for bias and the loss of precision when studies at high or unclear risk of bias are excluded. Meta-regression can be used to compare results from studies at high and low risk of bias,but such comparisons lack power,15 and lack of a significant difference should not be interpreted as implying the absence of bias.A third strategy is to present a meta-analysis of all studies while providing a summary of the risk of bias across studies.However,this runs the risk that bias is downplayed in the discussion and conclusions of a review,so that decisions continue to be based, at least in part,on flawed evidence.This risk could be reduced by incorporating summary assessments into broader,but explicit, measures of the quality of evidence for each important outcome, for example using the GRADE system.16This can help to ensure that judgments about the risk of bias,as well as other factors affecting the quality of evidence(such as imprecision, heterogeneity,and publication bias),are considered when interpreting the results of systematic reviews.1718 DiscussionDiscrepancies between the results of different systematic reviews examining the same question1920and between meta-analyses and subsequent large trials21have shown that the results of meta-analyses can be biased,which may be partly caused by biased results in the trials they include.We believe our risk of bias tool is one of the most comprehensive approaches to assessing the potential for bias in randomised trials included in systematic reviews or meta-analyses.Inclusion of details of trial conduct,on which judgments of risk of bias are based,provides greater transparency than previous approaches,allowing readers to decide whether they agree with the judgments made.There is continuing uncertainty,and great variation in practice,over how to assess potential for bias in specific domains within trials, how to summarise bias assessments across such domains,and how to incorporate bias assessments into meta-analyses.A recent study has found that the tool takes longer to complete than other tools(the investigators took a mean of8.8minutes per person for a single predetermined outcome using our tool compared with1.5minutes for a previous rating scale for quality of reporting).22The reliability of the tool has not been extensively studied,although the same authors observed that larger effect sizes were observed on average in studies rated as at high risk of bias compared with studies at low risk of bias.22 By explicitly incorporating judgments into the tool,we acknowledge that agreements between assessors may not be as high as for some other tools.However,we also explicitly target the risk of bias rather than reported characteristics of the trial. It would be easier to assess whether a drop-out rate exceeds 20%than whether a drop-out rate of21%introduces an important risk of bias,but there is no guarantee that results from a study with a drop-out rate lower than20%are at low risk of bias.Preliminary evidence suggests that incomplete outcome data and selective reporting are the most difficult items to assess; kappa measures of agreement of0.32(fair)and0.13(slight) respectively have been reported for these.22It is important that guidance and training materials continue to be developed for all aspects of the tool,but particularly these two.We hope that widespread adoption and implementation of the risk of bias tool,both within and outside the Cochrane Collaboration,will facilitate improved appraisal of evidence by healthcare decision makers and patients and ultimately lead to better healthcare.Improved understanding of the ways in which flaws in trial conduct may bias their results should also lead to better trials and more reliable evidence.Risk of bias assessments should continue to evolve,taking into account any new empirical evidence and the practical experience of authors of systematic reviews.Contributors:All authors contributed to the drafting and editing of the manuscript.JPTH,DGA,PCG,PJ,DM,ADO,KFS and JACS contributed to the chapter in the Cochrane Handbook for Systematic Reviews of Interventions on which the paper is based.JPTH will act as guarantor.Development meeting participants(May2005):Doug Altman(co-lead), Gerd Antes,Chris Cates,Jon Deeks,Peter Gøtzsche,Julian Higgins (co-lead),Sally Hopewell,Peter Jüni(organising committee),Steff Lewis, Philippa Middleton,David Moher(organising committee),Andy Oxman, Ken Schulz(organising committee),Nandi Siegfried,Jonathan Sterne, Simon Thompson.Other contributors to tool development:Hilda Bastian,Rachelle Buchbinder,Iain Chalmers,Miranda Cumpston,Sally Green,Peter Herbison,Victor Montori,Hannah Rothstein,Georgia Salanti,Guido Schwarzer,Ian Shrier,Jayne Tierney,Ian White and Paula Williamson. Evaluation meeting participants(March2010):Doug Altman(organising committee),Elaine Beller,Sally Bell-Syer,Chris Cates,Rachel Churchill, June Cody,Jonathan Cook,Christian Gluud,Julian Higgins(organising committee),Sally Hopewell,Hayley Jones,Peter Jűni,Monica Kjeldstrøm,Toby Lasserson,Allyson Lipp,Lara Maxwell,Joanne McKenzie,Craig Ramsey,Barney Reeves,Jelena Savović(co-lead), Jonathan Sterne(co-lead),David Tovey,Laura Weeks(organising committee).Other contributors to tool evaluation:Isabelle Boutron,David Moher (organising committee),Lucy Turner.Funding:The development and evaluation of the risk of bias tool was funded in part by The Cochrane Collaboration.The views expressed in this article are those of the authors and not necessarily those of The Cochrane Collaboration or its registered entities,committees or working groups..JPTH was also funded by MRC grant number U.1052.00.011. DGA was funded by Cancer Research UK grant number C-5592.DM was funded by a University Research Chair(University of Ottawa).The Canadian Institutes of Health Research provides financial support to the Cochrane Bias Methods Group.Competing interests:All authors have completed the ICJME unified disclosure form at /coi_disclosure.pdf(available on request from the corresponding author)and declare support from the Cochrane Collaboration for the development and evaluation of the tool described;they have no financial relationships with any organisations that might have an interest in the submitted work in the previous three years and no other relationships or activities that could appear to have influenced the submitted work.Provenance and peer review:Not commissioned;externally peer reviewed.1Kleijnen J,Gøtzsche P,Kunz RH,Oxman AD,Chalmers I.So what’s so special about randomisation?In:Maynard A,Chalmers I,eds.Non-random reflections on health services research:on the25th anniversary of Archie Cochrane’s Effectiveness and Efficiency.BMJ Books,1997:93-106.2Wood L,Egger M,Gluud LL,Schulz K,Jüni P,Altman DG,et al.Empirical evidence of bias in treatment effect estimates in controlled trials with different interventions andoutcomes:meta-epidemiological study.BMJ2008;336:601-5.3Egger M,Davey Smith G,Altman DG,eds.Systematic reviews in health care: meta-analysis in context.BMJ Books,2001.4Moher D,Jadad AR,Nichol G,Penman M,Tugwell P,Walsh S.Assessing the quality of randomized controlled trials—an annotated bibliography of scales and checklists.Controlled Clin Trials1995;12:62-73.5Jüni P,Altman DG,Egger M.Systematic reviews in health care:assessing the quality of controlled clinical trials.BMJ2001;323:42-6.6West S,King V,Carey TS,Lohr KN,McKoy N,Sutton SF,et al.Systems to rate the strength of scientific evidence.Evidence report/technology assessment no47.AHRQ publication No02-E016.Agency for Healthcare Research and Quality,2002.7Crowe M,Sheppard L.A review of critical appraisal tools show they lack rigor:alternative tool structure is proposed.J Clin Epidemiol2011;64:79-89.8Lundh A,Gøtzsche PC.Recommendations by Cochrane Review Groups for assessment of the risk of bias in studies.BMC Med Res Methodol2008;8:22.9Higgins JPT,Green S,eds.Cochrane handbook for systematic reviews of interventions .Wiley,2008.10Greenland S,O’Rourke K.On the bias produced by quality scores in meta-analysis,anda hierarchical view of proposed solutions.Biostatistics2001;2:463-71.11Jüni P,Witschi A,Bloch R,Egger M.The hazards of scoring the quality of clinical trials for meta-analysis.JAMA1999;282:1054-60.12Gluud LL.Bias in clinical intervention research.Am J Epidemiol2006;163:493-501. 13Higgins JPT,Altman DG.Assessing risk of bias in included studies.In:Higgins JPT, Green S,eds.Cochrane handbook for systematic reviews of interventions.Wiley,2008:187-241.14Kredo T,Van der Walt J-S,Siegfried N,Cohen K.Therapeutic drug monitoring of antiretrovirals for people with HIV.Cochrane Database Syst Rev2009;3:CD007268. 15Higgins JPT,Thompson SG.Controlling the risk of spurious findings from meta-regression.Stat Med2004;23:1663-82.Summary pointsSystematic reviews should carefully consider the potential limitations of the studies includedThe Cochrane Collaboration has developed a new tool for assessing risk of bias in randomised trialsThe tool separates a judgment about risk of bias from a description of the support for that judgment,for a series of items covering different domains of bias16Guyatt GH,Oxman AD,Vist GE,Zunz R,Falck-Ytter Y,Alonso-Coello P,et al.GRADE: an emerging consensus on rating quality of evidence and strength of recommendations.BMJ2008;336:924-6.17Schünemann HJ,Oxman AD,Higgins JPT,Vist GE,Glasziou P,Guyatt GH,et al.Presenting results and“Summary of findings”tables.In:Higgins JPT,Green S,eds.Cochrane handbook for systematic reviews of interventions.Wiley,2008:335-8.18Schünemann HJ,Oxman AD,Vist GE,Higgins JPT,Deeks JJ,Glasziou P,et al.Interpreting results and drawing conclusions.In:Higgins JPT,Green S,eds.Cochrane handbook for systematic reviews of interventions.Wiley,2008:359-87.19Leizorovicz A,Haugh MC,Chapuis FR,Samama MM,Boissel JP.Low molecular weight heparin in prevention of perioperative thrombosis.BMJ1992;305:913-20.20Nurmohamed MT,Rosendaal FR,Buller HR,Dekker E,Hommes DW,Vandenbroucke JP,et al.Low-molecular-weight heparin versus standard heparin in general and orthopaedic surgery:a ncet1992;340:152-6.21Lelorier J,Benhaddad A,Lapierre J,Derderian F.Discrepancies between meta-analyses and subsequent large randomized,controlled trials.N Engl J Med1997;337:536-42.22Hartling L,Ospina M,Liang Y,Dryden DM,Hooton N,Krebs SJ,et al.Risk of bias versus quality assessment of randomised controlled trials:cross sectional study.BMJ2009;339:b4012.Accepted:22July2011Cite this as:BMJ2011;343:d5928This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License,which permits use,distribution,and reproduction in any medium,provided the original work is properly cited,the use is non commercial and is otherwise in compliance with the license.See:/licenses/by-nc/2.0/and /licenses/by-nc/2.0/legalcode.。