Hepatic fibrosis and cirrhosis The (myo)fibroblastic cell subpopulations involved
肝纤维化的英文名词解释

肝纤维化的英文名词解释Liver Fibrosis: An In-depth ExplorationIntroduction:Liver fibrosis, also known as hepatic fibrosis, refers to the excessive accumulation of extracellular matrix proteins—particularly collagen—in the liver, resulting in the progressive scarring and stiffening of the organ. It develops as a response to chronic liver injury and can eventually lead to cirrhosis if left untreated. In this article, we aim to provide a comprehensive understanding of liver fibrosis, its causes, progression, and potential treatments.Causes of Liver Fibrosis:Liver fibrosis can be caused by various factors, including chronic viral hepatitis B and C, excessive alcohol consumption, non-alcoholic fatty liver disease (NAFLD), autoimmunity disorders, and drug-induced liver injury. These conditions trigger an immune response, leading to inflammation and the activation of hepatic stellate cells—the primary cells involved in fibrogenesis.Progression of Liver Fibrosis:Liver fibrosis typically progresses through several stages, characterized by the accumulation of connective tissue and architectural changes in the liver. These stages are usually assessed using a scoring system known as the METAVIR or Ishak scoring system, which grades fibrosis from F0 (no fibrosis) to F4 (cirrhosis).Stage 1 (F1): Portal Fibrosis with Few SeptaAt this early stage, there is minimal scarring and fibrosis, mainly around the portal tracts in the liver. The condition is usually reversible at this point with appropriate treatment and lifestyle changes.Stage 2 (F2): Portal Fibrosis with Occasional SeptaProgressing from the first stage, the liver shows increased fibrosis, with occasional bridging septa formation between the portal tracts. Early intervention is crucial at this stage to prevent further advancement.Stage 3 (F3): Numerous Septa without CirrhosisThe liver now exhibits multiple bridging septa, potentially leading to the distortion of the liver architecture. Timely medical intervention is vital to slow down or halt the progression of liver fibrosis.Stage 4 (F4): CirrhosisIn the final stage of liver fibrosis, extensive scarring and the formation of regenerative nodules disrupt the normal liver structure and function. Cirrhosis can lead to severe complications, and liver transplantation may be the only viable treatment option.Potential Treatments for Liver Fibrosis:1. Lifestyle Changes: Adopting a healthy lifestyle is crucial in managing liver fibrosis. This includes maintaining a balanced diet, exercising regularly, avoiding excessive alcohol consumption, and reducing exposure to toxins.2. Antiviral Therapy: In cases where viral hepatitis is the underlying cause, antiviral medications can help suppress the replication of the virus, reduce inflammation, and slow down fibrosis progression.3. Pharmacological Interventions: Various pharmaceutical agents are being researched for their potential anti-fibrotic effects. These include drugs that target specific signaling pathways involved in fibrogenesis, such as transforming growth factor-beta (TGF-β) inhibitors and angiotensin receptor blockers (ARBs).4. Liver Transplantation: In severe cases of cirrhosis, where liver function is severely compromised, a liver transplant may be the only viable option. However, the availability of suitable donor organs limits the widespread use of this treatment.Conclusion:Liver fibrosis is a complex and progressive condition that can have significant implications for an individual's health. Timely diagnosis, understanding the underlying causes, and implementing appropriate treatments are crucial in managing and potentially halting the progression of this disease. Ongoing research and advancements in medical interventions hold promise for more effective treatments for liver fibrosis in the future.。
非酒精性脂肪性肝病的药物治疗进展

pharmacologic
Key words
Nonalcoholic Fatty Liver Disease;Drug Hepatoprotective
Therapy;Anti・-Obesity Agents;Lipid・-Lowering Agents;
Agents;Drug,Chinese Hemal
二甲双胍可降低肝脏糖异生以减少肝糖产生.同时增 加肌肉等外周组织对血糖的摄取和利用,改善胰岛素敏感 性。此外,二甲双胍还可作用于诱导胰岛素抵抗的肿瘤坏死 因子(TNF)咀,缓解冈TNF诱导所致的肝脂肪变、炎症和纤 维化。服用二甲双胍(2000 mg/d),3个月后血清转氨酶水平 明显降低,其疗效优于饮食控制组和维生素E组【8l。尽管 NAFLD患者对二甲双胍的耐受性较好.且大剂量使用后未 观察到明显不良反应191,但该药的有效性和安全性仍需进一 步证实。 噻唑烷二酮类通过活化细胞核转录因子过氧化物酶体 增生物激活受体(PPAR),调控与葡萄糖产生、转运、利用和 脂代谢相关的某些通路中相关基因的转录.提高脂肪组织 对胰岛索的敏感性。从而在代谢综合征中起重要作用。然 而,噻唑烷二酮类药物会引起体质量增加和脂肪组织重新 分布,冈此建议与二甲双胍类药物同时使用。曲格列酮是噻 唑烷二酮类药物的首代化合物,因有严重肝毒性.已被弃 用㈣。罗格列酮和吡格列酮是第二代产物,具有改善转氨酶 水平和脂肪变性的作用。有研究…l予NASH患者罗格列酮
DING
We嘲in,FA N Jiangao.Department of
Correspondence to:FAN Abstract
can
Jiangao,Emaih fanjiangao@gmail,corn
Nonalcoholic fatty liver
预防血吸虫英语作文600字

预防血吸虫英语作文600字Schistosomiasis Prevention: A Comprehensive Guide.Schistosomiasis, also known as bilharzia, is a parasitic disease caused by trematode worms of the genus Schistosoma. It is prevalent in tropical and subtropical regions of the world, primarily affecting impoverished communities with inadequate sanitation and access to clean water. Schistosomiasis poses significant health risks, impacting individuals, families, and entire communities.Transmission.Schistosoma parasites have a complex life cycle involving humans and freshwater snails as intermediate hosts. Humans become infected when they come into contact with contaminated water while wading, bathing, or fetching water. The parasite larvae, known as cercariae, penetrate the skin and mature into adult worms that reside in the blood vessels of the intestines or bladder.Symptoms.The severity of schistosomiasis symptoms depends on the species of parasite and the intensity of infection. Common symptoms include:Early-Stage Infection: Fever, chills, headaches, and muscle aches.Intestinal Schistosomiasis: Abdominal pain, diarrhea, blood in the stool.Urogenital Schistosomiasis: Frequent urination, pain during urination, blood in the urine.Complications.Untreated schistosomiasis can lead to severe complications, including:Intestinal Lesions: Scarring and damage to theintestines, leading to malnutrition and anemia.Urinary Tract Damage: Narrowing or blockage of the ureters and bladder, causing kidney damage.Pulmonary Hypertension: Blockage of the pulmonary arteries, leading to heart failure.Hepatic Fibrosis: Scarring of the liver, leading to cirrhosis.Prevention.Preventing schistosomiasis is crucial to safeguarding public health and improving the well-being of at-risk populations. Effective prevention strategies include:Safe Water Supply: Access to clean, uncontaminated drinking water is essential for reducing transmission.Sanitation Improvements: Proper sanitation facilities, including toilets and handwashing stations, prevent thecontamination of water sources with human waste.Snail Control: Reducing the population of freshwater snails, which serve as intermediate hosts for the parasite, can help break the transmission cycle.Health Education: Raising awareness about schistosomiasis and promoting healthy practices, such as avoiding contact with contaminated water, is crucial for prevention.Mass Drug Administration: In areas with high prevalence, mass drug administration programs with praziquantel, an effective medication against schistosomiasis, can be implemented to reduce infection rates.Control and Treatment.In addition to prevention, effective control and treatment measures are essential for managing schistosomiasis and mitigating its impact on communities.Diagnosis: Accurate diagnosis through laboratory tests is crucial for proper treatment.Treatment: Praziquantel is the primary drug used to treat schistosomiasis. It is safe and effective in killing the adult worms.Surveillance: Regular surveillance is necessary to monitor schistosomiasis prevalence and assess the effectiveness of prevention and control programs.Conclusion.Schistosomiasis prevention is a vital public health endeavor that requires a multifaceted approach involving governments, healthcare providers, and communities. By implementing comprehensive prevention strategies, safe water supply, improved sanitation, snail control, health education, and mass drug administration, we cansignificantly reduce the burden of schistosomiasis andimprove the health and well-being of vulnerable populations worldwide.。
肝脏毒理学
肝脏毒理学1.什么是肝脏毒理学和化学性肝损伤?肝脏毒理学(toxicology of the liver):是利用毒理学的基本方法和技术,研究外源化学物对肝的损害作用特点及其机制的学科,它是靶器官毒理学的一个重要研究领域。
化学性肝损害(chemically induced liver injury):化学物引起的各种急性和慢性肝损害。
短期暴露:肝细胞内脂质蓄积、肝细胞坏死、肝胆功能障碍长期暴露:肝硬化、瘤样改变2.为什么肝脏是外源化学物作用的重要靶器官?a.在机体内肝脏具有特殊的解剖位置、组织结构和生理生化特性。
肝脏最易作为外来化学物的毒作用靶器官。
b.肝脏是一个被血液充盈的器官,与血液循环密切相关,由于肝脏存在两套入肝血管,分别接受来自胃肠道血液与体循环的动脉血液,化学物质无论从何种途径进入机体,均可通过血液循环达到肝脏,尤其从消化道吸收的毒物,在进入血液循环以前毒物首先与肝脏接触。
c.肝脏作为化学毒物的生物转化器官,在一定条件下,化学毒物极易对肝脏造成损害作用,特别是经体内代谢增毒的外源化学物质在肝脏代谢转化后其有毒代谢产物可首先损害肝脏。
d.由胆汁排泄的有毒化学物质或代谢产物,可通过肝-肠循环系统再次进入肝脏发挥毒作用。
3.肝脏对外源性化学物的毒性反应有哪些?肝脏对外源化学物的毒性反应依赖于化学物性质、受损细胞群种类、接触剂量与方式等。
化学性肝损伤按其损伤发生的快慢可分为急性肝损伤与慢性肝损伤。
急性肝损伤(acute liver injury)一般是短期接触较大剂量肝毒物或肝脏功能不全时接触某种肝毒物引起,病理改变常见于肝细胞坏死、脂肪变性、胆汁淤积等。
慢性肝损伤(chronic liver injury)可因长期接触低剂量肝毒物引起,也可由一次急性坏死引起的后遗症,病理改变包括纤维化、硬变、癌变等。
一.肝细胞死亡(hepatocyte death)化学毒物引起肝细胞死亡有两种情况:细胞坏死(necrosis);细胞凋亡(apoptosis)二.脂肪变性(steatosis)三、胆汁淤积(cholestasis)胆汁淤积较脂肪肝和肝坏死少见,它常常是肝脏对化学毒物的一种急性毒性反应,其出现频率较脂肪肝与肝细胞坏死低,有时可傍有轻微的胆道炎症和肝细胞坏死。
肝纤维化讲解

ECM旳构成及主要功能
构成:蛋白质(胶原、弹力纤维)、糖蛋白 及蛋白多糖
功能:
1、支撑及维持组织构造、形态与修复 2、细胞接触面及半选择性弥散屏障 3、调整细胞分化、增殖、移行及信息传递 4、参加调整微循环、代谢及免疫反应
ECM 旳胶原蛋白质
间质性胶原(纤维形成胶原): I、III型:为肝内主要胶原成份,各占33%,I / III百分比为1:1;
非创伤性诊疗 创伤性诊疗
组织病理学诊疗
肝活检标本组织学检验是纤维化诊疗旳金原则 常规组织形态学评估 特殊旳组织学检验 肝纤维化组织学半定量评估系统 计算机图像分析系统
几种肝纤维化分期半定量评估系统
评分 Knodell
Ishak
Scheuer
0
无纤维化
无纤维化
无纤维化
1
汇管区扩大 有些PF±短纤维隔
V型:分布于血窦周围和门脉区,作为关键使I、III型胶原形 成粗大旳纤维;
VI型:分布于I、III、V型胶原形成旳纤维素之间起粘附作用; 基底膜胶原(非纤维形成胶原):
IV型:主要分布于肝血窦内皮下,是肝细胞和内皮细胞功 能性基底膜旳主要成份;
ECM 旳非胶原糖蛋白
纤维连接素(FN):在肝纤维化早期时增多,作为后来胶原 沉积旳支架;
TGFß1在肝纤维化形成所起旳中心作用
刺激ECM合成 增长I、III、IV型胶原、 FN 诱致HSC合成胶原 调整细胞增生 克制HSC增生,但刺激其转化
克制基质降解 降低MMPS合成 增长TIMPS旳合成并调整本身活性型旳变化
受体体现增强 TGFβ辅助受体合成↑
刺激其他生长因子受体(PDGF、TGFα)体现↑及整合素家族受体↑
参加肝纤维化旳细胞成份
非酒精性脂肪性肝病儿童肝组织病理特征分析

,- . DOI:10.3969/j.issn.1001-5256.2023.05.021非酒精性脂肪性肝病儿童肝组织病理特征分析刘 敏a,陈卫坚a,周峥珍a,覃小梅b,文 容a,姜 楠a,匡林芝a,郑台青a,张丽琼a,李双杰b湖南省儿童医院a.病理科,b.肝病中心,长沙410000通信作者:李双杰,2273858951@qq.com(ORCID:0000-0002-3792-6793)关键词:非酒精性脂肪性肝病;病理学,临床;儿童基金项目:湖南省卫生健康委科研项目计划(202206014267)Histopathologicalcharacteristicsoftheliverinchildrenwithnon-alcoholicfattyliverdiseaseLIUMina,CHENWeijiana,ZHOUZhengzhena,QINXiaomeib,WENRonga,JIANGNana,KUANGLinzhia,ZHENGTaiqinga,ZHANGLiqionga,LIShuangjieb.(a.DepartmentofPathology,b.LiverDiseaseCenter,HunanChildren’sHospital,Changsha410000,China)Correspondingauthor:LIShuangjie,2273858951@qq.com(ORCID:0000-0002-3792-6793)Keywords:Non-alcoholicFattyLiverDisease;Pathology,Clinical;ChildResearchfunding:ResearchProjectPlanofHunanProvincialHealthCommission(202206014267) 非酒精性脂肪性肝病(non-alcoholicfattyliverdisease,NAFLD)已成为全球儿童发生率最高的慢性肝病[1-2]。
Fibroscan对慢性乙型肝炎肝纤维化诊断的临床应用进展

Fibroscan对慢性乙型肝炎肝纤维化诊断的临床应用进展王荔【摘要】As "the gold standard" of fibrosis diagnosis, liver biopsy is not widely accepted in clinic use, because of its numerous drawbacks, such as its invasive nature which may lead to serious complications,false-negative diagnosis because of sampling error,and intra-and inter-observer variability. Transient elastography, also named as Fibroscan, is a non-invasive access to diagnose liver fibrosis and cirrhosis by measuring liver stiffness. Recently, researches about the clinic use of Fibroscan for diagnosis of liver fibrosis in chronic hepatitis B patients are becoming more and more,and the establishment of a unified diagnosis standard in combination with some other indexes to increase the diagnosis accuracy are the research hotspots.%肝活检目前仍是作为肝纤维化分期的金标准,但由于它的有创性和存在采样误差、观察者间变异性等局限性使它尚未普遍应用于临床.Fibroscan以超声为基础,利用切变弹性探测仪测定肝脏硬度值来判断肝纤维化和肝硬化分级,它符合肝纤维化无创评价需要的许多标准.近年来,Fibroscan对乙型肝炎导致的肝纤维化的研究日益增多,制订一个统一的诊断标准,并联合应用其他指标以提高对乙型肝炎肝纤维化的诊断准确率是当前研究的热点.【期刊名称】《医学综述》【年(卷),期】2012(018)015【总页数】3页(P2436-2438)【关键词】乙型肝炎;肝纤维化;瞬时弹性成像技术;无创诊断【作者】王荔【作者单位】泸州医学院附属医院超声诊断科,四川,泸州646100【正文语种】中文【中图分类】R445.1肝纤维化是包括慢性乙型肝炎在内的多种不同肝损伤向肝硬化发展的必经阶段,是肝脏纤维结缔组织过度沉积,以及细胞外基质合成和降解不平衡的结果。
肝纤维化的发病机制和治疗进展

2019年第9期广东化工第46卷总第395期·145·肝纤维化的发病机制和治疗进展黄素洁,薛晓文*(中国药科大学药学院,江苏南京21009)Pathogenesis and Treatment Progress of Liver FibrosisHuang Sujie,Xue Xiaowen*(School of Pharmacy,China Pharmaceutical University,Nanjing21009,China)Abstract:Liver fibrosis is a necessary process for many chronic liver diseases,which eventually leads to cirrhosis,liver dysfunction and a high risk of liver cancer.This article briefly introduces the pathogenesis of liver fibrosis and the main cellular molecules and signaling pathways involved,and summarizes the current research progress of anti-liver fibrotic drugs.At present,there are many anti-liver fibrosis drugs,but there is still a lack of clinically effective anti-liver fibrosis drugs.Keywords:liver fibrosis;signaling pathway;cytokines;treatment progress与其他器官相比,肝的纤维化同样是细胞外基质(extracellular matrix,ECM)和纤状胶原过度积累的结果。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
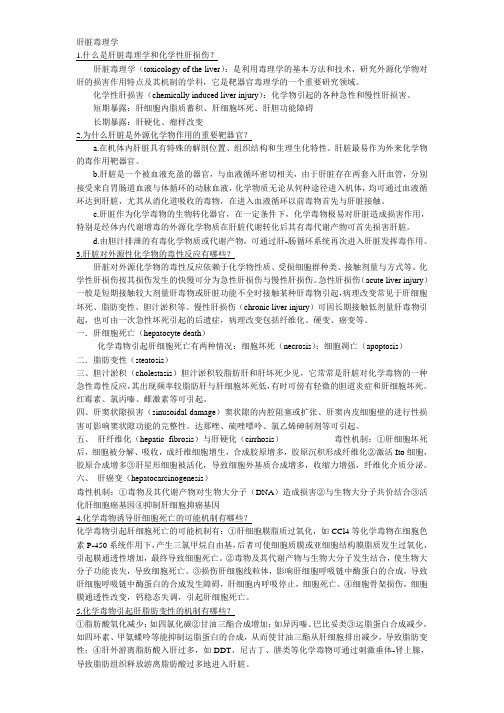
The International Journal of Biochemistry&Cell Biology38(2006)135–151Medicine in focusHepaticfibrosis and cirrhosis:The(myo)fibroblastic cellsubpopulations involvedChristelle Guyot a,S´e bastien Lepreux a,b,c,Chantal Combe a,Evelyne Doudnikoff c, Paulette Bioulac-Sage a,b,Charles Balabaud a,Alexis Desmouli`e re a,∗a GREF,INSERM E0362,Universit´e Victor Segalen Bordeaux2,146,rue L´e o-Saignat,Bordeaux Cedex,F-33076Franceb CHU Bordeaux,Hˆo pital Pellegrin,Service d’Anatomie Pathologique,Bordeaux,F-33076Francec Laboratoire d’Histologie-Embryologie,UFR II,Universit´e Victor Segalen Bordeaux2,Bordeaux,F-33076FranceReceived9June2005;received in revised form28August2005;accepted31August2005AbstractFibrosis,defined as the excessive deposition of extracellular matrix in an organ,is the main complication of chronic liver damage. Its endpoint is cirrhosis,which is responsible for significant morbidity and mortality.The accumulation of extracellular matrix observed infibrosis and cirrhosis is due to the activation offibroblasts,which acquire a myofibroblastic phenotype.Myofibroblasts are absent from normal liver.They are produced by the activation of precursor cells,such as hepatic stellate cells and portal fibroblasts.Thesefibrogenic cells are distributed differently in the hepatic lobule:the hepatic stellate cells resemble pericytes and are located along the sinusoids,in the Disse space between the endothelium and the hepatocytes,whereas the portalfibroblasts are embedded in the portal tract connective tissue around portal structures(vessels and biliary structures).Differences have been reported between these twofibrogenic cell populations,in the mechanisms leading to myofibroblastic differentiation,activation and “deactivation”,but confirmation is required.Second-layer cells surrounding centrolobular veins,fibroblasts present in the Glisson capsule surrounding the liver,and vascular smooth muscle cells may also express a myofibroblastic phenotype and may be involved infibrogenesis.It is now widely accepted that the various types of lesion(e.g.,lesions caused by alcohol abuse and viral hepatitis) leading to liverfibrosis involve specificfibrogenic cell subpopulations.The biological and biochemical characterisation of these cells is thus essential if we are to understand the mechanisms underlying the progressive development of excessive scarring in the liver. These cells also differ in proliferative and apoptotic capacity,at least in vitro.All this information is required for the development of treatments specifically and efficiently targeting the cells responsible for the development offibrosis/cirrhosis.©2005Elsevier Ltd.All rights reserved.Keywords:Fibroblast;Myofibroblast;Extracellular matrix;Liverfibrosis;Cirrhosis;RemodellingAbbreviations:CCl4,carbon tetrachloride;CRBP-1,cellular retinol-binding protein-1;MMP,matrix metalloproteinase;TGF-1,transforming growth factor-1;TIMP-1,tissue inhibitor of metalloproteinase-1∗Corresponding author.Tel.:+33557571771;fax:+33556514077.E-mail address:Alexis.Desmouliere@gref.u-bordeaux2.fr (A.Desmouli`e re).1.IntroductionThe processes of liver repair and offibrogenesis resemble a wound healing process.When injury and the associated acute inflammation response result in moder-ate cell necrosis and extracellular matrix damage,tissue repair normally takes place.In this process,dead cells are replaced by normal tissue,with regeneration of spe-cialised cells by proliferation of the surviving ones,for-mation of a granulation tissue,and tissue remodelling1357-2725/$–see front matter©2005Elsevier Ltd.All rights reserved. doi:10.1016/j.biocel.2005.08.021136 C.Guyot et al./The International Journal of Biochemistry&Cell Biology38(2006)135–151with scar formation.The specific regenerative capacities of the liver generally allow it to reconstitute itself entirely following acute,moderate lesions.However,chronic injuries to the liver do not always heal as effectively and fibrosis is the main complication of the many known chronic liver diseases.Various types of chronic injury, due to alcohol abuse,viral hepatitis(especially Hep-atitis B and C),drugs,metabolic diseases(mainly due to overload of iron or copper),autoimmune destruction of hepatocytes or bile duct epithelium,and congenital abnormalities may lead to liverfibrosis(for review,see Bataller&Brenner,2005).The liver parenchyma is divided into functional units called lobules.The lobules are polygonal,generally hexagonal,and each is1–2mm in diameter and com-posed of a labyrinth of interconnected hepatocyte plates separated by endothelium-lined sinusoids.Each lobule is crossed by a central structure,the centrolobular vein. The hepatocyte plates radiate out from the centrolobu-lar vein to the perimeter of the lobule;the portal triads (portal vein,hepatic artery,and bile ductule),and the surrounding connective tissue are typically found at the angles of the polygon(Fig.1a and b).Liverfibrosis is defined as the abnormal accumu-lation of extracellular matrix in the liver.Its endpoint is cirrhosis,which is responsible for a significant mor-bidity and mortality.Cirrhosis is an advanced stage of fibrosis,characterised by the formation of regenerative nodules of liver parenchyma separated byfibrotic septa. Three major mechanisms are involved in the generation of cirrhosis:cell death,aberrant extracellular matrix deposition(fibrosis),and vascular reorganisation. Fibrous septa connecting the portal tracts and hepatic veins form,leading to portovenous and arteriovenous shunting,and effective bypassing of the parenchymal nodules.This results in vascular thrombosis of the medium-sized and large portal veins and of the hepatic veins and the progression of parenchymal extinction to full-blown cirrhosis.Parenchymal extinction is the loss of continuous hepatocyte layers due tofibrosis of the parenchymal stroma(Wanless,2002).In most cases, significant lesions are observed only after months or years of injury.However,they may appear more rapidly in congenital liver diseases,such as biliary atresia.Liver fibrosis is reversible,whereas cirrhosis is generally irre-versible(Benyon&Iredale,2000;Bioulac-Sage et al., 2000).Prevention of the progression offibrosis to cir-rhosis is therefore a major clinical goal.Unfortunately, current treatments of the underlying diseases responsible for liver damage are only partly successful in preventing this progression.The poor prognosis of cirrhosis is aggravated by the frequent occurrence of hepatocellular carcinoma,which may also develop,albeit much more rarely,in normal or only slightlyfibrous livers.The accumulation of extracellular matrix observed infibrosis and cirrhosis is due to the activation of fibroblasts,which acquire a myofibroblastic phenotype. Myofibroblasts are absent from normal liver.They are produced by the activation of precursor cells,such as hepatic stellate cells(for review,see Lotersztajn,Julien, Teixeira-Clerc,Grenard,&Mallat,2005).It has been suggested that liverfibrogenic cells are heterogeneous, as the portalfibroblasts present in portal tracts may also play a major role in liverfibrogenesis(Dranoff et al.,2002;Kinnman et al.,2003;Knittel et al.,1999b; Tang,Tanaka,Marumo,&Sato,1994;Tuchweber, Desmouli`e re,Bochaton-Piallat,Rubbia-Brandt,& Gabbiani,1996).In this review,we will identify the variousfibrogenic cell subpopulations involved in liver fibrogenesis,and discuss the mechanisms underlying myofibroblastic differentiation and extracellular matrix deposition in various liver disease.Finally,we will eval-uate the possibility of tissue remodelling,which may renderfibrosis and cirrhosis reversible in some cases.2.Definition of the myofibroblastInflammation occurs in response to tissue damage, with the formation of a provisional matrix favouring cell migration and proliferation in the lesion.Granulation tissue,facilitating the replacement of the injured tissue, then develops.This tissue displaysfibroblast prolifera-tion,angiogenesis,and extracellular matrix deposition. During tissue repair and granulation tissue formation,fibroblasts acquire the smooth muscle features char-acteristic of myofibroblasts(for review,see Serini& Gabbiani,1999;Tomasek,Gabbiani,Hinz,Chaponnier, &Brown,2002),the main cell type in granulation tissue. Myofibroblasts therefore appear to be a morphological and functional intermediate betweenfibroblasts and the smooth muscle cells.Myofibroblasts contain cytoplas-mic bundles of microfilaments or stressfibres,which play a role in contraction,via mechanisms similar but not identical to those in smooth muscle cells.Myofi-broblasts are surrounded by an irregular basal mem-brane,and are connected to each other by gap junctions and to the extracellular matrix by focal contacts called fibronexi—transmembrane complexes containing intra-cellular microfilaments in continuity with extracellular fibronectinfibrils(Eyden,1993).Myofibroblasts are the main cellular type involved in extracellular matrix depo-sition during tissue repair,but they are also responsible for synthesising enzymes involved in matrix degrada-tion,tissue remodelling,and scar formation.C.Guyot et al./The International Journal of Biochemistry&Cell Biology38(2006)135–151137Fig.1.(a)Normal liver.Tissue section of a formalin-fixed paraffin-embedded normal human liver(haematoxylin-eosin-saffranin staining)showing a centrolobular vein(CLV),and a portal zone with a portal vein(PV),arteries(A),and bile ducts(BD),surrounded by dense connective tissue containing collagenous extracellular matrix and portalfibroblasts.In the parenchyma,numerous hepatocytes are seen,but the sinusoidal structures are not visible due to tissue treatment.(b)Diagram of a lobule.This schematic diagram shows the three-dimensional structures of the hepatic lobule as revealed by scanning electron microscopy.The central structure in the lobule is the centrolobular vein.Hepatocytic plates radiate out from the centrolobular vein to the perimeter of the lobule;the portal triads(portal vein,hepatic artery,and bile ductule),and the surrounding connective tissue are typically found at the angles of the polygon(for details,see text).CLV,centrolobular vein;K,Kupffer cell;HSC,hepatic stellate cells;HP, hepatocyte plate;SE,sinusoidal endothelium;S,sinusoid;BC,bile canaliculus;A,hepatic artery;CH,canal of Hering;PV,portal vein;BD,bile ductule;LmP,limiting plate.(c)Schematic diagram of the various liverfibroblastic cells able to acquire a myofibroblastic phenotype and involved infibrogenesis.The portalfibroblasts(PF)located in the portal tract connective tissue around bile ducts(BD),portal arteries(A),and portal veins (PV),and the second-layer cells(SLC),fibroblasts located around the smooth muscle cells(SMC)and the endothelium(E)of the centrolobular veins(CLV),can acquire a myofibroblastic phenotype,and these cells do not seem to be able to reacquire a quiescent phenotype;in contrast,the hepatic stellate cells(HSC)containing lipids droplets and located in the Disse space between the hepatocytes(H)and the sinusoidal endothelium (SE)can modulate their myofibroblastic differentiation,and present pericyte-like features suggesting that they function as liver-specific pericytes participating in the regulation of sinusoidal blood pressure.Myofibroblasts(MF)present microfilaments bundles and secrete large amounts of extracellular matrix.138 C.Guyot et al./The International Journal of Biochemistry&Cell Biology38(2006)135–151Myofibroblasts express different sets of cytoskeletalproteins that can be used as markers of cell differ-entiation;the study of their expression allows thecharacterization offibroblastic phenotypic modifica-tions corresponding to functional changes occurringduring physiological and pathological repair(for review,see Desmouli`e re&Gabbiani,1996;Schmitt-Gr¨a ff,Desmouli`e re,&Gabbiani,1994).The cytoskeleton of eukaryotic cells consists of threetypes offilament:(i)intermediatefilaments,whichstrengthen cells against mechanical stress;their compo-sition depends on cell type,(ii)microtubules,which playa crucial role in cell organisation,and direct intracellulartransport,and(iii)actin microfilaments,which deter-mine the shape of the cell surface and are necessary forwhole-cell locomotion.Actin microfilaments are thinandflexible.Six isoforms of actin exist:two cytoplasmicor non-muscle actins(and␥),and four muscle actins(two striated muscle actins,␣-skeletal and␣-cardiac,and two smooth muscle actins,␣and␥).Actinfilamentsassociate with many actin-binding proteins(capping,severing,crosslinking,bundling,nucleating,sequester-ing,or motor proteins),allowing thefilament to performvarious functions.Cytoskeleton components,and actinisoforms in particular,are useful tools for evaluatingphenotypic modifications in response to physiological orpathological situations(Chaponnier&Gabbiani,2004).Fully differentiated myofibroblasts express␣-smoothmuscle actin(Darby,Skalli,&Gabbiani,1990).How-ever,as pointed out by Tomasek et al.(2002),fibroblasticcells may present in some situations morphologicalcharacteristics of myofibroblasts(e.g.,microfilamentbundles of cytoplasmic actins),but they do not express ␣-smooth muscle actin.The term“protomyofibroblasts”has been proposed for these cells(Tomasek et al.,2002).Fibroblasts cultured in the presence of foetal calf serumgenerally display a mixture of protomyofibroblastic andmore differentiated myofibroblastic phenotypes.Thepresence of␣-smooth muscle actin is directly related tothe contractile activity of myofibroblasts.Indeed,it hasrecently been demonstrated,both in vitro and in vivo,that␣-smooth muscle actin levels are directly correlatedwith myofibroblast contraction(Hinz,Celetta,Tomasek,Gabbiani,&Chaponnier,2001a;Hinz,Mastrangelo,Iselin,Chaponnier,&Gabbiani,2001b).Protomyofi-broblasts and myofibroblasts may also produce othersmooth muscle cytoskeletal proteins,including desmin,caldesmon,and smooth muscle-myosin heavy chains(for review,see Desmouli`e re&Gabbiani,1996).Inter-estingly,global expression profiling studies offibroblastresponses to transforming growth factor-1(TGF-1)–a major inducer of myofibroblastic differentiation (Desmouli`e re,Geinoz,Gabbiani,&Gabbiani,1993)–have demonstrated the up-regulation of a number of genes generally expressed by highly differentiated smooth muscle cells.These genes included those encoding smooth muscle-myosin heavy chains,basic calponin,and smoothelin(Chambers,Leoni,Kaminski, Laurent,&Heller,2003).The stimulation of collagen type I and of␣-smooth muscle actin synthesis by TGF-1is strictly dependent on cellularfibronectin, and the ED-A splice variant of this glycoprotein in particular(Serini et al.,1998).Thus,myofibroblast differentiation is a complex process,regulated by at least one cytokine,an extracellular matrix component and mechanical tension(Hinz&Gabbiani,2003).Recent studies taking thesefindings into account have com-pared thefibronexus to a mature or supermature focal contact—a three-dimensional transcellular structure containing thefibronectin isoform ED-A and␣-smooth muscle actin.These structures are organised by forces of intracellular and extracellular origin and are involved in establishment and modulation of the myofibroblastic phenotype(Dugina,Fontao,Chaponnier,Vasiliev,& Gabbiani,2001).It has also been shown that␣-smooth muscle actin is essential for focal adhesion matu-ration in myofibroblasts(Hinz,Dugina,Ballestrem, Wehrle-Haller,&Chaponnier,2003).Myofibroblasts, unlike quiescentfibroblasts,also develop cadherin-type cell–cell adherens junctions,which are instrumental in myofibroblast contractile activity(Hinz,Pittet, Smith-Clerc,Chaponnier,&Meister,2004).Typical myofibroblasts have been found in normal tis-sues in various organs(e.g.,uterine submucosa,intesti-nal pericryptal cells,testicular stroma,periodontal liga-ment;for review,see Sch¨u rch,Seemayer,&Gabbiani, 1998),in which these cells are involved in visceral con-traction and/or organ remodelling.We can identify three groups of pathological situations in which myofibrob-lasts are the predominant cell type:response to injury and repair phenomena(hypertrophic scars and burn contrac-ture,organfibrosis),quasineoplastic proliferative condi-tions(fibromatosis),and stromal response to neoplasia (for review,see Sch¨u rch et al.,1998).3.(Myo)fibroblastic cells involved in liverfibrosis 3.1.The hepatic stellate cellHepatic stellate cells,which account for about 5–8%of cells in the normal liver,are characterised by a perisinusoidal distribution in the Disse space and long processes extending along and around sinusoids, between the hepatocyte plates(Fig.1a and b).ElectronC.Guyot et al./The International Journal of Biochemistry&Cell Biology38(2006)135–151139microscopy has shown that the nucleus-to-nucleus distance between two adjacent hepatic stellate cells is∼40m.Eight to10hepatic stellate cells lie along each sinusoid,between the centrolobular vein and the portal tract.The relationship between hepatic stellate cells and sinusoidal tubes is one of the most important features of these cells.Indeed,the close association of hepatic stellate cells with endothelial cells resembles that of pericytes in capillaries.However,in normal liver, the endothelium is discontinuous and presents multiple fenestrations without diaphragms,allowing the rapid transport of solutes across the subendothelial space.In normal liver,a basal lamina-like substance separates the two cell types but there is no true basement membrane. Cytoplasmic lipid droplets containing Vitamin A are present in most(75%)hepatic stellate cells in normal liver(Bioulac-Sage,Lafon,Le Bail,&Balabaud,1988; Sztark et al.,1986),and hepatic stellate cells constitute the largest cellular reservoir of Vitamin A in the body. Hepatic stellate cells are activated and change phenotype under conditions of stress or injury,often losing their lipid droplets upon activation.The biological markers of these cells also seem to change according to activation level or position within the lobule,making it difficult to use these markers to follow physiological or patho-logical responses.On activation,the hepatic stellate cells acquire a myofibroblastic phenotype(Fig.1c), contributing to the excessive extracellular matrix deposition observed in the pathological conditions of fibrosis and cirrhosis.Capillarisation of the sinusoids also occurs,with a continuous endothelium formed,and the presence of a true basal lamina.The experimental model of carbon tetrachloride (CCl4)treatment in rats has been extensively used to study liverfibrogenesis.It is widely accepted that a toxic metabolite of this molecule causes liver damage,but the identity of this metabolite remains l4treat-ment induces the necrosis of hepatocytes around cen-trolobular veins,and the accumulation of inflammatory cells.Following a single acute treatment,tissue repair occurs,with the appearance of a moderate number of␣-smooth muscle actin-expressing myofibroblastic cells. Following chronic injury,a large number of myofibrob-lastic cells accumulate around centrolobular veins.Septa containing myofibroblastic cells expressing␣-smooth muscle actin then develop between centrolobular areas, and large amounts of extracellular matrix are deposited. It is generally thought that the activated hepatic stellate cells are responsible for this extracellular matrix accu-mulation(for review,see Reeves&Friedman,2002). Hepatic stellate cells have been shown to migrate in vitro (Marra et al.,1999),suggesting that they may migrate to the lesion and take part in the repair process(Kinnman et al.,2000).Lorena et al.(2004)recently reported thatfibrillin-1 and␣-smooth muscle actin were both limited to vessel walls in the normal rat liver.Fibrillin-rich microfibrils are important structural elements abundant in connec-tive tissues.Depending on the location,microfibrils and microfibril-associated glycoproteins may be associated with an amorphous elastin core to form elasticfibres. In contrast to what has been reported for human liver (Dubuisson et al.,2001),in rat liver,fibrillin-1was either absent or present in only very small quantities in the Disse space around the sinusoids.After CCl4treatment, double immunohistochemical staining demonstrated the presence of bothfibrillin-1and␣-smooth muscle actin infibrotic lesions.This suggests that␣-smooth mus-cle actin-positive myofibroblasts are responsible for thefibrillin-1deposition observed duringfibrogenesis. Elastin and␣-smooth muscle actin were co-localised in septa developing after CCl4treatment,but activated␣-smooth muscle actin-positive hepatic stellate cells in the parenchyma did not contain elastin.Thus,in the CCl4 model,at least for the studied time points,the typical acti-vated hepatic stellate cells containing␣-smooth muscle actin seem to play little or no part in elastin deposition. These observations suggest that different liverfibroblast subpopulations are involved in deposition of the different extracellular matrix components and/or that there are dif-ferent subpopulations of hepatic stellate cells.Indeed,it has long been suggested that several subclasses of hep-atic stellate cells are present in the parenchyma(for a recent review,see Friedman,2004).An elegant study in mice transgenic for two reporter genes(two differentflu-orescent protein reporter genes expressed under control of the mouse␣-smooth muscle actin and collagen␣1(I) promoter/enhancers)recently clearly demonstrated in primary cultures of hepatic stellate cells,heterogeneous gene expression in hepatic myofibroblasts(Magness, Bataller,Yang,&Brenner,2004).3.2.The portalfibroblastThe animal model of bile duct proliferation andfibro-sis after ligation of the common bile duct has attracted considerable attention,because it simulates many histological features of human chronic biliaryfibrosis and cirrhosis.Few studies have examined the responses of differentfibrogenic cells and the cellular origin of the extracellular matrix components in this model offibrosis. It has been suggested that the cells involved are hepatic stellate cells reaching the portal region by proliferation and migration(Kinnman et al.,2000,2001).However,140 C.Guyot et al./The International Journal of Biochemistry&Cell Biology38(2006)135–151the involvement of portal tractfibroblasts around biliary structures in the portalfibrosis induced by common bile duct ligation has now been clearly demonstrated,at least for the early stages(Kinnman et al.,2003;Tuchweber et al.,1996).Hepatic stellate cells may become involved later,when the growing portal areas invade the parenchyma(Kinnman&Housset,2002;Tuchweber et al.,1996).Electron micrographs of the portal area in normal rats have demonstrated the presence of portal fibroblasts in the connective tissue around vessels and biliary structures,with a typical appearance of quiescent fibroblasts presenting few cytoplasmic processes.Two days after ligation,manyfibroblasts are observed surrounding proliferating ductules,with a few of these fibroblasts showing microfilament bundles(a feature of myofibroblastic differentiation)in their cytoplasmic processes(Tuchweber et al.,1996).The proliferation of biliary structures induced by common bile duct ligation is accompanied by a proliferation of portalfibroblasts, which form onion-like structures around biliary struc-tures.These portalfibroblasts acquire a myofibroblastic phenotype and are involved in the early deposition of extracellular matrix in the portal zones(Desmouli`e re et al.,1997)(Fig.1c).The portal connective tissue of normal liver contains only quiescentfibroblasts,with no portal myofibroblasts.Portal myofibroblasts appear when a lesion occurs in the portal zone.The bile duct ligation model is characterised by moderate inflam-mation,and the main factors responsible for inducing portal lesions are an increase in biliary pressure(Slott, Liu,&Tavoloni,1990)and probable modifications in bile composition.Cytokines,such as platelet-derived growth factor(Kinnman et al.,2003),and connective tissue growth factor(Sedlaczek et al.,2001)are also involved.Finally,recent studies on animal material and human samples have suggested that mesenchymal cells in the portal tract are of crucial importance in the development of liverfibrosis and cirrhosis(for review, see Ramadori&Saile,2004a).Transmission electron microscopy of normal human liver has demonstrated the presence of numerousfibroblastic cells in the portal tracts,constituting a major reservoir offibrogenic cells (Fig.2).3.3.Otherfibrogenic cellsSecond-layer cells located around centrolobular veins and described by Bhunchet and Wake(1992)(Fig.1c),fibroblasts present in the Glisson capsule surrounding the liver,and vascular smooth muscle cells may also be involved infibrogenesis,probably by modulation to myofibroblasticcells.Fig. 2.Normal human liver(transmission electron microscopy). Around the biliary epithelial cells of a bile duct(BD),numerous por-talfibroblasts(arrows)are observed.These cells(portalfibroblasts), together with hepatic stellate cells,represent a reservoir offibroblastic cells potentially involved infibrogenesis.After portal tract injury,por-talfibroblasts can proliferate and acquire a myofibroblastic phenotype.Beside very commonly used experimental models such as CCl4treatment and bile duct ligation,fibrosis can also be induced by the intraperitoneal injection of pig serum in rats(Bhunchet&Wake,1992;Rubin,Hutterer, &Popper,1968).These pig serum-sensitised animals accumulate extracellular matrix in the centrolobular and periportal zones and no necrotic hepatocytes or acute inflammatory reactions are observed.Prominentfibrotic septa are observed,extending out in a radial pattern from central veins and portal zones,resulting in the forma-tion of pseudolobules.However,thefibroblastic cells involved and the mechanisms leading to hepaticfibro-sis in this model are unknown.The vascular smooth muscle cells residing in the wall of portal vein branches and portal arteries have been implicated in the typical portal/periportalfibrosis observed in chronic schistoso-miasis(Andrade,Guerret,&Fernandes,1999).In addition,myofibroblasts are a major component in the stroma reaction,which develops in hepatocel-lular carcinoma(for review,see Desmouli`e re,Guyot, &Gabbiani,2004).In this cancer,they are involved in the synthesis of stromal extracellular matrix com-ponents,extracellular matrix-degrading proteinases,and pro-invasive factors,including hepatocyte growth factor.A number of experimental models have been developed but the origin of the(myo)fibroblastic cells involved in the stroma reaction observed in hepatocellular car-cinoma remains unclear.Progenitorfibroblastic cells have never been detected in the liver.In contrast,in the dermis,progenitor cellsC.Guyot et al./The International Journal of Biochemistry&Cell Biology38(2006)135–151141located in the dermal sheath surrounding the hair fol-licle have been shown to maintain and regenerate the dermal papilla and to play an important role in repair-ing the dermis after injury(Jahoda&Reynolds,2001). It is thought that the canals of Hering,which have been demonstrated to proliferate in disease states,may har-bour liver stem cells(Fausto&Campbell,2003;Theise et al.,1999).This suggests that the canals of Hering and the surrounding stromal cells may constitute a niche for hepatic stem cells(Saxena&Theise,2004).The canals of Hering have a highly strategic distribution(Fig.1b): they begin in the lobules,are lined partly by bile duct epithelial cells and partly by hepatocytes,and conduct bile from the bile canaliculi to terminal bile ducts in the portal tracts(Roskams et al.,2004).The production of large numbers of(myo)fibroblasts by local epithelial-mesenchymal transition has been reported during renal fibrogenesis(for review,see Kalluri&Neilson,2003). Further studies are required to confirm this process in the kidney but no equivalent mechanism has ever been observed in the liver.In addition tofibrogenic cells resident in the liver, circulating cells may play an essential role infibroge-nesis.An analysis of the tissues of humans receiving sex-mismatched organ or bone marrow transplants iden-tified bone marrow-derived myofibroblasts participating infibrogenic reactions in the liver(Forbes et al.,2004). Evidence has also been obtained that circulating pre-cursor cells migrate into wounds and contribute to the (myo)fibroblastic population of the repair tissue(Abe, Donnelly,Peng,Bucala,&Metz,2001).Indeed,Bucala, Spiegel,Chesney,Hogan,and Cerami(1994)identified a novel blood-borne cell subpopulation withfibroblast-like properties,which they referred to asfibrocytes(for review,see Quan,Cowper,Wu,Bockenstedt,&Bucala, 2004).Peripheral bloodfibrocytes may rapidly enter the injury site at the same time as circulating inflammatory cells.For example,it has been suggested that circulating fibrocytes represent a major source offibroblasts during the healing of extensive burn wounds,in which it may be difficult forfibroblasts to migrate from the edges of the injury(Yang et al.,2002).However,although this process seems very likely,no role forfibrocytes in the develop-ment of liverfibrosis has yet been definitively demon-strated.In conclusion,all these processes(the involve-ment offibrocytes,a process of epithelial-mesenchymal transdifferentiation,or the presence of liver progenitor fibroblastic cells)may represent alternative sources of (myo)fibroblasts,and could be involved in specific situ-ations,particularly when the size of the lesion increases, and when recruitment of the localfibroblasts is unable to“comply with the request”.3.4.General considerationsThe data now available suggest that there is a need to reconsider the role of hepatic stellate cells in the devel-opment of liverfibrosis.The pericyte-like characteristics of hepatic stellate cells,including their close relationship with endothelial cells and their expression of smooth muscle markers,have been discussed extensively in pre-vious publications(Blomhoff&Wake,1991;Pinzani, 1995).Hepatic stellate cells are probably“resting peri-cytes”that may be rapidly activated(e.g.,in response to changes in blood pressure),acquiring contractile prop-erties enabling them to regulate local blood pressure. Hepatic stellate cells have been shown to be activated early in transplantation,as demonstrated by the acute, transient production of␣-smooth muscle actin(Rubbia-Brandt et al.,1997).Moreover,ex vivo liver perfusion induces:(1)the early activation of hepatic stellate cells, which begin to produce␣-smooth muscle actin and(2) significant changes in the perisinusoidal extracellular matrix(Costa et al.,2001).Thesefindings are consis-tent with the view that hepatic stellate cells function as liver-specific pericytes,participating in the regulation of sinusoidal blood pressure.Several groups have shown that activated hepatic stel-late cells can revert to quiescence(Gaca et al.,2003; Sohara,Znoyko,Levy,Trojanowska,&Reuben,2002), suggesting that hepatic stellate cells have a plastic phe-notype.The role played by the extracellular matrix envi-ronment has been highlighted,and it has been shown that a basement membrane-like matrix induces the deac-tivation of hepatic stellate cells(Gaca et al.,2003).It has also clearly been demonstrated that the stiffness of the surrounding environment determines the phenotype of hepatic stellate cell(Wells,2005).Many studies have shown that activated hepatic stellate cells proliferate(for review,see Friedman,2000).Portal(myo)fibroblasts can also undergo several subcultures.It has been suggested that pure populations of hepatic stellate cells do not pro-liferate(Knittel et al.,1999b;Ramadori&Saile,2004a; personal observations),but further studies are required to confirm this.Rat liver myofibroblasts and hepatic stellate cells differ in CD95-mediated apoptosis and response to tumour necrosis factor-␣(Saile et al.,2002).Insulin-like growth factor-1induces DNA synthesis and apoptosis in rat liver hepatic stellate cells but DNA synthesis and pro-liferation in rat liver myofibroblasts(Saile et al.,2004). It has been suggested that liverfibroblastic cells other than typical hepatic stellate cells(e.g.,portalfibroblasts) may have been analysed in studies of hepatic stellate cells after several passages,and this interpretation has clearly been accepted by the authors of several recent。