尼达尼布乙磺酸盐(Nintedanib esylate,BIBF1120 esylate)-HPLC-Biochempartner
尼达尼布乙磺酸盐的合成

尼达尼布乙磺酸盐的合成
尼达尼布乙磺酸盐的合成方法如下:
1. 在反应溶剂中加入1-乙酰基-3-甲氧基(苯基)亚甲基-2-氧代二氢吲哚-6-甲酸甲酯(化合物A)与N-(4-氨基苯基)-N,4-二甲基-1-哌嗪乙酰胺(化合物B),反应结束后加入吡咯烷,析晶,用混合溶剂搅洗,干燥,生成(3Z)-3-(4-甲基-(4-甲基哌嗪-1-基)乙酰基氨基)苯基)氨基-(苯基)亚甲基-2-氧代-2,3-二氢吲哚-6-甲酸甲酯(化合物C)。
2. 化合物C与乙磺酸反应,析晶,过滤干燥,即可得到尼达尼布乙磺酸盐。
请注意,在进行化学合成时,应遵守安全操作规程,并使用适当的防护设备。
建议在专业化学实验室中进行合成,以确保安全和合规。
尼达尼布作用靶点

尼达尼布作用靶点
尼达尼布(Nedanib)是一种口服治疗肺癌的靶向药物,属于多酰胺酶抑制剂。
它作用于特定的信号通路,控制肿瘤细胞的生长和分裂,从而达到抑制癌症的效果。
尼达尼布的作用靶点主要包括以下几个步骤:
1.抑制EGFR基因突变。
EGFR基因突变是引起大部分肺癌的原因之一,在这种情况下肿瘤细胞会不受控制地生长和分裂,从而形成肿瘤。
尼达尼布可以抑制EGFR基因突变,从而控制肿瘤的生长和扩散。
它能针对多种EGFR突变,包括L858R、19del和21L858等等。
2.抑制ALKE突变。
ALKE基因突变也是引起肺癌的一种原因,尼达尼布能够抑制它的活性,控制肿瘤的生长和分裂。
3.抑制ROS1突变。
ROS1突变也是引起肺癌的一种原因,尼达尼布能够抑制其活性,控制肿瘤的生长和分裂。
4.抑制VEGFR、PDGR等活性。
VEGFR和PDGR是肿瘤血管生长的重要因素,尼达尼布能够抑制它们的活性,从而控制肿瘤血管的生长和扩散,降低肿瘤生长的速度。
5.抑制RAS-MAPK通路。
RAS-MAPK通路是多种肿瘤细胞的生长和分裂的信号通路,尼达尼布能够抑制这一通路的活性,从而控制肿瘤的生长和扩散。
总之,尼达尼布作为口服肺癌靶向药物,其作用靶点非常广泛,包括EGFR、ALKE、ROS1、VEGFR、PDGR和RAS-MAPK等信号通路,从而有效地控制了肿瘤的生长和扩散。
在使用尼达尼布治疗肺癌时,需要注意遵医嘱,采取正确的剂量和方法,以便获得最佳的治疗效果。
乙磺酸尼达尼布软胶囊详细说明书与重点

乙磺酸尼达尼布软胶囊英文名:Nintedanib esilate soft capsules汉语拼音:Yi Huang Suan Ni Da Ni Bu Ruan Jiao Nang【成份】本品主要成份为:乙磺酸尼达尼布,化学名称:1H-吲哚-6-羧酸,2,3-二氢-3-[[[4-[甲基[(4-甲基-1-哌嗪基)乙酰基]氨基]苯基]氨基]苯基亚甲基]-2-氧-,甲酯,(3Z)-,乙磺酸盐(1:1),化学结构式:分子式:C31H33N5O4·C2H6O3S或C33H39N5O7S,分子量:649.76g/mol(乙磺酸盐),539.62g/mol(游离碱)【性状】本品为淡粉棕色(100mg规格)或棕色(150mg规格)不透明的椭圆形软胶囊,内容物为亮黄色黏稠混悬液。
【适应症】本品用于治疗特发性肺纤维化(IPF)。
用于系统性硬化病相关间质性肺疾病(SSc-ILD)的药物。
【规格】按C31H33N5O4计算(1)100mg(2)150 mg。
【用法用量】应该由具有诊断和治疗IPF经验的医师启动本品的治疗。
本品推荐剂量为每次150mg,每日两次,给药间隔大约为12小时。
根据患者耐受程度可降低剂量至100mg,每日两次,治疗开始前及给药过程中需定期检查肝功能,一旦出现肝功能异常,应降低剂量或停药(参见【注意事项】、【不良反应】)。
本品应与食物同服,用水送服整粒胶囊。
本品有苦味,不得咀嚼或碾碎服用。
尚不清楚咀嚼或碾碎胶囊对尼达尼布药代动力学的影响。
如果漏服了一个剂量的药物,应在下一计划服药时间继续服用推荐剂量的药物,不应补服漏服的剂量。
不应超过推荐的每日最大剂量300mg。
剂量调整:如可适用,除了对症治疗以外,本品的不良反应处理(参见【注意事项】、【不良反应】)可包括降低剂量和暂时中断给药直至特定不良反应缓解至允许继续治疗的水平。
可采用完整剂量(每次150mg,每日两次)或降低的剂量(每次100mg,每日两次)重新开始本品治疗。
尼达尼布(Ofev,Nintedanib) FDA 官方说明书
尼达尼布(Ofev,Nintedanib) FDA官方说明书1 适应证和用途OFEV是适用为特发性肺纤维化(IPF)的治疗。
2 剂量和给药方法2.1 OFEV给予前检验用OFEV开始治疗前进行肝功能检验[见警告和注意事项(5.1)]。
2.2 推荐剂量OFEV的推荐剂量是150 mg每天2次给予间隔约12小时。
OFEV胶囊应与食物服用[见临床药理学(12.3)]和用液体整吞。
因为苦味不应咀嚼或压碎OFEV 胶囊。
不知道胶囊被咀嚼或压碎对nintedanib药代动力学的影响。
如丢失一剂OFEV,应在下一次时间表服用下一剂。
劝告患者不要弥补丢失剂量。
不要超过推荐的最大每天剂量300 mg。
2.3 由于不良反应剂量调整除了对症治疗,如适用,OFEV不良反应的处理可能需要减低剂量或暂时中断直至特异性不良反应解决至允许继续治疗的水平。
OFEV治疗可在完全剂量恢复(150 mg每天2次),或在减低剂量(100 mg每天2次),随后可增加至完整剂量。
如一例患者不能耐受100 mg每天2次,终止用OFEV 治疗[见警告和注意事项(5.1,5.2,5.4,5.6)和不良反应(6.1)]。
对肝酶升高可能需要剂量调整或中断。
对天门冬氨酸氨基转移酶(AST)或丙氨酸氨基转移酶(ALT)正常上限(ULN) >3倍至<5倍无严重肝损伤征象,中断治疗或减低OFEV至100 mg每天2次。
一旦肝酶已恢复至基线值,可能在减低剂量(100 mg每天2次)再次引人用OFEV治疗,随后可增加至完整剂量(150 mg每天2次)[见警告和注意事项(5.1)和不良反应(6.1)]。
对AST或ALT升高ULN >5 倍或>3倍ULN与严重肝损伤特征或症状终止OFEV。
3 剂型和规格150 mg胶囊:棕色,不透明,椭圆形,软胶囊印有黑色勃林格殷格翰公司标志和"150"。
100 mg胶囊:桃色,不透明,椭圆形,软胶囊印有黑色勃林格殷格翰公司标志和"100"。
尼达尼布作用机制
尼达尼布作用机制
尼达尼布(Nebivolol)是一种治疗高血压的药物。
它属于β受
体阻滞剂药物的一种,在治疗高血压的过程中,能有效地缓解心脏负荷,减少血液循环阻力,降低血压,从而保护心血管系统的健康。
尼达尼布与其他β受体阻滞剂药物不同的是,它具有刺激一类
β受体的作用。
这类受体能够促使血管扩张,从而使血流更加顺畅,
并且能够减少心脏压力。
尼达尼布的作用主要通过以下几个方面得以
体现:
第一,尼达尼布能够通过作用于肺小动脉和肺毛细血管内皮细胞
的一类受体,刺激血管内皮细胞生成一种重要的信号分子一氧化氮(NO),从而促使血管扩张,增加血流量,从而降低血压。
第二,尼达尼布还可作用于心肌细胞的一类β1受体,通过阻滞
这类受体,降低心率,使心脏更加节约地工作,从而减少心脏耗氧量,预防心脏病的发生。
第三,尼达尼布还能通过抑制另一种β受体β2受体,减少交感
神经的刺激,改善自主神经系统稳定性,降低血压和减少心率,保护
心血管系统的健康。
总之,尼达尼布是一种高效的降压药物,其作用主要通过刺激血
管扩张、降低心率等多种机制来实现。
在使用过程中,需要严格遵守
医嘱,注意检查治疗效果和不良反应,从而达到优化治疗效果,保护心血管系统健康的目的。
尼达尼布胶囊全处方说明书
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use OFEV safely and effectively. See full prescribing information for OFEV.OFEV® (nintedanib) capsules, for oral useInitial U.S. Approval: 2014----------------------------INDICATIONS AND USAGE--------------------------- OFEV is a kinase inhibitor indicated for the treatment of idiopathic pulmonary fibrosis (IPF). (1)----------------------DOSAGE AND ADMINISTRATION----------------------- ∙Recommended dosage: 150 mg twice daily approximately 12 hours apart taken with food. (2.2)∙Consider temporary dose reduction to 100 mg, treatment interruption, or discontinuation for management of adverse reactions. (2.3, 5.1, 5.2, 6)∙Prior to treatment, conduct liver function tests. (2.1, 5.1)---------------------DOSAGE FORMS AND STRENGTHS---------------------- Capsules: 150 mg and 100 mg (3)-------------------------------CONTRAINDICATIONS------------------------------ None-----------------------WARNINGS AND PRECAUTIONS------------------------ ∙Elevated liver enzymes: ALT, AST, and bilirubin elevations have occurred with OFEV. Monitor ALT, AST, and bilirubin before and during treatment.Temporary dosage reductions or discontinuations may be required. (2.1,5.1)∙Gastrointestinal disorders: Diarrhea, nausea, and vomiting have occurred with OFEV. Treat patients at first signs with adequate hydration andantidiarrheal medicine (e.g., loperamide) or anti-emetics. DiscontinueOFEV if severe diarrhea, nausea, or vomiting persists despite symptomatic treatment. (5.2)∙Embryofetal toxicity: Women of childbearing potential should be advised of the potential hazard to the fetus and to avoid becoming pregnant. (5.3) ∙Arterial thromboembolic events have been reported. Use caution when treating patients at higher cardiovascular risk including known coronary artery disease. (5.4) ∙Bleeding events have been reported. Use OFEV in patients with known bleeding risk only if anticipated benefit outweighs the potential risk. (5.5)∙Gastrointestinal perforation has been reported. Use OFEV with caution when treating patients with recent abdominal surgery. Discontinue OFEVin patients who develop gastrointestinal perforation. Only use OFEV inpatients with known risk of gastrointestinal perforation if the anticipatedbenefit outweighs the potential risk. (5.6)------------------------------ADVERSE REACTIONS------------------------------- Most common adverse reactions (≥5%) are: diarrhea, nausea, abdominal pain, vomiting, liver enzyme elevation, decreased appetite, headache, weight decreased, and hypertension. (6.1)To report SUSPECTED ADVERSE REACTIONS, contact Boehringer Ingelheim Pharmaceuticals, Inc. at (800) 542-6257 or (800) 459-9906 TTYor FDA at 1-800-FDA-1088 or /medwatch.-------------------------------DRUG INTERACTIONS------------------------------∙Coadministration of P-gp and CYP3A4 inhibitors may increase nintedanib exposure. Monitor patients closely for tolerability of OFEV. (7.1)-----------------------USE IN SPECIFIC POPULATIONS------------------------∙Nursing mothers: Discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother. (8.3)∙Hepatic impairment: Monitor for adverse reactions and consider dose modification or discontinuation of OFEV as needed for patients with mildhepatic impairment. OFEV is not recommended for use in patients withmoderate or severe hepatic impairment. (8.6, 12.3)∙Renal impairment: The safety and efficacy of OFEV have not been studied in patients with severe renal impairment and end-stage renal disease. (8.7,12.3)∙Smokers: Decreased exposure has been noted in smokers which may alter the efficacy profile of OFEV. (8.8)See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.Revised:10/2014_______________________________________________________________________________________________________________________________________FULL PRESCRIBING INFORMATION: CONTENTS*1INDICATIONS AND USAGE2DOSAGE AND ADMINISTRATION2.1Testing Prior to OFEV Administration2.2Recommended Dosage2.3Dosage Modification due to Adverse Reactions3DOSAGE FORMS AND STRENGTHS4CONTRAINDICATIONS5WARNINGS AND PRECAUTIONS5.1Elevated Liver Enzymes5.2Gastrointestinal Disorders5.3Embryofetal Toxicity5.4Arterial Thromboembolic Events5.5Risk of Bleeding5.6Gastrointestinal Perforation6ADVERSE REACTIONS6.1Clinical Trials Experience7DRUG INTERACTIONS7.1P-glycoprotein (P-gp) and CYP3A4 Inhibitors and Inducers7.2Anticoagulants8USE IN SPECIFIC POPULATIONS8.1Pregnancy8.3Nursing Mothers8.4Pediatric Use8.5Geriatric Use8.6Hepatic Impairment8.7Renal Impairment8.8Smokers10OVERDOSAGE11DESCRIPTION12CLINICAL PHARMACOLOGY12.1Mechanism of Action12.2Pharmacodynamics12.3Pharmacokinetics13NONCLINICAL TOXICOLOGY13.1Carcinogenesis, Mutagenesis, Impairment of Fertility14CLINICAL STUDIES16HOW SUPPLIED/STORAGE AND HANDLING17PATIENT COUNSELING INFORMATION*Sections or subsections omitted from the full prescribing information are not listed._______________________________________________________________________________________________________________________________________FULL PRESCRIBING INFORMATIONANDUSAGE1 INDICATIONSOFEV is indicated for the treatment of idiopathic pulmonary fibrosis (IPF).2 DOSAGE AND ADMINISTRATION2.1 Testing Prior to OFEV AdministrationConduct liver function tests prior to initiating treatment with OFEV [see Warnings and Precautions (5.1)].2.2 Recommended DosageThe recommended dosage of OFEV is 150 mg twice daily administered approximately 12 hours apart.OFEV capsules should be taken with food [see Clinical Pharmacology (12.3)] and swallowed whole with liquid. OFEV capsules should not be chewed or crushed because of a bitter taste. The effect of chewing or crushing of the capsule on the pharmacokinetics of nintedanib is not known.If a dose of OFEV is missed, the next dose should be taken at the next scheduled time. Advise the patient to not make up for a missed dose. Do not exceed the recommended maximum daily dosage of 300 mg.2.3 Dosage Modification due to Adverse ReactionsIn addition to symptomatic treatment, if applicable, the management of adverse reactions of OFEV may require dose reduction or temporary interruption until the specific adverse reaction resolves to levels that allow continuation of therapy. OFEV treatment may be resumed at the full dosage (150 mg twice daily), or at the reduced dosage (100 mg twice daily), which subsequently may be increased to the full dosage. If a patient does not tolerate 100 mg twice daily, discontinue treatment with OFEV [see Warnings and Precautions (5.1, 5.2, 5.4, 5.6) and Adverse Reactions (6.1)].Dose modifications or interruptions may be necessary for liver enzyme elevations. For aspartate aminotransferase (AST) or alanine aminotransferase (ALT) >3 times to <5 times the upper limit of normal (ULN) without signs of severe liver damage, interrupt treatment or reduce OFEV to 100 mg twice daily. Once liver enzymes have returned to baseline values, treatment with OFEV may be reintroduced at a reduced dosage (100 mg twice daily), which subsequently may be increased to the full dosage (150 mg twice daily) [see Warnings and Precautions (5.1) and Adverse Reactions (6.1)]. Discontinue OFEV for AST or ALT elevations >5 times ULN or >3 times ULN with signs or symptoms of severe liver damage.3 DOSAGE FORMS AND STRENGTHS150 mg capsules: brown, opaque, oblong, soft capsules imprinted in black with the Boehringer Ingelheim company symbol and "150".100 mg capsules: peach, opaque, oblong, soft capsules imprinted in black with the Boehringer Ingelheim company symbol and "100".4 CONTRAINDICATIONSNonePRECAUTIONSAND5 WARNINGS5.1 Elevated Liver EnzymesThe safety and efficacy of OFEV has not been studied in patients with moderate (Child Pugh B) or severe (Child Pugh C) hepatic impairment. Treatment with OFEV is not recommended in patients with moderate or severe hepatic impairment [see Use in Specific Populations (8.6) and Clinical Pharmacology (12.3)].In clinical trials, administration of OFEV was associated with elevations of liver enzymes (ALT, AST, ALKP, GGT). Liver enzyme increases were reversible with dose modification or interruption and not associated with clinical signs or symptoms of liver injury. The majority (94%) of patients with ALT and/or AST elevations had elevations <5 times ULN. Administration of OFEV was also associated with elevations of bilirubin. The majority (95%) of patients with bilirubin elevations had elevations <2 times ULN [see Use in Specific Populations (8.6) and Clinical Pharmacology (12.3)].Conduct liver function tests (ALT, AST, and bilirubin) prior to treatment with OFEV, monthly for 3 months, and every 3 months thereafter, and as clinically indicated. Dosage modifications or interruption may be necessary for liver enzyme elevations [see Dosage and Administration (2.1, 2.3)].5.2 Gastrointestinal DisordersDiarrheaDiarrhea was the most frequent gastrointestinal event reported in 62% versus 18% of patients treated with OFEV and placebo, respectively [see Adverse Reactions (6.1)]. In most patients, the event was of mild to moderate intensity and occurred within the first 3 months of treatment. Diarrhea led to permanent dose reduction in 11% of patients treated with OFEV compared to 0 placebo-treated patients. Diarrhea led to discontinuation of OFEV in 5% of the patients compared to <1% of placebo-treated patients.Dosage modifications or treatment interruptions may be necessary in patients with adverse reactions of diarrhea. Treat diarrhea at first signs with adequate hydration and antidiarrheal medication (e.g., loperamide), and consider treatment interruption if diarrhea continues [see Dosage and Administration (2.3)]. OFEV treatment may be resumed at the full dosage (150 mg twice daily), or at the reduced dosage (100 mg twice daily), which subsequently may be increased to the full dosage. If severe diarrhea persists despite symptomatic treatment, discontinue treatment with OFEV.Nausea and VomitingNausea was reported in 24% versus 7% and vomiting was reported in 12% versus 3% of patients treated with OFEV and placebo, respectively [see Adverse Reactions (6.1)]. In most patients, these events were of mild to moderate intensity. Nausea led to discontinuation of OFEV in 2% of patients. Vomiting led to discontinuation of OFEV in 1% of the patients.For nausea or vomiting that persists despite appropriate supportive care including anti-emetic therapy, dose reduction or treatment interruption may be required [see Dosage and Administration (2.3)]. OFEV treatment may be resumed at the full dosage (150 mg twice daily), or at the reduced dosage (100 mg twice daily), which subsequently may be increased to the full dosage. If severe nausea or vomiting does not resolve, discontinue treatment with OFEV.5.3 Embryofetal ToxicityOFEV can cause fetal harm when administered to a pregnant woman. Nintedanib was teratogenic and embryofetocidal in rats and rabbits at less than and approximately 5 times the maximum recommended human dose (MRHD) in adults (on an AUC basis at oral doses of 2.5 and 15 mg/kg/day in rats and rabbits, respectively). If OFEV is used during pregnancy, or if the patient becomes pregnant while taking OFEV, the patient should be advised of the potential hazard to a fetus. Women of childbearing potential should be advisedto avoid becoming pregnant while receiving treatment with OFEV and to use adequate contraception during treatment and at least 3 months after the last dose of OFEV [see Use in Specific Populations (8.1)].5.4 Arterial Thromboembolic EventsArterial thromboembolic events have been reported in patients taking OFEV. In clinical trials, arterial thromboembolic events were reported in 2.5% of patients treated with OFEV and 0.8% of placebo-treated patients. Myocardial infarction was the most common adverse reaction under arterial thromboembolic events, occurring in 1.5% of OFEV-treated patients compared to 0.4% of placebo-treated patients.Use caution when treating patients at higher cardiovascular risk including known coronary artery disease. Consider treatment interruption in patients who develop signs or symptoms of acute myocardial ischemia.5.5 Risk of BleedingBased on the mechanism of action (VEGFR inhibition), OFEV may increase the risk of bleeding. In clinical trials, bleeding events were reported in 10% of patients treated with OFEV and in 7% of patients treated with placebo.Use OFEV in patients with known risk of bleeding only if the anticipated benefit outweighs the potential risk.5.6 Gastrointestinal PerforationBased on the mechanism of action, OFEV may increase the risk of gastrointestinal perforation. In clinical trials, gastrointestinal perforation was reported in 0.3% of patients treated with OFEV, compared to 0 cases in the placebo-treated patients.Use caution when treating patients who have had recent abdominal surgery. Discontinue therapy with OFEV in patients who develop gastrointestinal perforation. Only use OFEV in patients with known risk of gastrointestinal perforation if the anticipated benefit outweighs the potential risk.REACTIONS6 ADVERSEThe following adverse reactions are discussed in greater detail in other sections of the labeling:∙Liver Enzyme and Bilirubin Elevations [see Warnings and Precautions (5.1)]∙Gastrointestinal Disorders [see Warnings and Precautions (5.2)]∙Embryofetal Toxicity [see Warnings and Precautions (5.3)]∙Arterial Thromboembolic Events [see Warnings and Precautions (5.4)]∙Risk of Bleeding [see Warnings and Precautions (5.5)]∙Gastrointestinal Perforation [see Warnings and Precautions (5.6)]6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.The safety of OFEV was evaluated in over 1000 IPF patients with over 200 patients exposed to OFEV for more than 2 years in clinical trials.OFEV was studied in three randomized, double-blind, placebo-controlled, 52-week trials. In the phase 2 (Study 1) and phase 3 (Studies 2 and 3) trials, 723 patients with IPF received OFEV 150 mg twice daily and 508 patients received placebo. The median duration of exposure was 10 months for patients treated with OFEV and11 months for patients treated with placebo. Subjects ranged in age from 42 to 89 years (median age of 67 years). Most patients were male (79%) and Caucasian (60%).The most frequent serious adverse reactions reported in patients treated with OFEV, more than placebo, were bronchitis (1.2% vs. 0.8%) and myocardial infarction (1.5% vs. 0.4%). The most common adverse events leading to death in patients treated with OFEV, more than placebo, were pneumonia (0.7% vs. 0.6%), lung neoplasm malignant (0.3% vs. 0%), and myocardial infarction (0.3% vs. 0.2%). In the predefined category of major adverse cardiovascular events (MACE) including MI, fatal events were reported in 0.6% of OFEV-treated patients and 1.8% of placebo-treated patients.Adverse reactions leading to permanent dose reductions were reported in 16% of OFEV-treated patients and 1% of placebo-treated patients. The most frequent adverse reaction that led to permanent dose reduction in the patients treated with OFEV was diarrhea (11%).Adverse reactions leading to discontinuation were reported in 21% of OFEV-treated patients and 15% of placebo-treated patients. The most frequent adverse reactions that led to discontinuation in OFEV-treated patients were diarrhea (5%), nausea (2%), and decreased appetite (2%).The most common adverse reactions with an incidence of ≥5% and more frequent in the OFEV than placebo treatment group are listed in Table 1.Table 1 Adverse Reactions Occurring in ≥5% of OFEV-treated Patients and More Commonly Than Placebo in Studies 1, 2, and 3Adverse Reaction OFEV, 150 mgn=723 Placebo n=508Gastrointestinal disordersDiarrhea 62% 18%Nausea 24% 7%Abdominal pain a 15% 6%Vomiting 12% 3%Hepatobiliary disordersLiver enzyme elevation b 14% 3% Metabolism and nutrition disordersDecreased appetite 11% 5%Nervous systemic disordersHeadache 8% 5%InvestigationsWeight decreased 10% 3%Vascular disordersHypertension c 5% 4%a Includes abdominal pain, abdominal pain upper, abdominal pain lower, gastrointestinal pain and abdominal tenderness.b Includes gamma-glutamyltransferase increased, hepatic enzyme increased, alanine aminotransferase increased, aspartateaminotransferase increased, hepatic function abnormal, liver function test abnormal, transaminase increased, blood alkalinephosphatase-increased, alanine aminotransferase abnormal, aspartate aminotransferase abnormal, and gamma-glutamyltransferaseabnormal.c Includes hypertension, blood pressure increased, hypertensive crisis, and hypertensive cardiomyopathy.In addition, hypothyroidism was reported in patients treated with OFEV, more than placebo (1.1% vs. 0.6%).7 DRUGINTERACTIONS7.1 P-glycoprotein (P-gp) and CYP3A4 Inhibitors and InducersNintedanib is a substrate of P-gp and, to a minor extent, CYP3A4 [see Clinical Pharmacology (12.3)]. Coadministration with oral doses of a P-gp and CYP3A4 inhibitor, ketoconazole, increased exposure to nintedanib by 60%. Concomitant use of P-gp and CYP3A4 inhibitors (e.g., erythromycin) with OFEV may increase exposure to nintedanib [see Clinical Pharmacology (12.3)]. In such cases, patients should be monitored closely for tolerability of OFEV. Management of adverse reactions may require interruption, dose reduction, or discontinuation of therapy with OFEV [see Dosage and Administration (2.3)].Coadministration with oral doses of a P-gp and CYP3A4 inducer, rifampicin, decreased exposure to nintedanib by 50%. Concomitant use of P-gp and CYP3A4 inducers (e.g., carbamazepine, phenytoin, and St. John’s wort) with OFEV should be avoided as these drugs may decrease exposure to nintedanib [see Clinical Pharmacology (12.3)].7.2 AnticoagulantsNintedanib is a VEGFR inhibitor, and may increase the risk of bleeding. Monitor patients on full anticoagulation therapy closely for bleeding and adjust anticoagulation treatment as necessary [see Warnings and Precautions (5.5)].8 USE IN SPECIFIC POPULATIONS8.1 PregnancyPregnancy Category D. [See Warnings and Precautions (5.3)]OFEV can cause fetal harm when administered to a pregnant woman. If OFEV is used during pregnancy, or if the patient becomes pregnant while taking OFEV, the patient should be apprised of the potential hazard to a fetus. Women of childbearing potential should be advised to avoid becoming pregnant while receiving treatment with OFEV.In animal reproduction toxicity studies, nintedanib caused embryofetal deaths and teratogenic effects in rats and rabbits at less than and approximately 5 times the maximum recommended human dose (MRHD) in adults (on a plasma AUC basis at maternal oral doses of 2.5 and 15 mg/kg/day in rats and rabbits, respectively). Malformations included abnormalities in the vasculature, urogenital, and skeletal systems. Vasculature anomalies included missing or additional major blood vessels. Skeletal anomalies included abnormalities in the thoracic, lumbar, and caudal vertebrae (e.g., hemivertebra, missing, or asymmetrically ossified), ribs (bifid or fused), and sternebrae (fused, split, or unilaterally ossified). In some fetuses, organs in the urogenital system were missing. In rabbits, a significant change in sex ratio was observed in fetuses (female:male ratio of approximately 71%:29%) at approximately 15 times the MRHD in adults (on an AUC basis at a maternal oral dose of 60 mg/kg/day). Nintedanib decreased post-natal viability of rat pups during the first 4 post-natal days when dams were exposed to less than the MRHD (on an AUC basis at a maternal oral dose of 10 mg/kg/day).8.3 Nursing MothersNintedanib and/or its metabolites are excreted into the milk of lactating rats. Milk and plasma of lactating rats have similar concentrations of nintedanib and its metabolites. Excretion of nintedanib and/or its metabolites into human milk is probable. There are no human studies that have investigated the effects of OFEV on breast-fed infants. Because of the potential for serious adverse reactions in nursing infants from OFEV, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.8.4 Pediatric UseSafety and effectiveness in pediatric patients have not been established.8.5 Geriatric UseOf the total number of subjects in phase 2 and 3 clinical studies of OFEV, 60.8% were 65 and over, while 16.3% were 75 and over. In phase 3 studies, no overall differences in effectiveness were observed between subjects who were 65 and over and younger subjects; no overall differences in safety were observed between subjects who were 65 and over or 75 and over and younger subjects, but greater sensitivity of some older individuals cannot be ruled out.8.6 Hepatic ImpairmentNintedanib is predominantly eliminated via biliary/fecal excretion (>90%) [see Clinical Pharmacology (12.3)]. No dedicated pharmacokinetic (PK) study was performed in patients with hepatic impairment. Monitor for adverse reactions and consider dose modification or discontinuation of OFEV as needed for patients with mild hepatic impairment (Child Pugh A). The safety and efficacy of nintedanib has not been investigated in patients with hepatic impairment classified as Child Pugh B or C. Therefore, treatment of patients with moderate (Child Pugh B) and severe (Child Pugh C) hepatic impairment with OFEV is not recommended [see Warnings and Precautions (5.1)].8.7 Renal ImpairmentBased on a single-dose study, less than 1% of the total dose of nintedanib is excreted via the kidney [see Clinical Pharmacology (12.3)]. Adjustment of the starting dose in patients with mild to moderate renal impairment is not required. The safety, efficacy, and pharmacokinetics of nintedanib have not been studied in patients with severe renal impairment (<30 mL/min CrCl) and end-stage renal disease.8.8 SmokersSmoking was associated with decreased exposure to OFEV [see Clinical Pharmacology (12.3)], which may alter the efficacy profile of OFEV. Encourage patients to stop smoking prior to treatment with OFEV and to avoid smoking when using OFEV.10 OVERDOSAGEIn the trials, one patient was inadvertently exposed to a dose of 600 mg daily for a total of 21 days. A non-serious adverse event (nasopharyngitis) occurred and resolved during the period of incorrect dosing, with no onset of other reported events. Overdose was also reported in two patients in oncology studies who were exposed to a maximum of 600 mg twice daily for up to 8 days. Adverse events reported were consistent with the existing safety profile of OFEV. Both patients recovered. In case of overdose, interrupt treatment and initiate general supportive measures as appropriate.11 DESCRIPTIONOFEV capsules contain nintedanib, a kinase inhibitor [see Mechanism of Action (12.1)]. Nintedanib is presented as the ethanesulfonate salt (esylate), with the chemical name 1H-Indole-6-carboxylic acid, 2,3-dihydro-3-[[[4-[methyl[(4-methyl-1-piperazinyl)acetyl]amino]phenyl]amino]phenylmethylene]-2-oxo-,methyl ester, (3Z)-, ethanesulfonate (1:1).Its structural formula is:N N N H N HO N C H 3OOO CH 3CH 3C H 3SO O ONintedanib esylate is a bright yellow powder with an empirical formula of C 31H 33N 5O 4·C 2H 6O 3S and a molecular weight of 649.76 g/mol.OFEV capsules for oral administration are available in 2 dose strengths containing 100 mg or 150 mg of nintedanib (equivalent to 120.40 mg or 180.60 mg nintedanib ethanesulfonate, respectively). The inactive ingredients of OFEV are the following: Fill Material: triglycerides, hard fat, lecithin. Capsule Shell: gelatin, glycerol, titanium dioxide, red ferric oxide, yellow ferric oxide, black ink.12 CLINICAL PHARMACOLOGY12.1 Mechanism of ActionNintedanib is a small molecule that inhibits multiple receptor tyrosine kinases (RTKs) and non-receptor tyrosine kinases (nRTKs). Nintedanib inhibits the following RTKs: platelet-derived growth factor receptor (PDGFR) α and β, fibroblast growth factor receptor (FGFR) 1-3, vascular endothelial growth factor receptor (VEGFR) 1-3, and Fms-like tyrosine kinase-3 (FLT3). Among them, FGFR, PDGFR, and VEGFR have been implicated in IPF pathogenesis. Nintedanib binds competitively to the adenosine triphosphate (ATP) binding pocket of these receptors and blocks the intracellular signaling which is crucial for the proliferation, migration, andtransformation of fibroblasts representing essential mechanisms of the IPF pathology. In addition, nintedanib inhibits the following nRTKs: Lck, Lyn and Src kinases. The contribution of FLT3 and nRTK inhibition to IPF efficacy is unknown.12.2 PharmacodynamicsCardiac ElectrophysiologyIn a study in renal cell cancer patients, QT/QTc measurements were recorded and showed that a single oral dose of 200 mg nintedanib as well as multiple oral doses of 200 mg nintedanib administered twice daily for 15 days did not prolong the QTcF interval.12.3 PharmacokineticsThe PK properties of nintedanib were similar in healthy volunteers, patients with IPF, and cancer patients. The PK of nintedanib is linear. Dose proportionality was shown by an increase of nintedanib exposure with increasing doses (dose range 50 to 450 mg once daily and 150 to 300 mg twice daily). Accumulation upon multiple administrations in patients with IPF was 1.76-fold for AUC. Steady-state plasma concentrations were achieved within one week of dosing. Nintedanib trough concentrations remained stable for more than one year. The inter-individual variability in the PK of nintedanib was moderate to high (coefficient of variation ofstandard PK parameters in the range of 30% to 70%), intra-individual variability low to moderate (coefficients of variation below 40%).AbsorptionNintedanib reached maximum plasma concentrations approximately 2 to 4 hours after oral administration as a soft gelatin capsule under fed conditions. The absolute bioavailability of a 100 mg dose was 4.7% (90% CI: 3.62 to 6.08) in healthy volunteers. Absorption and bioavailability are decreased by transporter effects and substantial first-pass metabolism.After food intake, nintedanib exposure increased by approximately 20% compared to administration under fasted conditions (90% CI: 95.3% to 152.5%) and absorption was delayed (median t max fasted: 2.00 hours; fed: 3.98 hours), irrespective of the food type.DistributionNintedanib follows bi-phasic disposition kinetics. After intravenous infusion, a high volume of distribution which was larger than total body volume (V ss: 1050 L) was observed.The in vitro protein binding of nintedanib in human plasma was high, with a bound fraction of 97.8%. Serum albumin is considered to be the major binding protein. Nintedanib is preferentially distributed in plasma with a blood to plasma ratio of 0.87.EliminationThe effective half-life of nintedanib in patients with IPF was 9.5 hours (gCV 31.9%). Total plasma clearance after intravenous infusion was high (CL: 1390 mL/min; gCV 28.8%). Urinary excretion of unchanged drug within 48 hours was about 0.05% of the dose after oral and about 1.4% of the dose after intravenous administration; the renal clearance was 20 mL/min.MetabolismThe prevalent metabolic reaction for nintedanib is hydrolytic cleavage by esterases resulting in the free acid moiety BIBF 1202. BIBF 1202 is subsequently glucuronidated by UGT enzymes, namely UGT 1A1, UGT 1A7, UGT 1A8, and UGT 1A10 to BIBF 1202 glucuronide. Only a minor extent of the biotransformation of nintedanib consisted of CYP pathways, with CYP 3A4 being the predominant enzyme involved. The major CYP-dependent metabolite could not be detected in plasma in the human absorption, distribution, metabolism, and elimination study. In vitro, CYP-dependent metabolism accounted for about 5% compared to about 25% ester cleavage.ExcretionThe major route of elimination of drug-related radioactivity after oral administration of [14C] nintedanib was via fecal/biliary excretion (93.4% of dose), and the majority of OFEV was excreted as BIBF 1202. The contribution of renal excretion to the total clearance was low (0.65% of dose). The overall recovery was considered complete (above 90%) within 4 days after dosing.Specific PopulationsAge, Body Weight, and SexBased on population PK analysis, age and body weight were correlated with nintedanib exposure. However,t heir effects on exposure are not sufficient to warrant a dose adjustment. There was no influence of sex on the exposure of nintedanib.Renal ImpairmentBased on a population PK analysis of data from 933 patients with IPF, exposure to nintedanib was not influenced by mild (CrCl: 60 to 90 mL/min; n=399) or moderate (CrCl: 30 to 60 mL/min; n=116) renal impairment. Data in severe renal impairment (CrCl below 30 mL/min) was limited.。
石药「尼达尼布」首仿报产!特发性肺纤维化靶向药
石药「尼达尼布」首仿报产!特发性肺纤维化靶向药5 月 7 日,Insight 数据库显示,石药集团恩必普药业「尼达尼布软胶囊」仿制药首家报产,该药原研为勃林格殷格翰的乙磺酸尼达尼布(Nintedanib Esylate,Ofev®),2018 年销售额 11 亿欧元,同比增长 28.7%。
以下是Insight 数据库(https:///)显示的尼达尼布软胶囊受理号时光轴:尼达尼布软胶囊原研尼达尼布是一种三联血管激酶抑制剂,其作用靶点有血小板源生长因子(PDGF)、血管内皮生长因子(VEGF)和碱性纤维母细胞生长因子(bFGF)。
三项关键性研究的汇总数据结果显示,Ofev 可使IPF 疾病进展延缓约50%,IPF 急性加重的风险显著下降47%,全因死亡率风险降低 30%,并使治疗期间的死亡率显著下降 43%。
乙磺酸尼达尼布,是勃林格殷格翰自主研发的抗肺纤维化(IPF)创新靶向药, 2014 年 10 月 15 日获美国 FDA 批准;2015 年 7 月,尼达尼布被纳入ATS/ERS/JRS/ALAT 特发性肺纤维化诊治国际循证指南的推荐用药,当年销售额也冲到3 亿欧元,后面一直保持稳定的增长;2017 年 9 月在中国获批上市,上市后的商品名为维加特®。
Insight 数据库(https://)显示,石药集团尼达尼布按新 4 类仿制药申报,已经处于研发第一梯队,并且获批后视同通过一致性评价。
此外,尼达尼布软胶囊还有豪森、科伦药业等8 家企业已经获批临床。
除仿制药外,东阳光药业的1 类新药伊非尼酮(yinfenidone,HEC585)也已经处于国内临床 1 期;并于 2017 年 2 月在美国获批临床,并获得FDA 孤儿药资格认定,用于治疗特发性肺纤维化(IPF)。
查询中国专利局显示,原研乙磺酸尼达尼布的化合物专利(公开号:CN1671660A)要到 2023 年 7 月 18 日到期,石药集团抢先布局,待专利到期后可第一时间投放中国市场。
尼达尼布杂质全套结构整理
Nintedanib尼达尼布杂质结构图整理英文名称:Nintedanib英文同义名称:BIBF 1120,ntedanib,Vargatef中文名称:尼达尼布中文其他名称:尼达尼布乙烷磺酸盐尼达尼布是由德国勃林格殷格翰公司研发的一种口服给药的三重酪氨酸激酶抑制剂,靶点包括血小板源生长因子(PDGF)、血管内皮生长因子(VEGF) 和碱性纤维母细胞生长因子(bFGF),也可抑制MAPK和Akt激活。
目前主要用于肿瘤治疗,如结肠直肠癌、卵巢癌、多发性骨髓瘤等。
针对呼吸系统疾病的研究主要围绕晚期非小细胞肺癌(NSCLC)和特发性肺间质纤维化(IPF) 的临床治疗开展。
2014年6月勃林格殷格翰公司宣布,尼达尼布治疗特发性肺纤维化(IPF)的上市许可申请获得欧洲药品管理局(EMA)的确认、并被EMA纳入加速审批名单。
2014年10月15日,美国食品与药品管理局FDA批准尼达尼布(nintedanib,商品名:Ofev)和吡非尼酮(pirfenidone,商品名:Esbriet)两种新的口服药物用于特发性肺纤维化(IPF)治疗。
IPF是一种对人类危害严重的致命性肺部疾病,患者在诊断之后的中位生存期仅为2至3年。
在今天之前,尚无一种IPF治疗药物获得FDA批准。
尼达尼布此前已被FDA授予突破性治疗药物的地位,此次批准也使尼达尼布成为首个、也是唯一一个获准用于治疗IPF的酪氨酸激酶抑制剂(TKI)。
尼达尼布针对已被证实在肺纤维化病理机制中具有潜在影响的生长因子受体发挥作用,其中最为重要的就是血小板源性生长因子受体(PDGFR)、成纤维细胞生长因子受体(FGFR)和血管内皮生长因子受体(VEGFR)。
通过阻断这些参与纤维化进程的信号转导通路,尼达尼布被认为有望能够通过减少肺功能下降速度、从而减缓IPF疾病进展。
公司目前还在针对尼达尼布作为癌症治疗选择开展临床研发工作,包括非小细胞肺癌、卵巢癌、结直肠癌和肝细胞肝癌。
药物尼达尼布(Nintedanib)合成检索总结报告
药物尼达尼布(Nintedanib)合成检索总结报告
一、尼达尼布(Nintedanib)简介
尼达尼布(Nintedanib)于2014年10月15日在美国上市。
尼达尼布(Nintedanib)抑制多种受体酪氨酸激酶(RTKs)和非受体酪氨酸激酶(nRTKs),适用于特发性肺纤维化。
尼达尼布(Nintedanib)分子结构式如下:
英文名称:Nintedanib
中文名称:尼达尼布
本文主要对尼达尼布(Nintedanib)的合成路线、关键中间体的合成方法及实验操作方法进行了文献检索并作出了总结。
二、尼达尼布(Nintedanib)合成路线
合成路线一:
合成路线二:合成路线三:合成路线四:合成路线五:
三、尼达尼布(Nintedanib)合成检索总结报告(一) 尼达尼布(Nintedanib)中间体3的合成
(二) 尼达尼布(Nintedanib)中间体4的合成方法一
(三) 尼达尼布(Nintedanib)中间体4的合成方法二①尼达尼布(Nintedanib)中间体7的合成。
《尼达尼布乙磺酸盐对糖脂代谢机制的研究》
《尼达尼布乙磺酸盐对糖脂代谢机制的研究》一、引言随着现代生活方式的改变,糖脂代谢紊乱已成为全球性的健康问题。
尼达尼布乙磺酸盐作为一种新型的药物,在临床应用中表现出了显著的疗效。
然而,关于其作用机制,尤其是对糖脂代谢的影响尚不明确。
本文旨在探讨尼达尼布乙磺酸盐对糖脂代谢机制的研究,以期为临床应用提供理论依据。
二、材料与方法1. 材料本研究所用材料为尼达尼布乙磺酸盐,以及相关实验动物(如小鼠、大鼠等)的糖脂代谢相关指标样本。
2. 方法(1)建立动物模型:选用健康的小鼠和大鼠,建立糖脂代谢紊乱模型,以模拟人类糖脂代谢紊乱的情况。
(2)实验分组:将动物分为实验组和对照组,实验组给予尼达尼布乙磺酸盐治疗。
(3)样本收集与检测:在治疗前后分别收集动物血液、肝脏等组织样本,检测糖脂代谢相关指标的变化。
(4)数据分析:采用统计学方法对实验数据进行处理与分析。
三、实验结果1. 尼达尼布乙磺酸盐对糖代谢的影响实验结果显示,给予尼达尼布乙磺酸盐治疗后,实验组动物的血糖水平明显降低,胰岛素敏感性提高。
这表明尼达尼布乙磺酸盐可能通过促进胰岛素受体敏感性,改善糖代谢紊乱。
2. 尼达尼布乙磺酸盐对脂代谢的影响实验还发现,尼达尼布乙磺酸盐能够显著降低实验组动物的总胆固醇、甘油三酯等血脂水平,提高高密度脂蛋白胆固醇水平。
这表明尼达尼布乙磺酸盐可能具有调节脂质代谢的作用。
3. 尼达尼布乙磺酸盐的作用机制探讨通过对实验组和对照组的样本进行基因表达、蛋白质水平等检测,发现尼达尼布乙磺酸盐可能通过激活某些酶的活性,促进脂肪酸的氧化分解,同时抑制脂肪合成相关基因的表达,从而改善糖脂代谢紊乱。
四、讨论本研究表明,尼达尼布乙磺酸盐能够显著改善糖脂代谢紊乱,其作用机制可能与激活脂肪酸氧化分解、抑制脂肪合成相关基因的表达有关。
这一发现为尼达尼布乙磺酸盐在临床应用中提供了新的理论依据。
然而,本研究仍存在一定局限性,如样本量较小、实验时间较短等,需进一步开展大规模、长期的临床试验以验证本研究的结论。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
r e tn
b
6.511 7.108 7.281 7.584
h c io
r a p em
r e tn
400
r a p m
r e tn
200 0 0
===================================================================== Area Percent Report ===================================================================== Sorted By : Signal Multiplier : 1.0000 Dilution : 1.0000 Use Multiplier & Dilution Factor with ISTDs
bio
2
m e ch
4
r e tn
8
bio
m e ch
10
r a p
12
r e tn
14 min
m
r a p
r e tn
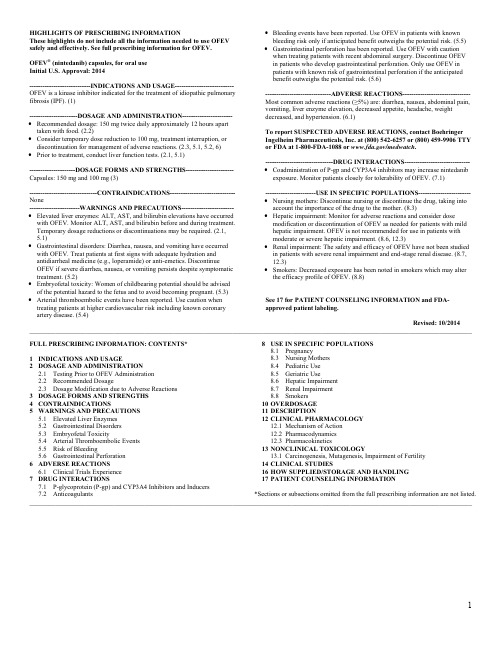
Signal 1: VWD1 A, Wavelength=210 nm
Peak RetTime Type Width Area Height Area # [min] [min] [mAU*s] [mAU] % ----|-------|----|-------|----------|----------|--------| 1 6.511 MM 0.0924 21.10839 3.80764 0.6217 2 6.793 MF 0.0573 3349.94336 973.63055 98.6682 3 7.108 FM 0.1139 12.21335 1.78661 0.3597 4 7.281 FM 0.0957 6.06081 1.05581 0.1785 Agilent HPLC 6/22/2018 4:39:56 PM SYSTEM
Data File D:\2018\TEST\DATA\20180622\20180622-03 2018-06-22 14-36-45\HX201806223.D Sample Name: M-6-22-14 ===================================================================== Acq. Operator : SYSTEM Seq. Line : 3 Acq. Instrument : Agilent HPLC Location : 15 Injection Date : 6/22/2018 3:22:41 PM Inj : 1 Inj Volume : 5.000 µl Different Inj Volume from Sample Entry! Actual Inj Volume : 1.000 µl Acq. Method : D:\2018\TEST\DATA\20180622\20180622-03 2018-06-22 14-36-45\5-(10)-100(5)-140-210.M Last changed : 6/22/2018 2:36:45 PM by SYSTEM Analysis Method : D:\2018\TEST\DATA\20180622\20180622-03 2018-06-22 14-36-45\5-(10)-100(5)-140-210.M (Sequence Method) Last changed : 6/22/2018 4:39:35 PM by SYSTEM (modified after loading) Additional Info : Peak(s) manually integrated
m e h
r a p
r e tn
m
r a p
r e tn
b
r e tn
r a p m e h c io
r a p
r e tn
b h c io
r a p em
r e tn
r a p m
bio
r e tn
m e ch
r e tn
bio
m e ch
r a p
r e tn
m
r a p
bio
r e tn
m e ch
bio
m e ch
r a p
r e tn
c o bi
m e h
r a p
r e tn
r e tn
r e tn
Page
r e tn
1 of 2
Data File D:\2018\TEST\DATA\20180622\20180622-03 2018-06-22 14-36-45\HX201806223.D Sample Name: M-6-22-14 Peak RetTime Type Width Area Height Area # [min] [min] [mAU*s] [mAU] % ----|-------|----|-------|----------|----------|--------| 5 7.584 MM 0.0727 5.83387 1.33764 0.1718 Totals :
r a p
r e tn
c o bi
m e h
r a p
r e tn
Agilent HPLC 6/22/2018 4:39:56 PM SYSTEM
r e tn
Page
r e tn
2 of 2
m
r a p
r e tn
b
h c io
p m e
r e n t r a
c o i b
ห้องสมุดไป่ตู้
m e h
r a p
r e tn
m
r a p
800
600
b
r a p m e h c io
r a p
6
6.793
mAU
r e tn
VWD1 A, Wavelength=210 nm (D:\2018\TEST\DATA\20180622\20180622-03 2018-06-22 14-36-45\HX201806223.D)
m
r a p
r e tn
3395.15978
===================================================================== *** End of Report ***
b
h c io
p m e
981.61826
r e n t r a
c o i b