Cardiovascular effects of the macrolide antibiotic tilmicosin
泰乐菌素 (Tylosin) ,亦称泰农、泰乐霉素,是美国于 年从弗氏链霉菌

泰拉霉素的研究进展
泰拉霉素的研究进展张刚;郭丽清;徐金雷;梁景乐;吴家鑫【摘要】泰拉霉素是一种动物专用的大环内酯类抗生素,主要应用于防治猪和牛的呼吸系统疾病.秦拉霉素具有抗菌活性强、抗菌谱广、吸收迅速、生物利用度高、消除半衰期超长、药效持久、单次给药即可完成整个治疗过程等优点.为了促进泰拉霉素的合理应用、研制和开发,通过对其合成方法、作用机理、抗菌活性、检测方法、药代动力学、药效学、生物安全性和残留等相关研究进展进行综述.【期刊名称】《北京联合大学学报(自然科学版)》【年(卷),期】2017(031)002【总页数】6页(P48-53)【关键词】秦拉霉素;大环内脂;研究进展【作者】张刚;郭丽清;徐金雷;梁景乐;吴家鑫【作者单位】中牧实业股份有限公司,北京 100070;中牧实业股份有限公司,北京100070;中牧实业股份有限公司,北京 100070;中牧实业股份有限公司,北京100070;中牧实业股份有限公司,北京 100070【正文语种】中文【中图分类】R914泰拉霉素(Tulathromycin),又称泰拉菌素、土拉霉素、托拉霉素,是由美国辉瑞公司(Pfizer)开发的动物专用半合成的大环内酯类抗生素,商品名为瑞可新(Draxxin),2004年该药在美国和欧盟上市,2008年该药被我国农业部允许在动物生产中使用。
泰拉霉素的分子式为C41H79N3O12,相对分子质量为806.23,由13元氮杂内酯环和15元氮杂内酯环两种同分异构体以1∶9的比例组成的混合物(结构式如图1所示),且两者之间可以相互转化;其结构特点为具有3个碱性氨基基团,在溶液中呈强负电性,pKa值分别为8.6,9.6和9.9,这有利于穿透革兰氏阴性菌的外膜,当氨基未离子化时,呈亲脂性,代谢稳定。
[1]泰拉霉素主要用于防治由胸膜肺炎放线杆菌、支原体、巴氏杆菌、副嗜血杆菌、支气管败血性博德特菌等引起的猪、牛呼吸系统疾病。
泰拉霉素具有药物吸收速度快、药效持久、生物利用度高等优点。
西尼地平
34 . 特殊毒理学试验 研究结果显示 : 西尼地平无致畸、 致突变、 致癌作用 , 无依赖性 。 4药代动力学研究 . . 健康男性志愿者 1 次性 口服西尼地平, 剂量分别 为 5 、lmg 0 mg 0 、2 mg后 ,18小 时至 22小 时血 . . 药浓度达最高值 ,有关的药动学 的药动力学参数
剂量 T x ma ( / UC (’-4 ) ma fC xn T12 A 0 2
开始给药直至怀孕后的第 7天 。 结果未见西尼地平对 雄鼠的生育能力和雌鼠的受精能力有不 良的影响 , 所 有剂量的雌鼠着床点数、活胎数、死胎数、死胎吸收 数均未见异常 ,所产的幼鼠也未见畸形或异常 。
维普资讯
20 0 7年 3月 l 日 . . No 2 5 07 1 .
技 术 市 场
西 地 平
中国医药技术与市场网 (t :w wzv . m. ht / w . pc c p/ a o n 网络实名: 中国药品) 常年开设医药科技成果靴 E , 欢迎浏览 !
增加心率 , 对心肌抑制较弱 , 并且还有较强的扩张冠 脉作用这些综合 的降压效果均优于硝苯地平等传统 钙拮抗剂 。 临床还表明, 品在降压的同时, 木 还能降 低脂质过氧化酶浓度和致动脉粥样硬化指数( 低密度
5 0 mg k ,皮下注射途径给药和腹腔注射途径给 00 /g
药 L 5 分别达到 1 4 mg k Do 5 / g和 2 5 mg k 。 8 3 3 / g 雄 性大鼠n.途径和腹腔途径给予西尼地平其 L o 1 i l  ̄ Ds分
阿奇霉素FDAlabel
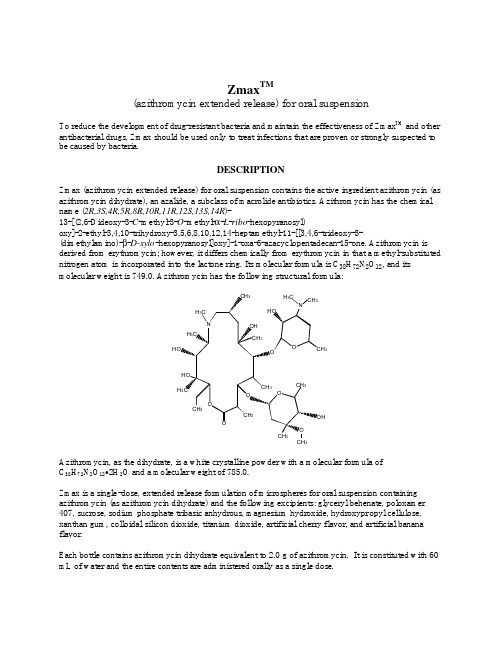
Zmax TM(azithromycin extended release) for oral suspensionTo reduce the development of drug-resistant bacteria and maintain the effectiveness of Zmax TM and other antibacterial drugs, Zmax should be used only to treat infections that are proven or strongly suspected to be caused by bacteria.DESCRIPTIONZmax (azithromycin extended release) for oral suspension contains the active ingredient azithromycin (as azithromycin dihydrate), an azalide, a subclass of macrolide antibiotics. Azithromycin has the chemical name (2R,3S,4R,5R,8R,10R,11R,12S,13S,14R)-13-[(2,6-Dideoxy-3-C-methyl-3-O-methyl-α-L-ribo-hexopyranosyl)oxy]-2-ethyl-3,4,10-trihydroxy-3,5,6,8,10,12,14-heptamethyl-11-[[3,4,6-trideoxy-3- (dimethylamino)-β-D-xylo-hexopyranosyl]oxy]-1-oxa-6-azacyclopentadecan-15-one. Azithromycin is derived from erythromycin; however, it differs chemically from erythromycin in that a methyl-substituted nitrogen atom is incorporated into the lactone ring. Its molecular formula is C38H72N2O12, and its molecular weight is 749.0. Azithromycin has the following structural formula:33Azithromycin, as the dihydrate, is a white crystalline powder with a molecular formula ofC38H72N2O12•2H2O and a molecular weight of 785.0.Zmax is a single-dose, extended release formulation of microspheres for oral suspension containing azithromycin (as azithromycin dihydrate) and the following excipients: glyceryl behenate, poloxamer 407, sucrose, sodium phosphate tribasic anhydrous, magnesium hydroxide, hydroxypropyl cellulose, xanthan gum, colloidal silicon dioxide, titanium dioxide, artificial cherry flavor, and artificial banana flavor.Each bottle contains azithromycin dihydrate equivalent to 2.0 g of azithromycin. It is constituted with 60 mL of water and the entire contents are administered orally as a single dose.CLINICAL PHARMACOLOGYPharmacokineticsZmax is an extended release microsphere formulation. Based on data obtained from studies evaluatingthe pharmacokinetics (PK) of azithromycin in healthy adult subjects a higher peak serum concentration(C max) and greater systemic exposure (AUC0-24) of azithromycin are achieved on the day of dosingfollowing a single 2.0 g dose of Zmax versus 1.5 g of azithromycin tablets administered over 3 days (500 mg/day) or 5 days (500 mg on day 1, 250 mg/day on days 2-5) [Table 1]. Consequently, due to thesedifferent PK profiles, Zmax is not interchangeable with azithromycin tablet 3-day and 5-day dosingregimens.Table 1. Mean (SD) Pharmacokinetic Parameters for Azithromycin on Day 1 Following theAdministration of a Single Dose of 2.0 g Zmax or 1.5 g of Azithromycin Tablets Given over 3 Days(500 mg/day) or 5 Days (500 mg on Day 1 and 250 mg on Days 2-5) to Healthy Adult SubjectsAzithromycin RegimenPharmacokineticParameter*Zmax[n=41]†3-day ‡[n=12]5-day ‡[n=12]C max (µg/mL)0.821(0.281)0.441(0.223)0.434(0.202)T max§ (hr)5.0(2.0-8.0)2.5(1.0-4.0)2.5(1.0-6.0)AUC0-24 (µg·hr/mL)8.62(2.34)2.58(0.84)2.60(0.71)AUC0-8¶(µg·hr/mL)20.0(6.66)17.4(6.2)14.9(3.1)t1/2 (hr)58.8(6.91)71.8(14.7)68.9(13.8)* Zmax, 3-day and 5-day regimen parameters obtained from separate PK studies † n = 21 for AUC0-8 and t1/2‡ C max, T max and AUC0-24 values for Day 1 only§Median (range)¶ Total AUC for the 1-day, 3-day and 5-day regimensSD = standard deviationC max = maximum serum concentrationT max = time to C maxAUC = area under concentration vs. time curvet1/2 = terminal serum half-lifeAbsorptionIn a two-way crossover study, sixteen healthy adult subjects were administered single doses of 2.0 g Zmax and azithromycin powder for oral suspension (POS) (2 × 1.0 g sachets). The mean C max and AUC0-t of azithromycin were lower by 57% and 17%, respectively with Zmax compared to azithromycin POS. The bioavailability of Zmax relative to azithromycin POS was 83%. On average, peak serum concentrations were achieved approximately 2.5 hours later following Zmax administration compared to azithromycin POS. Thus, single 2.0 g doses of Zmax and azithromycin POS are not bioequivalent and are not interchangeable.When a 2.0 g dose of Zmax was administered to 15 healthy adult subjects following a high-fat meal (150 kcal from proteins, 250 kcal from carbohydrates and 500-600 kcal from fats) the mean azithromycin C max increased by 115% and the mean AUC0-t increased by 23% as compared to administration in a fasted state. When a 2.0 g dose of Zmax was administered to 88 adult subjects following a standard meal (56 kcal from proteins, 316 kcal from carbohydrates, and 207 kcal from fats) the mean azithromycin C max increased by 119% and the mean AUC0-72 increased 12% as compared to administration in the fasted state. (See DOSAGE AND ADMINISTRATION.)In a two-way crossover study, 39 healthy adult subjects were administered 2.0 g dose of Zmax alone and with 20 mL of regular strength aluminum and magnesium hydroxide antacid. Following the administration of Zmax with an aluminum and magnesium hydroxide antacid, the rate and extent of azithromycin absorption were not altered.DistributionThe serum protein binding of azithromycin is concentration dependent, decreasing from 51% at0.02 µg/mL to 7% at 2.0 µg/mL.Following oral administration, azithromycin is widely distributed throughout the body with an apparent steady-state volume of distribution of 31.1 L/kg.Higher azithromycin concentrations in tissues than in plasma or serum have been observed. The extensive distribution of drug to tissues may be relevant to clinical activity. The antimicrobial activity of azithromycin is pH related and appears to be reduced with decreasing pH. Hence, high tissue concentrations should not be interpreted as being quantitatively related to clinical efficacy. Selected tissue (or fluid) concentration and tissue (or fluid) to plasma/serum concentration ratios are shown in Table 2.Table 2. Azithromycin Concentrations Following a 500 mg Dose in Adults*TISSUE OR FLUID TIME AFTERDOSE (hr) TISSUE OR FLUIDCONCENTRATION(µg/g or µg/mL)CORRESPONDINGPLASMA OR SERUMCONCENTRATION(µg/mL)TISSUE (FLUID)PLASMA (SERUM)RATIOSKIN 72-96 0.4 0.012 35LUNG 72-96 4.0 0.012 >100 SPUTUM†2-4 1.0 0.64 2 SPUTUM‡10-12 2.9 0.1 30 TONSIL§9-18 4.5 0.03 >100 TONSIL§180 0.9 0.006 >100 CERVIX¶19 2.8 0.04 70 * Azithromycin tissue concentrations were originally determined using 250 mg capsules.† Sample was obtained 2-4 hours after the first dose.‡ Sample was obtained 10-12 hours after the first dose.§ Dosing regimen of two doses of 250 mg each, separated by 12 hours.¶Sample was obtained 19 hours after a single 500 mg dose.The extensive tissue distribution was confirmed by examination of additional tissues and fluids (bone, ejaculum, prostate, ovary, uterus, salpinx, stomach, liver, and gallbladder). However, the clinical significance of these tissue concentration data is unclear as clinical data from adequate andwell-controlled studies of azithromycin treatment of infections in these additional body sites are not available.Following a regimen of 500 mg of azithromycin tablets on the first day and 250 mg daily for 4 days, only very low concentrations were noted in cerebrospinal fluid (less than 0.01 µg/mL) in the presence ofnon-inflamed meninges.MetabolismIn vitro and in vivo studies to assess the metabolism of azithromycin have not been performed.EliminationSerum azithromycin concentrations following a single 2.0 g dose of Zmax declined in a polyphasic pattern with a terminal elimination half-life of 59 hours. The prolonged terminal half-life is thought to be due to a large apparent volume of distribution.Biliary excretion of azithromycin, predominantly as unchanged drug, is a major route of elimination. Over the course of a week, approximately 6% of the administered dose appears as unchanged drug in urine.Special PopulationsRenal InsufficiencyAzithromycin pharmacokinetics was investigated in 42 adults (21 to 85 years of age) with varying degrees of renal impairment. Following the oral administration of a single 1.0 g dose of azithromycin (4 ×250 mg capsules), the mean C max and AUC0-120 increased by 5.1% and 4.2%, respectively in subjects with GFR 10 to 80 mL/min compared to subjects with normal renal function (GFR >80 mL/min). The meanC max and AUC0-120 increased 61% and 35%, respectively in subjects with end-stage renal disease (GFR<10 mL/min) compared to subjects with normal renal function (GFR >80 mL/min). Based upon the pharmacokinetic data for azithromycin in subjects with renal impairment, no dose adjustment for Zmax is recommended in patients with GFR >10 mL/min. (See DOSAGE AND ADMINISTRATION.)Hepatic InsufficiencyThe pharmacokinetics of azithromycin in subjects with hepatic impairment has not been established.GenderThe impact of gender on the pharmacokinetics of azithromycin has not been evaluated for Zmax. However,previous studies have demonstrated no significant differences in the disposition of azithromycin between male and female subjects. No dosage adjustment of Zmax is recommended based on gender.Geriatric PatientsThe pharmacokinetics of azithromycin following administration of Zmax has not been evaluated in geriatric patients.Pediatric PatientsZmax is not approved for pediatric patients.Drug-Drug InteractionsDrug interaction studies were performed with azithromycin capsules and tablets (doses ranged from 500 to 1200 mg) and drugs likely to be co-administered. The effects of co-administration of azithromycin on the pharmacokinetics of other drugs are shown in Table 3 and the effects of other drugs on the pharmacokinetics of azithromycin are shown in Table 4.Co-administration of azithromycin capsules and tablets at therapeutic doses had a modest effect on the pharmacokinetics of the drugs listed in Table 3. Although the drug interaction studies were not conducted with Zmax , no potential drug interactions are expected since the total exposure to azithromycin is comparable for Zmax and the other azithromycin regimens. Therefore, no dosage adjustment of drugs listed in Table 3 is recommended when co-administered with Zmax. (See PRECAUTIONS - Drug Interactions.)Co-administration of azithromycin tablets with efavirenz or fluconazole had a modest effect on the pharmacokinetics of azithromycin. Nelfinavir significantly increased the C max and AUC of azithromycin. Similar results are expected with Zmax . Although no dosage adjustment of Zmax is recommended when administered with drugs listed in Table 4, close monitoring for known side effects of azithromycin, such as liver enzyme abnormalities and hearing impairment, is warranted when co-administered with nelfinavir. (See PRECAUTIONS - Drug Interactions.)Table 3. Drug Interactions: Pharmacokinetic Parameters for Co-administered Drugs in the Presence of AzithromycinRatio (with/without Azithromycin) ofCo-administered DrugPharmacokinetic Parameters (90%CI); No Effect = 1.00 Co-administeredDrugDose of Co-administeredDrugDose of Azithromycin*nMean C max Mean AUC Atorvastatin 10 mg/day × 8 days500 mg/day PO on days 6-812 0.83 (0.63 to 1.08)1.01 (0.81 to 1.25)Carbamazepine200 mg/day × 2 days, then 200 mg BID × 18 days 500 mg/day PO for days 16-1870.97 (0.88 to 1.06) 0.96 (0.88 to 1.06) Cetirizine20 mg/day × 11 days500 mg PO on day 7, then 250 mg/day on days 8-11141.03 (0.93 to 1.14) 1.02 (0.92 to 1.13) Didanosine 200 mg PO BID × 21 days1,200 mg/day POon days 8-21 6 1.44 (0.85 to 2.43)1.14 (0.83 to 1.57)Efavirenz 400 mg/day × 7days600 mg PO on day 7 14 1.04† 0.95† Fluconazole 200 mg PO single dose 1,200 mg POsingle dose18 1.04 (0.98 to 1.11)1.01 (0.97 to 1.05)Indinavir 800 mg TID × 5days1,200 mg PO on day 5 18 0.96 (0.86 to 1.08)0.90 (0.81 to 1.00)Midazolam 15 mg PO on day 3 500 mg/day PO × 3days12 1.27 (0.89 to 1.81)1.26 (1.01 to 1.56)Nelfinavir 750 mg TID × 11 days1,200 mg PO onday 9 14 0.90 (0.81 to 1.01)0.85 (0.78 to 0.93)Rifabutin 300 mg/day × 10days500 mg PO on day 1, then 250 mg/day on days 2-106‡NASildenafil 100 mg on days 1 and 4 500 mg/day PO × 3days12 1.16 (0.86 to 1.57)0.92 (0.75 to 1.12)Theophylline 4 mg/kg IV on days 1, 11, 25 500 mg PO on day7, then 250 mg/dayon days 8-11101.19 (1.02 to 1.40) 1.02 (0.86 to 1.22) Theophylline 300 mg PO BID × 15 days500 mg PO on day6, then 250 mg/day on days 7-108 1.09 (0.92 to 1.29)1.08 (0.89 to 1.31)Triazolam 0.125 mg on day 2 500 mg PO on day1, then 250 mg/day on day 2121.06†1.02†Trimethoprim/ Sulfamethoxazole 160 mg/800 mg/day PO × 7 days 1,200 mg PO on day 7120.85(0.75 to 0.97)/0.90 (0.78 to 1.03)0.87(0.80 to 0.95)/0.96 (0.88 to 1.03)Zidovudine 500 mg/day PO × 21 days600 mg/day PO × 14 days5 1.12 (0.42 to 3.02)0.94 (0.52 to 1.70)Zidovudine500 mg/day PO × 21 days1,200 mg/day PO × 14 days41.31 (0.43 to 3.97) 1.30 (0.69 to2.43)NA = not available* Refers to azithromycin capsules and tablets unless specified † 90% confidence interval not reported‡ Mean rifabutin concentrations one-half day after the last dose of rifabutin were 60 ng/mL when co-administered with azithromycin and 71 ng/mL when co-administered with placebo.Table 4. Drug Interactions: Pharmacokinetic Parameters for Azithromycin in the Presence of Co-administered Drugs (See PRECAUTIONS - Drug Interactions )Ratio (with/without co-administereddrug) of AzithromycinPharmacokinetic Parameters (90%CI); No Effect = 1.00 Co-administeredDrugDose of Co-administeredDrugDose of Azithromycin*nMean C max Mean AUC Efavirenz 400 mg/day × 7 days600 mg PO on day 714 1.22 (1.04 to 1.42)0.92† Fluconazole 200 mg PO single dose1,200 mg PO single dose18 0.82 (0.66 to 1.02)1.07 (0.94 to 1.22)Nelfinavir 750 mg TID × 11 days1,200 mg PO on day 914 2.36 (1.77 to 3.15)2.12 (1.80 to 2.50)Rifabutin300 mg/day × 10 days500 mg PO on day 1, then 250 mg/day on days 2-106‡NAAl and Mg hydroxide20 mL regular strength, single dose2.0 g Zmax, single dose390.99 (0.93 to 1.06) 0.99 (0.92 to 1.08)NA = not available* Refers to azithromycin capsules and tablets unless specified † 90% confidence interval not reported‡ Mean azithromycin concentrations one day after the last dose were 53 ng/mL when co-administered with 300 mg daily rifabutin and 49 ng/mL when co-administered with placebo.Microbiology Azithromycin acts by binding to the 50S ribosomal subunit of susceptible microorganisms, thus interfering with microbial protein synthesis. Nucleic acid synthesis is not affected.Azithromycin concentrates in fibroblasts, epithelial cells, macrophages, and circulating neutrophils and monocytes. In vitro incubation techniques have shown that the ratio of intracellular to extracellular concentration was >30 after one hour incubation. In vivo studies suggest that concentration inmacrophages and circulating white blood cells may contribute to drug distribution to inflamed tissues.Azithromycin has been shown to be active against most isolates of the following microorganisms, both in vitro and in clinical infections as described in the INDICATIONS AND USAGE section.Aerobic and facultative Gram-positive microorganisms Streptococcus pneumoniaeNOTE: Erythromycin- and penicillin-resistant Gram-positive isolates may demonstrate cross-resistance to azithromycin.Aerobic and facultative Gram-negative microorganisms Haemophilus influenzae Moraxella catarrhalis“Other” microorganisms Chlamydophila pneumoniae Mycoplasma pneumoniaeBeta-lactamase production should not affect azithromycin activity.The following in vitro data are available, but their clinical si gnificance is unknown.At least 90% of the following microorganisms exhibit an in vitro minimum inhibitory concentration (MIC) less than or equal to the susceptible breakpoints for azithromycin. However, the safety and effectiveness of azithromycin in treating clinical infections due to these microorganisms have not been established in adequate and well-controlled trials.Aerobic and facultative Gram-positive microorganismsStaphylococcus aureusStreptococcus pyogenesStreptococcus agalactiaeStreptococci (Groups C, F, G)Viridans group streptococciAerobic and facultative Gram-negative microorganismsBordetella pertussisLegionella pneumophilaAnaerobic microorganismsPeptostreptococcus speciesPrevotella bivia“Other” microorganismsUreaplasma urealyticumSusceptibility Testing Methods:in vitro susceptibility test results for antimicrobial drugs used in local hospitals and practice areas to the physician as periodic reports that describe the susceptibility profile of nosocomial and community-acquired pathogens. These reports should aid the physician in selecting the most effective antimicrobial.Dilution techniques:Quantitative methods are used to determine antimicrobial minimum inhibitory concentrations (MICs). These MICs provide estimates of the susceptibility of bacteria to antimicrobial compounds. The MICs should be determined using a standardized procedure. Standardized procedures are based on a dilution method1,3 (broth or agar) or equivalent with standardized inoculum concentrations and standardized concentrations of azithromycin powder. The MIC values should be interpreted according to criteria provided in Table 5.Diffusion techniques:Quantitative methods that require measurement of zone diameters also provide reproducible estimates of the susceptibility of bacteria to antimicrobial compounds. One such standardized procedure2,3 requires the use of standardized inoculum concentrations. This procedure uses paper disks impregnated with 15-µg azithromycin to test the susceptibility of microorganisms to azithromycin. The disk diffusion interpretive criteria are provided in Table 5.Table 5. Susceptibility Test Result Interpretive Criteria for AzithromycinMinimum Inhibitory Concentrations (µg/mL)Disk Diffusion (zone diameters in mm)PathogenS I R* S I R* Haemophilus spp. ≤ 4 -- -- ≥ 12 -- -- Streptococci includingS. pneumoniae< 0.5 1 > 2 ≥ 18 14-17 ≤ 13* The current absence of data on resistant strains precludes defining any category other than “susceptible.” If strains yield MIC results other than susceptible, they should be submitted to a reference laboratory for further testing.No interpretive criteria have been established for testing Moraxella catarrhalis. This species is not usually tested.A report of “susceptible” indicates that the pathogen is likely to be inhibited if the antimicrobial compound reaches the concentrations usually achievable. A report of “intermediate” indicates that the result should be considered equivocal, and, if the microorganism is not fully susceptible to alternative, clinically feasible drugs, the test should be repeated. This category implies possible clinical applicability in body sites where the drug is physiologically concentrated or in situations where high dosage of drug can be used. This category also provides a buffer zone, which prevents small uncontrolled technical factors from causing major discrepancies in interpretation. A report of “resistant” indicates that the pathogen is not likely to be inhibited if the antimicrobial compound reaches the concentrations usually achievable; other therapy should be selected.QUALITY CONTROLStandardized susceptibility test procedures require the use of quality control microorganisms to control the technical aspects of the test procedures. Standard azithromycin powder should provide the range of values noted in Table 6. Quality control microorganisms are specific strains of organisms with intrinsic biological properties. QC strains are very stable strains, which will give a standard and repeatable susceptibility pattern. The specific strains used for microbiological quality control are not clinically significant.Table 6. Acceptable Quality Control Ranges for AzithromycinQC Strain Minimum InhibitoryConcentrations (µg/mL)Disk Diffusion (zone diameters in mm)Haemophilus influenzaeATCC 49247 1.0-4.0 13-21 Streptococcus pneumoniaeATCC 49619 0.06-0.25 19-25INDICATIONS AND USAGEZmax is indicated for the treatment of patients with mild to moderate infections caused by susceptible strains of the designated microorganisms in the specific conditions listed below. Please see DOSAGE AND ADMINISTRATION for specific dosing recommendations.AdultsAcute bacterial sinusitis due to Haemophilus influenzae, Moraxella catarrhalis or Streptococcus pneumoniae.Community-acquired pneumonia due to Chlamydophila pneumoniae, Haemophilus influenzae, Mycoplasma pneumoniae or Streptococcus pneumoniae, in patients appropriate for oral therapy. (See CLINICAL STUDIES.)To reduce the development of drug-resistant bacteria and maintain the effectiveness of Zmax and other antibacterial drugs, Zmax should be used only to treat infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy.Appropriate culture and susceptibility tests should be performed before treatment to determine the causative organism and its susceptibility to Zmax. Therapy with Zmax may be initiated before results of these tests are known; once the results become available, antimicrobial therapy should be adjusted accordingly.CONTRAINDICATIONSZmax is contraindicated in patients with known hypersensitivity to azithromycin, erythromycin or any macrolide or ketolide antibiotic.WARNINGSSerious allergic reactions, including angioedema, anaphylaxis, and dermatologic reactions including Stevens-Johnson syndrome and toxic epidermal necrolysis have been reported rarely in patients on azithromycin therapy using other formulations. Although rare, fatalities have been reported. (See CONTRAINDICATIONS.) Despite initially successful symptomatic treatment of the allergic symptoms, when symptomatic therapy was discontinued, the allergic symptoms recurred soon thereafter in some patients without further azithromycin exposure. These patients required prolonged periods of observation and symptomatic treatment. The relationship of these episodes to the long tissue half-life of azithromycin and subsequent exposure to antigen has not been determined.If an allergic reaction occurs, appropriate therapy should be instituted. Physicians should be aware that reappearance of the allergic symptoms may occur when symptomatic therapy is discontinued.Pseudomembranous colitis has been reported with nearly all antibacterial agents and may range in severity from mild to life-threatening. Therefore, it is important to consider this diagnosis in patients who present with diarrhea subsequent to the administration of antibacterial agents. Treatment with antibacterial agents alters the normal flora of the colon and may permit overgrowth of clostridia. Studies indicate that a toxin produced by Clostridium difficile is a primary cause of “antibiotic-associated colitis.”After the diagnosis of pseudomembranous colitis has been established, therapeutic measures should be initiated. Mild cases of pseudomembranous colitis usually respond to discontinuation of the drug alone. In moderate to severe cases, consideration should be given to management with fluids and electrolytes, protein supplementation, and treatment with an antibacterial drug clinically effective against Clostridium difficile colitis.PRECAUTIONSGeneralBecause azithromycin is principally excreted via the liver, caution should be exercised when azithromycin is administered to patients with impaired hepatic function. Due to the limited data in subjects with GFR <10 mL/min, caution should be exercised when prescribing azithromycin in these patients. (See CLINICAL PHARMACOLOGY - Special Populations - Renal Insu fficiency.)Prolonged cardiac repolarization and QT interval, imparting a risk of developing cardiac arrhythmia and torsades de pointes, have been seen in treatment with other macrolides. A similar effect with azithromycin cannot be completely ruled out i n patients at increased risk for prolonged cardiac repolarization.Prescribing Zmax in the absence of a proven or strongly suspected bacterial infection is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistant bacteria. Information for PatientsPatients should be instructed to take Zmax on an empty stomach (at least 1 hour before or 2 hours following a meal).Patients should be instructed to immediately contact a physician if any signs of an allergic reaction occur. Patients who vomit within the first hour should contact their health care provider about further treatment. Keep bottle tightly closed. Store at room temperature. Use within 12 hours of constitution. Shake bottle well before use. The entire contents of the bottle should be consumed.Patients should be advised that Zmax may be taken without regard to antacids containing magnesium hydroxide and/or aluminum hydroxide.Patients should be counseled that antibacterial drugs including Zmax should only be used to treat bacterial infections. They do not treat viral infections (e.g., the common cold). Not taking the complete prescribed dose may (1) decrease the effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by Zmax or other antibacterial drugs in the future.Drug InteractionsCo-administration of nelfinavir at steady-state with a single dose of azithromycin (2 × 600 mg tablets) results in increased azithromycin serum concentrations. Although a dose adjustment of azithromycin is not recommended when administered in combination with nelfinavir, close monitoring for known side effects of azithromycin, such as liver enzyme abnormalities and hearing impairment, is warranted. (See ADVERSE REACTIONS.)Azithromycin did not affect the prothrombin time response to a single dose of warfarin. However, prudent medical practice dictates careful monitoring of prothrombin time in all patients treated with azithromycin and warfarin concomitantly. Concurrent use of macrolides and warfarin in clinical practice has been associated with increased anticoagulant effects.Drug interaction studies were performed with azithromycin and other drugs likely to be co-administered. (See CLINICAL PHARMACOLOGY - Drug-Drug Interactions.) When used in therapeutic doses, azithromycin had a modest effect on the pharmacokinetics of atorvastatin, carbamazepine, cetirizine, didanosine, efavirenz, fluconazole, indinavir, midazolam, rifabutin, sildenafil, theophylline (intravenous and oral), triazolam, trimethoprim/sulfamethoxazole or zidovudine. Co-administration with efavirenz or fluconazole had a modest effect on the pharmacokinetics of azithromycin. No dosage adjustment of either drug is recommended when azithromycin is co-administered with any of the above agents.Interactions with the drugs listed below have not been reported in clinical trials with azithromycin; however, no specific drug interaction studies have been performed to evaluate potential drug-drug interaction. Nonetheless, they have been observed with macrolide products. Until further data are developed regarding drug interactions when azithromycin and these drugs are used concomitantly, careful monitoring of patients is advised:Digoxin–elevated digoxin concentrations.Ergotamine or dihydroergotamine–acute ergot toxicity characterized by severe peripheralvasospasm and dysesthesia.Cyclosporine, hexobarbital and phenytoin concentrations.Laboratory Test InteractionsThere are no reported laboratory test interactions.Repeat TreatmentStudies evaluating the use of repeated courses of Zmax have not been conducted.Carcinogenesis, Mutagenesis, Impairment of FertilityLong-term studies in animals have not been performed to evaluate carcinogenic potential. Azithromycin has shown no mutagenic potential in standard laboratory tests: mouse lymphoma assay, human lymphocyte clastogenic assay, and mouse bone marrow clastogenic assay. No evidence of impaired fertility due to azithromycin was found in rats given daily doses up to 10 mg/kg (approximately 0.05 times the single 2.0 g oral adult human dose on a mg/m2 basis).PregnancyTeratogenic Effects. Pregnancy Category B: Reproduction studies have been performed in rats and mice at doses up to moderately maternally toxic dose concentrations (i.e., 200 mg/kg/day). These daily doses in rats and mice, based on mg/m2, are estimated to be approximately equivalent to one or one-half of, respectively, the single adult oral dose of 2.0 g. In the animal studies, no evidence of harm to the fetus due to azithromycin was found. There are, however, no adequate and well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, azithromycin should be used during pregnancy only if clearly needed.。
血管壁的结构

内膜由内皮、内皮下层、内弹性膜组成。
内皮下层位于内皮之外,为较薄的疏松结缔组织,内含少量平滑肌纤维。
内弹性膜由弹性蛋白构成,弹性膜上有许多小孔。
在中动脉的横切面上,因血管壁收缩,使内弹性膜呈波浪状,可做为内、中膜的分界线;中膜较厚,主要由10~40层平滑肌组成,故称肌性动脉;在平滑肌之间有少量弹性纤维和胶原纤维。
平滑肌纤维的舒缩可控制管径的大小,调节器官的血流量。
此外平滑肌纤维具有产生结缔组织和基质的功能;外膜厚度与中膜相近,由疏松结缔组织组成。
在外膜与中膜交界处有外弹性膜相隔,外膜中有小血管、淋巴管神经分布。
中膜增生:media hyperplasia内膜增生:intimal hyperplasia波生坦对大鼠颈动脉再狭窄的影响及其病理机制发表时间:2010-7-1 9:48:43 来源:创新医学网推荐作者:吴桂平张彦红付鑫李颖曲晓婷王涤非作者单位:沈阳医学院沈洲医院心血管内科,辽宁沈阳110002【摘要】目的探讨波生坦对大鼠颈动脉再狭窄的影响及其病理机制。
方法选取Wistar大鼠65只,随机分为假手术组、损伤组及波生坦组。
损伤组及波生坦组模拟临床经皮冠状动脉形成术(PTCA)过程行左颈总动脉球囊损伤致内膜剥落,波生坦组给予波生坦100 mg·kg-1·d-1灌胃(术前1 d直至处死)。
观测术后不同时相点的内膜,中膜动态增殖情况,并采用免疫组化法检测α 平滑肌肌动蛋白(α SMA)和抗增殖细胞核抗原(PCNA)。
结果损伤组术后28 d新生内膜增生达峰值,波生坦组术后14 d内膜增生达峰值。
术后14、28、45 d波生坦组内膜面积较损伤组明显减小(P<0.001)。
术后14 d的波生坦组内膜PCNA的阳性率与损伤组比较显著降低(P<0.01)。
术后14 d α actin的阳性表达率较损伤组明显增加(P<0.01)。
结论波生坦组可通过抑制血管内膜过度增殖及减少血管平滑肌细胞的增殖,转型和迁移而有效预防PTCA术后再狭窄的发生。
一种新型大环内酯类抗菌剂-泰地罗新

一种新型大环内酯类抗菌剂-泰地罗新作者:王宏磊,刘义明,徐飞等来源:《兽医导刊》 2017年第8期泰地罗新(Tildipirosin) 是一种新型动物专用十六元环大环内酯类半合成抗生素,最早是由英特威国际有限公司(Intervet InternationalBV)开发的,为泰乐菌素的衍生物。
2011 年3 月8 日,荷兰英特威公司以泰地罗新为主要成分的无菌注射液( 商品名为Zuprevo) 通过了欧盟兽用药品委员会(CVMP) 的审批,随后在欧盟国家相继批准上市,CAS 号为328898-40-4。
现今,全球的猪、牛养殖业面临的主要问题是呼吸系统的高发病率和死亡率。
泰地罗新是广谱抗菌药,对一些革兰氏阳性和革兰氏阴性细菌均有较强的抗菌活性,对引起猪、牛呼吸系统疾病的病原菌尤其敏感。
而且具备动物专用、用量少、一次给药全程治疗、超长的消除半衰期、生物利用度高、低残留、使用安全等优点。
一、理化性质泰地罗新是一种半合成的天然泰乐菌素的衍生物,分子式为C41H71N3O8,相对分子质量为734.02,化学名为20,23- 二哌啶基-5-O- 碳霉胺糖基- 泰乐内酯,常温下为一种白色粉末,熔点为192℃,溶于极性有机溶剂( 如丙酮、甲醇等),微溶于水。
它是一种16 个环的大环内酯类抗生素,其独特的化学结构是在C20 和C23 上含有两个哌啶取代基,C5 上有一部分碳霉糖,其环上的三个N 原子易于质子化。
结构式见图1。
二、作用机制泰地罗新与其他大环内酯类药物的作用机理相同,能不可逆地与敏感菌的核糖体50S 亚基的23SrRNA 结合,抑制氨酞tRNA 的氨酸末端的结合, 进而抑制mRNA-氨酞-tRNA- 核糖的复合物的形成。
但不与哺乳动物的80S 核糖体结合,这可能是其毒性较小的原因之一。
三、药理学研究1. 抗菌活性。
泰地罗新的体外抗菌活性受pH 值的影响较大,在酸性环境时,环上的三个氨基不同程度的被质子化,使其形成不同的带电形式(0,1,2,3),导致其不溶于脂类化合物中,致使通过细菌细胞膜的能力下降,影响了抗菌效果。
新型甘氨酰四环素类抗生素——替吉环素
新型甘氨酰四环素类抗生素——替吉环素替吉环素(tigecycline,GAR-936,TygacilTM)是首个被美国FDA批准临床使用的甘氨酰四环素类抗生素,用来治疗各种复杂性腹腔内感染(complicated intra-abdominal infections,cIAI)、复杂性皮肤和皮肤结构感染(complicated skin and skin-structure infections,cSSSI),包括复杂阑尾炎、烧伤感染、腹腔内脓肿、深层软组织感染以及溃疡感染等。
1体外抗菌活性Hoban DJ等[1]在体外药敏实验中,研究了替吉环素对6 792株临床分离的革兰阴性和革兰阳性菌的抗菌活性。
研究显示:4 692株革兰阴性菌中,不动杆菌属约占10.5%,其中鲍氏不动杆菌最常见,共427株,替吉环素对不动杆菌属的MIC90为0.25~2 μg/mL,对鲍氏不动杆菌的MIC90为1 μg/mL,替吉环素对鲍氏不动杆菌的抗菌活性较阿米卡星、头孢他定、头孢曲松、亚胺培南等的抗菌活性高8倍以上;肠杆菌属共3 201株,占68.2%,替吉环素的MIC90为1 μg/mL;对产ESBL酶的大肠埃希菌、肺炎克雷伯菌、产酸克雷伯菌株,替吉环素的MIC90为2 μg/mL,仍有较高的抗菌活性。
2 100株革兰阳性菌中,粪肠球菌344株,11株为VRE,替吉环素的MIC90为0.12 μg/mL;屎肠球菌145株,77株为VRE,替吉环素的MIC90为0.06~0.25 μg/mL;金黄色葡萄球菌837株,348株为MRSA,替吉环素的MIC90为0.25 μg/mL;肺炎链球菌435株,54株为PRSP,替吉环素的MIC90为0.03~0.25 μg/mL,也都有良好的抗菌活性。
当然,体外药敏实验有效不能证明体内同样有效,需经临床实验进一步证实。
2药效学和药动学替吉环素是米诺环素的衍生物,属时间依赖型杀菌剂,抗菌谱广,对包括耐甲氧西林金黄色葡萄球菌(MRSA)、耐青霉素肺炎链球菌(PRSP)等革兰阳性菌,耐万古霉素肠球菌(VRE)及多数革兰阴性杆菌均具良好的抗菌活性。
10%盐酸土霉素可溶性粉
盐酸土霉素可溶性粉说明书
兽用非处方药
【兽药名称】通用名称:盐酸土霉素可溶性粉
商品名称:无
英文名称:Oxytetracycline Hydrochloride Soluble Powder
汉语拼音:Yansuan Tumeisu Kerongxingfen
【主要成分】盐酸土霉素。
【性状】本品为淡黄色粉末。
【药理作用】四环素类抗生素。
土霉素通过可逆性地与细菌核糖体30S亚基上的受体结合,干扰tRNA与mRNA形成核糖体复合物,阻止肽链延长而抑制蛋白质合成,从而使细菌的生长繁殖迅速被抑制。
土霉素对革兰氏阳性菌和阴性菌均有抑制作用。
细菌对土霉素和多西环素存在交叉耐药性。
【适应证】用于治疗猪、鸡敏感大肠杆菌、沙门氏菌、巴氏杆菌及支原体引起的感染性疾病。
【用法与用量】以土霉素计。
混饮:每1L水,猪100~200mg,鸡150~250mg。
连用3~5日。
【不良反应】长期应用可引起二重感染和肝脏损害。
【注意事项】1、本品不宜与青霉素类药物和含钙盐、铁盐及多价金属离子的药物或饲料合用。
2、与强利尿药同用可使肾功能损害加重。
3、不宜与含氯量多的自来水和碱性溶液混合。
4、肝功能严重受损的患畜禁用。
【休药期】猪7日;鸡5日,弃蛋期2日。
【规格】10%
【包装】500g
【贮藏】遮光,密闭,干燥处保存。
【有效期】2年
【生产日期】见喷码
【生产批号】见喷码
【有效期至】见喷码。
替米考星固体分散体在猪体内的药代动力学研究
2021年第5期(总第225期)糾畜希欢浚矗doi:10.3969/j.issn.1006-4907.2021.05.013替米考星固体分散体在猪体内的药代动力学研究唐达,伍涛※(重庆市畜牧科学院,重庆402460)摘要:研究替米考星固体分散体在猪体内的药代动力学特征,并评价其与市售替米考星肠溶颗粒的生物等效性。
釆用高效液相色谱法(HPLC)测定血浆中替来考星浓度,通过PKSolver2.0药动学程序计算药动学参数。
市售替米考星肠溶颗粒和替米考星固体分散体在猪体内的药动学行为均符合一级吸收一室模型,分别为(2.72±0.14)、(2.55±0.21)h,分别为(1.53±0.26)(1.81±0.19)|ig/mL,AUCo-oo分别为(33.31±2.19)^(45.47±2.62)小g-h/mL,替米考星固体分散体相对肠溶颗粒的相对生物利用度提高至136.5%。
结果表明,替米考星固体分散体具有更好的肠溶缓释作用及更高的生物利用度,具有一定的生物安全性,在猪体内保持药效时间更久。
关键词:替米考星;固体分散体;猪;药代动力学;生物利用度中图分类号:S859.796文献标识码:A文章编号:1006-4907(2021)05-0029-04Pharmacokinetics of Tilmicosin Solid Dispersion in SwinesTang Da,Wu Tao*(Chongq ing A cademy of A nimal Sciences,Chongqing402460,PRC.)Abstract:Study the pharmacokmetics of tilmicosin solid dispersion in pigs and evaluate its bioequivalence with commercial tilmicosin enteric coated granules.The plasma concentrations of tilmicosin were analyzed by HPLC.The pharmacokinetic parameters were calculated by PKSolver2.0pharmacokinetic program.The concentration-time curve of tilmicosin solid dispersion and commercial tilmicosin enteric coated granules were fitted a two compartment open model with first order absorption.The main pharmacokinetic parameters of were(2.72±0.14)(2.55±0.2l)h,were (1.53±0.26)(1.81±0.19)ug/ml,AUC“were(33.31±2.19)(45.47±2.62)ug»hAnl.The relative bioavailability of t ilmicosin SD group was increased to136.5%compared with enteric coated granule group.In conclusion,tilmicosin solid dispersion shows better performance of sustained release, which improves biosafety and last longer in pig.Keywords:Tilmicosin;Solid dispersion;Swine;Pharmacokinetics;Bioequivalence替米考星(Tilmicosin,TMC)是畜禽专用大环内脂类抗生素叫是预防和治疗呼吸道疾病的首选药物叫市场份额巨大%本研究选用性能稳定旳的肠溶性载体丙烯酸树脂Eudragit L100和新型两亲性非离子型共聚物网聚乙烯己内酰胺-聚乙酸乙烯酯-聚乙二醇接枝共聚物(Soluplus)为联合载体,制备了替米考星固体分散体(JMC SD),使替米考星过胃、肠溶靶向控释,有效减少口服替米考星在胃中溶解基金项目:重庆市技术创新与应用发展专项面上项目《肠溶缓释型替米考星固体分散体的创制与应用》(cstc2019jscx-msxmX0344)o 作者简介:唐达(1988-),男,重庆荣昌人,助理研究员,硕士,研究方向:兽药制剂,***************。
盐酸氨溴索对胸部外科手术致PS 下降的保护作用
材料和方法
=>>> 年 =? 月至 ?@@@ 年 A 月中山医 院胸外科开左胸行食管癌根治术主动脉弓上吻合术 患者 ?B 例, 男性 ?@ 例, 女性 B 例, 年龄 B? C DE 岁, 平 均 F= G ?A 岁。随 机 分 成 实 验 组 =@ 例 和 对 照 组 =B 例。所有患者均无原发肺部疾病, 术前胸部 H 线检 查无异常。两组间术前肺功能 I<、 1JI= 、 1JI =K 及 血气分析 ! ), (" ! ), L? 、 <L? 及手术时间均无显著差异 (表 =) 。 M @ G @A)
动物实验及人体研究表明, 开胸手术由于机械 通气、 手术挤压等原因造成肺损伤及肺泡表面活性 物质 (QJ,’*D&)O LJ)R&N2&D2, 下降, 是产生术后肺不 $%) [.] 张等并发症的主要原因 。盐酸氨溴索 ( &’()*+*,, 万方数据
商品名: 沐舒坦, 可刺激肺泡 ! 型上皮细 ’JN*LJ,K&D)
入 ?K 利多卡因, 静脉泵入咪唑安定每小时 =A@ ! -V 间断静脉给予维库溴铵维持, 不用任何吸入全麻 R-, 药。气管插管后行机械通气, I7 W =@ P* V R-, XX W =@ 次 V P5%, 术中监 测 ;3L? 、 15L? W = G @, N Y J W = Y ?, J7& 维持循环稳定。 <L? , 给药方法 实验组术前 ! 天给予每日静脉滴注 盐酸氨溴索 = ( 。对照组不用 - .$,(#5%-,# N%-,#(,5P) 任何呼吸药物。 标本采集及处理 手术前气管插管后及手术结 束拔除气管插管前, 分别用 L*:P394 .1?@ 型纤维支 气管镜行右肺中叶 (非手术侧) 及左肺上叶舌段 (手 术侧) 支气管肺泡灌洗 ( ./0) , 其中为防止灌洗的稀 释作用, 术前分别灌洗右肺中叶内侧段和左肺上舌 段, 术后分别灌洗右肺中叶外侧段和左肺下舌段。 每次灌入 !DZ 生理盐水 A@ P*, 通气 ? P5% 后用负压 (! G !! C =! G ! R8)) , 抽吸至无菌容器, 收集灌洗液。 重复灌洗 ? 次, 总灌入量 =@@ P*。收集的 ./01 以 ? 层无菌纱布过滤后以 = A@@ V P5% 离心 =@ P5%, 分离出 上清液分装后置 [ F@Z 保存待测定。 分 别 采 用 .)#2*,2, \)4$% 和 改 良 ( 780) , 饱和卵磷脂 ( ;)28<) 和总 0$U#: 法测定总磷脂 蛋白 ( 78) 。为修正因肺泡灌洗液对 8; 稀释程度的 不同所致偏差, 取 ;)28< V 780 和 ;)28< V 78 比值作为 判断 8; 活性水平的指标。 组内比较采用配对 # 检验, 组间 比较采用等方差 # 检验。 统计学处理 测定 方 法
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
J. vet. Pharmacol. Therap. 19, 225-232, 1996.
SYSTEMIC PHARMACOLOGY
Cardiovascular effects of the macrolide antibiotic tilmicosin, administered alone and in combination with propranolol or dobutamine, in conscious unrestrained dogs
B. W. MAIN Main, B.W., Means, J.R., Rinkema, L.E., Smith, W.C., Sarazan, R.D.
Cardiovascular effects of the macrolide antibiotic tilmicosin, administered alone J. R. MEANS
and in combination with propranolol or dobutamine, in conscious unrestrained
dogs. J. vet. Pharmacol. Therap. 19, 225-232. L. E. RINKEMA
W. C. SMITH &
R. D. SARAZAN
Tilmicosin(TM), a macrolide antibiotic and active ingredient in formulated
Micotil 300m (Eli Lilly and Co., Indianapolis, IN. USA), is the active ingredient Lilly Research Laboratories, Greenfield, IN
in a formulated animal product used for the treatment of respiratory tract
46140, USA infections in cattle. Owing to the concern of governmental regulatory agencies
over the possibility of an accidental injection of the antibiotic to a livestock handler, the cardiovascular effects of sub lethal doses of TM were evaluated in
conscious mixed-breed dogs. Left ventricular function, systemic arterial blood pressure, and heart rate (HR) responses to TM alone and in combination with propranolol(P) or dobutamine HCI(D0B) were evaluated. Dogs were instru- mented with indwelling micromanometers implanted in the left ventricular chamber and in the thoracic aorta. Cardiovascular variables were recorded, and the peak value of the first derivative of left ventricular pressure (dp/dt(,,,,) was used as an index of left ventricular inotropic state. Six treatments were randomly assigned to each of the six dogs using a Latin square design. The six treatments were vehicle, TM alone (2.5 mg/kg of body weight), TM
immediately followed by P, and TM immediately followed by 1 of 3 dosages
of DOB infused for ~45 min. Additionally, doses of
TM alone (0.25. 1.0, 2.5,
and 5.0 mg/kg) were administered to complete a dose-response curve. TM caused dose dependent decreases in (dp/dt(,,,,) and aortic pulse pressure. HR increased dose-dependently. Left ventricular end-diastolic pressure increased at the 2.5 and 5.0 mg/kg dosages. Left ventricular systolic pressure was reduced
dose-dependently at the 2.5 and 5.0 mg/kg dosages. Treatment with P
exacerbated the negative inotropic effect and the decrease in left ventricular systolic pressure, but did not attenuate the tachycardia associated with TM treatment. DOB attenuated the changes in ventricular inotropic state in a dose-
dependent manner. DOB infusion also restored left ventricular systolic pressure at dosages of 3 or 10 pg/min/kg. Our data indicate that toxic doses of TM may
have a negative inotropic effect in conscious dogs. HR increased in a dose- dependent manner and was not the result of (31-receptor stimulation. DOB reversed some, but not all, of the effects caused by TM administration.
(Paper received 31 October 1994; accepted for publication 18 December 1995)
Bradley W. Main, Lilly Research Laboratories, Drop GL45, PO Box 708, Greenfield IN, 46140, USA
INTRODUCTION Tilmicosin is a macrolide antibiotic intended for use in the treatment of bacterial infections in livestock. The antibiotic is intended for subcutaneous (SC) administration in cattle with respiratory tract infections. Initial toxicologic data indicated that lethal doses were accompanied by an increase in HR and an apparant loss of ventricular function. The present study was designed with regard to discussions with European regulatory agencies, who expressed concerns about the accidental injection of formulated antibiotic to a livestock handler. The purpose of the present study was to provide detailed data
01996 Blackwell Science Ltd 225 226 B.W. Main
et al.
on the effects of a sub lethal dose (2.5 mg/kg body weight) of tilmicosin alone or in combination with a positive inotrope (dobutamine HCI). A p-adrenergic antagonist (propranolol) was also used to rule out P-agonist activity, as earlier studies that
monitored only HR indicated that HR increased after tilmicosin administration. Additionally. dosages of 0.25. 1.0, 2.5. and 5.0 mg/kg were used to determine the dose-related effects of the compound. MATERIALS AND METHODS Dogs and surgical preparation Mixed-breed dogs (1 1-18.7-months-old) were obtained from a commercial breeder. Mean body weight was 18.3 kg. Dogs were conditioned to canvas jackets, plastic Elizabethan collars, and flexible metal tethers for a minimum of 2 days before surgery. Injectable antibiotic was administered 1 day before surgery. General anaesthesia was induced with a 2% solution of an ultrashort-acting anesthetic (Brevital@ Eli LiUy and Co. India- napolis, IN, USA), 0.5 mL/kg given i.v. to egect. Anesthesia was maintained with isoflurane in 100% 02. A left-sided thoracotomy was performed with each dog positioned in right lateral recumbency. A micromanometer (Konigsberg Inc, Pasadena, CA. USA) was implanted in the descending thoracic aorta through a stab incision and was tied in place, using purse-string sutures of synthetic, non-absorbable suture material. Next, the pericardium was opened and partially resected. A second micromanometer was implanted in the left ventricular chamber through a stab incision in the ventricular apex and was tied in place, using a purse-string suture. The thorax was closed in several layers, and the instrument wires were routed subcutaneously to their exit point between the scapulae. Silver electrodes were implanted SC in the right shoulder and the left hip to record ECG. A sterile cannula was placed in a femoral vein and exteriorized through an incision on the dorsal surface of the dog, near the instrumentation wires. The cannula and wires were routed to a specially designed pocket on the dog's jacket. Post-operative analgesics were administered during and after recovery from general anaesthe- sia, as required for signs of pain. Antibiotic therapy was continued for 4 days after surgery. Each cannula was flushed with heparinked saline solution (5 U of heparin/mL) at least once daily to maintain cannula patency. All dogs were allowed at least 2 weeks to recover from any surgical procedure prior to dosing and data collection. Treatment groups The study was conducted in 2 segments. In phase 1. six dogs were assigned at random to 6 treatment orders, using a Latin square design. The dose of tilmicosin remained fixed at 2.5 mg/ kg. The 6 treatments were vehicle. tilmicosin alone, tilmicosin immediately followed by propranolol treatment, and tilmicosin followed by 1 of 3 dosages of dobutamine HCI infused for ~45 min. In phase 2 of the study, doses of 0.25, 1.0. and 5.0 mg/kg were administered to obtain dose-response informa- tion. The dosing regimen was as follows: Treatment Compounds Adminiskred Intravenously Treatment. 2.5 mg/kg tilmicosin; 2.5 mg/kg tilmicosin + 1 pg/ min/kg dobutamine HCI: 2.5 mg/kg tilmicosin + 3 pg/min/kg