偏头痛诊断标准
偏头痛诊断及中医分型辨证治疗

中医药治疗7.1分型论治7.1.1瘀阻脑络型:偏头痛偏于头部一侧,呈现痛如锥刺,痛处固定,日轻夜重,病程较长,反复发作,经久不愈,健忘心悸,妇女有月经失调,舌质紫暗,脉弦涩。
治则:通窍化瘀,止痛。
拟方:通窍活血汤(郁金、菖蒲、当归、丹参、白芍、川芎、蔓荆子、菊花、白芷、甘草)。
7.1.2风客脑络型:偏头痛偏于头部一侧或全头痛,呈现痛因风寒而诱发,呈跳痛或掣痛,舌淡红苔薄白,脉弦而紧。
治则:通窍疏风,活络止痛。
拟方:通窍疏风汤(郁金、菖蒲、丹参、白芍、川芎、蔓荆子、防风、羌活、木瓜、秦艽、白芷、甘草)。
7.1.3肝气郁结型: 偏头痛偏于头部一侧,呈胀痛伴眩暈,心烦失眠,两胁串痛,每因情绪激动、恼怒而诱发,口苦,舌淡紅苔白,脈弦。
治则:通窍解郁,止痛。
拟方:通窍解郁汤(郁金、菖蒲、当归、柴胡、香附、夏枯头、白芍、川芎、蔓荆子、白芷、甘草)。
7.1.4肝阳上亢型:偏头痛偏于头部一侧,呈胀痛或抽掣痛,痛时面红耳鸣,心烦易怒,舌红少苔,脉弦细而数。
治则:通窍潜阳,熄风止痛。
拟方:通窍熄风汤(郁金、菖蒲、当归、石决明、生龙牡、白芍、川芎、蔓荆子、天麻、菊花、夏枯草、甘草)。
7.1.5痰浊上蒙型:偏头痛偏于头部一侧,呈沉重而昏蒙,胸脘满闷,呕恶纳呆,吐痰涎,舌苔白腻,脉弦滑。
治则:通窍化痰,降逆止痛。
拟方:通窍祛痰汤(半夏、胆南星、茯苓、陈皮、白术、天麻、郁金、菖蒲、川芎、蔓荆子、白芷、甘草)。
7.1.6肝肾阴虚型:偏头痛偏于头部一侧,呈现时轻时重,脑空耳鸣,腰膝酸软,咽干口燥,心烦失眠,舌红少苔,脉弦细数。
治则:通窍益阴,止痛。
拟方:通窍益阴汤(郁金、菖蒲、女贞子、旱莲草、山萸肉、枸杞、丹参、赤芍、川芎、蔓荆子、天麻、菊花、甘草)。
7.1.7气血两虚型:偏头痛偏于头部一侧,痛而乏力,遇劳加剧,汗出气短,畏风怕冷;痛而且晕,心悸不宁,面色少华,神疲,舌质淡、苔薄白,脉细弱。
治则:益气养血,固本止痛,拟方:通窍双补汤(郁金、菖蒲、党参、黄芪、白术、熟地黄、当归、丹参、白芍、川芎、蔓荆子、白芷、甘草)。
头痛的国际分类(第三版)中文
The international Classification of Headache disorders, 3rd Editon2.1.2 Infrequent episodic tension-type headache not associated with pericranial tenderness2.2.1 Frequent episodic tension-type headache associated with pericranial tenderness2.2.2 Frequent episodic tension-type headache not associated with pericranial tenderness2.3.2 Chronic tension-type headache not associated with pericranial tenderness3.3.1 Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) 3.3.1.1 Episodic SUNCT3.3.1.2 Chronic SUNCT3.3.2 Short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms (SUNA)3.3.2.1 Episodic SUNA3.3.2.2 Chronic SUNA3.4 Hemicrania continua3.5 Probable trigeminal autonomic cephalalgia3.5.1 Probable cluster headache3.5.2 Probable paroxysmal hemicrania3.5.3 Probable short-lasting unilateral neuralgiform headache attacks3.5.4 Probable hemicrania continua4.其它的原发性头痛Other primary headache disorders )4.1 Primary cough headache原发性咳嗽头痛4.1.1 Probable primary cough headache4.2 Primary exercise headache原发性运动性头痛4.2.1 Probable primary exercise headache4.3 Primary headache associated with sexual activity原发性性活动伴随的头痛4.3.1 Probable primary headache associated with sexual activity4.4 Primary thunderclap headache原发性霹雳头痛4.5 Cold-stimulus headache冷刺激性头痛4.5.1 Headache attributed to external application of a cold stimulus4.5.2 Headache attributed to ingestion or inhalation of a cold stimulus4.5.3 Probable cold-stimulus headache4.5.3.1 Headache probably attributed to external application of a cold stimulus4.5.3.2 Headache probably attributed to ingestion or inhalation of a cold stimulus则可两者均可作为诊断4.10 New daily persistent headache (NDPH) 新症每日持续性头痛4.10.1 Probable new daily persistent headach二、继发性头痛(the secondary headaches)5.缘于头、颈部外伤的头痛(Headache attributed to trauma or injury to the head and/or neck)5.1 Acute headache attributed to traumatic injury to the head5.1.1 Acute headache attributed to moderate or severe traumatic injury to the head5.1.2 Acute headache attributed to mild traumatic injury to the head5.2 Persistent headache attributed to traumatic injury to the head5.2.1 Persistent headache attributed to moderate or severe traumatic injury to the head5.2.2 Persistent headache attributed to mild traumatic injury to the head5.3 Acute headache attributed to whiplash5.4 Persistent headache attributed to whiplash5.5 Acute headache attributed to craniotomy5.6 Persistent headache attributed to craniotomy6.缘于头颈部血管疾病的头痛(Headache attributed to cranial or cervical vascular disorder )6.1 Headache attributed to ischaemic stroke or transient ischaemic attack6.1.1 Headache attributed to ischaemic stroke (cerebral infarction)6.1.2 Headache attributed to transient ischaemic attack (TIA)6.2 Headache attributed to non-traumatic intracranial haemorrhage6.2.1 Headache attributed to non-traumatic intracerebral haemorrhage非外伤性脑出血6.2.2 Headache attributed to non-traumatic subarachnoid haemorrhage (SAH)6.2.3 Headache attributed to non-traumatic acute subdural haemorrhage (ASDH)急性硬膜下血肿6.3 Headache attributed to unruptured vascular malformation未破裂的血管畸形6.3.1 Headache attributed to unruptured saccular aneurysm囊性动脉瘤6.3.2 Headache attributed to arteriovenous malformation (AVM) 动静脉畸形6.3.3 Headache attributed to dural arteriovenous fistula (DAVF) 硬膜动静脉瘘6.3.4 Headache attributed to cavernous angioma 海绵窦血管瘤6.3.5 Headache attributed to encephalotrigeminal or leptomeningeal angiomatosis (Sturge Weber syndrome)脑三叉神经或软脑膜血管瘤病6.4 Headache attributed to arteritis6.4.1 Headache attributed to giant cell arteritis (GCA) 颞动脉炎6.4.2 Headache attributed to primary angiitis of the central nervous system (PACNS)6.4.3 Headache attributed to secondary angiitis of the central nervous system (SACNS)6.7.1 Headache attributed to an intracranial endovascular procedure6.7.2 Angiography headache6.7.3 Headache attributed to reversible cerebral vasoconstriction syndrome (RCVS)6.7.3.1 Headache probably attributed to reversible cerebral vasoconstrictionsyndrome (RCVS)6.7.4 Headache attributed to intracranial arterial dissection颅内动脉夹层6.8 Headache attributed to genetic vasculopathy6.8.1 Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL)6.8.2 Mitochondrial Encephalopathy, Lactic Acidosis and Stroke-like episodes (MELAS)6.8.3 Headache attributed to another genetic vasculopathy6.9 Headache attributed to pituitary apoplexy垂体卒中7.缘于非血管性颅内疾病的头痛(Headache attributed to non-vascular intracranial disorder )7.1 Headache attributed to increased cerebrospinal fluid pressure颅内压增高7.1.1 Headache attributed to idiopathic intracranial hypertension (IIH)7.1.2 Headache attributed to intracranial hypertension secondary to metabolic, toxic or hormonal causes7.1.3 Headache attributed to intracranial hypertension secondary to hydrocephalus7.2 Headache attributed to low cerebrospinal fluid pressure颅内压低下7.2.1 Post-dural puncture headache腰穿后7.2.2 CSF fistula headache脑脊液漏7.2.3 Headache attributed to spontaneous intracranial hypotension自发性低颅压7.3 Headache attributed to non-infectious inflammatory disease非感染性炎性疾病7.3.1 Headache attributed to neurosarcoidosis7.3.2 Headache attributed to aseptic (non-infectious) meningitis7.3.3 Headache attributed to other non-infectious inflammatory disease7.3.4 Headache attributed to lymphocytic hypophysitis7.3.5 Syndrome of transient Headache and Neurological Deficits with cerebrospinal fluid Lymphocytosis (HaNDL)7.4 Headache attributed to intracranial neoplasia颅内新生物7.4.1 Headache attributed to intracranial neoplasm7.4.1.1 Headache attributed to colloid cyst of the third ventricle7.4.2 Headache attributed to carcinomatous meningitis癌性脑膜炎7.4.3 Headache attributed to hypothalamic or pituitary hyper- or hyposecretion7.5 Headache attributed to intrathecal injection鞘内注射7.6 Headache attributed to epileptic seizure7.6.1 Hemicrania epileptica癫痫半颅痛7.6.2 Post-ictal headache癫痫发作后头痛7.7 Headache attributed to Chiari malformation type I (CM1)7.8 Headache attributed to other non-vascular intracranial disorder8.缘于物质或物质戒断的头痛(Headache attributed to a substance or its withdrawal)8.1 Headache attributed to use of or exposure to a substance or its withdrawal缘于某种物质的应用或戒断8.1.1.2 Delayed NO donor-induced headache8.1.2 Phosphodiesterase (PDE) inhibitor-induced headache磷酸二酯酶抑制剂8.1.3 Carbon monoxide (CO)-induced headache一氧化碳诱发8.1.4 Alcohol-induced headache酒精诱发8.1.4.1 Immediate alcohol-induced headache8.1.4.2 Delayed alcohol-induced headache8.1.5 Headache induced by food and/or additive由于食物成分/添加剂诱发8.1.5.1 Monosodium glutamate (MSG)-induced headache谷氨酸单钠盐(味精)8.1.6 Cocaine-induced headache可卡因诱发8.1.7 Histamine-induced headache组织胺诱发8.1.7.1 Immediate histamine-induced headache8.1.7.2 Delayed histamine-induced headache8.1.8 Calcitonin gene-related peptide (CGRP)-induced headache降钙素基因相关多肽诱发8.1.8.1 Immediate CGRP-induced headache8.1.8.2 Delayed CGRP-induced headache8.1.9 Headache attributed to exogenous acute pressor agent8.1.10 Headache attributed to occasional use of non-headache medication8.1.11 Headache attributed to long-term use of non-headache medication8.1.12 Headache attributed to exogenous hormone8.1.13 Headache attributed to use of or exposure to other substance8.2.4 Opioid-overuse headache鸦片类8.2.5 Combination-analgesic-overuse headache复合制剂过度应用8.2.6 Medication-overuse headache attributed to multiple drug classes not individually over used联合用药所致8.2.7 Medication-overuse headache attributed to unverified overuse of multiple drug classes8.2.8 Medication-overuse headache attributed to other medication8.3 Headache attributed to substance withdrawal物质戒断8.3.1 Caffeine-withdrawal headache咖啡因8.3.2 Opioid-withdrawal headache鸦片类8.3.3 Oestrogen-withdrawal headache雌激素8.3.4 Headache attributed to withdrawal from chronic use of other substance9.缘于感染的头痛(Headache attributed to infection)9.1 Headache attributed to intracranial infection颅内感染9.1.1 Headache attributed to bacterial meningitis or meningoencephalitis细菌性脑膜炎/脑膜脑炎9.1.1.1 Acute headache attributed to bacterial meningitis or meningoencephalitis9.1.1.2 Chronic headache attributed to bacterial meningitis or meningoencephalitis9.1.1.3 Persistent headache attributed to past bacterial meningitis or meningoencephalitis9.1.2 Headache attributed to viral meningitis or encephalitis病毒性脑膜炎或脑炎9.1.2.1 Headache attributed to viral meningitis9.1.2.2 Headache attributed to viral encephalitis9.1.3 Headache attributed to intracranial fungal or other parasitic infection真菌或寄生虫感染9.1.3.1 Acute headache attributed to intracranial fungal or other parasitic infection9.1.3.2 Chronic headache attributed to intracranial fungal or other parasitic infection9.1.4 Headache attributed to brain abscess脑脓肿9.1.5 Headache attributed to subdural empyema硬膜下积脓9.2 Headache attributed to systemic infection系统感染9.2.1 Headache attributed to systemic bacterial infection系统细菌感染9.2.1.1 Acute headache attributed to systemic bacterial infection9.2.1.2 Chronic headache attributed to systemic bacterial infection9.2.2 Headache attributed to systemic viral infection系统病毒感染9.2.2.1 Acute headache attributed to systemic viral infection9.2.2.2 Chronic headache attributed to systemic viral infection9.2.3 Headache attributed to other systemic infection其他系统感染9.2.3.1 Acute headache attributed to other systemic infection9.2.3.2 Chronic headache attributed to other systemic infection10.缘于内环境紊乱的头痛(Headache attributed to disorder of homoeostasis)10.1 Headache attributed to hypoxia and/or hypercapnia缺氧和/或高碳酸血症10.1.1 High-altitude headache高海拔头痛10.1.2 Headache attributed to aeroplane travel飞行头痛10.1.3 Diving headache潜水头痛10.1.4 Sleep apnoea headache睡眠呼吸暂停性头痛10.2 Dialysis headache10.3 Headache attributed to arterial hypertension高血压性头痛10.3.1 Headache attributed to phaeochromocytoma嗜络细胞瘤10.3.2 Headache attributed to hypertensive crisis without hypertensive encephalopathy无高血压脑病的高血压危象10.3.3 Headache attributed to hypertensive encephalopathy高血压脑病10.3.4 Headache attributed to pre-eclampsia or eclampsia先兆子痫10.3.5 Headache attributed to autonomic dysreflexia自主反射障碍10.4 Headache attributed to hypothyroidism甲状腺低下10.5 Headache attributed to fasting禁食10.6 Cardiac cephalalgia心源性头痛10.7 Headache attributed to other disorder of homoeostasis其他内环境稳定失调疾患11.缘于头、颈、眼、耳、鼻、鼻窦、牙、口或其他头面部结构病变的头面痛(Headache or facial pain attributed to disorder of the cranium, neck,eyes, ears, nose, sinuses, teeth, mouth or other facial or cervical structure )11.1 Headache attributed to disorder of cranial bone颅骨11.2 Headache attributed to disorder of the neck 颈部11.2.1 Cervicogenic headache11.2.2 Headache attributed to retropharyngeal tendonitis11.2.3 Headache attributed to craniocervical dystonia11.3 Headache attributed to disorder of the eyes眼睛11.3.1 Headache attributed to acute glaucoma急性青光眼11.3.2 Headache attributed to refractive error屈光不正11.3.3 Headache attributed to heterophoria or heterotropia (latent or persistent squint)斜视11.3.4 Headache attributed to ocular inflammatory disorder11.3.5 Headache attributed to trochleitis11.4 Headache attributed to disorder of the ears耳朵11.5 Headache attributed to disorder of the nose or paranasal sinuses鼻子或鼻窦11.5.1 Headache attributed to acute rhinosinusitis急性鼻窦炎11.5.2 Headache attributed to chronic or recurring rhinosinusitis11.6 Headache attributed to disorder of the teeth or jaw11.7 Headache attributed to temporomandibular disorder (TMD)11.8 Head or facial pain attributed to inflammation of the stylohyoid ligament11.9 Headache or facial pain attributed to other disorder of cranium, neck, eyes, ears, nose,sinuses, teeth, mouth or other facial or cervical structure12.缘于精神疾病的头痛(Headache attributed to psychiatric disorder)12.1 Headache attributed to somatization disorder躯体化障碍12.2 Headache attributed to psychotic disorder精神疾病三、脑神经痛、中枢和原发性颜面痛及其他头痛(painful cranial neuropathies, other facial pains and other headaches)13.脑神经痛和中枢性颜面痛(Painful cranial neuropathies and other facial pains)13.1 Trigeminal neuralgia三叉神经痛13.1.1 Classical trigeminal neuralgia13.1.1.1 Classical trigeminal neuralgia, purely paroxysmal13.1.1.2 Classical trigeminal neuralgia with concomitant persistent facial pain13.1.2 Painful trigeminal neuropathy13.1.2.1 Painful trigeminal neuropathy attributed to acute Herpes zoster13.1.2.2 Post-herpetic trigeminal neuropathy13.1.2.3 Painful post-traumatic trigeminal neuropathy13.1.2.4 Painful trigeminal neuropathy attributed to multiple sclerosis (MS) plaque13.1.2.5 Painful trigeminal neuropathy attributed to space-occupying lesion13.1.2.6 Painful trigeminal neuropathy attributed to other disorder13.2 Glossopharyngeal neuralgia舌咽神经痛13.3 Nervus intermedius (facial nerve) neuralgia中间神经痛(面神经痛)13.3.1 Classical nervus intermedius neuralgia13.6 Headache attributed to ischaemic ocular motor nerve palsy缺血性眼神经麻痹13.7 Tolosa-Hunt syndrome13.8 Paratrigeminal oculosympathetic (Raeder’s) syndrome13.9 Recurrent painful ophthalmoplegic neuropathy复发性痛性眼肌麻痹13.10 Burning mouth syndrome (BMS)13.11 Persistent idiopathic facial pain (PIFP)13.12 Central neuropathic pain中枢神经痛13.12.1 Central neuropathic pain attributed to multiple sclerosis (MS)13.12.2 Central post-stroke pain (CPSP)14. 其他头痛(Other headache disorders)。
偏头痛诊断与防治专家共识

偏头痛诊断与防治专家共识一、偏头痛的相关概念偏头痛特征是发作性的、多为偏侧的、中重度、搏动样头痛,一般持续4~72小时,可伴有恶心、呕吐,光、声或活动可加重头痛,安静环境中休息则可缓解头痛。
先兆指发生在头痛之前或伴随头痛一起发生的完全可逆的局灶性神经系统症状,表现为视觉、感觉、言语、运动等的缺损或刺激症状。
大多数先兆为视觉症状,常为双眼同向症状,如视物模糊、暗点、闪光、亮点亮线或视物变形。
感觉症状多呈面-手区域分布。
先兆症状一般在5~20min内逐渐形成,持续不超过60min。
不同先兆可以接连出现。
偏头痛是一种常见和慢性的神经血管病疾患,患病率为5%~10%,儿童期和青春期起病,中青年期达发病高峰,女性多见,常有遗传背景。
偏头疼主要有无先兆偏头痛(普通型偏头痛)和有先兆偏头痛(经典型偏头痛)。
以往曾将偏头痛诊断为“血管性头痛”、“神经性头痛”或“血管神经性头痛”。
1988年后,国际头痛学会(IHS)就不再推荐使用。
二.偏头痛的分类2004年IHS将偏头痛归为原发性头痛,包括6个亚型,以无先兆偏头痛和有先兆偏头痛为常见。
三、偏头痛的诊断偏头痛的诊断主要依据临床表现如头痛的部位、性质、程度、持续时间、伴随症状、先兆表现以及活动对头痛的影响。
在临床实践中,首先要排除继发性头痛,然后再考虑是否有其他类型的原发性头痛。
出现以下情况要进行神经影象学检查:①异常的神经系统检查发现;②头痛频率或程度的急性加重;③头痛性质变化;④50岁后新发的头痛或突然发生的剧烈头痛;⑤多种治疗无效的头痛;⑥有头晕、麻木等其他症状。
脑电图、TCD等检查不推荐作为常规诊断检查。
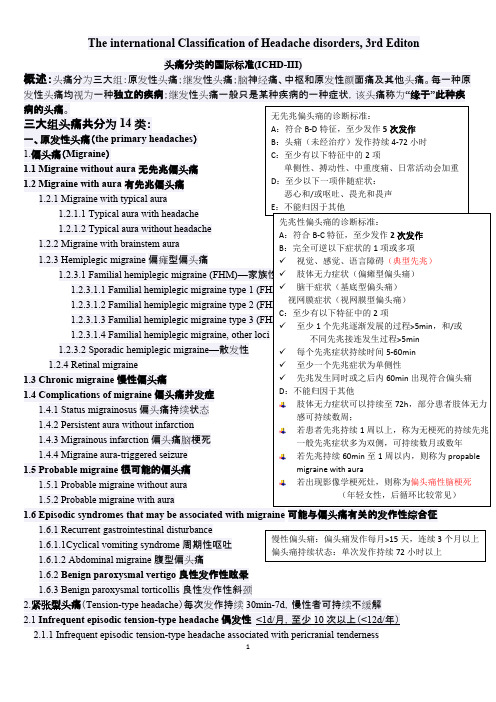
无先兆偏头痛的诊断标准:A.符合B—D项特征的至少5次发作;B.头痛发作(未经治疗或治疗无效)持续4~72h;C.至少有下列中的2项头痛特征:①单侧性,②搏动性,③中或重度疼痛,④日常活动会加重头痛或头痛时避免此类活动;D.头痛过程中至少伴随下列1项:①恶心和/或呕吐,②畏光和畏声。
masld的诊断标准

MASD的诊断标准如下:一、偏头痛(migraine )诊断标准:1. 具有≥5 次每月的头痛发作,发作时伴有恶心、呕吐、畏光和/或声光敏感;2. 发作时间在至少72 小时及以上,有间歇期;3. 排除症状性(继发性)偏头痛(如颅内血肿、脑肿瘤等)。
二、有先兆的偏头痛(ACMAS ) :除了满足上述对偏头痛的诊断标准外,还需要具有至少一次典型的偏头痛,同时具有至少一次的典型偏头痛发作过程中的先兆症状。
先兆可以是视觉、感觉或言语的丧失,或特定的感知异常。
三、儿童青少年期发作者需考虑的其他诊断:在考虑偏头痛时,医生应排除其他可能的神经系统疾病。
例如,对于儿童和青少年(<18 岁)患者,除了要考虑焦虑、应激和其他躯体疾病外,还要考虑是否存在学习压力、学校恐惧症等心理因素。
此外,还应考虑是否存在以下疾病:周期性综合征、癫痫、脑积水、脑肿瘤、光敏感性头痛和创伤等。
四、临床类型:1. 典型偏头痛(典型为有先兆的偏头痛):普通型偏头痛和特殊类型偏头痛(如:丛集性头痛和偏瘫性偏头痛);2. 不典型偏头痛:包括眼疲劳、易怒和肌肉痛性偏头痛等;3. 复杂型偏头痛:在诊断复杂型偏头痛时,需考虑是否存在视觉异常症状。
五、混合型偏头痛:在典型的先兆同时出现非典型先兆的情况下,诊断为混合型偏头痛。
六、伴随症状:在诊断过程中,伴随症状也是重要的参考指标。
例如,对于儿童患者来说,伴随的睡眠障碍可能是偏头痛发作的预警信号。
伴随症状包括但不限于恶心、呕吐、畏光和声光敏感等。
七、鉴别诊断:除了上述心理因素外,还需与其他可能影响儿童和青少年健康的情况进行鉴别,如低血糖症、尿毒症、高血钙等代谢性脑病;以及各种器质性神经系统疾病,如脑肿瘤、脑积水等。
以上就是MASD的诊断标准,希望对您有所帮助。
偏头痛的诊断标准

偏头痛的诊断标准
根据国际头痛学会(International Headache Society)制定的《头痛分类和诊断标准》(ICHD-3)中,偏头痛的诊断标准如下:
1.特发性偏头痛(Migraine without aura)的诊断标准:
- 至少发作五次以上符合下列特征的头痛发作:
a. 持续4-72小时(未经治疗或治疗效果不佳);
b. 头痛为脉冲样、搏动性的;
c. 头痛严重程度适中或重度,影响日常活动;
d. 伴随恶心、呕吐、光过敏或声过敏;
e. 头痛加重或活动加重头痛;
- 排除其他疾病的头痛。
2.特发性偏头痛(Migraine with aura)的诊断标准:
- 至少发作两次以上符合下列特征的头痛发作:
a. 具有可逆性的视觉、感觉性、语言或运动性神经系统症状,通常持续不超过一小时;
b. 头痛在神经系统症状发生后60分钟内开始,或在神经系统症状已解除的48小时内开始;
- 上述神经系统症状不是脑血管疾病的结果;
- 排除其他疾病的头痛。
值得注意的是,以上诊断标准仅适用于成年人。
对于儿童和青少年,诊断标准略有不同。
如果遇到偏头痛症状,最好咨询医生进行详细的病史询问和身体检查,并根据相关诊断标准进行判断。
偏头痛症状及分类有哪些?
偏头痛症状及分类有哪些?偏头痛症状有哪些1.先兆性偏头痛常伴恶心、呕吐、畏光或畏声、易激惹、气味恐怖及疲劳感等,可见颞动脉突出,头颈部活动使头痛加重,睡眠后减轻。
大多数患者头痛发作时间为2小时至1天,儿童持续2~8h。
头痛频率不定,50%以上的患者每周发作不超过1次。
女性患者在妊娠第2周或第三个季度及绝经后常见发作缓解。
其次为躯体感觉先兆,如一侧肢体和(或)面部麻木、针刺感和感觉异常等;运动先兆较少可表现单肢无力;也可出现轻度意识模糊、症状轻微的失语、头晕、步态不稳和倦睡等。
2.无先兆的偏头痛也称普通偏头痛,是临床最常见类型,约占偏头疼患者的80%,鲜有家族史。
缺乏典型的先兆,少数患者可出现轻微而短暂的视觉模糊。
常为反复发作的双侧颞部及眶周疼痛,可为搏动性,疼痛持续时伴颈肌收缩可使症状复杂化。
发作时常有头皮触痛,呕吐偶可使头痛终止。
头痛持续时间较长,可达数日。
发作期间或发作后通常无神经系统体征。
普通和典型偏头痛的一种有用的床边检查是,压迫同侧颈动脉或颞浅动脉可使头痛程度减轻。
药物可以部分控制的偏头痛一般不会限制患者的日常活动,随着年龄的增长,头痛程度可逐渐减轻,发作次数也逐渐减少。
3.特殊类型偏头痛偏头痛发作期或头痛消退后可伴明显的神经功能缺损,包括偏瘫、偏侧感觉缺失、失语或视觉障碍等。
(1)偏瘫型偏头痛临床少见,多在儿童期发病。
偏瘫可为偏头痛的先兆症状,可单独发生,亦可伴偏侧麻木、失语、偏头痛消退后偏瘫可持续10分钟至数周不等。
部分婴幼儿有偏瘫而无头痛,间隔数周出现交替性偏瘫,可完全恢复,不遗留任何神经系统症状。
(2)基底型偏头痛较多见于儿童和青春期女性,多有家族史,发作与月经周期有关。
出现头重脚轻、眩晕、复视、眼球震颤、耳鸣、构音障碍、双侧肢体麻木及无力、共济失调、意识改变、跌倒发作和黑目蒙、视野缺损等视觉先兆,先兆症状持续20~30min,然后出现枕部搏动性头痛,常伴恶心,呕吐。
(3)复杂型偏头痛症状同有先兆的偏头痛,先兆在头痛发作过程中仍然持续存在,延续时间在1小时至l周之内。
中国偏头痛诊治指南要点
中国偏头痛诊治指南要点一、诊断标准:1.头痛符合偏头痛特点:重度、搏动性、阵发性头痛、单侧或交替性头痛、头痛持续4-72小时。
2.至少两种头痛特异症状(恶心、呕吐、光过敏、声音过敏)。
3.排除其他原因引起的头痛,如颅内病变、颈椎病、心脑血管疾病等。
二、分类和分级:根据头痛特征和症状分为偏头痛无特异症状、偏头痛合并其他疾病、慢性偏头痛三类。
根据发作频率分为低频偏头痛(每月<15天)和高频偏头痛(每月≥15天)。
三、非药物治疗:1.生活方式调整:保持规律作息、避免过度劳累和精神紧张、避免过度饮食和酗酒、避免过度用眼、维持适当体重、定期进行有氧运动。
2.采用行为治疗:放松训练、认知行为治疗、生物香精油疗法等。
3.饮食与补充剂:避免食物和饮料引起偏头痛的触发因素,如巧克力、咖啡、红葡萄酒等,适当补充镁、维生素B2、叶酸等。
四、急性治疗:1.非麻醉类止痛药:乙酰氨基酚、阿司匹林、布洛芬等。
2.麻醉类止痛药:布洛米芬、舒芬太尼、依托咪酯等。
3.三联药物:三联药物包括三氟拉嗪、阿米替林和咖啡因。
4.抗血管活性药物:三唑酮等。
5.滋补肝肾药物:肉桂附子丸、细辛颗粒等。
五、预防治疗:1.一线药物:甲氧硝酮、丙戊酸钠、地尔硫卓、托吡酯等。
2.二线药物:普鲁卡因胶囊、地塞米松、美拉索康等。
3.神经肌肉阻滞:布洛维卡因、肉毒素A等。
4.心理治疗:认知行为治疗、生物反馈治疗等。
六、二次性头痛的处理:对于头痛合并其他疾病的患者,应首先针对基础病进行治疗,同时根据头痛特点采取相应药物治疗。
七、儿童和特殊人群的头痛治疗:对于儿童和孕妇等特殊人群,应慎重选择药物治疗,优先考虑非药物治疗。
总结起来,中国偏头痛诊治指南主要包括头痛的诊断标准、分类和分级、非药物治疗、急性治疗、预防治疗、二次性头痛的处理以及儿童和特殊人群的头痛治疗。
这些指南旨在提供给临床医生对偏头痛患者进行诊断和治疗的依据,帮助患者减少头痛的发作频率和降低头痛的严重程度。
偏头痛的诊断与治疗ppt课件
3.完全可恢复的言语障碍
C. 至少符合以下2条:
1.双侧视觉症状和/或单侧感觉症状 2.至少一个先兆症状逐渐发展时间≥5分钟和/或不同的
先兆症状接连出现≥5分钟 3.每个症状≥5分钟并且≤60分钟
编辑课件
14
1.2.2 无偏头痛头痛的典型先兆 (续一)
编辑课件
6
偏头痛的IHS分类(续二)
1.6 很可能的偏头痛
1.6.1 很可能的无先兆性偏头痛
1.6.2 很可能的先兆性偏头痛
1.6.5 很可能的慢性偏头痛
编辑课件
7
眼肌麻痹型偏头痛
眼肌麻痹性偏头痛已经从第1章.偏头痛中移到 第13章.颅神经痛和与中枢疾患有关的面痛。 13.17眼肌麻痹型偏头痛
A.至少两次发作满足标准B
3.完全可恢复的言语障碍
C. 至少符合以下2条:
1.至少一个先兆症状逐渐发展时间≥5分钟和/或不同的
先兆症状接连出现≥5分钟
编辑课件
18
1.2.4 家族性偏瘫性偏头痛 (FHM)(续一)
–2.每个症状≥5分钟并且≤24小时 –3.在先兆期或先兆症状随后60分钟之内出现
符合1.1 无先兆性偏头痛的B-D标准的头痛
D.在先兆期或先兆症状随后60分钟之内 出现符合无先兆性偏头痛的B-D标准 的头痛
E.不归因于其他疾患
编辑课件
13
1.2.2 无偏头痛头痛的典型先兆
A.至少2次发作符合标准B~D
B.先兆包括至少以下一条,但是没有运动障碍:
1.完全可恢复的视觉症状,包括阳性症状(如闪烁的 光、斑点或线)和/或阴性症状(如视野缺损)
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
偏头痛诊断标准
偏头痛的诊断标准主要基于国际疼痛临床诊断协议的诊断标准,主要分为以下三个方面:
1、症状特征:患者报告长期(>4次/月)出现一侧头部或颈部疼痛,压榨、拉伸及剧烈移动感觉使痛苦恶化,约有一半病例伴有恶心和呕吐,可持续数小时到数天,随原发因素而变化。
2、病因:恒性因素有精神压力、低血糖、季节性、睡眠背景、自发性及药物性等;触发性因素有疲劳、噪声、眼睛疲劳、香烟及兴奋性刺激等。
3、实验室检查:通常情况下,偏头痛的家族史和神经学检查正常,没有神经萎缩或病理改变;其它检查诸如血液检查,甲状腺及肾功能检查,电致反射测定,脑池压力检查,MRIs及脑电图等也可用于排除其它疾病。