人PBMC中的细胞类型
PBMC提取

PBMC(peripheral blood mononuclear cell),外周血单个核细胞,顾名思义,其主要细胞类型为血液里边具有单个核的细胞,主要包括淋巴细胞(T\B),单核细胞,吞噬细胞,树突状细胞和其他少量细胞类型。
其中淋巴细胞占很大一部分。
分离PBMC的主要目的是为了将多核细胞和红细胞去除,从而能够很方便地模拟体外的血液免疫环境。
Ficoll是蔗糖的多聚体,呈中性,平均分子量为400,000,当密度为1.2g/ml 仍未超出正常生理性渗透压,也不穿过生物膜。
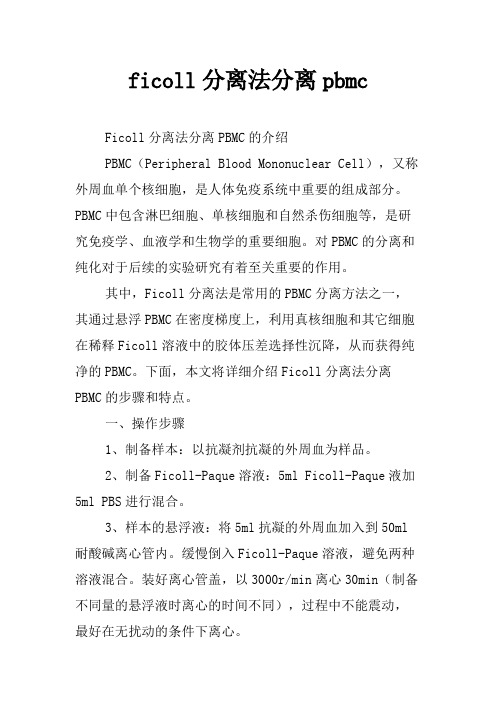
红细胞、粒细胞比重大,离心后沉于管底;淋巴细胞和单核细胞的比重小于或等于分层液比重,离心后漂浮于分层液的液面上,也可有少部分细胞悬浮在分层液中。
吸取分层液液面的细胞,就可从外周血中分离到单个核细胞。
注意事项全血溶液可以加在Ficoll上层或者下层,但是最终都必须保证两种溶液分层清晰。
分离PBMC第一步离心的时候,一定不能设置或设置低水平的制动。
否则将分层混乱。
步骤:配制所需的溶液:a. 细胞培养基:RPMI 1640+10% FBS+1% P/S;b. 细胞冻存液:FBS中加入10%DMSO;c.将10ml全血转入50ml离心管中,加入10ml PBS溶液稀释,轻轻混匀;d.取两支15ml离心管,先加入5ml Ficoll溶液。
然后将稀释的血液轻轻加到两支离心管的ficoll上层,一定要轻柔,避免两种溶液混合在一起,每只离心管各10ml稀释血液;2,000rpm,20min,注意,降速设置中一定要设置成no break,或者只有1-2成的制动。
离心完毕将得到如图所示分层;PBMC所在细胞层为白色。
此时可以用吸管将该层细胞吸取在另一干净的15ml 离心管中。
e.加入PBS至10-15ml,1,500rpm,10min离心后去掉上清,再加入培养基进行相同操作的清洗;f.加入5-10ml培养基重悬细胞,进行后续计数培养或者铺板;g.细胞冻存:将细胞离心收集之后,用细胞冻存液重悬。
人外周血单个核细胞的采集、分离和保存标准
人外周血单个核细胞的采集、分离和保存标准全文共四篇示例,供读者参考第一篇示例:人外周血单个核细胞(Peripheral Blood Mononuclear Cells, PBMCs)的采集、分离和保存是在医学研究和临床诊断中非常重要的步骤。
PBMCs是一类具有免疫功能的细胞,包括淋巴细胞、单核细胞和浆细胞,能够在机体的免疫应答中发挥重要作用。
为了保证试验结果的准确性和可靠性,对PBMCs的采集、分离和保存必须按照相应的标准进行操作。
一、采集1. 选择合适的采集方法:一般常用的采集方法包括静脉抽血和手指取血等,静脉抽血常用于采集较多血液量的情况,手指取血则适用于采集少量血液的情况。
2. 确保采集操作标准化:在采集PBMCs的过程中,应该遵守严格的消毒和无菌操作规程,以防止细菌和病毒的污染。
3. 采集完整的血液样本:为了确保PBMCs的纯度和稳定性,应该尽量避免气泡和血细胞破损导致的RNA降解等情况。
二、分离1. 使用适当的分离方法:一般常用的PBMCs分离方法包括密度梯度离心和磁珠分选等,密度梯度离心适用于分离较大量的PBMCs,磁珠分选则适用于分离特定类型的细胞。
2. 选择合适的分离液:密度梯度离心中一般使用的分离液包括Ficoll和Percoll等,磁珠分选中则需要选择特定的磁珠标记物。
3. 保证分离效率和纯度:在PBMCs的分离过程中,应该确保细胞的分离效率和纯度,避免细胞的损失和杂质的混入。
三、保存1. 选择合适的保存条件:PBMCs的保存条件包括温度、储存液和容器等要素,应该选择适合PBMCs存活的条件进行保存。
2. 快速冻存PBMCs:为了避免细胞的降解和失活,应该在采集和分离PBMCs后尽快将其冻存。
3. 定期监测保存效果:在存储PBMCs的过程中,应该定期监测PBMCs的存活率和纯度,以确保PBMCs的质量和稳定性。
对于人外周血单个核细胞的采集、分离和保存,在操作的过程中应该严格按照相应的标准进行,以确保PBMCs的质量和稳定性,为后续的研究和临床应用提供可靠的基础。
ficoll分离法分离pbmc
ficoll分离法分离pbmcFicoll分离法分离PBMC的介绍PBMC(Peripheral Blood Mononuclear Cell),又称外周血单个核细胞,是人体免疫系统中重要的组成部分。
PBMC中包含淋巴细胞、单核细胞和自然杀伤细胞等,是研究免疫学、血液学和生物学的重要细胞。
对PBMC的分离和纯化对于后续的实验研究有着至关重要的作用。
其中,Ficoll分离法是常用的PBMC分离方法之一,其通过悬浮PBMC在密度梯度上,利用真核细胞和其它细胞在稀释Ficoll溶液中的胶体压差选择性沉降,从而获得纯净的PBMC。
下面,本文将详细介绍Ficoll分离法分离PBMC的步骤和特点。
一、操作步骤1、制备样本:以抗凝剂抗凝的外周血为样品。
2、制备Ficoll-Paque溶液:5ml Ficoll-Paque液加5ml PBS进行混合。
3、样本的悬浮液:将5ml抗凝的外周血加入到50ml 耐酸碱离心管内。
缓慢倒入Ficoll-Paque溶液,避免两种溶液混合。
装好离心管盖,以3000r/min离心30min(制备不同量的悬浮液时离心的时间不同),过程中不能震动,最好在无扰动的条件下离心。
4、取上清液:离心结束后,可以清晰地看到上清液、白膜和红血块。
样品中的细胞被Ficoll在稀释液中的胶体压力亲和力离心到离心管的木纹间。
无线假底离心管是离心过程中压力拍打细胞下沉粘连的机会最小的离心材料。
在冰上开盖依次取出,将悬浮液上清液倒在装有PBS的无菌离心管中。
5、PBS的加入:加入PBS,摇匀,离心1800r/min,10min。
取出,弃上清液。
6、PBS的加入和离心:重复上一步2次。
最后一次离心弃掉PBS,留下沉淀细胞。
二、特点1、相对纯净度高:Ficoll-Paque是一种密度梯度介质,利用细胞的沉降速度和浮力进行分离。
使不同密度的细胞分层,从而实现分离。
使用该分离方法分离PBMC,可获得高度纯净的细胞,最大限度减少不同细胞系之间的干扰。
hpbmc淋巴细胞的培养方法
hpbmc淋巴细胞的培养方法HPBMC(Human Peripheral Blood Mononuclear Cells)是指人外周血单个核细胞,其中包括淋巴细胞、单核细胞和浆细胞。
淋巴细胞是一类重要的免疫细胞,对于免疫系统的功能发挥起着至关重要的作用。
因此,淋巴细胞的培养方法对于研究免疫系统的功能和机制至关重要。
本文将介绍HPBMC淋巴细胞的培养方法。
为了获得HPBMC,我们需要采集新鲜的外周血样本。
在采集外周血样本时,需要使用消毒的器具,避免污染。
一般来说,我们可以选择采用静脉采血的方式,将外周血收集到抗凝剂处理的试管中。
接下来,我们需要将外周血样本进行分离,获取到其中的HPBMC。
常用的分离方法有密度梯度离心法和负选择法。
密度梯度离心法是将外周血样本加入到含有密度梯度溶液的离心管中,经过离心后,不同细胞类型会分布在不同的密度层中,从而实现淋巴细胞的分离。
负选择法是使用磁珠或抗体等对非淋巴细胞进行标记,通过磁力或柱子的作用,将非淋巴细胞分离出去,从而获得HPBMC。
获得HPBMC后,我们需要对其进行培养。
首先,我们需要选择合适的培养基。
常用的培养基包括RPMI-1640培养基、DMEM培养基等。
在培养基中,我们需要添加适当浓度的血清、抗生素和其他生长因子等,以提供细胞所需的营养物质和环境。
接下来,我们将HPBMC加入到培养基中,并将其转移到培养皿中。
在培养过程中,我们需要控制培养皿中的温度、湿度和CO2浓度等环境因素。
一般来说,培养温度为37摄氏度,湿度为95%,CO2浓度为5%。
在培养过程中,我们需要定期更换培养基,以保证细胞的生长和增殖。
通常情况下,每隔2-3天更换一次培养基。
此外,我们还可以根据实验需要添加不同的刺激物,如抗原、细胞因子等,以模拟特定的免疫反应。
在培养的过程中,我们可以通过显微镜观察细胞的形态和增殖情况。
如果需要进一步分析细胞的免疫功能,我们可以使用流式细胞术、ELISA等技术进行检测。
人外周血内皮祖细胞的分离、培养、扩增和鉴定
人外周血内皮祖细胞的分离、培养、扩增和鉴定目的:研究人外周血内皮祖细胞的分离、培养、扩增和鉴定方法。
方法:采用密度梯度离心法分离人外周血单个核细胞,用EGM-2培养基在多聚赖氨酸包被的培养板中进行诱导培养,动态地观察贴壁细胞的生长状况,免疫组织化学技术检测培养细胞表面标志物的表达。
结果:人外周血单个核细胞经体外培养至第2天,呈贴壁生长,细胞形态为大小相近的圆球体;第4天一些细胞开始出现尾状物,形态呈蝌蚪样改变,部分细胞聚集形成细胞簇;至第7天细胞形态变长,呈梭形改变,细胞间相互围绕呈环形,并有集落出现,免疫组织化学染色CD133、CD34、VEGFR-2和Ⅷ因子表达均呈阳性。
结论:运用本实验方法可以成功实现人外周血内皮祖细胞的分离、培养和扩增。
标签:内皮祖细胞;外周血;细胞培养内皮祖细胞(Endothelial Progenitor Cells,EPCs)是血管内皮细胞的前体细胞,亦称血管母细胞(angioblast),EPCs不仅参与胚胎血管生成,而且也参与出生后的血管新生过程。
近些年来人们对EPCs在血管形成、心脑血管疾病和创伤愈合等方面的作用进行了广泛的研究[1],EPCs移植技术已成为治疗心脑血管疾病的一种新兴的方法[2],具有广阔的临床应用前景。
但由于EPCs的来源有限,目前的培养方法尚不能满足基础研究和临床治疗的需要,在本实验中,笔者研究从来源相对广泛的人外周血中分离培养EPCs,为EPCs的应用提供一种便捷有效的分离方法。
1 材料和方法1.1 材料:主要试剂和仪器:内皮细胞培养基(Endothelial Cell Growth Medium-2,EGM-2)(Lonza公司)。
人淋巴细胞分离液(天津灝洋生物制品有限公司)。
鼠抗人CD133单克隆抗体、血管内皮生长因子受体2(Vascular Endothelial Growth Factor Receptor 2,VEGFR-2)(北京博奥森生物技术有限公司)。
PBMC细胞分类及不同细胞比例
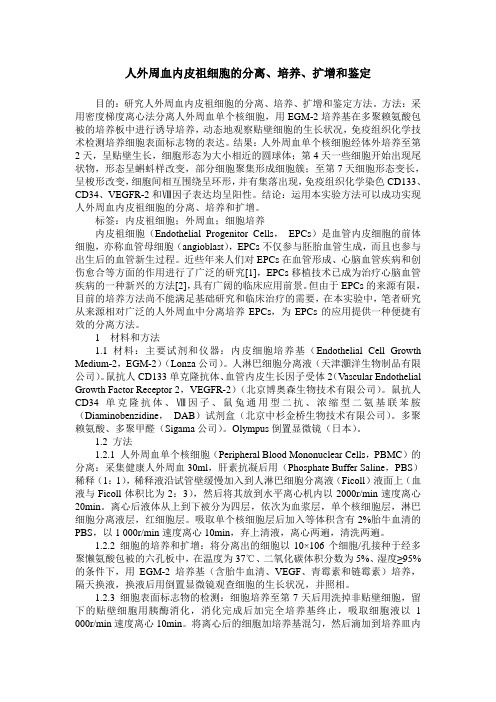
20ml血液大概提取6PBMCPBMC(外周血单个核细胞)包含淋巴细胞( T、B、NK)、单核细胞和树突状细胞。
在人体中这些细胞的比率因人而异。
在多半研究中,淋巴细胞约占PBMC的70~90%,单核细胞约为10~30%,树突状细胞特别少,约为1~2%。
对此中占多半的淋巴细胞进一步细分,可发现此中70~85%为CD3+T细胞(折算成PBMC的比率约45~70%),5~20%为B细胞(折算成PBMC的比率约15%),5~20%为NK细胞(折算成PBMC的比率约15%)。
CD3+T细胞由CD4+T细胞(约占PBMC25~60%)和CD8+T细胞(约占PBMC5~30%),比率约2:1。
CD4+和CD8+T细胞均可进一步分为初始T(naiveT)、接触过抗原的中心记忆性、效应记忆性和效应性T细胞。
关于这些亚群,因为不一样研究使用的标志不一样,故比率亦相差较大。
CD4+T细胞又称为协助性T细胞,可依据细胞因子表达的不一样而持续分为不一样的功能亚群,包含调理性T细胞、Th1、Th2、Th17、Th9、滤泡协助性 T、TR1等亚群。
这些亚群的划分只会愈来愈复杂。
CD8+细胞毒性T细胞此刻可大概分为200个功能表型。
循环B细胞包含过渡型、未致敏、记忆型以及浆母细胞,各个亚群比率不一。
循环树突状细胞包含浆细胞样树突状细胞和髓系来源树突状细胞。
循环单核细胞可分为经典型单核细胞和非经典型CD16+促炎症反响单核细胞(约占单核的10%)。
人类免疫系统功能研究极其依靠PBMC的表型和功能评估,所以对外周血各种亚群表型和功能、PBMC与组织免疫细胞的不一样进行充足认识是特别必需的。
pbmc分离注意事项
PBMC分离注意事项一、摘要PBMC( Peripheral Blood Mononuclear Cells,外周血单个核细胞)分离是生物医学研究中常见的实验操作之一。
PBMC包括淋巴细胞、单核细胞、树突状细胞等,在免疫学、肿瘤学、血液学等领域的研究中具有重要意义。
然而,在进行PBMC分离时,需要注意许多细节和操作要点,以确保实验结果的准确性和可靠性。
本文将就PBMC分离的实验准备、操作过程和后续处理等方面的注意事项进行详细讨论,旨在提高实验操作效率和实验结果质量。
二、实验准备注意事项在开始PBMC分离之前,需要进行充分的实验准备工作。
以下是一些需要注意的事项:1.血液样本的采集和处理在进行PBMC分离之前,需要采集血液样本。
采血时应注意以下几点:首先,要选择适当的采血时间,如清晨空腹采血可以提高检测结果的稳定性;其次,应选择适当的采血方式,如静脉采血或动脉采血;最后,应使用适当的抗凝剂来处理血液样本,以避免血液凝固。
在采集血液样本后,应尽快将样本送往实验室进行处理。
2.实验器材和试剂的准备在实验前,需要准备好所需的实验器材和试剂。
应选择适当的离心管、吸管、细胞筛等实验器材,并确保这些器材的清洁度和无菌状态。
此外,需要准备适当的分离介质、洗涤液、培养基等试剂,并确保这些试剂的质量和浓度符合实验要求。
三、操作过程注意事项在PBMC分离的操作过程中,应注意以下事项:1.离心速度和时间的选择离心是PBMC分离的重要步骤之一。
在选择离心速度和时间时,应根据实验要求和实际情况进行权衡。
离心速度过高或时间过长可能导致细胞损伤或失活;离心速度过低或时间过短则可能导致分离不充分。
因此,需要根据分离介质的特性和所需细胞类型进行选择和调整。
2.操作过程的无菌化处理在PBMC分离过程中,应保持操作的无菌化处理。
所有实验器材和试剂应保持清洁和无菌状态,以避免污染和交叉感染。
此外,实验操作应在无菌操作台或超净工作台中进行,并穿戴适当的个人防护装备。
人PBMC中的细胞类型
Types of immune cells present in human PBMCPosted on November 22, 2012by Andrea in PBMC Basics with 1 CommentWhen peripheral whole blood is drawn for human immune system studies, it is often processed to remove red blood cells by density gradient centrifugation. Most commonly this method uses Ficoll Paque, a solution of high molecular weight sucrose polymers, a product of GE HealthcareLtd. Ficoll separates whole blood into two fractions above and below the density of 1.077g/ml.Peripheral blood mononuclear cells (PBMC) are the populations of immune cells that remain at the less dense, upper interface of the Ficoll layer, often referred to as the buffy coat and are the cells collected when the Ficoll fractionation method is used.Erythrocytes (red blood cells) and polymorphonuclear cells (PMNs) which include neutrophils and eosinophils are generally removed during this fractionation as they are denser then 1.077g/ml. Basophils, however can be greater or less dense then 1.077g/ml and thus may be present to a small degree in the less dense PBMC fraction.PBMCs include lymphocytes (T cells, B cells, and NK cells), monocytes, and dendritic cells. In humans, the frequencies of these populations vary across individuals. In my experience as well as that of others, lymphocytes are typically in the range of 70 – 90% of PBMCs, monocytes range from 10 –30% of PBMCs, while dendritic cells are rare, being only 1 – 2% ofPBMCs. The frequencies of cell types within the lymphocyte population include 70 – 85% CD3+ T cells (45 – 70% of PBMC), 5 – 20% B cells (up to 15% of PBMC), and 5 – 20% NK cells (up to 15% of PBMC).The CD3+ compartment is composed of CD4 (25 – 60% of PBMC)and CD8 T cells (5 – 30% of PBMC), in a roughly 2:1ratio. Both CD4 and CD8 T cells can be further subsetted into naïve, and the antigen-experienced central memory, effector memory, and effector subtypes that exist in resting or activated states. Multiple markers can be used to identify these compartments to varying similarities and thus the frequencies reported by people using different markers may vary.CD4 T cells are known as helper T cells and can be further classified into various functional subtypes based on the expression profiles of specific cytokines, surface markers, or transcription factors. These include regulatory T cells, T H1, T H2, and T H17 cells as well as other described subpopulations such as T H9, follicular helper, and T R1 types. These classifications howeverwill certainly become more complex in the future, as recently the cytotoxic CD8 T cell compartment has been to shown to be extremely heterogenous in marker expression and function and may be comprised of roughly 200 functional phenotypes.Circulating B cells include transitional, naïve, and memory subtypes as well as plasmablasts, all of which can be found at varying populations in peripheral blood. Circulating dendritic cells include plasmacytoid dendritic cells as well as myeloid derived dendritic cells. Circulating monocytes have been described as either being classical monocytes or nonclassical CD16+ proinflammatory monocytes, which comprise up to 10% of the monocytes in peripheral blood and have unique functions compared with classical monocytes.Human immune system studies rely heavily on the phenotypic and functional assessments of PBMCs. In order to take advantage of PBMCs for human immune studies, it is important to know what populations are represented in peripheral blood and how PBMC populations differ in distribution and function from tissue immune cells. Finally it is critical to become familiar with the identifying surface and intracellular markers and the types of assays best suited for human PBMC studies. The markers most suitable for identification of the major immune populations in human PBMC using flow cytometry will be the topic of the next blog.。
pbmc细胞提取方法精选全文
可编辑修改精选全文完整版pbmc细胞提取方法PBMC细胞提取方法引言PBMC(Peripheral Blood Mononuclear Cells)是外周血中的单个核细胞,包括淋巴细胞、单核细胞和NK细胞等,是研究免疫学、血液疾病和感染病原体等领域的重要细胞来源。
本文将介绍一种常用的PBMC细胞提取方法,旨在为研究者提供一种可行的操作步骤。
材料与试剂1. 外周血样本:新鲜采集的外周血样本(推荐使用抗凝剂如EDTA 进行处理)。
2. PBS缓冲液:含有2 mM EDTA的磷酸盐缓冲液。
3. 密度梯度离心液:如Ficoll-Paque Plus。
步骤1. 收集外周血样本使用适当的采血针和抗凝管收集外周血样本,避免血液污染和凝固。
2. 加入PBS缓冲液将外周血样本转移到15 ml离心管中,每1 ml外周血加入2 ml预先加热的PBS缓冲液,缓慢混合。
3. 密度梯度离心将外周血样本缓慢地均匀地加入到15 ml离心管中含有密度梯度离心液的管内,避免悬浮。
注意,加入的体积应不超过离心管的80%。
然后,轻轻离心管以保持梯度的稳定性。
4. 离心分层PBMC将离心管置于离心机中,以400g的速度离心30分钟。
离心后,可以看到形成三个不同的层次:上层为透明的血清,中间为白色的PBMC层,底层为红色的红细胞。
5. 收集PBMC层使用长颈的移液器,小心地收集PBMC层,避免污染或干扰其他层次的细胞。
将PBMC转移至新的离心管中。
6. 洗涤PBMC向PBMC悬浮液中加入PBS缓冲液,并以1000g的速度离心10分钟。
倒掉上清,避免损失PBMC。
重复此步骤两次以彻底洗涤PBMC。
7. 计数和保存PBMC使用细胞计数板或自动细胞计数器计数PBMC的数量,根据实验需求调整细胞浓度。
根据实验需要,将PBMC悬浮液分装到冻存管中,添加适当的冻存液,迅速冷冻保存。
结论PBMC细胞提取是一种常用的实验操作步骤,通过密度梯度离心的方法,可以有效地从外周血中分离出PBMC。
pbmc增殖实验原理
pbmc增殖实验原理
PBMC增殖实验是一种常用的细胞生物学实验,用于研究外周血
单个核细胞(PBMC)的增殖能力。
PBMC是一种混合细胞群,包括淋
巴细胞、单核细胞和自然杀伤细胞等。
进行PBMC增殖实验的原理主
要包括以下几个方面:
1. PBMC分离和培养,首先,从外周血中分离PBMC,通常采用
密度梯度离心法。
然后将PBMC进行培养,提供适当的营养物质和生
长因子,以促进其生长和增殖。
2. 刺激因子的作用,在培养PBMC的过程中,可以加入不同的
刺激因子,如激活剂、抗原或药物等,以模拟体内的免疫应答过程。
这些刺激因子可以激活PBMC,促进其增殖和分化。
3. 测定增殖活性,通过不同的方法来测定PBMC的增殖活性,
常用的方法包括MTT法、放射性核素标记法、流式细胞术等。
这些
方法可以定量或定性地评估PBMC的增殖能力。
4. 数据分析和解释,最后,对实验结果进行数据分析和解释,
比较不同条件下PBMC的增殖活性,探讨刺激因子对PBMC增殖的影
响,从而揭示PBMC在免疫应答中的作用和调控机制。
总的来说,PBMC增殖实验的原理是通过培养PBMC并加入刺激因子,测定其增殖活性,从而研究PBMC在免疫应答中的生物学特性和调控机制。
这种实验方法在免疫学和临床医学研究中具有重要的应用价值。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Types of immune cells present in human PBMC
Posted on November 22, 2012by Andrea in PBMC Basics with 1 Comment
When peripheral whole blood is drawn for human immune system studies, it is often processed to remove red blood cells by density gradient centrifugation. Most commonly this method uses Ficoll Paque, a solution of high molecular weight sucrose polymers, a product of GE Healthcare
Ltd. Ficoll separates whole blood into two fractions above and below the density of 1.077g/ml.
Peripheral blood mononuclear cells (PBMC) are the populations of immune cells that remain at the less dense, upper interface of the Ficoll layer, often referred to as the buffy coat and are the cells collected when the Ficoll fractionation method is used.
Erythrocytes (red blood cells) and polymorphonuclear cells (PMNs) which include neutrophils and eosinophils are generally removed during this fractionation as they are denser then 1.077g/ml. Basophils, however can be greater or less dense then 1.077g/ml and thus may be present to a small degree in the less dense PBMC fraction.
PBMCs include lymphocytes (T cells, B cells, and NK cells), monocytes, and dendritic cells. In humans, the frequencies of these populations vary across individuals. In my experience as well as that of others, lymphocytes are typically in the range of 70 – 90% of PBMCs, monocytes range from 10 –30% of PBMCs, while dendritic cells are rare, being only 1 – 2% of
PBMCs. The frequencies of cell types within the lymphocyte population include 70 – 85% CD3+ T cells (45 – 70% of PBMC), 5 – 20% B cells (up to 15% of PBMC), and 5 – 20% NK cells (up to 15% of PBMC).
The CD3+ compartment is composed of CD4 (25 – 60% of PBMC)
and CD8 T cells (5 – 30% of PBMC), in a roughly 2:1
ratio. Both CD4 and CD8 T cells can be further subsetted into naïve, and the antigen-experienced central memory, effector memory, and effector subtypes that exist in resting or activated states. Multiple markers can be used to identify these compartments to varying similarities and thus the frequencies reported by people using different markers may vary.
CD4 T cells are known as helper T cells and can be further classified into various functional subtypes based on the expression profiles of specific cytokines, surface markers, or transcription factors. These include regulatory T cells, T H1, T H2, and T H17 cells as well as other described subpopulations such as T H9, follicular helper, and T R1 types. These classifications however
will certainly become more complex in the future, as recently the cytotoxic CD8 T cell compartment has been to shown to be extremely heterogenous in marker expression and function and may be comprised of roughly 200 functional phenotypes.
Circulating B cells include transitional, naïve, and memory subtypes as well as plasmablasts, all of which can be found at varying populations in peripheral blood. Circulating dendritic cells include plasmacytoid dendritic cells as well as myeloid derived dendritic cells. Circulating monocytes have been described as either being classical monocytes or nonclassical CD16+ proinflammatory monocytes, which comprise up to 10% of the monocytes in peripheral blood and have unique functions compared with classical monocytes.
Human immune system studies rely heavily on the phenotypic and functional assessments of PBMCs. In order to take advantage of PBMCs for human immune studies, it is important to know what populations are represented in peripheral blood and how PBMC populations differ in distribution and function from tissue immune cells. Finally it is critical to become familiar with the identifying surface and intracellular markers and the types of assays best suited for human PBMC studies. The markers most suitable for identification of the major immune populations in human PBMC using flow cytometry will be the topic of the next blog.。