英文病例模板
内科英文病历材料模板
HUAZHONG UNIVERSITY OF SCIENCE AND TECHNOLOGY TONGJI MEDICAL COLLEGE ACCESSORY TONGJI HOSPITALHospitalization Records for None-operation Division Division: __________ Ward: __________ Bed: _________ Case No. ___________Name: ______________ Sex: __________ Age: ___________ Nation: ___________ Birth Place: ________________________________ Marital Status:____________ Work-organization & Occupation: _______________________________________ Living Address & Tel: _________________________________________________ Date of admission: _______Date of history taken:_______ Informant:__________ Chief Complaint: ___________________________________________________History of Present Illness:___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________Past History:General Health Status: 1.good 2.moderate 3.poorDisease history: (if any, please write down the date of onset, brief diagnosticand therapeutic course, and the results.)Respiratory system:1. None2.Repeated pharyngeal pain3.chronic cough4.expectoration:5. Hemoptysis6.asthma7.dyspnea8.chest pain_______________________________________________________________ Circulatory system:1.None2.Palpitation3.exertional dyspnea4..cyanosis5.hemoptysis6.Edema of lower extremities7.chest pain8.syncope9.hypertension_______________________________________________________________ Digestive system:1.None2.Anorexia3.dysphagia4.sour regurgitation5.eructation6.nausea7.Emesis8.melena9.abdominal pain 10.diarrhea11.hematemesis 12.Hematochezia 13.jaundice_______________________________________________________________ Urinary system:1.None2.Lumbar pain3.urinary frequency4.urinary urgency5.dysuria6.oliguria7.polyuria8.retention of urine9.incontinence of urine10.hematuria 11.Pyuria 12.nocturia 13.puffy face_______________________________________________________________ Hematopoietic system:1.None2.Fatigue3.dizziness4.gingival hemorrhage5.epistaxis6.subcutaneous hemorrhage_______________________________________________________________ Metabolic and endocrine system:1.None2.Bulimia3.anorexia4.hot intolerance5.cold intolerance6.hyperhidrosis7.Polydipsia8.amenorrhea9.tremor of hands 10.character change 11.Marked obesity12.marked emaciation 13.hirsutism 14.alopecia15.Hyperpigmentation 16.sexual function change_______________________________________________________________ Neurological system:1.None2.Dizziness3.headache4.paresthesia5.hypomnesis6. Visual disturbance7.Insomnia8.somnolence9.syncope 10.convulsion 11.Disturbance of consciousness12.paralysis 13. vertigo_______________________________________________________________ Reproductive system:1.None2.others_______________________________________________________________Musculoskeletal system:1.None2.Migrating arthralgia3.arthralgia4.artrcocele5.arthremia6.Dysarthrosis7.myalgia8.muscular atrophy_______________________________________________________________ Infectious Disease:1.None2.Typhoid fever3.Dysentery4.Malaria 4.Schistosomiasis4.Leptospirosis 7.Tuberculosis 8.Epidemic hemorrhagic fever9.others_______________________________________________________________ Vaccine inoculation:1.None2.Yes3.Not clearVaccine detail __________________________________________ Trauma and/or operation history:Operations:1.None2.YesOperation details:_______________________________________ Traumas:1.None2.YesTrauma details:_________________________________________ Blood transfusion history:1.None2.Yes ( 1.Whole blood 2.Plasma3.Ingredient transfusion)Blood type:____________ Transfusion time:___________Transfusion reaction1.None2.YesClinic manifestation:_____________________________ Allergic history:1.None2.Yes3.Not clearallergen:________________________________________________clinical manifestation:_____________________________________Personal history:Custom living address:____________________________________________ Resident history in endemic disease area:_____________________________ Smoking: 1.No 2.YesAverage ___pieces per day; about___yearsGiving-up 1.No 2.Yes (Time:_______________________) Drinking: 1.No 2.YesAverage ___grams per day; about ___yearsGiving-up 1.No 2.Yes(Time:________________________) Drug abuse:1.No 2.YesDrug names:_______________________________________ _______________________________________________________________Marital and obstetrical history:Married age: __________years old Pregnancy ___________timesLabor _______________times(1.Natural labor: _______times 2.Operative labor: ________times3.Natural abortion: ______times4.Artificial abortion: _______times5.Premature labor:__________times6.stillbirth__________times)Health status of the Mate:1.Well2.Not fineDetails: _______________________________________________ Menstrual history:Menarchal age: _______ Duration ______day Interval ____daysLast menstrual period: ____________ Menopausal age: ____years oldAmount of flow: 1.small 2. moderate 3. largeDysmenorrheal: 1. presence 2.absence Menstrual irregularity 1. No 2.Yes Family history: (especially pay attention to the infectious and hereditary diseaserelated to the present illness)Father: 1.healthy 2.ill:________ 3.deceased cause: ___________________ Mother:1.healthy 2.ill:________ 3.deceased cause: ___________________ Others: ________________________________________________________ The anterior statement was agreed by the informant.Signature of informant: Datetime:Physical ExaminationVital signs:Temperature:______0C Blood pressure:_______/_______mmHg Pulse: _____ bpm (1.regular 2.irregular_____________________________) Respiration: ___bpm (1.regular 2.irregular____________________________) General conditions:Development: 1.Normal 2.Hypoplasia 3.HyperplasiaNutrition: 1.good 2.moderate 3.poor 4.cachexiaFacial expression: 1.normal 2.acute 3.chronic other_____________________ Habitus: 1.asthenic type 2.sthenic type 3.ortho-thenic typePosition: 1.active 2.positive pulsive 4.other_______________________ Consciousness: 1.clear 2.somnolence 3.confusion 4.stupor 5.slight coma6.mediate coma7.deep coma8.deliriumCooperation: 1Yes 2.No Gait: 1.normal 2.abnormal______Skin and mucosa:Color: 1.normal 2.pale 3.redness 4.cyanosis 5.jaundice 6.pigmentationSkin eruption:1.No 2.Yes( type: __________distribution:__________________) Subcutaneous bleeding: 1.no 2.yes (type:_______distribution:______________) Edema:1. no 2.yes ( location and degree________________________________) Hair: 1.normal 2.abnormal(details_____________________________________) Temperature and moisture: normal cold warm dry moist dehydration Liver palmar : 1.no 2.yes Spider angioma (location:________________) Others: __________________________________________________________ Lymph nodes: enlargement of superficial lymph node:1.no2.yesDescription: ________________________________________________ Head:Skull size:1.normal 2.abnormal (description:____________________________) Skull shape:1.normal 2.abnormal(description:___________________________) Hair distribution :1.normal 2.abnormal(description:______________________) Others:___________________________________________________________ Eye: exophthalmos:___________eyelid:____________conjunctiva:__________ sclera:________________Cornea:_______________________Pupil: 1.equally round and in size 2.unequal (R______mm L_______mm)Pupil reflex: 1.normal 2.delayed (R___s L___s ) 3.absent (R___L___)others:______________________________________________________ Ear: Auricle 1.normal 2.desformation (description:_______________________) Discharge of external auditory canal:1.no 2.yes (1.left 2.right quality:_____)Mastoid tenderness 1.no 2.yes (1.left 2.right quality:__________________)Disturbance of auditory acuity:1.no 2.yes(1.left 2.right description:_______) Nose: Flaring of alae nasi :1.no 2.yes Stuffy discharge 1.no 2.yes(quality______) Tenderness over paranasal sinuses:1.no 2.yes (location:_______________) Mouth: Lip______________Mucosa_____________Tongue________________ Teeth:1.normal 2. Agomphiasis 3. Eurodontia 4.others:____________________Gum :1.normal 2.abnormal (Description____________________________)Tonsil:___________________________Pharynx:_____________________Sound: 1.normal 2.hoarseness 3.others:_____________________________ Neck:Neck rigidity 1.no 2.yes (______________transvers fingers)Carotid artery: 1.normal pulsation 2.increased pulsation 3.marked distention Trachea location: 1.middle 2.deviation (1.leftward_______2.rightward______) Hepatojugular vein reflux: 1. negative 2.positiveThyroid: 1.normal 2.enlarged _______ 3.bruit (1.no 2.yes ________________)Chest:Chest wall: 1.normal 2.barrel chest 3.prominence or retraction:( left________right_________Precordial prominence__________) Percussion pain over sternum 1.No 2.YesBreast: 1.Normal 2.abnormal _______________________________________ Lung:Inspection: respiratory movement 1.normal 2.abnormal_____________ Palpation: vocal tactile fremitus:1.normal 2.abnormal _______________pleural rubbing sensation:1.no 2.yes______________________Subcutaneous crepitus sensation:1.no 2.yes________________ Percussion:1. resonance 2. Hyperresonance &location_____________3 Flatness&location_________________________________4. dullness & location:_______________________________5.tympany &location:_______________________________lower border of lung: (detailed percussion in respiratory disease)midclavicular line : R:_____intercostae L:_____intercostaemidaxillary line: R:______intercostae L:_____intercostaescapular line: R:______intercostae L:_____intercostaemovement of lower borders:R:_______cmL:__________cm Auscultation: Breathing sound : 1.normal 2.abnormal _______________Rales:1.no 2.yes__________________________________ Heart: Inspection:Apical pulsation: 1.normal 2.unseen 3.increase 4.diffuseSubxiphoid pulsation: 1.no 2.yesLocation of apex beat: 1.normal 2.shift (______ intercosta,distance away from left MCL______cm) Palpation:Apical pulsation:1. normal 2.lifting apex impulse 3.negative pulsationThrill:1.no 2.yes(location:___________ phase:_________________)Percussion: relative dullness border: 1.normal 2.abnormalAuscultation: Heart rate:___bpm Rhythm:1.regular 2.irregular_______Heart sound: 1.normal 2.abnormal________________________Extra sound: 1.no 2.S3 3.S4 4. opening snapP2_________ A2_________Pericardial friction sound:1.no 2.yesMurmur: 1.no 2.yes (location____________phase_____________quality______intensity________ transmission___________effects of position_________________________________effects of respiration______________________________Peripheral vascular signs:1.None2.paradoxical pulse3.pulsus alternans4. Water hammer pulse5.capillary pulsation6.pulse deficit7.Pistol shot sound8.Duroziez signAbdomen:Inspection: Shape: 1.normal 2.protuberance 3.scaphoid 4.frog-bellyGastric pattern 1.no 2.yes Intestinal pattern 1.no 2.yesAbdominal vein varicosis 1.no 2.yes(direction:______________ )Operation scar1.no 2.yes ________________________________ Palpation: 1.soft 2. tensive (location:____________________________)Tenderness: 1.no 2.yes(location:_______________________)Rebound tenderness:1.no 2.yes(location:________________)Fluctuation: 1.present 2.abscentSuccussion splash: 1.negative 2.positiveLiver:_______________________________________________Gallbladder: __________________Murphy sign:____________Spleen:______________________________________________Kidneys:____________________________________________Abdominal mass:______________________________________Others:______________________________________________ Percussion: Liver dullness border: 1.normal 2.decreased 3.absentUpper hepatic border:Right Midclavicular Line ________IntercostaShift dullness:1.negative 2.positive Ascites:_____________degreePain on percussion in costovertebral area: 1.negative 2.positve ____ Auscultation: Bowel sounds : 1.normal 2.hyperperistalsis 3.hypoperistalsis4.absence Gurgling sound:1.no 2.yesVascular bruit 1.no 2.yes (location_____________________) Genital organ: 1.unexamined 2.normal 3.abnormalAnus and rectum: 1.unexamined 2.normal 3.abnormalSpine and extremities:Spine: 1.normal 2.deformity (1.kyphosis 2.lordosis 3.scoliosis)3.Tenderness(location______________________________)Extremities:1.normal 2.arthremia & arthrocele (location_________________)3.Ankylosis (location__________)4.Aropachy: 1.no 2.yes5.Muscular atrophy (location_______________________) Neurological system:1.normal 2.abnormal_______________________________ _____________________________________________________________________Important examination results before hospitalized___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ Summary of the history:______________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ Initial diagnosis:_____________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________ ___________________________________________________________Recorder:Corrector:。
呼吸科英文病历范文
呼吸科英文病历范文ENGLISHCASE700756(Respiratory department)----------------------------Name: Liyuzhen `Age:42 yearsSex: FemaleRace: HanOccupation: Free occupationNationality: ChinaMarried status: married Addre: Qianjing Road No.16, Wuhan Hankou.thDate of admiion: July 26, 2001thDate of record: July 26, 2001Present illne:Two days ago the patient suddenly started to cough and feelHer spirit,sleep,appetite were normal.stool and urine werenormal, too.----------------------------PastHistory:General health status: normalOperation history: thyroidectomy.Infection history: No history of tuberculosis or hepatitis.Allergic history: allergic to a lot of drugs such as sulfanilamideTraumatic history: No traumatic history----------------------------SystemreviewRespiratorysystem: No history of repeated pharyngodynia, chroniccough, expectoration, hemoptysis, asthma, dyspneaor chest pain.Circulation system: No history of palpitation, hemoptysis, legsedema, short breath after sports, hypertension,precordium pain or faintne.Digestive system: No history of low appetite, sour regurgitation,belching, nausea, vomiting, abdominal distension,abdominal pain, constipation, diarrhea, hemaptysis,melena, hematochezia or jaundice.Urinary system: No history of lumbago, frequency of urination,urgency of urination, odynuria, dysuria, bloodyurine, polyuria or facial edemaHematopoietic system: No history of acratia, dizzine, gingivalbleeding, nasal bleeding, subcutaneous bleedingor ostealgia.Endocrine system: No history of appetite change, sweating, chillyexceive thirst, polyuria, hands tremor, character alternation, obesity, emaciation, hair change, pig- mentation or amenorrhea.Kinetic system: No history of wandering arthritis, joint pain, red swelling of joint, joint deformity, muscle painor myophagism.Neural system: No history of dizzine ,headache, vertigo, in- somnia, disturbance of consciousne, tremor, conv-ulsion, paralysis or abnormal sensation.--------------------------- Personal History:She was born in Hubei.She never smokes andDrinks.No exposurehistory to toxic substances,and infected water.Her menstruation was normal.LMP:23/7,2001----------------------------Family History:Her parents are living and well.No congenitaldisease in her family.---------------------------- PhysicalExaminationVital signs:T 36.6`C , P 80/min, R 22/min, BP120/80mmHg. General inspection: The patient is a well developed, well nou- rished adult female apparently in no acute distre,pleasant and cooperative.Skin:Normally free of eruption or unusual pigmentation. Lymphnodes: There are no swelling of lymphnodes. Head: Normal skull.No baldne, noscars.Eyes: No ptosis.Extraocular normal.Conjuctiva normal.The Pupils are round, regular, and react to light and ac-Ears: Externally normal.Canals clear.The drums normal.Nose: No abnormalities noted.Mouth and throat: lips red, tongue red.Alveolar ridges normal. Tonsils atrophil and uninfected.Neck: No adenopathy.Thyroid palpable,but not enlarged.No Abnormal pulsations.Trachea in middle.Chest and lung: Normal contour.Breast normal.Expansion equal. Fremitus normal.No unusual areas of dullne.Diaphr-agmatic position and excursion normal.No abnormal br-eath sound.No moist rales heard.No audible pleural fric-ion.There are lots of rhonchi rales and whoop can be heard thHeart: P.M.I 0.5cm to left of midolavicular line in 5 inter- Space.Forceful apex beat.No thrills.No pathologicheart murmur.Heart beat 80 and rhythm is normal. Abdomen: Flat abdomen.Good muscle tone.No distension.No v- isible peristalsis.No rigidity.No ma palpable.Tenderne (-), rebound tenderne (-).Liver and spleenare not palpable.Shifting dullne (-).Bowl soundsnormal.Systolic blowing murmur can be heard at theright side of the navel.Extremities: No joint disease.Muscle strength normal.No ab- normal motion.Thumb sign(+).Wrist sign(+).Neural system:Knee jerk (-).Achilles jerk (-).Babinski sign (-).Oppenheim sign (-).Chaddock sign (-).Conda sign (-).Hoffmann sign (-).Neck tetany (-)Kernig sign (-).Brudzinski sign (-).Genitourinary system: Normal.Rectum: No tenderne------Out-patient department data:No----------------------------Historysummary1).Li Yuzhen, female, 42y.2).Cough and dyspnea for 2 days3).PE: T 36.6`C, P 80/min, R 22/min, BP120/80mmHg.superficial nodes were not palpable.Normal vision.Upper palate haunch--uped.HR: 80bpm, rhythm is normal.There are lots of rho-nchi rales and whoop can be heard .Flat abdomen, Tenderne (-),rebound tenderne (-).Liver and spleen are not pal-pable.Shifting dullne (-).Bowl sounds normal..4).Outpatient data: see above.----------------------------Impreion: Bronchial asthmaSignature:He Lin 95-10033《英文病历.doc》。
门诊病历英文模板
门诊病历英文模板Name:Joe Bloggs(姓名:乔。
伯劳格斯)Date:1st January 2000(日期:2000年1月1日)Time:0720(时间:7时20分)Place:A&E(地点:事故与急诊登记处)Age:47 years(年龄:47岁)Sex:male(性别:男)Occupation:HGV(heavy goods vehicle)driver(职业:大型货运卡车司机) PC(presenting complaint)(主诉)4-hour crushing retrosternal chest pain(胸骨后压榨性疼痛4小时)HPC(history of presenting complaint)(现病史)Onset:4 hours of“crushing tight”retrosternal chest pain,radiating to neck and both arms,gradual onset over 5-10 minutes.(起病特征:胸骨后压榨性疼痛4小时,向颈与双臂放射,5-10分钟内渐起病)Duration:persistent since onset(间期:发病起持续至今)Severe:“worst pain ever had”(严重性:“从未痛得如此厉害过)Relieving/exacerbating factors缓解与恶化因素GTN(glyceryl trinitrate)provided no relief although normally relieves pain in minutes,no other relieving/exacerbating factors.(硝酸甘油平时能)。
英文病历书写模板 medical history questionnaire
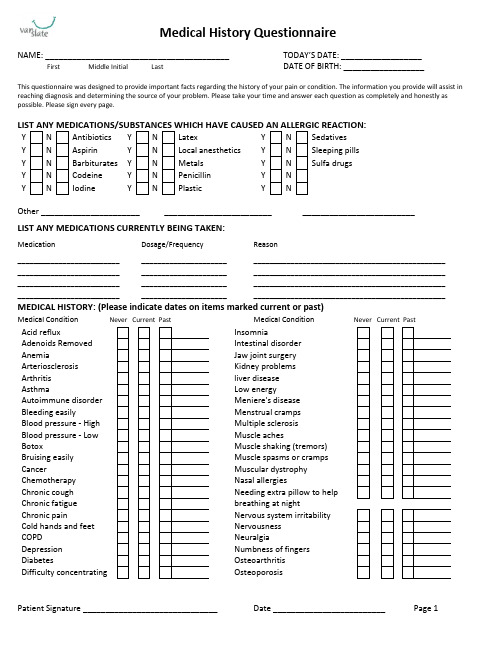
Medical History QuestionnaireNAME: _________________________________________TODAY’S DATE: __________________ First Middle Initial LastDATE OF BIRTH: __________________This questionnaire was designed to provide important facts regarding the history of your pain or condition. The information you provide will assist in reaching diagnosis and determining the source of your problem. Please take your time and answer each question as completely and honestly as possible. Please sign every page.N Antibiotics Y N LatexY N Sedatives N AspirinY N Local anesthetics Y N Sleeping pills N Barbiturates Y N Metals Y N Sulfa drugsN Codeine Y N Penicillin Y N NIodineY NPlasticY NOther ______________________ ________________________ _________________________LIST ANY MEDICATIONS CURRENTLY BEING TAKEN:MedicationDosage/FrequencyReason_________________________ _____________________ _______________________________________________ _________________________ _____________________ _______________________________________________ _________________________ _____________________ _______________________________________________ _________________________ ____________________________________________________________________ MEDICAL HISTORY: (Please indicate dates on items marked current or past)Medical ConditionMedical ConditionAcid refluxInsomniaAdenoids RemovedIntestinal disorder AnemiaJaw joint surgery ArteriosclerosisKidney problems Arthritisliver disease AsthmaLow energyAutoimmune disorder Meniere's disease Bleeding easilyMenstrual cramps Blood pressure - HighMultiple sclerosis Blood pressure - Low Muscle achesBotoxMuscle shaking (tremors) Bruising easilyMuscle spasms or cramps CancerMuscular dystrophy ChemotherapyNasal allergiesChronic coughNeeding extra pillow to help Chronic fatiguebreathing at nightChronic painNervous system irritability Cold hands and feet Nervousness COPDNeuralgiaDepressionNumbness of fingers DiabetesOsteoarthritis Difficulty concentratingOsteoporosisPatient Signature ______________________________ Date _________________________ Page 1Medical condition Never Current Past Medical condition Never Current PastDifficulty sleeping Ovarian cysts Dizziness Parkinson's disease Emphysema Poor circulationEpilepsy Prior orthodontic treatment Excessive thirst Psychiatric care Fibromyalgia Radiation treatment Fluid retention Rheumatic fever Frequent cough Rheumatoid arthritis Frequent illnessesScarlet fever Frequent stressful situations ScoliosisGeneral anesthesia Shortness of breath Glaucoma Sinus problems Gout Skin disorder Hay Fever Sleep apnea Hearing impaired Slow healing sores Heart attackSpeech difficulties Heart disorder StrokeHeart murmur Swelling in ankles or feet Heart pacemaker Swollen, stiff or painful joints Heart valve replacement Tendency for ear infections Hemophilia Tendency for frequent colds Hepatitis Tendency for sore throats Hypertension Thyroid disorder HypoglycemiaTired muscles Immune system disorder Tonsils removed Injury to face Tuberculosis Injury to mouth Tumors Injury to neckUrinary disorders Injury to teethWisdom teeth extractionMedical conditionMedical condition Other ____________________ADDITIONAL MEDICAL HISTORY ITEMS:Recreational Drugs HIV/AIDSN Appendectomy Y N HeartYN ThyroidN Back Y N Hernia repair Y N TonsillectomyN EarY N Lung Y N Uvulectomy NGallbladderY NNasalY NPeriodontalPatient Signature _________________________________Date____________________Page 2FAMILY HISTORY Has any member of your family had (parent, sibling or grandparent):YNCancer YNSleep disorder YNFather snoresY N Heart disease Y N Obesity Y NMother snoresYNDiabetesY NThyroid troubleYNFather has sleep apnea Y N Stroke Y N High blood pressure Y N Mother has sleep apnea SOCIAL HISTORY:Tobacco Use:smokedAlcohol Use:Caffeine Intake:None Coffee/Tea/Soda #cups per day: _______Additional:Page 3。
英文病历书写疼痛
英文病历书写:疼痛(1)当上楼梯时,突然痛了起来,并且持续不止。
The pain came on suddenly while walking up the stairs and it was persistent.疼痛的发生感觉疼痛 feel (have; suffer from) a pain; pain is felt in ; feel painful头痛 have a headache; be troubled with a headache; feel a pain in one's head患剧烈头痛 have a nasty (bad) headache时常头痛 be subject (a martyr) to headaches有撞击似的两侧性头痛 have bilateral pounding headaches头痛逐渐地变为频发(较不严重) headaches gradually become more frequent (less severe)ex1:咀嚼时,有偶发的、暂时的、不可言状的疼痛或敏感。
There is occasional, transient, nondescript pain, or sensibility during mastication.ex2:该齿对于压迫作痛,且有钝麻如咬的疼痛。
The tooth became sore to pressure and there is a dull gnawing pain.发生时间ex1:Epigastric pain comes immediately after meal.ex2:Colic pain came on and off since yesterday.ex3:This pain has been relentlessly postprandial, regardless of the character of her meals.ex4:The joint pains were present mainly at night, with relief during the day.ex5:The mild frontal headaches were usually present upon awakening,but not severe enough to require analgesics.ex6:The pain usually commenced within 30 minutes after meals and lasted 1 to 3 hours.发生原因ex1:He described the pain as dull and aching, occurring approximately once a week, unrelated to food intake, and radiating to his back.(2)起初疼痛无变化,但数小时时变成发作性的'痛。
soap英文病历
soap英文病历Title: SOAP English Medical RecordsIntroduction:SOAP (Subjective, Objective, Assessment, Plan) is a widely used method for documenting patient information in medical records. This article aims to provide an accurate and comprehensive overview of SOAP English medical records. The article will be structured with an introduction, main body, and conclusion. The main body will consist of five major points, each divided into 3-5 subpoints, explaining the intricacies of SOAP English medical records.Main Body:1. Subjective:1.1 Patient Background:- Provide patient demographic information such as name, age, gender, and contact details.- Include relevant medical history, including previous illnesses, surgeries, and allergies.- Document the patient's chief complaint, presenting symptoms, and duration of symptoms.- Record any relevant information provided by the patient or their family members.1.2 Present Illness:- Describe the current medical condition in detail, including the onset, progression, and severity of symptoms.- Document any factors that may have contributed to the illness.- Include a timeline of events leading up to the current condition.- Record any treatments or medications the patient has already tried.1.3 Review of Systems:- Systematically document the patient's symptoms and complaints related to each body system.- Include information on constitutional symptoms, such as fever, weight loss, or fatigue.- Record any positive or negative findings in each system, such as respiratory, cardiovascular, gastrointestinal, etc.- Mention any relevant family history that may impact the patient's condition.2. Objective:2.1 Physical Examination:- Document the findings of a thorough physical examination, including vital signs, general appearance, and specific organ system assessments.- Describe any abnormalities or notable observations.- Include results of laboratory tests, imaging studies, or other diagnostic procedures.- Record the patient's height, weight, and body mass index (BMI).2.2 Assessment:- Summarize the healthcare provider's assessment of the patient's condition.- Include a differential diagnosis, listing possible conditions based on the subjective and objective findings.- Discuss any further diagnostic tests required to confirm or rule out specific conditions.- Mention any consultations or referrals to other specialists.2.3 Diagnostic Impressions:- Provide a concise summary of the confirmed diagnosis or a list of potential diagnoses.- Include the rationale behind the diagnosis, considering the patient's symptoms, physical examination, and test results.- Discuss any complications or comorbidities related to the diagnosis.- Mention any chronic conditions that may impact the patient's current illness.3. Plan:3.1 Treatment Plan:- Outline the proposed treatment options, including medications, therapies, or procedures.- Specify the dosage, frequency, and duration of medications.- Discuss potential side effects or contraindications of the chosen treatment.- Mention any lifestyle modifications or patient education required.3.2 Follow-up:- Schedule any necessary follow-up appointments or tests.- Specify the expected timeline for improvement or resolution of symptoms.- Discuss any potential red flags or warning signs that require immediate medical attention.- Mention any referrals to other healthcare providers or specialists.3.3 Patient Education:- Provide information to the patient regarding their condition, treatment options, and expected outcomes.- Discuss any lifestyle modifications or self-care measures the patient should undertake.- Address any concerns or questions the patient may have.- Offer resources or references for additional information.Conclusion:In conclusion, SOAP English medical records provide a structured and comprehensive approach to documenting patient information. The subjective section captures the patient's background, present illness, and review of systems. The objective section includes physical examination findings and diagnostic impressions. The plan section outlines the treatment plan, follow-up, and patient education. By following this organized format, healthcare providers can ensure accurate and consistent documentation of patient care.。
全身酸痛病历模板范文
全身酸痛病历模板范文英文回答:Medical History Template for General Body Aches and Pains.Patient Name: [Insert Patient Name]Date of Birth: [Insert Date of Birth]Gender: [Insert Gender]Contact Information: [Insert Contact Information]Chief Complaint:The patient presents with complaints of general body aches and pains.Present Illness:The patient reports experiencing widespread body aches and pains for the past [insert duration]. The pain is described as a dull, constant ache that affects multiple areas of the body. The intensity of the pain varies throughout the day and is not relieved by rest or over-the-counter pain medications.Medical History:The patient has a history of [insert relevant medical conditions]. [Insert any known allergies or sensitivities]. The patient has previously received treatment for [insert relevant treatments or surgeries]. The patient is currently taking [insert current medications].Review of Systems:The patient denies any recent trauma or injury. There are no associated symptoms such as fever, chills, headache, or joint swelling. The patient reports no recent changes in weight or appetite. There are no symptoms suggestive ofrespiratory, gastrointestinal, cardiovascular, or neurological disorders.Family History:There is no significant family history of similar symptoms or medical conditions.Social History:The patient denies any tobacco, alcohol, or illicit drug use. The patient reports a sedentary lifestyle and no recent changes in physical activity or exercise routine.Physical Examination:On physical examination, the patient appears generally well-nourished and in no acute distress. Vital signs are within normal limits. Generalized tenderness is noted upon palpation of various muscle groups. No joint swelling or deformities are observed. Neurological examination reveals normal strength, sensation, and reflexes.Laboratory and Diagnostic Tests:[Insert any laboratory or diagnostic tests performed, if applicable]. Results are pending and will be reviewed upon receipt.Assessment and Plan:Based on the patient's history, physical examination, and initial laboratory findings, the working diagnosis is generalized musculoskeletal pain. Further evaluation and management will be guided by the results of additional tests. Treatment options may include pain management strategies, physical therapy, and lifestyle modifications.Patient Education and Follow-up:The patient will be educated about the potential causes of generalized body aches and pains and the importance of adhering to the recommended treatment plan. Follow-up appointments will be scheduled to monitor the patient'sprogress and adjust the treatment plan as needed.中文回答:全身酸痛病历模板范文。
英文病历报告作文模板
英文病历报告作文模板Patient Information- Name: [Patient's Full Name]- Gender: [Male/Female]- Age: [Patient's age]- Date of Admission: [MM/DD/YYYY]Chief ComplaintThe patient presented with [specific symptoms/complaints] which started [duration].History of Present IllnessThe patient reported [detailed description ofsymptoms/complaints]. The symptoms worsened over the past [duration]. The patient experienced [associated symptoms] and tried [any self-medication or home remedies] but noticed no improvement. There was no history of trauma or injury.Past Medical HistoryThe patient has a history of [chronic/acute medical conditions, if any] which includes [specific conditions]. The patient has taken[previous medications/treatments] for these conditions.Social HistoryThe patient has a [specific occupation] and lives in [specific area]. The patient does [specific habits] such as smoking or drinking alcohol [frequency]. There is no significant family medical history.Physical Examination- Vital Signs:- Blood Pressure: [value] mmHg- Heart Rate: [value] bpm- Respiratory Rate: [value] bpm- Temperature: [value]C- General Appearance:The patient appears [general appearance of the patient].- Systemic Examination:- Cardiovascular: [specific findings]- Respiratory: [specific findings]- Gastrointestinal: [specific findings]- Neurological: [specific findings]- Musculoskeletal: [specific findings]Laboratory and Imaging Findings- Blood Test Results:- Complete Blood Count: [values]- Biochemical Profile: [values]- Others: [specific findings]- Imaging:- [Specific imaging tests performed]- Results: [specific findings]DiagnosisAfter evaluating the patient's medical history, physical examination, and laboratory/imaging findings, the following diagnosis was made:[Primary Diagnosis]Treatment and ManagementThe patient was started on [specific treatment plan] which includes [medications, therapies, or procedures]. The patient wasadvised to [specific instructions] and scheduled for [follow-up tests/appointments, if any].Follow-upThe patient will be followed up in [specific time frame] to assess the response to treatment and manage any complications that may arise. The patient was given contact information for any urgent concerns or changes in symptoms.Discussion and ConclusionThis case report highlights the presentation, evaluation, and management of a patient with [specific condition]. The patient's symptoms were appropriately addressed through a systematic approach involving history taking, physical examination, and laboratory/imaging investigations. The provided treatment plan aims to address the underlying cause and improve the patient's overall well-being. Continuous monitoring and follow-up will guide further management decisions.Note: This medical case report is fictional and serves as a template for educational purposes. Any resemblance to actualpatients is purely coincidental.。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Medical Records for Admission
Medical Number: 701721 General information
Name:Liu Side
Age: Eighty
Sex: Male
Race:Han
Nationality:China
Address: NO.**, Dandong Road, Jiefang Rvenue, Hankou, Hubei. Tel: ****** Occupation: Retired
Marital status: Married
Date of admission: Aug 6th, 2001
Date of record: 11Am, Aug 6th, 2001 Complainer of history: patient’s son and wife Reliability: Reliable
Chief complaint: Upper abdominal pain for ten days, hematemesis, hematochezia and unconsciousness for four hours.
Present illness:
The patient felt upper abdominal pain for about ten days ago. He didn’t pay attention to it and thought he had ate something wrong. At 6 o’clock this morning he fainted and rejected lots of blood and gore. Then hemafecia began. His family sent him to our hospital and received emergent treatment. So the patient was accepted as “upper gastrointestine hemorrhage and hemorrhagic shock”.
Since the disease coming on, the patient didn’t urinate.
Past history
The patient is healthy before.
No history of infective diseases. No allergy history of food and drugs. Personal history
He was born in Wuhan on Nov 19th, 1921 and almost always lived in Wuhan. His living conditions were good. No bad personal habits and customs.
Family history: His parents have both deads.
Physical examination
T 36.5℃, P 130/min, R 23/min, BP 100/60mmHg. He was well developed and moderately nourished. Active position. His consciousness was not clear. His face was pale and the skin was not stained yellow. No cyanosis. No pigmentation. No skin eruption. Spider angioma was not seen. Superficial lymph nodes were not found enlarged. Respiratory movement was bilaterally symmetric with the frequency of 23/min. No pleural friction fremitus. Resonance was heard during percussion. No abnormal breath sound was heard. No wheezes. No rales. Border of the heart was normal. Heart sounds were strong and no splitting. Rate 150/min. Cardiac rhythm was not regular. No pathological murmurs. Abdomen was flat and soft. No bulge or depression. No abdominal wall varices. Gastralintestinal type or peristalses were not seen. Tenderness was obvious around the navel and in upper abdoman. There was not rebound tenderness on abdomen or renal region. Liver and spleen was untouched. No masses. Shifting dullness negative. No vascular murmurs. No edema.
Physiological reflexes were existent without any pathological ones.
Investigation
Blood-Rt: Hb 69g/L RBC 2.70×1012/L WBC 1.1×109/L PLT 120×109/L
History summary
1.Patient was male, 80 years old
2.Upper bellyache ten days, haematemesis, hemafecia and unconsciousness for four hours.
3.No special past history.
4.Physical examination: T 37.5℃, P 130/min, R 23/min, BP 100/60mmHg Superficial lymph nodes were not found enlarged. Heart rate was 150/min. Cardiac rhythm was not regular. Tenderness was obvious around the navel and in upper abdomen. No rebound tenderness. Liver and spleen was untouched. No masses. Shifting dullness negative. No other positive signs.
5.investigation information:
Blood-Rt: Hb 69g/L RBC 2.70×1012/L WBC 1.1×109/L PLT 120×109/L
Impression: upper gastrointestine hemorrhage
hemorrhagic shock
Signature: He Lin。