恶性黑色素瘤治疗(基因突变靶向治疗)
2020年恶性黑色素瘤治疗进展(最新推荐)

其他?
仁爱| 卓越| 奉献| 创新
2020 ASCO 涉及4项口头发言
仁爱| 卓越| 奉献| 创新
ASCO 10005(标准剂量-回顾性研究)
• 真实世界里,与单免疫治疗相比,双免疫治疗ORR(32% vs 13%)与OS(20.4 vs 8.8 mo)更优; • 安全性方面,G3/4级副反应,双免疫组31%,Ipi组33%;
OpACIN-neo研究
仁爱| 卓越| 奉献| 创新
ASCO 10002 PRADO研究-小结
Q3:近期看大手术可以不做远期疗效?
• 研究进一步证实了OpACIN-neo研究使用的低剂量Y药联合O药的高缓解率且低毒; • 影像学缓解率(低)与病理缓解率(高)不一致; • 与TLND(治疗性淋巴结清扫)相比,标记性淋巴结切除手术方式降低了副反应,提高了生活质量; • 从近期研究结果看,对于新辅助治疗后获得CR或接近CR的患者,可以避免大手术.
仁爱| 卓越| 奉献| 创新
ASCO 10004(剂量减量/疗程不减)
• 低剂量ipi(1mg/kg)联合K药显示了显著的抗肿瘤效应,iORR为27%; • 低剂量ipi(1mg/kg)联合K药的3-4级不良反应发生率(27%)要低于标准剂量的Y药联合O药的发生率
(59%,历史数据)
仁爱| 卓越| 奉献| 创新
新辅助目前不是临床常规,特别是肢端型和粘膜型患者 需要降期的手术患者只建议BRAF突变的患者(疗效好)
仁爱| 卓越| 奉献| 创新
三、PD-1单抗耐药后治疗策略
10003 10004 10005 10006
仁爱| 卓越| 奉献| 创新
SITC于2020.3耐药定义
晚期治疗——原发耐药:PD/SD<6m;继发耐药:CR/PR/SD>6m 辅助治疗——原发耐药(早期复发):<12周;晚期复发:>12周
黑色素瘤晚期使用靶向药效果如何

黑色素瘤是一种侵袭性强、预后差的恶性肿瘤,好发生于 30 岁以上的成人和老年人,男性多于女性,而且男性病人死亡率较高,儿童罕见此病。
当黑色素瘤到了晚期时,很容易出现其他脏器组织的扩散转移,手术切除的可能性很小,因此药物治疗成了重要的治疗方法,那黑色素瘤晚期使用靶向药效果如何呢?靶向药是通过一种血管内皮生长因子的合成,抑制肿瘤血管的生存,使肿瘤细胞在生长过程中发生缺血、坏死,从而达到治疗黑色素瘤的目的。
相对于传统的化疗,靶向药在疗效和毒副作用方面都具有明显的优势,能控制病情发展,抑杀机体内的癌细胞,改善症状,延长患者生命。
但是靶向药也会带来一定的副作用,如腹泻、恶心呕吐等,还易出现耐药性,患者在服用一年左右的时间就会耐药,达不到治疗的效果。
另外并非所有的患者都能获得很好的疗效,一般临床上可以通过检测基因的方法,确定使用相应的药物达到良好的效果。
不过靶向药的价格也是非常高的,患者在选择时一定要考虑自身的具体病情和经济状况。
黑色素瘤病情复杂,尤其是当到了晚期时病情较重,患者单纯依靠靶向药物治疗效果可能并不理想,需要联合其他有效的治疗手段,如中医等。
中医联合靶向药有助于减缓患者耐受的程度,缓解靶向药的副作用,还能抑制肿瘤,提高整体的治疗效果,进一步延长患者生命。
对于不能或者不愿服用靶向药的患者,也可以考虑中医治疗为主。
中医在治疗时使用中草药,所需的费用要低很多,且副作用小,像年龄大、身体弱的患者也能耐受。
中医治疗黑色素瘤从整体出发,能在一定程度上控制病情,也会帮助患者调理机体,提高患者的免疫力和抵抗力,对于提高生存质量,延长生存时间有积极的作用。
中医治疗能够将治疗与调理同时进行,注重补充患者的元气,应及时配合治疗,由于出身于中医世家,袁希福自幼便接触中医,熟读中医古典名著。
此后,其还曾先后至北京中医药大学及中国中医研究院深造,为从事中医治疗肿瘤打下坚实的理论基础。
从医近40年来,袁希福接诊各类肿瘤患者数万名,其中不少都是复发患者,或病属晚期,甚至是被判“死刑”的末期患者。
恶性黑色素瘤的免疫治疗进展

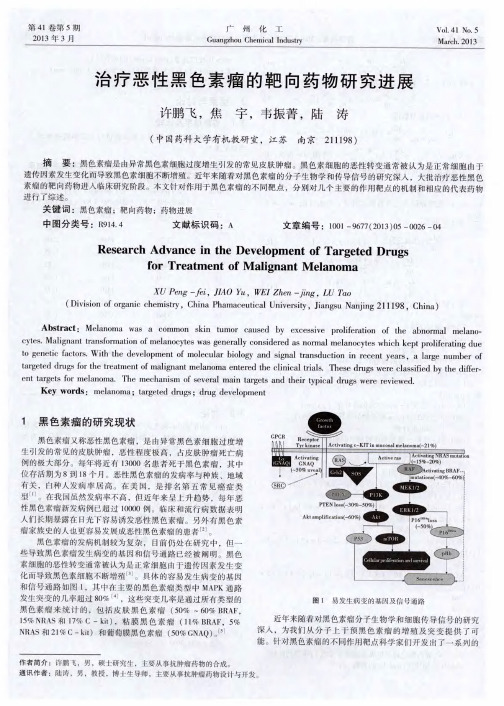
恶性黑色素瘤的免疫治疗进展齐忠慧;斯璐【摘要】恶性黑色素瘤病死率高、预后差,但随着基础免疫学和肿瘤生物学的迅速发展,针对恶性黑色素瘤发生发展、侵袭转移的过程所进行的免疫治疗正进入一个新时期,黑色素瘤患者的生存获得可观改善.目前免疫治疗主要围绕PD-1单克隆抗体、CTLA-4单克隆抗体、免疫联合治疗展开.Pembrolizumab、Nivolumab、Ipilimumab单用、Nivolumab联合Ipilimumab以及Talimogene laherparepvec均已被证明是有效和安全的,已被美国食品药品管理局(FDA)批准用于恶性黑色素瘤的治疗.该文概述了目前免疫治疗药物的最新进展,并探讨其前景及挑战.【期刊名称】《医药导报》【年(卷),期】2019(038)008【总页数】7页(P997-1003)【关键词】恶性黑色素;免疫治疗;免疫检查点抑制剂;免疫联合治疗【作者】齐忠慧;斯璐【作者单位】北京大学肿瘤医院暨北京市肿瘤防治研究所肾癌黑色素瘤内科、恶性肿瘤发病机制及转化研究教育部重点实验室,北京 100142;北京大学肿瘤医院暨北京市肿瘤防治研究所肾癌黑色素瘤内科、恶性肿瘤发病机制及转化研究教育部重点实验室,北京 100142【正文语种】中文【中图分类】R979.1恶性黑色素瘤(malignant melanoma,MM)恶性程度极高,全球每年新发病例约20万例,我国每年新发病例达2万例[1]。
早期黑色素瘤患者术后5年总体生存率(overall survival,OS)较高,晚期黑色素瘤患者术后5年OS为24%~29%,ⅢC、Ⅳ期患者5年OS仅10%~19%。
传统化疗单药总体反应率(overall response rate,ORR)均小于20%,BRAF抑制剂的ORR虽达50%,但存在爆发性耐药问题。
白细胞介素2、肿瘤疫苗、过继T细胞疗法因为不良反应重或疗效欠佳未得以推广[2-3]。
相比之下,以免疫检查点抑制剂为首的免疫治疗可显著延长患者OS,降低死亡及复发风险,改善无进展生存期(progression-free survival,PFS)。
黑色素瘤能治愈吗 怎么治疗黑色素瘤
黑色素瘤能治愈吗怎么治疗黑色素瘤*导读:黑色素瘤能治愈吗?……
黑色素瘤是一种多发于成人身上,发病率低,但恶性程度极高的肿瘤。
因此,患者第一时间发现了,要趁早就医。
越早治疗,治愈的机会就越大。
虽然黑色素瘤恶性程度高,但是也有治愈的可能。
患者要保持积极的心态,选择正确的疗法,到正规的医院就医。
黑色素瘤可分为良性黑色素瘤和恶性黑色素瘤。
良性黑色素瘤较恶性黑色素瘤而言,比较容易治愈。
但它的早期症状往往会被人忽略。
当患者发现黑色素瘤越来越粗糙的时候,并且伴随着片状的脱屑。
严重时甚至会出血、渗液,异常瘙痒、溃疡等。
这些都是恶性黑色素瘤的早期症状,当出现以上症状时就要及早就医了。
那么,该如何治疗黑色素瘤呢?
*一、手术疗法
患者一旦发现自己得了黑色素瘤,要尽早进行手术割除,选择正规的医院尽早就医,可以选择生物治疗或放化疗、分子靶向治疗等科学的治疗方法,越早治疗,治疗的效果就越好。
\
*二、饮食疗法
患者不仅要外治还要内调,患者的饮食要多样化,营养要均衡。
首先,患者们要少食富含蛋白质的食物,蛋白质摄入过多反
而会增加肠道的负担,消弱肠道的消化吸收功能。
因此,患者要适当减少蛋白质的摄入。
其次,应多吃富含维生素C、维生素A 的食物,多吃能抑制病情的食物,比如卷心菜等等。
多吃富含营养的干果种子,多吃新鲜的绿色蔬菜,多吃低脂肪的食物,比如鸡肉、瘦肉等。
患者要切忌辛辣刺激的食物,不暴饮暴食,不吃腌制的食物,忌烟酒。
患者要切忌盲目用药,要坚持科学的治疗方法,科学饮食,才能最大程度上提高了治愈的可能性。
治疗恶性黑色素瘤的靶向药物研究进展
一
6 2 4 4在恶性黑色素瘤治疗 中具有较强的抗癌 活性 和较好 的耐受 性 。但最近一次 大规模 的二期 临床试 验关于 比较 A Z D 6 2 4 4与 替莫唑胺 ,A Z D 6 2 4 4的反 应率 只有 1 2 % ,并 且在 P F S上也 没 有有任何 的优势 。
பைடு நூலகம்
的经常突变激活提供 了潜在的理论基础 ( 例如 ,经常出现的 B— 制剂 A Z D 6 2 4 4和替莫唑胺比较 ,反应率没有提高 ,对 P F S也没有 R a f V 6 0 0 E突变) 。由于 B R A F突变几率 和致癌潜力相 对较 高 ,研 影响。相 比较而言 ,G S K l I 2 0 2 1 2更有前途 ,反应率约为 4 0 %,并 究者长期致力于开发选择性抑制 B R A F的药物 。开始 尝试使用索 且现在正处于和 B R A F抑制剂联合用药的临床研究阶段。 拉非尼治疗黑色素瘤患者 ,由于索拉非尼对靶标 B R A F选择性较 2 . 2.1 AZD62 4 4 差 而导 致 对 野生 型 B R A F产 生 脱靶 效 应 ,治 疗效 果 不 是很 成 A Z D 6 2 4 4 / S e l u m e t i n i b( 图4 )是该 类药 物 中第一 个进 入 临 功 。最近开发 出了一些高选择性的药物 ,只对突变 型 B R A F 床一期 的药物 , 目前 已进 入针对 多个肿 瘤株 的临床 二期 研究 。 产 生抑制作用 ,对野生型 B R A F几乎不产生作用。 ME K信号分子抑制剂 A Z D 6 2 4 4联合化疗在 动物模 型 中已经 显
黑色素瘤最佳治疗方案

黑色素瘤最佳治疗方案黑色素瘤,也称为恶性黑色素瘤,是一种高度侵袭性的皮肤癌症,由于其高度恶性和易转移的特点,因此需要早期诊断和科学合理的治疗方案。
本文将介绍黑色素瘤的治疗方法,包括手术治疗、放疗、化疗和靶向治疗等。
1. 手术治疗手术治疗是黑色素瘤最主要的治疗方法之一,对于早期病变的黑色素瘤患者来说,手术切除病变部位是最有效的治疗手段之一。
手术切除应尽可能彻底,包括肿瘤组织的切除以及周围正常组织的安全保留。
对于深度浸润和转移性黑色素瘤,手术可用于减轻症状和延长生存期,但常常不能治愈。
2. 放疗放疗在黑色素瘤的治疗中有一定的作用,可以用于术后辅助治疗、转移灶的局部控制和减轻疼痛等症状。
对于无法手术切除的患者、术后高风险因素患者以及肺、骨或脑等器官转移的患者,放疗可以有效地控制病情进展。
3. 化疗化疗在黑色素瘤的治疗中有限的作用,处理复发和转移性疾病时可以作为一种选择。
常用的化疗药物包括达卡巴噻嘧啶、亚甲基丁苯环酮等,但是由于黑色素瘤对化疗药物的反应较差,疗效有限。
4. 靶向治疗近年来,靶向治疗在黑色素瘤的治疗中取得了一定的突破。
靶向治疗是通过针对黑色素瘤细胞中特定的分子靶点,选择合适的药物进行治疗。
例如,BRAF V600E突变是黑色素瘤常见的阳性突变,针对该突变可以使用BRAF抑制剂如达西利尼或维米非尼进行治疗。
此外,CTLA-4抑制剂如伊皮利慎在黑色素瘤的治疗中也显示出了良好的疗效。
5. 免疫治疗免疫治疗在黑色素瘤的治疗中也显示出了一定的效果。
通过激活患者自身的免疫系统,增强对肿瘤细胞的识别和清除能力。
免疫检查点抑制剂如PD-1抑制剂和PD-L1抑制剂,可以抑制黑色素瘤细胞表面PD-1/PD-L1的相互作用,恢复患者的免疫应答,提高治疗效果。
综上所述,针对不同阶段和特点的黑色素瘤,最佳的治疗方案可能是多种治疗方法的综合应用。
早期诊断和早期治疗是提高黑色素瘤治愈率和生存期的关键。
此外,治疗方案的选择应根据患者的具体情况进行个体化治疗,包括年龄、身体状况、病变特点、转移情况等因素的综合考虑。
盘点黑色素瘤治疗方法及临床进展
盘点黑色素瘤治疗方法及临床进展展开全文在2011年前,转移性黑色素瘤患者的生存时间很短。
近年来,伴随着靶向和免疫治疗的兴起,转移性黑色素瘤几乎无药可用的局面被扭转。
同时,早中期黑色素瘤患者也有了更多选择。
下文将针对近年来靶向及免疫治疗在黑色素瘤领域的临床进展撷英介绍。
Part.1靶向治疗进展1. 与黑色素瘤相关的基因突变一部分黑色素瘤被发现存在基因突变,其中,最常见的就是BRAF 突变。
在国外,近50%的黑色素瘤患者存在BRAF突变,我国也有近1/4的患者携带该突变[1]。
与没有突变的患者相比,携带该突变的患者预后更差——与野生型相比,死亡风险会增加3倍[1]。
BRAF基因位于MAPK通路(即RAS/RAF/MEK/ERK通路)上,它是一条生长因子信号转导通路。
BRAF基因在通路中,负责编码丝氨酸/苏氨酸特异性激酶,能够调控黑色素细胞的生长、分化和死亡。
最常见的BRAF突变为缬氨酸(V)突变为谷丙氨酸(E)(BRAF V600E),其次为缬氨酸(V)突变为赖氨酸(K)(BRAFV600K)。
除了最常见的BRAF突变,其他与黑色素瘤突变相关的突变包括NRAS(突变率为13.25%)、MEK1(6%)、KIT(2.6%)、CTNNB1(2%)、GNA11(2%)、GNAQ(1%)。
有意思的是,黑色素瘤的突变基本都是排他性的,这意味着患者通常只可能发生1种突变[2]。
2. 目前可用的黑色素瘤靶向药BRAF抑制剂+MEK抑制剂针对BRAF突变的BRAF抑制剂,显著地改善了黑色素瘤患者的生存。
但用药后却难免发生耐药。
随后的研究发现,在BRAF抑制剂的基础上,添加MEK抑制剂,不仅能够显著提高有效率,还能阻止耐药的发生。
目前已获得美国食品与药物管理局(FDA)批准的BRAF抑制剂和MEK抑制剂包括:① BRAF抑制剂:•达拉非尼(商品名:Tafinlar)•维罗非尼(商品名:Zelboraf)•Encorafenib(商品名:Braftovi)② MEK抑制剂:•曲美替尼(商品名:Mekinist)•考比替尼(商品名:Cotellic)•Binimetinib(商品名:Mektovi)这些药及组合方案的获批情况如下表所示。
恶性黑色素瘤诊断与治疗PPT

恶性黑色素瘤的危害
皮肤癌:恶性黑色 素瘤是一种皮肤癌, 可导致皮肤损伤和 病变
转移:恶性黑色素 瘤可转移到其他器 官,如淋巴结、肝 脏、肺等
死亡率高:恶性黑 色素瘤的死亡率较 高,尤其是晚期患 者
治疗困难:恶性黑 色素瘤的治疗难度 较大,需要综合治 疗,如手术、化疗 、放疗等
03
恶性黑色素瘤的诊断方法
保持良好的心理 状态,避免焦虑 和抑郁
定期进行体检, 监测身体状况, 及时发现并处理 并发症
复发与转移的监测与处理
定期随访:监测患者的病情变化,及时发现复发和转移 影像学检查:如CT、MRI等,用于监测肿瘤的复发和转移情况 实验室检查:如肿瘤标志物检测,用于监测肿瘤的复发和转移情况 治疗方案:根据复发和转移的情况,制定相应的治疗方案,如手术、放疗、化疗等
术后护理:伤口护理、预防感 染、定期复查等
放射治疗
放射治疗原理:利用高能射线 杀死肿瘤细胞
放射治疗方法:外照射、内照 射、立体定向放射治疗等
放射治疗适应症:适用于局部 晚期、转移性恶性黑色素瘤
放射治疗副作用:皮肤反应、 骨髓抑制、胃肠道反应等
化学治疗
化学药物:如顺 铂、卡铂等
作用机制:通过 抑制肿瘤细胞的 DNA合成,阻 止肿瘤细胞的生 长和繁殖 Nhomakorabea 病理学检查
组织病理学检 查:通过显微 镜观察组织切 片,判断肿瘤 的性质和分期
免疫组织化学 检查:通过检 测肿瘤细胞表 面的抗原,判 断肿瘤的性质
和分期
基因检测:通 过检测肿瘤细 胞的基因突变, 判断肿瘤的性
质和分期
细胞遗传学检 查:通过检测 肿瘤细胞的染 色体异常,判 断肿瘤的性质
和分期
影像学检查
其他治疗方法
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Inhibition of Mutated, Activated BRAF in Metastatic MelanomaKeith T. Flaherty, M.D., Igor Puzanov, M.D., Kevin B. Kim, M.D., Antoni Ribas, M.D., Grant A. McArthur, M.B., B.S., Ph.D., Jeffrey A.Sos man, M.D., Peter J. O'Dw yer, M.D., Richard J. Lee, M.D., Ph.D., Joseph F. Grippo, Ph.D., Keith Nolop, M.D., and Paul B. Chapman,M.D.BACKGROUNDThe identification of somatic mutations in the gene encoding the serine–threonine protein kinase B-RAF (BRAF)in the majority of melanomas offers an opportunity to test oncogene-targeted therapy for this disease.Metastatic melanoma is an aggressive disease for which there are few effective therapies. The two therapiesapproved by the Food and Drug Administration, high-dose interleukin-2 and dacarbazine, are each associatedwith response rates of only 10 to 20% and a small percentage of complete responses; neither is thought toimprove overall survival.1,2 In randomized trials, the median survival among patients treated with dacarbazinewas less than 8 months.3,4A search for mutations in a component of the mitogen-activated protein (MAP) kinase pathway in a large panel ofcommon cancers revealed that 40 to 60% of melanomas, and 7 to 8% of all cancers, carry an activating mutation in the gene encoding the serine–threonine protein kinase B-RAF (BRAF). 5-15 Ninety percent of reported BRAF mutations result in a substitution of glutamic acid for valine at amino acid 600 (the V600E mutation). This BRAF mutation constitutively activates BRAF and downstream signal transduction in the MAP kinase pathway. BRAF mutations are also found in 40 to 70% of papillary or anaplastic thyroid cancers6-8,16-18 and in a small percentage of several other types of tumor.PLX4032 (Plexxikon; RG7204, Roche Pharmaceuticals) is a potent inhibitor of BRAF with the V600E mutation.Preclinical studies showed that PLX4032 and its analogue PLX4720 inhibit the kinase activity of BRAF with the V600E mutation at low nanomolar concentrations, abrogate signaling through the MAP kinase pathway, andblock proliferation of cells carrying BRAF with the V600E mutation in vitro at high nanomolar concentrations.17,18 Orally administered PLX4720 inhibits the growth — and, at higher doses, induces the regression — of human melanoma tumors transplanted into immunocompromised mice. None of these effects are observed in normal tissues or in tumor cells that lack a BRAF mutation.We conducted a trial of the use of PLX4032 in patients with metastatic cancer. The primary goals were to define the safety and pharmacokinetic characteristics of treatment with continuous, twice-daily administration ofPLX4032, to determine the maximum dose that could be administered until adverse effects prevented furtherdose increases (i.e., the recommended phase 2 dose), and to determine the objective response rate, the duration of response, and the rate of progression among patients who had melanoma tumors with the V600E BRAFmutation and who were given the recommended phase 2 dose of PLX4032.METHODSStudy DesignThe study was sponsored by Plexxikon and Roche Pharmaceuticals, which provided the study drug. The study was designed by two academic authors and one industry author. All authors made the decision to submit themanuscript for publication. All authors analyzed the data, prepared the manuscript, and vouch for the completeness and accuracy of the data and analyses. The study was conducted in accordance with the protocol.Dose-Escalation PhasePLX4032 was initially in a crystalline formulation. In the dose-escalation phase of the study, which involved several consecutively enrolled groups of three to six patients, the first group received 200 mg of PLX4032 by mouth daily; subsequent groups received the drug at higher doses, according to a dose-escalation scheme. This formulation was found to have poor bioavailability (see the Results section), and enrollment for thedose-escalation phase was halted while the drug was reformulated as a highly bioavailable microprecipitated bulk powder, initially as a 40-mg capsule and subsequently as 80-mg and 120-mg capsules, as well as 240-mg tablets. Enrollment was resumed, with newly enrolled patients receiving the microprecipitated-bulk-powder formulation at a dose of 160 mg (two 80-mg capsules) twice daily, with subsequent escalation.Patients received continuous therapy with PLX4032 unless unacceptable side effects or disease progression occurred. Doses were not escalated unless the patients receiving the highest current dose had been observed for at least 4 weeks and dose-limiting side effects had been reported in fewer than a third. Dose escalation in a given patient was permitted if the safety and adverse-effect profile had been established for the next highest dose. The recommended phase 2 dose was defined as the highest dose at which no more than one of six patients had dose-limiting side effects.Extension PhaseOnce the recommended phase 2 dose had been identified, an extension cohort was treated at this dose. In this cohort, all patients had melanoma and a prospectively identified V600E BRAF mutation. The primary objective in the extension cohort was to determine the response rate. Secondary objectives were to define the toxicity and pharmacokinetics of PLX4032 more precisely and to obtain data on pharmacodynamic effects.PatientsEligibility criteria included the provision of written informed consent, an age of 18 years or older, solid tumors confirmed histologically that were refractory to standard therapy or for which standard or curative therapy did not exist, Eastern Cooperative Oncology Group performance status score of 0 (able to be fully active and carry out all predisease activities without restriction) or 1 (unable to perform physically strenuous activity but ambulatory and able to carry out work of a light or sedentary nature, such as light housework or office work),19 life expectancy of 3 months or longer, absence of known progressing or unstable brain metastases, and adequate hematologic, hepatic, and renal function.The dose-escalation phase of the trial was open to patients with any type of tumor, although patients who had melanomas with the V600E mutation in BRAF were overrepresented because of the selective activity of PLX4032 against such tumors in preclinical testing. For the extension cohort, eligibility was restricted to patients with melanomas harboring a V600E BRAF mutation, as ascertained by means of a polymerase-chain-reaction assay (TaqMan, Applied Biosystems). This assay involves hybridizing a probe specific to the 1799T→A substitution that results in the V600E BRAF mutation with DNA isolated from formalin-fixed, paraffin-embedded tumor tissue and determining the presence or absence of amplification after repeated chain-reaction cycles.20Study AssessmentsSafety evaluations were conducted at baseline, day 8, day 15, day 29, and every 4 weeks thereafter. These evaluations included a physical examination, electrocardiography, laboratory studies that included a complete blood count, clinical chemical testing, and urinalysis. Adverse events were graded according to the Common Terminology Criteria for Adverse Events (version 3.0)(/protocolDevelopment/electronic_applications/docs/ctcaev3.pdf). During the trial, squamous-cell carcinoma, keratoacanthoma type, was observed in several patients (see the Results section). As a result, the protocol was amended to ensure that patients underwent dermatologic evaluations at baseline and every 2 months during the study; computed tomographic (CT) scans of the chest were analyzed for the appearance of new lesions suggestive of a primary cancer.CT studies were performed at 8-week intervals during therapy in all patients and at the end of the first 4 weeks of therapy in some patients. The findings were judged according to the Response Evaluation Criteria in Solid Tumors (RECIST), version 1.0. A complete response was defined as the disappearance of all target lesions, and a partial response as a decrease by at least 30% in the sum of the largest diameter of each target lesion, relative to the corresponding sum at baseline. Progressive disease was defined as an increase by at least 20% in the sum of the largest diameter of each target lesion, relative to the smallest corresponding diameter recorded since the start of treatment, or the appearance of one or more new lesions. Stable disease was defined as the absence of shrinkage sufficient for a partial response and the absence of enlargement sufficient for progressive disease, relative to the corresponding sum at baseline. Progression-free survival was defined as the time from the first day of treatment to the first documentation of disease progression or death, whichever occurred first.Pharmacokinetic assessments were made on day 1 and day 15 of the first 4 weeks of therapy, and single plasma samples were obtained every 4 weeks during the study. Plasma samples were analyzed by means ofhigh-performance liquid chromatography, with detection by means of mass spectroscopy.Patients in the dose-escalation phase who were receiving a dose greater than 160 mg twice daily and patients in the extension cohort underwent 18F-fluorodeoxyglucose–positron-emission tomography (FDG-PET) at baseline and on day 15 of the first 4 weeks of therapy. Selected patients underwent tumor biopsy before the start of therapy as well as on day 15. Biopsy specimens were immediately fixed in formalin for analysis of phosphorylated extracellular signal-regulated kinase (ERK), the protein cyclin D1, and the monoclonal antibody Ki-67 by means of immunohistochemistry. The sampled tumors were cutaneous or superficial lymph-node lesions; except in the case of one patient, sequential biopsy specimens were not taken from the same lesion.Statistical AnalysisFor the primary end point of a partial or complete response in the extension cohort, we calculated that a sample of 32 patients would provide 95% confidence (α=0.05), with 80% power (β=0.20), that an observed response rate of 40% would be consistent with a true response rate of more than 10%, which was considered justification for further study. For this report, January 31, 2010, was the cutoff date for the safety and efficacy follow-up.RESULTSPatientsFifty-five patients were enrolled in the dose-escalation phase of the study (see Fig. 2 in the Supplementary Appendix, available with the full text of this article at ); 32 additional patients with metastatic melanoma that carried the V600E BRAF mutation were treated at the recommended phase 2 dose in the extension phase(Table 1TABLE 1Baseline Characteristics of the Patients, According to Study Cohort.). The majority of patients (49 of 55 [89%]) in the dose-escalation cohort had metastatic melanoma; 3 of the remaining 6 patients had papillary thyroid cancer that carried the V600E BRAF mutation. Screening for the V600E BRAF mutations was not a requirement for study entry during the dose-escalation phase, but throughout the trial, an increasing number of patients were prospectively identified as having the mutation (for a total of 16 of the 21 patients with melanoma who were enrolled in the groups receiving 240 mg twice daily to 1120 mg twice daily).The initial crystalline formulation of PLX4032 was found to have no dose-limiting side effects or antitumor activity at doses of 200 mg daily to 1600 mg twice daily in consecutively enrolled groups of patients. Since the serum levels detected were lower than the levels predicted in preclinical models to be effective, amicroprecipitated-bulk-powder formulation with substantially higher bioavailability was developed and used for the remainder of the study; the lowest dose was 160 mg twice daily, and escalated doses were 240, 320 or 360, 720, and 1120 mg twice daily (Fig. 2 in the Supplementary Appendix). Patients who had been receiving the crystalline formulation were switched to the microprecipitated-bulk-powder formulation. The protocol allowed the dose to be reduced if side effects developed.Once the recommended phase 2 dose was established for the microprecipitated-bulk-powder formulation in the dose-escalation cohort, the extension cohort was enrolled. All patients in the extension cohort had melanoma carrying the V600E BRAF mutation (Table 1).Adverse EventsDuring the latter part of the dose-escalation phase of the trial, when the microprecipitated-bulk-powder formulation of PLX4032 was used, dose-limiting toxic effects were not observed until a dose of 720 mg twice daily was given. At the next-highest dose given to one group of patients, 1120 mg twice daily, four of the six patients had dose-limiting side effects: three patients with grade 3 rash (two of whom also had grade 3 fatigue) and onepatient with grade 3 arthralgia (Table 2TABLE 2Drug-Related Adverse E vents of Grade 2 or HigherReported in More Than 5% of the 87 Study Patients, According to the Dose of P LX4032 Given Tw ice Daily.). A dose of 960 mg twice daily was evaluated and determined to be tolerated in the first six patients given the dose, so it was established as the recommended phase 2 dose for the extension cohort. Those six patients were included as the first six patients in the extension cohort. In the extension cohort, 13 patients (41%) required a dose reduction during therapy (to 720 mg twice daily in 10 patients, to 600 mg twice daily in 1 patient, and to 480 mg twice daily in2 patients). The most common PLX4032-related grade 2 or3 side effects observed were arthralgia, rash, nausea, photosensitivity, fatigue, cutaneous squamous-cell carcinoma, pruritus, and palmar–plantar dysesthesia (Table 2). In total, 89% of all side effects were grade 1 or 2. Rashes were evenly distributed among the face or neck, trunk, and extremities.Eight patients in the dose-escalation cohort (15%) and 10 patients in the extension cohort (31%) had cutaneous squamous-cell carcinomas, with a total of 35 carcinomas. These were reviewed centrally, and all but one either were keratoacanthoma type or had features of a keratoacanthoma. The median time to the appearance of a cutaneous squamous-cell carcinoma was 8 weeks; the majority of the carcinomas were resected, and in no case did they lead to discontinuation of treatment. No squamous-cell carcinomas at other organ sites were observed during the study.PharmacokineticsPharmacokinetic analyses revealed that exposure increased with the dose throughout the range of doses of the microprecipitated-bulk-powder formulation that were administered, with exposure being proportional to dose for doses of 240 mg twice daily through 960 mg twice daily. At the recommended phase 2 dose, 960 mg twice daily, the mean (±SD) area under the plasma concentration–time curve over a 24-hour period (AUC0–24) was 1741±639μM×hour (Figure 1A FIGURE 1Mean PLX4032 Concentrations over a 24-Hour Period.), and the mean maximum concentration at steady state was 86±32 μM (Figure 1B). The mean PLX4032 level on day 15, after repeated dosing, was six to nine times the mean level on day 1, and its mean half-life was approximately 50 hours (range, 30 to 80). With the twice-daily dosing regimen, all patients were exposed to relatively constant daily levels of the drug at steady state.PharmacodynamicsTumor-biopsy specimens that had been obtained at baseline and at day 15 were available for seven of the patients in the extension cohort who were receiving PLX4032 at the recommended phase 2 dose. Tumor levels of phosphorylated ERK, cyclin D1, and Ki-67 were markedly reduced at day 15 as compared with baseline in allspecimens tested (Figure 2A FIGURE 2Repr esentative Findings of the E ffect of P LX4032 at theRecommended Phase 2 Dose in Study P atients w ith Melanoma That Carried the V600E Mutation.). This finding suggests that PLX4032 inhibited the MAP kinase pathway, resulting in decreased cyclin D1 levels and decreased proliferation. In virtually all patients, a marked decrease in tumor uptake of FDG was noted at day 15 (Figure 2B).Tumor ResponseDose-Escalation PhaseNo responses were observed at doses of 160 mg twice daily of the microprecipitated-bulk-powder formulation or at any dose of the crystalline formulation. Of the patients receiving doses of 240 mg or more twice daily, 16 had melanoma with tumors that harbored the V600E BRAF mutation. Among these 16 patients, a partial or complete response was seen in the 1 patient receiving 240 mg twice daily, 2 of the 4 patients receiving 320 or 360 mg twice daily, 4 of the 6 patients receiving 720 mg twice daily, and 4 of the 5 patients receiving 1120 mg twice daily. The overall response rate was 69% (11 of 16 patients), with 10 partial responses and 1 complete response (Fig. 1A in the Supplementary Appendix). Responses were seen at all sites of metastatic disease, including the liver, small bowel, and bone (Figure 2C). The duration of the response ranged from 2 to more than 18 months, with 4 patients still having a partial or complete response at the data cut-off date (Fig. 1B in the Supplementary Appendix). In addition to the patients with melanoma, the 3 patients with papillary thyroid cancer had a partial or complete response, with the response lasting 8 months in 1 patient (who was progression-free for 12 months) and stable disease lasting 11 and 13 months in each of the other 2 patients.A total of 5 patients with metastatic melanoma whose tumors did not have a BRAF mutation received doses of 240 mg or more twice daily. None had evidence of tumor regression during the study; 4 had progressive disease within the first 2 months of treatment.Extension PhaseThe extension cohort consisted solely of patients who had melanoma with the V600E BRAF mutation. All were treated at the recommended phase 2 dose of 960 mg twice daily. A total of 26 of the 32 patients had a response (81%), with a complete response in 2 patients and a partial response in 24 patients (Figure 3A FIGURE3Antitumor Response in E ach of the 32 Patients in the Extension Cohort.). Among patients with symptomatic metastatic disease, improvement of symptoms, such as a reduced need for narcotics for pain in 3 patients, was reported within 1 to 2 weeks. As in the dose-escalation cohort, we observed tumor responses in visceral organs and bone metastases as well as more typically responsive sites such as the lungs and lymph nodes. Responses were also routinely observed in patients with elevated lactate dehydrogenase levels (10 partial responses among the 13 patients) and in patients who had received more than one previous type of therapy (11 partial responses among the 16 patients). To date, 16 of the 32 patients are still in the study; the estimated median progression-free survival among these patients is more than 7 months, on the basis of a Kaplan–Meier analysis. The estimated median overall survival has not been reached.DISCUSSIONOur trial shows that therapy targeting tumors containing activating V600E BRAF mutations can induce complete or partial tumor regression in patients. PLX4032 induced complete or partial tumor regression in 81% of patients who had melanoma with the V600E BRAF mutation. Responses were observed at all sites of disease, including the bone, liver, and small bowel. During the dose-escalation phase of the trial, we also saw responses in patientswho were receiving doses below the recommended phase 2 dose. These efficacy data are particularly encouraging in light of the high disease burden in most of our patients and the presence of symptomatic diseas e in many of them.Most side effects related to PLX4032 appeared to be proportional to the dose and exposure to the drug. Cutaneous side effects, fatigue, and arthralgia predominated. In the extension cohort, at the dose of 960 mg twice daily, approximately 40% of patients required a short- or long-term reduction in dose to 720 mg, 600 mg, or 480 mg twice daily, many for grade 2 side effects. Squamous-cell carcinoma, keratoacanthoma type, developed in a total of 10 of 32 patients (31%); we also observed squamous-cell carcinoma, keratoacanthoma type, in patients in the dose-escalation cohort. The characteristic rapid eruption of individual, dome-shaped, nonpigmented lesions and histologic findings were present in each case. Usually, squamous-cell carcinoma, keratoacanthoma type, are well-differentiated tumors with very low invasive potential and no metastatic potential; our data do not allow us to determine their behavior in patients receiving PLX4032. Recent data show that BRAF inhibitors can activate the MAP kinase pathway in cells that lack a BRAF mutation.21-23 This activation may pertain to some of the side effects seen with PLX4032.Though the early response to PLX4032 seems to occur reliably, responsive tumors can develop resistance to treatment. Among the patients in the dose-escalation cohort who had a response to treatment, the duration of the response ranged from 2 to more than 18 months. The mechanism of secondary tumor resistance is not yet known. We also observed that in some patients with V600E BRAF mutations, the tumors showed resistance without evidence of an early response. The mechanism of this primary refractory state is currently under investigation. To date, we have not seen ―gatekeeper‖ BRAF mutations in resistant tumors, although this issue requires more investigation.Sorafenib, which inhibits BRAF (both the wild type and the V600E mutant) and v-raf-1 murine leukemia viral oncogene homologue 1 (RAF1), has been studied in melanoma. In animal models of melanoma, sorafenib has not shown selective activity against tumors carrying BRAF mutations, and in clinical trials, sorafenib used either alone or in combination with chemotherapy has not had significant antimelanoma effects.24-27 It is possible that the non-BRAF effects of sorafenib mediate side effects that limit the likelihood of achieving a drug concentration that is high enough to inhibit the V600E BRAF mutation.It is now clear that melanomas can be categorized by specific molecular changes that drive their proliferation.28 The overriding hypothesis is that inhibition of the activated pathway in the individual tumor will lead to tumor regression. There is recent preliminary evidence that imatinib can induce regression in 33% of the small proportion of melanomas driven by mutations in KIT (the v-kit Hardy–Zuckerman 4 feline sarcoma viral oncogene homologue).29 In our study, PLX4032 induced responses in the vast majority of melanomas caused by BRAF mutations, which constitute 40 to 60% of all melanomas. We do not yet know whether treatment with PLX4032 will improve overall survival; an ongoing phase 3 trial ( number, NCT01006980) is addressing that question.Supported by Plexxikon and Roche Pharmaceuticals.Drs. Flaherty, Puzanov, Kim, Ribas, McArthur, Sosman, O'Dwyer, and Chapman report the receipt by their institutions of grant support from Plexxikon to conduct this clinical trial; Drs. Flaherty, Puzanov, Kim, Ribas,Sosman, and Chapman report receiving consulting fees or reimbursement for travel expenses from Roche Pharmaceuticals; Dr. Sosman reports pending receipt of grant support from Roche Pharmaceuticals; Dr. O'Dwyer reports receiving grant support from Plexxikon; Drs. Lee and Grippo report being employees of Roche Pharmaceuticals; and Dr. Nolop reports being an employee of Plexxikon, holding equity in the company, and receiving reimbursement for travel expenses from the company. No other potential conflict of interest relevant to this article was reported.Disclosure forms provided by the authors are available with the full text of this article at .SOURCE INFORMATIONFrom the Abramson Cancer Center of the University of Pennsylvania, Philadelphia (K.T.F., P.J.O.); Massachusetts General Hospital Cancer Center, Boston (K.T.F.); Vanderbilt University, Nashville (I.P., J.A.S.); the University of Texas M.D. Anderson Cancer Center, Houston (K.B.K.); UCLA, Los Angeles (A.R.); Peter MacCallum Cancer Centre, East Melbourne, VIC, Australia (G.A.M.); Roche Pharmaceuticals, Nutley, NJ (R.J.L., J.F.G.); Plexxikon, Berkeley, CA (K.N.); and Memorial Sloan-Kettering Cancer Center, New York (P.B.C.).Address reprint requests to Dr. Flaherty at Massachusetts General Hospital Cancer Center, 55 Fruit St., Yawkey 9E, Boston, MA 02114, or at kflaherty@.We thank Drs. Katherine Nathanson and X iaowei X u (of the University of Pennsylvania) for leading the analysis of tumors for BRAF mutations and the immunohistochemical analysis of phosphorylated ERK and Ki-67 during the dose-escalation part of the study, Drs. Astrid Koehler and Michael Stumm (of Roche Pharmaceuticals) for leading these analyses during the extension part of the study, and Dr. Ruben Ayala (of Roche Pharmaceuticals) for the pharmacokinetic analysis.。