冠脉病变SYNTAX_评分_值得收藏(附图)
SYNTAX评分和冠脉风险

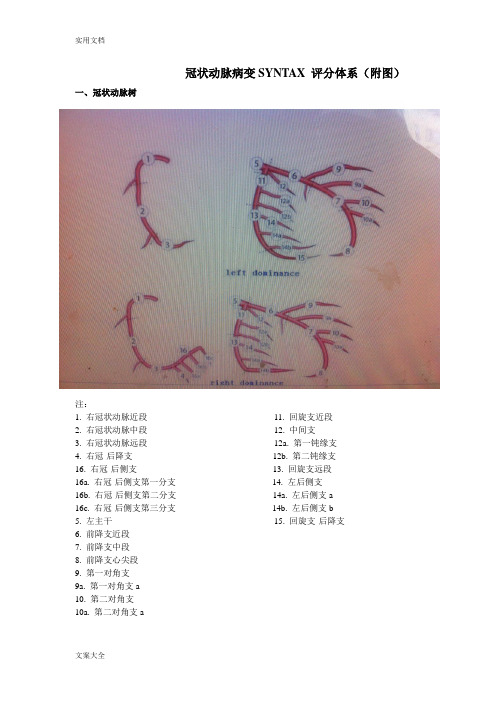
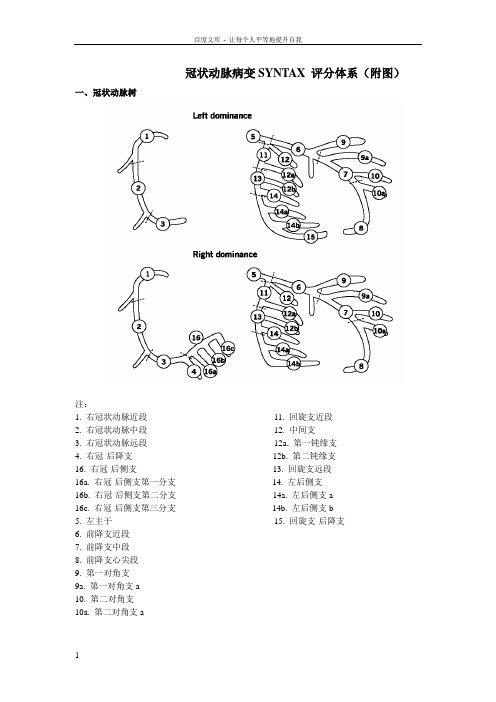
11. 回旋支近段 12. 中间支 12a. 第一钝缘支 12b. 第二钝缘支 13. 回旋支远段 14. 左后侧支 14a. 左后侧支a 14b. 左后侧支b 15. 回旋支-后降支
二、各节段的权重因数
冠脉节段
右优势型冠脉ຫໍສະໝຸດ 左优势型冠脉1. 右冠状动脉近段 2. 右冠状动脉中段 3. 右冠状动脉远段 4. 右冠-后降支 16. 右冠-后侧支 16a. 右冠-后侧支第一分支 16b. 右冠-后侧支第二分支 16c. 右冠-后侧支第三分支
因此,SYNTAX试验中左主干和(或)三支病变 PCI治疗的患者,SYNTAX评分不仅是一种有用的 描述性工具,还可以预测一年的临床结果。 SYNTAX评分不是CABG组显著临床结果鉴别器; 这并不奇怪,因为外科发病率和死亡率取决于合 并症(如,伴或不伴COPD、肾损伤、卒中病史 等)而不是冠脉解剖结构本身。外科患者,风险 能够在包括联合发生率在内的评分系统中得到更 可靠的反映,如EuroSCORE评分和Parsonnet评 分。在《EuroIntervention》中,SYNTAX试验中 随机进行PCI患者的1年结果中,Serruys和他的 同事们证实了SYNTAX评分的价值以及再现性。
界定患者单支、双支、三支病变的局限性 是显而易见的,复杂病变或对手术的挑战 会根据伴或不伴解剖因素的病变,包括分 叉病变、慢性闭塞、迂曲血管、钙化、弥 漫性疾病等而改变,而作为高水平分层对 此没有任何帮助。
SYNTAX评分是一种血管造影工具,用于 对冠脉疾病复杂性进行分级。与以前的评 分系统不同,SYNTAX评分用于完整的冠 脉树,在SYNTAX试验中,在进行再次血 管重建手术之前,由心脏外科医生和介入 心脏病学家组成的心脏团队非正式的同意 计算SYNTAX评分。重要的是,SYNTAX 评分反映了冠脉解剖结构,而不是治疗策 略。
Gensini评分和SYNTAX评分--冠状动脉病变积分

Gensini评分和SYNTAX评分--冠状动脉病变积分冠脉病变的形态和狭窄的程度决定了治疗方案的选择,目前以Gensini评分和SYNTAX评分系统较为常用,两者侧重点不同,各有优缺点。
Gensini评分反映的是斑块的负荷情况,但没有涉及分叉、钙化和扭曲病变特征;SYNTAX评分反映的是斑块的类型及PCI的复杂程度,不仅能描述冠脉病变解剖结构,还可以在临床医生为高危患者制定最佳治疗方案时提供指导。
对于病变既适于PCI又适于CABG、且预期外科手术病死率低的患者,可用SYNTAX评分帮助制定治疗决策。
Gensini评分根据造影结果,对每支冠脉血管病变狭窄程度进行定量评定,狭窄程度以最严重处为标准,狭窄直径<25%计1分,25%≤直径<50%计2分,50%≤直径<75%计4分,75%≤直径<90%计8分,90%≤直径<99%计16分,≥99%计32分。
根据不同冠脉分支将以上得分乘以相应系数:左主干病变,得分x5;左前降支近段x2.5,中段得分x1.5,远段得分x1;第一对角支x1,第二对角支x0.5;左回旋支近段×2.5,远段和后降支均x1,后侧支×0.5;右冠近、中、远段和后降支均x1。
各病变支得分总和即为患者的冠状动脉病变狭窄程度总积分。
SYNTAX评分SYNTAX评分采用冠状动脉树16分段法,综合考虑冠状动脉的优势分型、病变部位、狭窄程度以及病变特征,对直径≥1.5mm的血管进行评分。
该评分系统共包括12个问题,内容包括优势分型、病变数、累及节段和病变特征(完全闭塞、三分叉、分叉、主动脉冠状动脉开口病变、严重扭曲、病变长度>20mm、严重钙化、血栓、弥漫/小血管病变),对每一病变进行评分后的总分值即为 SYNTAX积分。
冠状动脉树16分段法冠状动脉树16分段法各节段权重病变特征及加分SYNTAX评分系统中除根据优势分型、病变数和累及节段进行评分外,同时需考虑是否存在完全闭塞、三分叉、分叉、主动脉-开口病变、严重扭曲、病变长度>20mm、严重钙化、血栓、弥漫/小血管病变,如有则需根据病变特征进行相应的加分。
syntax评分

08年长城会上听专家讲了Syntax score评分方法,这评分方法比较复杂,主要是依据冠脉造影的结果来判断。
在准备阅读之前,先要熟悉冠脉解剖的节段分布情况:(上图为左优势型冠脉解剖分布,下图为右优势型解剖分布)Figure 1. Definition of the coronary tree segments(冠脉束血管段的识别)1. RCA proximal: From the ostium to one half the distance to the acute margin of the heart.2. RCA mid: From the end of first segment to acute margin of heart.3. RCA distal: From the acute margin of the heart to the origin of the posterior descending artery.4. Posterior descending artery: Running in the posterior interventricular groove.16. Posterolateral branch from RCA: Posterolateral branch originating from the distal coronary artery distal to the crux.16a. Posterolateral branch from RCA: First posterolateral branch from segment 16.16b. Posterolateral branch from RCA: Second posterolateral branch from segment 16.16c. Posterolateral branch from RCA: Third posterolateral branch from segment 16.5. Left main: From the ostium of the LCA through bifurcation into left anterior descending and left circumflex branches.6. LAD proximal: Proximal to and including first major septal branch.7. LAD mid: LAD immediately distal to origin of first septal branch and extending to the point where LAD forms an angle (RAO view). If thisangle is not identifiable this segment ends at one half the distance from the first septal to the apex of the heart.8. LAD apical: Terminal portion of LAD, beginning at the end of previous segment and extending to or beyond the apex.9. First diagonal: The first diagonal originating from segment 6 or 7.9a. First diagonal a: Additional first diagonal originating from segment 6 or 7, before segment 8.10. Second diagonal: Originating from segment 8 or the transition between segment 7 and 8. 10a. Second diagonal a: Additional second diagonal originating from segment 8.11. Proximal circumflex artery: Main stem of circumflex from its origin of left main and including origin of first obtuse marginal branch.12. Intermediate/anterolateral artery: Branch from trifurcating left main other than proximal LAD or LCX. It belongs to the circumflex territory.12a. Obtuse marginal a: First side branch of circumflex running in general to the area of obtuse margin of the heart.12b. Obtuse marginal b: Second additional branch of circumflex running in the same direction as 12.13. Distal circumflex artery: The stem of the circumflex distal to the origin of the most distal obtuse marginal branch, and running along the posteriorleft atrioventricular groove. Caliber may be small or artery absent.14. Left posterolateral: Running to the posterolateral surface of the left ventricle. May be absent or a division of obtuse marginal branch.14a. Left posterolateral a: Distal from 14 and running in the same direction.14b. Left posterolateral b: Distal from 14 and 14 a and running in the same direction.15. Posterior descending: Most distal part of dominant left circumflex when present. It gives origin to septal branches. When this arteryis present, segment 4 is usually absent。
冠脉病变SYNTAX评分值得收藏附图
冠状动脉病变SYNTAX 评分体系(附图)一、冠状动脉树注:1. 右冠状动脉近段11. 回旋支近段2. 右冠状动脉中段12. 中间支3. 右冠状动脉远段12a. 第一钝缘支4. 右冠-后降支12b. 第二钝缘支16. 右冠-后侧支13. 回旋支远段16a. 右冠-后侧支第一分支14. 左后侧支16b. 右冠-后侧支第二分支14a. 左后侧支a16c. 右冠-后侧支第三分支14b. 左后侧支b5. 左主干15. 回旋支-后降支6. 前降支近段7. 前降支中段8. 前降支心尖段9. 第一对角支9a. 第一对角支a10. 第二对角支10a. 第二对角支a二、各节段的权重因数冠脉节段右优势型冠脉左优势型冠脉1. 右冠状动脉近段 1 02. 右冠状动脉中段 1 03. 右冠状动脉远段 1 04. 右冠-后降支 1 /16. 右冠-后侧支0.5 /16a. 右冠-后侧支第一分支0.5 /16b. 右冠-后侧支第二分支0.5 /16c. 右冠-后侧支第三分支0.5 /5. 左主干 5 66. 前降支近段 3.5 3.57. 前降支中段 2.5 2.58. 前降支心尖段 1 19. 第一对角支 1 19a. 第一对角支a 1 110. 第二对角支0.5 0.510a. 第二对角支a 0.5 0.511. 回旋支近段 1.5 2.512. 中间支 1 112a. 第一钝缘支 1 112b. 第二钝缘支 1 113. 回旋支远段0.5 1.514. 左后侧支0.5 114a. 左后侧支a 0.5 114b. 左后侧支b 0.5 115. 回旋支-后降支/ 1三、病变不良特征评分血管狭窄-完全闭塞×5-50-99%狭窄×2完全闭塞-大于3个月或闭塞时间不祥+1-钝型残端+1-桥侧枝+1-闭塞后的第一可见节段+1/每一不可见节段-边支-边支小于1.5mm +1三叉病变-1个病变节段+3-2个病变节段+4-3个病变节段+5-4个病变节段+6分叉病变-A、B、C型病变+1-E、D、F、G型病变+2-角度小于70°+1开口病变+1严重扭曲+2长度大于20mm +1严重钙化+2血栓+1弥漫病变/小血管病变+1/每一节段四、SYNTAX评分系统SYNTAX积分通过计算机程序计算得出。
syntax评分
08年长城会上听专家讲了Syntax score评分方法,这评分方法比较复杂,主要是依据冠脉造影的结果来判断。
在准备阅读之前,先要熟悉冠脉解剖的节段分布情况:(上图为左优势型冠脉解剖分布,下图为右优势型解剖分布)Figure 1. Definition of the coronary tree segments(冠脉束血管段的识别)1. RCA proximal: From the ostium to one half the distance to the acute margin of the heart.2. RCA mid: From the end of first segment to acute margin of heart.3. RCA distal: From the acute margin of the heart to the origin of the posterior descending artery.4. Posterior descending artery: Running in the posterior interventricular groove.16. Posterolateral branch from RCA: Posterolateral branch originating from the distal coronary artery distal to the crux.16a. Posterolateral branch from RCA: First posterolateral branch from segment 16.16b. Posterolateral branch from RCA: Second posterolateral branch from segment 16.16c. Posterolateral branch from RCA: Third posterolateral branch from segment 16.5. Left main: From the ostium of the LCA through bifurcation into left anterior descending and left circumflex branches.6. LAD proximal: Proximal to and including first major septal branch.7. LAD mid: LAD immediately distal to origin of first septal branch and extending to the point where LAD forms an angle (RAO view). If thisangle is not identifiable this segment ends at one half the distance from the first septal to the apex of the heart.8. LAD apical: Terminal portion of LAD, beginning at the end of previous segment and extending to or beyond the apex.9. First diagonal: The first diagonal originating from segment 6 or 7.9a. First diagonal a: Additional first diagonal originating from segment 6 or 7, before segment 8.10. Second diagonal: Originating from segment 8 or the transition between segment 7 and 8. 10a. Second diagonal a: Additional second diagonal originating from segment 8.11. Proximal circumflex artery: Main stem of circumflex from its origin of left main and including origin of first obtuse marginal branch.12. Intermediate/anterolateral artery: Branch from trifurcating left main other than proximal LAD or LCX. It belongs to the circumflex territory.12a. Obtuse marginal a: First side branch of circumflex running in general to the area of obtuse margin of the heart.12b. Obtuse marginal b: Second additional branch of circumflex running in the same direction as 12.13. Distal circumflex artery: The stem of the circumflex distal to the origin of the most distal obtuse marginal branch, and running along the posteriorleft atrioventricular groove. Caliber may be small or artery absent.14. Left posterolateral: Running to the posterolateral surface of the left ventricle. May be absent or a division of obtuse marginal branch.14a. Left posterolateral a: Distal from 14 and running in the same direction.14b. Left posterolateral b: Distal from 14 and 14 a and running in the same direction.15. Posterior descending: Most distal part of dominant left circumflex when present. It gives origin to septal branches. When this arteryis present, segment 4 is usually absent。
冠脉病变SYNTAX评分,值得收藏(附图)
冠状动脉病变SYNTAX 评分体系(附图)一、冠状动脉树注:1. 右冠状动脉近段11. 回旋支近段2. 右冠状动脉中段12. 中间支3. 右冠状动脉远段12a. 第一钝缘支4. 右冠-后降支12b. 第二钝缘支16. 右冠-后侧支13. 回旋支远段16a. 右冠-后侧支第一分支14. 左后侧支16b. 右冠-后侧支第二分支14a. 左后侧支a16c. 右冠-后侧支第三分支14b. 左后侧支b5. 左主干15. 回旋支-后降支6. 前降支近段7. 前降支中段8. 前降支心尖段9. 第一对角支9a. 第一对角支a10. 第二对角支10a. 第二对角支a二、各节段的权重因数冠脉节段右优势型冠脉左优势型冠脉1. 右冠状动脉近段 1 02. 右冠状动脉中段 1 03. 右冠状动脉远段 1 04. 右冠-后降支 1 /16. 右冠-后侧支0.5 /16a. 右冠-后侧支第一分支0.5 /16b. 右冠-后侧支第二分支0.5 /16c. 右冠-后侧支第三分支0.5 /5. 左主干 5 66. 前降支近段 3.5 3.57. 前降支中段 2.5 2.58. 前降支心尖段 1 19. 第一对角支 1 19a. 第一对角支a 1 110. 第二对角支0.5 0.510a. 第二对角支a 0.5 0.511. 回旋支近段 1.5 2.512. 中间支 1 112a. 第一钝缘支 1 112b. 第二钝缘支 1 113. 回旋支远段0.5 1.514. 左后侧支0.5 114a. 左后侧支a 0.5 114b. 左后侧支b 0.5 115. 回旋支-后降支/ 1三、病变不良特征评分血管狭窄-完全闭塞×5-50-99%狭窄×2完全闭塞-大于3个月或闭塞时间不祥+1-钝型残端+1-桥侧枝+1-闭塞后的第一可见节段+1/每一不可见节段-边支-边支小于1.5mm +1三叉病变-1个病变节段+3-2个病变节段+4-3个病变节段+5-4个病变节段+6分叉病变-A、B、C型病变+1-E、D、F、G型病变+2-角度小于70°+1开口病变+1严重扭曲+2长度大于20mm +1严重钙化+2血栓+1弥漫病变/小血管病变+1/每一节段四、SYNTAX评分系统SYNTAX积分通过计算机程序计算得出。
冠脉病变SYN评分值得收藏附图

冠脉病变S Y N评分值得收藏附图集团公司文件内部编码:(TTT-UUTT-MMYB-URTTY-ITTLTY-冠状动脉病变SYNTAX评分体系(附图)一、冠状动脉树注:1.右冠状动脉近段11.回旋支近段2.右冠状动脉中段12.中间支3.右冠状动脉远段12a.第一钝缘支4.右冠-后降支12b.第二钝缘支16.右冠-后侧支13.回旋支远段16a.右冠-后侧支第一分支14.左后侧支16b.右冠-后侧支第二分支14a.左后侧支a 16c.右冠-后侧支第三分支14b.左后侧支b5.左主干15.回旋支-后降支6.前降支近段7.前降支中段8.前降支心尖段9.第一对角支9a.第一对角支a10.第二对角支10a.第二对角支a二、各节段的权重因数冠脉节段右优势型冠脉左优势型冠脉三、病变不良特征评分2.右冠状动脉中段103.右冠状动脉远段104.右冠-后降支1/16.右冠-后侧支0.5/16a.右冠-后侧支第一分支0.5/16b.右冠-后侧支第二分支0.5/16c.右冠-后侧支第三分支0.5/5.左主干566.前降支近段3.53.57.前降支中段2.52.58.前降支心尖段119.第一对角支119a.第一对角支a1110.第二对角支0.50.510a.第二对角支a0.50.511.回旋支近段1.52.512.中间支1112a.第一钝缘支1112b.第二钝缘支1113.回旋支远段0.51.514.左后侧支0.5114a.左后侧支a0.5114b.左后侧支b0.5115.回旋支-后降支/1血管狭窄-完全闭塞×5-50-99%狭窄×2完全闭塞-大于3个月或闭塞时间不祥+1-钝型残端+1-桥侧枝+1-闭塞后的第一可见节段+1/每一不可见节段-边支-边支小于1.5mm+1三叉病变-1个病变节段+3-2个病变节段+4-3个病变节段+5-4个病变节段+6分叉病变-A、B、C型病变+1-E、D、F、G型病变+2-角度小于70°+1开口病变+1严重扭曲+2长度大于20mm+1严重钙化+2血栓+1弥漫病变/小血管病变+1/每一节段四、SYNTAX评分系统SYNTAX积分通过计算机程序计算得出。
冠脉解剖及应用(Syntax评分)

冠状动脉解剖---右冠状动脉
窦房结动脉 圆锥支
右室支 左室后支
房室结动脉
锐缘支
后降支
冠状动脉解剖---左优势型与右优势型与 均衡性
• 右优势型( 85% ):RCA走行于右房室沟,到达后十字 交叉处,在后十字交叉或近后十字交叉处分出后降支后, 向左室隔面走行并发出1个或多个左室后支后终止。
• 左优势型( 8% ):即左回旋支优势,左回旋支粗大,除 发出钝缘支外,还发出左室后支和后降支,而RCA 细小 ,未达到后十字交叉处。
左室的血液供应
❖ 前间壁、前壁—LAD ❖ 前侧壁—LAD(对角支)和LCX(钝缘支) ❖ 后侧壁—LCX(RCA) ❖ 下壁—多为RCA(后降支),亦可为LCX,偶有部分来
源LAD
❖ 后壁—RCA(左室后侧支)和/或LCX ❖ 室间隔:前上2/3和心尖部—LAD,后下1/3—RCA
冠脉解剖总结---冠状动脉与心脏各 部分的供血关系
16c. Posterolateral branch from RCA: Third posterolateral branch from segment 16
左冠状动脉分段
5. Left main: From the ostium of the LCA through bifurcation into left anterior descending and left circumflex branches.
• 均衡型( 7% ): RCA到达后十字交叉处发出后降支, 左室后支则起源于左回旋支成为其终端分支,二者均不越 过后十字交叉。
冠状动脉解剖---左优势型与右优势型与 均衡性
冠状动脉解剖---右优势型
左室后支 支
后降支
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
冠状动脉病变SYNTAX 评分体系(附图)
令狐采学
一、冠状动脉树
注:
1. 右冠状动脉近段11. 回旋支近段
2. 右冠状动脉中段12. 中间支
3. 右冠状动脉远段12a. 第一钝缘支
4. 右冠-后降支12b. 第二钝缘支
16. 右冠-后侧支13. 回旋支远段
16a. 右冠-后侧支第一分支14. 左后侧支
16b. 右冠-后侧支第二分支14a. 左后侧支a
16c. 右冠-后侧支第三分支14b. 左后侧支b
5. 左主干15. 回旋
支-后降支
6. 前降支近段
7. 前降支中段
8. 前降支心尖段
9. 第一对角支
9a. 第一对角支a
10. 第二对角支
10a. 第二对角支a
二、各节段的权重因数
冠脉节段右优势型冠脉左优势型冠脉
1. 右冠状动脉近段 1 0
2. 右冠状动脉中段 1 0
3. 右冠状动脉远段 1 0
4. 右冠-后降支 1 /
16. 右冠-后侧支0.5 /
16a. 右冠-后侧支第一分支0.5 /
16b. 右冠-后侧支第二分支0.5 /
16c. 右冠-后侧支第三分支0.5 /
5. 左主干 5 6
6. 前降支近段 3.5 3.5
7. 前降支中段 2.5 2.5
8. 前降支心尖段 1 1
9. 第一对角支 1 1
9a. 第一对角支a 1 1
10. 第二对角支0.5 0.5
10a. 第二对角支a 0.5 0.5
11. 回旋支近段 1.5 2.5
12. 中间支 1 1
12a. 第一钝缘支 1 1
12b. 第二钝缘支 1 1
13. 回旋支远段0.5 1.5
14. 左后侧支0.5 1
14a. 左后侧支a 0.5 1
三、病变
不良特
征评分
血管狭窄
-完全闭塞 ×5
-50-99%狭窄 ×2
完全闭塞
-大于3个月或闭塞时间不祥 +1
-钝型残端 +1
-桥侧枝 +1
-闭塞后的第一可见节段 +1/每一不可见节段
-边支 -边支小于1.5mm +1
三叉病变
-1个病变节段 +3
-2个病变节段 +4
-3个病变节段 +5
-4个病变节段 +6
分叉病变
-A 、B 、C 型病变 +1
-E 、D 、F 、G 型病变 +2
-角度小于70° +1
开口病变 +1
严重扭曲 +2
长度大于20mm +1
严重钙化 +2
血栓 +1
弥漫病变/小血管病变 +1/每一节段
四、SYNTAX 评分系统
14b. 左后侧支b 0.5 1
15. 回旋支-后降支 / 1
SYNTAX积分通过计算机程序计算得出。
运算法则包含12个问题。
前3个问题为冠脉优势型、病变数以及病变的血管节段数。
最多的病变数为12个,每个病变被冠以1、2、3……依此类推。
每个病变可能累及1或多个节段。
通过累及的节段将计算出每个病变的积分。
后9个问题为病变的不良特征,根据不良特征得出每个病变的积分。
每个病变积分相加得出SYNTAX积分。
1.冠脉优势型
2.病变数目
3.病变的节段数
病变特征
4.完全闭塞
i.节段数
ii.闭塞时间(大于3个月)
iii.钝型残端
iv.桥侧枝
v.闭塞以远节段数
vi.边支
5.三分叉病变
i.节段数
6.分叉病变
i.分叉类型
ii.成角(小于70度)
7.开口病变
8.严重扭曲
9.长度大于20mm
10.严重钙化
11.血栓
12.弥漫病变/小血管病变
定义:
1.冠脉优势型:a)右优势型:后降支由右冠发出(第四节段)
b):左优势型:后降支由左冠发出(第四节段)。
在SYNTAX 评分中无均衡型冠脉的选择。
2.完全闭塞:TIMI血流0级。
3.桥侧枝:平行血管的连接近远端的小通道
4.三分叉病变:三根血管交汇一起,一根主支和2根边支。
只
有下述分支才定义为三分叉病变:3/4/16/16a、5/6/11/12、11/12a/12b/13、6/7/9/9a 和7/8/10/10a。
5.双分叉病变:一根主支和一根大于1.5mm的边支交汇一起的
病变。
只有下述分支才定义为双分叉病变:5/6/11、6/7/9、7/8/10、11/13/12a、13/14/14a、3/4/16 和13/14/15。
6.发自主动脉的开口病变:指第1或第5节段,如左冠双开口,
则第6和第11节段也属于开口病变。
7.大于20mm的长病变:狭窄大于50%病变的长度,分叉病变
中至少有一支病变大于20mm。
8.严重钙化:至少一个投照体位见围绕整个管腔的钙化病变。
9.血栓:多投照体位狭窄处或远端血栓或下游的可见栓塞。
10.弥漫病变/小血管病变:大于75%长度的血管直径小于2mm。
注1:多个前后病变
如果多个前后病变的距离小于3个参考血管的直径,可以把它们作为一个病变看待来记分。
如果每个病变的距离大于3个参考血管直径,应作为独立病变。
注2:完全闭塞病变
闭塞病变的长度通过闭塞点和侧枝可见的第一个血管节段来计算。
如下图所示:
注3:分叉病变分型
边支血管直径至少1.5mm以上才构成分叉病变。
采用Duke分型法(如下图)。
举例1:
举例2:。