骨科英文书籍精读(42)|骨折晚期并发症之肌肉挛缩
臀肌挛缩症

功能锻炼
• 术后48小时,走一字步:挺胸抬头双肩水 平,双下肢交叉直线行走。3次/天,30分钟 /次。 • 术后3~4天,在走一字步的基础上逐步增 加紧臀外展并膝下蹲练习:双脚并拢,双 手平举,足跟不能离地,腰背部挺直。3次/ 天,重复运动200次。
功能锻炼
• 术后第7天,在纠正异常 步态的基础上,进行腿部 锻炼(翘二郎腿,踢毽子), 翘腿时端坐于靠背椅上, 背部紧贴靠背,一腿过膝, 交叉架于另一腿上,左右 腿交叉,进行左右摆臀主 动伸展运动。3次/天,30 度和强度,必须循序渐进, 逐渐加大,既要防止运动幅度过大,造成 软组织损伤,影响伤口愈合,又要防止怕 痛苦,训练方法不正确,造成软组织粘连 影响疗效。总之坚持科学,有效长期的康 复训练,才能彻底改变患者不良的姿势和 步态,使患者康复。
健康教育
• 任何注射用药物都有刺激性,但由于药物分子结 构及分子团大小不同,对人体组织的刺激程度也 各异。 • 对儿童应尽量避免臀肌注射,尤其避免用苯甲醇 做溶媒的药物注射。 • 确实需要肌肉注射的,疗程以5天为宜。对注射部 位用热毛巾外敷,每日2次,每次10分钟。 • 对一些较多地接受肌肉注射的患儿,在每一注射 疗程结束后,应给予适当的理疗,改善局部组织 的血液循环,加速肌肉功能的恢复,同时进行髋 关节的内收、内旋及屈曲运动锻炼。
术后护理
• 潜在并发症护理: 术后用绷带或其他约束 带绷拢双膝使双下肢成内收位, 并用软枕垫 高双下肢, 使髋关节、膝关节呈屈曲位, 既 利于臀肌的松弛也可减轻疼痛。术后仰卧 4h 后更换体位。双侧臀肌挛缩症患者仰卧 与俯卧交替, 预防骶尾部压疮的发生。指导 在床上练习起坐,防止切断的挛缩束接触, 粘连。
护理问题
• 局部血肿:与术中止血 不彻底、术后引流欠佳 有关 。 • 护理目标:避免血肿发 生或发生后及时处理。 • 护理措施:保持引流的 通畅,做好管路护理。
骨科英文书籍精读(90)|桡骨头骨折

骨科英文书籍精读(90)|桡骨头骨折FRACTURED HEAD OF RADIUSRadial head fractures are common in adults but are hardly ever seen in children (probably because the proximal radius is mainly cartilaginous) whereas radial neck fractures occur in children more frequently.Mechanism of injuryA fall on the outstretched hand with the elbow extended and the forearm pronated causes impaction of the radial head against the capitulum. The radial head may be split or broken. In addition, the articular cartilage of the capitulum may be bruised or chipped; this cannot be seen on x-ray but is an important complication. The radial head is also sometimes fractured during elbow dislocation.Clinical featuresThis fracture is sometimes missed, but tenderness on pressure over the radial head and pain on pronation and supination should suggest the diagnosis.X-rayThree types of fracture are identified and classified by Mason as:Type I An undisplaced vertical split in the radial headType II A displaced single fragment of the headType III The head broken into several fragments (comminuted).An additional Type IV has been proposed, for those fractures with an associated elbow dislocation.Special radial head views, rather than simple PA and lateralviews are needed to fully assess the fracture. The wrist also should be x-rayed to exclude a concomitant injury of the distal radioulnar joint, which would signify damage to the interosseous membrane (acute longitudinal radioulnar dissociation).TreatmentAn undisplaced split (Type I)Worthwhile pain relief can be achieved by aspirating the haematoma and injecting local anaesthetic. The arm is held in a collar and cuff for 3 weeks; active flexion, extension and rotation are encouraged. The prognosis for this injury is very good, although there is often some loss of elbow extension.A single large fragment (Type II)If the fragment is displaced, it should be reduced and held with one or two small headless screws.A comminuted fracture (Type III)This is a challenging injury. Always assess for an associated soft tissue injury:Rupture of the medial collateral ligament;Rupture of the interosseous membrane (Essex Lopresti lesion);Combined fractures of the radial head and coronoid process plus dislocation of the elbow – the ‘terrible triad’.If any of these is present, excision of the radial head is contra-indicated; this may lead to intractible instability of the elbow or forearm. The head must be meticulously reconstructed with small headless screws or replaced with a metal spacer. A medial collateral rupture, if unstable after replacing or fixing the radial head, should be repaired.Radial head excision usually gives a good long-term result if there are no contraindications; however, wrist pain from ulnarhead impaction, valgus instability of the elbow and trochleo-olecranon arthritis can develop.ComplicationsJoint stiffness is common and may involve both the elbow and the radioulnar joints. Even with minimally displaced fractures the elbow can take several months to recover, and stiffness may occur whether the radial head has been excised or not.Myositis ossificans is an occasional complication. Recurrent instability of the elbow can occur if the medial collateral ligament was also injured and the radial head excised.---from 《Apley’s System of Orthopaedics and Fractures》重点词汇整理:outstretched /ˌaʊtˈstretʃt/adj. 伸开的;扩张的v. 伸出;扩大;伸展得超出…的范围(outstretch的过去分词形式)pronate /'pronet/vt. 旋前;将手掌向下或向后转动vi. 俯身;伏身capitulum /kə'pɪtʃʊləm/n.桡骨小头[组织][生物] 小头,骨端;[植] 头状花序supination /,sju:pi'neiʃən/n. 旋后;反掌姿势concomitant /kənˈkɑːmɪtənt/n. 伴随物adj. 相伴的;共存的;附随的the distal radioulnar joint桡尺远侧关节 /,reidiəu'ʌlnə/adj. 桡尺骨的the interosseous membrane骨间膜membrane /ˈmembreɪn/n. 膜;薄膜;羊皮纸longitudinal /ˌlɑːndʒəˈtuːdnl/adj. 长度的,纵向的;经线的dissociation /dɪˌsoʊsiˈeɪʃn,dɪˌsoʊʃiˈeɪʃn/n. 分解,分离;分裂aspirate/'æspərət/n. 送气音;抽出物adj. 送气音的vt. 送气发音;吸入haematoma /,hi:mə'təumə, ,hem-/n. [病理] 血肿local anaesthetic局部麻醉/ˌænəsˈθetɪk/n. 麻醉剂;麻药adj. 麻醉的prognosis /prɑːɡˈnoʊsɪs/n. [医] 预后;预知Rupture of the medial collateral ligament; 内侧副韧带断裂;collateral /kəˈlætərəl/adj. 附属的;旁系的;并行的n. 抵押品,担保品;旁系亲属coronoid process[解剖] 冠突;[解剖] 喙突 /'kɔrənɔid/adj. 冠状的;喙状的contraindications /ˌkɑːntrəˌɪndɪˈkeɪʃn/n. [医] 禁忌症;禁忌征候valgus/'vælɡəs/n. 外翻足的人;外翻足adj. 外翻的trochleo-olecranon arthritis 滑车鹰嘴关节炎Myositis/,maiəu'saitis/n. [外科]骨化性肌炎;肌炎,肌肉发炎百度翻译:桡骨头骨折桡骨头骨折在成人中很常见,但在儿童中很少见(可能是因为桡骨近端主要是软骨),而桡骨颈骨折在儿童中更常见。
骨科学 英语

骨科学 英语Ankle: Achilles Tendonitis 跟腱炎Ankle: Ruptured Achilles Tendon 跟腱破裂Ankle: Sprain 踝部扭伤Ankle Fracture 踝部骨折Ankylosing Spondylitis 关节黏连脊椎炎Aseptic Necrosis 无菌的骨疽Back Pain: Approach to Management 怎样处理背痛问题Back Pain: Prevention 预防背痛Baker's Cyst 贝勾氏囊Bones 骨骼的功能Bone Tumors 骨肿瘤Bunions 姆趾黏液囊肿大Carpal tunnel syndrome 腕管综合症Colles Fracture 桡骨下端骨折Compression Fracture of the Vertebrae 脊椎压迫性骨折Dislocation 脱臼Dupuytren Contracture 掌挛缩病Elbow: Golfer's Elbow 高尔夫球肘Elbow: Tennis Elbow 网球肘Fibromyalgia 纤维组织肌痛Flat Foot 扁平足Foot: Hammer Toe 锤状趾Foot: Plantar Fasciitis 足底筋膜炎Foot: Ulcers 脚溃疡Fracture 骨折Fracture: Bones in the Foot 脚部骨折Fracture: Clavicle 锁骨骨折Fracture Types 骨折的种类Frozen Shoulder 凝肩Ganglion 腱鞘囊肿Hand Fracture 手骨折Hand: Tenosynoritis 手部腱鞘滑膜炎Heel Spurs 脚跟骨刺和发炎Herniated Disk 椎间盆后凸。
外科学 第五篇 骨外科(翻译版)
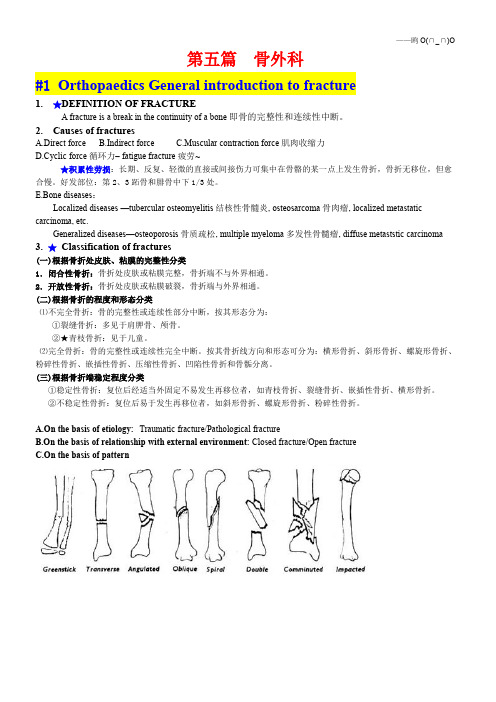
第五篇骨外科#1Orthopaedics General introduction to fracture1.★DEFINITION OF FRACTUREA fracture is a break in the continuity of a bone即骨的完整性和连续性中断。
2.Causes of fracturesA.Direct forceB.Indirect forceC.Muscular contraction force肌肉收缩力D.Cyclic force循环力–fatigue fracture疲劳~★积累性劳损:长期、反复、轻微的直接或间接伤力可集中在骨骼的某一点上发生骨折,骨折无移位,但愈合慢。
好发部位:第2、3跖骨和腓骨中下1/3处。
E.Bone diseases:Localized diseases—tubercular osteomyelitis结核性骨髓炎,osteosarcoma骨肉瘤,localized metastatic carcinoma,etc.Generalized diseases—osteoporosis骨质疏松,multiple myeloma多发性骨髓瘤,diffuse metaststic carcinoma3.★Classification of fractures(一)根据骨折处皮肤、粘膜的完整性分类1.闭合性骨折:骨折处皮肤或粘膜完整,骨折端不与外界相通。
2.开放性骨折:骨折处皮肤或粘膜破裂,骨折端与外界相通。
(二)根据骨折的程度和形态分类⑴不完全骨折:骨的完整性或连续性部分中断,按其形态分为:①裂缝骨折:多见于肩胛骨、颅骨。
②★青枝骨折:见于儿童。
⑵完全骨折:骨的完整性或连续性完全中断。
按其骨折线方向和形态可分为:横形骨折、斜形骨折、螺旋形骨折、粉碎性骨折、嵌插性骨折、压缩性骨折、凹陷性骨折和骨骺分离。
(三)根据骨折端稳定程度分类①稳定性骨折:复位后经适当外固定不易发生再移位者,如青枝骨折、裂缝骨折、嵌插性骨折、横形骨折。
骨科英文书籍精读(93)|肘关节脱位(2)

Medial epicondyledegrees; after 3 weeks movements are begun under supervision.Head of radiusThe combination of ligament disruption and a type II or III radial head fracture is an unstable injury; stability is restored only by healing or repair of the ligaments and restoration of the radial pillar – either by fracture fixation or (in the case of a comminuted fracture) by prosthetic replacement of the radial head. The medial collateral ligament may also be repaired to protect the radial head fixation or implant from undue valgus stress.Olecranon processIn the rare forward dislocation of the elbow, the olecranon process may fracture; a large piece of the olecranon is left behind as a separatefragment. Open reduction with internal fixation is the best treatment.Side-swipe injuriesThese severe fracture-dislocations are often associated with damage to the large vessels of the arm. The priorities are repair of any vascular injury, skeletal stabilization and soft tissue coverage. This is demanding surgery, necessitating a high level of expertise, and is best undertaken in a unit specialising in upper limb injuries.Persistent instabilityIn cases where the elbow remains unstable after the bone and joint anatomy has been restored, a hinged external fixator can be applied inorder to maintain mobility while the tissues heal.---from 《Apley’s System of Orthopaedics and Fractures》重点词汇整理:trochlear groove.滑车沟。
骨科英文书籍精读(371)|踝部骨折(2)

骨科英文书籍精读(371)|踝部骨折(2)我们正在精读国外经典骨科书籍《Apley’s System of Orthopaedics and Fractures》,想要对于骨科英文形成系统认识,为以后无障碍阅读英文文献打下基础,请持续关注。
中国十大名师之一赖世雄老师说过,学习英语没有捷径,少就是多,快就是慢。
不要以量取胜,把一个音标、一个单词、一段对话、一篇文章彻底搞透,慢慢积累,你会发现,你并不比每天走马观花的输入大量英文学的差。
Clinical featuresAnkle fractures are seen in skiers, footballers and climbers; an older group includes women with postmenopausal osteoporosis.A history of a severe twisting injury, followed by intense pain and inability to stand on the leg suggests something more serious than a simple sprain. The ankle is swollen and deformity may be obvious. The site of tenderness is important; if both the medial and lateral sides are tender, a double injury (bony or ligamentous) must be suspected.X-rayAt least three views are needed: anteroposterior, lateral and a 30-degree oblique 'mortise’ view. The level of the fibular fracture is often best seen in the lateral view; diastasis may not be appreciated without the mortise view. Further x-rays may be needed to exclude a proximal fibular fracture.From a careful study of the x-rays it should be possible to reconstruct the mechanism of injury. The four most common patterns are shown in Figure 31.5.TreatmentSwelling is usually rapid and severe, particularly in the higher energy injuries. If the injury is not dealt with within a few hours, definitive treatment may have to be deferred for several days while the leg is elevated so that the swelling can subside; this can be hastened by using a foot pump (which also reduces the risk of deep-vein thrombosis).Fractures are visible on x-ray; ligaments are not.Always look for clues to the invisible ligament injury –widening of the tibiofibular space, asymmetry of the talotibial space, widening of the medial joint space, or tilting of the talus –before deciding on a course of action.Like other intra-articular injuries, ankle fractures must be accurately reduced and held if later mechanical dysfunction is to be prevented. Persistent displacement of the talus, or a step in the articular surface, leads to increased stress and predisposes tosecondary osteoarthritis.In assessing the accuracy of reduction, four objectives must be met: (1) the fibula must be restored to its full length; (2) the talus must sit squarely in the mortise, with the talar and tibial articular surfaces parallel; (3) the medial joint space must be restored to its normal width, i.e. the same width as the tibio-talar space (about 4 mm); (4) oblique x-rays must show that there is no tibiofibular diastasis.Ankle fractures are often unstable. Whatever the method of reduction and fixation, the position must be checked by x-ray during the period of healing.---from 《Apley’s System of Orthopaedics and Fractures》postmenopausal osteoporosis绝经后骨质疏松症suspect /səˈspekt/v. 怀疑;猜想n. 嫌疑犯adj. 靠不住的;可疑的diastasis may not be appreciated without the mortise view. 如果没有踝穴视图,可能无法鉴别分离。
volkmann挛缩名词解释

volkmann挛缩名词解释
Volkmann挛缩是一种医学术语,用于描述肌肉在过度收缩时出现的症状。
这种情况通常发生在肌肉受到长时间持续性压迫或血液供应不足的情况下。
当肌肉受到压迫或血液供应不足时,通常会出现肌肉疼痛、僵硬和功能障碍的症状。
这可能是由于肌肉纤维内的代谢产物积累、缺氧、营养不良或神经损伤引起的。
其中,Volkmann挛缩是一种严重的肌肉病理状态,可以导致肌肉的坏死和功能损伤。
Volkmann挛缩主要发生在四肢肌肉,尤其是在手和腕部。
常见的引起Volkmann挛缩的原因包括骨折、关节脱位、肌肉损伤和动脉闭塞等。
当这些情况发生时,肌肉会过度收缩,导致血管收缩,进一步加重肌肉组织的损伤。
早期识别和干预是防止Volkmann挛缩并减少其严重程度的关键。
如果患者出现严重的疼痛、肿胀和功能障碍,应及时就医进行全面评估。
治疗方法通常包括解除压力、恢复正常血液供应、物理治疗以及必要时手术干预。
总之,Volkmann挛缩是一种由肌肉过度收缩引起的病理状态,常见于肌肉受到压迫或血液供应不足的情况下。
及早识别和干预是预防和治疗Volkmann挛缩的关键。
如果出现相关症状,应及时就医以获取专业的医疗建议和治疗。
Volkmann挛缩
• 拇内收肌筋膜间室综合征的检查方法: 牵引拇指使其处于外展位,藉此紧张拇 内收肌,根据有无症状做出判断。大鱼 际肌很少发生筋膜间室综合征。
• 筋膜间室测压,尤其是第一骨间背侧肌、 大鱼际肌及小鱼际肌筋膜间室的压力测 定对诊断有意义。 筋膜间室内压力增高 使筋膜间室综合征的诊断得到证实。 • Whitesides,Mubarak和Matsen等用不同 的方法测定筋膜间室内压力。
• 疼痛是最常见的症状,但在昏迷病人不 能发现。被动牵拉手指加重疼痛,前臂 因肿胀而出现紧张和触痛,指尖灵敏度 降低或消失。 • 两点辨别试验可用来帮助判断神经缺血 情况, Gelbernan等曾报道九例压力超 过30mmHg的筋膜间室综合征,这九位 清醒病人中有四例病人正中神经的两点 辨别距离超过1cm。
前臂及手部筋膜室间隔综合征 及缺血性肌肉挛缩的治疗
苏州大学附属第一医院 骨科 杨同其
一、历史回顾 • 1881年 , Volkmann在他的经典著作中首 先报道了麻痹性挛缩,他发现在动脉供 血不足或肌肉缺血后几个小时之内即可 发生此症。他认为绷带包扎过紧是产生 供血不足的原因,这种认为外在压力是 麻痹性挛缩主要原因的观点在英文文献 中持续了相当 一段时间。
• 切口从肱二 头肌肌膜内 侧开始,斜 行跨过肘横 纹,向远侧 直达手掌, 以便打开腕 管,注意切 口与腕横纹 勿成直角。
• 分开变性的肌纤维束,清除血肿。怀疑 有肱动脉损伤时,显露并探查有无活动 性出血。如果血流不畅,打开血管外膜, 观察膜下有无血凝块、痉挛或内膜撕裂。 必要时切除血管外膜并行血管吻合或动 脉移植。
• 继续向远端解剖,注意保护正中神经。 松解旋前圆肌的起点,用手术刀或锋利 的骨膜起子在骨膜下松解指深屈肌的起 点。然后松解旋前圆肌的远侧起点、掌 长肌和桡侧腕屈肌的起点。之后,游离 指浅屈肌的起点,暴露肘关节囊。松解 尺侧腕屈肌的远侧起点,勿损伤尺神经。 显露骨间膜,反复屈伸手 指,以帮助确 定起点的哪些部位需做进一步分离。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
骨科英文书籍精读(42)|骨折晚期并发症之肌肉挛缩
MUSCLE CONTRACTURE
Following arterial injury or compartment syndrome, the patient may develop ischaemic contractures of the affected muscles (Volkmann’s ischaemic contracture). Nerves injured by ischaemia sometimes recover, at least partially; thus the patient presents with deformity and stiffness, but numbness is inconstant. The sites most commonly affected are the forearm and hand, leg and foot.
In a severe case affecting the forearm, there will be wasting of the forearm and hand, and clawing of the fingers. If the wrist is passively flexed, the patient can extend the fingers, showing that the deformity is largely due to contracture of the forearm muscles. Detachment of the flexors at their origin and along the interosseous membrane in the forearm may improve the deformity, but function is no better if sensation and active movement are not restored. A pedicle nerve graft, using the proximal segments of the median and ulnar nerves may restore protective sensation in the hand, and tendon transfers (wrist extensors to finger and thumb flexors) will allow active grasp. In less severe cases, median nerve sensibility may be quite good and, with appropriate tendon releases and transfers, the patient regains a considerable degree of function.
Ischaemia of the hand may follow forearm injuries, or swelling of the fingers associated with a tight forearm bandage or plaster. The intrinsic hand muscles fibrose and shorten, pulling the fingers into flexion at the metacarpophalangeal joints, but the interphalangeal joints remain straight. The thumb is
adducted across the palm (Bunnell’s ‘intrinsic-plus’ position).
Ischaemia of the calf muscles may follow injuries or operations involving the popliteal artery or its divisions. This is more common than is usually supposed. The symptoms, signs and subsequent contracture are similar to those following ischaemia of the forearm. One of the causes of late claw-toe deformity is an undiagnosed compartment syndrome.
---from 《Apley’s System of Orthopaedics and Fractures》P721
重点词汇整理:
muscle contracture肌肉挛缩
inconstant /ɪnˈkɑːnstənt/adj. 变化无常的;易变的;多变的
clawing of the fingers 爪形手
passively flexed被动弯曲,
interosseous membrane 前臂骨间膜
/,intər'ɔsiəs/adj. 骨间的;小腿骨间的;前臂骨间的
/ˈmembreɪn/n. 膜;薄膜
active movement主动活动
restored/ri'stɔ:d/v. 修复(restore的过去式);恢复健康adj. 精力充沛的;精力恢复的
pedicle nerve graft,椎弓根神经移植
grasp /ɡræsp/v. 抓牢,握紧;试图抓住;理解,领悟;毫不犹豫地抓住(机会)n. 抓,握;理解,领会;力所能及,把握;权力,控制
regain/rɪˈɡeɪn/n. 收复;取回vt. 恢复;重新获得;收回vi. 上涨intrinsic hand muscles手内在肌
fibrose形成纤维性组织
metacarpophalangeal joints掌指关节
interphalangeal joints指间关节
adduct /'ædʌkt/n. [化学] 加合物vt. 使内收
calf muscles腓肠肌群;小腿后肌
/kæf/n. [解剖] 腓肠,小腿;小牛;小牛皮
popliteal artery 腘动脉
/pɔp'litiəl, ,pɔpli'ti-/adj. 腘的,腿弯部的
This is more common than is usually supposed. The symptoms, signs and subsequent contracture are similar to those following ischaemia of the forearm.这种情况比人们通常想象的更为常见。
症状、体征和随后的挛缩类似于那些随之而来的前臂缺血。
百度翻译:
肌肉挛缩
动脉损伤或室间隔综合征后,患者可能出现受影响肌肉的缺血挛缩(沃尔克曼缺血挛缩)。
因缺血而受伤的神经有时会恢复,至少部分恢复;因此病人会出现畸形和僵硬,但麻木是不稳定的。
最常受影响的部位是前臂和手、腿和脚。
在严重影响前臂的情况下,前臂和手会消瘦,手指会被抓。
如果手腕被动弯曲,患者可以伸出手指,说明畸形主要是由于前臂肌肉挛缩所致。
屈肌在其起点和前臂骨间膜的分离可以改善畸形,但如果感觉和主动运动不恢复,功能就不好。
利用正中神经和尺神经近端节段的带蒂神经移植可以恢复手部的保护性感觉,肌腱转移(手腕伸肌到手指和拇指屈肌)将允许主动抓握。
在不太严重的情况下,正中神经的敏感性可能相当好,适当的肌腱松解和转移,患者可以恢复相当程度的功能。
手部缺血可能是前臂损伤,或手指肿胀与前臂绷带或石膏绷带紧密相关。
手的固有肌肉纤维化并变短,手指在掌指关节处弯曲,但指间关节保持笔直。
拇指在手掌上内收(邦内尔的“内在加”位置)。
小腿肌肉的缺血可能发生在损伤或涉及腘动脉或其分支的手术之后。
这比通常想象的要普遍。
症状、体征和随后的挛缩与前臂缺血后
的症状相似。
晚期爪趾畸形的原因之一是未确诊的筋膜室综合征。