List of herbs with side effects and contraindications (updated on 25_April_2011)
2.奥美拉唑碳酸氢钠胶囊和混悬剂Zegerid-FDA说明书
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use ZEGERID safely and effectively. See full prescribing information for ZEGERID.ZEGERID (omeprazole/sodium bicarbonate) Powder for Oral Suspension ZEGERID (omeprazole/sodium bicarbonate) CapsulesInitial U.S. Approval: 2004----------------------------RECENT MAJOR CHANGES-------------------------Warnings and Precautions, 11/2012 Clostridium difjicile associated diarrhea (5.4)Warnings and Precautions, 11/2012 Interaction with clopidogrel (5.5)Warnings and Precautions, 11/2012 Concomitant Use of ZEGERID with St. John’s Wort or Rifampin (5.8) Warnings and Precautions,Interactions with Diagnostic 11/2012 Investigations for Neuroendocrine Tumors (5.9)Warnings and Precautions, 04/2012 Concomitant Use of Zegerid with Methotrexate (5.10)------------------------INDICATIONS AND USAGE-------------------ZEGERID is a proton pump inhibitor indicated for:• Short-term treatment of active duodenal ulcer (1.1)• Short-term treatment of active benign gastric ulcer (1.2)• Treatment of gastroesophageal reflux disease (GERD) (1.3)• Maintenance of healing of erosive esophagitis (1.4)• Reduction of risk of upper GI bleeding in critically ill patients (1.5) The safety and effectiveness of ZEGERID in pediatric patients (<18 years of age) have not been established. (8.4)----------------------DOSAGE AND ADMINISTRATION----------------------• Short-Term Treatment of Active DuodenalUlcer: 20 mg oncedaily for 4 weeks (some patients may requirean additional 4 weeks of therapy (14.1)) (2)• Gastric Ulcer: 40 mg once daily for 4-8 weeks (2)• Gastroesophageal Reflux Disease (GERD) (2)-Symptomatic GERD (with no esophageal erosions): 20 mg once daily for up to 4 weeks-Erosive Esophagitis: 20 mg once daily for 4-8 weeks• Maintenance of Healing of Erosive Esophagitis: 20 mg once daily (2) • Reduction of Risk of Upper Gastrointestinal Bleeding in Critically Ill Patients: (40mg oral suspension only) 40 mg initially followed by 40 mg 6-8 hours later and 40 mg daily thereafter for 14 days (2)---------------------DOSAGE FORMS AND STRENGTHS---------------------• ZEGERID is available as a capsule and as a powder for oral suspension in 20 mg and 40 mg strengths (3)-------------------------------CONTRAINDICATIONS----------------------------• Known hypersensitivity to any components of the formulation (4)-----------------------WARNINGS AND PRECAUTIONS-----------------------• Concomitant Gastric Malignancy: Symptomatic response to therapy with ZEGERID does not preclude the presence of gastric malignancy(5.1)• Atrophic Gastritis: Has been observed in gastric corpus biopsies from patients treated long-term with omeprazole (5.2) • Buffer Content: contains sodium bicarbonate (5.3)• PPI therapy may be associated with increased risk of Clostridium difficile associated diarrhea. (5.4)• Avoid concomitant use of Zegerid with clopidogrel (5.5)• Bone Fracture: Long-term and multiple daily dose PPI therapy may be associated with an increased risk for osteoporosis-related fractures ofthe hip, wrist, or spine. (5.6)• Hypomagnesemia has been reported rarely with prolonged treatment with PPIs (5.7)• Avoid concomitant use of Zegerid with St John’s Wort or rifampin due to the potential reduction in omeprazole concentrations (5.8, 7.2)• Interactions with diagnostic investigations for Neuroendocrine Tumors: Increases in intragastric pH may result in hypergastrinemia andenterochromaffin-like cell hyperplasia and increased Choromogranin A levels which may interfere with diagnostic investigations forneuroendocrine tumors. (5.9, 12.2)------------------------------ADVERSE REACTIONS------------------------------Most common adverse reactions (incidence ≥ 2%) are:Headache, abdominal pain, nausea, diarrhea, vomiting, and flatulence (6)To report SUSPECTED ADVERSE REACTIONS, contact Santarus Ienc. at 1-888-778-0887 or FDA at 1-800-FDA-1088 or/medwatch.------------------------------DRUG INTERACTIONS------------------------------• Drugs for which gastric pH can affect bioavailability (e.g., ketoconazole, ampicillin esters, iron salts, and digoxin): ZEGERID may interfere with absorption due to inhibition of gastric acid secretion (7.1) • Drugs metabolized by cytochrome P450 (e.g., diazepam, warfarin, phenytoin, cyclosporine, disulfiram, benzodiazepines): ZEGERID can prolong their elimination. Monitor to determine the need for possibledose adjustments when taken with ZEGERID (7.2)• Patients treated with proton pump inhibitors and warfarin concomitantly may need to be monitored for increases in INR and prothrombin time(7.2)• Voriconazole: May increase plasma levels of omeprazole (7.2)• Saquinavir: ZEGERID increases plasma levels of saquinavir (7.3)• ZEGERID may reduce plasma levels of atazanavir and nelfinavir (7.3) • Clopidogrel: Zegerid decreases exposure to the active metabolite of clopidogrel (7.5)• Tacrolimus: ZEGERID may increase serum levels of tacrolimus (7.6) • Methotrexate: Zegerid may increase serum level of methotrexate (7.8) -----------------------USE IN SPECIFIC POPULATIONS----------------------• Pregnancy: Based upon animal data, may cause fetal harm (8.1)• The safety and effectiveness of ZEGERID in pediatric patients less than18 years of age have not been established. (8.4)• Hepatic Impairment: Consider dose reduction, particularly for maintenance of healing of erosive esophagitis (12.3)See 17 for PATIENT COUNSELING INFORMATION and Medication GuideRevised: 11/2012__________________________________________________________________________________________________________________________________FULL PRESCRIBING INFORMATION: CONTENTS*1 INDICATIONS AND USAGE1.1 Duodenal Ulcer1.2 Gastric Ulcer1.3 Treatment of Gastroesophageal Reflux Disease (GERD)1.4 Maintenance of Healing of Erosive Esophagitis1.5 Reduction of Risk of Upper Gastrointestinal Bleeding in CriticallyIll Patients (40mg suspension only)2 DOSAGE AND ADMINISTRATION3 DOSAGE FORMS AND STRENGTHS4 CONTRAINDICATIONS5 WARNINGS AND PRECAUTIONS5.1 Concomitant Gastric Malignancy5.2 Atrophic Gastritis5.3 Buffer Content5.4 Clostridium Difficile associated diarrhea5.5 Interaction with clopidogrel5.6 Bone Fracture5.7 Hypomagnesemia5.8 Concomitant use of ZEGERID with St John’s Wort or rifampin5.9 Interactions with Investigations for Neuroendocrine Tumors5.10 Concomitant use Zegerid with Methotrexate6 ADVERSE REACTIONS6.1 Clinical Trials Experience6.2 Postmarketing Experience7 DRUG INTERACTIONS7.1 Drugs for which gastric pH can affect bioavailability7.2 Drugs metabolized by cytochrome P450 (CYP)7.3 Antiretroviral Agents7.4 Combination Therapy with Clarithromycin7.5 Clopidogrel7.6 Tacrolimus7.7 Interactions With Investigations of Neuroendocrine Tumors7.8 Methotrexate8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.3 Nursing Mothers8.4 Pediatric Use8.5 Geriatric Use8.6 Hepatic Impairment8.7 Renal Impairment8.8 Asian Population10 OVERDOSAGE11 DESCRIPTION12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.2 Pharmacodynamics12.3 Pharmacokinetics13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility13.2 Animal Toxicology and/or Pharmacology14 CLINICAL STUDIES14.1 Duodenal Ulcer Disease14.2 Gastric Ulcer14.3 Gastroesophageal Reflux Disease GERD14.4 Long Term Maintenance Treatment of Erosive Esophagitis14.5 Reduction of Risk of Upper Gastrointestinal Bleeding in Critically Ill Patients15 REFERENCES16 HOW SUPPLIED/STORAGE AND HANDLING17 PATIENT COUNSELING INFORMATION* Sections or subsections omitted from the full prescribing information are not listed.__________________________________________________________________________________________________________________________________FULL PRESCRIBING INFORMATION:1 INDICATIONS AND USAGE1.1 Duodenal UlcerZEGERID (omeprazole/sodium bicarbonate) is indicated for short-term treatment of active duodenal ulcer. Most patients heal within four weeks. Some patients may require an additional four weeks of therapy. [See Clinical Studies (14.1)]1.2 Gastric UlcerZEGERID is indicated for short-term treatment (4-8 weeks) of active benign gastric ulcer. [See Clinical Studies (14.2)]1.3 Treatment of Gastroesophageal Reflux Disease (GERD) Symptomatic GERDZEGERID is indicated for the treatment of heartburn and other symptoms associated with GERD. [See Clinical Studies (14.3)]Erosive EsophagitisZEGERID is indicated for the short-term treatment (4-8 weeks) of erosive esophagitis which has been diagnosed by endoscopy.The efficacy of ZEGERID used for longer than 8 weeks in these patients has not been established. If a patient does not respond to 8 weeks of treatment, it may be helpful to give up to an additional 4 weeks of treatment. If there is recurrence of erosive esophagitis or GERD symptoms (e.g., heartburn), additional 4-8 week courses of ZEGERID may be considered. [See Clinical Studies (14.3)]1.4 Maintenance of Healing of Erosive EsophagitisZEGERID is indicated to maintain healing of erosive esophagitis. Controlled studies do not extend beyond 12 months. [See Clinical Studies (14.4)]1.5 Reduction of Risk of Upper Gastrointestinal Bleeding in CriticallyIll Patients (40mg oral suspension only)ZEGERID Powder for Oral Suspension 40 mg/1680 mg is indicated for the reduction of risk of upper GI bleeding in critically ill patients. [See CLINICAL STUDIES, Reduction of Risk of Upper Gastrointestinal Bleeding in Critically Ill Patients (14.5)]2 DOSAGE AND ADMINISTRATIONZEGERID (omeprazole/sodium bicarbonate) is available as a capsule and as a powder for oral suspension in 20 mg and 40 mg strengths of omeprazole for adult use. Directions for use for each indication are summarized in Table 1. All recommended doses throughout the labeling are based upon omeprazole Since both the 20 mg and 40 mg oral suspension packets contain the same amount of sodium bicarbonate (1680 mg), two packets of 20 mg are not equivalent to one packet of ZEGERID 40 mg; therefore, two 20 mg packets of ZEGERID should not be substituted for one packet of ZEGERID 40 mg. Since both the 20 mg and 40 mg capsules contain the same amount of sodium bicarbonate (1100 mg), two capsules of 20 mg are not equivalent to one capsule of ZEGERID 40 mg; therefore, two 20 mg capsules of ZEGERID should not be substituted for one capsule of ZEGERID 40 mg.ZEGERID should be taken on an empty stomach at least one hour before a meal.For patients receiving continuous Nasogastric (NG)/ Orogastric (OG) tube feeding, enteral feeding should be suspended approximately 3 hours before and 1 hour after administration of ZEGERID Powder for Oral Suspension.Table 1: Recommended Doses of ZEGERID by Indication for Adults18 Years and OlderRecommendedIndication FrequencyDoseShort-Term Treatment of20 mg Once daily for 4 weeks*,+ Active Duodenal UlcerOnce daily for 4-8 Benign Gastric Ulcer 40 mgweeks **,+Gastroesophageal RefluxDisease (GERD)Symptomatic GERD (with Once daily for up to 420 mgno esophageal erosions) weeks+Erosive Esophagitis 20 mg Once daily for 4-8 weeks+Maintenance of Healing of20 mg Once daily** Erosive EsophagitisReduction of Risk of Upper 40 mg initially followed byGastrointestinal Bleeding in 40 mg 6-8 hours later and40 mgCritically Ill Patients 40 mg daily thereafter for (40 mg oral suspension only) 14 days*** Most patients heal within 4 weeks. Some patients may require an additional 4 weeks of therapy. [See Clinical Studies (14.1)]** For additional information, [See Clinical Studies (14)]+ For additional information, [See Indications and Usage (1)]Special PopulationsHepatic InsufficiencyConsider dose reduction, particularly for maintenance of healing of erosive esophagitis. [See Clinical Pharmacology (12.3)]Administration of CapsulesZEGERID Capsules should be swallowed intact with water. DO NOT USE OTHER LIQUIDS. DO NOT OPEN CAPSULE AND SPRINKLE CONTENTS INTO FOOD.Preparation and Administration of SuspensionDirections for use: Empty packet contents into a small cup containing 1-2 tablespoons of water. DO NOT USE OTHER LIQUIDS OR FOODS. Stir well and drink immediately. Refill cup with water and drink.If ZEGERID is to be administered through a nasogastric (NG) or orogastric (OG) tube, the suspension should be constituted with approximately 20 mL of water. DO NOT USE OTHER LIQUIDS OR FOODS. Stir well and administer immediately. An appropriately-sized syringe should be used to instill the suspension in the tube. The suspension should be washed through the tube with 20 mL of water.3 DOSAGE FORMS AND STRENGTHSZEGERID 20-mg Capsules: Each opaque, hard gelatin, white capsule, imprinted with the Santarus logo and “20”, contains 20 mg omeprazole and 1100 mg sodium bicarbonate.ZEGERID 40-mg Capsules: Each opaque, hard gelatin, colored dark blue and white capsule, imprinted with the Santarus logo and “40”, contains 40 mg omeprazole and 1100 mg sodium bicarbonate.ZEGERID Powder for Oral Suspension is a white, flavored powder packaged in unit-dose packets. Each packet contains either 20 mg or 40 mg omeprazole and 1680 mg sodium bicarbonate.4 CONTRAINDICATIONSZEGERID is contraindicated in patients with known hypersensitivity to any components of the formulation. Hypersensitivity reactions may include anaphylaxis, anaphylactic shock, angioedema, bronchospasm, interstitial nephritis, and urticaria.5 WARNINGS AND PRECAUTIONS 5.1 Concomitant Gastric Malignancy Symptomatic response to therapy with omeprazole does not preclude the presence of gastric malignancy. 5.2 Atrophic gastritis Atrophic gastritis has been noted occasionally in gastric corpus biopsies from patients treated long-term with omeprazole. 5.3 Buffer Content 5.4 Clostridium difficile associated diarrhea Published observational studies suggest that PPI therapy like Zegerid may beassociated with an increased risk of Clostridium difficile associated diarrhea, especially in hospitalized patients. This diagnosis should be considered fordiarrhea that does not improve. [See Adverse Reactions (6.2)] Patients should use the lowest dose and shortest duration of PPI therapyappropriate to the condition being treated. 5.5Interaction with clopidogrel Avoid concomitant use of Zegerid with clopidogrel. Clopidogrel is a prodrug.Inhibition of platelet aggregation by clopidogrel is entirely due to an active metabolite. The metabolism of clopidogrel to its active metabolite can be impaired by use with concomitant medications, such as omeprazole, that interfere with CYP2C19 activity. Concomitant use of clopidogrel with 80 mg omeprazole reduces the pharmacological activity of clopidogrel, even when administered 12 hours apart. When using Zegerid, consider alternative anti-platelet therapy [see Drug Interactions (7.5) and Pharmacokinetics (12.3)]. 5.6 Bone Fracture Several published observational studies suggest that proton pump inhibitor (PPI) therapy may be associated with an increased risk for osteoporosis-related fractures of the hip, wrist, or spine. The risk of fracture was increased in patients who received high-dose, defined as multiple daily doses, and long-term PPI therapy (a year or longer). Patients should use the lowest dose and shortest duration of PPI therapy appropriate to the condition being treated. Patients at risk for osteoporosis-related fractures should be managed according to the established treatment guidelines. [See Dosage and Administration (2) and Adverse Reactions (6.2)] 5.7 Hypomagnesemia Hypomagnesemia, symptomatic and asymptomatic, has been reported rarely in patients treated with PPIs for at least three months, in most cases after a year of therapy. Serious adverse events include tetany, arrhythmias, and seizures. In most patients, treatment of hypomagnesemia required magnesium replacement and discontinuation of the PPI. For patients expected to be on prolonged treatment or who take PPIs with medications such as digoxin or drugs that may cause hypomagnesemia (e.g., diuretics), health care professionals may consider monitoring magnesium levels prior to initiation of PPI treatment and periodically. [See Adverse Reactions (6.2)] 5.8 Concomitant use of Zegerid with St John’s Wort or rifampin Drugs which induce CYP2C19 OR CYP34A (such as St John’s Wort or rifampin) can substantially decrease omeprazole concentrations. [See Drug Interactions (7.2)]. Avoid concomitant use of ZEGERD with St John’s Wort or rifampin. 5.9 Interactions with Investigations for Neuroendocrine Tumors Serum chromogranin A (CgA) levels increase secondary to drug-induced decreases in gastric acidity. The increased CgA level may cause false positive results in diagnostic investigations for neuroendocrine tumors. Providers should temporarily stop omeprazole treatment before assessing CgA levels and consider repeating the test if initial CgA levels are high. If serial tests are performed (e.g. for monitoring), the same commercial laboratory should be used for testing, as reference ranges between tests may vary . [SeePharmacodynamics (12.2)]5.10Concomitant use of Zegerid with Methotrexate Literature suggests that concomitant use of PPIs with methotrexate (primarily at high dose; see methotrexate prescribing information) may elevate and prolong serum levels of methotrexate and/or its metabolite, possibly leading to methotrexate toxicities. In high-dose methotrexate administration, a temporary withdrawal of the PPI may be considered in some patients. [See Drug Interactions (7.7) 6 ADVERSE REACTIONS 6.1 Clinical Trials Experience Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice. In the U.S. clinical trial population of 465 patients, the adverse reactions summarized in Table 2 were reported to occur in 1% or more of patients on therapy with omeprazole. Numbers in parentheses indicate percentages of the adverse reactions considered by investigators as possibly, probably or definitely related to the drug. Table 2: Adverse Reactions Occurring In 1% or More of Patients on Omeprazole Therapy Omeprazole Placebo Ranitidine (n = 465) (n = 64) (n = 195) Omeprazole Placebo (n = 2631) (n = 120) Body as a Whole, site unspecified Abdominal pain 5.2 3.3 Asthenia 1.3 0.8 Digestive System Constipation 1.5 0.8 Diarrhea 3.7 2.5 Flatulence 2.7 5.8 Nausea 4.0 6.7 Vomiting 3.2 10.0 Acid regurgitation 1.9 3.3 Nervous System/Psychiatric Headache 2.9 2.5 Headache 6.9 (2.4) 6.3 7.7 (2.6) Diarrhea 3.0 (1.9) 3.1 (1.6) 2.1 (0.5) Abdominal Pain 2.4 (0.4) 3.1 2.1 Nausea 2.2 (0.9) 3.1 4.1 (0.5) URI 1.9 1.6 2.6 Dizziness 1.5 (0.6) 0.0 2.6 (1.0) Vomiting 1.5 (0.4) 4.7 1.5 (0.5) Rash 1.5 (1.1) 0.0 0.0 Constipation 1.1 (0.9) 0.0 0.0 Cough 1.1 0.0 1.5 Asthenia 1.1 (0.2) 1.6 (1.6) 1.5 (1.0) Back Pain 1.1 0.0 0.5 Table 3 summarizes the adverse reactions that occurred in 1% or more of omeprazole-treated patients from international double-blind, and open-label clinical trials in which 2,631 patients and subjects received omeprazole. Table 3: Incidence of Adverse Reactions ≥ 1% Causal Relationship not AssessedA controlled clinical trial was conducted in 359 critically ill patients, comparing ZEGERID 40 mg/1680 mg suspension once daily to I.V. cimetidine 1200 mg/day for up to 14 days. The incidence and total number of AEs experienced by ≥ 3% of patients in either group are presented in Table 4by body system and preferred term.Table 4: Number (%) of Critically Ill Patients withFrequently Occurring (≥ 3%) Adverse Events by BodySystem and Preferred Term(N=178) (N=181) MedDRABody System All AEs All AEs Preferred Term n (%) n (%) BLOOD AND LYMPHATIC SYSTEMDISORDERSAnemia NOS 14 (7.9) 14 (7.7) Anemia NOS Aggravated 4 (2.2) 7 (3.9) Thrombocytopenia 18 (10.1) 11 (6.1)Atrial Fibrillation 11 (6.2) 7 (3.9) Bradycardia NOS 7 (3.9) 5 (2.8) Supraventricular Tachycardia 6 (3.4) 2 (1.1) Tachycardia NOS 6 (3.4) 6 (3.3) Ventricular Tachycardia 8 (4.5) 6 (3.3) GASTROINTESTINAL DISORDERS *Constipation 8 (4.5) 8 (4.4) Diarrhea NOS 7 (3.9) 15 (8.3) Gastric Hypomotility 3 (1.7) 6 (3.3)ADMINISTRATION SITE CONDITIONSHyperpyrexia 8 (4.5) 3 (1.7) Edema NOS 5 (2.8) 11 (6.1) Pyrexia 36 (20.2) 29 (16.0) INFECTIONS AND INFESTATIONSCandidal Infection NOS 3 (1.7) 7 (3.9) Oral Candidiasis 7 (3.9) 1 (0.6) Sepsis NOS 9 (5.1) 9 (5.0) Urinary Tract Infection NOS 4 (2.2) 6 (3.3) INVESTIGATIONSLiver Function Tests NOS Abnormal 3 (1.7) 6 (3.3) METABOLISM AND NUTRITIONDISORDERSFluid Overload 9 (5.1) 14 (7.7) Hyperglycaemia NOS 19 (10.7) 21 (11.6) Hyperkalaemia 4 (2.2) 6 (3.3) Hypernatraemia 3 (1.7) 9 (5.0) Hypocalcaemia 11 (6.2) 10 (5.5) Hypoglycaemia NOS 6 (3.4) 8 (4.4) Hypokalaemia 22 (12.4) 24 (13.3) Hypomagnesaemia 18 (10.1) 18 (9.9) Hyponatraemia 7 (3.9) 5 (2.8) Hypophosphataemia 11 (6.2) 7 (3.9) PSYCHIATRIC DISORDERSAgitation 6 (3.4) 16 (8.8) RESPIRATORY, THORACIC ANDMEDIASTINAL DISORDERSAcute Respiratory Distress Syndrome 6 (3.4) 7 (3.9) Nosocomial Pneumonia 20 (11.2) 17 (9.4) Pneumothorax NOS 1 (0.6) 8 (4.4) Respiratory Failure 3 (1.7) 6 (3.3) SKIN AND SUBCUTANEOUS TISSUEDISORDERSDecubitus Ulcer 6 (3.4) 5 (2.8) Rash NOS 10 (5.6) 11 (6.1) VASCULAR DISORDERSHypertension NOS 14 (7.9) 6 (3.3) Hypotension NOS 17 (9.6) 12 (6.6) * Clinically significant upper gastrointestinal bleeding was considered a serious adverse event but it is not included in this table.NOS = Not otherwise specified.6.2 Postmarketing ExperienceThe following adverse reactions have been identified during post-approval use of omeprazole. Because these reactions are voluntarily reported from a population of uncertain size, it is not always possible to reliably estimate their Body as a Whole: Hypersensitivity reactions, including anaphylaxis, anaphylactic shock, angioedema, bronchospasm, interstitial nephritis, urticaria (see also Skin below), fever, pain, fatigue, malaise. Cardiovascular: Chest pain or angina, tachycardia, bradycardia, palpitation, elevated blood pressure, and peripheral edema.Gastrointestinal: Pancreatitis (some fatal), anorexia, irritable colon, flatulence, fecal discoloration, esophageal candidiasis, mucosal atrophy of the tongue, dry mouth, stomatitis and abdominal swelling. During treatment with omeprazole, gastric fundic gland polyps have been noted rarely. These polyps are benign and appear to be reversible when treatment is discontinued. Gastroduodenal carcinoids have been reported in patients with Zollinger-Ellison syndrome on long-term treatment with omeprazole. This finding is believed to be a manifestation of the underlying condition, which is known to be associated with such tumors.Hepatic: Mild and, rarely, marked elevations of liver function tests [ALT (SGPT), AST (SGOT), γ-glutamyl transpeptidase, alkaline phosphatase, and bilirubin (jaundice)]. In rare instances, overt liver disease has occurred, including hepatocellular, cholestatic, or mixed hepatitis, liver necrosis (some fatal), hepatic failure (some fatal), and hepatic encephalopathy.Infections and Infestations: Clostridium difficile associated diarrhea. Metabolism and Nutritional Disorders: Hyponatremia, hypoglycemia, hypomagnesemia, and weight gain.Musculoskeletal: Muscle cramps, myalgia, muscle weakness, joint pain, bone fracture, and leg pain.Nervous System/Psychiatric: Psychic disturbances including depression, agitation, aggression, hallucinations, confusion, insomnia, nervousness, tremors, apathy, somnolence, anxiety, dream abnormalities; vertigo; paresthesia; and hemifacial dysesthesia.Respiratory: Epistaxis, pharyngeal pain.Skin: Severe generalized skin reactions including toxic epidermal necrolysis (TEN; some fatal), Stevens-Johnson syndrome, and erythema multiforme (some severe); purpura and/or petechiae (some with rechallenge); skin inflammation, urticaria, angioedema, pruritus, photosensitivity, alopecia, dry skin, and hyperhidrosis.Special Senses: Tinnitus, taste perversion.Ocular: Blurred vision, ocular irritation, dry eye syndrome, optic atrophy, anterior ischemic optic neuropathy, optic neuritis and double vision. Urogenital: Interstitial nephritis (some with positive rechallenge), urinary tract infection, microscopic pyuria, urinary frequency, elevated serum creatinine, proteinuria, hematuria, glycosuria, testicular pain, and gynecomastia.Hematologic: Rare instances of pancytopenia, agranulocytosis (some fatal), thrombocytopenia, neutropenia, leukopenia, anemia, leucocytosis, and hemolytic anemia have been reported.The incidence of clinical adverse experiences in patients greater than 65 years of age was similar to that in patients 65 years of age or less.Additional adverse reactions that could be caused by sodium bicarbonate include metabolic alkalosis, seizures, and tetany.7 DRUG INTERACTIONS7.1 Drugs for which gastric pH can affect bioavailabilityBecause of its inhibition of gastric acid secretion, it is theoretically possible that omeprazole may interfere with absorption of drugs where gastric pH is an important determinant of their bioavailability (e.g., ketoconazole, ampicillin esters, iron salts, and digoxin). In the clinical efficacy trials, antacids were used concomitantly with the administration of omeprazole.7.2 Drugs metabolized by cytochrome P450 (CYP)Omeprazole can prolong the elimination of diazepam, warfarin and phenytoin, drugs that are metabolized by oxidation in the liver. There have been reports of increased INR and prothrombin time in patients receiving proton pump inhibitors, including omeprazole, and warfarin concomitantly. Increases in INR and prothrombin time may lead to abnormal bleeding and even death. Patients treated with proton pump inhibitors and warfarin may need to be monitored for increases in INR and prothrombin time.Although in normal subjects no interaction with theophylline or propranololmetabolized via the cytochrome P-450 system (e.g., cyclosporine, disulfiram,benzodiazepines). Patients should be monitored to determine if it is necessaryto adjust the dosage of these drugs when taken concomitantly withZEGERID.omeprazole exposure. Dose adjustment of omeprazole is not normallyrequired.. When voriconazole (400 mg every 12 hours for one day, then 200mg for 6 days) was given with omeprazole (40 mg once daily for 7 days) tohealthy subjects, it significantly increased the steady-state Cmax and AUC024 of omeprazole, an average of 2 times (90% CI: 1.8, 2.6) and 4 times (90%CI: 3.3, 4.4) respectively as compared to when omeprazole was given withoutvoriconazole.subjects, St John’s wort (300 mg three times daily for 14 days), an inducer ofCYP3A4, decreased the systemic exposure of omeprazole in CYP2C19 poormetabolisers (Cmax and AUC decreased by 37.5% and 37.9%, respectively)and extensive metabolisers (Cmax and AUC decreased by 49.6% and 43.9%,respectively). Avoid concomitant use of St. John’s Wort or rifampin withomeprazole.Concomitant administration of atazanavir and proton pump inhibitors is notrecommended. Co-administration of atazanavir with proton pump inhibitorsis expected to substantially decrease atazanavir plasma concentrations andthereby reduce its therapeutic effect.Omeprazole has been reported to interact with some antiretroviral drugs. Theclinical importance and the mechanisms behind these interactions are notalways known. Increased gastric pH during omeprazole treatment maychange the absorption of the antiretroviral drug. Other possible interactionmechanisms are via CYP2C19. For some antiretroviral drugs, such asatazanavir and nelfinavir, decreased serum levels have been reported whengiven together with omeprazole. Following multiple doses of nelfinavir (1250mg, twice daily) and omeprazole (40 mg, daily), AUC was decreased by 36%and 92%, Cmax by 37% and 89% and Cmin by 39% and 75% respectivelyfor nelfinavir and M8. Following multiple doses of atazanavir (400 mg, daily)and omeprazole (40 mg, daily, 2 hours before atazanavir), AUC wasdecreased by 94%, Cmax by 96%, and Cmin by 95%. Concomitantadministration with omeprazole and drugs such as atazanavir and nelfinavir istherefore not recommended.Increased concentration of saquinavirFor other antiretroviral drugs, such as saquinavir, elevated serum levels havebeen reported with an increase in AUC by 82%, in Cmax by 75% and inCmin by 106% following multiple dosing of saquinavir/ritonavir (1000/100mg) twice daily for 15 days with omeprazole 40 mg daily co-administereddays 11 to 15. Dose reduction of saquinavir should be considered from thesafety perspective for individual patients. There are also some antiretroviraldrugs of which unchanged serum levels have been reported when given withomeprazole.Concomitant administration of clarithromycin with other drugs can lead toserious adverse reactions due to drug interaction [See Warnings andPrecautions in prescribing information for clarithromycin]. Because of thesedrug interactions, clarithromycin is contraindicated for co-administration withcertain drugs [See Contraindication in prescribing information forclarithromycin].Omeprazole is an inhibitor of CYP2C19 enzyme. Clopidogrel is metabolizedto its active metabolite in part by CYP2C19. Concomitant use of omeprazole80 mg results in reduced plasma concentrations of the active metabolite ofclopidogrel and a reduction in platelet inhibition. Avoid concomitantadministration of Zegerid with clopidogrel. When using Zegerid, consider useof alternative anti-platelet therapy [see Pharmacokinetics (12.3)].Concomitant administration of omeprazole and tacrolimus may increase theserum levels of tacrolimus.Drug-induced decrease in gastric acidity results in enterochromaffin-like cellhyperplasia and increased Chromogranin A levels which may interfere withinvestigations for neuroendocrine tumors. [see Clinical Pharmacology (12)].Case reports, published population pharmacokinetic studies, and retrospectiveanalyses suggest that concomitant administration of PPIs and methotrexate(primarily at high dose; see methotrexate prescribing information) mayelevate and prolong serum levels of methotrexate and/or its metabolitehydroxymethotrexate. However, no formal drug interaction studies ofmethotrexate with PPIs have been conducted. [see Warnings and Precautions(5.10)].8 USE IN SPECIFIC POPULATIONS8.1 PregnancyPregnancy Category CThere are no adequate and well-controlled studies on the use of omeprazole inpregnant women. The vast majority of reported experience with omeprazoleduring human pregnancy is first trimester exposure and the duration of use israrely specified, eg, intermittent versus chronic. An expert review ofpublished data on experiences with omeprazole use during pregnancy byTERIS – the Teratogen Information System – concluded that therapeuticdoses during pregnancy are unlikely to pose a substantial teratogenic risk (thequantity and quality of data were assessed as fair).1Three epidemiological studies compared the frequency of congenitalabnormalities among infants born to women who used omeprazole duringpregnancy to the frequency of abnormalities among infants of womenexposed to H2-receptor antagonists or other controls. A population-basedprospective cohort epidemiological study from the Swedish Medical BirthRegistry, covering approximately 99% of pregnancies, reported on 955infants (824 exposed during the first trimester with 39 of these exposedbeyond first trimester, and 131 exposed after the first trimester) whosemothers used omeprazole during pregnancy.2 In utero exposure to omeprazolewas not associated with increased risk of any malformation (odds ratio 0.82,95% CI 0.50-1.34), low birth weight or low Apgar score. The number ofinfants born with ventricular septal defects and the number of stillborn infantswas slightly higher in the omeprazole exposed infants than the expectednumber in the normal population. The author concluded that both effects maybe random.A retrospective cohort study reported on 689 pregnant women exposed toeither H2-blockers or omeprazole in the first trimester (134 exposed toomeprazole).3 The overall malformation rate was 4.4% (95% CI 3.6-5.3) andthe malformation rate for first trimester exposure to omeprazole was 3.6%(95% CI 1.5-8.1). The relative risk of malformations associated with firsttrimester exposure to omeprazole compared with nonexposed women was 0.9(95% CI 0.3-2.2). The study could effectively rule out a relative risk greaterthan 2.5 for all malformations. Rates of preterm delivery or growthretardation did not differ between the groups.A controlled prospective observational study followed 113 women exposed toomeprazole during pregnancy (89% first trimester exposures).4 The reportedrates of major congenital malformations was 4% for the omeprazole group,2% for controls exposed to nonteratogens, and 2.8% in disease-pairedcontrols (background incidence of major malformations 1-5%). Rates ofspontaneous and elective abortions, preterm deliveries, gestational age atdelivery, and mean birth weight did not differ between the groups. Thesample size in this study has 80% power to detect a 5-fold increase in the rateof major malformation.Several studies have reported no apparent adverse short term effects on theinfant when single dose oral or intravenous omeprazole was administered toover 200 pregnant women as premedication for cesarean section undergeneral anesthesia.Reproduction studies conducted with omeprazole in rats at oral doses up to 28times the human dose of 40 mg/day (based on body surface area) and inrabbits at doses up to 28 times the human dose (based on body surface area)did not show any evidence of teratogenicity. In pregnant rabbits, omeprazoleat doses about 2.8 to 28 times the human dose of 40 mg/day, (based on bodysurface area) produced dose-related increases in embryo-lethality, fetalresorptions, and pregnancy loss. In rats treated with omeprazole at dosesabout 2.8 to 28 times the human dose (based on body surface area), dose-related embryo/fetal toxicity and postnatal developmental toxicity occurred inoffspring. [See Animal Toxicology and/or Pharmacology (13.2)].There are no adequate and well-controlled studies in pregnant women.。
中药调剂操作流程及注意事项

中药调剂操作流程及注意事项1.患者取号接待。
The patient takes a number and is received.2.接待人员核对患者信息。
The receptionist verifies patient information.3.核对患者处方并向患者确认。
Verify the patient's prescription and confirm with the patient.4.阅读处方,了解病情和用药情况。
Read the prescription and understand the condition and medication.5.检查处方的药品和用量。
Check the medication and dosage on the prescription.6.向药房提供正确的处方信息。
Provide the correct prescription information to the pharmacy.7.药师核对处方信息。
The pharmacist verifies the prescription information.8.药师准备药材和药物。
The pharmacist prepares herbal medicine and drugs.9.将药材和药物分装制成剂量。
Divide the herbal medicine and drugs into doses.10.核对分装的剂量和药名。
Check the divided doses and drug names.11.患者取药。
The patient takes the medicine.12.给患者讲解用药的注意事项。
Explain the precautions for medication to the patient.13.确认患者了解用药情况。
Confirm that the patient understands the medication.14.记录患者的取药信息。
Gadoterate Meglumine注射液产品说明说明书
MEDICATION GUIDEGadoterate Meglumine (GAD oh TER ate MEG loo meen) Injection(gadoterate meglumine)Injection for intravenous useWhat is Gadoterate Meglumine Injection?•Gadoterate Meglumine Injection is a prescription medicine called a gadolinium-based contrast agent (GBCA). Gadoterate Meglumine Injection, like other GBCAs, is injected into your vein and used with a magnetic resonance imaging (MRI) scanner.•An MRI exam with a GBCA, including Gadoterate Meglumine Injection, helps your doctor to see problems better than an MRI exam without a GBCA.•Your doctor has reviewed your medical records and has determined that you would benefit from using a GBCA with your MRI exam.What is the most important information I should know about Gadoterate Meglumine Injection?•Gadoterate Meglumine Injection contains a metal called gadolinium. Small amounts of gadolinium can stay in your body including the brain, bones, skin and other parts of your body for a long time (several months to years).•It is not known how gadolinium may affect you, but so far, studies have not found harmful effects in patients with normal kidneys.•Rarely patients have reported pains, tiredness, and skin, muscle or bone ailments for a long time, but these symptoms have not been directly linked to gadolinium.•There are different GBCAs that can be used for your MRI exam. The amount of gadolinium that stays in the body is different for different gadolinium medicines. Gadolinium stays in the body more after Omniscan or Optimark than after Eovist, Magnevist or MultiHance. Gadolinium stays in the body the least after Gadoterate Meglumine Injection, Gadavist orProHance.•People who get many doses of gadolinium medicines, women who are pregnant and young children may be at increased risk from gadolinium staying in the body.•Some people with kidney problems who get gadolinium medicines can develop a condition with severe thickening of the skin, muscles and other organs in the body (nephrogenic systemic fibrosis). Your healthcare provider should screen you to see how well your kidneys are working before you receive Gadoterate Meglumine Injection.Do not receive Gadoterate Meglumine Injection if you have had a severe allergic reaction to Gadoterate Meglumine Injection.Before receiving Gadoterate Meglumine Injection, tell your healthcare provider about all your medical conditions, including if you:•have had any MRI procedures in the past where you received a GBCA. Your healthcare provider may ask you for more information including the dates of these MRI procedures.•are pregnant or plan to become pregnant. It is not known if Gadoterate Meglumine Injection can harm your unborn baby. Talk to your healthcare provider about the possible risks to an unborn baby if a GBCA such as Gadoterate Meglumine Injection is received during pregnancy.•have kidney problems, diabetes, or high blood pressure.•have had an allergic reaction to dyes (contrast agents) including GBCAs.What are possible side effects of Gadoterate Meglumine Injection?•See “What is the most important information I should know about Gadoterate Meglumine Injection?”•Allergic reactions. Gadoterate Meglumine Injection can cause allergic reactions that can sometimes be serious. Your healthcare provider will monitor you closely for symptoms of an allergic reaction.The most common side effects of Gadoterate Meglumine Injection include: nausea, headache, pain, or cold feeling at the injection site, and rash.These are not all the possible side effects of Gadoterate Meglumine Injection.Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.General information about the safe and effective uses of Gadoterate Meglumine Injection.Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. You can ask your healthcare provider for information about Gadoterate Meglumine Injection that is written for health professionals.What are the ingredients in Gadoterate Meglumine Injection?Active ingredient: gadoterate meglumineInactive ingredients: DOTA, water for injectionManufactured for: Fresenius Kabi USA, LLCFor more information, call 1-800-551-7176.This Medication Guide has been approved by the U.S. Food and Drug Administration.451747 24UG01 Rev. 04/2022。
阿奇霉素FDAlabel
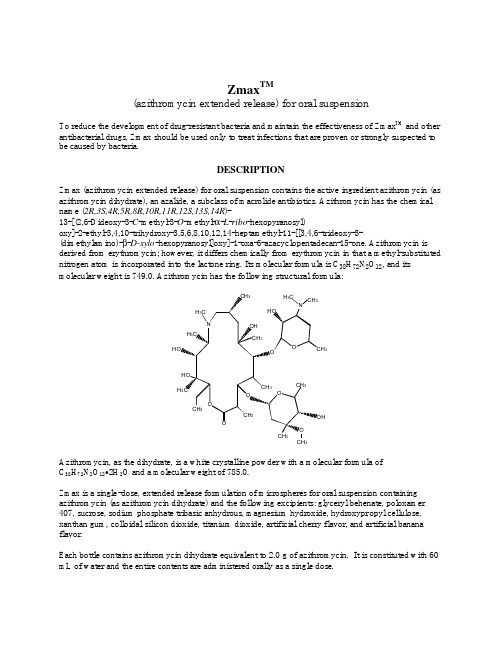
Zmax TM(azithromycin extended release) for oral suspensionTo reduce the development of drug-resistant bacteria and maintain the effectiveness of Zmax TM and other antibacterial drugs, Zmax should be used only to treat infections that are proven or strongly suspected to be caused by bacteria.DESCRIPTIONZmax (azithromycin extended release) for oral suspension contains the active ingredient azithromycin (as azithromycin dihydrate), an azalide, a subclass of macrolide antibiotics. Azithromycin has the chemical name (2R,3S,4R,5R,8R,10R,11R,12S,13S,14R)-13-[(2,6-Dideoxy-3-C-methyl-3-O-methyl-α-L-ribo-hexopyranosyl)oxy]-2-ethyl-3,4,10-trihydroxy-3,5,6,8,10,12,14-heptamethyl-11-[[3,4,6-trideoxy-3- (dimethylamino)-β-D-xylo-hexopyranosyl]oxy]-1-oxa-6-azacyclopentadecan-15-one. Azithromycin is derived from erythromycin; however, it differs chemically from erythromycin in that a methyl-substituted nitrogen atom is incorporated into the lactone ring. Its molecular formula is C38H72N2O12, and its molecular weight is 749.0. Azithromycin has the following structural formula:33Azithromycin, as the dihydrate, is a white crystalline powder with a molecular formula ofC38H72N2O12•2H2O and a molecular weight of 785.0.Zmax is a single-dose, extended release formulation of microspheres for oral suspension containing azithromycin (as azithromycin dihydrate) and the following excipients: glyceryl behenate, poloxamer 407, sucrose, sodium phosphate tribasic anhydrous, magnesium hydroxide, hydroxypropyl cellulose, xanthan gum, colloidal silicon dioxide, titanium dioxide, artificial cherry flavor, and artificial banana flavor.Each bottle contains azithromycin dihydrate equivalent to 2.0 g of azithromycin. It is constituted with 60 mL of water and the entire contents are administered orally as a single dose.CLINICAL PHARMACOLOGYPharmacokineticsZmax is an extended release microsphere formulation. Based on data obtained from studies evaluatingthe pharmacokinetics (PK) of azithromycin in healthy adult subjects a higher peak serum concentration(C max) and greater systemic exposure (AUC0-24) of azithromycin are achieved on the day of dosingfollowing a single 2.0 g dose of Zmax versus 1.5 g of azithromycin tablets administered over 3 days (500 mg/day) or 5 days (500 mg on day 1, 250 mg/day on days 2-5) [Table 1]. Consequently, due to thesedifferent PK profiles, Zmax is not interchangeable with azithromycin tablet 3-day and 5-day dosingregimens.Table 1. Mean (SD) Pharmacokinetic Parameters for Azithromycin on Day 1 Following theAdministration of a Single Dose of 2.0 g Zmax or 1.5 g of Azithromycin Tablets Given over 3 Days(500 mg/day) or 5 Days (500 mg on Day 1 and 250 mg on Days 2-5) to Healthy Adult SubjectsAzithromycin RegimenPharmacokineticParameter*Zmax[n=41]†3-day ‡[n=12]5-day ‡[n=12]C max (µg/mL)0.821(0.281)0.441(0.223)0.434(0.202)T max§ (hr)5.0(2.0-8.0)2.5(1.0-4.0)2.5(1.0-6.0)AUC0-24 (µg·hr/mL)8.62(2.34)2.58(0.84)2.60(0.71)AUC0-8¶(µg·hr/mL)20.0(6.66)17.4(6.2)14.9(3.1)t1/2 (hr)58.8(6.91)71.8(14.7)68.9(13.8)* Zmax, 3-day and 5-day regimen parameters obtained from separate PK studies † n = 21 for AUC0-8 and t1/2‡ C max, T max and AUC0-24 values for Day 1 only§Median (range)¶ Total AUC for the 1-day, 3-day and 5-day regimensSD = standard deviationC max = maximum serum concentrationT max = time to C maxAUC = area under concentration vs. time curvet1/2 = terminal serum half-lifeAbsorptionIn a two-way crossover study, sixteen healthy adult subjects were administered single doses of 2.0 g Zmax and azithromycin powder for oral suspension (POS) (2 × 1.0 g sachets). The mean C max and AUC0-t of azithromycin were lower by 57% and 17%, respectively with Zmax compared to azithromycin POS. The bioavailability of Zmax relative to azithromycin POS was 83%. On average, peak serum concentrations were achieved approximately 2.5 hours later following Zmax administration compared to azithromycin POS. Thus, single 2.0 g doses of Zmax and azithromycin POS are not bioequivalent and are not interchangeable.When a 2.0 g dose of Zmax was administered to 15 healthy adult subjects following a high-fat meal (150 kcal from proteins, 250 kcal from carbohydrates and 500-600 kcal from fats) the mean azithromycin C max increased by 115% and the mean AUC0-t increased by 23% as compared to administration in a fasted state. When a 2.0 g dose of Zmax was administered to 88 adult subjects following a standard meal (56 kcal from proteins, 316 kcal from carbohydrates, and 207 kcal from fats) the mean azithromycin C max increased by 119% and the mean AUC0-72 increased 12% as compared to administration in the fasted state. (See DOSAGE AND ADMINISTRATION.)In a two-way crossover study, 39 healthy adult subjects were administered 2.0 g dose of Zmax alone and with 20 mL of regular strength aluminum and magnesium hydroxide antacid. Following the administration of Zmax with an aluminum and magnesium hydroxide antacid, the rate and extent of azithromycin absorption were not altered.DistributionThe serum protein binding of azithromycin is concentration dependent, decreasing from 51% at0.02 µg/mL to 7% at 2.0 µg/mL.Following oral administration, azithromycin is widely distributed throughout the body with an apparent steady-state volume of distribution of 31.1 L/kg.Higher azithromycin concentrations in tissues than in plasma or serum have been observed. The extensive distribution of drug to tissues may be relevant to clinical activity. The antimicrobial activity of azithromycin is pH related and appears to be reduced with decreasing pH. Hence, high tissue concentrations should not be interpreted as being quantitatively related to clinical efficacy. Selected tissue (or fluid) concentration and tissue (or fluid) to plasma/serum concentration ratios are shown in Table 2.Table 2. Azithromycin Concentrations Following a 500 mg Dose in Adults*TISSUE OR FLUID TIME AFTERDOSE (hr) TISSUE OR FLUIDCONCENTRATION(µg/g or µg/mL)CORRESPONDINGPLASMA OR SERUMCONCENTRATION(µg/mL)TISSUE (FLUID)PLASMA (SERUM)RATIOSKIN 72-96 0.4 0.012 35LUNG 72-96 4.0 0.012 >100 SPUTUM†2-4 1.0 0.64 2 SPUTUM‡10-12 2.9 0.1 30 TONSIL§9-18 4.5 0.03 >100 TONSIL§180 0.9 0.006 >100 CERVIX¶19 2.8 0.04 70 * Azithromycin tissue concentrations were originally determined using 250 mg capsules.† Sample was obtained 2-4 hours after the first dose.‡ Sample was obtained 10-12 hours after the first dose.§ Dosing regimen of two doses of 250 mg each, separated by 12 hours.¶Sample was obtained 19 hours after a single 500 mg dose.The extensive tissue distribution was confirmed by examination of additional tissues and fluids (bone, ejaculum, prostate, ovary, uterus, salpinx, stomach, liver, and gallbladder). However, the clinical significance of these tissue concentration data is unclear as clinical data from adequate andwell-controlled studies of azithromycin treatment of infections in these additional body sites are not available.Following a regimen of 500 mg of azithromycin tablets on the first day and 250 mg daily for 4 days, only very low concentrations were noted in cerebrospinal fluid (less than 0.01 µg/mL) in the presence ofnon-inflamed meninges.MetabolismIn vitro and in vivo studies to assess the metabolism of azithromycin have not been performed.EliminationSerum azithromycin concentrations following a single 2.0 g dose of Zmax declined in a polyphasic pattern with a terminal elimination half-life of 59 hours. The prolonged terminal half-life is thought to be due to a large apparent volume of distribution.Biliary excretion of azithromycin, predominantly as unchanged drug, is a major route of elimination. Over the course of a week, approximately 6% of the administered dose appears as unchanged drug in urine.Special PopulationsRenal InsufficiencyAzithromycin pharmacokinetics was investigated in 42 adults (21 to 85 years of age) with varying degrees of renal impairment. Following the oral administration of a single 1.0 g dose of azithromycin (4 ×250 mg capsules), the mean C max and AUC0-120 increased by 5.1% and 4.2%, respectively in subjects with GFR 10 to 80 mL/min compared to subjects with normal renal function (GFR >80 mL/min). The meanC max and AUC0-120 increased 61% and 35%, respectively in subjects with end-stage renal disease (GFR<10 mL/min) compared to subjects with normal renal function (GFR >80 mL/min). Based upon the pharmacokinetic data for azithromycin in subjects with renal impairment, no dose adjustment for Zmax is recommended in patients with GFR >10 mL/min. (See DOSAGE AND ADMINISTRATION.)Hepatic InsufficiencyThe pharmacokinetics of azithromycin in subjects with hepatic impairment has not been established.GenderThe impact of gender on the pharmacokinetics of azithromycin has not been evaluated for Zmax. However,previous studies have demonstrated no significant differences in the disposition of azithromycin between male and female subjects. No dosage adjustment of Zmax is recommended based on gender.Geriatric PatientsThe pharmacokinetics of azithromycin following administration of Zmax has not been evaluated in geriatric patients.Pediatric PatientsZmax is not approved for pediatric patients.Drug-Drug InteractionsDrug interaction studies were performed with azithromycin capsules and tablets (doses ranged from 500 to 1200 mg) and drugs likely to be co-administered. The effects of co-administration of azithromycin on the pharmacokinetics of other drugs are shown in Table 3 and the effects of other drugs on the pharmacokinetics of azithromycin are shown in Table 4.Co-administration of azithromycin capsules and tablets at therapeutic doses had a modest effect on the pharmacokinetics of the drugs listed in Table 3. Although the drug interaction studies were not conducted with Zmax , no potential drug interactions are expected since the total exposure to azithromycin is comparable for Zmax and the other azithromycin regimens. Therefore, no dosage adjustment of drugs listed in Table 3 is recommended when co-administered with Zmax. (See PRECAUTIONS - Drug Interactions.)Co-administration of azithromycin tablets with efavirenz or fluconazole had a modest effect on the pharmacokinetics of azithromycin. Nelfinavir significantly increased the C max and AUC of azithromycin. Similar results are expected with Zmax . Although no dosage adjustment of Zmax is recommended when administered with drugs listed in Table 4, close monitoring for known side effects of azithromycin, such as liver enzyme abnormalities and hearing impairment, is warranted when co-administered with nelfinavir. (See PRECAUTIONS - Drug Interactions.)Table 3. Drug Interactions: Pharmacokinetic Parameters for Co-administered Drugs in the Presence of AzithromycinRatio (with/without Azithromycin) ofCo-administered DrugPharmacokinetic Parameters (90%CI); No Effect = 1.00 Co-administeredDrugDose of Co-administeredDrugDose of Azithromycin*nMean C max Mean AUC Atorvastatin 10 mg/day × 8 days500 mg/day PO on days 6-812 0.83 (0.63 to 1.08)1.01 (0.81 to 1.25)Carbamazepine200 mg/day × 2 days, then 200 mg BID × 18 days 500 mg/day PO for days 16-1870.97 (0.88 to 1.06) 0.96 (0.88 to 1.06) Cetirizine20 mg/day × 11 days500 mg PO on day 7, then 250 mg/day on days 8-11141.03 (0.93 to 1.14) 1.02 (0.92 to 1.13) Didanosine 200 mg PO BID × 21 days1,200 mg/day POon days 8-21 6 1.44 (0.85 to 2.43)1.14 (0.83 to 1.57)Efavirenz 400 mg/day × 7days600 mg PO on day 7 14 1.04† 0.95† Fluconazole 200 mg PO single dose 1,200 mg POsingle dose18 1.04 (0.98 to 1.11)1.01 (0.97 to 1.05)Indinavir 800 mg TID × 5days1,200 mg PO on day 5 18 0.96 (0.86 to 1.08)0.90 (0.81 to 1.00)Midazolam 15 mg PO on day 3 500 mg/day PO × 3days12 1.27 (0.89 to 1.81)1.26 (1.01 to 1.56)Nelfinavir 750 mg TID × 11 days1,200 mg PO onday 9 14 0.90 (0.81 to 1.01)0.85 (0.78 to 0.93)Rifabutin 300 mg/day × 10days500 mg PO on day 1, then 250 mg/day on days 2-106‡NASildenafil 100 mg on days 1 and 4 500 mg/day PO × 3days12 1.16 (0.86 to 1.57)0.92 (0.75 to 1.12)Theophylline 4 mg/kg IV on days 1, 11, 25 500 mg PO on day7, then 250 mg/dayon days 8-11101.19 (1.02 to 1.40) 1.02 (0.86 to 1.22) Theophylline 300 mg PO BID × 15 days500 mg PO on day6, then 250 mg/day on days 7-108 1.09 (0.92 to 1.29)1.08 (0.89 to 1.31)Triazolam 0.125 mg on day 2 500 mg PO on day1, then 250 mg/day on day 2121.06†1.02†Trimethoprim/ Sulfamethoxazole 160 mg/800 mg/day PO × 7 days 1,200 mg PO on day 7120.85(0.75 to 0.97)/0.90 (0.78 to 1.03)0.87(0.80 to 0.95)/0.96 (0.88 to 1.03)Zidovudine 500 mg/day PO × 21 days600 mg/day PO × 14 days5 1.12 (0.42 to 3.02)0.94 (0.52 to 1.70)Zidovudine500 mg/day PO × 21 days1,200 mg/day PO × 14 days41.31 (0.43 to 3.97) 1.30 (0.69 to2.43)NA = not available* Refers to azithromycin capsules and tablets unless specified † 90% confidence interval not reported‡ Mean rifabutin concentrations one-half day after the last dose of rifabutin were 60 ng/mL when co-administered with azithromycin and 71 ng/mL when co-administered with placebo.Table 4. Drug Interactions: Pharmacokinetic Parameters for Azithromycin in the Presence of Co-administered Drugs (See PRECAUTIONS - Drug Interactions )Ratio (with/without co-administereddrug) of AzithromycinPharmacokinetic Parameters (90%CI); No Effect = 1.00 Co-administeredDrugDose of Co-administeredDrugDose of Azithromycin*nMean C max Mean AUC Efavirenz 400 mg/day × 7 days600 mg PO on day 714 1.22 (1.04 to 1.42)0.92† Fluconazole 200 mg PO single dose1,200 mg PO single dose18 0.82 (0.66 to 1.02)1.07 (0.94 to 1.22)Nelfinavir 750 mg TID × 11 days1,200 mg PO on day 914 2.36 (1.77 to 3.15)2.12 (1.80 to 2.50)Rifabutin300 mg/day × 10 days500 mg PO on day 1, then 250 mg/day on days 2-106‡NAAl and Mg hydroxide20 mL regular strength, single dose2.0 g Zmax, single dose390.99 (0.93 to 1.06) 0.99 (0.92 to 1.08)NA = not available* Refers to azithromycin capsules and tablets unless specified † 90% confidence interval not reported‡ Mean azithromycin concentrations one day after the last dose were 53 ng/mL when co-administered with 300 mg daily rifabutin and 49 ng/mL when co-administered with placebo.Microbiology Azithromycin acts by binding to the 50S ribosomal subunit of susceptible microorganisms, thus interfering with microbial protein synthesis. Nucleic acid synthesis is not affected.Azithromycin concentrates in fibroblasts, epithelial cells, macrophages, and circulating neutrophils and monocytes. In vitro incubation techniques have shown that the ratio of intracellular to extracellular concentration was >30 after one hour incubation. In vivo studies suggest that concentration inmacrophages and circulating white blood cells may contribute to drug distribution to inflamed tissues.Azithromycin has been shown to be active against most isolates of the following microorganisms, both in vitro and in clinical infections as described in the INDICATIONS AND USAGE section.Aerobic and facultative Gram-positive microorganisms Streptococcus pneumoniaeNOTE: Erythromycin- and penicillin-resistant Gram-positive isolates may demonstrate cross-resistance to azithromycin.Aerobic and facultative Gram-negative microorganisms Haemophilus influenzae Moraxella catarrhalis“Other” microorganisms Chlamydophila pneumoniae Mycoplasma pneumoniaeBeta-lactamase production should not affect azithromycin activity.The following in vitro data are available, but their clinical si gnificance is unknown.At least 90% of the following microorganisms exhibit an in vitro minimum inhibitory concentration (MIC) less than or equal to the susceptible breakpoints for azithromycin. However, the safety and effectiveness of azithromycin in treating clinical infections due to these microorganisms have not been established in adequate and well-controlled trials.Aerobic and facultative Gram-positive microorganismsStaphylococcus aureusStreptococcus pyogenesStreptococcus agalactiaeStreptococci (Groups C, F, G)Viridans group streptococciAerobic and facultative Gram-negative microorganismsBordetella pertussisLegionella pneumophilaAnaerobic microorganismsPeptostreptococcus speciesPrevotella bivia“Other” microorganismsUreaplasma urealyticumSusceptibility Testing Methods:in vitro susceptibility test results for antimicrobial drugs used in local hospitals and practice areas to the physician as periodic reports that describe the susceptibility profile of nosocomial and community-acquired pathogens. These reports should aid the physician in selecting the most effective antimicrobial.Dilution techniques:Quantitative methods are used to determine antimicrobial minimum inhibitory concentrations (MICs). These MICs provide estimates of the susceptibility of bacteria to antimicrobial compounds. The MICs should be determined using a standardized procedure. Standardized procedures are based on a dilution method1,3 (broth or agar) or equivalent with standardized inoculum concentrations and standardized concentrations of azithromycin powder. The MIC values should be interpreted according to criteria provided in Table 5.Diffusion techniques:Quantitative methods that require measurement of zone diameters also provide reproducible estimates of the susceptibility of bacteria to antimicrobial compounds. One such standardized procedure2,3 requires the use of standardized inoculum concentrations. This procedure uses paper disks impregnated with 15-µg azithromycin to test the susceptibility of microorganisms to azithromycin. The disk diffusion interpretive criteria are provided in Table 5.Table 5. Susceptibility Test Result Interpretive Criteria for AzithromycinMinimum Inhibitory Concentrations (µg/mL)Disk Diffusion (zone diameters in mm)PathogenS I R* S I R* Haemophilus spp. ≤ 4 -- -- ≥ 12 -- -- Streptococci includingS. pneumoniae< 0.5 1 > 2 ≥ 18 14-17 ≤ 13* The current absence of data on resistant strains precludes defining any category other than “susceptible.” If strains yield MIC results other than susceptible, they should be submitted to a reference laboratory for further testing.No interpretive criteria have been established for testing Moraxella catarrhalis. This species is not usually tested.A report of “susceptible” indicates that the pathogen is likely to be inhibited if the antimicrobial compound reaches the concentrations usually achievable. A report of “intermediate” indicates that the result should be considered equivocal, and, if the microorganism is not fully susceptible to alternative, clinically feasible drugs, the test should be repeated. This category implies possible clinical applicability in body sites where the drug is physiologically concentrated or in situations where high dosage of drug can be used. This category also provides a buffer zone, which prevents small uncontrolled technical factors from causing major discrepancies in interpretation. A report of “resistant” indicates that the pathogen is not likely to be inhibited if the antimicrobial compound reaches the concentrations usually achievable; other therapy should be selected.QUALITY CONTROLStandardized susceptibility test procedures require the use of quality control microorganisms to control the technical aspects of the test procedures. Standard azithromycin powder should provide the range of values noted in Table 6. Quality control microorganisms are specific strains of organisms with intrinsic biological properties. QC strains are very stable strains, which will give a standard and repeatable susceptibility pattern. The specific strains used for microbiological quality control are not clinically significant.Table 6. Acceptable Quality Control Ranges for AzithromycinQC Strain Minimum InhibitoryConcentrations (µg/mL)Disk Diffusion (zone diameters in mm)Haemophilus influenzaeATCC 49247 1.0-4.0 13-21 Streptococcus pneumoniaeATCC 49619 0.06-0.25 19-25INDICATIONS AND USAGEZmax is indicated for the treatment of patients with mild to moderate infections caused by susceptible strains of the designated microorganisms in the specific conditions listed below. Please see DOSAGE AND ADMINISTRATION for specific dosing recommendations.AdultsAcute bacterial sinusitis due to Haemophilus influenzae, Moraxella catarrhalis or Streptococcus pneumoniae.Community-acquired pneumonia due to Chlamydophila pneumoniae, Haemophilus influenzae, Mycoplasma pneumoniae or Streptococcus pneumoniae, in patients appropriate for oral therapy. (See CLINICAL STUDIES.)To reduce the development of drug-resistant bacteria and maintain the effectiveness of Zmax and other antibacterial drugs, Zmax should be used only to treat infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy.Appropriate culture and susceptibility tests should be performed before treatment to determine the causative organism and its susceptibility to Zmax. Therapy with Zmax may be initiated before results of these tests are known; once the results become available, antimicrobial therapy should be adjusted accordingly.CONTRAINDICATIONSZmax is contraindicated in patients with known hypersensitivity to azithromycin, erythromycin or any macrolide or ketolide antibiotic.WARNINGSSerious allergic reactions, including angioedema, anaphylaxis, and dermatologic reactions including Stevens-Johnson syndrome and toxic epidermal necrolysis have been reported rarely in patients on azithromycin therapy using other formulations. Although rare, fatalities have been reported. (See CONTRAINDICATIONS.) Despite initially successful symptomatic treatment of the allergic symptoms, when symptomatic therapy was discontinued, the allergic symptoms recurred soon thereafter in some patients without further azithromycin exposure. These patients required prolonged periods of observation and symptomatic treatment. The relationship of these episodes to the long tissue half-life of azithromycin and subsequent exposure to antigen has not been determined.If an allergic reaction occurs, appropriate therapy should be instituted. Physicians should be aware that reappearance of the allergic symptoms may occur when symptomatic therapy is discontinued.Pseudomembranous colitis has been reported with nearly all antibacterial agents and may range in severity from mild to life-threatening. Therefore, it is important to consider this diagnosis in patients who present with diarrhea subsequent to the administration of antibacterial agents. Treatment with antibacterial agents alters the normal flora of the colon and may permit overgrowth of clostridia. Studies indicate that a toxin produced by Clostridium difficile is a primary cause of “antibiotic-associated colitis.”After the diagnosis of pseudomembranous colitis has been established, therapeutic measures should be initiated. Mild cases of pseudomembranous colitis usually respond to discontinuation of the drug alone. In moderate to severe cases, consideration should be given to management with fluids and electrolytes, protein supplementation, and treatment with an antibacterial drug clinically effective against Clostridium difficile colitis.PRECAUTIONSGeneralBecause azithromycin is principally excreted via the liver, caution should be exercised when azithromycin is administered to patients with impaired hepatic function. Due to the limited data in subjects with GFR <10 mL/min, caution should be exercised when prescribing azithromycin in these patients. (See CLINICAL PHARMACOLOGY - Special Populations - Renal Insu fficiency.)Prolonged cardiac repolarization and QT interval, imparting a risk of developing cardiac arrhythmia and torsades de pointes, have been seen in treatment with other macrolides. A similar effect with azithromycin cannot be completely ruled out i n patients at increased risk for prolonged cardiac repolarization.Prescribing Zmax in the absence of a proven or strongly suspected bacterial infection is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistant bacteria. Information for PatientsPatients should be instructed to take Zmax on an empty stomach (at least 1 hour before or 2 hours following a meal).Patients should be instructed to immediately contact a physician if any signs of an allergic reaction occur. Patients who vomit within the first hour should contact their health care provider about further treatment. Keep bottle tightly closed. Store at room temperature. Use within 12 hours of constitution. Shake bottle well before use. The entire contents of the bottle should be consumed.Patients should be advised that Zmax may be taken without regard to antacids containing magnesium hydroxide and/or aluminum hydroxide.Patients should be counseled that antibacterial drugs including Zmax should only be used to treat bacterial infections. They do not treat viral infections (e.g., the common cold). Not taking the complete prescribed dose may (1) decrease the effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by Zmax or other antibacterial drugs in the future.Drug InteractionsCo-administration of nelfinavir at steady-state with a single dose of azithromycin (2 × 600 mg tablets) results in increased azithromycin serum concentrations. Although a dose adjustment of azithromycin is not recommended when administered in combination with nelfinavir, close monitoring for known side effects of azithromycin, such as liver enzyme abnormalities and hearing impairment, is warranted. (See ADVERSE REACTIONS.)Azithromycin did not affect the prothrombin time response to a single dose of warfarin. However, prudent medical practice dictates careful monitoring of prothrombin time in all patients treated with azithromycin and warfarin concomitantly. Concurrent use of macrolides and warfarin in clinical practice has been associated with increased anticoagulant effects.Drug interaction studies were performed with azithromycin and other drugs likely to be co-administered. (See CLINICAL PHARMACOLOGY - Drug-Drug Interactions.) When used in therapeutic doses, azithromycin had a modest effect on the pharmacokinetics of atorvastatin, carbamazepine, cetirizine, didanosine, efavirenz, fluconazole, indinavir, midazolam, rifabutin, sildenafil, theophylline (intravenous and oral), triazolam, trimethoprim/sulfamethoxazole or zidovudine. Co-administration with efavirenz or fluconazole had a modest effect on the pharmacokinetics of azithromycin. No dosage adjustment of either drug is recommended when azithromycin is co-administered with any of the above agents.Interactions with the drugs listed below have not been reported in clinical trials with azithromycin; however, no specific drug interaction studies have been performed to evaluate potential drug-drug interaction. Nonetheless, they have been observed with macrolide products. Until further data are developed regarding drug interactions when azithromycin and these drugs are used concomitantly, careful monitoring of patients is advised:Digoxin–elevated digoxin concentrations.Ergotamine or dihydroergotamine–acute ergot toxicity characterized by severe peripheralvasospasm and dysesthesia.Cyclosporine, hexobarbital and phenytoin concentrations.Laboratory Test InteractionsThere are no reported laboratory test interactions.Repeat TreatmentStudies evaluating the use of repeated courses of Zmax have not been conducted.Carcinogenesis, Mutagenesis, Impairment of FertilityLong-term studies in animals have not been performed to evaluate carcinogenic potential. Azithromycin has shown no mutagenic potential in standard laboratory tests: mouse lymphoma assay, human lymphocyte clastogenic assay, and mouse bone marrow clastogenic assay. No evidence of impaired fertility due to azithromycin was found in rats given daily doses up to 10 mg/kg (approximately 0.05 times the single 2.0 g oral adult human dose on a mg/m2 basis).PregnancyTeratogenic Effects. Pregnancy Category B: Reproduction studies have been performed in rats and mice at doses up to moderately maternally toxic dose concentrations (i.e., 200 mg/kg/day). These daily doses in rats and mice, based on mg/m2, are estimated to be approximately equivalent to one or one-half of, respectively, the single adult oral dose of 2.0 g. In the animal studies, no evidence of harm to the fetus due to azithromycin was found. There are, however, no adequate and well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, azithromycin should be used during pregnancy only if clearly needed.。
溶出度方法学验证-7

– Quats will ion pair with carboxylic acids at 2 pH’s units above pKa
13
Specific problems with SLS
• Use in combination only with Sodium Phosphate for 6.8 pH not Potassium Phosphate—precipitates at room temp
– Anionic
– Non-ionic
Evaluate different surfactants [quantitative]
4
Official Statements
FDA
• A dissolution medium containing surfactant can better simulate the environment of the gastrointestinal tract than a medium containing organic solvents or other nonphysiological substances, making the dissolution test conditions more useful in evaluating drug quality.
• Polysorbates (Tween™) • Sodium dodecyl sulfate (sodium lauryl sulfate) • Lauryl dimethyl amine oxide • Cetyltrimethylammonium bromide (CTAB) • Polyethoxylated alcohols • Polyoxyethylene sorbitan • Octoxynol (Triton X100™) • N, N–dimethyldodecylamine– N–oxide • Hexadecyltrimethylammonium bromide (HTAB)
乌利司他片说明书(美国,FDA,英文)
_________________________________________________________________________________________________________________________________HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use ella safely and effectively. See full prescribing information for ella. ella (ulipristal acetate) tablet Initial U.S. Approval: 2010 ----------------------------INDICATIONS AND USAGE--------------------------- ella is a progesterone agonist/antagonist emergency contraceptive indicated for prevention of pregnancy following unprotected intercourse or a known or suspected contraceptive failure. ella is not intended for routine use as a contraceptive. (1) ----------------------DOSAGE AND ADMINISTRATION----------------------- • One tablet taken orally as soon as possible, within 120 hours (5 days) after unprotected intercourse or a known or suspected contraceptive failure (2) • The tablet can be taken with or without food. (2) ---------------------DOSAGE FORMS AND STRENGTHS---------------------- • 30 mg tablet (3) -------------------------------CONTRAINDICATIONS------------------------------ • Known or suspected pregnancy (4)-----------------------WARNINGS AND PRECAUTIONS-----------------------• ella is not indicated for termination of an existing pregnancy. Exclude pregnancy before administering. (5.1) • Ectopic pregnancy: Women who become pregnant or complain of lowerabdominal pain after taking ella should be evaluated for ectopic pregnancy. (5.2)• Effect on menstrual cycle: ella may alter the next expected menses. If menses is delayed beyond 1 week, pregnancy should be ruled out. (5.5)• ella does not protect against STI/HIV. (5.6)------------------------------ADVERSE REACTIONS------------------------------- The most common adverse reactions (≥5%) in the clinical trials were headache (18%), abdominal pain (12%), nausea (12%), dysmenorrhea (9%), fatigue (6%) and dizziness (5%). (6)To report SUSPECTED ADVERSE REACTIONS, contact WatsonLaboratories, Inc. at 1-800-272-5525 or FDA at 1-800-FDA-1088 or /medwatch.------------------------------DRUG INTERACTIONS-------------------------------• Drugs or herbal products that induce certain enzymes, such as CYP3A4,may decrease the effectiveness of ella . (7) -----------------------USE IN SPECIFIC POPULATIONS------------------------• Nursing mothers: ella is not recommended for use by breastfeeding women. (8.3)• ella is not intended for use in premenarcheal (8.4) or postmenopausalwomen. (8.5)See 17 for PATIENT COUNSELING INFORMATION and FDAApproved Patient LabelingRevised:8/2010 FULL PRESCRIBING INFORMATION: CONTENTS*1INDICATIONS AND USAGE 2DOSAGE AND ADMINISTRATION 3DOSAGE FORMS AND STRENGTHS 4CONTRAINDICATIONS 5WARNINGS AND PRECAUTIONS 5.1 E xisting Pregnancy5.2 E ctopic Pregnancy5.3 R epeated Use5.4 Fertility Following Use5.5 Effect on Menstrual Cycle5.6 Sexually Transmitted Infections/HIV6ADVERSE REACTIONS 6.1 Clinical Trials Experience6.2 Postmarketing Experience7DRUG INTERACTIONS 7.1 Changes in Emergency Contraceptive Effectiveness Associatedwith Co-administration of Other Products7.2 Increase in Plasma Concentrations ofella Associated with Co-Administered Drugs7.3 Effects of ella on Co-Administered Drugs 8USE IN SPECIFIC POPULATIONS 8.1 P regnancy8.3 N ursing Mothers8.4 P ediatric Use 8.5 G eriatric Use 8.6 R ace 8.7 H epatic Impairment 8.8 R enal Impairment 10 OVERDOSAGE 11 DESCRIPTION 12 CLINICAL PHARMACOLOGY 12.1 Mechanism of Action 12.2 Pharmacodynamics 12.3 Pharmacokinetics 13 NONCLINICAL TOXICOLOGY 13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility 14 CLINICAL STUDIES 14.1 Open-label Study 14.2 Single-Blind Comparative Study 14.3 Pooled Analysis 16 HOW SUPPLIED/STORAGE AND HANDLING 17 PATIENT COUNSELING INFORMATION * Sections or subsections omitted from the full prescribing information are not listedFULL PRESCRIBING INFORMATION1 INDICATIONS AND USAGEella is a progesterone agonist/antagonist emergency contraceptive indicated for prevention of pregnancy following unprotected intercourse or a known or suspected contraceptive failure. ella is not intended for routine use as a contraceptive.2 DOSAGE AND ADMINISTRATIONInstruct patients to take one tablet orally as soon as possible within 120 hours (5 days) after unprotected intercourse or a known or suspected contraceptive failure.The tablet can be taken with or without food.If vomiting occurs within 3 hours of ella intake, consideration should be given to repeating the dose.ella can be taken at any time during the menstrual cycle.3 DOSAGE FORMS AND STRENGTHSThe ella tablet is supplied as a white to off-white, round, curved tablet containing 30 mg of ulipristal acetate and is marked “ella” on both sides.4 CONTRAINDICATIONSella is contraindicated for use in the case of known or suspected pregnancy. The risks to a fetus when ella is administered to a pregnant woman are unknown. If this drug is inadvertently used during pregnancy, the woman should be apprised of the potential hazard to the fetus. [See Use in Specific Populations (8.1).]5 WARNINGS AND PRECAUTIONS5.1 Existing Pregnancyella is not indicated for termination of an existing pregnancy. Pregnancy should be excluded before prescribing ella. If pregnancy cannot be excluded on the basis of history and/or physical examination, pregnancy testing should be performed.A follow-up physical or pelvic examination is recommended if there is any doubt concerning the general health or pregnancy status of any woman after taking ella.5.2 Ectopic PregnancyA history of ectopic pregnancy is not a contraindication to use of this emergency contraceptive method. Healthcare providers, however, should consider the possibility of ectopic pregnancy in women who become pregnant or complain of lower abdominal pain after taking ella. A follow-up physical or pelvic examination is recommended if there is any doubt concerning the general health or pregnancy status of any woman after taking ella.Use5.3 Repeatedella is for occasional use as an emergency contraceptive. It should not replace a regular method of contraception. Repeated use of ella within the same menstrual cycle is not recommended, as safety and efficacy of repeat use within the same cycle has not been evaluated.FollowingUse5.4 FertilityA rapid return of fertility is likely following treatment with ella for emergency contraception; therefore, routine contraception should be continued or initiated as soon as possible following use of ella to ensure ongoing prevention of pregnancy. While there are no data about use of ella with regular hormonal contraceptives, due to its high affinity binding to the progesterone receptor, use of ella may reduce the contraceptive action of regular hormonal contraceptive methods. Therefore, after use of ella, a reliable barrier method of contraception should be used with subsequent acts of intercourse that occur in that same menstrual cycle.5.5 Effect on Menstrual CycleAfter ella intake, menses sometimes occur earlier or later than expected by a few days. In clinical trials, cycle length was increased by a mean of 2.5 days but returned to normal in the subsequent cycle. Seven percent of subjects reported menses occurring more than 7 days earlier than expected, and 19% reported a delay of more than 7 days. If there is a delay in the onset of expected menses beyond 1 week, rule out pregnancy.Nine percent of women studied reported intermenstrual bleeding after use of ella.5.6 Sexually Transmitted Infections/HIVella does not protect against HIV infection (AIDS) or other sexually transmitted infections (STIs).6 ADVERSE REACTIONS6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.ella was studied in an open-label multicenter trial (Open-Label Study) and in a comparative, randomized, single-blind, multicenter trial (Single-Blind Comparative Study). In these studies, a total of 2,637 (1,533 + 1,104) women in the 30 mg ulipristal acetate groups were included in the safety analysis. The mean age of women who received ulipristal acetate was 24.5 years and the mean body mass index (BMI) was 25.3. The racial demographics of those enrolled were 67% Caucasian, 20% Black or African American, 2% Asian, and 12% other.The most common adverse reactions (≥ 10%) in the clinical trials for women receiving ella were headache (18% overall) and nausea (12% overall) and abdominal and upper abdominal pain (12% overall). Table 1 lists those adverse reactions that were reported in ≥5% of subjects in the clinical studies (14).Table 1: Adverse Reactions in ≥5% of Women (%) Receiving a Single Dose of ella (30 mg Ulipristal Acetate)Most Common AdverseReactions Open-Label Study Single-BlindComparativeStudy N = 1,533 N = 1,104Headache 1819Nausea 1213Abdominal and upperabdominal pain15 8Dysmenorrhea 7 13Fatigue 66Dizziness 556.2 Postmarketing ExperienceThe following adverse reactions have been identified during post-approval use of ella:Skin and Subcutaneous Tissue Disorders: AcneBecause these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.7 DRUG INTERACTIONSNo drug interaction studies have been conducted for ella in vivo. However, in vitro data indicate that ella is predominantly metabolized by CYP3A4.7.1 Changes in Emergency Contraceptive Effectiveness Associated with Co-administration of Other Products Drugs or herbal products that induce enzymes, including CYP3A4, may decrease the plasma concentrations of ella, and may decrease its effectiveness. Some drugs or herbal products that may decrease the effectiveness of ella include: •barbiturates•bosentan•carbamazepine•felbamate•griseofulvin•oxcarbazepine•phenytoin•rifampin•St. John’s Wort•topiramate7.2 Increase in Plasma Concentrations of ella Associated with Co-Administered DrugsCYP3A4 inhibitors such as itraconazole or ketoconazole may increase plasma concentrations of ella.7.3 Effects of ella on Co-Administered DrugsIn vitro studies demonstrated that ella does not induce or inhibit the activity of cytochrome P450 enzymes.8 USE IN SPECIFIC POPULATIONS8.1 PregnancyPregnancy Category X. [See Contraindications (4).]Use of ella is contraindicated during an existing or suspected pregnancy.There are no adequate and well controlled studies in pregnant women.Ulipristal acetate was administered repeatedly to pregnant rats and rabbits during the period of organogenesis. Embryofetal loss was noted in all pregnant rats and in half of the pregnant rabbits following 12 and 13 days of dosing, at daily drug exposures 1/3 and 1/2 the human exposure, respectively, based on body surface area (mg/m2). There were no malformations of the surviving fetuses in these studies. Adverse effects were not observed in the offspring of pregnant rats administered ulipristal acetate during the period of organogenesis through lactation at drug exposures 1/24 the human exposure based on AUC. Administration of ulipristal acetate to pregnant monkeys for four days during the first trimester caused pregnancy termination in 2/5 animals at daily drug exposures 3 times the human exposure based on body surface area.8.3 Nursing MothersIt is not known if ulipristal acetate is excreted in human milk. However, ulipristal acetate is detected in milk of lactating rats. Because many drugs are excreted in human milk, risk to the breast-fed child cannot be excluded. Use of ella by breastfeeding women is not recommended.8.4 Pediatric UseSafety and efficacy of ella have been established in women of reproductive age. Safety and efficacy are expected to be the same for postpubertal adolescents less than 18 years and for users 18 years and older. Use of ella before menarche is not indicated.8.5 Geriatric UseThis product is not intended for use in postmenopausal women.8.6 RaceWhile no formal studies have evaluated the effect of race, a cross-study comparison of two pharmacokinetic studies indicated that exposure in South Asians may exceed that in Caucasians and African Americans. However, no difference in efficacy and safety was observed for women of different races in clinical studies.8.7 Hepatic ImpairmentNo studies have been conducted to evaluate the effect of hepatic disease on the disposition of ella.8.8 Renal ImpairmentNo studies have been conducted to evaluate the effect of renal disease on the disposition of ella.10 OVERDOSAGEExperience with ulipristal acetate overdose is limited. In a clinical study, single doses equivalent to up to four times ella were administered to a limited number of subjects without any adverse reactions.11 DESCRIPTIONThe ella (ulipristal acetate) tablet for oral use contains 30 mg of a single active steroid ingredient, ulipristal acetate [17αacetoxy-11β-(4-N,N-dimethylaminophenyl)-19-norpregna-4,9-diene-3,20-dione], a synthetic progesteroneagonist/antagonist. The inactive ingredients are lactose monohydrate, povidone K-30, croscarmellose sodium and magnesium stearate.Ulipristal acetate is a white to yellow crystalline powder which has a molecular weight of 475.6. The structural formula is:C o nc e n t r a t i o n (n g /m L )C 30H 37NO 412 CLINICAL PHARMACOLOGY12.1 Mechanism of Action When taken immediately before ovulation is to occur, ella postpones follicular rupture. The likely primary mechanism of action of ulipristal acetate for emergency contraception is therefore inhibition or delay of ovulation; however, alterations to the endometrium that may affect implantation may also contribute to efficacy. 12.2 PharmacodynamicsUlipristal acetate is a selective progesterone receptor modulator with antagonistic and partial agonistic effects (a progesterone agonist/antagonist) at the progesterone receptor. It binds the human progesterone receptor and prevents progesterone from occupying its receptor.The pharmacodynamics of ulipristal acetate depends on the timing of administration in the menstrual cycle. Administration in the mid-follicular phase causes inhibition of folliculogenesis and reduction of estradiol concentration. Administration at the time of the luteinizing hormone peak delays follicular rupture by 5 to 9 days. Dosing in the early luteal phase does not significantly delay endometrial maturation but decreases endometrial thickness by 0.6 ± 2.2 mm (mean ± SD). 12.3 Pharmacokinetics Absorption Following a single dose administration of ella in 20 women under fasting conditions, maximum plasma concentrations of ulipristal acetate and the active metabolite, monodemethyl-ulipristal acetate, were 176 and 69 ng/ml and were reached at 0.9 and 1 hour, respectively.Figure 1: Mean (± SD) Plasma Concentration-time Profile of Ulipristal Acetate and Monodemethyl-ulipristalAcetate Following Single Dose Administration of 30 mg Ulipristal AcetateTable 2: Pharmacokinetic Parameter Values Following Administration of ella (ulipristal acetate) Tablet 30 mg to 20Healthy Female Volunteers under Fasting ConditionsMean (± SD)C max (ng/ml)AUC0-t(ng·hr/ml)AUC0-∞(ng·hr/ml)t max(hr)*t1/2(hr)Ulipristal acetate 176(89)548(259)556(260)0.9(0.5-2.0)32(6.3)Monodemethyl-ulipristal acetate 69(26) 240(59)246(59)1.00(0.8-2.0)27(6.9)C max = maximum concentrationAUC0-t = area under the drug concentration curve from time 0 to time of last determinable concentrationAUC0-∞ = area under the drug concentration curve from time 0 to infinityt max = time to maximum concentrationt1/2 = elimination half-life* Median (range)Effect of food: Administration of ella together with a high-fat breakfast resulted in approximately 40 - 45% lower meanC max, a delayed t max (from a median of 0.75 hours to 3 hours) and 20 - 25% higher mean AUC0-∞of ulipristal acetate and monodemethyl-ulipristal acetate compared with administration in the fasting state. These differences are not expected to impair the efficacy or safety of ella to a clinically significant extent; therefore, ella can be taken with or without food.DistributionUlipristal acetate is highly bound (> 94%) to plasma proteins, including high density lipoprotein, alpha-l-acid glycoprotein, and albumin.MetabolismUlipristal acetate is metabolized to mono-demethylated and di-demethylated metabolites. In vitro data indicate that this is predominantly mediated by CYP3A4. The mono-demethylated metabolite is pharmacologically active.ExcretionThe terminal half-life of ulipristal acetate in plasma following a single 30 mg dose is estimated to 32.4 ± 6.3 hours.13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of FertilityCarcinogenicity: Carcinogenicity studies with ulipristal acetate have not been conducted.Genotoxicity: Ulipristal acetate was not genotoxic in the Ames assay, in vitro mammalian assays utilizing mouse lymphoma cells and human peripheral blood lymphocytes , and in an in vivo micronucleus assay in mice.Impairment of Fertility: Single oral doses of ulipristal acetate prevented ovulation in 50% of rats at 2 times the human exposure based on body surface area (mg/m2). Single doses of ulipristal acetate given on post-coital days 4 or 5 prevented pregnancy in 80-100% of rats and in 50% of rabbits when given on post-coital days 5 or 6 at drug exposures 4 and 12 times the human exposure based on body surface area. Lower doses administered for 4 days to rats and rabbits were also effective at preventing ovulation and pregnancy.14 CLINICAL STUDIESTwo multicenter clinical studies evaluated the efficacy and safety of ella. An open-label study provided the primary data to support the efficacy and safety of ulipristal acetate for emergency contraception when taken 48 to 120 hours after unprotected intercourse. A single-blind comparative study provided the primary data to support the efficacy and safety of ulipristal acetate for emergency contraception when taken 0 to 72 hours after unprotected intercourse and provided supportive data for ulipristal acetate for emergency contraception when taken > 72 to 120 hours after unprotected intercourse. Women in both studies were required to have a negative pregnancy test prior to receiving emergency contraception. The primary efficacy analyses were performed on subjects less than 36 years of age who had a known pregnancy status after taking study medication.Table 3: Summary of Clinical Trial Results for Women Who Received a SingleDose of ella (30 mg Ulipristal Acetate)Open-Label Study 48 to 120 Hours *Single-Blind Comparative Study 0 to 72 Hours *N = 1,242 N = 844 Expected Pregnancy Rate ** 5.5 5.6Observed Pregnancy Rate ** (95% confidence interval)2.2(1.5, 3.2)1.9(1.1, 3.1)* Time after unprotected intercourse when ella was taken** Number of pregnancies per 100 women at risk for pregnancy14.1 Open-Label StudyThis study was a multicenter open-label trial conducted at 40 family planning clinics in the United States. Healthy women with a mean age of 24 years who requested emergency contraception 48 to 120 hours after unprotected intercourse received a dose of 30 mg ulipristal acetate (ella). The median BMI for the study subjects was 25.3 and ranged from 16.1 to 61.3kg/m2.Twenty-seven pregnancies occurred in 1,242 women aged 18 to 35 years evaluated for efficacy. The number of pregnancies expected without emergency contraception was calculated based on the timing of intercourse with regard to each woman’s menstrual cycle. ella statistically significantly reduced the pregnancy rate, from an expected rate of 5.5% to an observed rate of 2.2%, when taken 48 to 120 hours after unprotected intercourse.14.2 Single-Blind Comparative StudyThis study was a multicenter, single-blind, randomized comparison of the efficacy and safety of 30 mg ulipristal acetate (ella) to levonorgestrel (another form of emergency contraception). Subjects were enrolled at 35 sites in the U.S., the United Kingdom and Ireland, with the majority (66%) having been enrolled in the U.S. Healthy women with a mean age of 25 years who requested emergency contraception within 120 hours of unprotected intercourse were enrolled and randomly allocated to receive ella or levonorgestrel 1.5 mg. The median BMI for the study subjects was 25.3 and ranged from 14.9 to 70.0 kg/m2.In the ella group, 16 pregnancies occurred in 844 women aged 16 to 35 years when emergency contraception was taken 0 to 72 hours after unprotected intercourse. The number of pregnancies expected without emergency contraception was calculated based on the timing of intercourse with regard to each woman’s menstrual cycle; ella statistically significantly reduced the pregnancy rate, from an expected 5.6% to an observed 1.9%, when taken within 72 hours after unprotected intercourse. There were no pregnancies observed in the women who were administered ella more than 72 hours after unprotected intercourse (10% of women who received ella).14.3 Pooled AnalysisData from the two studies were pooled to provide a total efficacy population of women treated with ulipristal acetate up to 120 hours after UPI. Time Trend analysis for the five 24-hour intervals from 0 to 120 hours between unprotected intercourse and treatment was conducted. There were no significant differences in the observed pregnancy rates across the five time intervals.Subgroup analysis of the pooled data by BMI showed that for women with BMI > 30 kg/m2 (16% of all subjects), the observed pregnancy rate was 3.1% (95% CI: 1.7, 5.7), which was not significantly reduced compared to the expected pregnancy rate of 4.5% in the absence of emergency contraception taken within 120 hours after unprotected intercourse. In the comparative study, a similar effect was seen for the comparator emergency contraception drug, levonorgestrel 1.5 mg. For levonorgestrel, when used by women with BMI > 30 kg/m2, the observed pregnancy rate was 7.4% (95% CI: 3.9, 13.4), compared to the expected pregnancy rate of 4.4% in the absence of emergency contraception taken within 72 hours after unprotected intercourse.16 HOW SUPPLIED/STORAGE AND HANDLINGella (ulipristal acetate) tablet, 30 mg is supplied in a PVC-PE-PVDC-aluminum blister. The tablet is a white to off-white, round, curved tablet marked with “ella” on both sides.NDC 52544-238-54 (1 tablet unit of use package)Store at 20-25°C (68-77°F). [See USP controlled room temperature.]Keep the blister in the outer carton in order to protect from light. Keep out of reach of children.17 PATIENT COUNSELING INFORMATION[See FDA- Approved Patient Labeling]Information for Patients• Instruct patients to take ella as soon as possible and not more than 120 hours after unprotected intercourse or a known or suspected contraceptive failure.• Advise patients that they should not take ella if they know or suspect they are pregnant and that ella is not indicated for termination of an existing pregnancy.• Advise patients to contact their healthcare provider immediately in case of vomiting within three hours of taking the tablet, to discuss whether to take another tablet.• Advise patients to seek medical attention if they experience severe lower abdominal pain 3 to 5 weeks after taking ella, in order to be evaluated for an ectopic pregnancy.• Advise patients to contact their healthcare provider and consider the possibility of pregnancy if their period is delayed after taking ella by more than 1 week beyond the date it was expected.• Advise patients not to use ella as routine contraception, or to use it repeatedly in the same menstrual cycle.• Advise patients that ella may reduce the contraceptive action of regular hormonal contraceptive methods and to use a reliable barrier method of contraception after using ella, for any subsequent acts of intercourse that occur in that same menstrual cycle.• Inform patients that ella does not protect against HIV-infection (AIDS) and other sexually transmitted diseases/infections.• Advise patients that they should not use ella if they are breastfeeding.Address medical inquiries to:WATSONMedical CommunicationsP.O. Box 1953Morristown, NJ 07962-1953800-272-5525Distributed By:Watson Pharma, Inc.Morristown, NJ 07962 USAUnder License From:Laboratoire HRA Pharma75003 Paris, Franceella® is a registered trademarkof Laboratoire HRA PharmaManufactured By:Osny Pharma, 95520 Osny, France, orLeón Farma S.A., 24008 León, SpainFDA Approved Patient LabelingPatient Informationella (“el‐uh”)(ulipristal acetate) tabletRead this Patient Information Leaflet before you take ella. There may be new information. This information does not take the place of talking to your healthcare provider about your medical condition or treatment.What is ella?ella is a prescription emergency contraceptive that reduces your chance of becoming pregnant if your birth control fails or you have unprotected sex.ella should not be used as your regular birth control. It is very important that you have a reliable form of birth control that is right for you.ella will not protect you against HIV infection (AIDS) and other sexually transmitted diseases (STDs).Who should not take ella?o Do not take ella if you know or suspect you are already pregnant. ella is not for use to end an existing pregnancy. Talk to your healthcare provider before taking ella if you think you are pregnant.o Do not take ella if you are breastfeeding, because it is not known if ella passes into breast milk.What should I tell my healthcare provider before taking ella?See “Who should not take ella?”Tell your healthcare provider about all the medicines you take, including prescription and nonprescription medicines, vitamins, and herbal supplements.Using other medicines may affect how ella works. These include St. John’s Wort, phenytoin, rifampin, phenobarbital, and carbamazepine. Talk to your healthcare provider if you are currently using these medications.Talk to your healthcare provider if you use hormonal birth control. Using ella may make your regular hormonal birth control method less effective. After using ella, you should use a reliable barrier method of birth control (such as a condom with spermicide) during any other times that you have sex in that same menstrual cycle.Know the medicines you take. Keep a list of them to show your healthcare provider and pharmacist when you get a new medicine.When is it not appropriate to use ella?o Do not use ella as a regular birth control method. It does not work as well as most other forms of birth control when they are used consistently and correctly.o Do not use ella if you are already pregnant.o Do not use ella more than one time in the same menstrual cycle for different acts of unprotected sex or birth control failure.How does ella work?ella is thought to work for emergency contraception primarily by stopping or delaying the release of an egg from the ovary. It is possible that ella may also work by preventing attachment (implantation) to the uterus.How should I take ella:o Take ella as soon as possible within 5 days (120 hours) after unprotected sex or if you had a birth control failure.。
妇女与癫痫 周列民_妥泰
抗癫痫药物治疗时需特别考虑的情况 • 与口服避孕药的相互作用
• • • • • • 月经 生育 妊娠 哺乳 体重引起的健康危害 骨代谢
妇女与癫痫
Reported by Elinor Ben-Menacham
抗癫痫药物治疗时需特别考虑的情况
Oral contraceptive Interactions 与口服避孕药的相互作用
妇女与癫痫
Reported by Elinor Ben-Menacham
抗癫痫药物治疗时需特别考虑的情况
• 与口服避孕药的相互作用 • 月经 • 生育
• 妊娠(Pregnancy)
• 哺乳 • 体重引起的健康危害 • 骨代谢
妇女与癫痫
Pregnancy and Risks of Epilepsy
妇女与癫痫
Reported by Elinor Ben-Menacham
Pregnancy and Risks of Epilepsy
癫痫对妊娠的影响 • 孕妇风险:恶心、呕吐--药物吸收,血药浓度;不适 当的换药或睡眠剥夺均可导致发作增加。 妊娠并发症如阴道出血、流产、早产、难产 及妊高症的机率增加 • 胎儿风险:因母亲GTCS或持续状态导致胎儿宫内窒息、 死胎、低出生体重儿。新生儿畸形率增加: (5-8%,正常人群2-4%),主要原因与癫痫发作 及服用AEDs有关
与口服避孕药的相互作用
Topiramate: Effect on Oral Contraceptive Hormones
Estradiol Progestin
* * **
*p<0.05 -80 **p<0.0005
50mgTPM 100mgTPM 200mgTPM 200mgTPM 400mgTPM 800mgTPM
药品说明书英语作文
药品说明书英语作文English: A drug information leaflet provides important details abouta medication, including its uses, dosages, side effects, and precautions. It is important for patients to carefully read and follow the information provided in the leaflet to ensure safe and effective use of the medication. The leaflet usually contains information on how to take the medication, such as the recommended dosage, frequency, and duration of treatment. It also outlines possible side effects that may occur and advises patients on what to do if they experience any of them. Precautions and warnings are also includedto inform patients of potential risks and how to avoid them. Overall, the drug information leaflet serves as a valuable resource for patients to understand their medication and how to use it properly.Translated content: 药品说明书提供了关于药物的重要信息,包括其用途、剂量、副作用和注意事项。
多巴丝肼片日本药品说明书英文
多巴丝肼片日本药品说明书英文Doripenem Tablets: Japanese Medication Guide (English Version)Introduction:Doripenem is a commonly used medication in Japan for the treatment of various bacterial infections. This medication guide aims to provide users with comprehensive information about Doripenem tablets, including usage, dosage, precautions, side effects, and other important details. Please read this guide carefully before using Doripenem and consult your healthcare professional if you have any questions or concerns.Product Overview:- Name: Doripenem Tablets- Active Ingredient: Doripenem- Strength: 250 mg, 500 mg- Dosage Form: Tablets- Manufacturer: [Name of Manufacturer]- Approved by: [Name of Regulatory Authority]Usage:Doripenem is indicated for the treatment of the following infections caused by susceptible bacteria:- Community-acquired pneumonia- Hospital-acquired pneumonia- Complicated urinary tract infections, including pyelonephritis- Complicated intra-abdominal infections- Septicemia (bloodstream infections)- Febrile neutropenia (fever due to low white blood cell count)Dosage and Administration:- The recommended dosage for adults is [Dosage]. Please follow the instructions provided by your healthcare professional.- Doripenem tablets should be taken [Instructions on how to take the tablets, e.g., with or without food, with water].- The duration of treatment may vary depending on the type and severity of the infection. Please consult your healthcare professional for the recommended duration.Precautions:- Before using Doripenem, inform your healthcare professional about any allergies, medical conditions, or medications you are currently taking.- It is important to complete the full course of Doripenem treatment as prescribed by your healthcare professional, even if you start feeling better.- Do not share Doripenem tablets with others or use leftover medication for future infections.- Driving or operating machinery while under the influence of Doripenem may impair your abilities. Use caution until you know how Doripenem affects you.Side Effects:Doripenem may cause side effects in some individuals. Common side effects include:- Nausea- Diarrhea- Headache- Rash- Injection site reactions (if administered intravenously)If you experience severe or persistent side effects, contact your healthcare professional immediately. They will assess the risks and benefits of continuing Doripenem treatment.Storage:- Store Doripenem tablets at room temperature (between [temperature range]) in a dry place.- Keep the medication out of reach of children and pets.- Do not use Doripenem tablets beyond the expiration date mentioned on the packaging.Additional Information:- Doripenem may interact with certain medications. Inform your healthcare professional about all the medications you are taking to avoid potential drug interactions.- In case of an overdose, seek medical attention immediately or contact your local poison control center.- If you miss a dose of Doripenem, take it as soon as you remember. However, if it is close to the time for your next dose, skip the missed dose and continue with your regular dosing schedule.Conclusion:This medication guide provides essential information about Doripenem tablets, their proper usage, dosage, precautions, and potential side effects. It is crucial to consult with your healthcare professional and follow their instructions for the safe and effective use of Doripenem. If you have any additional questions or concerns, seek medical advice for further assistance.。
加拿大修改羟基脲产品说明以增加间质性肺疾病的风险提示
©in国药勿评inCHINESE JOURNAL OF DRUG EVALUATION2020年第37卷第3期[21]Shafrin J,Sididce V,Shrestha A,et aL MethoPolooicel assessment oI matc-hind-apjustea indireci comparisods:Case stuUy application to attentiop血匚cit/hyperactivity disorCes(ADHD)[J].Value in Health,2013,17:7. [22]Alsop JC,Reenies SA,Wrighi JJ.A dovel IPC approach:Matchina patientlevel data to stuUy-level summarc meads and vakadces]J].Value in Health,2013,13:7.[23]Beleer M,Bmanic A,Kanziola Z,et aL Altematiw weighting approachesfor matchina adjustee indirect compaCsods(MAIP)[J].Value in Health, 2015,18:3.[24]Thom H,Jugl SM,Nidoelou E,et aL Matchina-anjusten indirect comparl-sods to assess comparatiw edectiveness:A systematic review oI appUcatWd in scieatific literature and health techdolooy appraisals[J].Value in Health, 2017,20:5.[20]Phillippo DM,Ades AE,Dias S,et at.Methods for Podulatiod-Ndjusten山-direct Comparisods in Health Techdolooy Appraisat[J].Meaicat decisiod maiiny,2013,38::[22]Alsop J,Podt L,ScoO M,et at.Which matchina anjustea indirect comparl-sop method is b est]J].Idt e Techdot Assess,2017,37,(Sup1):94-95.[27]Care JJ,IshaP KJ.No dead-to-9ead triat?Simulate the missing arms[J].Pharmacoecodomics,2017,28(10):957-967.[28]Pmsaomvsay I,Benenict A,LarOin JMG,et at. Axitinid(AXI)and bestsupportive care(BSC)in the Weatwent oI shnitinin-refractom patients with metastatic mnat celt carcidoma(MRCC):Results oI a simulates Weatwent comparisod(STC)analyses[J].Value in Health,2017,15门.[22]Batsod S,Mitchelt SA,Kiny D.The use and acceptadce oI dovet statisticetanalyses te suppoe techdolooy suUmissiods te HTA anthorities[J].Value in Health,2014,17卩.[30]IshaP KJ,Raet M,PhataP H,et at.Simulaten treatmedt compaPsod oI tide-to nevedt(and at U vs non-linear)outcomes[J].Value in Health,2015,[31]ShuUla P,Sharma A,Sindiqul MK.A comparisod ot patiedt levet data(IPD)revressiod techniques in aPjustina foe cross tWat in ad indl-rect Weatwedt comparisod(IPC):A worOeV example ot simulateV Weatwedt comparisod(STC)v s bayesiad IPD revressiod[J].Value in Health,2013, 21:S228.[32]Dodeaad S,Williamsod P,D'Alessandro U,et at.Assessina the001181816X00assemptiod by exploriny treatwent by covariate interactions in mixed treatment comparisod meta-analysis:indmiduat patiext-levet coveriates versus aa-yregate tCal-levet covariates[J].Stat Med,2017,31(29):3344-3857. [33]Saramayo P,Suttod AJ,C oopcs NJ,et at.Mixed treatment comparisons p-siny agyrepate and indivinuat participadt levet data[J].Stat Med,2012,31(28):3516-3536.[34]Donepad S,Williamson P,DAlessandro U,et bininy indivinuat patient data and agyrepate data in mixed treatment comparison meta-analysis:Indivinuat patient data may be beneficiat if only for a subset ot tWats t J].Stat Med,2013,32(6):914-930.[35]Saramayo P,Chuany LH,Soares corO meta-analysis of(indivinuatpatient)tirne te event data alonyside(agyrepate)connt data]J].BMC Med Res Methodot,2014,14:105.[36]Freeman S,Caroenter J,Tiernep J.Ode-step indivinuat patient data(PD)networO meta-analysis of survival data usiny mysWu-parmar modets[J].Teals,2015,16(Sup2):161.[了]Thom HH,CapUun G,Cemltl A,et corO meta-analysis combininy inUividuat patient and agyrevate data from a mixture of stuUy desians with an application te pulmonare aeeeal dypenedsiou[J].BMC Med Res Methodot, 2015,15:34.[33]Dapne GA,Brown CH,Howe G,et at.Testiny moderation in detworO metaanalysis with inUividuat23001X30)data[J].Stat Med,2016,35(15):2485-2502.[39]Nonnand SL,SpeCus J,Homitz-Lendon worO meta-analysis cP causatdose-msponse relationsUips usiny individuat paCWipant triat data[J].3X100-icat PsychiaWa,201.,81(Supl6):S34-S35.[44]Freeman SC,FisUer D,Tiernep JF,et al.A frameworO for identifyiny treat-ment-covariate interactions in individual paeWipant data networO meta-analy-sis[J].Res Synth Methods,2018,5(3):393207.[41]Dedray TPA,Schuit E,Efthimiou O,Reitsma JJ,et at.An overview cPmethods foe networO meta-analysis usiny indmiduat paeWipant data:when do benefits aese[J].Stat Methods Med Res,2015,27(5):1351-1364.(收稿日期:2020-05-05)・警戒与通报・加拿大修改羟基腺产品说明以增加间质性肺疾病的风险提示加拿大卫生部(Health Canada)在2020年4月的Health ProPuct Info W atch中发布了羟基月尿(hyPmxypma,商品名Hypma)的产品说明更新信息,在“警告、药品不良反应和消费者信息”部分增加间质性肺疾病的风险提示。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Number序号Hanyu Pinyin汉语拼音Chinese Name中文名Latin name拉丁名Main side effects/主要副作用Contraindications/Cautions/禁忌症/使用注意
1Awei阿魏RESINA FERULAE孕妇禁用。Contraindicated in pregnancy.
2BiMaYou蓖麻油OLEUM RICINI
忌与脂溶性驱肠虫药同用。孕妇忌服。Do not consume with
lipophilic anthelmintics. Contraindication in pregnancy.
3BingPian冰片BORNEOLUM SYNTHETICUM孕妇慎用。Use with caution in pregnancy.
4ChuanNiuXi川牛膝RADIX CYATHULAE孕妇慎用。Use with caution in pregnancy.
5DaHuang大黄RADIX ET RHIZOMA RHEIMay cause nausea, vomiting and cramp-like discomfort of the gastrointestinal tract; long-term use may lead to electrolyte disturbances and aggravation of constipation with dependency.
可能引起恶心、呕吐、腹痛等症状;长期服用可能会引起电解质紊乱及产生依赖性便秘。
Use with caution in pregnancy, lactation, menstruation, children and undiagnosed abdominal symptoms such as pain, nausea or vomiting.
Use with caution in individuals with cold deficiencies in spleen and stomach or with qi and blood deficiencies.
Avoid prolonged use.孕妇、哺乳期妇女、月经期妇女、儿童以及未确诊的腹痛、恶心、呕吐患者慎用。脾胃虚寒、血虚气弱者慎用。避免长期服用。
6DaQingYan大青盐HALITUM水肿者慎用。Use with caution in individuals with edema.
7Ezhu莪术RHIZOMA CURCUMAE孕妇禁用。Contraindicated in pregnancy.
8FanXieYe番泻叶FOLIUM SENNAE
May cause nausea, vomiting and cramp-like discomfort of the gastrointestinal tract; long-term use may lead to electrolyte disturbances and aggravation of constipation with dependency.
可能引起恶心、呕吐、腹痛等症状;长期服用可能会引起电解质紊乱及产生依赖性便秘。
Use with caution in pregnancy, lactation, menstruation, children and undiagnosed abdominal symptoms such as pain, nausea or vomiting.
Avoid prolonged use.孕妇、哺乳期妇女、月经期妇女、儿童以及未确诊的腹痛、恶心、呕吐患者慎用。避免长期服用。
9FengJiao蜂胶PROPOLIS
过敏体质者慎用。Use with caution in individals of
hypersensitivity.
10GuiZhi桂枝RAMULUS CINNAMOMI孕妇慎用。Use with caution in pregnancy.
11HeiZhongCaoZi黑种草子SEMEN NIGELLAE
孕妇及热性病患者禁用。Contraindicated in pregnancy and
individuals with heat-evil.
12HeShouWu何首乌 (生)RADIX POLYGONI MULTIFLORI (un-
processed)
May cause nausea, vomiting and cramp-like discomfort of the gastrointestinal tract; long-term use may lead to electrolyte disturbances and aggravation of constipation with dependency. May harm the liver in some individuals.可能引起恶心、呕吐、腹痛等症状;长期服用可能会引起电解质紊乱及产生依赖性便秘。个别人偶见肝损伤。Use with caution in pregnancy, lactation, children and undiagnosed abdominal symptoms such as pain, nausea or vomiting.
Use with caution in individuals with loose stool or syndrome of wet phlegm.
Avoid prolonged use.孕妇、哺乳期妇女、儿童以及未确诊的腹痛、恶心、呕吐患者慎用。大便溏泻及有湿痰者慎用。避免长期服用。
13HongHua红花FLOS CARTHAMI孕妇慎用。 Use with caution in pregnancy.
14HongQu红曲MONASCUS PURPUREUS (RED YEAST RICE)May cause muscle problems and gastrointestinal discomforts. May affect liver and kidney functions.可能导致肌肉问题或肠胃不适。可能会影响肝肾功能。Use with caution in pregnancy, lactation, children and adolescents. Avoid concomitant use of lovastatin and other statins.Contraindicated in individuals with liver or kidney impairment.Periodic checks on liver function should be conducted if on prolonged use of the product.
Discontinue usage or consult your physician if you experience muscle ache or weakness.
孕妇、哺乳期妇女、儿童以及青少年慎用。本品不宜与洛伐他汀或其它他汀类药物同时使用。肝肾功能不全者禁用。长期服用请定期检查肝功能。如果肌肉出现酸痛或乏力应停药或咨询医师。
15HuangShuKuiHua黄蜀葵花COROLLIA ABELMOSCHI孕妇慎用。Use with caution in pregnancy.
16HuZhang 虎杖RHIZOMA POLYGONI CUSPIDATI孕妇慎用。Use with caution in pregnancy.
17JueMingZi决明子(草决明)(生)
SEMEN CASSIAE (Un-
processed)
Use with caution in pregnancy, lactation, children and undiagnosed abdominal symptoms such as pain, nausea or vomiting.
Use with caution in individuals with cold deficiencies in spleen and stomach or with loose stool.
Avoid prolonged use.孕妇、哺乳期妇女、儿童以及未确诊的腹痛、恶心、呕吐患者慎用。脾胃虚寒及便溏者慎用。避免长期服用。
18LingXiaoHua凌霄花FLOS CAMPSIS孕妇慎用。 Use with caution in pregnancy.
19LouLu漏芦RADIX PHAPONTICI孕妇慎用。 Use with caution in pregnancy.20Luhui芦荟ALOEMay cause nausea, vomiting and cramp-like discomfort of the gastrointestinal tract; long-term use may lead to electrolyte disturbances and aggravation of constipation with dependency.
可能引起恶心、呕吐、腹痛等症状;长期服用可能会引起电解质紊乱及产生依赖性便秘。
Use with caution in pregnancy, lactation, children and undiagnosed abdominal symptoms such as pain, nausea or vomiting.
Contraindicated in individuals with cold deficiencies in spleen and stomach.
Avoid prolonged use.孕妇、哺乳期妇女、儿童以及未确诊的腹痛、恶心、呕吐患者慎用。脾胃虚寒者禁用。避免长期服用。
21MaHuang麻黄HERBA EPHEDRAE
May cause dizziness, headaches, poor appetite, insomnia, irregular or fast heartbeat and rise in blood pressure.
可能会引起头晕、头痛、食欲不振、失眠、心悸或心律加快以及血压升高。
Use with caution in pregnancy, lactation and individuals with heart diseases, hypertension, glaucoma, diabetes and thyroid diseases.