C3W1L06 supplemental notes
3Adrop test standard
WILLIAMS-SONOMAPACKAGE TEST REPORT Page 1 of 3
C/N (5506)301-0380 WM- La WSH33865 WILLIAMS-SONOMA, INC. LAB NUMBER: (5506)301-0380
151 UNION STREET LAB LOCATION: HONG KONG
SAN FRANCISCO, CA 94111 USA CONCEPT: WS
DIVISION: MAILORDER / RETAIL / E-COMMERCE ATTN: PACKAGING DEPT. (914) BUYER: CARLA DEYKIN Packaging@wsgc.com DATE IN: OCT 31, 2006 C.C.: VILLA WARE – KAREN CARPENTER DATE OUT: NOV 09, 2006 BRADY MARKETING – MEGHAN MOD. LOG IN: /
STORNETTA WORKING DAYS: 7
ADDENDUM DATE: /
OVERALL RATING PASS X FAIL
TESTING FOR Packaged Product Transit Testing – ISTA 3A-Modified (150 pounds or less) WL – 9070 – US/CN
ISTA-1AModified ISTA 1B-Modified ISTA 3A-Modified PALLETIZED OTHER
Product Description: BBQ PIZZA GRILL SKU(s): 6899405 Season: FALL Distribution Lot Quantity: 1 Manufacturer: VILLA WARE Country of Origin: CHINA Product Color: BEIGE STONE AND STAINLESS STEEL Charge Vendor: Yes: XNo: Previously Tested: Yes: XNo: Previous Report No.: (5506)257-0564 Shipped Over-Packaged: Yes: XNo: Package Dimensions (In.): 21”x9.5”x18.625” Package Weight (lbs.): 19.5 lbs. Number of Units Per Master Carton: 1 Number of Units Per Inner Cartons:1 Inner Carton Dimensions: 18.375”x7”x15.625” Addendum Report: Yes: No: X Reason For Addendum: N/L List Each Test Outsourced And The Lab That Performed The Testing (Even If It Was Another MTL-ACTS Lab) NONE
大副批注

1.Steel coil:Coldrolledsteel sheetin coilRemarks:9 coilcoverpartlybroken .Ship'sN/R forqualityandquantityas pershipperandbayuquantally.8 coilslightlyrusty onsurface.6 coilcoverspartlyrusty andedgeprotectorspartlybent.5 coilcoverspartlycrimped.3 coilcoverspartlyband off .2.Hot rolledsteelplate:Remarks:3 P'cspartlyrusty.3.Playwood:Remarks:9 CRT'sone sidecoverpartlybrokeneach.2 CRT'stop sidecoverpartly wetby sweateach.Cause ofdamage:Found instow/found indischaegehandling.Ship isnotresponsibel forquantity,quality,no.of peices,bundlesandbrokencovers,splinting, cutting,di scoloratio ndecay of crts ,post mark not clear. Any wet owing torain or sea water due to before loading exposure to the elements. Oil stain to the cargo due tooil tire of forklift, and any kind of latent deffect of damage. Ship'sN/R for any damage and risk of the cargo due to shipN/Rwere properly and effectivel y lashed and secured under the supervisio n of ship's chief officer/super cargo.4.STEELCARGO: Remarks: All steelcargopartlyrusty priortodischarging.Lot 53B'dlesmild steelflat bars:4 Bu'dlescontent15 pcsbent.Lot 95B'dlesseamiessblacksteel pipe:3 B'dlesstrappingburstcontentloosed.B'dles mild steel flat bar: 3 B'dles content slightly bent.5.SHIP'SREMAR KS:a. All cargoes discharge d as loaded.b. All cargoes completed discharge from ship.c. 8 p'kges shorted in dispute,th e figure should retally onshore. d. Theship isN/R for above shortage.6.SHIP'S REMAR KS:Ship'sN/R for quality and quantity according to shanghai tally,and ship's N/Rdamage of deck cargoes loaded.7.SHIP'S REMAR KS:Ship's remarks as per P &I report.a.All cargos stored on the open yard.b. All cargoes slightly rusty on surface.c. Weight & quality unknown, quantity as per costaco shanghai branch SG 03.8.BULK CARGO: Total cargo loaded based on draft survey=6, 030,000 MT.9.Remarks:2520Bundelsofdeformedbar -partlyrust-stained/spotted onsurfaceprior toloading. 62Bundelsofdeformedbar -somepieceswirepartlybent atedgesection5 logisticsin steel-somebundelssheet pileironstrappingburst andpartlyrustystained.10.Remarks:shipper's load, count and measure:Ship notresponsible for shortofcontent.brokenband,splitting,cutting,erasedmarks, discolouration, foranymoisture,any wetowing torain andsea water,for oiland tiretrack owing toforkliftand anykind ofdamage.29 CRTspartlycover vet& partlycovertorn.2 CRTsone sidecover torneach.9CRTswet bysweat &coverpartly torneach.2CRTs partly band off each.11 .STOWA GE PLAN REMAKS :a. PLS balance cgo 300 mt for adjust trim.b. PLS keep cgo even keel in hold.c. PLS keep ship upright.d. PLS check ship's draft and note C/O in time .12 .SHIP REMAR KS: SHIPPER S,LOAD, COUNT AND MEASUR EMENT:VESSELNOTRESPONSIBLEFORVOLUME, NO.OFPIECESPERBUNDLES/ PACKAGEBROKENBANDS,SPLITTING,CHAFING,DISCOLOURATION, STAINEDCARGOERASEDMARKINGS, WETBY RAINOR ANYOTHERWATER BEFORE LOADIN G, OIL AND TYRE MARKS OWING TO FORKLIF TS MIXEDMARKINGS OFCARGO,ANDANYKIND OFDAMAGEINCLUDINGDUE TOINHERENT VICEOFPROPERTIES OFCARGOANDROUGNHANDLINGBYFORKLIFT/CRANEDRIVERS ANDDETERIORATION OFGOODS. 13. Remarks:Same assurveyordamagereport thisdamagerepotmake bysurveyorship's N/Rthisreport.2 bundles partly rusted on surface prior to loading.3 bundles some pieces were bent at places during loading.4 bundles steel wires were cut off prior to loading14 .Remarks: SHIPPER S/ CHARTE RS LOAD, SECURE & TALLY, AND SHIP'SN/R FOR THE SAME.EACH BUNDLE PARTLY TO MODER ATELY RUSTY AND SCRATC HECD/ CHAFEDON SURFAC E PRIOR TO LOADIN G.36 BUNDLE S STEEL WIRE CUT OFF PRIOR TO LOADIN G.IT WAS RAINY DURING LOADIN G . Weight measure subject to the survey report only.15 .30 CRTS COVER PARTLY STAINED, BROKEN, WET,BUN DLES OFF BEFORE LOADING, SHIP'S N/R FORANY DAMAGE . SHIPPED ON DECK AT SHIPPER' S RISK.ALL CASES NO ANY CHOCKIN G AND LASHING BY STEVEDO RE,SHIP'SN/R FORE ANY DAMAGE .。
2006丙肝治疗(英文)-AGA

American Gastroenterological Association Medical Position Statement on the Management of Hepatitis CH epatitis C accounts for a sizable proportion ofcases of chronic liver disease,liver disease deaths,and cases of hepatocellular carcinoma and rep-resents the most common indication for liver trans-plantation.Projections based on the current preva-lence of infection and anticipated rates of progression suggest that the morbidity and mortality,as well as the medical care costs attributable to hepatitis C virus (HCV)infection,will escalate alarmingly during the next2decades.The substantial clinical and economic impact of hepatitis C focuses attention on the critical need to prevent and control HCV infection.Public health measures,changes in behavior to avoid blood-borne infections,and screening of donated blood and organs for HCV have reduced dramatically the frequency of new infections,and substantial progress has been achieved in antiviral therapy for hepatitis C.Applied effectively,contemporary antiviral therapy can pre-vent chronic infection in almost all persons with acute hepatitis C and can cure chronic liver disease associ-ated with HCV infection in as many as half of patients with compensated,HCV-associated liver disease.In short,hepatitis C is an important public health prob-lem whose consequences can be reduced by appropri-ate application of antiviral therapy.Because the de-mand for management of chronic hepatitis C has increased so considerably over the past decade,the American Gastroenterological Association developed a technical review1and this medical position statement. This medical position statement,which contains practice guidelines intended for physicians,nurse practitioners,physician assistants,and other health care workers who participate in the care of patients with hepatitis C,includes suggestions for preferable approaches to the management of persons with hepa-titis C.These guidelines,which are recommendations intended to assist physicians and other health care workers in arriving at reasoned patient care decisions,2 are designed to beflexible rather than rigidly inflex-ible universally applied“standards of care.”Although these recommendations should be followed in most cases,management decisions are left to the individual physician and health care worker based on the circum-stances of the individual patient.As in previous guide-lines issued by the American Gastroenterological As-sociation,specific recommendations are based on relevant published information.ScreeningRoutine screening of all asymptomatic adults, who have a low prior probability of HCV infection,is not recommended.Among high-risk groups(eg,in-jection drug users,persons who received a transfusion before1992[when donor screening for antibody to HCV was introduced],persons with hemophilia who received clotting factors before1987,persons with frequent percutaneous exposures,immigrants from countries with a high prevalence of HCV infection, and persons with clinical or biochemical evidence for chronic liver disease,even among asymptomatic per-sons),diagnostic testing for HCV infection has been recommended by the US Public Health Service,expert panels,and professional medical specialty societies. Spouses of persons with chronic hepatitis C are also candidates for HCV serologic testing.Persons in whom the diagnosis of hepatitis C is established are candidates for hepatitis A and hepatitis B vaccines.Pretreatment Diagnostic Evaluationof Patients With ChronicHepatitis CPersons with a reactive enzyme immunoassay for antibody to HCV,the presence of HCV RNA,and compensated liver disease are potential candidates for antiviral therapy.Currently,antiviral therapy is not recommended routinely for patients with hepatic de-compensation;patients with a history of severe,un-controlled psychiatric disorder;and/or patients with severe hematologic cytopenias.Elevation of alanine aminotransferase(ALT)and aspartate aminotransferase levels is not a requirement for therapy.All candidates for antiviral therapy should be tested for HCV RNA with a quantitative amplifi-cation assay and should be tested for HCV genotype. Patients in whom antiviral therapy is being considered are candidates for liver biopsy,the gold standard for ©2006by the American Gastroenterological Association0016-5085/06/$32.00doi:10.1053/j.gastro.2005.11.011GASTROENTEROLOGY2006;130:225–230determining histologic grade and stage,unless the po-tential for complications is unacceptably high.For pa-tients with moderate to severefibrosis(Ishak stageՆ3, METAVIR stageՆF2;please see technical review1for histologic scoring systems),antiviral therapy is recom-mended uniformly.For patients with milder histologic disease,progression may be sufficiently slow to justify monitoring without imminent therapeutic intervention in a proportion of these patients(see Treatment Recom-mendations).For patients with genotypes2and3,the likelihood of response is so high that the benefits of treatment may outweigh the importance of histologic considerations;therefore,some authorities forego a base-line liver biopsy in patients with genotypes2and3.Data to support routine ultrasonography for localization of the liver before liver biopsy are insufficient to justify man-dating prebiopsy ultrasonography in all cases and for all practitioners regardless of levels of skill and experience.Treatment of Chronic Hepatitis CThe current standard of care for the treatment of previously untreated patients with chronic hepatitis C is combination pegylated interferon(PEG-IFN)alfa by subcutaneous injection once a week and oral riba-virin daily.For patients with contraindications to ribavirin but who have indications for antiviral ther-apy,PEG-IFN represents the best available treatment. Two PEG-IFN alfa preparations are available:(1) PEG-IFN alfa-2b,administered at a weight-based, 1.5-g/kg dose,and(2)PEG IFN alfa-2a,adminis-tered at afixed,180-g dose.Randomized controlled trials(RCTs)have shown that combination PEG-IFN alfa and ribavirin therapy can achieve a sustained virologic response(SVR)in54%–56%of patients: 42%–52%of patients with genotype1and76%–84% of those with genotypes2and3.Whether one of these PEG-IFN/ribavirin regimens or weight-based modifi-cations of the2regimens will prove to be superior is the subject of ongoing trials.Predictors of response to therapy in these large RCTs are displayed in Table 1. The results of a single,large RCT support a recom-mendation that patients with genotype1require48 weeks of therapy with higher daily doses of ribavirin (1000–1200mg,depending on weightϽ75orՆ75 kg)(some clinicians may wish to adhere to the Food and Drug Administration–approved800mg daily dose of ribavirin when used with PEG-IFN alfa-2b, especially in patients who weighϽ65kg),while patients with the more treatment-favorable genotypes 2and3can be treated for only24weeks and with only 800mg of ribavirin daily.Moreover,12weeks of therapy suffices in patients with genotypes2and3in whom HCV RNA levels are undetectable at week4.In the group of patients with genotypes2and3,patients with genotype2are more likely than those with genotype3to achieve an SVR;for patients with genotype3who have high levels of HCV RNA or advancedfibrosis on liver biopsy,many authorities recommend treatment for48weeks.Pending addi-tional data,in patients with genotypes2and3,cli-nicians may wish to consider higher doses of ribavirin or a longer duration of therapy on an individual basis, taking into account considerations such as high viral level,cirrhosis,or delayed response to therapy.For patients with genotype4,48weeks of treatment with PEG-IFN alfa plus full-dose(1000–1200mg)ribavi-rin is recommended.The potential added benefit of a broader range(800–1400mg)of ribavirin weight-based dosing as part of combination therapy with PEG-IFN is currently being studied.Therapy is indicated for previously untreated pa-tients with chronic hepatitis C,circulating HCV RNA,elevated aminotransferase levels,evidence on liver biopsy of moderate to severe hepatitis grade and stage(METAVIR stageՆF2,Ishak stageՆ3,septal or bridgingfibrosis),and compensated liver disease. Patients with milder histologic changes(META-VIR stage F1,Ishak stageϽ3)(and normal serum aminotransferase activity;see following text)appear to respond as well as patients with more advanced his-tologic changes;such patients can be counseled about the reduced risk of disease progression but still can be offered therapy.If a decision is made to defer therapy in patients with mild disease,periodic laboratory and histologic monitoring should be pursued;however, data to support a recommendation on the frequency of histologic monitoring are wanting.Table1.Predictors of Response to PEG-IFN Plus Ribavirin Therapy in RCTs Conducted in PreviouslyUntreated,Immunocompetent Patients WithCompensated Chronic Hepatitis CNon-genotype1Low HCV RNA levelsAbsence of cirrhosis/bridgingfibrosisDuration of therapy(for genotype1)Age40years or youngerLighter body weightNonblack ethnicityAdherenceAbsence of steatosis on liver biopsyNOTE.Non-genotype1is the most influential predictor of response to standard of care therapy with combination PEG-IFN plus ribavirin.The relative weighting of variables analyzed in RCTs of PEG-IFN/ribavirin combination therapy is presented in the technical review.1226AMERICAN GASTROENTEROLOGICAL ASSOCIATION GASTROENTEROLOGY Vol.130,No.1Current contraindications to therapy include de-compensated cirrhosis(see following text),pregnancy, uncontrolled depression or severe mental illness,ac-tive substance abuse in the absence of concurrent participation in a drug treatment program,advanced cardiac or pulmonary disease,severe cytopenias,poorly controlled diabetes,retinopathy,seizure disorders,im-munosuppressive treatment,autoimmune diseases,or other inadequately controlled comorbid conditions.Monitoring Response to Antiviral TherapyBaseline and12-week monitoring of HCV RNA levels should be performed with the same quan-titative amplification assay.An early virologic re-sponse(EVR),defined as aՆ2-log10reduction in HCV RNA levels during thefirst12weeks of therapy, is a valuable clinical milestone.In the absence of an EVR,the likelihood of an SVR is0–3%.If the only goal of therapy is to achieve an SVR,therapy can be discontinued after12weeks if an EVR is not achieved. Potentially,histologic benefit can accrue even in the absence of an SVR;therefore,some authorities treat beyond12weeks even in patients who have not achieved an EVR.For documentation of a virologic response at the end of therapy(end-of-treatment re-sponse)or an SVRՆ6months after completing ther-apy,a more sensitive quantitative assay with a lower limit ofՅ50IU/mL,if available,or a qualitative HCV RNA assay is recommended.Clinical and virologic monitoring during therapy should be conducted at intervals ranging from once a month to once every3months.Frequent hematologic monitoring is necessary to identify marked anemia,neu-tropenia,and thrombocytopenia;monitoring of thyroid-stimulating hormone level is indicated to identify hypo-thyroidism or hyperthyroidism.Management of Side Effects of AntiviralTherapySide effects of antiviral therapy are listed in Table 2.Flu-like side effects of IFN can be managed with acetaminophen or nonsteroidal anti-inflammatory drugs,sleep-promoting agents can be used for insom-nia,and antidepressants can be used for depression. For management of neutropenia,dose reduction suf-fices,and the addition of granulocyte colony-stimu-lating factor is generally not recommended,although it may be considered in individual cases of severe neutropenia.Ribavirin is contraindicated in pregnancy,necessi-tating strict precautions and contraception in women of childbearing age and their sexual partners and in HCV-infected men with female partners of childbear-ing age.Treatment with ribavirin should be avoided in patients with ischemic cardiovascular and cerebro-vascular disease and in patients with renal insuffi-ciency.If anemia occurs,options include ribavirin dose reduction or the addition of erythropoietin.Approach to Other Patient PopulationsNormal aminotransferase activity.Patients with persistently normal ALT levels generally do not progress histologically,while responses to combina-tion antiviral therapy in patients with normal ALT levels are indistinguishable from response rates in patients with elevated ALT activity.Patients with normal ALT activity are candidates for antiviral ther-apy or for monitoring without intervention,as deter-mined on an individual basis and as influenced by patient factors such as motivation,genotype,histo-logic activity,andfibrosis.Cirrhosis.Patients with compensated cirrhosis who can tolerate therapy are candidates for treatment. In patients with decompensated cirrhosis,antiviral therapy is not recommended;instead,referral for liver transplantation is indicated.Although patients with decompensated cirrhosis are not routine candidates for Table2.Side Effects of Antiviral TherapyRelated to IFNFlu-like symptomsMarrow suppression(especially leukopenia andthrombocytopenia)Emotional effects(irritability,difficulty concentrating,memorydisturbances,depression)Autoimmune disorders(especially thyroiditis)Hair lossRashDiarrheaSleep disordersVisual disorders(rarely retinal hemorrhages,especially in diabetic patients and hypertensive patients)Weight lossSeizuresHearing lossPancreatitisInterstitial pneumonitisInjection site reactionsRelated to ribavirinHemolytic anemiaChest congestion,dry cough,and dyspneaPruritusSinus disordersRashGoutNauseaDiarrheaTeratogenicityJanuary2006AMERICAN GASTROENTEROLOGICAL ASSOCIATION227IFN-based antiviral therapy,attempts to eradicate hepatitis C viremia with progressively escalated,low-dose antiviral therapy before transplantation have met with limited,early success;however,data supporting this approach are insufficient to justify its adoption outside of clinical trials conducted at established cen-ters by experienced investigators.Previous relapsers and nonresponders.Patients in whom HCV RNA is undetectable during and at the end of therapy but reappears again after completion of therapy(relapsers)are likely to respond and experience a relapse again with a subsequent course of the same therapy.The chance of achieving an SVR in relapsers, however,may be as high as40%–50%if re-treatment is pursued with more effective therapy.If this group of patients is to be re-treated,ideally,a different,more effective regimen should be used.Therapy with PEG-IFN and ribavirin should be strongly considered for patients who experienced a relapse after a course of standard IFN/ribavirin combination therapy,while a longer duration of therapy in patients who experienced a relapse after12months of treatment with PEG-IFN plus ribavirin is of unproven efficacy.For nonresponders to a previous course of standard IFN monotherapy,re-treatment with PEG-IFN plus ribavirin can increase the frequency of responsiveness to approximately20%;for nonresponders to a previ-ous course of standard IFN plus ribavirin,re-treat-ment with PEG-IFN plus ribavirin can increase the frequency of responsiveness to approximately10%. Expectations for responsiveness to re-treatment are lower in patients with genotype1,cirrhosis,high baseline HCV RNA levels,and black ethnicity.Such factors,in addition to a patient’s tolerance to previous therapy and severity of underlying liver disease, should be taken into consideration when making in-dividualized decisions about the re-treatment of prior nonresponders.Given the difficulty of clearing hepatitis C viremia, nonresponder patients have been considered as candi-dates for long-term maintenance therapy.Hypotheti-cally,maintenance IFN alfa therapy in prior nonre-sponders might retard the progression offibrosis and limit the progression of cirrhosis to end-stage liver disease and hepatocellular carcinoma.Therefore,sev-eral large,multicenter RCTs of long-term(2–4years) therapy with low-dose PEG-IFN are in progress to assess the effect of maintenance therapy on histologic and clinical end points in patients with chronic hep-atitis C and advancedfibrosis.The results of these trials will be required before recommendations can be made for chronic maintenance therapy in those with advanced histologicfibrosis who fail to achieve an SVR.Acute hepatitis C.The risk of HCV infection after an accidental needlestick is sufficiently low to delay antiviral therapy until HCV infection is docu-mented virologically and biochemically.Patients with acute hepatitis C are candidates for antiviral therapy after a period of observation to allow for potential spontaneous clearance.Case series have focused pri-marily on IFN or PEG-IFN monotherapy adminis-tered for12–24weeks.Although combination IFN or PEG-IFN/ribavirin has not been shown to be superior to IFN monotherapy,conventional doses of PEG-IFN/ ribavirin combination therapy may represent a reason-able approach to treatment of patients with acute hepatitis C.In fact,the optimal regimen,dose,time to initiate therapy,duration of therapy,or benefit of adding ribavirin to IFN therapy has not been estab-lished,and the infrequency of acute hepatitis C will likely confound the prospective comparison of differ-ent treatment regimens.Based on available data,most authorities would initiate treatment no later than2–3 months after presentation with acute hepatitis and would extend therapy for at least24weeks.Injection drug or alcohol use.Therapy is recom-mended for recovered drug users,including those on methadone maintenance,and,based on a case-by-case review,for active drug users,especially when in con-junction with drug treatment programs.Additional randomized trials will be required to evaluate the following:the safest and most effective treatment regimens;the levels of and factors favoring compli-ance;the risk of recidivism;side effect profiles,in-cluding the risk of depression;and the effect of anti-viral therapy on methadone requirements. Abstinence should be recommended before and during antiviral treatment in alcoholic persons,and treatment of alcohol abuse should be linked with efforts to treat hepatitis C in alcoholic patients.A safe level of alcohol consumption in patients with hepatitis C has not been established.Hematologic disorders.The therapeutic ap-proach in this group of patients may depend on the underlying hematologic disorder.For example,in thalassemic patients,primary therapy should be fo-cused on reducing iron overload.Chronic hepatitis C may be treated with PEG-IFN plus ribavirin,al-though data supporting the safety and efficacy of ribavirin,at full or reduced doses,in these populations are limited,because registration trials of PEG-IFN plus ribavirin excluded patients with these disorders specifically.In patients with a genetic predisposition228AMERICAN GASTROENTEROLOGICAL ASSOCIATION GASTROENTEROLOGY Vol.130,No.1to anemia,ribavirin-associated hemolysis would be predicted to be more severe,transfusion requirements may increase during antiviral therapy,and data pro-viding guidelines for ribavirin dosing are unavail-able.Treatment guidelines for hemophiliac patients are the same as those in the nonhemophiliac popula-tion.The risk of pretreatment liver biopsy is higher but can be minimized by coordination with hemato-logic expertise.Children.For children,the general principles of management are the same as those for adults,except that treatment is not recommended for children younger than 3years.End-stage renal disease.Currently,ribavirin is contraindicated in patients with renal failure;how-ever,clinical trials are in progress to assess the safety and efficacy of low-dose ribavirin combined with PEG-IFN.At present,the role of antiviral therapy in patients with end-stage renal disease remains unde-fined.For individual patients,the potential benefit of therapy should be weighed against the higher risk of toxicity,and treatment should be undertaken in cen-ters with experienced clinicians,ideally in clinical trials.For PEG-IFN alfa-2a,a dose reduction from 180to135g is recommended by the manufacturer for patients with renal failure;for PEG-IFN alfa-2b, the manufacturer makes no specific recommendation about dose reduction for patients with renal failure, but50%dose reductions are recommended for other clinical indications(eg,hematologic).Patients with end-stage renal disease and chronic hepatitis C who are candidates for kidney transplantation should be evaluated for advanced hepaticfibrosis,which is asso-ciated with reduced graft and patient survival.Extrahepatic disease.In patients with cutaneous vasculitis and glomerulonephritis resulting from HCV-associated mixed essential cryoglobulinemia,indefinite maintenance therapy may be required.Hepatitis C–as-sociated B-cell lymphoma may respond to antiviral therapy.Human immunodeficiency virus and HCV coinfec-tion.All patients with human immunodeficiency virus (HIV)infection should be screened for HCV infection; among those with HCV infection,evaluation of candi-dacy for antiviral therapy should be undertaken(includ-ing liver biopsy).Ideally,the HIV infection should be well controlled with antiretroviral therapy before treat-ment of the HCV infection is initiated.Optimal therapy consists of PEG-IFN alfa at the routine weekly dose plus ribavirin at a daily dose of600–800mg(higher if tolerated)for48weeks,regardless of genotype.Because of potential drug-drug interactions in patients on HIV treatment regimens that include didanosine,HIV regi-mens should be altered in those starting combination therapy for HCV infection.If didanosine is critical to the HIV regimen,ribavirin should be avoided.Liver transplantation.Results of antiviral therapy for hepatitis C after liver transplantation have been dis-appointing,and results of clinical trials are mixed at best. Whether begun prophylactically immediately after transplantation to prevent reinfection or initiated to treat established posttransplantation hepatitis C,antiviral therapy,even with combination PEG-IFN alfa and riba-virin,may suppress HCV replication but results in an SVR inϽ20%of treated patients.Moreover,IFN,PEG-IFN,and ribavirin have not been well tolerated after liver transplantation,necessitating dose reductions for adverse events such as anemia and serious infections.Therefore, after liver transplantation,the risks and benefits of anti-viral therapy should be weighed carefully for each pa-tient,and treatment should be initiated with caution by transplantation teams experienced in the treatment of hepatitis C.Because immunosuppression increases HCV replication,which is associated with increased HCV-associated liver injury and may contribute to disease progression,doses of immunosuppressive drugs should be kept to a minimum in patients who undergo liver transplantation for chronic hepatitis C.Other TherapiesClinical trials have failed to demonstrate the ef-ficacy of phlebotomy,amantadine,IFN gamma,inter-leukin-10,or thymosin␣-1in patients with chronic HCV infection,although additional trials for some of these agents are continuing.IFN beta offers no advantage over IFN alfa and is not approved for the treatment of hepatitis C.Currently,none of these can be recom-mended.Similarly,alternative and complementary ther-apies have not been proven to be effective in clinical trials and are not recommended.JULES L.DIENSTAGJ.G.McHUTCHISONReferences1.Dienstag JL,McHutchison JG.American Gastroenterological Asso-ciation technical review on the management of hepatitis C.Gas-troenterology2005;129.2.American Gastroenterological Association.Position and policystatement:policy statement on the use of medical practice guide-lines by managed care organizations and insurance carriers.Gas-troenterology1995;108:925–926.Address requests for reprints to:Chair,Clinical Practice and Eco-nomics Committee,AGA National Office,c/o Membership Depart-January2006AMERICAN GASTROENTEROLOGICAL ASSOCIATION229ment,4930Del Ray Avenue,Bethesda,Maryland20814.Fax:(301) 654-5920.The Medical Position Statements(MPS)developed under the aegis of the American Gastroenterological Association(AGA)and its Clinical Practice and Economics Committee(CPEC)were approved by the AGA Governing Board.The data used to formulate these recommendations are derived from the data available at the time of their creation and may be supplemented and updated as new information is assimilated. These recommendations are intended for adult patients,with the intent of suggesting preferred approaches to specific medical issues or problems.They are based upon the interpretation and assimilation of scientifically valid research,derived from a comprehensive review of published literature.Ideally,the intent is to provide evidence based upon prospective,randomized placebo-controlled trials;however, when this is not possible,the use of experts’consensus may occur.The recommendations are intended to apply to health care providers of all specialties.It is important to stress that these recommendations should not be construed as a standard of care.The AGA stresses that thefinal decision regarding the care of the patient should be made by the physician with a focus on all aspects of the patient’s current medical situation.This document presents the official recommendations of the Amer-ican Gastroenterological Association(AGA)on“Management of Hep-atitis C.”It was approved by the Clinical Practice and Economics Committee on September17,2005,and by the AGA Governing Board on November6,2005.230AMERICAN GASTROENTEROLOGICAL ASSOCIATION GASTROENTEROLOGY Vol.130,No.1。
MBT3906DW1T1G中文资料
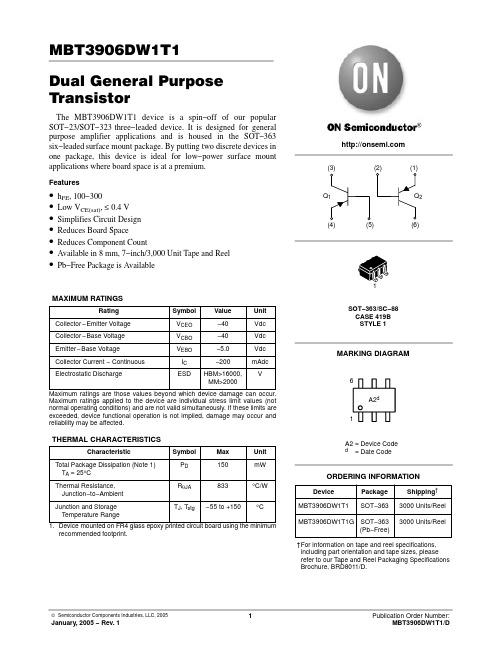
MBT3906DW1T1Dual General Purpose TransistorThe MBT3906DW1T1 device is a spin−off of our popular SOT−23/SOT−323 three−leaded device. It is designed for general purpose amplifier applications and is housed in the SOT−363six−leaded surface mount package. By putting two discrete devices in one package, this device is ideal for low−power surface mount applications where board space is at a premium.Features•h FE , 100−300•Low V CE(sat), ≤ 0.4 V •Simplifies Circuit Design •Reduces Board Space•Reduces Component Count•Available in 8 mm, 7−inch/3,000 Unit Tape and Reel •Pb−Free Package is AvailableMAXIMUM RATINGSMaximum ratings applied to the device are individual stress limit values (not normal operating conditions) and are not valid simultaneously. If these limits are exceeded, device functional operation is not implied, damage may occur and reliability may be affected.THERMAL CHARACTERISTICSrecommended footprint.Device Package Shipping †ORDERING INFORMATIONMBT3906DW1T1SOT−3633000 Units/Reel MBT3906DW1T1GSOT−363(Pb−Free)3000 Units/Reel†For information on tape and reel specifications,including part orientation and tape sizes, please refer to our T ape and Reel Packaging Specifications Brochure, BRD8011/D.ELECTRICAL CHARACTERISTICS (T A = 25°C unless otherwise noted)OFF CHARACTERISTICSON CHARACTERISTICS (Note 2)SMALL−SIGNAL CHARACTERISTICSELECTRICAL CHARACTERISTICS (T= 25°C unless otherwise noted) (Continued)SWITCHING CHARACTERISTICSFigure 1. Delay and Rise TimeEquivalent Test Circuit Figure 2. Storage and Fall TimeEquivalent Test Circuit10 < t 1 < 500 * T otal shunt capacitance of test jig and connectorsTYPICAL TRANSIENT CHARACTERISTICSFigure 3. CapacitanceREVERSE BIAS (VOLTS)2.03.05.07.0101.00.1Figure 4. Charge DataI C , COLLECTOR CURRENT (mA)1.02.03.05.07.01020305070100200C A P A C I T A N C E (p F )1.02.03.0 5.07.010200.20.30.50.7T J = 25°C T J = 125°CFigure 5. Turn−On Time I C , COLLECTOR CURRENT (mA)7010020030050050T I M E (n s )1.02.03.01020705100Figure 6. Fall TimeI C , COLLECTOR CURRENT (mA)5.07.0305020010307201.02.03.010*******5.07.03050200TYPICAL AUDIO SMALL−SIGNAL CHARACTERISTICSNOISE FIGURE VARIATIONS(V CE = −5.0 Vdc, T A = 25°C, Bandwidth = 1.0 Hz)Figure 7. f, FREQUENCY (kHz)2.03.04.05.01.00.1Figure 8.R g , SOURCE RESISTANCE (k OHMS)N F , N O I S E F I G U R E (d B )1.02.0 4.01020400.20.401000.1 1.0 2.0 4.01020400.20.4100h PARAMETERS(V CE = −10 Vdc, f = 1.0 kHz, T A = 25°C)Figure 9. Current GainI C , COLLECTOR CURRENT (mA)7010020030050Figure 10. Output AdmittanceI C , COLLECTOR CURRENT (mA)h , D C C U R R E N T G A I Nh , O U T P U T A D M I T T A N C E ( m h o s )Figure 11. Input Impedance I C , COLLECTOR CURRENT (mA)Figure 12. Voltage Feedback RatioI C , COLLECTOR CURRENT (mA)301005010202.03.05.07.0101.00.10.21.02.0 5.00.5100.30.5 3.00.72.05.010201.00.20.5o e h , I N P U T I M P E D A N C E (k O H M S )i e 0.10.21.02.0 5.0100.30.5 3.00.10.21.02.0 5.0100.30.5 3.0750.10.21.02.0 5.0100.30.5 3.0f e m 70300.77.00.77.07.03.00.70.30.77.00.77.0h , V O L T A G E F E E D B A C K R A T I O (x 10 )r e −4TYPICAL STATIC CHARACTERISTICSFigure 13. DC Current GainI C , COLLECTOR CURRENT (mA)0.30.50.71.02.00.20.1h , D C C U R R E N T G A I N (N O R M A L I Z E D )0.5 2.0 3.01050700.20.30.11001.00.720030205.07.0F EFigure 14. Collector Saturation RegionI B , BASE CURRENT (mA)0.40.60.81.00.20.1V , C O L L E C T O R E M I T T E R V O L T A G E (V O L T S )0.5 2.0 3.0100.20.301.00.7 5.07.0CE0.070.050.030.020.01Figure 15. “ON” Voltages I C , COLLECTOR CURRENT (mA)0.40.60.81.00.2Figure 16. Temperature CoefficientsI C , COLLECTOR CURRENT (mA)V , V O L T A G E (V O L T S )− 0.500.51.0− 1.0− 1.5− 2.0, T E M P E R A T U R E C O E F F I C I E N T S (m V / C )°V qPACKAGE DIMENSIONSSOT−363/SC−88CASE 419B−02ISSUE UNOTES:1.DIMENSIONING AND TOLERANCING PER ANSI Y14.5M, 1982.2.CONTROLLING DIMENSION: INCH.3.419B−01 OBSOLETE, NEW STANDARD 419B−02.DIMA MIN MAX MIN MAX MILLIMETERS 1.80 2.200.0710.087INCHESB 1.15 1.350.0450.053C 0.80 1.100.0310.043D 0.100.300.0040.012G 0.65 BSC 0.026 BSC H −−−0.10−−−0.004J 0.100.250.0040.010K 0.100.300.0040.012N 0.20 REF 0.008 REF S2.00 2.200.0790.087STYLE 1:PIN 1.EMITTER 22.BASE 23.COLLECTOR 14.EMITTER 15.BASE 16.COLLECTOR 2*For additional information on our Pb−Free strategy and solderingdetails, please download the ON Semiconductor Soldering and Mounting Techniques Reference Manual, SOLDERRM/D.SOLDERING FOOTPRINT*ON Semiconductor and are registered trademarks of Semiconductor Components Industries, LLC (SCILLC). SCILLC reserves the right to make changes without further notice to any products herein. SCILLC makes no warranty, representation or guarantee regarding the suitability of its products for any particular purpose, nor does SCILLC assume any liability arising out of the application or use of any product or circuit, and specifically disclaims any and all liability, including without limitation special, consequential or incidental damages.“Typical” parameters which may be provided in SCILLC data sheets and/or specifications can and do vary in different applications and actual performance may vary over time. All operating parameters, including “Typicals” must be validated for each customer application by customer’s technical experts. SCILLC does not convey any license under its patent rights nor the rights of others. SCILLC products are not designed, intended, or authorized for use as components in systems intended for surgical implant into the body, or other applications intended to support or sustain life, or for any other application in which the failure of the SCILLC product could create a situation where personal injury or death may occur. Should Buyer purchase or use SCILLC products for any such unintended or unauthorized application, Buyer shall indemnify and hold SCILLC and its officers, employees, subsidiaries, affiliates,and distributors harmless against all claims, costs, damages, and expenses, and reasonable attorney fees arising out of, directly or indirectly, any claim of personal injury or death associated with such unintended or unauthorized use, even if such claim alleges that SCILLC was negligent regarding the design or manufacture of the part. SCILLC is an Equal Opportunity/Affirmative Action Employer. This literature is subject to all applicable copyright laws and is not for resale in any manner.PUBLICATION ORDERING INFORMATION。
剑桥雅思6第一套听力Section3真题+解析

剑桥雅思6第一套听力Section3真题+解析剑桥雅思6第一套听力Section 3真题+ 解析***** 3 Questions 21-30Question 21Choose the correct letter, A, B or C.21 What is Brian going to do before the course starts?A attend a classB write a reportC read a bookQuestions 22-25Complete the table below.Write NO MORE THAN TWO WORDS for each answer.Questions 26-30Complete the summary below.Write NO MORE THAN TWO WORDS for each answer.Business CentreThe Business Resource Centre contains materials such as books and manuals to be used for training. It is possible to hire26................... and27................... .There are materials for working on study skills(e.g.28................... ) and other subjects include finance and29...................30................... membership costs £50 per year.题型:选择,表格填空,句子填空考查技能:听出具体信息场景:课程咨询场景背景介绍学校经常会接到很多关于课程设置、课程内容及学校周边环境和设施的咨询电话。
双重显示万用表 (U3402A)

CAT II 300 V
等电位
IEC 测量类别 II。在 II 类过电压条 件下,输入端子可以连接到主电 路 (最高可达 300 VAC)。
设备由双重绝缘或加强绝缘保护
Keysight U3402A 用户及维修指南
3
一般安全信息
在此仪器的操作、维修和修理各个阶段中,必须遵循下面的一般安全预防措施。 如果未遵循这些预防措施或本手册其他部分说明的特定警告,则会违反有关仪器 的设计、制造和用途方面的安全标准。Keysight Technologies 对用户不遵守这些 预防措施的行为不承担任何责任。
– 请勿更换部件或修改仪器,以避免引发其他危险。将仪器返回至 Keysight 技术销售与维修处进行维修,以确保功能部件安全。
– 请勿操作已损坏的仪器,因为仪器中内置的安全保护功能部件可能已损坏 (物理损坏、过于潮湿或者任何其他原因)。这时候请断开电源并且只有在 经过维修培训的人员证实操作安全后才使用本仪器。如果需要,请将仪器返 回至 Keysight 技术销售与维修处进行维修以确保安全功能部件工作正常。
CSA 标记是加拿大标准协会的注 册商标。
RCM 标记是 Spectrum Management Agency of Australia 的注册商标。它 表示符合根据 1992 年的《无线通 信法案》的条款制订的 Australia EMC Framework 规定。
此仪器符合 WEEE 指令 (2002/96/EC) 标记要求。此附加产品标签说明 不得将此电气/电子产品丢弃在 家庭垃圾中。
切勿丢弃在家庭垃圾中。 要退还不需要的仪器,请与您最近的 Keysight 服务中心联系,或访问 /en/companyinfo/environment/takeback.shtml 了 解 详 细信息。
三星电容命名规则
●3 CAPACITANCE TEMPERATURE CHARACTERISTICS
▶ CLASS Ⅰ(Temperature Compensation)
Symbol
C P R S T U L
EIA Code
C0G(CH) P2H R2H S2H T2H U2J S2L
Temperature Coefficient(PPM/℃)
Multilayer Ceramic Capacitor
Multilayer Ceramic Capacitor
■ INTRODUCTION
MLCC(Multilayer Ceramic Capacitor) is SMD(Surface Mounted Device) type capacitor that is used in wide ranges of capacitance. MLCC is paid more attentions than other capacitors due to the better frequency characteristics, higher reliability, higher withstanding voltage and so on. MLCC is made of many layers of ceramic and inner electrodes like sandwich. Pd was used for inner electrodes. But the price of Pd was skyrocketed and Pd was replaced by the BME(Base Metal Electrode), which reduced the total cost of MLCC. This inner electrode is connected to outer termination for surface mounting, which is composed of three layers, Cu or Ag layer, Ni plating layer, and SnPb or Sn plating layer. Most of MLCCs become Pb free by the environmental issue at present. MLCC is divided into two classes. Class I(C0G, etc) is the temperature compensating type. It has a small TCC(Temperature Coefficient of Capacitance) and a better frequency performance. Therefore, it is used in RF applications such as cellular phone, tuner, and so on. Class II(X7R, X5R, Y5V, etc) is the high dielectric constant type, which is used in general electronic circuit. Especially high capacitance MLCC is replacing other capacitors (Tantalum and Aluminum capacitor) due to the low ESR(Equivalent Series Resistance) value.
焊接控制手册--中英文对照版
目 录/CONTENT1.目的 Purpose2.编写依据 Compiling basis3.焊接工程师职责 Responsibility of welding engineer4.焊接质量检查员职责 Responsibility of quality inspector5.焊接工艺(PQR、WPS)welding procedure6.电焊工管理 Welder management7.焊接消耗品控制 Welding consumable control8.焊接追踪程式计划 Weld tracking plan9.附录 Attachment1)焊接工艺指导书(WPS)Welding Procedure Specification2)Acceptance criteria for welds焊缝验收准则3)合格焊工登记表Registration form for accepted welder4)焊条日发放记录表Record form for daily issuing rods5)焊丝日发放记录表Record form for daily issuing wires1、目的 Purpose为了确保CSPC南海石化项目管道焊接工程质量,特编制此焊接控制手册。
We establish this welding control manual so as to assure welding project quality for piping of CSPC Nanhai Petrochemicals Project.2、编制依据 BasisCSPC南海石化项目文件:CSPC Nanhai Petrochemicals documents:1)PR-8710-0000-0025 Welding Program Procedure《焊接计划》2)PR-8710-0000-0026 Welder Training And Qualification Procedure 《焊工培训和资格评定》3)PR-8710-0000-0038 Welding Control Procedure 《焊接控制程序》4)DEP 30.10.60.18-CSPC Welding of metals5)GN-8710-3000-1002 《电焊工考试与管理规则》(附件十二) GN-8710-3000-1002《electric welder examination and managementregulation》(attachment twelve)美国机械工程师协会标准:American Society of Mechanical Engineer Codes:ASME B31.1、 ASME B31.3、 ASME IX国内标准:national standardGBJ50236-98、GB50235-973、现场焊接工程师职责responsibility of field welding engineer3.1.负责准备、发布、保存被业主批准的焊接程序、标准、规范及焊工数据库、程序资格认定测试、WPS以及PQR认定记录。
IPC-A-610国际标准中英文对照
0-2
IPC-A-610 国际标准中英文对照 Table of Contents(cont.)目录(续)
4.4.3 Adhesive Bondintical..........................86
Components.....................62
4.4.7 Wire Dress for Terminations to
安装-水平-轴向引脚-无支撑的孔
Connectors Without Strain/Stress
5.2.3 Horizontal-Radial Leaded .......90
Relief.........................69
4.2.2 Excess Solder....................35 多锡
4.2.3 Threaded Fasteners...............36 紧固螺钉 4.2.3.1 Minimum Torque for Electrical
Connections.....................38 电气连接的最小扭力
1.4 Terms & Definitions .............5 术语及定义
1.4.1 Classification ..............5 分类
1.4.8 Meniscus(Component)...............10 弯月板(组件)
1.5 Examples and Illustrations...........10 实例和图标
1.4.4.4 Solder Destination Side......9 焊锡终点面
0-1
IPC-A-610 国际标准中英文对照
ASTM A743-2017 一般用耐腐蚀铬铁及镍铬铁合金铸件
Current edition approved Nov. 1, 2017. Published November 2017. Originally approved in 1977. Last previous edition approved in 2014 as A743/A743M – 13aɛ1. DOI: 10.1520/A0743_A0743M-17.
1.2 The values stated in either inch-pound units or SI units are to be regarded separately as standard. Within the text, the SI units are shown in brackets. The values stated in each system are not exact equivalents; therefore, each system must be used independently of the other. Combining values from the two systems may result in nonconformance with the specification. Inch-pound units are applicable for material ordered to Specification A743 and SI units for material ordered to Specification A743M.