右侧星状神经节阻滞引起阵发性呛咳
右侧星状神经节阻滞对急诊脑外伤患者气管插管心血管反应的影响

c a s e s wi t h t r a u ma t i c b r a i n i n j u r y
WANG Yi n g, L I Yo n g l e , W U Gu a n g y i
( De p a r t m e n t o f A n e s t h e s i o l o g o f A il f i a t e d Ho s p i t a l o f He b e i U n i v e r s t t y , B a o d i n g 0 7 1 0 0 0 , C h i n a )
第3 0 卷 第4 期
2 0 1 3年 8 月
医 学 研 究 与 教 育
Me d i c a l R e s e a r c h a n d E d u c a t i o n
V0 l - 3 0 NO. 4
Au g.神经节阻滞对 急诊脑 外伤 患者气管插 管心血管反应 的 影 响
t o t r a c h e a l i n t u b a t i o n i n e me r g e n c y c a s e s wi t h t r a u ma t i c b r a i n i n j u r y . Me t h o d s 8 0 e me r g e n c y c a s e s wi t h
超声引导下的星状神经节阻滞

减少并发症
超声引导可避免损伤周围血管 、神经和脏器,降低穿刺相关 并发症的发生率。
个体化治疗
超声引导可根据患者个体差异 调整穿刺路径和药物剂量,实
现个体化治疗。
星状神经节阻滞概述
02
星状神经节的结构和功能
结构
星状神经节是由第7、8颈神经和第1胸神经的前支组成的交感神经节,位于颈 椎横突前方。
功能
创新神经阻滞技术
借鉴超声引导下星状神经节阻滞的成功经验,探 索其他神经阻滞方法的新技术、新路径。
3
个性化治疗方案
针对不同患者和病情,研究制定个性化的神经阻 滞治疗方案,提高治疗效果和患者生活质量。
THANKS.
实时成像技术
研发实时、高清的超声成像技术,以更准确地监测神经节位置及周 围结构,提高阻滞成功率。
智能化辅助系统
引入人工智能等先进技术,辅助医生进行超声引导下星状神经节阻 滞的操作,减少人为误差。
其他神经阻滞方法的研究与应用
1 2
比较研究
开展超声引导下星状神经节阻滞与其他神经阻滞 方法的比较研究,评估各种方法的优劣,为临床 提供更多选择。
并发症的处理方法
局部出血与血肿
立即停止操作,压迫止血,必要时使用止血药物。
局部感染
加强抗感染治疗,必要时切开引流。
喉返神经麻痹
观察为主,多数可自行恢复,必要时使用神经营养药物。
霍纳综合征
无需特殊处理,可自行恢复。
未来展望与研究方
06
向
超声引导下技术的进一步优化
提高操作精度
通过技术改进,提高超声引导下星状神经节阻滞的定位精度,降 低操作难度,减少并发症风险。
超声引导下星状神
05
经节阻滞的并发症
麻醉学中级专业知识单选习题库及参考答案
麻醉学中级专业知识单选习题库及参考答案一、单选题(共100题,每题1分,共100分)1、星状神经节阻滞中患者突然出现呼吸困难,最可能的原因是A、局部麻醉药注入椎动脉B、局部麻醉药注入骨膜C、气胸D、膈神经麻痹E、局部麻醉药注入蛛网膜下腔正确答案:E2、术中失血,Hb<60 g/L时,输注_____A、浓缩红细胞B、凝血酶原复合物C、血小板浓缩物D、新鲜冰冻血浆E、冷沉淀物正确答案:A3、随着年龄的增长,正确的心血管系统的变化是_____A、瓣膜系统的弹性降低B、心肌纤维的数量减少C、心输出量增加D、血压降低E、心血管的可逆性增加正确答案:A4、男,55岁,颊癌原发灶切除术半年,拟在神经阻滞麻醉下完成单纯颈淋巴清扫术。
2.穿刺部位_____A、胸锁乳突肌中点B、单侧颈部中点C、颈正中皮肤下D、胸锁乳突肌前缘与颈外静脉交叉点前方E、胸锁乳突肌后缘中点与颈外静脉交叉点后下方正确答案:E5、男,32岁,车祸致颈椎骨折,胸3平面以下皮肤感觉消失,拟择期行椎板减压内固定术。
1.麻醉术前查体,重点应注意_____A、尿常规B、胸部物理检查C、血常规D、心电图结果E、肾功能不全正确答案:B6、下列哪项叙述是错误的_____A、罗哌卡因没有运动阻滞与感觉阻滞分离效应B、氟烷全麻时,辅用局麻药不宜加肾上腺素C、对甲亢病人,局麻药中不宜加肾上腺素D、不同部位的黏膜,吸收局麻药的速度不同E、局部浸润麻醉是阻滞组织中的神经末梢正确答案:A7、有关瓣膜性心脏病患者麻醉的特点,不正确的说法是_____A、主动脉瓣狭窄患者麻醉的关键是维持心肌氧的供需平衡B、主动脉瓣关闭不全患者用扩血管药可减少反流量C、二尖瓣关闭不全患者需要稍快的心率D、心功能Ⅱ级、二尖瓣狭窄伴关闭不全的患者,手术危险性极大E、二尖瓣狭窄患者要注意控制心率正确答案:D8、肌松药最先作用的是:A、肋间肌B、喉肌C、四肢肌D、隔肌E、咬肌正确答案:E9、支气管痉挛时患者出现明显通气困难,以气道压峰值升高和呼气性呼吸困难为特征。
星状神经节阻滞-王莉

带你认识神奇的星状神经节阻滞!
广元市第一人民医院麻醉科 王莉
星状神经节阻滞的来源:
此疗法来源颇为传奇, 1883年Liverpool 和
Alexander在结扎椎动脉治 疗癌症时无意中损伤了患者
的星状神经节。
这个现象治疗疾病。
结果意想不到的事 情发生了:术后这 位肿瘤病人的疼痛 明显减轻,全身情
阻滞疗效的判定
有关SGB阻滞疗效的判定,临床除了对于疼 痛缓解程度的判定外,主要还是对于交感功 能的测试。Malmqvist 等界定了一个严格的 SGB 术成功的标准(其中 4 个符合算为阻滞 成功):
• ① Horner 综合征; • ②皮肤温度升高≥ 34℃; • ③皮肤血流量增加≥50%(激光多普勒血流仪测定); • ④尺侧皮肤阻抗反应消失; • ⑤桡侧皮肤阻抗反应消失。
况好转。
星状神经节阻 滞的来源:
此后许多年中一直采用外科手术切 断颈部交感神经,1920年开始推广 非手术经皮的星状神经节阻滞疗法。
据说上世纪七十年代日本一位首相 患面瘫,一位麻醉医生用星状神经 节阻滞将其治愈,让星状神经节阻 滞在日本风靡一时。这个麻醉医生
也为此一举成名。
什么是星状神经节阻滞?
注射2~3分钟后病人出现同侧霍纳(Horner’s) 氏征,则表明阻滞成功。
传统方法
普通病人针进入约2cm左右,针尖触及到横突时病 人不出现异感。
对肥胖和粗短颈的病人,可能深到2.5-3cm左右。
如果发现进针比这更深,则有可能针尖刺进两个横 突之间。应立即将针退出,再调整针尖向头侧或尾 侧方向穿刺,直至针尖触及到横突骨性感觉。
星状神经节位于 人的脖子两侧
因为它的形状像 星星,所以取名 星状神经节。
星状神经节阻滞联合早期康复训练治疗脑卒中后吞咽障碍

毒 性 心 肌 炎 的 实 验 研 究 [ ] 中 国 中 西 医 结 合 杂 志 , 98 1 J 19 , 8
( )4 0 8 8 : 8 —4 2
[] 郭林妮 3
全 国心 肌 炎 心 肌 病学 术 研 讨 会 纪 要 [] 中 华 心血 管 病 J
[] Cru t n 20 ,0 ( ) 17 —18 J i l i ,0 1 14 9 :0 6 0 2 c ao [ ] 于 小 华 , 双 杰 , 英 珍 , .柯 萨奇 一腺 病 毒 受 体 与 病 毒 性 心 5 李 杨 等 肌 炎 [] 心 血 管 病 学 进 展 ,04,5 6 :4 —4 6 J. 20 2 ( )4 3 4
接 训 练 改 善 吞 咽 肌 肌 力 和 协 调 性 ( 度 刺 激 、 物 反 馈 、 温 生
星 状 神经 节 阻滞联 合早 期 康 复训 练 ' - Zx , 脑 卒 中后 吞 咽障碍 口7
.
赵
丽, 李建 霞 , 吴学英 , 秀伟 王
( 北省 南皮县人 民 医院 , 北 南皮 0 10 ) 河 河 6 50
[ 要 ] 目的 观 察 星 状 神 经 节 阻 滞联 合早 期康 复训 练 治 疗 脑卒 中后 吞 咽 障碍 患 者 的效 果 。方 法 将 16例 患 摘 0 者 随机 分 成 治 疗 组 5 6例 和 对 照 组 5 0例 , 均进 行 常规 早 期 康 复 训 练 , 疗 组 联 合 应 用 星 状神 经 节 阻滞 治 疗 。2组 治 疗 治
后 治疗 组 血 清 肌 酸 磷 酸 激 酶 、 冬 氨 酸转 氨 酶 及 血 清 乳 酸 脱 天 氢 酶 较 治疗 前 明显 降 低 , 对 照 组 治疗 前 后 降 低 不 明 显 。 提 而
麻醉学主治医师考试模拟题及答案

麻醉学主治医师考试模拟题及答案A1型题:每一道考试题下面有A、B、C、D、E五个备选答案,请从中选择一个最佳答案。
1、TURP手术时麻醉平面应达到A、T8B、T12C、T10D、T4E、T6正确答案:C答案解析:麻醉平面达到T10 就足够。
2、臂丛神经阻滞时,腋入路不能阻滞的神经是A、桡神经B、尺神经C、肌皮神经D、正中神经E、前臂内侧皮神经正确答案:C答案解析:经腋路阻滞时,肌皮神经和肋间臂神经常不能阻滞,即使改变穿刺针方向或增加局麻药量,至少仍有25%皮神经阻滞不完善。
3、臂丛神经阻滞引起霍纳综合征的原因是阻滞了A、喉返神经B、星状神经节C、膈神经D、迷走神经E、颈丛神经正确答案:B答案解析:麻药经椎间孔至椎旁引起星状神经节阻滞,导致上睑下垂,瞳孔缩小,额部无汗,鼻塞,甚至上肢运动、感觉功能障碍,称为霍纳综合征。
4、长期卧床的骨科手术病人应特别注意A、上呼吸道感染B、心功能障碍C、术后疼痛D、肌肉萎缩E、深静脉血栓形成正确答案:E答案解析:尤其是下肢的血栓。
5、成年人屏气试验的正常值是A、>15秒B、>20秒C、>30秒D、>35秒E、>40秒正确答案:C答案解析:屏气试验的正常值是>30秒,短于20秒者大多为肺功能异常。
心肺功能异常是憋气时间缩短的主要原因。
6、低流量麻醉的优点不包括A、麻醉平稳B、用药量少C、麻醉深度容易调节D、减少环境污染E、改善气道的温度和湿度正确答案:C答案解析:低流量麻醉具有麻醉平稳,用药量少,降低费用,减少环境污染,改善气道温度和湿度等优点。
7、低温疗法中深低温是指体温在A、34℃以上B、32~34℃C、28~32℃D、22℃以下E、28℃以下正确答案:E答案解析:低温治疗分为三类:降温至32~34℃为浅低温,28~32℃为中度低温,小于28℃为深低温。
8、定位棘突的体表标志不正确的是A、两肩胛下角连线为T 棘突B、颈部最大突起的棘突为CC、两肩胛冈内侧连线为T 棘突D、两髂嵴最高点连线为L 棘突E、髂后上棘连线为S 骶椎正确答案:A答案解析:直立位两上肢垂于体侧时,两侧肩胛冈内侧端连线,通过第3胸椎棘突。
麻醉学选择题汇编
没有太细致甄别,因为我们学的是《麻醉学》,有些是《临床麻醉学》的试卷题目……1、引起舌后坠的主要原因为()A、口腔分泌物或异物阻塞;B、站立时因重力作用,下颌骨和舌肌的松弛造成舌体坠向咽部阻塞气道。
C仰卧位时因重力作用,下颌骨和舌肌的松弛造成舌体坠向咽部阻塞气道。
D、咽部异物刺激喉诱发的声门关闭活动增强。
2、临床最常用的气管插管方法为()A、经口明视法;B、经口盲探法;C、经鼻明视法;D、经鼻盲探法。
3、麻醉期间中心静脉压测定最常选择静脉是()A、贵要静脉;B、颈内静脉;C、股静脉;D、锁骨下静脉。
4、合并冠心病手术病人麻醉期间控制性降压最常用药物是()A、异氟烷;B、硝酸甘油;C、艾司洛尔;D、硝普钠。
5、有关麻醉前禁食禁饮哪项不正确:()A、在应激情况下胃排空加速;B、成人择期手术前禁食12 小时,禁饮4 小时;C、小儿禁食4~8 小时,禁水2~3时;D、急症病人病情紧急时,不能等待禁食,应立即手术;E、饱胃病人必需立即手术时,应采取避免呕吐误吸的措施。
患者,男,52岁,择期行直肠癌根治术。
术前合并慢性阻塞性肺疾病、肺心病,丧失体力劳动能力。
6、麻醉前病情评估分级为:()A、ASAⅡ级;B、ASA Ⅲ级;C、ASA Ⅳ;D、ASA ⅢE级。
7、病人术前肺功能检查最重要的指标是:()A、TVB、VC;C、FEV1;D、FRC。
8、为最大限度地预防术后呼吸并发症,最重要的维护肺功能的措施是?()A、术前三天预防性抗生素治疗;B、锻炼胸式呼吸;C、吹气球锻炼肺活量;D、间断低浓度吸氧。
9、为避免麻醉早期血流动力学,术前2小时复方氯量化钠液500毫升,其目的是补充()。
A、生理需要量;B、生理消耗量;C、额外损失;D、均是。
10、患者术前血红蛋白98g/L,切除直肠过程中出血约400毫升,此时输血宜选择?()A、浓缩红细胞;B、新鲜血浆;C、全血;D、血小板。
1、下列哪项不是麻醉前检诊的目的(E )A、获得有关病史B、完善术前准备并制定合适的麻醉方案C、指导病人配合麻醉D、解除病人的焦虑和恐惧E、取得病人的同意和信任,确保麻醉无任何风险2、在评估病人的呼吸系统时,有关对其肺功能的评估,下列哪项不正确(D)A、可为术前准备及术中、术后的呼吸管理提供可靠的依据。
星状神经节阻滞操作方法
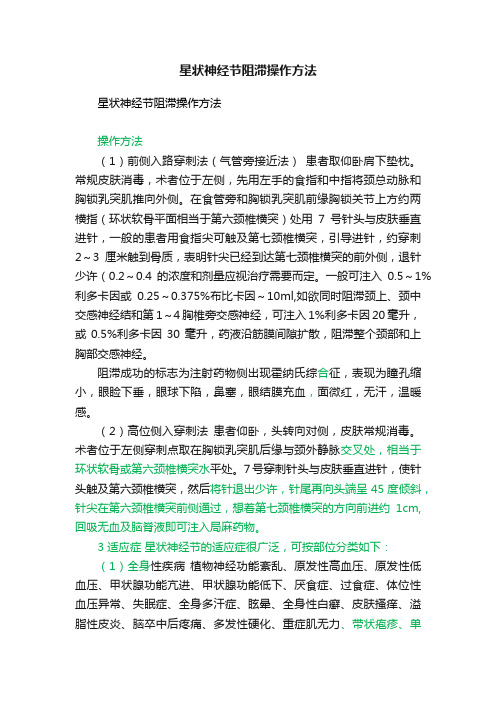
星状神经节阻滞操作方法星状神经节阻滞操作方法操作方法(1)前侧入路穿刺法(气管旁接近法)患者取仰卧肩下垫枕。
常规皮肤消毒,术者位于左侧,先用左手的食指和中指将颈总动脉和胸锁乳突肌推向外侧。
在食管旁和胸锁乳突肌前缘胸锁关节上方约两横指(环状软骨平面相当于第六颈椎横突)处用7号针头与皮肤垂直进针,一般的患者用食指尖可触及第七颈椎横突,引导进针,约穿刺2~3厘米触到骨质,表明针尖已经到达第七颈椎横突的前外侧,退针少许(0.2~0.4的浓度和剂量应视治疗需要而定。
一般可注入0.5~1%利多卡因或0.25~0.375%布比卡因~10ml,如欲同时阻滞颈上、颈中交感神经结和第1~4胸椎旁交感神经,可注入1%利多卡因20毫升,或0.5%利多卡因30毫升,药液沿筋膜间隙扩散,阻滞整个颈部和上胸部交感神经。
阻滞成功的标志为注射药物侧出现霍纳氏综合征,表现为瞳孔缩小,眼睑下垂,眼球下陷,鼻塞,眼结膜充血,面微红,无汗,温暖感。
(2)高位侧入穿刺法患者仰卧,头转向对侧,皮肤常规消毒。
术者位于左侧穿刺点取在胸锁乳突肌后缘与颈外静脉交叉处,相当于环状软骨或第六颈椎横突水平处。
7号穿刺针头与皮肤垂直进针,使针头触及第六颈椎横突,然后将针退出少许,针尾再向头端呈45度倾斜,针尖在第六颈椎横突前侧通过,想着第七颈椎横突的方向前进约1cm,回吸无血及脑脊液即可注入局麻药物。
3 适应症星状神经节的适应症很广泛,可按部位分类如下:(1)全身性疾病植物神经功能紊乱、原发性高血压、原发性低血压、甲状腺功能亢进、甲状腺功能低下、厌食症、过食症、体位性血压异常、失眠症、全身多汗症、眩晕、全身性白癣、皮肤搔痒、溢脂性皮炎、脑卒中后疼痛、多发性硬化、重症肌无力、带状疱疹、单纯性疱疹、传染性单核细胞增多症、慢性疲劳综合症、反射性交感神经萎缩症、幻肢痛、断肢痛、糖尿病。
(2)头部疾患脱毛症、头痛(包括偏头痛、紧张性头痛、群集性头痛、颞动脉炎性头痛)脑血栓、脑血管痉挛、脑梗塞等。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Distal Squeeze Technique Increases Venous Blood Flow and Allows for EasyIdentification of VeinsWith Ultrasound Accepted for Publication:8August2009To the Editor:I dentification of vascular structures dur-ing regional anesthesia procedures with ultrasound can help to identify target nerves and plan for an appropriate needle approach to avoid puncture and intravas-cular injection.Arteries can be identified by their relative resistance to collapse from pressure exerted by the ultrasound probe along with the characteristic pulsa-tileflow demonstrated by color or pulse wave Doppler.Veins often go unidentified, leading to patient morbidity1,2and poten-tial mortality.Because of their ease of collapse with minimal ultrasound probe pressure and their low-velocity-flow states that are not always well represented on ultrasound by color Doppler,veins can bedifficult to recognize with ultrasound.We describe a novel technique to identify small or collapsed veins using any standard ultrasound with color Doppler. Once an area is identified that could con-tain venous structures,color Doppler is activated.During real-time ultrasound, any distal part of the patient’s correspond-ing extremity is compressed or squeezed. This compression of the distal muscles and veins significantly increases venous bloodflow that is then represented more reliably by color Doppler on ultrasound (Fig.1).This technique may be repeated several times for complete evaluation of veins in an area and is well tolerated by patients.Other techniques can be used to visualize low-flow blood vessels such as probe tilt,adjustment of pulse repetition frequency,and increasing color gain,but none of these are effective in evaluating veins that are collapsed.Squeezing a distal extremity,as described here,results in the ability to evaluate both low-flow and com-pletely collapsed venous structures.We have found this distal compression technique to be very useful in the identification of veins that are often closely associated with nerves.We routinely use this technique in the axillaq and the popliteal regions bysqueezing the arm and calf,respectively.David B.Auyong,MDDepartment of AnesthesiologyVirginia Mason Medical CenterSeattle,WAJames G.Benonis,MDPresbyterian Anesthesia Associates,P.A.Charlotte,NCJeff Gonzales,MDPark Ridge Anesthesiology AssociatesAdvocate Lutheran General HospitalPark Ridge,ILEditor’s Note:James P.Rathmell served asthe acting editor-in-chief for this article.REFERENCES1.Dolan J,McKinlay S.Early detectionof intravascular injection duringultrasound-guided axillary brachialplexus block.Reg Anesth Pain Med.2009;34:182.2.Zetlaoui PJ,Labbe JP,Benhamou D.Ultrasound guidance for axillary plexusblock does not prevent intravascularinjection.Anesthesiology.2008;108:761.Ultrasound-GuidedInterfascial Injection forPeripheral Obturator NerveBlock in the ThighAccepted for Publication:29June2009To the Editor:W e read with interest the recent arti-cle by Sinha et al,1describing anultrasound-guided obturator nerve blockwithout the need to specifically identifyeither the anterior or the posteriorbranches of the obturator nerve.Theauthors described placement of a needleand local anesthetic injection into a fascialplane bounded by the pectineus andadductor brevis muscle followed by asecond injection into a fascial planebetween adductor brevis and adductormagnus muscles.Owing to the consider-able diversity in the sensory distributionof the obturator nerve,the authors havecorrectly taken loss of hip adduction asthe end point for a successful block.2However,the pectineus muscle,normallyinnervated by both the obturator nerveand femoral nerves,also providesan FIGURE1.A,Transverse ultrasound image of the popliteal space with superimposed color Doppler signal showing the popliteal artery in red V without compression of the calf,the vein is not readily seen.B,The same transverse ultrasound image of the popliteal space with superimposed color Doppler signal after compression of the calf showing augmented venous signal in blue.C,The simple method for squeezing the calf to augment venousflow during ultrasound imaging in the popliteal space.L ETTERS TO THE E DITORimportant contribution to hip adduction.3 Placement of local anesthetic within the fascial planes of the thigh and in the volumes described by Sinha et al may also be expected anesthetize those branches of the femoral nerve supplying pectineus muscle,thus contributing to a reduction in hip adduction.The authors may therefore have overestimated the loss of motor function attributable to obturator nerve block alone.A more accurate assessment of the contribution of the obturator nerve to hip adduction may have been achieved if blockade of the femoral nerve had been undertaken before obturator nerve block.However,one significant advantage of interfascial injection omitted in the article by Sinha et al is the ability to place local anesthetic at some distance from the peripheral nerve of interest.In this way, anesthesia can be achieved without the need for a needle to be in close contact with neural structures.Rosemary Snaith,MB,ChB,MRCP,FRCA John Dolan,BSc,MSc,PhD,MB,ChB,FFARCSIDepartment of AnaesthesiaGlasgow Royal InfirmaryGlasgow,Scotland,UKREFERENCES1.Sinha SK,Abrams JH,Houle TT,Weller RS.Ultrasound-guided obturator nerve block:an interfascial injection approach withoutnerve stimulation.Reg Anesth Pain Med.2009;34:261Y264.2.Bouaziz H,Vial F,Jochum D,Macalou D,Heck M,Meuret P,et al.An evaluation of thecutaneous distribution after obturator nerveblock.Anesth Analg.2002;94:445Y449.3.Standring S.Gray’s Anatomy.39th ed.NewY ork,NY:Churchill Livingstone;2005.Reply to Drs.Snaithand DolanAccepted for Publication:6November2009 To the Editor:W e thank Drs.Snaith and Dolan for their interest in our study and the opportunity to respond to their comments.1 The nonobturator contribution to thigh adduction was acknowledged in the intro-duction of our study,and previous stud-ies have shown that femoral nerve block can result in up to25%reduction in ad-ductor motor strength(AMS)by block-ing the adductors innervated by femoralnerve.2,3Similarly,a sciatic nerve blockmay decrease AMS by11%T7%.4Thisis specifically why we chose50%or greaterreduction in AMS to indicate successfulobturator nerve block(ONB),which standsin contrast to other investigators who haveaccepted any reduction in AMS to indicateONB.Drs.Snaith and Dolan may havemisinterpreted the intent of our study,which was not to determine B the loss ofmotor function attributable to the obtura-tor nerve,[but to identify successful ONBwith expected nociceptive block of thearticular branches to the knee.We would disagree that a superiordesign would have been to provide femoralblock before obturator block.If so de-signed,critics might suggest that the localanesthetic solution used for the femoralblock could spread to the obturator nerveand cause partial blockade.The lack ofreliable sensory distribution of the obtura-tor nerve would prevent one from rulingout such a partial blockade,and contribu-tion of the obturator nerve to adductionmight be underestimated if that were thequestion under investigation.Would notsciatic contribution to thigh adduction alsohave to be eliminated by sciatic block be-fore ONB?Finally,we would agree with thetheoretical advantage of interfascial injec-tion proposed,except that this presumesthe nerve of interest can be unequivocallyidentified before placing the needle B atsome distance[from it.Our techniqueuses ultrasound to correctly identify mus-cles and intervening fascia;no additionaltime was spent to specifically identify theobturator nerve,and although its ultra-sound appearance has been described,it isnot always obvious.Sanjay K.Sinha,MBBSJonathan H.Abrams,MDDepartment of AnesthesiologySt Francis Hospital and Medical CenterHartford,CTTimothy T.Houle,PhDRobert S.Weller,MDDepartment of AnesthesiologyWake Forest University School of MedicineWinston-Salem,NCREFERENCES1.Dolan J,Snaith R.Ultrasound-guidedinterfascial injection for peripheral obturatornerve block in the thigh.Reg AnesthPain Med.2010;35:314Y315.2.Macalou D,Trueck S,Meuret P,et al.Postoperative analgesia after total kneereplacement:the effect of an obturator nerveblock added to the femoral3-in-1nerveblock.Anesth Analg.2004;99:251Y254.3.Bouaziz H,Vial F,Jochum D,et al.Anevaluation of the cutaneous distributionafter obturator nerve block.Anesth Analg.2002;94:445Y449.4.Jochum D,Iohom G,Choquet O,et al.Addinga selective obturator nerve block to theparasacral sciatic nerve block:an evaluation.Anesth Analg.2004;99:1544Y1549.Does Lack of AnestheticAssistance Justifya SuboptimalUltrasound-Guided RegionalAnesthetic Technique?Accepted for Publication:24July2009To the Editor:W e read with interest the letter byPham Dang et al1describing aneedle-side handle as an aid when under-taking a peripheral nerve block under ul-trasound guidance.The rationale for thisincludes having one hand free for injec-tion of local anesthetic and adjustment ofthe ultrasound parameters when anestheticassistance is unavailable.Proper body er-gonomics to handle the transducer and theneedle are essential for block safety andsuccess in addition to avoiding operatorfatigue and body injury.2To provide morecontrol of the probe and a stable ultra-sound image,it is recommended that theoperator holds the probe at its distal endwith part of the hand in contact with thepatient.2In this way,the hand is comfort-ably supported while continually observ-ing and accurately positioning the needletip before and during injection of local an-esthetic.From the authors’description andillustrations provided the operator clampsthe needle side handle between second andthirdfingers of the hand.With the handnow unsupported,the freefingers hold theultrasound probe at its more proximal endwhere small movements translate into rela-tively large movements at the distal endof the transducer and thus the ultrasoundimage.Changing a recommended tech-nique to a suboptimal one risks both blockfailure and potential complications and cannever be justified even for the lack of anavailable anesthetic assistant.Aside frominjecting local anesthetic and adjusting theultrasound settings,an anesthetic assistantis also a valuable asset in monitoring andreassuring the sedated patient while theanesthesiologist concentrates more on thenerve block.Regional Anesthesia and Pain Medicine&Volume35,Number3,May-June2010Letters to the EditorACKNOWLEDGMENTThere have been no external finan-cial resources supporting this work.Rosemary Snaith,MB,ChB,MRCP ,FRCAJohn Dolan,BSc,MSc,PhD,MB,ChB,FFARCSIDepartment of Anaesthesia Glasgow Royal Infirmary Glasgow,Scotland,UKREFERENCES1.Pham Dang C,Pilet P ,Heymann eful side handle for holding needle during ultrasound-guided regional anesthesia.Reg Anesth Pain Med .2009;34:382Y 383.2.Chan VWS.Ultrasound Imaging for Regional Anesthesia.A Practical Guide .2nd ed.Toronto,Canada:Ultrasound for Regional Anesthesia,2008.Reply to Drs.Snaithand DolanAccepted for Publication:21October 2009To the Editor:Ithank Drs.Snaith and Dolan for their interest in my B home-made side handle [described to compensate the lack of anesthetic assistant during the practice of ultrasound-guided regional anesthesia (UGRA).1To their qualification of the side handle (SH)as a suboptimal tech-nique,I would like to point out some arguments showing that indeed the SHis designed to optimize the UGRA technique.Let us consider the problem with the anesthetic assistant.I believe that the assistant will not be very happy if he/she has in the same time to help and care for patient’s cardiorespiratory monitoring,se-dation,or comfort.In my institution,our anesthetist nurses care for the patient’s monitoring and comfort.I do care for all the rest in relation with UGRA,thanks to the SH.Drs Snaith and Dolan seem ignoring that,in many hospitals around the world,practitioners perform alone the single-shot regional techniques,based on nerve stimulation.The SH could allow them to move into the increasingly pop-ular UGRA with the same autonomy.The SH will permit the practitioner to free the hand that has served the needle direction and do the whole UGRA procedure by him-self.With the free hand,he/she switches and tunes himself/herself the nerve stimu-lator,feels himself/herself the pressure while injecting a chosen volume of anes-thetics around the nerve,promptly stops injecting in case of intraneural or intravas-cular or atypical spread of local anesthetics,adjusts the ultrasound parameters,writes annotation,and saves the desirable video clips.In other words,there is a continual,direct,and convenient interaction between the practitioner and the portable ultrasound machine.To my belief,this is a major tech-nical advance.As for the recommended and ref-erenced way of probe holding,2I noticed that it is to achieve a control of the probe and to avoid fatigue.The SH is designedto reach the same goal but in a different manner.The fingers of the hand holding the probe,by clamping the SH,unify the probe to the needle inserted deep in the skin and muscle.Anchored in this way,the probe is less likely to slide away.It is always possible to tilt or rotate slightly the probe unified to the needle to better visualize the relationship between target nerve and needle.The playing of fingers (video clips and photographs available on demand)is playful,and it is a child’s play.The finger movements vary with the pe-ripheral nerve block approaches.The aim is to seize the SH and achieve the B immo-bile needle technique.[3For information,there is a possibility to train oneself in the office by puncturing a sponge and moving around a computer mouse used like an ultrasound probe.The exercise consists of clamping or pinching the SH between different fingers of the hand holding the probe.The SH can be pinned flat on the probe by the first finger or immobilized by posing simply the index on the end of the long segment.Conveniently,adjust-ments are possible by pushing on the short segment with the index of the hand hold-ing the needle hub and making the SH slide over the needle to an appropriate level then turning the SH around the nee-dle to help it into the finger clamp.Consider ergonomics,the SH is a solution.Finger movements create condi-tion for hand relaxation,which is not achievable if the hand is clutching the probe.By freeing the hand that has served the needle drive,the SH in fact frees and relaxes the rest of the body.This results in a relaxed attitude for the practitioner’s neck,shoulders,and back as shown in Figure 1.This contrasts with the tense and rigid attitude usually seen,which involves 2hands,one holding the probe and the opposite holding the needle.This rigid attitude induces a stress to the 2shoulders and to the whole vertebral column.Charles Pham Dang,MDHo ˆtel-DieuCHU de Nantes,FranceREFERENCES1.Pham Dang C,Pilet P ,Heymann eful side handle for holding needle during ultrasound-guided regional anesthesia.Reg Anesth Pain Med .2009;34:382Y 383.2.Chan VWS.Ultrasound Imaging for Regional Anesthesia.A Practical Guide .2nd ed.Toronto,Canada:Ultrasound for Regional Anesthesia,2008.3.Winnie AP .An B immobile needle [for nerve blocks.Anesthesiology .1969;31:577Y578.FIGURE 1.Side handle and ergonomics.The probe is unified to the needle by the SH clamped by the fingers of the right hand in contact with the patient.The free left hand is seizing the syringe for injection.The practitioner is analyzing the Sonoscan displayed on the screen.Note the practitioner’s relaxed attitude good for ergonomics.The portable ultrasound machine is installed in line with the practitioner’s eyes and within his/her arm’s stretch.Letters to the Editor Regional Anesthesia and Pain Medicine&Volume 35,Number 3,May-June 2010Why Puncturing a Lumbar Tattoo During Epidural Analgesia Cannot Induce an Epidermoid TumorAccepted for Publication:20September 2009.To the Editor:Lumbar tattoos in young women have been at the center of an unresolved controversy since 2002.1Indeed,reported cases of epidermoid tumors caused by epidermal tissue entrapment by hollow needles after lumbar punctures have led anesthesiologists to speculate a theoreti-cal risk of introducing tattoo pigments into the epidural space during epidural analgesia,followed by potential compli-cations such as epidermal tumors and/or chemical arachnoiditis.1Based on that hypothesis,not only literature in the field of obstetrical anesthesiology but also books,media,and Internet forums have been flooded with the convincing fantasy that young parturients with lumbar tattoos could not undergo epidural analgesia.B Guidelines [have been provided,such as puncturing in a free spot within the tattoo,selecting another free vertebral interspace,nicking the skin before insertion of the needle,or even avoiding epidural anesthe-sia.2Despite rare publications discussing the true relevance of such risks,3,4precau-tionary principle still dictates blindly that the anesthesiologist avoid puncturing a lumbar tattoo.5The following images of tattooed skin are intended to show why it is irrele-vant and irrational to believe that punctur-ing a tattoo will result in the development of a B postpuncture tattoo-induced epider-mal tumor.[During tattooing,pigments areintroduced through the epidermis in the dermis.However,the pigments deposited within the epidermis just after the proce-dure are progressively lost during the heal-ing phase when the superficial layers of the epidermis peel away.6Pigments located in the dermis are mostly assimilated by macrophages and fibroblasts.Most of the macrophages migrate to the lymphatics,whereas some remain in the perivascular area,and eventually,some pigments are left free in the extracellular area within loose fibrous connective tissue (Fig.1).6Therefore,as the epidermis is devoid of tattoo pigments,it is impossible that B epi-dermal tissue coring [can include any pig-ment.Moreover,according to a forensic pathologist specializing in tattooing pa-thology,the pigments are B fixed [and sta-tionary within the dermis and cannot be mobilized by the needle or migrate along the needle track.5Therefore,if a needle is introduced through a tattoo,it would be more likely to entrap macrophages and/or fibroblasts with intracellular pigments than free the pigment itself.Potential tumoral consequences,if they do exist,will be the result of cell introduction and the epidu-ral analgesia itself rather than the pig-ments.If an anesthesiologist wants to avoid the pigments in the dermis while punctur-ing,our picture shows that he will have to make an incision to the hypodermis before puncturing.The risk of epidermoid tumor is re-lated to epidermal tissue coring during puncture not because of the presence of an underlying B harmless [tattoo.Such com-plications were reported in the 1950s in patients who had multiple punctures with hollow needles long before lumbar tattoos were fashionable.The concerns of Douglas and Swenerton 1were legitimate at first,but there is absolutely no data to support such risk.Nicolas Kluger,MDService de Dermatologie Universite ´MontpellierHo ˆpital Saint-Eloi Montpellier,France Sylvie Fraitag,MDService d’anatomopathologie Ho ˆpital Necker-Enfant MaladesParis,FranceBernard Guillot,MDService de Dermatologie Universite ´MontpellierHo ˆpital Saint-Eloi Montpellier,FranceJean-Christian Sleth,MDService d’anesthe ´sie-re ´animationPolyclinique Saint-RochMontpellier,FranceREFERENCES1.Douglas MJ,Swenerton JE.Epiduralanesthesia in three parturients with lumbar tattoos:a review of possible implications.Can J Anaesth .2002;49:1057Y 1060.2.Raynaud L,Mercier FJ,Auroy Y,Benhamou D,SOS ALR.Epiduralanaesthesia and lumbar tattoo:what to do?Ann Fr Anesth Reanim .2006;25:71Y 73.3.Sleth JC.Epidural anaesthesia and lumbar tattoo.Histology of tattoo:the missing link?Ann Fr Anesth Reanim .2007;26:266Y 267.4.Kluger N,Sleth JC,Guillot B.Lumbar tattoos and lumbar puncture:the emperor’s new clothes?Can J Anaesth .2007;54:855.5.Mercier FJ,Bonnet MP .Tattooing andvarious piercing:anaesthetic considerations.Curr Opin Anaesthesiol .2009;22:436Y 441.6.Sperry K.Tattoos and tattooing.Part II:Gross pathology,histopathology,medical complications,and applications.Am J Forensic Med Pathol .1992;13:7Y 17.Important Structures to BeKnown for a Safe Ultrasound-Guided Supraclavicular Plexus BlockAccepted for Publication:24September 2009To the Editor:We read with great interest the letter to the editor by Manickam et al 1about an incidental finding of a variant relation of the brachial plexus to the subclavian artery on the first rib.During a routine ultrasound,the authors found a surprising dissociation of the subclavian artery of 1.5cm from the brachial plexus,which ought to be adjacent to the latter structure.The dissociation was caused by a hypo-echoic structure,which was not inter-preted or named by the authors.OntheFIGURE 1.Left,Biopsy of tattooed skin (hematoxylin-eosin stain).Exogenous pigments are located in the mid and deep dermis.The epidermis is devoid of pigments.Right,Close-up view of tattoo pigments (Perls stain).Most of the pigment deposits have been assimilated by macrophages,and few pigments are left free between collagen bundles.Regional Anesthesia and Pain Medicine&Volume 35,Number 3,May-June 2010Letters to the Editorother hand,the author stated that this dissociation has never been reported in regional anesthesia literature.However,this surprising dissociation is anatom-ically easily explicable and corresponds to a very well known structure separating the artery from the brachial plexus.This structure was already mentioned 150years ago,2and this could be found in many anatomical textbooks;the scalenus mini-mus muscle.As some examples,Gray 3mentions this muscle as a frequently present muscle arising from the anterior border of the seventh cervical vertebra to run caudally and to insert on the first rib just behind the groove of the subclavian artery.Much more can be found in German literature.Hafferl 4described this structure not only as frequently present but also as a very thick and round muscular structure.The muscle’s origin can be extended to the fifth cervical vertebra.More important is that the tendon of the muscle is spread-ing shortly before the insertion on the first teral fibers might insert on the sec-ond and even third ribs,whereas the medial fibers insert in the pleural dome.As a con-sequence,the muscle reaches quite an im-pressive thickness (Fig.1)and can explain a hypoechoic structure.Because of the in-sertion in the pleural dome,this muscle is also named the B tensor pleurae muscle,[Rarely,the muscle can be replaced by liga-mentous fibers.In this case,the structure is described as the costopleurovertebral lig-ament.This ligament is one of the lig-amentous fixations of the pleural dome and is listed as the Zuckerkandl ligaments.4Other Zuckerkandl ligaments are the costopleural,vertebropleural,and esopha-gopleural ligaments.If a costopleurover-tebral ligament would be present,this would result in a hyperechoic structure.What is more,recent anatomical textbooks summarize this very frequently present muscle,providing variations,blood and nerve supply,as well as the function.5We certainly agree that,with the up-coming ultrasound techniques,some struc-tures cannot be easily assigned.Images can be misinterpreted,and structures such as the muscles might be shown as differing images from patient to patient.Neverthe-less,this is not the case for the findings mentioned by Manickam et al.1Anatomi-cal textbooks and literature provide much information about the supraclavicular region as well as about the interscalene gap.However,the correct interpretation of such findings and ultrasound images strengthens the demand for more knowl-edge of sonoanatomy,which could be provided by special workshops about this topic.As a consequence,the collaborationbetween the anesthetist and the anatomist has to be intensified.It also forces us as anatomists to incorporate our existing knowledge of sound anatomy and its vari-ations in the interpretation of ultrasound images.We would recommend researching not only anesthesiology but also anatomy literature and textbooks,which might be quite helpful.Georg C.Feigl,MD Manuel Dreu,MDInstitute of Anatomy Medical University GrazGraz,AustriaREFERENCES1.Manickam BP ,Oosthuysen SA,Parikh MK.Supraclavicular brachial plexusblock-variant relation of brachial plexus to subclavian artery in the first rib.Reg Anesth Pain Med .2009;34:383Y 384.2.Henle DJ.Muskellehre.In:Henle,ed.Handbuch der Systematischen Anatomie .1st V olume,3rd part.Braunschweig,Germany:Friedrich Viehweg und Sohn;1858:125.3.Bannister LH.Respiratory system.In:Gray’s Anatomy .38th ed.New Y ork,NY:Elsevier Churchill Livingstone;1995:1663.4.Hafferl A.Die Muskulatur.In:Hafferl A,ed.Die Anatomie der Pleurakuppel .Berlin,Germany:Julius Springer Verlag;1939:20.nz T,Wachsmuth W .Regiosternocleidomastoidea.In:Lanz-Wachsmuth,ed.Praktische Anatomie:Neck .New Y ork,NY:Springer Verlag;2004:371.Transient Cough Attacks After Right Stellate Ganglion BlockAccepted for Publication:13October 2009To the Editor:Stellate ganglion block (SGB)is a commonly used technique for a variety of diagnostic,therapeutic,and prognostic purposes.It is associated with some complications because of the anatomical properties of the ganglion.1We present a case with transient cough attacks as an unusual complication of SGB.A 69-year-old woman was diagnosed with complex regional pain syndrome and scheduled for right SGB once a day for 10days.Stellate ganglion block was performed using the paratracheal approach at the C6level.The first tree blocks wereuneventful.FIGURE 1.Ventral view of a left scalenovertebral triangle.The subclavian artery (SA)is passing the first rib (FR)as well as the brachial plexus (BP).The scalenus minimusmuscle (ScMM)disassociates both structures and inserts at the pleural dome (PD)with a very thick tendon.Letters to the Editor Regional Anesthesia and Pain Medicine&Volume 35,Number 3,May-June 2010No complication was observed during the fourth block and the patient was sent home,but2hrs after the procedure,she reported a coughing attack lasting1hr. Because the patient responded well to the blocks,we decided to continue the block on day5,and the procedure was again uneventful.Ten minutes after the sixth block,we witnessed another coughing ep-isode that lasted10mins without inter-ruption.Because the second attack was short and not life-threatening,it was de-cided to continue SGBs with smaller vol-umes,and6mL of0.25%bupivacaine was given at the seventh block.Unfortu-nately,10mins after the procedure,she had a similar cough attack lasting50mins. Result of the physical examination was unremarkable.Stellate ganglion block was stopped,and treatment continued with pregabalin.To the best of our knowledge,episo-dic coughing after SGB has been reported by Naveira and Morales2in only2patients. The authors theorized that the cough attack was due to the aspiration of saliva after recurrent laryngeal nerve paralysis.The right and left recurrent laryngeal nerves branch from the vagus nerve,but their route to reach the larynx is differ-ent.The left laryngeal nerve loops under and around the arch of the aorta(liga-mentum arteriosum)before ascending dor-sally in the left tracheoesophageal sulcus, whereas the right branch loops obliquely around the right subclavian artery and leads into the right tracheoesophageal sul-cus.When the recurrent laryngeal nerve branches at the cervical level,it is called a nonrecurrent nerve.3Nonrecurrent laryn-geal nerve mainly appears on the right side,with an incidence of0.3%to1.6%. The left nonrecurrent laryngeal nerve is rare(0.04%).4Both recurrent and nonre-current laryngeal nerves are located closer to the site of SGB on the right side and may be affected more frequently during right SGB.Our case and the other2re-ported cases had SGB on the right side.The cough reflex is initiated by ac-tivation of chemically and mechanically sensitive vagal afferent nerves.5,6The recurrent laryngeal nerve is responsible for the motor innervations of the laryngeal muscles that control the glottic opening and also carries sensitivefibers from a part of the larynx and trachea.RNL blockade after SGB leads to vocal cord paralysis and/or loss of sensation in the subglottic area.The glottis may not close tightly,which may allow aspiration of saliva into the trachea.Cough is regulated both voluntarily and involuntarily.The force and duration of cough are related to the degree of stimulus,the psychological state,and the social situation of the individual.Thenumber and the force of cough are alsounder conscious control but in ways notyet adequately quantified or described.7Because coughing may be voluntarilyinitiated or exaggerated by the patient,itmay not be considered as an importantsymptom by the clinician and not re-ported as a complication of SGB unlessit is severe.Naveira and Morales reported thatthe cough attack was ceased by inhaledlidocaine administration after SGB,butinhibition of the cough reflex is a well-known risk factor to increase lower airwayinfections.8We do not recommend inhi-biting the cough reflex unless the coughattack leads to hypoxia or hemodynamicdisturbances.In conclusion,we think that coughattack is most probably due to recurrentlaryngeal nerve anesthesia that allows as-piration into the trachea and should beconsidered as a complication of SGB.Fur-thermore,to determine whether these com-plications occur more frequently duringright SGB,studies comparing complicationfrequencies for both sides are required.Sebnem At N c N,MD,PhDKursat Akoz,MDDepartment of AnaesthesiologyDivision of AlgologyMersin UniversityFaculty of MedicineMersin,TurkeyREFERENCES1.Stanton-Hicks plications ofsympathetic blocks for extremity pain.TechReg Anesth Pain Manag.2007;11:148Y151.2.Naveira FA,Morales A.Treatment ofpersistent cough after stellate ganglion block.Reg Anesth.1993;18:312Y314.3.Toniato A,Mazzarotto R,Piotto A,BernanteP,Pagetta C,Pelizzo MR.Identification of thenonrecurrent laryngeal nerve during thyroidsurgery:20-year experience.World J Surg.2004;28:659Y661.4.Maranillo E,Vazquez T,Quer M,et al.Potential structures that could be confusedwith a nonrecurrent inferior laryngeal nerve:an anatomic ryngoscope.2008;118:56Y60.5.Canning BJ.Encoding of the cough reflex.Pulm Pharmacol Ther.2007;20:396Y401.6.Canning BJ,Mori N,Mazzoneb SB.Vagalafferent nerves regulating the cough reflex.Respir Physiol Neurobiol.2006;152:223Y242.7.Canning BJ.Anatomy and neurophysiologyof the cough reflex,ACCP evidence-basedclinical practice guidelines.Chest.2006;129:33Y47.8.Hall AP,Fox AJ,Raphael AF,Nandwani N,Smith G.Upper airway reactivity andupper respiratory tract infection:effect ofnebulized lidocaine.Br J Anaesth.1999;82:857Y860.Illusory IntravascularNeedle PlacementAn UnusualUltrasound ArtifactAccepted for Publication:27October2009To the Editor:V arious artifacts have been reportedin the literature pertaining to the useof ultrasound.1Y3We describe an appar-ent intravascular penetration during anultrasound-guided infraclavicular block.A51-year-old man presented forelective repair of a right upper-extremityarteriovenousfistula.With the ultrasoundprobe(HFL38Â/13-6MHz linear probe,SonoSite S Series;SonoSite Inc,Bothell,Wash)on the right deltopectoral groove inthe parasagittal plane,an18-gauge insu-lated Tuohy needle(StimuCath;ArrowInternational,Reading Pa),connected toa nerve stimulator(Stimuplex HNS11;B.Braun Medical Inc,Bethlehem,Pa),wasintroduced using ultrasound guidance.Thenerve stimulator was not yet switchedon at this stage.Upon approaching thelateral cord of the brachial plexus with theneedle B in plane[to the ultrasound probe,the ultrasound image appeared to show theneedle tip to be inside the axillary artery(Fig.1A).The needle was open to am-bient pressure,but there was no backflowof blood.After negative aspiration forblood,a test dose with epinephrine wasinjected through the needle with nega-tive results.Hydrodissection by the localanesthetic showed the injection to beoutside the artery,with the lateral cordbeing B pushed away[from the artery(Fig.1B).All3cords were separatelyblocked,placing10mL of0.75%ropiva-caine on each cord.No adverse effectswere noted.This case clearly illustrates that theappearance of apparent intravascular pene-tration may,in fact,be due to artifact.Apossible explanation for this appearanceis the so-called B side-lobe artifact.[Anultrasound image consists of a main beamof sound with the shape of an invertedcone(main lobe)and B side lobes.[4Sidelobes consist of beams of lesser intensityon either side of the main beam(Fig.2A).Side lobes may have sufficient intensityto produce significant echoes from strongRegional Anesthesia and Pain Medicine&Volume35,Number3,May-June2010Letters to the Editor。