72898-Control de Vibraciones y sus medidas correctoras
基于转铁蛋白受体(TfR1)的肿瘤与脑部疾病靶向治疗研究进展
基于转铁蛋白受体(TfR1)的肿瘤与脑部疾病靶向治疗研究进展人转铁蛋白受体(TfR1)在不同组织器官中普遍表达,其主要功能是协助转铁蛋白在细胞和血脑屏障内外转运,维持细胞铁平衡。
在肿瘤细胞中以及血脑屏障中,TfR1的表达水平明显高于正常细胞组织,因此,TfR1被认为是肿瘤靶向治疗和脑部疾病靶向治疗的重要靶点。
基于TfR1靶向治疗的药物载体主要有转铁蛋白(Tf)、抗TfR1抗体、TfR1结合肽,这些生物大分子能与TfR1特异性结合,结合之后可以通过受体介导的跨胞转运机制进入细胞或穿过血脑屏障。
将小分子药与这些载体偶联可以促进许多亲水性的化疗药物或神经治疗药物进入肿瘤细胞或血脑屏障,而许多中枢神经治疗性大分子则主要通过融合蛋白的方式与抗TfR1抗体连接转运进入中枢神经系统。
Abstract:Human TfR1 was universally expressed in different tissues. The major function of TfR1 was to facilitate delivery of transferrin across cells and blood-brain barrier(BBB). As a result, iron homo-stasis was maintained. TfR1 was recognised as a critical target for tumor and brain disease therapy due to its over expression in tumor cells and BBB. In recent years, drug carriers based on TfR1 recognition were developed such as Transferrin (Tf), anti-TfR1 antibody and TfR1 binding peptide. These carriers bind to TfR1 specifically and enter into cell or BBB through receptor mediated endocytosis. Chemicals conjugated with these carriers can be facilitated to enter into tumor cells and brain tissue. Therapeutic proteins can be engineered to fused with anti-TfR1 antibody and transported across BBB.Key words:TfR1; Tumor target therapy;Brain directed delivery1轉铁蛋白受体(TfR1)简介转铁蛋白受体(TfR1)是一种在不同组织和细胞系中普遍表达的糖蛋白。
恩曲替尼化学式-概述说明以及解释
恩曲替尼化学式-概述说明以及解释1.引言1.1 概述概述恩曲替尼(英文名称:Entrectinib)是一种靶向抗癌药物,属于酪氨酸激酶抑制剂。
它通过抑制肿瘤细胞中的激酶信号通路,发挥抗肿瘤的作用。
恩曲替尼被广泛应用于非小细胞肺癌、神经母细胞瘤和其他肿瘤的治疗。
该药物的化学性质使其具备出色的抗肿瘤效果。
恩曲替尼的分子式为C31H34Cl2N5O3,分子量为602.54克/摩尔。
其分子结构复杂,由多个不同原子组成的编织网状结构构成。
这种特殊的结构赋予了恩曲替尼优异的特性,包括其强大的抑制肿瘤生长能力和独特的靶向治疗机制。
除了化学性质外,恩曲替尼还具有一系列独特的物理性质。
该药物为白色或类白色结晶粉末,具有极高的纯度要求。
其熔点为210-215,在这个温度范围内可以保持稳定。
此外,恩曲替尼在常温下可溶于一些有机溶剂,如二氯甲烷和二甲基亚砜,但不溶于水。
在药理作用方面,恩曲替尼主要表现出针对肿瘤细胞的抗增殖和抗转移能力。
它通过干扰肿瘤细胞的激酶信号通路,阻止肿瘤细胞的分裂和生长。
此外,恩曲替尼还具有特异性靶向治疗作用,能够选择性地抑制特定的激酶,从而实现精确的治疗效果。
然而,恩曲替尼也存在一些副作用,如恶心、呕吐、疲劳和食欲不振等,这些副作用需在使用时留意并及时处理。
综上所述,恩曲替尼作为一种靶向抗肿瘤药物,具有复杂的化学性质、独特的物理性质以及较广泛的药理作用。
进一步的研究和应用将有助于更好地发掘恩曲替尼的潜力,为肿瘤治疗提供新的突破和可能性。
1.2 文章结构文章结构部分的内容如下:文章结构部分主要介绍了整篇文章的组织结构和内容安排。
本文的目录分为引言、正文和结论三个部分。
引言部分主要是对整篇文章的背景和目的进行概述,并对恩曲替尼的化学式进行引入。
接着,文章结构部分将详细介绍恩曲替尼的化学性质、物理性质和药理作用。
最后,结论部分将对恩曲替尼的化学性质、物理性质和药理作用进行总结。
在正文部分,恩曲替尼的化学性质将包括分子式、分子量和结构式的介绍。
信迪利单抗结合改良DCF方案在胃部恶性肿瘤患者治疗中的应用效果研究

信迪利单抗结合改良DCF方案在胃部恶性肿瘤患者治疗中的应用效果研究吴小珍,胡晓波,戴盈英苏州市第九人民医院药学部,江苏苏州215299[摘要]目的研究在胃部恶性肿瘤患者接受治疗的过程中选择信迪利单抗结合改良DCF方案(多西他赛+顺铂+氟尿嘧啶)方案取得的临床效果。
方法选取2020年3月—2023年3月苏州市第九人民医院收治的72例胃部恶性肿瘤患者作为研究对象,采用随机数表法平均分组,对照组中36例患者接受改良DCF方案来开展治疗,观察组中36例患者在接受改良DCF方案(多西他赛+顺铂+氟尿嘧啶)治疗的同时,应用信迪利单抗治疗。
对比两组治疗效果。
结果治疗后,观察组客观有效率为77.78%,疾病控制率为91.67%,优于对照组的52.78%、72.22%,差异有统计学意义(χ2=4.963、4.560,P<0.05);同时观察组癌胚抗原、糖类抗原、干扰素、白细胞介素等指标更优,差异有统计学意义(P<0.05)。
结论对于胃部恶性肿瘤患者开展治疗期间,信迪利单抗结合改良DCF方案具有良好的治疗效果。
[关键词]信迪利单抗;改良DCF方案;胃部恶性肿瘤;应用效果[中图分类号]R4 [文献标识码]A [文章编号]2096-1782(2023)09(b)-0009-04Efficacy of Sintilimab Combined with Modified DCF Regimen in the Treat⁃ment of Gastric Malignant TumorsWU Xiaozhen, HU Xiaobo, DAI YingyingDepartment of Pharmacy, Suzhou Ninth People's Hospital, Suzhou, Jiangsu Province, 215299 China[Abstract] Objective To study the clinical effect of Sintilimab combined with modified DCF regimen (docetaxel + cis⁃platin + fluorouracil) during the treatment of patients with gastric malignant tumors. Methods A total of seventy-two patients with gastric malignancies treated in Suzhou Ninth People's Hospital from March 2020 to March 2023 were se⁃lected as the study subjects. They were grouped averagely according to random number table method, thirty-six pa⁃tients in the control group received the modified DCF regimen, and thirty-six patients in the observation group re⁃ceived the modified DCF regimen (docetaxel + cisplatin + fluorouracil) at the same time received Sintilimab. The treat⁃ment effects of the two groups were compared. Results After the treatment, the objective effective rate and disease con⁃trol rate of the observation group were 77.78% and 91.67%, which were better than those of the control group (52.78% and 72.22%), and the difference was statistically significant (χ2=4.963, 4.560, P<0.05). The indexes of carcinoembry⁃onic antigen, carbohydrate antigen, interferon and interleukin in the observation group were better, and the differences were statistically significant (P<0.05).Conclusion During the treatment of gastric malignant tumor patients, Sintilimab combined with improved DCF regimen not only has good therapeutic effect.[Key words] Sintilimab; Improved DCF program; Gastric malignancy; Application effect胃部恶性肿瘤是胃肠道恶性肿瘤中占比较高的一种,由于胃部恶性肿瘤的发病相对比较隐匿,因此患者在发病初期很难及时发现病变,在确诊时往往已经处于晚期[1]。
08版依替巴肽注射液国外说明书
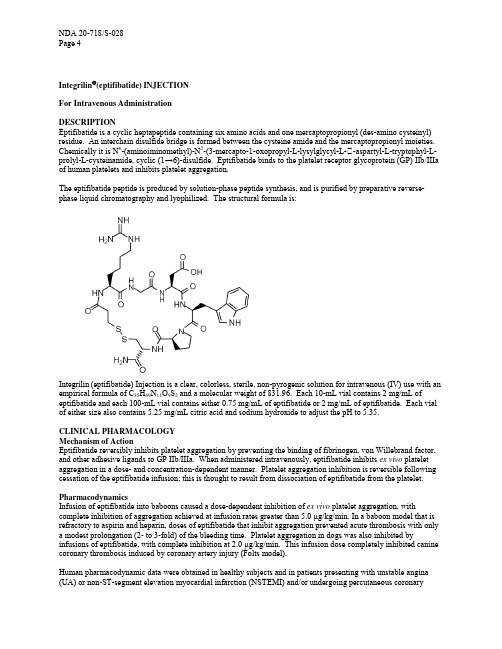
Integrilin®(eptifibatide) INJECTIONFor Intravenous AdministrationDESCRIPTIONEptifibatide is a cyclic heptapeptide containing six amino acids and one mercaptopropionyl (des-amino cysteinyl) residue. An interchain disulfide bridge is formed between the cysteine amide and the mercaptopropionyl moieties. Chemically it is N6-(aminoiminomethyl)-N2-(3-mercapto-1-oxopropyl-L-lysylglycyl-L-�-aspartyl-L-tryptophyl-Lprolyl-L-cysteinamide, cyclic (1→6)-disulfide. Eptifibatide binds to the platelet receptor glycoprotein (GP) IIb/IIIa of human platelets and inhibits platelet aggregation.The eptifibatide peptide is produced by solution-phase peptide synthesis, and is purified by preparative reverse-phase liquid chromatography and lyophilized. The structural formula is:Integrilin (eptifibatide) Injection is a clear, colorless, sterile, non-pyrogenic solution for intravenous (IV) use with an empirical formula of C35H49N11O9S2 and a molecular weight of 831.96. Each 10-mL vial contains 2 mg/mL of eptifibatide and each 100-mL vial contains either 0.75 mg/mL of eptifibatide or 2 mg/mL of eptifibatide. Each vial of either size also contains 5.25 mg/mL citric acid and sodium hydroxide to adjust the pH to 5.35.CLINICAL PHARMACOLOGYMechanism of ActionEptifibatide reversibly inhibits platelet aggregation by preventing the binding of fibrinogen, von Willebrand factor, and other adhesive ligands to GP IIb/IIIa. When administered intravenously, eptifibatide inhibits ex vivo platelet aggregation in a dose- and concentration-dependent manner. Platelet aggregation inhibition is reversible following cessation of the eptifibatide infusion; this is thought to result from dissociation of eptifibatide from the platelet. PharmacodynamicsInfusion of eptifibatide into baboons caused a dose-dependent inhibition of ex vivo platelet aggregation, with complete inhibition of aggregation achieved at infusion rates greater than 5.0 µg/kg/min. In a baboon model that is refractory to aspirin and heparin, doses of eptifibatide that inhibit aggregation prevented acute thrombosis with only a modest prolongation (2- to 3-fold) of the bleeding time. Platelet aggregation in dogs was also inhibited by infusions of eptifibatide, with complete inhibition at 2.0 µg/kg/min. This infusion dose completely inhibited canine coronary thrombosis induced by coronary artery injury (Folts model).Human pharmacodynamic data were obtained in healthy subjects and in patients presenting with unstable angina (UA) or non-ST-segment elevation myocardial infarction (NSTEMI) and/or undergoing percutaneous coronaryinterventions. Studies in healthy subjects enrolled only males; patient studies enrolled approximately one-third women. In these studies, eptifibatide inhibited ex vivo platelet aggregation induced by adenosine diphosphate (ADP) and other agonists in a dose- and concentration-dependent manner. The effect of eptifibatide was observed immediately after administration of a 180-µg/kg intravenous bolus. Table 1 shows the effects of dosing regimens of eptifibatide used in the IMPACT II and PURSUIT studies on ex vivo platelet aggregation induced by 20 µM ADP in PPACK-anticoagulated platelet-rich plasma and on bleeding time. The effects of the dosing regimen used in ESPRIT on platelet aggregation have not been studied.Table 1Platelet Inhibition and Bleeding TimeIMPACT II PURSUIT135/0.5* 180/2.0** Inhibition of platelet aggregation 15 min after bolus 69% 84% Inhibition of platelet aggregation at steady state 40-50% >90% Bleeding-time prolongation at steady state <5x <5x Inhibition of platelet aggregation 4h after infusion discontinuation <30% <50% Bleeding-time prolongation 6h after infusion discontinuation 1x 1.4x* 135-µg/kg bolus followed by a continuous infusion of 0.5 µg/kg/min.** 180-µg/kg bolus followed by a continuous infusion of 2.0 µg/kg/min.The eptifibatide dosing regimen used in the ESPRIT study included two 180-µg/kg bolus doses given 10 minutes apart combined with a continuous 2.0 µg/kg/min infusion.When administered alone, eptifibatide has no measurable effect on prothrombin time (PT) or activated partial thromboplastin time (aPTT) (see also PRECAUTIONS, Drug Interactions section).There were no important differences between men and women or between age groups in the pharmacodynamic properties of eptifibatide. Differences among ethnic groups have not been assessed.PharmacokineticsThe pharmacokinetics of eptifibatide are linear and dose-proportional for bolus doses ranging from 90 to 250 µg/kg and infusion rates from 0.5 to 3.0 µg/kg/min. Plasma elimination half-life is approximately 2.5 hours. Administration of a single 180-µg/kg bolus combined with an infusion produces an early peak level, followed by a small decline prior to attaining steady state (within 4-6 hours). This decline can be prevented by administering a second 180-µg/kg bolus 10 minutes after the first. The extent of eptifibatide binding to human plasma protein is about 25%. Clearance in patients with coronary artery disease is about 55 mL/kg/h. In healthy subjects, renal clearance accounts for approximately 50% of total body clearance, with the majority of the drug excreted in the urine as eptifibatide, deaminated eptifibatide, and other, more polar metabolites. No major metabolites have been detected in human plasma.In patients with moderate to severe renal insufficiency (creatinine clearance <50 mL/min using the Cockcroft-Gault equation), the clearance of eptifibatide is reduced by approximately 50% and steady-state plasma levels approximately doubled (see WARNINGS and DOSAGE AND ADMINISTRATION).Special PopulationsPatients in clinical studies were older (range 20-94 years) than those in the clinical pharmacology studies. Elderly patients with coronary artery disease demonstrated higher plasma levels and lower total body clearance of eptifibatide when given the same dose as younger patients. Limited data are available on lighter weight (<50 kg) patients over 75 years of age.No studies have been conducted in patients with hepatic impairment.Males and females have not demonstrated any clinically significant differences in the pharmacokinetics of eptifibatide.CLINICAL STUDIESEptifibatide was studied in three placebo-controlled, randomized studies. PURSUIT evaluated patients with acute coronary syndromes: unstable angina (UA) or non-ST-segment elevation MI (NSTEMI). Two other studies, ESPRIT and IMPACT II, evaluated patients about to undergo a percutaneous coronary intervention (PCI). Patients underwent primarily balloon angioplasty in IMPACT II and intracoronary stent placement, with or without angioplasty, in ESPRIT.Non-ST-segment Elevation Acute Coronary SyndromeNon-ST-segment elevation acute coronary syndrome is defined as prolonged (≥10 minutes) symptoms of cardiac ischemia within the previous 24 hours associated with either ST-segment changes (elevation between 0.6 mm and 1 mm or depression >0.5 mm), T-wave inversion (>1 mm), or positive CK-MB. This definition includes "unstable angina" and "NSTEMI" but excludes myocardial infarction that is associated with Q waves or greater degrees ofST-segment elevation.PURSUIT (Platelet Glycoprotein IIb/IIIa in Unstable Angina: Receptor Suppression Using Integrilin Therapy)PURSUIT was a 726-center, 27-country, double-blind, randomized, placebo-controlled study in 10,948 patients presenting with UA or NSTEMI. Patients could be enrolled only if they had experienced cardiac ischemia at rest (≥10 minutes) within the previous 24 hours and had either ST-segment changes (elevations between 0.6 mm and 1 mm or depression >0.5 mm), T-wave inversion (>1 mm), or increased CK-MB. Important exclusion criteria included a history of bleeding diathesis, evidence of abnormal bleeding within the previous 30 days, uncontrolled hypertension, major surgery within the previous 6 weeks, stroke within the previous 30 days, any history of3 hemorrhagic stroke, serum creatinine >2.0 mg/dL, dependency on renal dialysis, or platelet count <100,000/mm.Patients were randomized to either placebo, eptifibatide 180-µg/kg bolus followed by a-2.0 µg/kg/min infusion (180/2.0), or eptifibatide 180-µg/kg bolus followed by a 1.3-µg/kg/min infusion (180/1.3). The infusion was continued for 72 hours, until hospital discharge, or until the time of coronary artery bypass grafting (CABG), whichever occurred first, except that if PCI was performed, the eptifibatide infusion was continued for 24 hours after the procedure, allowing for a duration of infusion up to 96 hours.The lower-infusion-rate arm was stopped after the first interim analysis when the two active-treatment arms appeared to have the same incidence of bleeding.Patient age ranged from 20 to 94 (mean 63) years, and 65% were male. The patients were 89% Caucasian, 6% Hispanic, and 5% Black, recruited in the United States and Canada (40%), Western Europe (39%), Eastern Europe (16%), and Latin America (5%).This was a "real world" study; each patient was managed according to the usual standards of the investigational site; frequencies of angiography, PCI, and CABG therefore differed widely from site to site and from country to country. Of the patients in PURSUIT, 13% were managed with PCI during drug infusion, of whom 50% received intracoronary stents; 87% were managed medically (without PCI during drug infusion).The majority of patients received aspirin (75-325 mg once daily). Heparin was administered intravenously or subcutaneously, at the physician's discretion, most commonly as an intravenous bolus of 5000 U followed by a continuous infusion of 1000 U/h. For patients weighing less than 70 kg, the recommended heparin bolus dose was 60 U/kg followed by a continuous infusion of 12 U/kg/h. A target aPTT of 50 to 70 seconds was recommended. A total of 1250 patients underwent PCI within 72 hours after randomization, in which case they received intravenous heparin to maintain an activated clotting time (ACT) of 300 to 350 seconds.The primary endpoint of the study was the occurrence of death from any cause or new myocardial infarction (MI) (evaluated by a blinded Clinical Endpoints Committee) within 30 days of randomization.Compared to placebo, eptifibatide administered as a 180-µg/kg bolus followed by a 2.0-µg/kg/min infusion significantly (P=0.042) reduced the incidence of endpoint events (see Table 2). The reduction in the incidence of endpoint events in patients receiving eptifibatide was evident early during treatment, and this reduction was maintained through at least 30 days (see Figure 1). Table 2 also shows the incidence of the components of the primary endpoint, death (whether or not preceded by an MI) and new MI in surviving patients at 30 days.Table 2Clinical Events In The PURSUIT StudyPlacebo Eptifibatide (180/2.0) P-value(n = 4739) (n = 4722)Death or MI n (%)7 days 552 (11.6%) 477 (10.1%) 0.01630 daysDeath or MI (Primary Endpoint) 745 (15.7%) 672 (14.2%) 0.042 Death 177 (3.7%) 165 (3.5%)Nonfatal MI 568 (12.0%) 507 (10.7%)Figure 1: Kaplan-Meier Plot of Time to Death or Myocardial Infarction Within 30 Days of RandomizationTreatment with eptifibatide prior to determination of patient management strategy reduced clinical events regardless of whether patients ultimately underwent diagnostic catheterization, revascularization (i.e., PCI or CABG surgery) or continued to receive medical management alone. Table 3 shows the incidence of death or MI within 72 hours.Table 3Clinical Events (Death or MI) in the PURSUIT Study Within 72 Hours of Randomization180/2.0Overall Patient Population n =4739 n =4722– At 72 hours7.6%5.9%Patients undergoing early PCI n =631 n =619– Pre-procedure (nonfatal MI only) 5.5% 1.8% – At 72 hours14.4%9.0%Patients not undergoing early PCI n =4108 n =4103– At 72 hours6.5%5.4%All of the effect of eptifibatide was established within 72 hours (during the period of drug infusion), regardless ofmanagement strategy. Moreover, for patients undergoing early PCI, a reduction in events was evident prior to theprocedure. An analysis of the results by sex suggests that women who would not routinely be expected to undergo percutaneouscoronary intervention (PCI) receive less benefit from eptifibatide (95% confidence limits for relative risk of 0.94 to 1.28) than do men (0.72 to 0.90). This difference may be a true treatment difference, the effect of other differencesin these subgroups, or a statistical anomaly. No differential outcomes were seen between male and female patientsundergoing PCI(see results for ESPRIT). Follow-up data were available through 165 days for 10,611 patients enrolled in the PURSUIT trial (96.9 percent of the initial enrollment). This follow-up included 4566 patients who received eptifibatide at the 180/2.0 dose. As reported by the investigators, the occurrence of death from any cause or new myocardial infarction for patients followed for at least 165 days was reduced from 13.6 percent with placebo to 12.1 percent with eptifibatide 180/2.0. Percutaneous Coronary InterventionIMPACT II (Integrilin to Minimize Platelet Aggregation and Prevent Coronary Thrombosis II) IMPACT II was a multicenter, double-blind, randomized, placebo-controlled study conducted in the United States in 4010 patients undergoing PCI. Major exclusion criteria included a history of bleeding diathesis, major surgery within 6 weeks of treatment, gastrointestinal bleeding within 30 days, any stroke or structural CNS abnormality, 3uncontrolled hypertension, PT >1.2 times control, hematocrit <30%, platelet count <100,000/mm , and pregnancy.Patient age ranged from 24 to 89 (mean 60) years, and 75% were male. The patients were 92% Caucasian, 5% Black, and 3% Hispanic. Forty-one percent of the patients underwent PCI for ongoing ACS. Patients were randomly assigned to one of three treatment regimens, each incorporating a bolus dose initiated immediately prior to PCI followed by a continuous infusion lasting 20 to 24 hours: 1) 135-µg/kg bolus followed by a continuous infusion of 0.5 µg/kg/min of eptifibatide (135/0.5); 2) 135-µg/kg bolus followed by a continuous infusion of 0.75-µg/kg/min of eptifibatide (135/0.75); or 3) a matching placebo bolus followed by a matching placebo continuous infusion.Each patient received aspirin and an intravenous heparin bolus of 100 U/kg, with additional bolus infusions of up to2000 additional units of heparin every 15 minutes to maintain an activated clotting time (ACT) of 300 to 350seconds.The primary endpoint was the composite of death, MI, or urgent revascularization, analyzed at 30 days afterrandomization in all patients who received at least one dose of study drug.As shown in Table 4, each eptifibatide regimen reduced the rate of death, MI, or urgent intervention, although at 30days, this finding was statistically significant only in the lower-dose eptifibatide group.As in the PURSUIT study, the effects of eptifibatide were seen early and persisted throughout the 30-day period.Table 4Clinical Events in the IMPACT II StudyEptifibatide EptifibatidePlacebo(135/0.5) (135/0.75)n (%) n (%) n (%)Abrupt(3.3%)Closure 65 (5.1%) 36 (2.8%) 43 P-value vs placebo 0.003 0.030Death, MI, or Urgent Intervention24 hours 123 (9.6%) 86 (6.6%) 89 (6.9%)P-value vs placebo 0.006 0.01448 hours 131 (10.2%) 99 (7.6%) 102 (7.9%)P-value vs placebo 0.021 0.04530 days (primary endpoint) 149 (11.6%) 118 (9.1%) 128 (10.0%)P-value vs placebo 0.035 0.179Death or MI30 days 110 (8.6%) 89 (6.8%) 95 (7.4%)P-value vs placebo 0.102 0.272(10.3%)*6 months 151 (11.9%)* 136 (10.6%)* 130P-value vs placebo 0.297 0.182* Kaplan-Meier estimate of event rate.ESPRIT (Enhanced Suppression of the Platelet IIb/IIIa Receptor with Integrilin Therapy)The ESPRIT study was a multicenter, double-blind, randomized, placebo-controlled study conducted in the United States and Canada that enrolled 2064 patients undergoing elective or urgent PCI with intended intracoronary stent placement. Exclusion criteria included MI within the previous 24 hours, ongoing chest pain, administration of any oral anti-platelet or oral anticoagulant other than aspirin within 30 days of PCI (although loading doses of thienopyridine on the day of PCI were encouraged), planned PCI of a saphenous vein graft or subsequent “staged” PCI, prior stent placement in the target lesion, PCI within the previous 90 days, a history of bleeding diathesis, major surgery within 6 weeks of treatment, gastrointestinal bleeding within 30 days, any stroke or structural CNS3 abnormality, uncontrolled hypertension, PT >1.2 times control, hematocrit <30%, platelet count <100,000/mm, and pregnancy.Patient age ranged from 24 to 93 (mean 62) years and 73% of patients were male. The study enrolled 90% Caucasian, 5% African American, 2% Hispanic and 1% Asian patients. Patients received a wide variety of stents. Patients were randomized either to placebo or eptifibatide administered as an intravenous bolus of 180 µg/kg followed immediately by a continuous infusion of 2.0 µg/kg/min, and a second bolus of 180 µg/kg administered 10 minutes later (180/2.0/180). Eptifibatide infusion was continued for 18 to 24 hours after PCI or until hospital discharge, whichever came first. Each patient received at least one dose of aspirin (162-325 mg) and 60 U/kg of heparin as a bolus (not to exceed 6000 Units) if not already receiving a heparin infusion. Additional boluses of heparin (10-40 U/kg) could be administered in order to reach a target ACT between 200 and 300 seconds.The primary endpoint of the ESPRIT study was the composite of death, MI, urgent target vessel revascularization (UTVR) and “bailout” to open label eptifibatide due to a thrombotic complication of PCI (TBO) (e.g., visible thrombus, “no reflow,” or abrupt closure) at 48 hours. MI, UTVR and TBO were evaluated by a blinded Clinical Events Committee.As shown in Table 5, the incidence of the primary endpoint and selected secondary endpoints was significantly reduced in patients who received eptifibatide. A treatment benefit in patients who received eptifibatide was seen by 48 hours and at the end of the 30-day observation period.Table 5Clinical Events in the ESPRIT StudyPlacebo(n=1024) Death, MI, Urgent Target Vessel Revascularization, or Thrombotic “Bailout”48 Hours (primary endpoint) 30 Days 108 (10.5%) 120 (11.7%)Death, MI, or Urgent Target Vessel Revascularization Eptifibatide180/2.0/180(n=1040)69 (6.6%)78 (7.5%)Relative Risk(95% CI)0.629 (0.471,0.840)0.640 (0.488,0.840)P-Value0.00150.001148 Hours95 (9.3%) 62 (6.0%) 0.643 (0.472, 0.004530 Days (key secondary 107 (10.4%) 71 (6.8%) 0.875) 0.0034 endpoint) 0.653 (0.490,0.871)Death or MI48 Hours94 (9.2%) 57 (5.5%) 0.597 (0.435, 0.001330 Days 104 (10.2%) 66 (6.3%) 0.820) 0.00160.625 ( 0.465,0.840)The need for thrombotic “bailout” was significantly reduced with eptifibatide at 48 hours (2.1% for placebo, 1.0% for eptifibatide; P=0.029). Consistent with previous studies of GP IIb/IIIa inhibitors, most of the benefit achieved acutely with eptifibatide was in the reduction of MI. Eptifibatide reduced the occurrence of MI at 48 hours from 9.0% for placebo to 5.4% (P=0.0015) and maintained that effect with significance at 30 days.There was no treatment difference with respect to sex in ESPRIT. Eptifibatide reduced the incidence of the primary endpoint in both men (95% confidence limits for relative risk: 0.54, 1.07) and women (0.24, 0.72) at 48 hours. Follow-up (12-month) mortality data were available for 2024 patients (1017 on eptifibatide) enrolled in the ESPRIT trial (98.1% of the initial enrollment). Twelve-month clinical event data were available for 1964 patients (988 on eptifibatide) representing 95.2% of the initial enrollment. As shown in Table 6, the treatment effect of eptifibatide seen at 48 hours and30 days appeared preserved at 6 months and 1 year. Most of the benefit was in reduction of MI.Table 6Clinical Events at 6 months and 1 year in the ESPRIT StudyPlacebo Eptifibatide Hazard Ratio180/2.0/180(n=1024) (n=1040) (95% CI)Death, MI, or Target Vessel Revascularization6 Months187 (18.5%) 146 (14.3%) 0.744 (0.599, 0.924)1 Year 222 (22.1%) 178 (17.5%) 0.762 (0.626, 0.929)Death, MI6 Months117 (11.5%) 77 (7.4%) 0.631 (0.473, 0.841)1 Year 126 (12.4%) 83 (8.0%) 0.630 (0.478, 0.832) Percentages are Kaplan-Meier event rates.INDICATIONS AND USAGEIntegrilin is indicated:• For the treatment of patients with acute coronary syndrome (unstable angina/non-ST- segment elevation myocardial infarction), including patients who are to be managed medically and those undergoing percutaneous coronary intervention (PCI). In this setting, Integrilin has been shown to decrease the rate of a combinedendpoint of death or new myocardial infarction.• For the treatment of patients undergoing PCI, including those undergoing intracoronary stenting. In this setting, Integrilin has been shown to decrease the rate of a combined endpoint of death, new myocardial infarction, or need for urgent intervention.In the IMPACT II, PURSUIT and ESPRIT studies of eptifibatide, most patients received heparin and aspirin (see CLINICAL STUDIES).CONTRAINDICATIONSTreatment with eptifibatide is contraindicated in patients with:• A history of bleeding diathesis, or evidence of active abnormal bleeding within the previous 30 days.• Severe hypertension (systolic blood pressure >200 mm Hg or diastolic blood pressure >110 mm Hg) not adequately controlled on antihypertensive therapy.• Major surgery within the preceding 6 weeks.• History of stroke within 30 days or any history of hemorrhagic stroke.• Current or planned administration of another parenteral GP IIb/IIIa inhibitor.• Dependency on renal dialysis.• Known hypersensitivity to any component of the product.WARNINGSBleedingBleeding is the most common complication encountered during eptifibatide therapy. Administration of eptifibatide is associated with an increase in major and minor bleeding, as classified by the criteria of the Thrombolysis in Myocardial Infarction Study group (TIMI) (see ADVERSE REACTIONS). Most major bleeding associated with eptifibatide has been at the arterial access site for cardiac catheterization or from the gastrointestinal or genitourinary tract.In patients undergoing percutaneous coronary interventions, patients receiving eptifibatide experience an increased incidence of major bleeding compared to those receiving placebo without a significant increase in transfusion requirement. Special care should be employed to minimize the risk of bleeding among these patients (see PRECAUTIONS). If bleeding cannot be controlled with pressure, infusion of eptifibatide and concomitant heparin should be stopped immediately.Renal InsufficiencyApproximately 50% of eptifibatide is cleared by the kidney in patients with normal renal function. Total drug clearance is decreased by approximately 50% and steady-state plasma eptifibatide concentrations are doubled in patients with an estimated creatinine clearance <50 mL/min (using the Cockcroft-Gault equation). Therefore, the infusion dose should be reduced to 1 µg/kg/min in such patients (see DOSAGE AND ADMINISTRATION). There has been no clinical experience in patients dependent on dialysis.Platelet Count <100,000/mm3Because it is an inhibitor of platelet aggregation, caution should be exercised when administering eptifibatide to patients with a platelet count <100,000/mm3; there has been no clinical experience with eptifibatide initiated in patients with a platelet count <100,000/mm3.PRECAUTIONSBleeding PrecautionsCare of the Femoral Artery Access Site in Patients Undergoing Percutaneous Coronary Intervention (PCI)In patients undergoing PCI, treatment with eptifibatide is associated with an increase in major and minor bleeding at the site of arterial sheath placement. After PCI, eptifibatide infusion should be continued until hospital discharge or up to 18 to 24 hours, whichever comes first. Heparin use is discouraged after the PCI procedure. Early sheath removal is encouraged while eptifibatide is being infused. Prior to removing the sheath, it is recommended thatheparin be discontinued for 3 to 4 hours and an aPTT of <45 seconds or ACT <150 seconds be achieved. In any case, both heparin and eptifibatide should be discontinued and sheath hemostasis should be achieved at least 2 to 4 hours before hospital discharge.Use of Thrombolytics, Anticoagulants, and Other Antiplatelet AgentsIn the IMPACT II, PURSUIT, and ESPRIT studies, eptifibatide was used concomitantly with unfractionated heparin and aspirin (see CLINICAL STUDIES). In the ESPRIT study, clopidogrel or ticlopidine were used routinely starting the day of PCI. Because eptifibatide inhibits platelet aggregation, caution should be employed when it is used with other drugs that affect hemostasis, including thrombolytics, oral anticoagulants, nonsteroidal anti-inflammatory drugs, and dipyridamole. To avoid potentially additive pharmacologic effects, concomitant treatment with other inhibitors of platelet receptor GP IIb/IIIa should be avoided.There is only a small experience with concomitant use of eptifibatide and thrombolytics. In a study of 180 patients with acute myocardial infarction (AMI), eptifibatide (in regimens up to a bolus of 180 µg/kg followed by a continuous infusion of 0.75 µg/kg/min for 24 hours) was administered concomitantly with the approved "accelerated" regimen of alteplase, a thrombolytic agent. The studied regimens of eptifibatide did not increase the incidence of major bleeding or transfusion compared to the incidence seen when alteplase was given alone.In the IMPACT II study, 15 patients received a thrombolytic agent in conjunction with the 135/0.5 dosing regimen, 2 of whom experienced a major bleed. In the PURSUIT study, 40 patients who received eptifibatide at the 180/2.0 dosing regimen received a thrombolytic agent, 10 of whom experienced a major bleed.In another AMI study involving 181 patients, eptifibatide (in regimens up to a bolus of 180 µg/kg followed by a continuous infusion of up to 2.0 µg/kg/min for up to 72 hours) was administered concomitantly with streptokinase (1.5 million units over 60 minutes), another thrombolytic agent. At the highest studied infusion rates (1.3 µg/kg/min and 2.0 µg/kg/min), eptifibatide was associated with an increase in the incidence of bleeding and transfusions compared to the incidence seen when streptokinase was given alone.These limited data on the use of eptifibatide in patients receiving thrombolytic agents do not allow an estimate of the bleeding risk associated with concomitant use of thrombolytics. Systemic thrombolytic therapy should be used with caution in patients who have received eptifibatide.Minimization of Vascular and Other TraumaArterial and venous punctures, intramuscular injections, and the use of urinary catheters, nasotracheal intubation, and nasogastric tubes should be minimized. When obtaining intravenous access, noncompressible sites (e.g., subclavian or jugular veins) should be avoided.Laboratory TestsBefore infusion of eptifibatide, the following laboratory tests should be performed to identify preexisting hemostatic abnormalities: hematocrit or hemoglobin, platelet count, serum creatinine, and PT/aPTT. In patients undergoing PCI, the activated clotting time (ACT) should also be measured.Maintaining Target aPTT and ACTThe aPTT should be maintained between 50 and 70 seconds unless PCI is to be performed. In patients treated with heparin, bleeding can be minimized by close monitoring of the aPTT. Table 7 displays the risk of major bleeding according to the maximum aPTT attained within 72 hours in the PURSUIT study.。
DERSIMELAGON 产品说明书

488 Scientific AbstractsSystemic sclerosis, myositis and related syndromes - aetiology, pathogenesis and animal modelsPOS0467 DERSIMELAGON, A NOVEL ORAL MELANOCORTIN1 RECEPTOR AGONIST, DEMONSTRATES DISEASE-MODIFYING EFFECTS IN PRECLINICAL MODELS OFSYSTEMIC SCLEROSISM. Kondo1, T. Suzuki1, Y. Kawano1, S. Kojima2, M. Miyashiro1, A. Matsumoto1, G. Kania3, P. Blyszczuk3, R. Ross4, P. Mulipa4, F. Del Galdo4, Y. Zhang5, J. H. W. Distler5. 1Mitsubishi T anabe Pharma Corporation, Research Unit/Immunology & Inflammation, Souyaku Innovative Research Division, Y okohama, Japan;2Mitsubishi T anabe Pharma Corporation, Discovery T echnology Laboratories, Souyaku Innovative Research Division, Y okohama, Japan;3University Hospital Zurich, University of Zurich, Center of Experimental Rheumatology, Department of Rheumatology, Schlieren, Switzerland;4University of Leeds, Leeds Instituteof Rheumatic and Musculoskeletal Medicine, Faculty of Medicine and Health, Leeds, United Kingdom;5Friedrich-Alexander-University Erlangen-Nürnberg (FAU) and University Hospital Erlangen, Department of Internal Medicine 3—Rheumatology and Immunology, Erlangen, GermanyBackground: Activation of melanocortin 1 receptor (MC1R) is known to have broad anti-inflammatory and anti-fibrotic effects. The bleomycin (BLM)-induced skin fibrosis murine model is well-established for systemic sclerosis (SSc). α-mel-anocyte-stimulating hormone, an endogenous ligand of MC1R, inhibits skin fibro-sis and MC1R knock-out enhances skin fibrosis in this model. These pieces of evidence suggest that MC1R agonism has potential in the treatment of SSc. Objectives: Dersimelagon phosphate (MT-7117) is an investigational small molecule that is an orally administered, selective agonist for MC1R. The purpose of this study is to investigate the potential of MT-7117 as a therapeutic agent for SSc by evaluat-ing its efficacy and mechanism of action in complementary preclinical models. The expression and distribution of MC1R in the skin of SSc patients was investigated. Methods: The effects of MT-7117 on skin fibrosis and lung inflammation were eval-uated in BLM-induced SSc murine models that were optimized for prophylactic and therapeutic evaluation. Microarray-based gene expression analysis and serum pro-tein profiling were performed to investigate the mechanism of action of MT-7117 in the BLM-induced SSc models. The effect of MT-7117 on TGF-β-induced activation of human dermal fibroblasts was evaluated in vitro. Immunohistochemical analyses of MC1R expression in skin samples from SSc patients were performed. Results: Prophylactic treatment with MT-7117 (≥0.3 mg/kg/day p.o.) significantly inhibited the increase in collagen content of the skin, the serum level of sur-factant protein D, and the weight of the lungs from BLM-induced skin fibrosis and lung inflammation model. Therapeutic treatment with MT-7117 (≥3 mg/kg/ day p.o.) significantly suppressed skin thickening and the numbers of myofi-broblasts in pre-established BLM-induced skin fibrosis model. Gene array anal-ysis using the BLM-induced SSc model demonstrated changes in numerous categories related to macrophages, monocytes, and neutrophils, followed by endothelial cell-related categories after treatment with MT-7117. In the analy-sis that focused on biological functions, categories of inflammatory response, activation of antigen-presenting cells, angiogenesis, atherosclerosis, vascu-logenesis, and vaso-occlusion were suppressed by MT-7117. In the analysis that focused on molecular signaling pathways, triggering receptor expressed on myeloid cells-1, IL-6, and oncostatin M involved in inflammation, and perox-isome proliferator-activated receptor that is related to fibrosis were all affected by MT-7117. Serum protein profiling using BLM-induced SSc model revealed that multiple SSc-related biomarkers including P-selectin, osteoprotegerin, cys-tatin C, growth and differentiation factor-15 and S100A9 were suppressed by MT-7117. MT-7117 inhibited the activation of human dermal fibroblasts by sup-pressing TGF-β-induced ACTA2 (encoding α-smooth muscle actin) mRNA ele-vation in vitro. Immunohistochemical analyses showed that MC1R positivity was observed in 40 of 50 diffuse cutaneous SSc patients. MC1R was expressed by monocytes/macrophages, neutrophils, blood vessels (endothelial cells), fibro-blasts, and epidermis (keratinocytes) in the skin of SSc patients. Conclusion: MT-7117 demonstrates disease-modifying effects in preclinical mod-els of SSc. Investigations of its mechanism of action and target expression anal-yses indicate that MT-7117 exerts its positive effects by affecting the pathologies of inflammation, vascular dysfunction, and fibrosis through inflammatory cells, endothelial cells, and fibroblasts. In view of its potent beneficial impact on all these three main pathologies of SSc, MT-7117 is a potential therapeutic agent for the treatment of clinically challenging SSc, which has diverse and difficult to treat symp-toms. A phase 2 clinical trial investigating the efficacy and tolerability of MT-7117 in patients with early, progressive diffuse cutaneous SSc is currently in progress. Disclosure of Interests: Masahiro Kondo Employee of: Mitsubishi Tanabe Pharma Corporation, Tsuyoshi Suzuki Employee of: Mitsubishi Tanabe Pharma Corporation, Yuko Kawano Employee of: Mitsubishi Tanabe Pharma Corpora-tion, Shinji Kojima Employee of: Mitsubishi Tanabe Pharma Corporation, Masa-hiko Miyashiro Employee of: Mitsubishi Tanabe Pharma Corporation, Atsuhiro Matsumoto Employee of: Mitsubishi Tanabe Pharma Corporation, Gabriela Kania: None declared, Przemyslaw Blyszczuk: None declared, rebecca ross:None declared, Panji Mulipa: None declared, Francesco Del Galdo Grant/ research support from: Prof. F. Del Galdo received fees and research supportfrom Abbvie, AstraZeneca, Boehringer-Ingelheim, Capella, Chemomab, Kymab, Janssen and Mitsubishi-Tanabe., Yun Zhang: None declared, Jörg H.W. DistlerGrant/research support from: Prof. J.H.W. Distler received consulting fees, lec-ture fees, and/or honoraria from Actelion, Active Biotech, Anamar, ARXX, aTyr,Bayer Pharma, Boehringer Ingelheim, Celgene, Galapagos, GSK, Inventiva, JB Therapeutics, Medac, Pfizer, Sanofi-Aventis, RedX, RuiYi and UCB. J. H. W.Distler is stock owner of 4D Science and Scientific head of FibroCure.DOI: 10.1136/annrheumdis-2022-eular.29POS0468 EXTRACELLULAR VESICLES FROM SERUM OFMYOSITIS PATIENTS AS CIRCULATING BIOMARKERSAND DISEASE MEDIATORSS. Kivity1,2, H. Kravitz3, C. Cohen3, D. Margoulis3, M. Amar3, G. Kazimirsky3,D. Ozeri4, A. Dori5, C. Brodie3. 1Meir Medical Center, Rheumatology Unit, KefarSava, Israel;2T el Aviv University, Sackler faculty of Medicine, T el Aviv-Y afo, Israel;3Bar-Ilan University, The Mina and Everard Goodman Faculty of Life Sciences,Ramat Gan, Israel;4T el-HaShomer The Sheba Medical Center, ZabludowiczCenter for Autoimmune Disease, Ramat Gan, Israel;5T el-HaShomer The ShebaMedical Center, Department of Neurology, T alpiot Medical Leadership Program,Sackler Faculty of Medicine, T el Aviv University, Ramat Gan, IsraelBackground: Inflammatory myopathies (IM) are a heterogeneous group of disor-ders characterized by autoimmune inflammatory destruction of skeletal muscles.It is many times associated with lung, skin and joint involvement. Identifying bio-markers that can differentiate IM from other muscle disorders may elucidate the pathophysiology of IM, guide novel therapies, monitor disease activity/responseto treatments and predict prognosis. Exosomes are membrane-bound nanove-sicles with diameters of 30-150 nm that contain multiple proteins, nucleic acid,lipids and other molecules in a tissue- and cell-specific manner. Exosomes are secreted by a large variety of cells, play major roles in cell-cell interactions, andhave recently emerged as circulating biomarkers in a variety of pathological con-ditions, including several autoimmune diseases.Objectives: To characterize exosomes from serum of IM patients, analyze pro-tein expression and study their potential mediators of disease pathologies.Methods: Serum was collected from patients suffering from IM(n=5) and from patients suffering from Becker (BMD) and Duchenne (DMD) muscular dystro-phies (n=6). Exosomes were isolated by Exoquick precipitation and analyzedfor size distribution and by nanoparticle tracking analysis (NTA) and by Westernblot for exosome markers. The effects of the isolated EVs on human satellitecell proliferation and differentiation and macrophage activation were examined. Results: Exosomes from IM patients decreased human satellite cell proliferation (51%, P<0.01) and inhibited their myogenic differentiation as indicated by lower fusionindex (24% inhibition, P<0.01) and expression of myosin heavy chain (72% inhibi-tion, P<0.001). Similar results were obtained also with exosomes derived from DMDand BMD patients; however, their inhibitory effect were more pronounced on MyoG expression. T reatment of macrophages with exosomes from IM patients significantly increased the expression of IL-10 (3-fold, P<0.001), compared to exosomes of healthy controls and DMD patients. Another significant difference was in the expression of sig-naling molecules: Thus, exosomes from BMD patients increased the phosphorylationof Erk and p38, whereas a smaller effect was induced by IM exosomes.Conclusion: Exosomes from IM patients decrease satellite cell proliferationand myogenic differentiation compared to healthy exosomes. In addition, these exosomes increased the expression of IL-10 in macrophages. These effects areunique to exosomes of IM patients compared to muscular dystrophies. These promising results suggest that serum exosomes should be further investigatedas a novel biomarker with potential therapeutic implications.Disclosure of Interests: Shaye Kivity Speakers bureau: BI, Abbvie, Lilly, Pfizer, Janssen, Neopharm, Grant/research support from: Sobi, Haya Kravitz: None declared, Coral Cohen: None declared, Darya Margoulis: None declared, MosheAmar: None declared, Gila Kazimirsky: None declared, David Ozeri Speakers bureau: Neopharm, Consultant of: Abbvie, Amir Dori Grant/research supportfrom: Biogen, Chaya Brodie Grant/research support from: Biogen.DOI: 10.1136/annrheumdis-2022-eular.63POS0469 ENDOTHELIAL TO MESENCHYMAL TRANSITIONAND SENESCENCE ARE PART OF THE FIBROTICPATHOGENESIS IN SYSTEMIC SCLEROSISY. H. Chiu1,2, J. Spierings1, J. M. Van Laar1, J. De Vries-Bouwstra3, M. VanDijk4, R. Goldschmeding4. 1University Medical Center Utrecht, Departmentof Rheumatology and Clinical Immunology, Utrecht, Netherlands;2T ri-ServiceGeneral Hospital, Division of Rheumatology/Immunology/Allergy, T aipei, T aiwan, Republic of China;3Leiden University Medical Center, The Department of on December 24, 2023 by guest. Protected by copyright./ Ann Rheum Dis: first published as 10.1136/annrheumdis-2022-eular.29 on 23 May 2022. Downloaded from。
血清同型半胱氨酸及心肌酶水平与精神分裂症的相关性研究

血清同型半胱氨酸及心肌酶水平与精神分裂症的相关性研究发布时间:2022-07-29T12:28:18.817Z 来源:《中国医学人文》2022年3月3期作者:孔培超[导读]血清同型半胱氨酸及心肌酶水平与精神分裂症的相关性研究孔培超(佛山市第三人民医院;广东佛山 528041)摘要:目的探讨精神分裂症患者血清同型半胱氨酸(HCY)及心肌酶水平的相关性,为临床对于精神分裂症诊治和病情观察提供参考价值。
方法选取2020年7月到2021年6月在我院住院治疗的50例精神分裂症患者作为观察组,另选50例同期在我院健康体检者作为对照组,所有研究对象均进行HCY及心肌酶水平检测,并用阳性及阴性症状量表(PANSS)对观察组患者进行病情评估。
结果观察组HCY、天冬氨酸氨基转移酶(AST)、乳酸脱氢酶(LDH)、肌酸磷酸激酶(CK)、肌酸激酶同工酶(CK-MB)水平均显著高于对照组,差异具有统计学意义(P<0.05);观察组患者血清HCY、CK、CK-MB水平与PANSS评分均呈正相关(P<0.05)。
结论精神分裂症患者血清HCY、AST、LDH、CK、CK-MB水平升高,HCY、CK、CK-MB水平与精神分裂症病情严重程度呈正相关。
关键词:精神分裂症;同型半胱氨酸;心肌酶;相关性研究Correlation between levels of serum homocysteine and myocardial enzyme and schizophrenia Abstract: Objective To explore the correlation of serum homocysteine (HCY) and myocardial enzyme levels in schizophrenia patients, and to provide a reference value for the clinical diagnosis and treatment and observation of schizophrenia. Methods 50 patients with schizophrenia hospitalized in our hospital from July 2020 to June 2021 were selected as the observation group, and 50 patients were examined in our hospital as the control group. All study subjects were tested for HCY and myocardial enzyme level, and the observation group were evaluated with the positive and negative symptom scale (PANSS).Results The levels of Hcy, aspartate aminotransferase (AST), lactate dehydrogenase (LDH), creatine phosphokinase (CK) and creatine kinase isoenzyme (CK-MB) in the observation group were significantly higher than those in the control group (P<0.05). he levels of serum Hcy, CK and CK-MB in the observation group were positively correlated with PANSS score (P<0.05).Conclusion The serum levels of HCY, AST, LDH, CK, and CK-MB were increased, and the HCY, CK, and CK-MB levels were positively associated with the severity of schizophrenia. Key words: schizophrenia; homocysteine; myocardial enzyme; correlation study精神分裂症是目前临床尚未明确病因、发病机制的一种常见精神疾病,青壮年患者较为常见,临床症状主要为意识、情感、智能、知觉等方面出现功能障碍,个体差异大、病情反复[1]。
Trodelvy产品说明书
Trodelvy® (sacituzumab govitecan‐hziy)(Intravenous)Document Number: MH‐0532 Last Review Date: 03/01/2022Date of Origin: 06/02/2020Dates Reviewed: 06/2020, 09/2020, 01/2021, 05/2021, 03/2022I.Length of AuthorizationCoverage will be provided for six months and may be renewed.II.Dosing LimitsA.Quantity Limit (max daily dose) [NDC Unit]:∙Trodelvy 180 mg single-dose vial:12 vials every 21 daysB.Max Units (per dose and over time) [HCPCS Unit]:∙432 billable units weekly for two doses every 21 daysIII.Initial Approval Criteria 1Coverage is provided in the following conditions:Submission of medical records (chart notes) related to the medical necessity criteriais REQUIRED on all requests for authorizations. Records will be reviewed at thetime of submission. Please provide documentation related to diagnosis, steptherapy, and clinical markers (i.e. genetic and mutational testing) supportinginitiation when applicable. Medical records may be submitted via direct uploadthrough the PA web portal or by fax.∙Patient at least 18 years of age; ANDUniversal Criteria 1∙Therapy will NOT be substituted for or used in combination with irinotecan; AND∙Patients that are homozygous for the uridine diphosphate-glucuronosyl transferase 1A1 (UGT1A1)*28 allele will be closely monitored for adverse reactions; AND∙Therapy will not be used in combination with UGT1A1 inhibitors (e.g., nilotinib, regorafenib, etc.) or inducers (e.g., phenytoin, carbamazepine, etc.); AND∙Used as single agent therapy; ANDBreast Cancer † ‡ 1-3∙Patient has unequivocal triple-negative disease [TNBC] (i.e., estrogen, progesterone, and HER2-negative)*; AND∙Patient was previously treated with at least two systemic therapies, at least one of them for metastatic disease; ANDo Patient has recurrent unresectable, locally advanced, or metastatic disease; ORo Patient has inflammatory breast cancer with no response to preoperative systemic therapyUrothelial Cancer (Bladder Cancer)† ‡ 1,2,10∙Patient has one of the following diagnoses:o Locally advanced or metastatic urothelial carcinoma; ORo Muscle invasive bladder cancer with local recurrence or persistent disease in a preserved bladder ‡; ORo Metastatic or local bladder cancer recurrence post-cystectomy ‡; ORo Primary carcinoma of the urethra ‡; ANDUsed for recurrent (excluding recurrence of stage T3-4 disease or palpable inguinal lymph nodes) or metastatic disease; ORo Metastatic upper genitourinary (GU) tract tumors ‡; ORo Metastatic urothelial carcinoma of the prostate ‡; AND∙Patient was previously treated with platinum-containing chemotherapy and programmed death (PD-1 or PD-L1)-directed therapy (e.g., avelumab, nivolumab, atezolizumab,durvalumab, etc.)† FDA approved indication(s); ‡ Compendia Recommended Indication(s); Ф Orphan Drug∙Immunohistochemistry (IHC) assay is 0 or 1+; OR∙Dual-probe in situ hybridization (ISH) assay indicating (Group 5) HER2/CEP17 ratio <2.0 AND average HER2 copy number <4.0 signals/cell; OR∙Concurrent dual-probe ISH and IHC assay results indicating one of the following: o(Group 2) HER2/CEP17 ratio ≥2.0 AND average HER2 copy number <4.0 signals/cell and concurrent IHC 0-1+ or 2+; ORo(Group 3) HER2/CEP17 ratio <2.0 AND average HER2 copy number ≥6.0 signals/cell and concurrent IHC 0-1+; ORo(Group 4) HER2/CEP17 ratio <2.0 AND average HER2 copy number ≥4.0 and <6.0 signals/cell and concurrent IHC 0-1+ or 2+9∙Immunohistochemistry (IHC) assay: Sample is considered ER/PR negative if the percentage of cancer cells staining on evaluation is <1% OR 0% of tumor cell nuclei are immunoreactiveNote: A sample may be deemed uninterpretable for ER or PR if the sample is inadequate(insufficient cancer or severe artifacts present, as determined at the discretion of thepathologist), if external and internal controls (if present) do not stain appropriately, or ifpre-analytic variables have interfered with the assay’s accuracy.IV.Renewal Criteria 1Coverage can be renewed based upon the following criteria:∙Patient continues to meet universal and other indication-specific relevant criteria such as concomitant therapy requirements (not including prerequisite therapy), performancestatus, etc. identified in section III; AND∙Disease response with treatment as defined by stabilization of disease or decrease in size of tumor or tumor spread; AND∙Absence of unacceptable toxicity from the drug. Examples of unacceptable toxicity include: severe hypersensitivity and infusion-related reactions, severe nausea/vomiting, severeneutropenia/febrile neutropenia, severe anemia, severe diarrhea, etc.V.Dosage/Administration 1Breast Cancer/ Bladder Cancer Administer 10 mg/kg as an intravenous infusion once weekly on Days 1 and 8 of 21-day treatment cycles. Continue treatment until disease progression or unacceptable toxicity. Do not administer doses greater than 10 mg/kg.VI.Billing Code/Availability InformationHCPCS Code:∙J9317 – Injection, sacituzumab govitecan-hziy, 2.5 mg; 1 billable unit = 2.5 mgNDC:∙Trodelvy 180 mg lyophilized powder in a single-dose vial: 55135-0132-xxVII.References1.Trodelvy [package insert]. Morris Plains, NJ; Immunomedics, Inc; October 2021. AccessedFebruary 2022.2.Referenced with permission from the NCCN Drugs & Biologics Compendium (NCCNCompendium®) sacituzumab govitecan. National Comprehensive Cancer Network, 2022.The NCCN Compendium® is a derivative work of the NCCN Guidelines®. NATIONALCOMPREHENSIVE CANCER NETWORK®, NCCN®, and NCCN GUIDELINES® aretrademarks owned by the National Comprehensive Cancer Network, Inc. To view the mostrecent and complete version of the Compendium, go online to . AccessedFebruary 2022.3.Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology(NCCN Guidelines®) for Breast Cancer 2.2022. National Comprehensive Cancer Network, 2022. NATIONAL COMPREHENSIVE CANCER NETWORK®, NCCN®, and NCCNGUIDELINES® are trademarks owned by the National Comprehensive Cancer Network, Inc. To view the most recent and complete version of the Guidelines, go online to .Accessed February 2022.4.Fahrenbruch R, Kintzel P, Bott AM, et al. Dose Rounding of Biologic and CytotoxicAnticancer Agents: A Position Statement of the Hematology/Oncology PharmacyAssociation. J Oncol Pract. 2018 Mar;14(3):e130-e136.5.Hematology/Oncology Pharmacy Association (2019). Intravenous Cancer Drug Waste IssueBrief. Retrieved from /images/hopa/advocacy/Issue-Briefs/Drug_Waste_2019.pdf6.Bach PB, Conti RM, Muller RJ, et al. Overspending driven by oversized single dose vials ofcancer drugs. BMJ. 2016 Feb 29;352:i788.7.Bardia A, Mayer IA, Vahdat LT, et al. Sacituzumab Govitecan-hziy in RefractoryMetastatic Triple-Negative Breast Cancer. N Engl J Med. 2019 Feb 21;380(8):741-751. doi:10.1056/NEJMoa1814213.8.Wolff AC, Hammond EH, Allison KH, et al. Human epidermal growth factor receptor 2testing in breast cancer: American Society of Clinical Oncology/College of AmericanPathologists Clinical Practice Guideline Focused Update. J Clin Oncol 2018;36:2105-2122.9.Allison KH, Hammond EH, Dowsett M, et al. Estrogen and Progesterone Receptor Testingin Breast Cancer: ASCO/CAP Guideline Update. J Clin Oncol 38:1346-1366.10.Tagawa S, Balar A, Petrylak, et al. TROPHY-U-01: A Phase II Open-Label Study ofSacituzumab Govitecan in Patients With Metastatic Urothelial Carcinoma ProgressingAfter Platinum-Based Chemotherapy and Checkpoint Inhibitors. J Clin Oncol. 2021 Aug1;39(22):2474-2485. doi: 10.1200/JCO.20.03489. Epub 2021 Apr 30.Appendix 1 – Covered Diagnosis Codes1010C50.011 Malignant neoplasm of nipple and areola, right female breastC50.012 Malignant neoplasm of nipple and areola, left female breastC50.019 Malignant neoplasm of nipple and areola, unspecified female breastC50.021 Malignant neoplasm of nipple and areola, right male breastC50.022 Malignant neoplasm of nipple and areola, left male breastC50.029 Malignant neoplasm of nipple and areola, unspecified male breastC50.111 Malignant neoplasm of central portion of right female breastC50.112 Malignant neoplasm of central portion of left female breastC50.119 Malignant neoplasm of central portion of unspecified female breastC50.121 Malignant neoplasm of central portion of right male breastC50.122 Malignant neoplasm of central portion of left male breastC50.129 Malignant neoplasm of central portion of unspecified male breastC50.211 Malignant neoplasm of upper-inner quadrant of right female breastC50.212 Malignant neoplasm of upper-inner quadrant of left female breastC50.219 Malignant neoplasm of upper-inner quadrant of unspecified female breast C50.221 Malignant neoplasm of upper-inner quadrant of right male breastC50.222 Malignant neoplasm of upper-inner quadrant of left male breastC50.229 Malignant neoplasm of upper-inner quadrant of unspecified male breast C50.311 Malignant neoplasm of lower-inner quadrant of right female breastC50.312 Malignant neoplasm of lower-inner quadrant of left female breastC50.319 Malignant neoplasm of lower-inner quadrant of unspecified female breast C50.321 Malignant neoplasm of lower-inner quadrant of right male breastC50.322 Malignant neoplasm of lower-inner quadrant of left male breastC50.329 Malignant neoplasm of lower-inner quadrant of unspecified male breastC50.411 Malignant neoplasm of upper-outer quadrant of right female breastC50.412 Malignant neoplasm of upper-outer quadrant of left female breastC50.419 Malignant neoplasm of upper-outer quadrant of unspecified female breast C50.421 Malignant neoplasm of upper-outer quadrant of right male breastC50.422 Malignant neoplasm of upper-outer quadrant of left male breastC50.429 Malignant neoplasm of upper-outer quadrant of unspecified male breast C50.511 Malignant neoplasm of lower-outer quadrant of right female breastC50.512 Malignant neoplasm of lower-outer quadrant of left female breastC50.519 Malignant neoplasm of lower-outer quadrant of unspecified female breast C50.521 Malignant neoplasm of lower-outer quadrant of right male breastC50.522 Malignant neoplasm of lower-outer quadrant of left male breastC50.529 Malignant neoplasm of lower-outer quadrant of unspecified male breastC50.611 Malignant neoplasm of axillary tail of right female breastC50.612 Malignant neoplasm of axillary tail of left female breastC50.619 Malignant neoplasm of axillary tail of unspecified female breastC50.621 Malignant neoplasm of axillary tail of right male breastC50.622 Malignant neoplasm of axillary tail of left male breastC50.629 Malignant neoplasm of axillary tail of unspecified male breastC50.811 Malignant neoplasm of overlapping sites of right female breastC50.812 Malignant neoplasm of overlapping sites of left female breastC50.819 Malignant neoplasm of overlapping sites of unspecified female breastC50.821 Malignant neoplasm of overlapping sites of right male breastC50.822 Malignant neoplasm of overlapping sites of left male breastC50.829 Malignant neoplasm of overlapping sites of unspecified male breastC50.911 Malignant neoplasm of unspecified site of right female breastC50.912 Malignant neoplasm of unspecified site of left female breastC50.919 Malignant neoplasm of unspecified site of unspecified female breastC50.921 Malignant neoplasm of unspecified site of right male breastC50.922 Malignant neoplasm of unspecified site of left male breastC50.929 Malignant neoplasm of unspecified site of unspecified male breastC61 Malignant neoplasm of prostateC65.1 Malignant neoplasm of right renal pelvisC65.2 Malignant neoplasm of left renal pelvisC65.9 Malignant neoplasm of unspecified renal pelvisC66.1 Malignant neoplasm of right ureterC66.2 Malignant neoplasm of left ureterC66.9 Malignant neoplasm of unspecified ureterC67.0 Malignant neoplasm of trigone of bladderC67.1 Malignant neoplasm of dome of bladderC67.2 Malignant neoplasm of lateral wall of bladderC67.3 Malignant neoplasm of anterior wall of bladderC67.4 Malignant neoplasm of posterior wall of bladderC67.5 Malignant neoplasm of bladder neckC67.6 Malignant neoplasm of ureteric orificeC67.7 Malignant neoplasm of urachusC67.8 Malignant neoplasm of overlapping sites of bladderC67.9 Malignant neoplasm of bladder, unspecifiedC68.0 Malignant neoplasm of urethraD09.0 Carcinoma in situ of bladderZ85.51 Personal history of malignant neoplasm of bladderZ85.59 Personal history of malignant neoplasm of other urinary tract organAppendix 2 – Centers for Medicare and Medicaid Services (CMS)Medicare coverage for outpatient (Part B) drugs is outlined in the Medicare Benefit Policy Manual (Pub. 100-2), Chapter 15, §50 Drugs and Biologicals. In addition, National Coverage Determination (NCD), Local Coverage Determinations (LCDs), and Local Coverage Articles (LCAs) may exist and compliance with these policies is required where applicable. They can be found at:https:///medicare-coverage-database/search.aspx. Additional indications may be covered at the discretion of the health plan.Medicare Part B Covered Diagnosis Codes (applicable to existing NCD/LCD/LCA): N/AJurisdiction Applicable State/US Territory ContractorE (1) CA, HI, NV, AS, GU, CNMI Noridian Healthcare Solutions, LLCF (2 & 3) AK, WA, OR, ID, ND, SD, MT, WY, UT, AZ Noridian Healthcare Solutions, LLC5 KS, NE, IA, MO Wisconsin Physicians Service Insurance Corp (WPS)6 MN, WI, IL National Government Services, Inc. (NGS)H (4 & 7) LA, AR, MS, TX, OK, CO, NM Novitas Solutions, Inc.8 MI, IN Wisconsin Physicians Service Insurance Corp (WPS) N (9) FL, PR, VI First Coast Service Options, Inc.J (10) TN, GA, AL Palmetto GBA, LLCM (11) NC, SC, WV, VA (excluding below) Palmetto GBA, LLCNovitas Solutions, Inc.L (12) DE, MD, PA, NJ, DC (includes Arlington &Fairfax counties and the city of Alexandria in VA)K (13 & 14) NY, CT, MA, RI, VT, ME, NH National Government Services, Inc. (NGS)15 KY, OH CGS Administrators, LLC。
盐酸苯海索片联合盐酸司来吉兰片治疗帕金森病的效果
DOI:10.16662/ki.1674-0742.2023.06.118盐酸苯海索片联合盐酸司来吉兰片治疗帕金森病的效果赵臣松,应国民,秦保健单县中心医院神经内科,山东菏泽274300[摘要]目的对帕金森病患者采用盐酸苯海索片联合盐酸司来吉兰片治疗的效果进行探究。
方法随机选择2020年1月—2021年6月单县中心医院收治的90例帕金森病患者,根据患者所接受的治疗方案不同平均分。
甲组(45例)接受盐酸司来吉兰片治疗,乙组(45例)则在甲组的基础之上接受盐酸苯海索片治疗。
对比两组的治疗效果、SCOPA-AUT评分、MMSE评分、UPDRS评分、氧化应激指标。
结果乙组的总有效率(97.78%)高于甲组(80.00%),差异有统计学意义(χ2=7.200,P<0.05)。
治疗后,乙组的SCOPA-AUT评分、UPDRS评分、MMSE评分低于甲组,NOS、SOD、PON1、CGP等氧化应激指标高于甲组,差异有统计学意义(P< 0.05)。
结论在治疗帕金森患者时,联合应用盐酸苯海索及盐酸司来吉兰能够达到很好的治疗效果,可以快速缓解各项症状,提高神经功能及认知功能,还可以改善机体抗氧化应激能力。
[关键词]帕金森;盐酸苯海索片;盐酸司来吉兰片;神经功能;认知功能;抗氧化应激能力[中图分类号]R246.1 [文献标识码]A [文章编号]1674-0742(2023)02(c)-0118-05Effect of Trihexyphenidyl Hydrochloride Tablets Combined with Selegiline Hydrochloride Tablets in the Treatment of Parkinson's DiseaseZHAO Chensong, YING Guomin, QIN BaojianDepartment of Neurology, Shanxian Central Hospital, Heze, Shandong Province, 274300 China[Abstract] Objective To investigate the therapeutic effect of benhexol hydrochloride combined with selegiline hydro‐chloride tablets on Parkinson's disease patients. Methods A total of 90 Parkinson's disease patients admitted to the Single County Central Hospital from January 2020 to June 2021 were selected randomly, and they were evenly divided according to the different treatment plans they received. Group A (45 cases) received treatment with selegiline hydro‐chloride tablets, while group B (45 cases) received treatment with benhexol hydrochloride tablets on top of group A. Compared the treatment efficacy, SCOPA-AUT score, MMSE score, UPDRS score, and oxidative stress indicators be‐tween the two groups. Results The total effective rate of group B (97.78%) was higher than that of group A (80.00%), and the difference was statistically significant (χ2=7.200, P<0.05). After treatment, the SCOPA-AUT score, UPDRS score, and MMSE score of group B were lower than those of group A, while oxidative stress indicators such as NOS, SOD, PON1, CGP were higher than those of group A, and the difference was statistically significant (P<0.05). Conclu⁃sion When treating Parkinson's patients, the combination of benhexol hydrochloride and selegiline hydrochloride can achieve good therapeutic effects, quickly alleviate various symptoms, improve neurological and cognitive functions, and also improve the body's antioxidant stress capacity.[Key words] Parkinson's disease; Trihexyphenidyl hydrochloride tablets; Selegiline hydrochloride tablets; Neurological function; Cognitive function; Antioxidant stress capacity帕金森病的主要发病群体为老年人群,该病具有比较复杂的发病机制,主要是由于中脑黑质多巴[作者简介] 赵臣松(1986-),男,本科,主治医师,研究方向为神经病学。
恩格列净联合西格列汀治疗老年2_型糖尿病患者的临床疗效分析
·药物与临床·糖尿病新世界 2023年3月DOI:10.16658/ki.1672-4062.2023.05.059恩格列净联合西格列汀治疗老年2型糖尿病患者的临床疗效分析臧道军,龚红燕江苏省常州市德安医院老年内科,江苏常州213000[摘要]目的探讨老年2型糖尿病患者使用恩格列净+西格列汀治疗的临床效果。
方法选取2020年1月—2021年12月常州市德安医院接诊的100例老年2型糖尿病患者作为研究对象,根据不同用药方式分为对照组与研究组,各50例,对照组接受西格列汀治疗,研究组接受恩格列净+西格列汀治疗,就两组患者血糖指标、炎性指标、胱抑素C(Cys-C)、血尿素氮(BUN)、血同型半胱氨酸(Hcy)指标进行比较。
结果治疗前两组血糖指标相比,差异无统计学意义(P>0.05),治疗后,研究组HbA1c、FPG及2 hPG明显低于对照组,差异有统计学意义(P<0.05);治疗前两组炎性指标比较,差异无统计学意义(P>0.05),治疗后,研究组IL-4、IL-6及TNF-α明显低于对照组,差异有统计学意义(P<0.05);治疗前两组Cys-C、BUN及Hcy相比,差异无统计学意义(P>0.05),治疗后,研究组患者Cys-C、BUN及Hcy明显低于对照组,差异有统计学意义(P<0.05)。
结论对于老年2型糖尿病患者开展恩格列净+西格列汀治疗能有效改善血糖指标,降低Hcy,提升肾功能,治疗效果显著。
[关键词] 老年人群;恩格列净;西格列汀;2型糖尿病[中图分类号] R4 [文献标识码] A [文章编号] 1672-4062(2023)03(a)-0059-04Clinical Efficacy Analysis of Empagliflozin Combined with Sitagliptin in the Treatment of Elderly Patients with Type 2 Diabetes MellitusZANG Daojun, GONG HongyanDepartment of Geriatric Medicine, Changzhou De'an Hospital, Changzhou, Jiangsu Province, 213000 China[Abstract] Objective To investigate the clinical effect of treatment with empagliflozin + sitagliptin in elderly patients with type 2 diabetes mellitus.Methods A total of 100 elderly patients with type 2 diabetes mellitus admitted to Chang⁃zhou De'an Hospital from January 2020 to December 2021 were selected as study subjects. The cases were divided into control group and study group according to different medication administration, fifty cases in each. The control group received sitagliptin treatment and the study group received empagliflozin + sitagliptin treatment. The blood glu⁃cose index, inflammatory index, cystatin C (Cys-C), blood urea nitrogen (BUN), and blood homocysteine (Hcy) index were compared between the two groups.Results There was no statistically significant difference in blood glucose in⁃dexes between the two groups before treatment (P>0.05). After treatment, HbA1c, FPG and 2 hPG of the study group were significantly lower than those in the control group, the difference was statistically significant (P<0.05). There was no statistically significant difference in inflammatory indexes between the two groups before treatment (P>0.05). After treatment, IL-4, IL-6 and TNF-α in the study group were significantly lower than those in the control group, the dif⁃ference was statistically significant (P<0.05). There was no statistically significant difference in the Cys-C, BUN and Hcy between the two groups before treatment (P>0.05). After treatment, the Cys-C, BUN and Hcy of the study group were significantly lower than those in the control group, the difference was statistically significant (P<0.05).Conclusion For elderly patients with type 2 diabetes mellitus, treatment with empagliflozin + sitagliptin can effec⁃tively improve blood glucose index, reduce Hcy and enhance renal function, with significant therapeutic effects.[作者简介]臧道军(1974-),男,本科,副主任医师,研究方向为老年内科。
安捷伦产品目录
15
Real-Time PCR
16
Mx3000P QPCR System
17
Brilliant III Ultra-Fast SYBR Green QPCR and QRT-PCR Reagents
18
Brilliant III Ultra-Fast QPCR and QRT-PCR Reagents
Agilent / STRATAGENE
Agilent website: /genomics
Welgene | Agilent Stratagene
威健股份有限公司 | Stratagene 總代理
Table of Content
Table of Contents
/ XL1-Red Competent Cells SoloPack Gold Supercompetent Cells
/ TK Competent Cells Specialty Cells
/ Classic Cells / Fine Chemicals For Competent Cells
適用於 UNG 去汙染或 bisulphite
sequencing
適用於 TA Cloning
最高敏感性
取代傳統 Taq 的好選擇
-
2
威健股份有限公司 | Stratagene 總代理
PCR Enzyme & Instrument
Agilent SureCycler 8800
市場上領先的 cycling 速度和 sample 體積 10 ~ 100 μL 簡易快速可以選擇 96 well 和 384 well 操作盤 優秀的溫控設備讓各個 well 都能保持溫度的穩定 七吋的高解析度觸控螢幕讓操作上更為簡便 可以透過網路遠端操控儀器及監控儀器 Agilent 專業的技術支援可以幫助您應對各種 PCR 的問題
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Expertos en Ruido y Vibraciones
El control de vibraciones es una materia de gran importancia especialmente cuando se producen en áreas con presencia de viviendas. A diferencia del ruido aéreo, las vibraciones se transmiten por las estructuras de las construcciones, alcanzando una mayor velocidad de transmisión dependiendo de su naturaleza.
Expertos en Ruido y Vibraciones
¿Qué son las vibraciones? Vibración es el movimiento oscilante que realiza una partícula alrededor de un punto fijo
Expertos en Ruido y Vibraciones
En la ejecución de medidas orientadas a evitar la transmisión de vibraciones, es fundamental poder llevarlas a cabo con anterioridad a la ubicación de las instalaciones ruidosas, pues la ejecución de medidas correctoras, una vez puesta en funcionamiento la actividad, conlleva una mayor complejidad debido a la imprevisión de estas medidas en el origen, y por tanto, debido a la falta de espacio y de otras necesidades.
Expertos en Ruido y Vibraciones
El control de las vibraciones ha de ser tenido en cuenta tanto en los efectos producidos sobre las personas, como en los producidos en los materiales a ellas expuestos.
Modos propios de vibración
Cada frecuencia de resonancia tiene asociado lo que se llama un modo propio de vibración, es decir, una forma particular de moverse que depende de las propiedades del objeto (geometría, masa, estado de carga, condiciones de contorno, etc). Hay puntos donde la amplitud de la vibración es máxima y otros puntos donde ésta se anula (nodos).
Expertos en Ruido y Vibraciones
RESONANCIA
El período de un péndulo depende únicamente de la longitud del hilo del que pende la masa.
Experimento: en una cuerda tensa colguemos tres péndulos, dos de igual longitud y uno más largo. El período de los dos primeros es el mismo, pero distinto del tercero. Coloquemos al más largo entre los cortos. A continuación, separemos de su posición de equilibrio uno de los péndulos cortos.
MEJORAS TÉCNICAS DISPONIBLES EN LA GESTIÓN ACÚSTICA Y VIBRACIONES
Control de Vibraciones y sus medidas correctoras
Ignacio González Svantek España, S.L.
Donde: awx, awy, awz son los valores de las aceleraciones de cada uno de los tres ejes ortogonales x, y, z. kx, ky, kz son las constantes de multiplicación cuyos valores dependen de la aplicación de la medición
Expertos en Ruido y Vibraciones
UNIDADES DE MEDIDA DE VIBRACIÓN
G’s m/s2
1 G = 9,80665 m/s2
Decibelio dB
a (dB) = 20 log a (m/s2) / 10-6 (m/s2)
Expertos en Ruido y Vibraciones
RESONANCIA
Al cabo de unos instantes, comprobaremos que el otro péndulo corto se empieza a mover y en pocos segundos lo hace con tanta intensidad como el primero, de manera que no podríamos distinguir cuál de los dos ha empezado a oscilar. Por el contrario, el péndulo largo no se ve afectado por la oscilación de los otros y permanece quieto .
Expertos en Ruido y Vibraciones
Importancia de la resonancia Ingeniería civil
Movimientos sísmicos
Expertos en Ruido y Vibraciones
Expertos en Ruido y Vibrቤተ መጻሕፍቲ ባይዱciones
¿A qué se debe este fenómeno?
Los péndulos de igual longitud tienen períodos de oscilación iguales. El primero provoca la oscilación del segundo transmitiéndole energía a través del hilo que los une. El tercer péndulo asiste al fenómeno del "paso" de energía de un péndulo al otro, pero no puede participar en él porque su período de oscilación es distinto. A este tipo fenómenos se le llama de resonancia y ocurre con mucha frecuencia en la naturaleza. Cuando una causa provoca una oscilación y cerca de ella se encuentra un objeto con la misma frecuencia propia que la de la oscilación, éste empieza a vibrar.
MOVIMIENTO ONDULATORIO
Expertos en Ruido y Vibraciones
MOVIMIENTO ONDULATORIO
Tenemos un muelle en su posición de equilibrio (XO). Si tiramos de él y lo separamos de su posición de equilibrio una distancia Xm, al soltarlo, el muelle volverá a la posición de equilibrio y la rebasará una distancia Xm igual a la distancia hasta la que fue alargado al principio. Si no hay rozamiento, este movimiento, llamado oscilatorio, se repetirá indefinidamente.
Expertos en Ruido y Vibraciones
MTVV
Máximo valor de la vibración transitoria: El valor máximo de la aceleración eficaz móvil cuando el tiempo de integración es igual a 1 segundo (Slow)